
NUCHAL TRANSLUCENCY MEASUREMENT IN THE FIRST TRIMESTER OF PREGNANCY OTHER AUTOSOMAL TRISOMIES
NUCHAL TRANSLUCENCY MEASUREMENT IN THE FIRST TRIMESTER OF PREGNANCY FOR SCREENING OF TRISOMY 21 AND OTHER AUTOSOMAL TRISOMIES May 2002 MSAC reference 04 Assessment report © Commonwealth of Australia 2003 ISBN 0 642 82139 9 ISSN (Print) ISSN (Online) 1443-7120 1443-7139 First printed August 2003 This work is copyright. Apart from any use as permitted under the Copyright Act 1968, no part may be reproduced by any process without prior written permission from the Commonwealth available from the Department of Communications, Information Technology and the Arts. Requests and inquiries concerning reproduction and rights should be addressed to the Manager, Copyright Services, Info Access, GPO Box 1920, Canberra ACT 2601. Electronic copies of the report can be obtained from the Medical Services Advisory Committee’s Internet site at: http://www.msac.gov.au Hard copies of the report can be obtained from: The Secretary Medical Services Advisory Committee Department of Health and Ageing Mail Drop Point 107 GPO Box 9848 Canberra ACT 2601 Inquiries about the content of the report should be directed to the above address. The Medical Services Advisory Committee (MSAC) is an independent committee which has been established to provide advice to the Commonwealth Minister for Health and Ageing on the strength of evidence available on new and existing medical technologies and procedures in terms of their safety, effectiveness and cost-effectiveness. This advice will help to inform Government decisions about which services should attract funding under Medicare. This report was prepared by MSAC with the assistance of Dr Elmer Villanueva and Ms Alexandra Raulli of the Australasian Cochrane Centre and Mr Anthony Harris of the Health Economics Unit, Monash University. The report was endorsed by the Commonwealth Minister for Health and Ageing on 16 October 2002. Publication approval number: 3142 MSAC recommendations do not necessarily reflect the views of all individuals who participated in the MSAC evaluation. Contents Executive summary.................................................................................................ix Introduction.............................................................................................................. 1 Background .............................................................................................................. 2 Nuchal translucency measurement in the first trimester of pregnancy.................... 2 Clinical need and burden of disease ............................................................................15 Existing procedures .......................................................................................................21 Comparators ...................................................................................................................24 Current reimbursement arrangements ........................................................................26 Approach to assessment......................................................................................... 28 Review of literature........................................................................................................28 Expert advice ..................................................................................................................32 Results of assessment............................................................................................. 33 Is it safe?..........................................................................................................................33 Is it effective?..................................................................................................................46 What are the economic considerations? .....................................................................60 Conclusions ............................................................................................................ 73 Safety................................................................................................................................73 Effectiveness...................................................................................................................73 Cost-effectiveness ..........................................................................................................73 Recommendations.................................................................................................. 74 Appendix A MSAC terms of reference and membership.................................... 75 Appendix B Supporting committee..................................................................... 77 Appendix C Studies included in the review ........................................................ 79 Appendix D Existing recommendations ............................................................. 80 Appendix E Ongoing primary studies ................................................................ 87 Appendix F Summary of meta-analysis of studies on nuchal translucency measurement in the detection of trisomy 21 applying set cutoff measures.......................................................................................... 89 Appendix G Summary of comparative studies of cost-effectiveness in screening for trisomy 21 using NT ultrasound, biochemical and age screening ......................................................................................................... 91 Nuchal translucency measurement in the first trimester of pregnancy iii Appendix H Modelled economic evaluation of nuchal translucency ultrasound screening under various alternative assumptions........................... 95 Appendix I Contact details for Australian centres accredited by the Fetal Medicine Foundation...................................................................... 97 Abbreviations.........................................................................................................121 References .............................................................................................................123 iv Nuchal translucency measurement in the first trimester of pregnancy Tables Table 1 Distribution of trisomy 21 and other chromosomal abnormalities detected in a multicentre trial of screening for trisomy 21 at 10 to 14 weeks of gestation using maternal age and nuchal translucency thickness ...................................................................................................................15 Table 2 Number of chorionic villus sampling and amniocentesis procedures, Victoria, 1989–99 ....................................................................................................18 Table 3 Indications for prenatal diagnostic testing by chorionic villus sampling or amniocentesis, Victoria, 1999 ..........................................................18 Table 4 Indications for prenatal diagnostic testing via chorionic villus sampling or amniocentesis in cases where trisomy 21 was diagnosed, Victoria, 1999...........................................................................................................19 Table 5 Frequency of reported outcomes of trisomy 21, Australia, 1987–96 ..............19 Table 6 Frequency and rate of trisomy 21, by State and Territory and nationally, 1991–96 .................................................................................................20 Table 7 Frequency and rate of terminations of pregnancy following a diagnosis of trisomy 21, Australia, 1993–96........................................................20 Table 8 Frequency distribution of terminations of pregnancy for trisomy 21 by gestational age, Australia, 1993–96..................................................................21 Table 9 Number of primary studies examining the use of selected maternal biochemical markers in the screening of trisomy 21 according to trimester of pregnancy............................................................................................23 Table 10 Distribution of Australian centres accredited by the Fetal Medicine Foundation to conduct nuchal translucency measurements, by State or Territory...............................................................................................................24 Table 11 Number of services in calendar year 2000 for specific Medicare item numbers ....................................................................................................................27 Table 12 Electronic databases (including edition) used in the review .............................28 Table 13 Search terms used to identify citationsa ...............................................................28 Table 14 Criteria for validity ..................................................................................................31 Table 15 Designation of levels of evidence .........................................................................31 Table 16 Summary of published recommendations by major international organisations on the safety of diagnostic ultrasound.........................................37 Table 17 Review of studies on the effects of prenatal screening for trisomy 21 on parental psychological outcomes and behaviours.........................................43 Table 18 The generic relationship between results of a screening procedure and disease status ............................................................................................................46 Table 19 General characteristics of retrieved studies focusing on the use of nuchal translucency measurement for the screening of trisomy 21 in the first trimester of pregnancy.............................................................................49 Table 20 Pooled MoM values for selected maternal biochemical marker studies during the second trimester of pregnancy ...........................................................53 Nuchal translucency measurement in the first trimester of pregnancy v Table 21 Estimated detection rate (%) for a false positive rate of 5 per cent for selected maternal biochemical marker combinations during the second trimester of pregnancy ..............................................................................54 Table 22 Pooled MoM values for selected maternal biochemical marker studies during the first trimester of pregnancy ................................................................55 Table 23 Estimated detection rate for a false positive rate of 5 per cent for selected biochemical markers and combinations of markers measured from 9 to 11 weeks of gestation............................................................................55 Table 24 Estimated detection rate (per cent) for a false positive rate of 5 per cent for selected biochemical markers and combinations of markers, according to gestational age...................................................................................56 Table 25 General characteristics of retrieved studies focusing on the use of nuchal translucency measurement in the first trimester and maternal biochemical markers in the second trimester for the screening of trisomy 21.................................................................................................................56 Table 26 Estimated detection rate for a fixed false positive rate of 5 per cent for variations of the "integrated test"...................................................................57 Table 27 Estimated detection rate for a 5 per cent false positive rate for the combined use of NT and selected biochemical markers and combinations of markers measured from 9 to 11 weeks of gestation.............58 Table 28 Estimated detection and false positive rates for combinations of screening modalities................................................................................................59 Table 29 Prevalence of trisomy 21 per 1,000 live births by age .......................................64 Table 30 Natural history of trisomy 21 pregnancy and screening characteristics assumed in primary analysis...................................................................................66 Table 31 Screening and diagnostic test characteristics assumed in primary analysis .......................................................................................................67 Table 32 Unit cost assumptions in primary analysis...........................................................67 Table 33 NT ultrasound screening for trisomy 21 for all pregnant women (260,000 live births).................................................................................................62 Table 34 Biochemical screening for trisomy 21 for all pregnant women (260,000 live births).................................................................................................69 Table 35 Primary cost-effectiveness analysis of pregnancy screening strategies for trisomy 21 compared with next best strategy: cost per trisomy 21 case detected ............................................................................................................69 Table C-1 General characteristics of studies on NT measurement meeting entry criteria .......................................................................................................................79 Table F-1 Performance characteristics of nuchal translucency measurements in collected studies, arranged according to cutoff values.......................................90 Table H-1 Cost per trisomy 21 case detected in women aged 35 years or overa ..............95 Table H-2 Cost per trisomy 21 case detected in women aged 30 years or overa ..............96 vi Nuchal translucency measurement in the first trimester of pregnancy Table H-3 Cost-effectiveness analysis of ultrasound screening plus biochemical screening compared with biochemical screening alone: cost per trisomy 21 case detecteda .......................................................................................97 Table H-4 Incremental cost-effectiveness of ultrasound and biochemical screening compared with biochemical screening alone by age groupa ............97 Table H-5 Cost-effectiveness where NT ultrasound screening increases the uptake of screening to 100% compared with 50% for biochemical screeninga ..................................................................................................................98 Table H-6 Cost per trisomy 21 case detected where nuchal translucency ultrasound screening substitutes for first trimester dating ultrasound in 80 per cent of pregnanciesa ...............................................................................99 Table H-7 Cost-effectiveness analysis of NT ultrasound screening plus biochemical screening in the first trimester compared with biochemical screening in the second trimester with varying levels of substitution for early ultrasound scanninga .........................................................99 Table H-8 Incremental cost-effectiveness of combined nuchal translucency ultrasound plus biochemical screening and biochemical screening alone under optimistic assumptions by age groupa ..........................................102 Nuchal translucency measurement in the first trimester of pregnancy vii Figures Figure 1 Fetus with subcutaneous collection of fluid at the back of the neck ................ 2 Figure 2 Sonogram (top) and schematic (bottom) showing measurement of nuchal translucency in an 11 week old fetus ......................................................... 3 Figure 3 Calliper placement on ultrasonographic images used in nuchal translucency................................................................................................................ 4 Figure 4 Maternal age-specific prevalence of trisomy 21 at various gestational ages .............................................................................................................................. 9 Figure 5 Risk for trisomy 21 for maternal age and nuchal translucency thickness ...................................................................................................................10 Figure 6 Distribution of selected age ranges of the Australian female population, nationwide and by State and Territory, June 2000 (per cent of total women)...............................................................................................16 Figure 7 Frequency of trisomy 21 live births and stillbirths and total birth rate for Australia, 1987–96 ............................................................................................16 Figure 8 Estimated frequency of trisomy 21 births (adjusted for terminations), by maternal age (completed years) and sex in South Australia, 1960– 1989 ...........................................................................................................................17 Figure 9 Schematic of proposed screening pathway showing broad choices and decisions available to the general population and expected outcomes ...........25 Figure 10 Frequency of amniocentesis services (MBS Item 16600) by State and Territory, 1998–2000 ..............................................................................................26 Figure 11 Frequency of chorionic villus sampling (CVS) services (MBS Item 16603) by State and Territory, 1998–2000 ..........................................................26 Figure 12 Outline of the search, retrieval and selection process .......................................30 Figure 13 Estimated positive predictive value (PPV) and negative predictive value (NPV) according to prevalence in the underlying populations..............47 viii Nuchal translucency measurement in the first trimester of pregnancy Executive summary The procedure Nuchal translucency (NT) refers to an ultrasound appearance that represents a subcutaneous accumulation of fluid seen in the neck of all late first trimester fetuses. Measurement of NT involves assessing the fetus in a similar plane to that used to measure the Crown Rump Length (CRL). The measurement and accurate calliper placement for an NT measurement is more prone to error than the CRL measurement and its accuracy relies heavily on operator experience and machine quality. A sagittal sonographic section of the fetus is acquired and the maximum reproducible thickness of the subcutaneous translucency between the skin and the subcutaneous tissues is measured. Measurement combined with maternal age and gestational age is used to determine whether there is a relatively high or low of the fetus being affected by trisomy 21 (also known as Down syndrome) in the fetus. Risk assessment for trisomy 18 and 13 is also calculated. Medical Services Advisory Committee – role and approach The Medical Services Advisory Committee (MSAC) is a key element of a measure taken by the Commonwealth Government to strengthen the role of evidence in health financing decisions in Australia. The MSAC advises the Commonwealth Minister for Health and Ageing on the evidence relating to the safety, effectiveness and costeffectiveness of new and existing medical technologies and procedures, and under what circumstances public funding should be supported. A rigorous assessment of the available evidence is thus the basis of decision making when funding is sought under Medicare. A team from the Australasian Cochrane Centre and the Health Economics Unit of Monash University was engaged to conduct a systematic review of literature and other available data on NT measurement and assess the strength of the evidence. A supporting committee with relevant expertise was established to ensure the assessment was clinically relevant and took into account consumer interests. The supporting committee evaluated the evidence and provided advice to the MSAC. Nuchal translucency measurement in the first trimester of pregnancy ix MSAC’s assessment of nuchal translucency measurement Clinical need During the period from 1987 to 1996, the national rate of trisomy 21 was relatively constant at about 12.8 per 10,000 births despite an ageing population of pregnant women. In 1999, about one in every 10 pregnant women had a prenatal diagnostic test. Although diagnostic testing of women less than 35 years of age has been increasing, most diagnostic tests relate to women aged 37 years or older. Moreover, diagnostic testing continues to be performed in a large number of women for which there is no indication other than ‘age’. In young women, maternal biochemical screening and ultrasound screening for the detection of fetal abnormalities is increasingly used. Safety The literature on the safety of ultrasound in pregnancy is scant considering its widespread use and acceptance. However numerous professional organisations have released recommendations about the use of specific types of ultrasonic imaging modalities based on maternal and fetal characteristics, and the potential for adverse outcomes. Most advocate the prudent use of the technology, stressing the importance of minimum output levels and exposure times. Effectiveness When used as a single modality, screening by measurement of NT in the first trimester has a detection rate for trisomy 21 of approximately 73-82 per cent at a false positive rate (FPR) of 5-8 per cent. For maternal biochemical screening, the comparable detection rate using double markers ((pregnancy-associated plasma protein-A (PAPP-A) and free beta human chorionic gonadotrophin (free β-hCG)) in the first trimester of pregnancy is 65 per cent at a FPR of 5 per cent. For maternal biochemical screening during the second trimester, the detection rate is approximately 67-69 per cent using triple marker testing (PAPP-A, free β-hCG and either alpha-fetoprotein (AFP) or unconjugated oestriol (uE3)) and approximately 70 per cent using the quadruple marker test (PAPP-A., free β-hCG, AFP and uE3). If used in combination in the first trimester, the detection rate with a 5 per cent FPR is 86 per cent for NT screening plus double markers, 87-88 per cent for NT screening plus triple markers and 88 per cent for NT screening plus quadruple markers. While an ultrasound examination at 11-13 weeks has a number of potential clinical benefits, this analysis examines only the assessment of NT screening as an alternative to biochemical screening for trisomy 21 as this is the most common cause of intellectual disability. x Nuchal translucency measurement in the first trimester of pregnancy Cost-effectiveness Complete and reliable information on current screening activity is unfortunately not available. Therefore the cost-effectiveness of NT ultrasound screening has been examined by comparing the expected cost of universal screening using each modality compared with no screening. The cost of a universal maternal biochemical screening program in the second trimester with 100 per cent uptake of pregnant women would be approximately $21.3m. If a combined screening program (incorporating NT ultrasound plus maternal biochemical screening in the first trimester) could achieve a 20 per cent improvement in the detection rate of trisomy 21 compared with second trimester biochemical screening, then this would cost $26.7 million more per year, with 253 more trisomy 21 cases detected. This represents an incremental cost was $105,484 per extra case detected. However if screening was restricted to women aged 30 years or over, then the cost per case detected would be one third less. If screening was restricted to women aged 35 years or over, then the cost per case detected would be halved. Sensitivity analysis around the main parameters of uncertainty suggested that, depending on the true detection rate in practice and the extent of substitution for current ultrasound and follow-up diagnostic tests in high risk pregnancies, the incremental cost per extra case detected would be between $43,825 and $141,664. When first trimester NT ultrasound screening alone is compared with maternal biochemical screening in the second trimester, it costs an additional $12.5m and detects an extra 188 cases of trisomy 21. It is worth noting that none of the above cost effectiveness ratios considers the social value of and cost of care for, a trisomy 21 birth. In addition, the report focuses on the relative performance of different screening modalities in the detection of trisomy 21 although it is understood that the inclusion of other abnormalities detected by ultrasound would most likely improve the cost effectiveness of NT screening. Recommendations The MSAC considers that nuchal translucency screening (NTS), and NTS in conjunction with first trimester maternal biochemical screening (T1MBS), are safe and effective where provided by individuals with appropriate expertise in NTS. Hence NTS providers need to be appropriately accredited. However, the MSAC recommends that public funding should not be supported for NTS or NTS in conjunction with T1MBS as stand alone services, due to their poor cost-effectiveness. Consideration should be given to public funding of NTS or NTS in conjunction with T1MBS by incorporating, as far as possible, provision of the services into existing services provided in early pregnancy. The Minister for Health and Ageing accepted these recommendations on 16 October 2002 Nuchal translucency measurement in the first trimester of pregnancy xi Introduction The Medical Services Advisory Committee (MSAC) has reviewed the use of nuchal translucency (NT) measurement in the first trimester of pregnancy for screening of trisomy 21 and other autosomal trisomies. The MSAC evaluates new and existing health technologies and procedures for which funding is sought under the Medicare Benefits Scheme in terms of their safety, effectiveness and cost-effectiveness, while taking into account other issues such as access and equity. The MSAC adopts an evidence-based approach to its assessments, based on reviews of the scientific literature and other information sources, including clinical expertise. The MSAC’s terms of reference and membership are shown in Appendix A. The MSAC is a multidisciplinary expert body, comprising members drawn from such disciplines as diagnostic imaging, pathology, surgery, internal medicine and general practice, clinical epidemiology, health economics, consumer affairs and health administration. This report summarises the assessment of current evidence for NT measurement in the first trimester for screening of trisomy 21 and other autosomal trisomies. Nuchal translucency measurement in the first trimester of pregnancy 1 Background Nuchal translucency measurement in the first trimester of pregnancy The procedure In the first trimester of pregnancy, the subcutaneous accumulation of fluid behind the neck (Figures 1 and 2) was termed nuchal translucency (NT) due to features seen on ultrasound (Brizot et al 1994, Nicolaides et al 1999a). Increased NT thickness was found to be associated with chromosomal defects in a number of case series reports during the last decade (Cullen et al 1990, Watson et al 1991, Shulman et al 1992, Suchet et al 1992, van Zalen-Sprock et al 1992, Johnson et al 1993, Nadel et al 1993). As a result of this finding, it was proffered that the measurement of NT might be a useful method in the screening of trisomy 21. Together with data gathered from ultrasonographic studies performed in the second trimester, these results formed the basis of the notion that NT might be a useful component in screening for Trisomy 21. Figure 1 Fetus with subcutaneous collection of fluid at the back of the neck Source: Nicolaides et al (1999a) The procedure involves techniques similar to the measurement of the fetal crown-torump length (CRL) with a sagittal sonographic section of the fetus viewed. The maximum thickness of the subcutaneous translucency between the skin and soft tissue overlying the cervical spine is then measured, with appropriate attention being given to the distinction between the fetal skin and the amnion, as both structures appear as thin membranes (Wald et al 1998). The fetus must be away from the amniotic membrane for a measurement to be taken. The fetus may be made to move by asking the pregnant woman to cough or by tapping the maternal abdomen. Measurement is achieved by placing the ultrasound callipers on the skin and soft tissue (Figure 3). 2 Nuchal translucency measurement in the first trimester of pregnancy Figure 2 Sonogram (top) and schematic (bottom) showing measurement of nuchal translucency in an 11 week old fetus Source: Hyett et al (1999) A few points of note are summarised below (Brizot et al 1994, Nicolaides et al 1999a, Stewart and Malone 1999): • Techniques, procedures and criteria must be standardised to achieve uniform results among different operators (Monni et al 1997, Blakemore 1998). Certification of sonographers has been suggested as a prerequisite to the performance of the procedure. • Personnel performing the ultrasonographic measurements should be able to reliably measure the fetal CRL and obtain a proper sagittal image of the fetus. Braithwaite et al (1996) suggested that an operator must have the ability to obtain accurate and reproducible results over approximately 80 transabdominal scans and about 100 scans using the transvaginal route, while Roberts et al (1995) and Bewley et al (1995) believe that external motivating factors may also have roles to play. • A transabdominal sonographic scan is the approach of choice in visualising the NT. Abdominal and vaginal ultrasounds produce similar results, but while there is some evidence that the use of a transvaginal probe improves reproducibility (Braithwaite and Economides 1995), the use of the transvaginal probe has been limited to cases in which the transabdominal approach has failed. Nuchal translucency measurement in the first trimester of pregnancy 3 Figure 3 Calliper placement on ultrasonographic images used in nuchal translucency Sources: Nicolaides et al (1999a) and Hyett et al (1999) 4 • The image should be magnified such that the fetus occupies 75 - 100 per cent of the scanned image. It is also important to increase magnification to a level where 0.1 mm increments between the sonogram callipers can be identified. • The ideal fetal CRL length is between 45 and 79 mm. The optimal age of gestation is between 11 weeks and 13 weeks and six days (Wald et al 1998, Nicolaides et al 1999a). The rates of success for taking NT measurements are inversely related to gestational age, peaking at 98 - 100 per cent at 11 to 13 weeks and falling to about 90 per cent at 14 weeks (Braithwaite et al 1996, Whitlow and Economides 1998, Nicolaides et al 1999a). • Measurements should be taken with the fetus in the neutral position. The position of the fetal neck has been shown to influence the measurement of NT, with hyperextension leading to increased sizes, and flexion to decreased sizes (Whitlow et al 1998, Nicolaides et al 1999a). Nuchal translucency measurement in the first trimester of pregnancy • The maximum thickness of the subcutaneous translucency should be measured by placing the callipers on the fetal structures as shown in Figure 3 (Nicolaides et al 1999a, Herman et al 2000). At least three separate measurements should be obtained and the mean value of these measurements reported (Stewart and Malone 1999). • Continuous assessment of the quality of processes and procedures is important (Blakemore 1998) since operator variability is a potential problem (although a few studies have demonstrated that inter- and intra-observer measurements vary by about 0.5 and 0.6 mm, respectively (Pandya et al 1995a, Pajkrt et al 1998, Schuchter et al 1998)). Herman et al (1998) recommend that regular reviews (audits) be instituted using the quality of scanned images in terms of magnification, section, calliper placement, and visualisation of the amnion separate from the nuchal membrane. Information from the scan may be used to determine other outcomes, which includes determination of fetal viability, detection of multiple pregnancies, dating of pregnancy and identification of chorionicity as well as providing reassurance to parents on the fetal status. An ultrasound can detect major fetal defects, which allows medical staff to be forewarned. Some abnormalities may be treated before birth and it is sometimes important to know that an abnormality is present to allow a delivery to be brought early, thus helping to minimise continuing damage from that abnormality before birth. Some abnormalities detected on ultrasound may require urgent treatment at birth if the baby is to have the best chance of healthy survival (de Crespigny and Dredge 1997). This dating, viability and other information are currently obtained from the early ultrasound scans (referred to in this report as ‘dating ultrasound scans’). A new ultrasound marker, the status of the fetal nasal bone in the NT scan, has been observed. A study by Cicero et al (2001) found that at 11-14 weeks of gestation, the nasal bone is visible by ultrasonography in 99.5 per cent of chromosomally normal fetuses. The absence of the nasal bone is not related to the NT thickness but is an independent marker for trisomy 21. It has been suggested that the NT thickness and the nasal bone markers can be combined to provide a substantial increase in sensitivity (Cicero et al 2001). The results of the sonogram are used to arrive at an estimation of risk. The results of other tests, as well as maternal factors including previous trisomy pregnancy, adjust these estimates. This use of screening for risk assessment purposes, known as “risk screening”, allows information from various sources to be combined into a common measure (Cuckle 1994). Risk screening has its basis in statistical theory and thus has both advantages and limitations (Royston and Thompson 1992, Wald et al 1996b). For instance, empirical validation has corroborated aspects of the method, as well as confirmed the importance of explicitly specifying both the underlying assumptions and models used, and the quality of the data utilised in model generation. This is because of their impacts on outcomes, recognising that any model has limits which temper inferences that may be made (Cuckle et al 1987, Wald et al 1988, Royston and Thompson 1992, Wald et al 1996b). Nuchal translucency measurement in the first trimester of pregnancy 5 Biochemical markers Biochemical markers are currently being used to screen for trisomy 21 in both the first and second trimesters. The most commonly used biochemical markers are alphafetoprotein (AFP), intact human chorionic gonadotrophin (hCG), unconjugated oestriol (uE3) and free beta-hCG. AFP is a glycoprotein produced by the fetal yolk sac. Merkatz et al (1984) first reported that maternal biochemical concentrations of AFP were approximately 25 per cent lower in the presence of fetal Down syndrome compared to unaffected singleton pregnancies. The decrease in AFP concentrations was shown to be independent of maternal age and therefore AFP measurements have been combined to a patient’s age related risk to compute an individualised risk for fetal trisomy 21 (Palomki 1987). Human chorionic gonadotrophin is a glycoprotein made up of two subunits, an alpha subunit and a beta-subunit (Morgan 1975) produced by the placental syncytiotrophoblast (Kurman 1984). The subunits exist either in their free form or are non-covalently bound to form intact hCG. The molecule is commonly measured as either intact human chorionic hormone (hCH) or hCG plus free beta (total hCG), the role of the free alphasubunit of hCG in screening for trisomy 21 has not been fully defined (Loncar et al 1995). Levels of hCG appear in maternal blood soon after implantation and increase rapidly until 8 weeks of gestation, remains constant to 12 weeks, declines to 18 weeks and remains constant until term (Kletzky 1985). Bogart et al (1987) first reported a raised maternal serum hCG associated with fetal trisomy 21. It is thought the association is due to trisomy 21 fetuses being immature. Given that maternal serum levels of hCG decline between 12-18 weeks of gestation, an immature trisomy 21 fetus will have a higher concentration of hCG than an unaffected fetus (Chew 1995). Oestriol is produced from fetal precursors by syncytiotrophoblasts and is secreted into the maternal blood where levels rise progressively throughout gestation (Chew 1995). In maternal serum it is measured as an unconjugated steroid. The association between low second trimester uE3 levels and pregnancies with trisomy 21 was first observed by Canick et al (1988). Once again it is thought that the association is due to trisomy 21 fetuses being immature. Other markers have also been considered useful in screening for trisomy 21, including pregnancy-associated plasma protein-a (PAPP-A), the beta subunit of human chorionic gonadotrophin (free β-hCG), and unconjugated oestriol (uE3) (Wald et al 1988, 1995, 1998), schwangerschaftsprotein 1 (SP1), cancer antigen 125 (CA-125), and dimeric and α-inhibin (Wald et al 1998). Schwangerschaftsprotein or pregnancy specific beta-1 glycoprotein is a non-hormonal protein produced by the syncytiotrophoblast of the placenta. The association between raised maternal serum SP-1 levels and trisomy 21 was first observed by Bartels and Lindermann (1988). CA-125 is an antigenic determinant on a high molecular weight glycoprotein. Hogdall et al (1992) suggested that maternal CA-125 levels may be associated with fetal aneuploidy. However a study by Van Blerk et al (1992) did not find a significant association between trisomy 21 and CA-125 levels. The physiological role of CA-125 is not currently understood (Chew 1995). 6 Nuchal translucency measurement in the first trimester of pregnancy Inhibins are circulating dimeric glycoprotein hormones synthesised by the gonads and the placenta (Haddow et al 1998a) and made up of several subunits. The alpha subunit can combine with one of two beta subunits (beta-A and beta-B) to form inhibin A or inhibin B. Van Lith et al (1992) found that inhibin levels in trisomy 21 pregnancies were significantly higher than in unaffected pregnancies. The philosophy of screening in pregnancy Screening in pregnancy aims to provide couples with increased reproductive choice. It should be voluntary and women should give informed consent. Screening in pregnancy is defined as the application of a test to pregnancies where risk of a particular disorder to the fetus is unknown. Screening tests alone cannot diagnose the disorder. Women whose pregnancies are classified to be “at increased risk” are offered further evaluation by a diagnostic test that can confirm or exclude the presence of the disorder in the fetus. If the diagnostic test confirms the presence of the disorder, the prospective parents can then decide whether or not to continue the pregnancy. There are risks to the fetus and financial outlays associated with screening and subsequent diagnostic procedures. While the concept of screening may appear straightforward and beneficial, these risks and outlays must be rigorously evaluated when considering a screening test. Some diseases or conditions may not be suitable for the application of a screening program. Moreover, broad criteria have been used to determine suitability relating to issues of cost-effectiveness and ethics (Hennekens and Buring 1987). These include some indication that the disorder is considered to be serious, has a significant prevalence in the population to be screened, and a possibility of exercising reproductive choice if a fetus is shown to be affected. Screening procedures should be convenient, easy to apply, virtually free of discomfort or risk, lead to a high level of case detection and a reasonably low level of false positive test results (Rothman and Greenland 1998). These characteristics are also expected to apply to further diagnostic tests that a person may undergo, although the sensitivity, specificity, level of discomfort, and risk associated with these diagnostic tests are often higher. When multiple screening tests are used, they may be applied sequentially or simultaneously. Sequential screening, also called two-stage screening, usually involves a less expensive, invasive and uncomfortable test initially. Those who screen positive then undergo the second test, which usually has a greater sensitivity and specificity and is usually more expensive, invasive and uncomfortable than the first test. The rationale behind sequential testing is that the combination produces a reduction in false positive rates (FPRs) and a higher net specificity (Gordis 2000). Simultaneous testing, also called parallel screening, involves applying multiple screening tests simultaneously. People are usually considered to have tested positive if they have a positive result on one or more of the tests, and are considered to have tested negative if they have a negative result on all of the tests. The rationale behind simultaneous testing is achieving fewer false negatives and higher net sensitivity. The decision to use either sequential or simultaneous testing is based on a number of practical considerations, the objectives of the testing and the setting in which the testing is done (Gordis 2000). Nuchal translucency measurement in the first trimester of pregnancy 7 The autosomal trisomies Autosomal trisomies arise when individuals have 47 chromosomes, instead of the normal number of 46. Trisomy occurs during the formation of a new individual. The most common type of viable human trisomy is trisomy 21 (Down syndrome). Others include trisomy 13 (Patau syndrome) and trisomy 18 (Edwards syndrome). Trisomy 21 (Down syndrome) Trisomy 21, or Down syndrome, is named after the English physician J. Langdon Down (1826–96) who described its characteristics in 1866 (Down 1866, Booth 1985), although isolated reports suggestive of the condition may be found as far back as the fifteenth century (Smith and Berg 1976, Booth 1985). Trisomy 21 manifests as short stature; brachycephaly (having a short head) and flattening of the skull along the antero-posterior aspect; hypotonia (diminished skeletal muscle tone); upslanting palpebral fissures; epicanthus (a fold of skin over the inner corner of the eye); tiny white spots (called Brushfield spots) on the iris; flat-bridge nose; protruding tongue; small ears; short, broad hands with deviation of the fifth finger (clinodactyly); and a single transverse palmar crease (called the simian crease) formed by the fusion of the proximal and distal palmar creases. Also associated with the condition are malformations of the cardiac and gastrointestinal systems, intellectual handicap and increased risks for hydrocephalus, cerebral palsy, epilepsy, hypothyroidism, leukaemia, and the early onset of Alzheimer’s disease (Fort et al 1984, Franceschi et al 1990, McVicker et al 1994, Brookes and Alberman 1996). The historical development of screening for trisomy 21 In 1909, Shuttleworth reported on the association between increased maternal age and the risk for trisomy 21 (Shuttleworth 1909). In the 1930s, Penrose presented incidence data in five year maternal age intervals to support the claim that the probability of giving birth to an infant with trisomy 21 rises rapidly after the age of 35. At about the same time, chromosomal abnormalities were postulated to be associated with the condition. Twenty five years later, Lejeune and colleagues demonstrated that the karyotype of persons with trisomy 21 had a total chromosomal number of 47, later discovered to be an extra copy of chromosome 21 (hence the term trisomy 21) (Lejeune et al 1959a, b). Subsequent discoveries identified other forms of trisomy 21 arising from translocation and mosaicism (Korenberg et al 1992). Since the mid 1960s, karyotyping of cells from the amniotic fluid has been used to diagnose trisomy 21 (Steele and Breg 1966, Valenti et al 1968). Following the hypothesis put forth by Shuttleworth (1909) and the ability to diagnose trisomy 21 through the use of karyotypes, the early 1970s saw the use of maternal age as the screening criterion on which to recommend amniocentesis (Figure 4). The cutoff maternal age for screening, first determined to be 40 years or older, was subsequently reduced to between ages 35 and 37, following widespread acceptance of the concept and general use of amniocentesis as a diagnostic technique. Overall, these potentially identified about 30 per cent of the total population of trisomy 21 cases in the oldest 5 to 10 per cent of the total pregnant population at a FPR of 5 per cent (Wald et al 1998, Nicolaides et al 1999b). 8 Nuchal translucency measurement in the first trimester of pregnancy Kuppermann et al recently reviewed the historical bases of the 35 year cutoff age. They suggested that four reasons led to the adoption of this specific policy in the late 1970s (Kuppermann et al 1999): • the desire to restrict access to prenatal diagnostic services because of the limited availability of providers who could perform the procedures and laboratories that could conduct cytogenetic analyses (NICHHD 1979); • economic analyses suggesting that at this age prenatal diagnosis was “cost beneficial” (i.e. the costs incurred by offering testing would be more than compensated for by the savings associated with averting births of infants with Trisomy 21) (Hook and Chambers 1977); • trisomy 21 incidence data showing an increase in risk at this maternal age (Shuttleworth 1909, Penrose 1934, Hook and Chambers 1977); and • risk benefit considerations suggesting that ‘the risk for the disease should be greater than the risk of the procedure’. 10 45 yrs Log risk (%) 40 yrs 1 35 yrs 30 yrs 25 yrs 0.1 20 yrs 10 15 20 25 30 35 40 Gestational age (weeks) Figure 4 Maternal age-specific prevalence of trisomy 21 at various gestational ages Source: Snijders et al (1999b) In the 1980s, the levels of certain maternal biochemical markers were found to be different in trisomy 21 compared with unaffected pregnancies. The basis of the “triple test” – composed of three maternal biochemical markers (alpha-fetoprotein, human chorionic gonadotrophin, and unconjugated oestriol) – was used in conjunction with maternal age to potentially identify about 60 per cent of trisomy 21 pregnancies in the second trimester at an FPR of 5 per cent (Wald et al 1988, 1998, Nicolaides et al 1999a). The discovery of other markers led to a proliferation of various combinations being used. Nuchal translucency measurement in the first trimester of pregnancy 9 At about the same time, the first report of an increase in the nuchal (neck) thickness in trisomy 21 pregnancies during the second trimester was reported by Benacerraf et al (1985). Correlates during the first trimester were found a few years later by Szabo and Gellen (1990), eventually giving rise to a screening procedure that combined ultrasound markers and maternal age (Nicolaides et al 1992). Figure 5 shows the risk of trisomy 21 according to maternal age and NT thickness (Taipale and Hiilesmaa 1999). 100 10 Log risk for trisomy 21 Age & NT > 4 mm Age & NT = 4 mm 1 Age & NT = 3 mm Age alone 0.1 Age & NT < 3 mm 0.01 20 25 30 35 40 45 Maternal age (years) Figure 5 Risk for trisomy 21 for maternal age and nuchal translucency thickness Source: Taipale and Hiilesmaa (1999) Other trisomies Trisomy 13 Trisomy 13 is a frequently lethal condition characterised by multiple congenital abnormalities involving virtually every organ system. Eighty per cent of liveborn affected babies die during the first month of life (Benacerraf 1998). Trisomy 13 occurs in about one in every 5,000 births and, due to the high mortality, prevalence is low (Benacerraf 1998). The major diagnostic features of trisomy 13 are microphthalmia (small eyes), holoprosencephaly (midline facial defects) including cleft lip and palate, and polydactyly (extra digits) (de Grouchy and Turleau 1983). One or all of the three features may be absent. The syndrome may still be suspected if specific clinical features are found. Those invariably present include profound mental and developmental handicap and undescended testes. Those present in about 80 per cent of cases include hypertelorism (abnormally increased distance between eyes) and low set ears. 10 Nuchal translucency measurement in the first trimester of pregnancy In more than half of cases, the following features present: • • • • • • • • • • • • • jitteriness and apneic spells; microcephaly (small head); congenital heart disease including ventricular septal defects; epicanthal folds (folds of skin over the inner corner of the eye); presumptive deafness; micrognathia (small jaw); extra skin at the nape of a relatively short neck; capillary hemangiomata (benign tumour involving blood vessels); long and narrow hyperconvex nails; retroflexible thumbs; flexion deformities of the fingers; single transverse palmar crease; and prominent calcaneus (heel bone) (Buyse 1990). Trisomy 13 is detectable in pregnancy by ultrasound and can be diagnosed prenatally by chorionic villus sampling (CVS) or amniocentesis. Clinical examination and chromosomal analysis can be used to diagnose infants. On autopsy, it is often diagnosed without chromosomal analysis as, in addition to the different malformations, histological evidence of organ abnormality in the central nervous system, eyes, pancreas, kidneys, and ovaries are characteristic. The pancreatic abnormality is a very specific feature that confirms the diagnosis (Buyse 1990). Prenatal sonographic detection has been established at as early as 12 weeks gestation, based on the presence of holoprosencephaly. The sonographic detection rate has been reported to be between 90 per cent and 100 per cent when a complete structural survey (including the heart) is accomplished (Benacerraf 1998). Ease of detection is attributable to the severity of the defects and the number of organ systems involved. Trisomy 18 As with trisomy 13, trisomy 18 is also usually lethal with up to 90 per cent of liveborn patients dying in their first year of life (Mange and Mange 1990). Trisomy 18 occurs in about one in every 3,333 births. Due to high mortality the prevalence is low (Benacerraf 1998). Nuchal translucency measurement in the first trimester of pregnancy 11 Trisomy 18 manifests as: • • • • • • • • • • • • profound mental and developmental handicap; undescended testes (all in 100 per cent of cases); difficulty with sucking; congenital heart disease (in more than 95 per cent of cases); low-set, fawn like ears with pointed upper portions; a long skull; a narrow palate and small mouth; small eyes; a short sternum; a single umbilical artery; overlapping fingers with flexion deformity and simple arches on six or more digits; a small, narrow pelvis and limited hip abduction (all in more than 80 per cent of cases). Certain features that occur more frequently and help diagnose trisomy 18 include: • • • • • • • • • • • • • heart and kidney defects; hypertonia (increased tone of skeletal muscles); high pitched cry; prominent occiput; meningomyelocele (hernial protrusion of the spinal cord); webbed neck; short sternum; thinning of the diaphragm; horseshoe kidney; limited hip abduction; distally implanted and retroflexible thumb; simple arches on the fingertips; and rocker-bottom feet (Buyse 1990). Trisomy 18 can be diagnosed in pregnancy through CVS or amniocentesis. Sonographic detection is possible in the early second trimester in 80 per cent of affected fetuses (Benacerraf 1998). 12 Nuchal translucency measurement in the first trimester of pregnancy Abnormalities detectable by ultrasound are: • • • • • • • • • • • • • • • • • • agenesis of the corpus callosum; choroid plexus cysts; posterior fossa abnormalities; micrognathia; low set ears; microphthalmos; hypertelorism; short radial ray; clenched hand with overlapping index finger; clubbed foot or rocker-bottom feet; renal anomalies; omphalocele (congenital herniation of viscera into the base of the umbilical cord); diaphragmatic hernia; undescended testes; heart defects; intrauterine growth restriction; polyhydramnios (excess of amniotic fluid); and increased NT thickness (detectable in the first trimester). Clinical examination and chromosomal analysis can be used to diagnose infants. There are also characteristic fetal features that are suggestive of trisomy 18 such as a small placenta, decreased fetal movement and small biparietal diameter of the fetal head (Buyse 1990). A dermatoglyphic inspection of the fingers and toes for simple arch patterns is also used. Nuchal translucency measurement in the first trimester of pregnancy 13 Other Conditions that can be Detected through Ultrasound Screening There are a number of other conditions that are frequently picked up in obstetric ultrasounds. These include: • • • • • • • • • • • • • • • • • • ventriculomegaly (enlarged ventricles); enlarged cisterna magna; microcephaly; agenesis of the corpus callosum; cleft lip and palate; midface hypoplasia (incomplete development); cyclopia (eye orbits fused into one cavity containing one eye); microphthalmia; hypotelorism (abnormally decreased distance between the eyes); nuchal thickening; neural tube defects; omphalocoele (protrusion of abdominal organs through a defect in the abdominal wall); echogenic enlarged kidneys; echoic bowel; echogenic chordae tendinaea and a single umbilical artery; cardiac defects; radial aplasia (absence of the radius); and polydactyly (Benacerraf 1998). Intended purpose The ultrasonographic measurement of NT is proposed as a method of identifying fetuses at risk for abnormalities, especially autosomal trisomies. It is acknowledged that the scan may be used to determine other outcomes, including dating of pregnancy, detection of multiple pregnancies, assessment of fetal viability, identification of chorionicity, and detection of structural organ defects. Moreover, nearly all cases of neural tube defects are detected by ultrasonography at 18 weeks of gestation. This report focuses on the use of ultrasonography as a screening test during the first trimester of pregnancy for trisomy 21. 14 Nuchal translucency measurement in the first trimester of pregnancy Detection of chromosomal defects other than trisomy 21 A large multicentre study in the United Kingdom on trisomy 21 screening in the first trimester of pregnancy (using maternal age and NT thickness) found almost as many cases of other chromosomal defects as those of trisomy 21 (about 325 cases in each group) (Snijders et al 1998). The results of the study are presented in Table 1. Table 1 Distribution of trisomy 21 and other chromosomal abnormalities detected in a multicentre trial of screening for trisomy 21 at 10 to 14 weeks of gestation using maternal age and nuchal translucency thickness Number of cases (%) from a population of 96,127 Number with NT thickness for CRL above the 95th centile (%) n=4,767 Trisomy 21 326 (0.34) 234 (71.78) Other chromosomal abnormalities Trisomy 18 Turner syndrome Trisomy 13 Triploidy Other abnormalitiesa 119 (0.12) 54 (0.06) 46 (0.05) 32 (0.03) 74 (0.08) 89 (74.79) 47 (87.04) 33 (71.74) 19 (59.38) 41 (55.40) CRL = crown-to-rump length; NT = nuchal translucency a Includes deletions, partial trisomies, unbalanced translocations and sex-chromosome aneuploidies Source: Snijders et al (1998) Sonographic findings (Nicolaides et al 1999a) associated with chromosomal abnormalities include: Trisomy 18 - intrauterine growth retardation (IUGR), bradycardia (heart beating more slowly than normal), and exomphalos (protrusion of the umbilicus) (Sherod et al 1997); Trisomy 13 - IUGR, failure of cleavage of the nascent prosencephalon resulting in deficits in brain and midline facial development (holoprosencephaly), and exomphalos (Snijders et al 1999); Turner syndrome - tachycardia and IUGR (Sebire et al 1998); and Triploidy - asymmetrical IUGR, bradycardia, holoprosencephaly, exomphalos, posterior fossa cysts and molar changes in the placenta (Jauniaux et al 1997). Clinical need and burden of disease Figure 6 shows the relative distributions of resident female Australians by age and State or Territory of residence as of June 2000. Nationwide, about 45.5 per cent of women were aged between 15 and 45, 16.7 per cent were 35 – 45 years of age and 13.7 per cent were between 37 and 45 years old. Of the women aged between 15 and 45, 36.8 per cent were between the ages of 35 and 45 while 30.1 per cent were aged between 37 and 45. There are also differences among States and Territories. Nuchal translucency measurement in the first trimester of pregnancy 15 60 15 to 45 35 to 45 Percentage of female population (%) 37 to 45 50 40 30 20 10 0 Australia NSW VIC QLD SA WA TAS NT ACT Region Figure 6 Distribution of selected age ranges of the Australian female population, nationwide and by State and Territory, June 2000 (per cent of total women) Source: Australian Bureau of Statistics (2000) During the period from 1987 to 1996, the national rate of trisomy 21 was relatively constant at around 12.8 per 10,000 births despite an older population of pregnant women. The frequency of trisomy 21 births over the same period was also relatively stable (Figure 7) (Hurst et al 1999). 400 350 15 Live births Still births Total birth rate 12 Frequency 250 9 200 6 150 Rate per 10,000 births 300 100 3 50 0 0 1987 1988 1989 1990 1991 1992 1993 1994 1995 1996 Year Figure 7 Frequency of trisomy 21 live births and stillbirths and total birth rate for Australia, 1987–96 Source: Hurst et al (1999) 16 Nuchal translucency measurement in the first trimester of pregnancy While national estimates are not available, Figure 8 shows the estimated frequency of trisomy 21 births for South Australia after adjustment for prenatally diagnosed and terminated trisomy 21 pregnancies (Staples et al 1991). The sex distribution of trisomy 21 births was about 351 males (58.9%) to 245 (41.4%) females, significantly different from the nontrisomy 21 live-birth sex distribution of 51.4 per cent males to 48.6 per cent females. Even after adjustment for terminated trisomy 21 pregnancies, the difference remains statistically significant. 50 45 Maternal age (years) 40 35 30 25 20 15 10 30 20 10 0 10 20 30 Trisomy births (frequency) Figure 8 Estimated frequency of trisomy 21 births (adjusted for terminations), by maternal age (completed years) and sex in South Australia, 1960–1989 Source: Staples et al (1991) In August 2000, the Victorian Perinatal Data Collection Unit and the Murdoch Children’s Research Institute released a report on the use of prenatal diagnostic testing in the State during 1999. It highlighted the following findings (Webley and Halliday 2000): • about 8.7 per cent of all pregnant women giving birth in Victoria had a prenatal diagnostic test done; • 60 per cent of those having a test done were 37 years or older. However diagnostic testing of women less than 35 years of age continues to increase; • a large number of women aged 35 to 36 continue to undergo diagnostic testing despite no indication other than ‘age’ being reported; • twenty per cent of the women proceeding to diagnostic testing chose this course of action on the basis of an abnormal ultrasound finding while another 9.5 per cent were responding to an abnormal maternal biochemical test; • over half of abnormal ultrasounds reported abnormal NT measurements; and • 109 fetuses with trisomy 21 were detected. An abnormal ultrasound was the indication in 62 per cent of these cases. In women aged less than 35, trisomy 21 was detected in 34 fetuses. Nuchal translucency measurement in the first trimester of pregnancy 17 Table 2 shows the number of CVS and amniocentesis procedures in Victoria from 1989 to 1999 (Webley and Halliday 2000). In 1999, for the first time since 1989, there was a decrease in the number of diagnostic procedures conducted in Victoria, mainly due to a decrease in the number of CVS procedures performed in the State. Table 2 Year 1989 Number of chorionic villus sampling and amniocentesis procedures, Victoria, 1989–99 Chorionic villus sampling 694 Amniocentesis Total 1,806 2,500 1990 916 1,861 2,777 1991 1,239 2,266 3,505 1992 1,448 2,383 3,831 1993 1,537 2,524 4,061 1994 1,559 2,823 4,382 1995 1,689 2,899 4,588 1996 1,957 3,036 4,993 1997 2,072 3,211 5,283 1998 2,179 3,121 5,300 1999 2,043 3,220 5,263 Source: Webley and Halliday (2000) A majority of Victorian women undergoing prenatal diagnostic testing by CVS or amniocentesis in 1999 did so due to advanced maternal age (i.e. being 37 years of age or more) alone. Of those undergoing diagnostic testing due to abnormal ultrasound results, 52.5 per cent cited an abnormal NT measurement (Webley and Halliday 2000). These findings are presented in Table 3. Table 3 Indications for prenatal diagnostic testing by chorionic villus sampling or amniocentesis, Victoria, 1999 Indication Age of at least 37 as the only indication 37 to 39 years old 40 years or older Subtotal Other indications within current guidelines Abnormal ultrasound Abnormal nuchal translucency screening result Fetal abnormality Increased maternal biochemical screening result Previous chromosome abnormality Single gene disorder History of chromosome rearrangement History of neural tube defect Repeat test Other reasonsa Subtotal Chorionic villus sampling Amniocentesis Total 694 452 1,146 1,089 524 1,613 1,783 976 2,759 444 368 76 1 112 74 21 0 5 5 662 598 178 420 502 33 6 13 5 32 19 1,208 1,042 546 496 503 145 80 34 5 37 24 1,870 a Includes infections in pregnancy (n=12), uniparental disomy test required (n=6), egg from older donor (n=2), risk of chromosome breakage (n=1), and others (n=3) Source: Webley and Halliday (2000) 18 Nuchal translucency measurement in the first trimester of pregnancy Table 4 shows, by indication, the number of fetuses detected with trisomy 21 by CVS and amniocentesis in Victorian women in 1999 (Webley and Halliday 2000). An abnormal ultrasound was an indication for diagnostic testing in 62.4 per cent of fetuses found to have trisomy 21. Of these, 50 per cent (34 of 68) were in pregnant women aged 37 or older. Table 4 Indications for prenatal diagnostic testing via chorionic villus sampling or amniocentesis in cases where trisomy 21 was diagnosed, Victoria, 1999 Chorionic villus sampling Indication and maternal age Amniocentesis Total Abnormal ultrasound Less than 35 years 35 to 36 years 37 to 39 years 40 years and above 12 3 12 13 16 3 3 6 28 6 15 19 Subtotal 40 28 68 Less than 35 years 35 to 36 years 37 to 39 years 40 years and above 0 0 1 15 6 6 8 5 6 6 9 20 Subtotal 16 25 41 56 53 109 Other indication Total Source: Webley and Halliday (2000) The number of reported induced abortions performed after prenatal diagnosis of trisomy 21 by amniocentesis or CVS increased over the period 1987 to 1996, reaching a high of 130 in 1994 (Table 5). About 9.2 per cent of infants with trisomy 21 were stillborn and 3.9 per cent of those born alive subsequently died in the neonatal period. Table 5 Frequency of reported outcomes of trisomy 21, Australia, 1987–96 Year Stillbirths Live births Induced abortions Neonatal deaths 1987 24 265 46 16 1988 21 282 55 8 1989 19 306 37 24 1990 29 312 71 8 1991 26 305 94 12 1992 42 277 113 5 1993 25 291 117 7 1994 41 261 130 11 1995 35 284 102 11 1996 27 255 113 9 Source: Hurst et al (1999) State and Territory specific estimates of trisomy 21 from 1991 to 1996 are summarised in Table 6. New South Wales, Victoria, and Queensland consistently accounted for about 80 per cent of all cases of trisomy 21 (Hurst et al 1999). Nuchal translucency measurement in the first trimester of pregnancy 19 Rates in New South Wales were consistently greater than Australia-wide averages. In 1996, the rates of trisomy 21 in New South Wales and Queensland were more than 25 per cent above the national rate. In the ACT, rates were approximately 50 per cent higher than the national rate in 1996. Table 6 Frequency and rate of trisomy 21, by State and Territory and nationally, 1991–96 State 1991–96 1995 1996 NSW 757 (14.4)a 148 (16.9) 132 (15.3) VIC 494 (12.7) 85 (13.3) 55 (8.7) QLD 379 (13.4) 58 (12.0) 75 (15.6) WA 160 (10.5) 29 (11.4) 22 (8.6) SA 121 (10.2) 25 (12.7) 16 (8.4) TAS 44 (10.7) 7 (10.3) 2 (2.9) ACT 44 (15.4) 6 (12.2) 9 (18.8) NT 16 (7.5) 3 (8.2) 1 (2.9) 361 (13.9) 312 (12.1) Australia 2,015 (12.9) a Figures in parentheses are rates per 10,000 births Source: Hurst et al (1999) National estimates of the frequency and rate of pregnancy terminations following a diagnosis of trisomy 21 over a four year period from 1993 to 1996 are shown in Table 7 (Hurst et al 1999). Table 7 Frequency and rate of terminations of pregnancy following a diagnosis of trisomy 21, Australia, 1993–96 Type of termination 1994 1995 1996 (4.5)b 130 (5.0) 106 (4.1) 116 (4.5) Induced births (20 to 27 weeks) 20 (0.8) 25 (1.0) 17 (0.7) 4 (0.2) All terminations (up to 27 weeks) 138 (5.3) 155 (5.9) 123 (4.7) 120 (4.7) Induced abortions (< 20 1993 weeks)a 118 a Includes terminations at unstated gestational ages b Figures in parentheses are rates per 10,000 births Source: Hurst et al (1999) Table 8 shows the frequency of terminations for trisomy 21 by gestational age in Australia from 1993 to 1996. Although most terminations appear to occur between 16 and 21 weeks, data on a significant number of terminations did not allow determination of gestational age. About 5 per cent of fetuses are terminated at less than 12 weeks and another 5 per cent more than 22 weeks into the pregnancy (Hurst et al 1999). 20 Nuchal translucency measurement in the first trimester of pregnancy Table 8 a Frequency distribution of terminations of pregnancy for trisomy 21 by gestational age, Australia, 1993–96 Gestational age (weeks) Frequency (%)a < 10 5 (0.9) 10–12 27 (5.0) 13–15 46 (8.6) 16–18 107 (20.0) 19–21 113 (21.1) 22–24 22 (4.1) 25–27 1 (0.2) Unstated 215 (40.1) All terminations 536 (100.0) Frequencies in parantheses are percentages of all trisomy 21 terminations Source: Hurst et al (1999) About 80 per cent of infants with trisomy 21 survive to age five (Dupont et al 1986, Baird and Sadovnick 1987, Hayes et al 1997) with about 40 per cent of survivors having major health problems (Brookes and Alberman 1996). Despite this, life expectancy has increased dramatically throughout the world (Merrick 2000). A study published in 1982 estimated the life expectancy of an individual with trisomy 21 to be about 35 years (Thase 1982). More recent estimates indicate the average age at death to be about 55 years (compared with the general population average of 66 years) in a United States cohort (Janicki et al 1999). Findings from this study also showed that, in spite of the increased morbidity associated with the condition, adults with trisomy 21 had similar causes of death to those of the general population. A Canadian cohort reported an average life expectancy of 68 years for people with trisomy 21 (Baird and Sadovnick 1989). Existing procedures Diagnostic tests The prenatal diagnosis of autosomal trisomies is made by amniocentesis or CVS. The tests are reviewed briefly below. Safety issues are discussed in the Results section. Amniocentesis Amniocentesis was introduced in the 1880s as a surgical procedure to treat polyhydramnios. In 1952, its first application as a diagnostic procedure was pioneered by Bevis (1952), who used the technique in the prediction of haemolytic disease in the newborn. Others soon showed that it was possible to determine the sex of the fetus using the technique (Fuchs and Riis 1956). Nuchal translucency measurement in the first trimester of pregnancy 21 In 1966, Steele and Breg demonstrated the feasibility of conducting karyotypic analysis of amniotic fluid cells (Steele and Breg 1966). Shortly thereafter, both Valenti et al (1968) and Nadler (1968) reported its use in the prenatal diagnosis of trisomy 21. It has since become an integral part of obstetric care and is considered the gold standard of invasive prenatal karyotyping procedures. Amniocentesis involves the aspiration of a small amount of amniotic fluid from the amniotic cavity through an ultrasound-guided percutaneous transabdominal puncture. Karyotyping of cellular material and biochemical tests are then performed to establish diagnoses. The procedure is traditionally carried out after 15 weeks of gestation. In the late 1980s, a technique called “early amniocentesis” was introduced, allowing for the collection of amniotic fluid before 15 weeks of gestation (Drugan et al 1988, Evans et al 1988). Chorionic villus sampling (CVS) CVS involves the ultrasound-guided insertion of a needle transabdominally or a catheter transcervically to aspirate a sample of placental tissue. Its use was suggested in the late 1960s (Mohr 1968) and was performed by direct endoscopic observation (Kullander and Sandahl 1973, Hahnemann 1974) or blindly (Horwell et al 1983) prior to the advent of ultrasound. CVS permits cellular karyotyping to be performed in the first trimester. It is generally accepted that the lower limit of gestational age for sampling is about 10 weeks although its use as early as the sixth week of pregnancy has been reported (Brambati et al 1991, Brambati 1992). CVS has the risk of inducing oromandibulofacial limb (OMFL) hypogenesis syndrome (involving craniofacial and limb abnormalities) in genetically normal infants where it is carried out too early in pregnancy. The malformations are thought to be due to lack of oxygen to developing tissues from either fetal blood loss or thrombus formation at the site of biopsy (WHO and PAHO 1999, Kaufman and Chang 2000). Maternal biochemical markers Biochemical testing has had an established place in screening for trisomy 21 (Loncar et al 1995, Muller and Bussieres 1996) since the first biochemical marker, alpha-fetoprotein (AFP) was found to be lower in serum taken from women with autosomal trisomy pregnancies (Merkatz et al 1984). Recent reviews have suggested the usefulness of pregnancy-associated plasma protein-a (PAPP-A), the beta subunit of human chorionic gonadotrophin (free β-hCG), and unconjugated oestriol (uE3) (Wald et al 1988, 1995, 1998). Other markers of interest include total and alpha (α) hCG, schwangerschaftsprotein 1 (SP1), cancer antigen 125 (CA-125), and dimeric and αinhibin (Wald et al 1998). The use of particular markers or combinations of markers in screening for trisomy 21 has been studied at different times during pregnancy (Table 9). In Australia, first trimester biochemical screening uses PAPP-A and free β-hCG. 22 Nuchal translucency measurement in the first trimester of pregnancy Table 9 Number of primary studies examining the use of selected maternal biochemical markers in the screening of trisomy 21 according to trimester of pregnancy Maternal biochemical marker First trimester Second trimester uE3 9 21 AFP 26 38 CA-125 2 5 PAPP-A 12 3 Free α-hCG 6 7 SP1 6 7 α inhibin 2 4 Dimeric inhibin A 3 6 Total hCG 14 28 Free β-hCG 17 12 uE3 = unconjugated oestriol; AFP = alpha-fetoprotein; CA-125 = cancer antigen 125; PAPP-A = pregnancy-associated plasma protein-a; hCG = human chorionic gonadotrophin; SP1 = schwangerschaftsprotein 1 Source: Wald et al (1998), Cuckle and van Lith (1999) International recommendations Existing international recommendations, position papers, and best practice guidelines are described in Appendix D. Fetal Medicine Foundation The UK-based Fetal Medicine Foundation (FMF) is supported by the International Society of Ultrasound in Obstetrics and Gynecology. The FMF conducts a process of training, certification and audit to ensure a high standard for NT scanning. The FMF awards certificates of competence to sonographers who have attended a theoretical course and passed relevant practical examinations. More specifically the FMF’s process of certification in the 11-14 week NT scan includes: • attendance at a theoretical course; • submission of a logbook of 50 images of NT measurements for assessment by the FMF; and • a practical examination in the measurement of NT at a recognised training centre. The conditions for continued involvement in the FMF program are: • submission of an automated six monthly audit report that details the distribution of NT measurements for each accredited centre; • submission of a back-up disc for a more detailed annual audit; and • submission of five images of NT measurements, along with the back-up, each year. Nuchal translucency measurement in the first trimester of pregnancy 23 The certification is open to anyone involved in obstetric ultrasound, including obstetricians, radiologists, radiographers and midwives. Only by complying with the regulations will an individual remain certified in the measurement of NT by the FMF (FMF 2000). Evidence that this results in increased detection rates was provided by Stewart and Malone (1999), who compared detection rates from FMF-affiliated centres with other independent centres (72% versus 50% respectively). Australian centres The FMF has accredited 121 centres in Australia (Table 10). Pooled preliminary data from two centres, the Melbourne Ultrasound for Women and Sydney Ultrasound for Women, suggest that Australian screening results are comparable with those reported for the FMF. O’Callaghan et al (2000) published an evaluation of 2,000 cases presenting for trisomy 21 risk estimation via first trimester ultrasound measurement of NT in Newcastle, New South Wales. Over a period of two years from September 1997, the authors followed the progress (either to birth or termination) of the first 1,000 cases, calculating a screen-positive rate of about 6.8 per cent using a risk cutoff of 1 in 300. Of 11 fetuses or babies with cytogenetically proven chromosomal abnormalities, eight were trisomy 21, two were trisomy 18, and one was 47 XXX. Of these 11 cases, nine screened positive with both of the exceptions being cases of trisomy 21. Recent estimates from regular FMF audits of Australian centres note that of 48,117 scans reported, 150 cases of trisomy 21 were detected with a detection rate of 87 per cent (Amanda Sampson, member of the supporting committee for MSAC Reference 04a, personal communication, 2002). A list of centres accredited by the FMF appears in Appendix I. Table 10 Distribution of Australian centres accredited by the Fetal Medicine Foundation to conduct nuchal translucency measurements, by State or Territory State a 24 Number of centres (%)a NSW 47 (39) VIC 30 (25) QLD 18 (15) WA 16 (13) TAS 2 (2) SA 4 (3) NT 0 (0) ACT 4 (3) Total 65 (100) Calculated from information provided by Ann Robertson, Special Projects Officer, RANZCOG, personal communication, August 2002 Nuchal translucency measurement in the first trimester of pregnancy Comparators For the purposes of this evaluation it was decided to compare NT screening with second trimester biochemical screening and also with first trimester biochemical screening where data were available. The diagnostic characteristics of both NT and biochemical screening procedures were compared when used as stand-alone tests and when used in combination. The screening pathway that was used in this evaluation is shown in Figure 9. CVS = chorionic villus sampling; NT = nuchal translucency Figure 9 Schematic of proposed screening pathway showing broad choices and decisions available to the general population and expected outcomes Data gained during the NT or biochemical screening procedure can be combined with information on other relevant factors (such as the mother’s age and clinical history) to arrive at an overall risk estimate. Depending on the result, a woman may choose to undergo a more definitive yet invasive test such as amniocentesis or CVS. Nuchal translucency measurement in the first trimester of pregnancy 25 Current reimbursement arrangements Figure 10 shows the frequency of amniocentesis services by State and Territory according to Health Insurance Comission (HIC) statistics from July 1998 to June 1999 and July 1999 to June 2000. However, these figures do not include procedures performed in the public sector for which no Medicare rebate was paid. The frequency of CVS services is shown in Figure 11. 1998-1999 1999-2000 Australian States & Territories TAS ACT SA WA QLD VIC NSW 0 1000 2000 3000 4000 Frequency of amniocentesis services Figure 10 Frequency of amniocentesis services (MBS Item 16600) by State and Territory, 1998–2000 Source: Health Insurance Commission (2000) 1998-1999 1999-2000 Australian States & Territories ACT TAS SA WA QLD VIC NSW 0 1000 2000 3000 4000 Frequency of CVS services Figure 11 Frequency of chorionic villus sampling (CVS) services (MBS Item 16603) by State and Territory, 1998–2000 Source: Health Insurance Commission (2000) 26 Nuchal translucency measurement in the first trimester of pregnancy Table 11 shows the frequencies of relevant items from the Medicare Benefits Schedule (MBS). Data relating to corresponding items obtained through the public sector were not available. Table 11 MBS Item numbera Number of services in calendar year 2000 for specific Medicare item numbers Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Total 35639 97 89 116 92 107 71 96 77 87 119 121 100 1,172 35640 1,412 1,550 2,064 1,596 2,061 1,794 1,916 2,273 1,825 1,737 2,050 1,710 21,988 35643 6,217 6,341 6,776 4,985 6,500 6,138 6,044 7,140 6,076 6,534 6,422 5,805 74,888 55054 2,304 2,802 3,170 2,766 3,372 3,415 3,422 4,112 3,742 3,849 3,904 3,391 40,249 55704 – 2, 994 5, 341 4,485 6,024 5,376 5,163 5,980 5,605 5,800 5,769 5,040 57,577 55705 – 431 1,192 826 1,153 999 969 1,085 1,074 960 1, 102 951 10,742 55706 – 6,440 10,656 8,973 13,190 11,674 10,764 12,858 12,671 13,481 13,492 11,593 125,792 2,918 3,365 2,520 3,943 3,735 4,038 4,433 4,243 4,520 4,485 3,431 45,216 66740 3,585 – = data not available a Item numbers: 35639: Uterus, curettage of [by a General Practitioner], with or without dilatation (including curettage for incomplete miscarriage) under general anaesthesia or under epidural or spinal (intrathecal) nerve block where undertaken in a hospital or approved day hospital facility, including procedures to which item 35626, 35627 or 35630 applies, where performed; 35640: Uterus, curettage of [by a specialist], with or without dilatation (including curettage for incomplete miscarriage) under general anaesthesia or under epidural or spinal (intrathecal) nerve block where undertaken in a hospital or approved day hospital facility, including procedures to which item 35626, 35627 or 35630 applies, where performed; 35643: Evacuation of the contents of the gravid uterus by curettage or suction curettage not being a service to which item 35639 or 35640 applies, including procedures to which item 35626, 35627 or 35630 applies, where performed; 55054: Ultrasonic cross-sectional echography, in conjunction with a surgical procedure using interventional techniques, not being a service associated with a service to which any other item in this group applies; 55704: Pelvis or abdomen, pregnancy related or pregnancy complication, fetal development and anatomy, ultrasound scan of, by any or all approaches, performed by or on behalf of a medical practitioner, where: (a) the patient is referred by a medical practitioner; and (b) the dating of the pregnancy (as confirmed by ultrasound) is 12 to 16 weeks of gestation; and (c) the service is not associated with a service to which an item in subgroup 2 or 3 of this group applies; and (d) the referring practitioner is not a member of a group of practitioners of which the first mentioned practitioner is a member; and (e) one or more of the following conditions are present: (i) hyperemesis gravidarum; (ii) diabetes mellitus; (iii) hypertension; (iv) toxaemia of pregnancy; (v) liver or renal disease; (vi) autoimmune disease; (vii) cardiac disease; (viii) alloimmunisation; (ix) maternal infection; (x) inflammatory bowel disease; (xi) bowel stoma; (xii) abdominal wall scarring; (xiii) previous spinal or pelvic trauma or disease; (xiv) drug dependency; (xv) thrombophilia; (xvi) significant maternal obesity; (xvii) advanced maternal age; (xviii) abdominal pain or mass (xix) uncertain dates; (xx) high risk pregnancy; (xxi) previous post dates delivery; (xxii) previous caesarean section; (xxiii) poor obstetric history; (xxiv) suspicion of ectopic pregnancy; (xxv) risk of miscarriage; (xxvi) diminished symptoms of pregnancy; (xxvii) suspected or known cervical incompetence; (xxviii) suspected or known uterine abnormality; (xxix) pregnancy after assisted reproduction; (xxx) risk of fetal abnormality); 55705: Pelvis or abdomen, pregnancy related or pregnancy complication, fetal development and anatomy, ultrasound scan of, by any or all approaches, where: (a) the patient is not referred by a medical practitioner; and (b) the dating of the pregnancy (as confirmed by ultrasound) is 12 to 16 weeks of gestation; and (c) the service is not associated with a service to which an item in subgroup 2 or 3 of this group applies; and (d) one or more of the following conditions are present: (i) hyperemesis gravidarum; (ii) diabetes mellitus; (iii) hypertension; (iv) toxaemia of pregnancy; (v) liver or renal disease; (vi) autoimmune disease; (vii) cardiac disease; (viii) alloimmunisation; (ix) maternal infection; (x) inflammatory bowel disease; (xi) bowel stoma; (xii) abdominal wall scarring; (xiii) previous spinal or pelvic trauma or disease; (xiv) drug dependency; (xv) thrombophilia; (xvi) significant maternal obesity; (xvii) advanced maternal age; (xviii) abdominal pain or mass; (xix) uncertain dates; (xx) high risk pregnancy; (xxi) previous post dates delivery; (xxii) previous caesarean section; (xxiii) poor obstetric history; (xxiv) suspicion of ectopic pregnancy; (xxv) risk of miscarriage; (xxvi) diminished symptoms of pregnancy; (xxvii) suspected or known cervical incompetence; (xxviii) suspected or known uterine abnormality; (xxix) pregnancy after assisted reproduction; (xxx) risk of fetal abnormality; 55706: Pelvis or abdomen, pregnancy related or pregnancy complication, fetal development and anatomy, ultrasound scan (not exceeding one service in any one pregnancy) of, by any or all approaches, with measurement of all parameters for dating purposes, where: (a) the patient is referred by a medical practitioner; and (b) the dating for the pregnancy (as confirmed by ultrasound) is 17 to 22 weeks of gestation; and (c) the service is not associated with a service to which an item in subgroup 2 or 3 of this group applies; and (d) the referring practitioner is not a member of a group of practitioners of which the first mentioned practitioner is a member; and (e) the service is not performed in the same pregnancy as item 55709; 66740: Quantitation, in pregnancy, of alpha-fetoprotein, human chorionic gonadotrophin, oestriol and any other substance to detect foetal abnormality, including a service described in one or more of items 66743, 66746, 73527 and 73529 (if performed) - one patient episode in a pregnancy. Source: Commonwealth Department of Health and Aged Care (1999). Nuchal translucency measurement in the first trimester of pregnancy 27 Approach to assessment Review of literature This review follows methods outlined in the Cochrane Collaboration Handbook (Clarke and Oxman 1999), the recommendations of the Cochrane Methods Group on Systematic Reviews of Screening and Diagnostic Tests (Cochrane Methods Group 1996), and other published guidelines on the assessment of diagnostic tests (Irwig et al 1994). Literature search The medical literature was searched to identify relevant studies and reviews for the period between 1966 and 2000. Searches were conducted using the databases shown in Table 12 and the search terms within Table 13. Table 12 Electronic databases (including edition) used in the review Database Period covered Best Evidence (Ovid) 1991 to March/April 2000 Biological Abstracts (Ovid) 1980 to June 2000 CINAHL (Ovid) 1982 to April 2000 Cochrane Library, including the Cochrane Database of Systematic Reviews, the Database of Abstracts of Reviews of Effectiveness, the Cochrane Controlled Trials Register, the Health Technology Assessment database, and the NHS Economic Evaluation database Issue 2, 2000 HealthSTAR 1975 to May 2000 Journals@Ovid 1993 to 2000 Medline (Ovid) 1966 to July 2000 National Guidelines Clearinghouse June 2000 Science Citation Index June 2000 Table 13 Search terms used to identify citationsa Safety (((prenatal or pre-natal or antenatal or ante-natal) and ultrasound) or (ultrasound and pregnancy)) and (adverse event or safety) (amniocentesis or chorion villus sampling) and (((first trimester or second trimester) and pregnancy) or ((prenatal or pre-natal or antenatal or ante-natal) and (diagnosis or screening))) ((prenatal or pre-natal or antenatal or ante-natal) and (diagnosis or screening)) and (anxiety or attitude to health or patient acceptance of health care) Ethics ((ethics or ethical) and ((prenatal or pre-natal or antenatal or ante-natal) and (diagnosis or screening))) Effectiveness (((((prenatal or pre-natal or antenatal or ante-natal) and (diagnosis or screening)) or ((prenatal or prenatal or antenatal or ante-natal) and ultrasound)) and (neck and first trimester pregnancy)) (((((prenatal or pre-natal or antenatal or ante-natal) and (diagnosis or screening)) or ((prenatal or prenatal or antenatal or ante-natal) and ultrasound)) and (pregnancy associated plasma protein A or human chorionic gonadotrophin or unconjugated oestriol or alpha-fetoprotein or cancer antigen 125 or dimeric inhibin A or alpha inhibin) Cost-effectiveness a 28 (((prenatal or pre-natal or antenatal or ante-natal) and (diagnosis or screening)) or ((prenatal or prenatal or antenatal or ante-natal) and ultrasound)) and (cost or cost-effectiveness)) Terms were searched as text words. A medical subject heading (MeSH) term search was conducted if allowed by the database Nuchal translucency measurement in the first trimester of pregnancy Electronic searching included the Internet sites of the following health technology assessment groups: • International Society of Technology Assessment in Health Care; • International Network of Agencies for Health Technology Assessment (and 28 • • • • • • • • • • member organisations); British Columbia Office of Health Technology Assessment (Canada); German Health Technology Assessment Project; Center for Medical Technology Assessment (Sweden); Scottish Health Purchasing Information Centre (Scotland); Medical Technology and Practice Patterns Institute (USA); National Institutes of Health (NIH) Office of Medical Applications of Research (USA); Office of Technology Assessment Archive (USA); RAND Corporation (USA); University HealthSystems Consortium (USA); and the Veterans Affairs Technology Assessment Program (USA). Relevant textbooks and book chapters were also obtained and read. Reference lists of publications were scanned and pertinent citations retrieved. Entry criteria Collected citations were filtered through a multilevel review process involving a team with skills in clinical medicine, public health, health information, basic science, clinical epidemiology and biostatistics. Articles were excluded if they met any of the following criteria: • focus was not on the measurement of NT or biochemical screening for trisomy 21 in the first or second trimesters of pregnancy; • studies enrolled fewer than 10 subjects; • studies neither presented data on the diagnostic characteristics of NT or biochemical screening nor contained data data from which these characteristics could be derived; • articles included data published in later studies; or • publications were in a language other than English. Figure 12 summarises the process of article selection and exclusion. An initial assessment of abstracts of collected citations selected out articles that did not meet inclusion criteria. Ambiguous or uncertain citations proceeded to the next stage. From the initial search of 1,269 articles there were 1,065 articles rejected. This left 204 articles to be assessed in full text form. Nuchal translucency measurement in the first trimester of pregnancy 29 The full text of the remaining citations was retrieved for further assessment. Any final decision made to reject a given article was based on a thorough reading of the complete article. Only the studies that successfully passed through all stages of this process are discussed in this report (138 studies). Initial search 1,269 articles Initial rejection 1,065 articles Full-text assessment 204 articles Final rejection 66 articles Articles accepted 138 articles Figure 12 Outline of the search, retrieval and selection process Data extraction The review extracted data from the included articles using an instrument created for this assessment. Two independent reviewers examined each article with differences in opinion resolved through consensus. Assessment of quality All accepted articles underwent an assessment of study quality based on criteria that focus on important aspects of study design (Table 14). 30 Nuchal translucency measurement in the first trimester of pregnancy Table 14 a Criteria for validity Criterion Description Possible ratings A Was the test compared with a valid reference standard? Yes, No, Unclear B Were the test and reference standard measured independently (blind) of each other? 1 – 5a C Was the choice of patients who were assessed by the reference standard independent of the test’s results? Yes, No, Unclear D Was the test measured independently of all other clinical information? Yes, No, Unclear E Was the reference standard measured before any interventions were started with knowledge of test results? Yes, No, Unclear Rating scale used is: 1 = test measured independently of reference standard and reference standard independently of test; 2 = test measured independently of reference standard but not vice versa; 3 = reference standard measured independently of test but not vice versa; 4 = test and reference standard not measured independently of each other; 5 = unclear Source: Cochrane Methods Group (1996) The review assessed evidence presented in the selected studies and classified it according to the National Health and Medical Research Council (NHMRC) revised hierarchy of evidence (Table 15). Table 15 Designation of levels of evidence I Evidence obtained from a systematic review of all relevant randomised controlled trials. II Evidence obtained from at least one properly designed randomised controlled trial. III-1 Evidence obtained from well-designed pseudo-randomised controlled trials (alternate allocation or some other method). III-2 Evidence obtained from comparative studies with concurrent controls and allocation not randomised (cohort studies), case-control studies or interrupted time series with control group. III-3 Evidence obtained from comparative studies with historical control, two and more single arm studies or interrupted time series without a parallel control group. IV Evidence obtained from case series, either post-test or pre-test and post-test. Source: NHMRC (2000) Conduct of meta-analysis Methods to assess heterogeneity in meta-analyses of diagnostic test accuracy are not fully developed. When the degree of homogeneity was acceptable on clinical grounds, summary estimates were derived using a random-effects model (DerSimonian and Laird 1986). Standard statistical convention was followed and a type I error (the probability of detecting a difference when one is not actually present) was assumed for all analyses to be 5 per cent (α=0.05). Nuchal translucency measurement in the first trimester of pregnancy 31 Expert advice Contact with primary authors and experts, in Australia and internationally, was initiated to supplement evidence drawn from the literature search. A supporting committee with expertise in obstetrics and gynaecology, clinical biochemistry, general practice, public health and consumer issues was established to evaluate the evidence and provide advice to the MSAC from a clinical perspective. In selecting members for supporting committees, the MSAC’s practice is to approach the appropriate medical colleges, specialist societies and associations for nominees. Membership of the supporting committee is provided at Appendix B. 32 Nuchal translucency measurement in the first trimester of pregnancy Results of assessment Is it safe? There are two key safety issues relating to NT measurement that need to be considered. These relate to the use of ultrasound in pregnancy and issues surrounding follow-up diagnostic tests for trisomy 21. A brief discussion of relevant psychological and ethical issues is also provided in this report. Safety of ultrasound in pregnancy The literature focusing on the safety of ultrasound in pregnancy is scant relative to its widespread use and acceptance, although it is expected that major adverse events would have come to light due to the ubiquitousness of the procedure. Miller et al (1998) raised concerns regarding studies having been conducted on older devices that did not have the power outputs of more modern equipment. US National Institutes of Health Consensus Development Program In 1984, the NIH and the Food and Drug Administration (FDA) Center for Devices and Radiological Health convened a joint Consensus Development Conference to examine the use of diagnostic imaging in pregnancy (Anonymous 1984). The theoretical risks posed by ultrasound to the fetus and the pregnant woman were among the many questions considered. The panel of experts conducted extensive reviews of the available primary literature and examined reports by the FDA, the Bureau of Radiological Health, the World Health Organization, and the National Council on Radiation Protection and Measurement. The panel observed that while epidemiological studies tended to support the safety of diagnostic ultrasound exposure in humans, with observed teratologic effects in animal studies seemingly due to exposure to significant hyperthermia, the effects were too important to be ignored. The panel recommended that further studies be conducted to determine the effects of ultrasound on biological systems, with the aim of identifying risk estimates applicable to human fetal development. European Federation of Societies for Ultrasound in Medicine and Biology and the World Federation of Ultrasound in Medicine and Biology A clinical safety statement released by the European Federation of Societies for Ultrasound in Medicine and Biology (EFSUMB) in 1998 noted that modern ultrasound equipment is subject to regulation of output signals (Anonymous 1998a). Nuchal translucency measurement in the first trimester of pregnancy 33 Provided that equipment meets international or specific national safety requirements and is used by competent and trained personnel, the EFSUMB makes the following recommendations: • there is no reason to withhold B- or M-mode scans for any clinical application, including the routine clinical scanning of every woman during pregnancy; • pulsed Doppler at maximum machine outputs and colour flow imaging with small colour boxes have the greatest potential for biological effects. In general, the informed use of Doppler ultrasound is not contraindicated. However, significant thermal effects on bone surfaces could not be excluded, especially at maximum machine outputs. Limited exposure of critical structures including regions of bone and gas is recommended; and • until further scientific information is available, prudence in limiting exposure of critical structures such as the fetal skull or spine during pulsed or colour Doppler scans, should be observed. In a subsequent statement published in the same year, the World Federation of Ultrasound in Medicine and Biology (WFUMB) endorsed similar statements on the biological effects of ultrasound (Anonymous 1998b). Relevant observations include: 34 • known diagnostic ultrasound equipment that is used for simple B-mode imaging, operates at acoustic outputs that are not capable of producing harmful temperature rises. Its use in medicine is, therefore, not contraindicated on thermal grounds. This includes endoscopic, transvaginal and transcutaneous applications; and • some Doppler diagnostic equipment has the potential to produce biologically significant temperature rises, specifically at bone/soft tissue interfaces. The effects of elevated temperatures may be minimised by keeping the time for which the beam passes through any one point in tissue, as short as possible. Where output power can be controlled, the lowest available power level consistent with obtaining the desired diagnostic information should be used. Although the data on humans are sparse, it is clear from animal studies that exposures resulting in temperatures less than 38.5°C can be used without reservation on thermal grounds. This includes obstetric applications. Nuchal translucency measurement in the first trimester of pregnancy Based on the EFSUMB and WFUMB statements, international consensus was achieved on the following recommendations: • • • Thermal effects – a diagnostic exposure that produces a maximum in situ temperature rise of no more than 1.5°C above normal physiological levels (37°C) may be used clinically without reservation on thermal grounds; – a diagnostic exposure that elevates embryonic and fetal in situ temperature above 41°C (4°C above normal) for five minutes or more should be considered potentially hazardous; – for diagnostic ultrasound systems that are capable of producing a tissue temperature increase greater than 1.5°C above normal, users should be provided with worst-case estimates of likely temperature increase for all pertinent operating modes; – the risk of adverse effects from heating increases with the duration of exposure. Thus, safety guidelines should include an appropriate duration factor; and – care should be taken to avoid unnecessary additional embryonic and fetal risk from ultrasound examinations of febrile patients. Non thermal effects – the possible occurrence of cavitation, either inertial or non-inertial, should be considered in assessing the safety of diagnostic or other forms of medical ultrasound; and – caution is required in applying results of studies on in vitro ultrasound biological effects, to medical ultrasound exposures in vivo. Education – diagnostic ultrasound has the potential to produce both false positive and false negative results. Misdiagnosis is far more dangerous than any effect that might result from ultrasound exposure. For this reason diagnostic ultrasounds should only be performed by people with sufficient training. American Institute of Ultrasound in Medicine The American Institute of Ultrasound in Medicine (AIUM) noted that ‘there are no confirmed biological effects on patients or instrument operators caused by exposures from present diagnostic ultrasound instruments. Although the possibility exists that such biological effects may be identified in the future, current data indicate that the benefits to patients of the prudent use of diagnostic ultrasound outweigh the risks, if any, that may be present’ (AIUM 2000). Nuchal translucency measurement in the first trimester of pregnancy 35 Australasian Society for Ultrasound in Medicine In late 1998 the following safety statements and recommendations were endorsed by the Australasian Society for Ultrasound in Medicine (ASUM 1998): 36 • grey scale imaging (by transcutaneous and transvaginal routes) is a well established procedure in diagnostic medicine. Nevertheless care should be exercised to ensure that examinations are performed prudently using the ALARA (as low as reasonably achievable) principle of applying the lowest acoustic output and dwell time necessary to obtain the necessary diagnostic information; • diagnostic exposure that produces a maximum temperature rise of 1.5°C above normal physiological levels may be used without reservation in clinical examination; • diagnostic exposure that elevates embryonic or fetal temperature above 41°C (i.e. 4°C above normal body temperature) for five minutes or more should be considered potentially hazardous; and • due to the potential for hyperthermia, duplex/Doppler ultrasound in febrile patients might present an additional embryonic or fetal risk. Nuchal translucency measurement in the first trimester of pregnancy Table 16 Issue Summary of published recommendations by major international organisations on the safety of diagnostic ultrasound ASUM WFUMB B-mode Exercise prudent use. Not contraindicated on thermal grounds when no gas is present. Doppler Use ALARA output and dwell time, particularly when bone or gas is present. Exposure levels User should pay attention to output or risk indicator. Thermal effects As per WFUMB + effects of heating reduced by minimising duration of exposure. Duplex/Doppler in febrile patients may present additional risk to the fetus or embryo. Nonthermal effects Presence of contrast agents should be considered in benefit/risk assessment of ultrasound examinations. First trimester exposure Use lowest available power consistent with obtaining good diagnostic information. Minimise time that the beam passes through one point. EFSUMB AIUM ODS/FDA Prudent use involves minimum output levels and exposure times. Refer to ODS. FDA upper intensity limit: ophthalmic exposures at <50 mW/cm2; others at <720 mW/cm2. Temperature rises ≤1.5°C (38°C) can be used without reservation. Obstetric exposures resulting in a temperature increase of 4°C for 5 minutes or more are potentially hazardous. At the FDA regulatory limit, the maximum temperature increase in the conceptus can exceed 2°C. FDA does not regulate TI. For general use, TI should be <6. When gas (including contrast agents) is present, exposure levels and duration should be reduced to the minimum to obtain required information. The threshold value of MI for extravasation of blood cells in mouse lungs is approximately 0.3. For general use, MI should be <1.9. Absence of knowledge about first trimester ultrasound exposures means that care is required in application of transvaginal ultrasound in early pregnancy. Epidemiology Insufficient evidence of a causal relationship between diagnostic ultrasound and adverse effects. Other Non medical use discouraged. AIUM = American Institute of Ultrasound in Medicine; ALARA = as low as reasonably achievable; ASUM = Australasian Society for Ultrasound in Medicine; EFSUMB = European Federation of Societies for Ultrasound in Medicine and Biology; FDA = Food and Drug Administration; MI = mechanical index; ODS = output display standard; TI = thermal index; WFUMB = World Federation of Ultrasound in Medicine and Biology Source: Barnett et al (2000) Nuchal translucency measurement in the first trimester of pregnancy 37 International recommendations and guidelines Barnett et al (2000) summarised published recommendations by major organisations (Table 16). They also identified gaps in which they believed research and policy to be required as follows: Use of ultrasound in the first trimester There is no published international policy on the safe use of ultrasound to examine uncomplicated pregnancy in the first trimester. Effects on the human central nervous system • Biological effects on the central nervous system may be found when sufficiently sensitive end points are used. Careful examination is needed to determine the possibility of adverse developmental effects and to establish whether there is a plausible epidemiological link to ultrasound exposure; and • Data are needed on human exposures at the levels currently available for obstetric examinations. Non clinical use of ultrasound imaging It would be appropriate for an international authority to develop guidelines since there is no agreed policy on clinically unnecessary, possibly inappropriate, uses of ultrasound. International Society for Ultrasound in Obstetrics and Gynecology The International Society for Ultrasound in Obstetrics and Gynecology (ISUOG) released a statement in 2000 affirming the recommendations that various organisations had previously made. The ISUOG stated that: • real time B-mode imaging is not contraindicated for routine clinical scanning of every pregnant woman; • the risk of damage to the fetus due to teratogenic agents such as heat, is great in the first trimester. Exposure time and output should be kept to the lowest levels consistent with obtaining diagnostic information and be limited to medically indicated procedures; and • education of ultrasound operators is of the utmost importance. Primary studies on second trimester exposure As previously noted, primary studies retrieved by the search focused on its use in the second trimester of pregnancy. The use of ultrasound in pregnancy has been hypothesised to be associated with increased risks of intrauterine growth retardation and low birth weight, childhood malignancies, delays in neurological development, and poor school performance (Pastore et al 1999, Ziskin 1999). 38 Nuchal translucency measurement in the first trimester of pregnancy Newnham et al (1993) studied 2,834 pregnant Western Australian women in a randomised controlled trial (RCT) examining the effects of intensive ultrasound and continuous Doppler flow imaging (at gestational ages of 18, 24, 28, 34 and 38 weeks) versus a single scan at 18 weeks. Further scans were conducted only at the request of a clinician. Women attending the public antenatal clinic at King Edward Memorial Hospital or the nearby private practices between May 1989 and November 1991 were enrolled. One of the criteria for enrolment was a gestational age of between 16 and 20 weeks. Ultrasound examinations were conducted by qualified sonographers. Measurements were made of the fetal biparietal and occipitofrontal diameters, head circumference, abdominal circumference, and femur length. The amniotic fluid volume was classified into one of five categories and the placental morphology and location carefully described. After the ultrasound, each woman in the intensive group had further biometry with amniotic fluid index calculated and umbilical cord and placental sites recorded. Systolic/diastolic ratios were determined from waveforms in the umbilical and arcuate arteries located within the placental vascular bed. Details of pregnancies, deliveries, and neonatal outcomes were taken from hospital notes. The allocation of each newborn to birth weight percentiles was done with charts that take into account variations based on maternal height, parity and fetal sex. Poor obstetric history was defined as three or more first trimester abortions, one or more second trimester abortions, a perinatal death or a preterm birth. Obstetric intervention was defined as induction of labour or elective caesarean section. Those receiving more frequent ultrasound examinations were found to be at increased risk of delivering infants with lower birth weights. Compared with controls, these women were 35 per cent (95% confidence interval (CI)=9, 67%; P=0.006) more likely to deliver babies at less than the 10th percentile for weight. The authors suggest that this is more likely to be due to restrictions in bone growth rather than to a reduction in placental nutrient supply (Evans et al 1996). Results from follow-up of the infants showed that the differences in birth weight were no longer present at one year of age. Weight and length at one year were similar between the groups, with babies exposed to more frequent ultrasound examinations in the womb gaining weight more rapidly postnatally than those in the control group (Macdonald et al 1996). Larger studies have failed to support this finding (Ziskin 1999). Using a database of more than 13,000 pregnancies, Grisso et al (Grisso et al 1994) found no suggestion of an increased risk for low birthweight in women having ultrasound during the first two trimesters of pregnancy. An RCT in Sweden enrolling 4,637 singleton pregnancies concluded that ultrasound exposure had no impact on childhood growth rates (Kieler et al 1997). A meta-analysis published in 1999 similarly failed to uncover an association (Salvesen and Eik-Nes 1999a). Nuchal translucency measurement in the first trimester of pregnancy 39 An association between ultrasound exposure and childhood cancers has not been demonstrated. In a matched case-control study enrolling 1,284 children in China, Shu et al (1994) failed to detect an association between ultrasound exposure and acute leukaemia, brain tumours, lymphomas or other childhood neoplasms. A population based case-control study using Swedish birth, death and cancer registers from 1973 to 1989 found that children with myeloid leukaemia were just as likely to have been exposed to ultrasound during the perinatal period as controls (odds ratio (OR)=0.85; 95% CI=0.62, 1.16) (Naumburg et al 2000). Results were similar for children with lymphatic leukaemia (OR=1.00; 95% CI=0.42, 2.40). Two other studies in the mid-1980s likewise failed to demonstrate an association (Cartwright et al 1984; Kinnier, Wilson and Waterhouse 1984). A recent meta-analysis has also confirmed this conclusion (Salvesen and Eik-Nes 1999a). There is mixed information regarding the effect of ultrasound on neurological development in infants and children. A small case-control study in Canada found that children with delayed speech (as evaluated by a speech pathologist) were almost three times more likely than controls to have been exposed to ultrasound during the perinatal period (OR=2.8; 95% CI=1.5, 5.3; P=0.001) (Campbell et al 1993). In another study from Sweden, 3,265 children of mothers participating in an RCT of ultrasound screening during pregnancy were followed up until the age of nine. In selfreports, parents did not detect delays in the development of their child’s speech, motor function or behaviour. The study failed to find any association between exposure to ultrasound and neurological deficits. Odds ratios for exposure to ultrasound versus non exposure were 1.19 for delayed speech (95% CI=0.79, 1.88) and 1.08 for delayed motor development (95% CI=0.83, 1.40) (Kieler et al 1998a). Similar long term follow-up of 2,011 children of subjects enrolled in two RCTs of routine ultrasonography in pregnancy in Norway failed to detect significant differences in school performance. Selected indicators were scores for reading, spelling, arithmetic and overall performance (as rated by the children’s teachers who were blinded to exposure status) as well as the incidence of dyslexia (Salvesen et al 1992). While not in itself an adverse event, there is some evidence from randomised controlled trials (Kieler et al 1998b) and a meta-analysis (Salvesen and Eik-Nes 1999b) that suggests an association between perinatal ultrasound exposure and an increased incidence of non right-handedness, especially in boys. Risks associated with trisomy 21 diagnosis Most of the available comparative data focusing on amniocentesis and CVS are derived from studies conducted in the 1980s. Expert clinical opinion suggests that these results do not reflect current experience in Australia. Amniocentesis Severe or life threatening adverse events from amniocentesis are extremely rare. Minor medical problems are not as infrequent, with two to three per cent of women in a US national registry reporting transient vaginal spotting or amniotic fluid leakage following the procedure (NICHHD Study Group 1976). Both are self-limiting and generally require only expectant management and reassurance. 40 Nuchal translucency measurement in the first trimester of pregnancy Following the procedure, there is a 0.5-1 per cent risk of spontaneous abortion above the natural background loss rate for a given age of gestation (NICHHD Study Group 1976, Tabor et al 1986). Chorionic villus sampling Two studies examining the fetal loss rate associated with CVS have given inconsistent results. A Canadian RCT (Lippman et al 1992) did not find a statistically significant difference in fetal loss rate in women assigned to CVS compared to those receiving amniocentesis. However, a European trial enrolling women across 31 centres in the United Kingdom, the Netherlands, Finland, Denmark, Switzerland and Germany showed statistically significantly higher rates in those having CVS (MRC 1991). While CVS is known to be more technically demanding than amniocentesis, with a steeper learning curve (Brambati et al 1990, Silver et al 1990), both require technical competence in medical and nursing staff (Brambati 1992). Obstetricians performing the procedure should have adequate training and experience to be able to successfully obtain tissue samples at the initial attempt in about 99 per cent of cases (Brambati 1992). A systematic review by Alfirevic et al (2000) compared classic amniocentesis with CVS using data from three large trials and the combined experience of about 9,000 women. Differences in maternal complication rates were apparent but none were life threatening. There were no differences in the rates of neonatal complications such as stillbirths or neonatal deaths. While some technical difficulties were reported, recent data collected by various Australian hospitals show a trend of decreasing laboratory failure rates for both CVS and amniocentesis, as well as decreasing rates of mosaicism. Maternal cell contamination rates have also fallen, with this drop attributed to greater experience in the operators providing the samples. Psychological issues associated with screening for trisomy 21 Patients often view screening as a means of reassurance rather than a way of identifying risk of abnormality, and they usually do not have a omprehensive understanding of the meaning of test results (Roelofsen et al 1993, Smith et al 1994). Screening tests can be perceived to be completely accurate and most patients are not aware of their limitations (Hall et al 2000). When patients receive negative test results, some believe that this rules out the possibility of an affected pregnancy (Hall et al 2000). In the same way, a positive test result can be perceived to be confirmation of an affected pregnancy. It is important that patients undergoing a screening test are given appropriate information and personal support so that misunderstandings and patient anxiety are better managed. Mulvey and Wallace (2000) studied 100 women on their first antenatal visit to the Monash Medical Centre to assess their knowledge and attitudes regarding screening for trisomy 21. The women had limited knowledge of trisomy 21 and of the available screening and diagnostic tests. When informed, the majority of women expressed a clear preference for first trimester screening tests for trisomy 21, regardless of the rate of miscarriage of trisomy 21 pregnancies between 10 and 15 weeks of gestation (Mulvey and Wallace 2000). Nuchal translucency measurement in the first trimester of pregnancy 41 For parents, the psychological issues associated with screening for trisomy 21 are anxiety and, on confirmation of a positive test result, emotions such as shock, disbelief, anger, resentment, bitterness, hostility, fear, loneliness and helplessness (Department of Human Services 2000). Having a child with a disability affects the whole family. Some common problems include pressure on the parents’ relationship with mothers often providing most of the care and fathers feeling left out. Fathers may miss out on support groups because they are at work. Siblings are also affected with many becoming resentful because they get less parental attention (Department of Human Services 2000). Table 17 lists studies that assess pregnant women’s experiences with screening tests for trisomy 21. In particular, they assessed women’s emotional well being in terms of anxiety and depression levels. All these studies have shown that, to some degree, screening causes anxiety. This is inevitable as screening identifies individuals with an increased risk of a serious medical disorder. Several authors have regarded anxiety as an adverse outcome, but it can only be interpreted as such if it is excessive and could have responsibly been avoided. While it is difficult to ascertain what level of anxiety the subjects experienced, it is clear from the studies that the degree of anxiety can be lessened by properly informing women of the risks and limitations of the screening tests and through appropriate counselling (Statham and Green 1993). 42 Nuchal translucency measurement in the first trimester of pregnancy Table 17 Reference Review of studies on the effects of prenatal screening for trisomy 21 on parental psychological outcomes and behaviours Participants Results Main conclusions Hall et al (2000) Parents of trisomy 21 children born from January 1992 to December 1993 were sampled from the National Down Syndrome Cytogenetics Register. After completion of five steps to obtaining informed consent from eligible parents, a final sample of 179 mothers (86 with a false negative result, 59 not offered a test, and 34 having declined a test) and 122 fathers (55 with a false negative result, 44 not offered a test, and 23 who had declined a test) was available. Seven mothers and six fathers did not complete the adjustment measures. Overall, regardless of screening history, parents adjusted well to having a child with trisomy 21. Mothers in the false negative group had higher parenting stress and more negative attitudes towards their children than mothers who declined the test. Fathers in the false negative group had higher parenting stress scores than fathers not offered a test. Parents in the false negative group were more likely to blame others for this outcome than parents who had declined the test. Blaming others was associated with poorer adjustment in both mothers and fathers. A false negative result on prenatal screening seems to have a small adverse effect on parental adjustment which is evident two to six years after the birth of an affected child. Goel et al (1998) 2,418 pregnant women in eight geographically diverse sites across Ontario. 2,020 (83.5%) were enrolled with 1,741 (86.2%) completing the follow-up. Baseline assessment was taken at 15 to 18 weeks gestation and follow-up at 24 weeks gestation. 1,177 (67.6%) underwent maternal serum screening. No overall adverse psychological effects as a result of testing were found at 24 weeks gestation. Women with a false positive result had a mean increase in anxiety score of 1.6, whereas women with a true negative result had a mean decrease of 1.1. Women who were not tested had a mean decrease of 0.4. The mean depression score increased by 0.5 in the false positive group, was unchanged in the true negative group, and increased by 0.2 in the group not tested. The results suggest that maternal serum screening in Ontario is not causing serious psychological harm to women. Santalahti et al (1996) 45 women with positive screening results were enrolled. Two women who underwent termination of pregnancy after the diagnosis of abnormality and one patient who had a miscarriage after amniocentesis were excluded. 46 controls (either with negative screening results or who were not screened) were matched for age, parity, education and previous miscarriages. Of the remaining 42 case women, 7 decided not to undergo further diagnostic tests, 2 had second serum testing with a normal result and 33 had amniocentesis or chorionic villus sampling. The positive screening result and wait for the final results negatively affected most of the 33 women and 6 were still worried after receiving final reassuring results. Receiving a positive serum screening result has a negative influence on women’s emotional well being. Williamson et al (1996) 621 women older than 38 years identified from the National Down Syndrome Cytogenetics Register from 1990 to 1991 who had pregnancies known to involve trisomy 21. In 577 (93%) cases, sufficient details were available to allow the distribution of a questionnaire to a named obstetrician. Questionnaires were completed (providing details based only on documentation in the antenatal case notes) on 430 pregnancies (75%). The outcome of pregnancy was a termination in 268 (62%) cases, a live born child with trisomy 21 in 144 (34%) instances, a stillbirth for 9 (2%) patients, and a miscarriage on 8 (2%) occasions. The outcome was not known in one case. Prenatal diagnosis was not offered in 7% of pregnancies, with late booking given as the main reason. Of women offered prenatal diagnosis, 76% accepted. There was no report of a normal fetus having been terminated as a consequence of incorrect prenatal diagnosis. However, in 10% of cases examined in the laboratory, the diagnosis of trisomy 21 could not be confirmed. The results suggest late booking was the main factor precluding the offer of prenatal diagnosis to women older than 38 years in the UK. The rate of confirmation of trisomy 21 in terminated fetuses was incomplete. Thornton et al (1995) 1,691 women booking antenatal care before 15 weeks gestation were randomised to three groups: control (routine information, n=587), individual information (n=561), and class information (n=563). Attendance at classes was lower than at individual sessions (OR=0.45). Uptake of screening for trisomy 21 was slightly increased when extra information was offered individually (OR=1.45). Offer of individual information reduced anxiety later in pregnancy and had no adverse effects. Women offered extra information had improved understanding and were more satisfied with the information they received. The results suggest that the offer of extra information does not cause undue anxiety and reduces the uptake of blood tests when background uptake rate is high (but not when it is low). High uptake of prenatal blood tests suggests compliant behaviour and the need for more information. Kidd et al (1993) Women less than 30 years of age presenting for antenatal care at less than 16 weeks of pregnancy. 309 were tested and 30 were not. 21 of 309 did not think that they had been tested; seven of 30 who were not tested thought they had been. There were no significant differences between the groups in anxiety, certainty or worry about the baby’s health. The results suggest that receipt of a negative result does not provide reassurance. Nuchal translucency measurement in the first trimester of pregnancy 43 Table 17 (contd) Review of studies on the effects of prenatal screening for trisomy 21 on parental psychological outcomes and behaviours Reference Participants Results Main conclusions Smith et al (1994) 353 women at less than 18 weeks gestation who attended one of five hospitals in the UK that offered routine serum screening for trisomy 21. 72% of women knew the screening test was a blood test, and 89% knew it was performed between 16 and 18 weeks of pregnancy. 32% knew that most women with positive results have normal babies and 38% knew that the test screened for trisomy 21. Screening program counselling did not manage the women’s information needs adequately, particularly the implications of screening results. Roelofsen et al (1993) Group A were women younger than 36 years who were not eligible for prenatal diagnosis (n=105). Group B were women aged 36 years or more who were eligible for prenatal diagnosis and who underwent either chorionic villus sampling or amniocentesis but not serum screening (n=155). Group A – 80% of respondents opted for the serum screening test either for reassurance (32%) or because it was the “obvious thing to do” (26%). 65% were not aware of possible drawbacks. 60% were satisfied with the information given. More than 70% would have accepted amniocentesis if they were found to be at increased risk. Serum screening was seen as a means of reassurance. Statham and Green (1993) 20 women who contacted Support After Termination For Abnormality about their experiences of serum screening for trisomy 21. All women were made anxious by their positive screening test regardless of who told them. The women’s experiences suggested that medical staff were unclear about the implications of screening tests and risk interpretation. Some women remained anxious even after a negative amniocentesis result. Staff did not always recognise women’s concerns while awaiting amniocentesis results. Implementation of serum screening does not always meet the needs of women that receive positive results. Appropriate support for participants should be ensured before screening is offered. Marteau et al (1992) Women younger than 38 years who had undergone maternal serum alpha-fetoprotein screening, including 346 women who received a negative result and 26 women who received an initial positive result. 637 were excluded for failure to complete questionnaires. Women who received initially positive results had higher levels of anxiety than women who received negative results. Women with initial positive results who went on to have amniocentesis were less worried about their baby’s health than those who did not have the amniocentesis. Initial positive results were associated with high levels of anxiety. The results suggest that amniocentesis can reduce anxiety following an abnormal AFP result. Keenan et al (1991) Controls (n=25) were women younger than 35 years with normal maternal serum alpha-fetoprotein results. Cases were 52 women younger than 35 years with low levels of alpha-fetoprotein. Anxiety was significantly lower in the control group than the group with low AFP before and after counselling. Counselling reduced anxiety in women with low AFP whether or not amniocentesis was performed. Although the increased anxiety level may persist at least until a definite chromosomal diagnosis by amniocentesis, this initial anxiety can be reduced through comprehensive genetic counselling. Group B – 55% would apply for serum screening for future pregnancy. 76% would accept amniocentesis if at higher risk. AFP = alpha-fetoprotein; OR = odds ratio Several studies have identified that health professionals often provide inadequate counselling support and are poorly informed, which can result in additional anxiety to patients (Marteau et al 1992b, Khalid et al 1994, Smith et al 1995, Sadler 1997). One of the ultimate choices of a screening test is termination of a pregnancy, with the personal feelings of health professionals sometimes affecting their objectivity in counselling (Khalid et al 1994). Inadequate training and the ethical dilemmas of health professionals can affect patient outcomes and should be considered when managing a screening program. Screening tests for trisomy 21 provide the opportunity to inform parents of the likelihood of birth of an affected child. This can lead to counselling about the consequences of the condition, allowing more informed decisions to be made about optimal care. The usefulness of the information derived from screening depends on parental preferences (Reed et al 1988) and has been found to be associated with the parents’ views on the acceptability of induced abortion and the perceived risk of the fetal abnormality. 44 Nuchal translucency measurement in the first trimester of pregnancy This perception of risk often plays a major role in any subsequent decisions and may sometimes outweigh the actual probability of the occurrence (Ekwo et al 1987, Drugan et al 1990, Evans et al 1990, Marteau et al 1991). Generally, this translates to the observation that the majority of women whose fetuses are diagnosed as having trisomy 21 seek elective terminations of the pregnancy (DiMaio et al 1987, Lustig et al 1988, Wald et al 1988, Haddow et al 1992, Phillips et al 1992, Spencer and Carpenter 1993, Morris et al 1994). The long term psychosocial consequences of second trimester termination of pregnancy for fetal abnormalities were examined in 84 women and their spouses two years after the event (White-van Mourik et al 1992). Most couples reported a state of emotional turmoil, with about 20 per cent of the women still experiencing regular bouts of crying, sadness and irritability. Husbands reported increased listlessness, loss of concentration, and irritability for up to 12 months after the termination. Confusing and conflicting feelings often led to social isolation and lack of communication (White-van Mourik et al 1992). Ethical issues associated with screening for trisomy 21 Screening during the prenatal period raises many important ethical concerns that relate to the pregnant woman and fetus. Most experts agree that before screening tests are performed, a clear statement of goals must be defined. Studies must show that these goals can be achieved with acceptable costs and benefits, that the population to be screened is informed about the issues, and that traditional standards of informed consent and confidentiality are maintained (Gross et al 1983, Fost 1992). Stranc et al (1997) noted four broad issues that apply to the dilemmas arising from prenatal screening and diagnosis: • Attitudes towards disability. Pressures acting on the parents to decide on termination or acceptance of a child with ‘preventable’ disability (or disability in general) must be explored. Decisions must be made about the degree of defect beyond which termination of the pregnancy is to be considered. • Clarity of benefit. The reason prenatal testing is to be performed must be made clear. The accrual of benefit to certain stakeholders must be understandable. • Freedom of choice. Prenatal diagnosis is an option exercised voluntarily by the patient. However, the physician may be required, either by law or by professional policy, to inform high risk patients of its availability. • Prioritisation. Choices may be limited by economic, as well as medical, constraints. The authors concluded that, while society may wish to reach a shared understanding of the bearing these diagnosed conditions have on the population, it will not be easy to reach this understanding (Gordon 1995, Mori et al 1995, Schafer et al 1995, Eisenberg and Schenker 1997). Nuchal translucency measurement in the first trimester of pregnancy 45 Is it effective? How is the effectiveness of screening and diagnostic tests measured? Diagnostic test results may be summarised in two-by-two tables as in Table 18. A screening test must be able to discriminate between those with disease and those without disease. In this discussion, we arbitrarily define a ‘positive’ test result as one in which disease status is implied, given a particular cutoff defined by the authors. Individuals who test positive for the disease in follow-up diagnostic testing are represented in cell ‘a’ and are called true positives (TPs). Individuals without the disease who test negative (the ‘d’ cell) are called true negatives (TNs). The result of a screening test may not reflect the actual disease status. When this occurs a false result is reported. These situations are illustrated by cells ‘b’ and ‘c’ in Table 18. In the case of the former (b), the test is positive in individuals without the disease; in the latter case (c), the test is negative in diseased individuals. These two sets of false results are called false positives (FPs) and false negatives (FNs), respectively. Table 18 The generic relationship between results of a screening procedure and disease status Screening test results True disease status Diseased Not diseased Total Positive a b a+b Negative c d c+d Total a+c b+d a+b+c+d a = number of diseased individuals detected by the test; b = number of individuals without disease detected by the test; c = number of diseased individuals not detected by the test; d = number of individuals without disease not detected by the test; a+b = total number of individuals testing positive; c+d = total number of individuals testing negative; a+c = total number of diseased individuals; b+d = total number of individuals without disease; a+b+c+d = total number of individuals studied Test accuracy is measured using four primary variables: sensitivity (Sen), specificity (Spe), positive predictive value (PPV), and negative predictive value (NPV). Sensitivity, also known as detection rate (DR), is the proportion of diseased individuals who test positive. It is a measure of the probability of correctly diagnosing a case, or the probability that any given case will be identified by the test. Referring to Table 18: DR = a TP = a + c TP + FN Specificity is the proportion of individuals without disease who test negative. It is the probability of correctly identifying a non diseased person with the screening test. Spe = d TN = b + d TN + FP The complement of specificity is called the false positive rate (FPR). FPR = 1 − Spe A successful screening test seeks to increase the detection rate for a given specificity or for a given FPR. 46 Nuchal translucency measurement in the first trimester of pregnancy Another perspective is gained by calculating the predictive values, PPV and NPV. The PPV is the probability that a person with a positive test has the disease. The NPV is the probability that a person with a negative test does not have the disease. The predictive values of a screening test depend on the detection rate, the specificity of the test and the prevalence of the condition in the population in which the test is being used. PPV = NPV = a TP = ; a + b TP + FP d TN = TN + FN c + d In many situations, the predictive values of a diagnostic test are more relevant to patients than its detection rate and specificity. However, the predictive values are directly related to the underlying prevalence of the condition in the population through the following expressions: PPV = NPV = DR × Prevalence (DR × Prevalence ) + FPR (1 − Prevalence [(1 − FPR ) ; (1 − FPR ) × (1 − Prevalence ) ) × (1 − Prevalence )] + [(1 − DR ) × Prevalence ] Therefore, a screening test is most effectively applied in populations at high risk for the condition (Figure 13). Screening the entire population for a relatively infrequent condition may yield comparatively few previously undiagnosed cases for the effort involved. 100 Estimated PPV or NPV (per cent) 90 80 70 60 50 40 30 20 10 0 0 10 20 30 40 50 60 70 80 90 100 Prevalence (per cent) Note: Detection rate and specificity are both set at 95% Figure 13 Estimated positive predictive value (PPV) and negative predictive value (NPV) according to prevalence in the underlying populations Nuchal translucency measurement in the first trimester of pregnancy 47 Likelihood ratios (LRs) offer the benefit of adjusting estimates of risk prior to undergoing the screening test (called the pre-test or prior odds of disease) to arrive at the probability of disease once test results are known (called the post-test or posterior odds of disease). Seen in another way, LRs express the odds that a given level of a test result would be expected in a patient with the condition compared with one without the condition. The likelihood ratio is related to detection rate and FPR as follows: LR = DR FPR Derivation of the post-test odds using LR is achieved through simple multiplication by the pre-test odds of disease: Pre-test odds × Likelihood ratio = Post-test odds Effectiveness of nuchal translucency screening in the first trimester The literature search identified 18 articles that met the entry criteria (Table 19). Most studies were in Europe, with the majority conducted in the United Kingdom. The studies present the findings from a total of 804 cases of trisomy 21 seen over a 13 year period. Most studies used amniocentesis or CVS as a “gold standard” for diagnosis, although some did not detail the reference test used. 48 Nuchal translucency measurement in the first trimester of pregnancy Table 19 General characteristics of retrieved studies focusing on the use of nuchal translucency measurement for the screening of trisomy 21 in the first trimester of pregnancy First author and year of publication Schwarzler et al (1999) Thilaganathan et al (1999) Snijders et al (1998) Martinez et al (1997) Kornman et al (1996) Hyett et al (1996) Scott et al (1996) Hafner et al (1995) Hyett et al (1995) Bewley et al (1995), Roberts et al (1995) Brambati et al (1995) Borrell et al (1996, 1997) Pandya et al (1995b) Szabo et al (1995) Nicolaides et al (1994), Pandya et al (1994) Hewitt (1993) Ville et al (1992) Savoldelli et al (1993) Population Quality criteria (ABCDE)b Location Dates of enrolment Cases UK 1996 to 1997 12 29.4c Y1YNY Karyotyping, pregnancy outcome UK 1994 to 1998 21 28.6c Y5NUY CVS UK ? 326 31 Y2YNY A or CVS Spain ? 9 38 Y2YNY CVS The Netherlands 1994 7 38 Y2YNY A or CVS UK Australia Austria UK 1993 to 1995 1993 to 1995 1993 to 1994 ? 70 8 4 36 ? 38c 26 ? Y2NNY Y2YNY Y2NNY Y2NUY CVS CVS A CVS UK 1992 to 1993 3 29.8c Y1YNY Karyotyping, pregnancy outcome Italy 1992 to 1993 26 ? Y2YNY CVS Spain 1991 to 1993 47 ? Y2YNY A or CVS UK 1990 to 1994 101 35 Y2NNY A or CVS Hungary ? 31 ? Y2YNY CVS, cordocentesis UK 1990 to 1994 61 35 Y1YYY A or CVS Australia France 1989 to 1993 1988 to 1991 5 9 35c ? Y1YNY Y2YNY A or CVS A or CVS Switzerland 1985 to 1991 28 ? Y2YNY CVS Maternal agea Reference test A = amniotomy; CVS = chorionic villus sampling; N = no; U = unclear; Y = yes; ? = unknown or unstated a Values are medians unless otherwise stated b Quality criteria are listed in Table 14 c Mean Three studies (Snijders et al 1998, Schwarzler et al 1999, Thilaganathan et al 1999) used CRL adjusted cutoff levels applied to NT thickness to estimate risk, since thickness normally increases with CRL length. Given this current perspective, best exemplified by Snijders et al (1998) and subsequent authors, those studies applying a set cutoff are reviewed for historical interest only (Ville et al 1992, Hewitt 1993, Savoldelli et al 1993, Nicolaides et al 1994, Pandya et al 1994, Bewley et al 1995, Brambati et al 1995, Comas et al 1995, Hafner et al 1995, Hyett et al 1995, Pandya et al 1995b, Roberts et al 1995, Szabo et al 1995, Borrell et al 1996, Hyett et al 1996, Kornman et al 1996, Scott et al 1996, Borrell et al 1997, Martinez et al 1997). Summaries of these studies are found in Appendix G. Nuchal translucency measurement in the first trimester of pregnancy 49 Snijders et al (Snijders et al 1998) reported on a multicentre study in the United Kingdom involving 22 centres and 96,127 women. A combination of maternal age and NT thickness at 10 to 14 weeks (from 306 sonographers with FMF certification) was used to estimate the risk for trisomy 21. The following criteria were used to standardise the results: • acquisition of a good sagittal section of the fetus; • appropriate image magnification, with the fetus occupying at least 75 per cent of the image; and • proper distinction made between fetal skin and amnion; and measurement of the maximum thickness of the subcutaneous translucency between the skin and the soft tissue overlying the cervical spine achieved. The NT thickness and CRL were measured transabdominally unless poor visualisation prompted a transvaginal ultrasound examination. Risk assessment was based on previous data and updated on the basis of a validation sample. After counselling, patients were offered a diagnostic test. For a risk cutoff of 1 in 300 for trisomy 21, the authors reported DR=82.2 per cent (268 out of 326), FPR=8.3 per cent (7,907 of 95,476), PPV=3.2 per cent (268 of 8,428) and NPV=99.9 per cent (87,569 of 87,699). For an FPR of 5 per cent, the sensitivity was 77 per cent (95% CI=72%, 82%). Of the 268 pregnancies affected by trisomy 21, early termination was chosen in 250 (93.3%) cases. Since intrauterine death of fetuses with trisomy 21 from 12 weeks to term is about 40 per cent, the authors could not be certain how many of the early terminations would have otherwise resulted in a live birth. Schwarzler et al (1999) prospectively evaluated 4,523 consecutive fetuses at 10 to 14 weeks of gestation in women attending a single London hospital from July 1996 to November 1997. Specially trained sonographers measured NT as the maximal sonoluscent zone between the inner aspect of the fetal skin and the outer aspect of the cervical spine. The maximum value of three measurements was recorded. Applying a 1 in 270 risk cutoff for trisomy 21, the authors reported the following results: DR=76.9 per cent, FPR=4.9 per cent; PPV=4.4 per cent, and NPV=99.9 per cent. Thilaganathan et al (1999) examined 9,802 pregnant women in the setting of a district general hospital. Using a 1 in 300 risk cutoff for trisomy 21, the authors reported DR=80.9 per cent (17 of 21) and PPV=2.1 per cent (1 in 49). Using these data, the estimated FPR and NPV were 8.2 per cent and 99.9 per cent, respectively. 50 Nuchal translucency measurement in the first trimester of pregnancy Factors affecting the effectiveness of the screening procedure Due to concerns about the generalisability of results, Wald et al (1998), Nicolaides et al (1999a), Malone et al (2000) and Stewart and Malone (1999) called for further studies to characterise and quantify the effect of sources of heterogeneity from physical, clinical and programmatic perspectives. Some probable causes of heterogeneity are described below. Physical factors The resolution of sonographic images depends on the wavelength of sound used. The use of 3 MHz transducers gives an effective resolution of about 1 mm with greater frequencies offering higher resolutions. Since NT measurements lie between 0 and 5 mm, image resolution influences the validity and repeatability of results. Clinical factors The variation of screening performance with age of gestation has not been fully determined (Wald et al 1998). In addition, the full natural history of increased NT in euploid fetuses with autosomal trisomies or affected pregnancies with NT measurements in the normal range have not been completely described (Borrell et al 1998, Maymon et al 1999, Stewart and Malone 1999). A common criticism applied to relevant prospective studies is that screening by NT detects cases of aneuploidy that would otherwise have died in utero. This gives inflated detection rates and implies that unnecessary procedures would have been performed on pregnant women when termination of the affected pregnancy is chosen. Snijders et al (1995) estimated that up to 40 per cent of affected fetuses identified at 10 to 14 weeks of gestation will die in the uterus. Some authors have used this finding to adjust the detection rate from the 82 per cent reported by Snijders et al (1998) to about 78 per cent (Cuckle 1998), 60 per cent (Haddow 1998), or 56 per cent (Reynolds 1998). Verification bias has been put forward by Mol and others as a possible explanation for the discrepancies in published detection rates (Hackshaw et al 1996, Mol et al 1996, Mol et al 1999). Verification bias arises when there are differential rates of diagnostic testing according to the results of a screening test. In the case of NT, the group with positive screening results is more likely to undergo karyotyping than the group screening negative. Mol et al suggested that this, coupled with the increased spontaneous fetal loss rates associated with increased NT, might lead to an overestimation of the detection rate. Mol et al conducted a systematic review of 25 published reports, 15 of which were assessed as being affected by verification bias. Detection rates for studies with verification bias were found to be higher than those without the bias (77% versus 55%). After adjusting for the bias and accounting for the increased fetal loss rate, the authors reported an estimated detection rate of 63 per cent (Mol et al 1999). Programmatic factors Standardisation of definitions and procedures Biagiotti et al (1997) examined the controversy of the proper definition of an abnormal NT measurement stemming from the proper choice of cutoff. They reported that the CRL dependent measures confer a potential advantage over absolute increases in NT by significantly reducing the FPR. Monni et al (1997) reported that the modification of techniques to adhere to published FMF guidelines improved detection rates from 30 per cent to 84 per cent. Nuchal translucency measurement in the first trimester of pregnancy 51 Quality assurance, monitoring and control Haddow et al (1998) reported that the overall success rate for obtaining NT images among 16 centres that had no specific training of sonographers or quality control measures was 83 per cent (61–100%). Pandya et al (1995a) prospectively assessed the repeatability of NT thickness measurement in fetuses of 10 to 14 weeks gestation by asking two of four operators to make six measurements each in 200 women (a total of 1,200 measurements). The authors found that the intraobserver, interobserver and caliper placement repeatability of fetal NT measurements were less than 0.54, 0.62 and 0.58 mm respectively, 95 per cent of the time. The authors concluded that measurement is highly reproducible when NT thickness is measured by well trained operators. A study by Roberts et al (1995), however, showed that 36 per cent of second measurements of NT by the same sonographer differ by about 1 mm. Readings in which two sonographers independently measured NT were found to vary by more than 1 mm in 71 per cent of cases. There is evidence to suggest that differences in calliper placement account for a large part of the variation in measurements (Pandya et al 1995a, Schuchter et al 1998), a situation that is expected to improve when automated imaging techniques are used (Bernardino et al 1998, Nicolaides et al 1999a). Implementation in routine practice Demonstration projects examining the feasibility of implementing routine screening for trisomy 21 using NT have shown that operator variability and variations in detection rates may be reduced with unified criteria addressing procedural aspects of the examination (Nicolaides et al 1999a). Reviews published by Malone et al (2000) and Stewart and Malone (1999) suggest that procedural factors might explain the large difference in procedural sensitivity when FMFaffiliated centres were compared with other independent centres (72% versus 50% respectively). Effect of a first trimester NT screening program on screening for trisomy 21 using maternal serum markers in the second trimester Due to the expected reduction in the prevalence of trisomy 21 if NT screening were implemented as a population screening technique, screening for trisomy 21 using maternal biochemical markers in the second trimester will suffer increases in FPRs and decreases in positive predictive values, sometimes by as much as five fold. Risk assessment calculations must take into consideration this shift in prevalence, especially as it applies to local experience (Stewart and Malone 1999, Malone et al 2000). 52 Nuchal translucency measurement in the first trimester of pregnancy Effectiveness of maternal biochemical marker screening Second trimester This section incorporates the results of a technology assessment and studies conducted by Wald et al (1994, 1996a, 1997a, 1998). Results are given in terms of median estimates for multiples of the median (MoM), which compare median levels of biochemical markers in affected pregnancies to those in unaffected pregnancies. A MoM of 1.00 implies that the biochemical marker level in affected pregnancies is at the level found in unaffected pregnancies. MoM values below 1 indicate that a lower median level is found. Values above 1 are interpreted as being higher than the norm. Only biochemical markers whose confidence intervals do not cross 1 demonstrate statistically significant differences between affected an non-affected pregnancies. Table 20 summarises results for particular biochemical markers in screening for trisomy 21. Table 20 Pooled multiple of the median (MoM) values for selected maternal biochemical marker studies during the second trimester of pregnancy Biochemical marker uE3 AFP CA-125 PAPP-A Free α-hCG SP1 α-inhibin Dimeric inhibin A Total hCG Free β-hCG Number of studies Number of trisomy 21 cases Pooled MoM 95% CI 21 38 5 3 7 733 1,328 81 64 239 0.72 0.75 0.94 0.97 1.43 0.68, 0.75 0.72, 0.78 0.74, 1.21 0.84, 1.11 1.12, 1.82 7 4 379 64 1.47 1.63 1.23, 1.76 1.01, 2.62 6 28 12 375 907 562 1.92 2.06 2.20 1.75, 2.15 1.95, 2.17 2.07, 2.33 AFP = alpha-fetoprotein; CA-125 = cancer antigen 125; CI = confidence interval; hCG = human chorionic gonadotrophin; MoM = multiple of the median; PAPP-A = pregnancy-associated plasma protein-a; SP1 = schwangerschaftsprotein 1; uE3 = unconjugated oestriol Source: Wald et al (1998) Pooled results indicate that eight markers are useful in the detection of trisomy 21: uE3, AFP, SP1, α-inhibin, dimeric inhibin A, total hCG, α- and β-hCG. Expected detection and false positive rates Estimated detection rates for 5 per cent FPRs of selected maternal biochemical markers used alone or in double, triple or quadruple combinations, are given in Table 21. Nuchal translucency measurement in the first trimester of pregnancy 53 Table 21 Estimated detection rate (%) for a false positive rate of 5 per cent for selected maternal biochemical marker combinations during the second trimester of pregnancy Biochemical marker Single markers AFP uE3 Total hCG α-hCG β-hCG Inhibin A 36 41 49 38 49 44 Double marker combinations uE3 45 Total hCG 54 56 α-hCG 45 53 51 β-hCG 54 57 – 55 Inhibin A 53 57 58 51 58 – Triple marker combinations uE3, inhibin A 60 – – uE3, β-hCG 60 – – uE3, α-hCG 56 – uE3, total hCG 59 Total hCG, inhibin A 64 – Total hCG, α-hCG 57 – α-hCG, β-hCG 60 – – β-hCG, inhibin A 64 – – α-hCG, inhibin A 58 – – 64 62 63 60 – 64 59 – – – 61 – – Quadruple marker combinations uE3, total hCG, inhibin A 67 uE3, α-hCG, inhibin A 66 – – uE3, β-hCG, inhibin A 67 – uE3, total hCG, α-hCG 63 uE3, β-hCG, α-hCG 65 α-hCG, β-hCG, inhibin A 67 68 Total hCG, α-hCG, inhibin A 65 66 – – – – – – – – – AFP = alpha-fetoprotein; hCG = human chorionic gonadotrophin; MoM = multiple of the median; uE3 = unconjugated oestriol – = data not available Source: Wald et al (1994, 1996a, 1997a, 1998) First trimester This section incorporates the results of a meta-analysis conducted by Cuckle and van Lith (1999), and Wald et al (1998). Results are given in terms of mean or median MoM (Table 22). However, Wald et al (1998) noted some limitations of maternal biochemical markers. For instance PAPP-A is known to lose discrimination after 13 to 14 weeks of gestation (Cuckle 1994). Similarly, free α-hCG is low in affected pregnancies before 12 weeks of gestation and dimeric inhibin A is relatively nondiscriminatory before 14 weeks of gestation. 54 Nuchal translucency measurement in the first trimester of pregnancy Table 22 Pooled multiple of the median (MoM) values for selected maternal biochemical marker studies during the first trimester of pregnancy Biochemical marker Number of studies Number of trisomy 21 cases PAPP-A Pooled MoM 95% CI 12 297 0.38 0.33, 0.43 uE3 8 9 210 226 0.71 0.74 0.59, 0.86 ? AFP 16 26 335 542 0.78 0.79 0.73, 0.84 ? SP1 6 111 0.81 ? Free α-hCG 6 162 1.00 0.85, 1.17 CA-125 2 34 1.14 0.72, 1.81 α-inhibin 2 34 1.27 0.92, 1.75 Total hCG 14 352 1.29 1.16, 1.44 Dimeric inhibin A Free β-hCG 3 112 1.59 0.96, 2.65 12 17 308 579 1.83 1.98 1.65, 2.03 ? MoM = multiple of the median; AFP = alpha-fetoprotein; CA-125 = cancer antigen 125; CI = confidence interval; hCG = human chorionic gonadotrophin; PAPP-A = pregnancy-associated plasma protein-a; SP1 = schwangerschaftsprotein 1; uE3 = unconjugated oestriol; ? = unstated or unknown; a = estimate for gestational age of 8-14 weeks Source: Wald et al (1998), Cuckle and van Lith (1999) Expected detection and false positive rates Discriminatory power of biochemical markers used alone or in combination is reported using estimates of the detection rate for a particular FPR. Table 23 shows the overall DR for selected biochemical markers. All values are estimated at a fixed FPR of 5 per cent. Table 23 Estimated detection rate for a false positive rate of 5 per cent for selected biochemical markers and combinations of markers measured from 9 to 11 weeks of gestation Biochemical marker Detection rate (%) Single markers: uE3 30.0a AFP 32.0 a Free β-hCG 41.8 PAPP-A 52.2 Double markers: PAPP-A and free β-hCG 64.6 Triple markers: PAPP-A, free β-hCG, and AFP 66.6 PAPP-A, free β-hCG, and uE3 68.6 Quadruple markers: PAPP-A, free β-hCG, AFP, and uE3 70.1 AFP = alpha-fetoprotein; hCG = human chorionic gonadotrophin; PAPP-A = pregnancy-associated plasma protein-a; uE3 = unconjugated oestriol a Estimate for 8–14 weeks age of gestation Source: Wald et al (1998), Cuckle and van Lith (1999) Discriminatory power is inversely related to gestational age (Table 24), with DR decreasing by as much as 50 per cent from 9 to 13 weeks (Cuckle 1994, Cuckle and van Lith 1999). Nuchal translucency measurement in the first trimester of pregnancy 55 Table 24 Estimated detection rate (per cent) for a false positive rate of 5 per cent for selected biochemical markers and combinations of markers, according to gestational age Gestational age (weeks) 9 10 11 12 13 PAPP-A and free β-hCG 71.6 65.6 58.2 50.9 46.4 PAPP-A, free β-hCG and AFP 73.1 67.5 60.4 53.7 49.3 PAPP-A, free β-hCG and uE3 74.6 69.3 63.0 57.3 53.9 PAPP-A, free β-hCG, AFP and uE3 75.8 70.8 64.9 59.4 56.1 Biochemical marker AFP = alpha-fetoprotein; hCG = human chorionic gonadotrophin; PAPP-A = pregnancy-associated plasma protein-a; uE3 = unconjugated oestriol Source: Cuckle and van Lith (1999) Effectiveness of a combination of nuchal translucency and maternal biochemical markers First trimester nuchal translucency plus second trimester maternal biochemical markers Table 25 shows some characteristics of three studies that examined the effect of introducing NT measurement in the first trimester on screening rates for trisomy 21 in women subsequently undergoing second trimester biochemical screening. The search identified a modelling study by Wald et al (1999) using data from previously published estimates and retrieved two primary studies by Kadir and Economides (1997) and Thilaganathan et al (1997) conducted in the United Kingdom in 1997. The two primary studies used CRL adjusted cutoffs for NT. Table 25 General characteristics of retrieved studies focusing on the use of nuchal translucency measurement in the first trimester and maternal biochemical markers in the second trimester for the screening of trisomy 21 Reference Location Dates of enrolment Population Cases Wald et al (1999) Maternal agea Quality criteria (ABCDE)b Reference test not applicable Kadir and Economides (1997) UK 1995 to 1996 8 ?c Y2NNY Karyotyping, pregnancy outcome Thilaganathan et al (1997) UK 1994 to 1996 8 28.8 Y2NNY Karyotyping, pregnancy outcome N = no; Y = yes a Values are means b Quality criteria are listed in Table 14 c Unknown or unstated 56 Nuchal translucency measurement in the first trimester of pregnancy Wald et al (1999) used an “integrated test” involving a combined assessment of results from tests conducted in the first two trimesters of pregnancy. Specifically this incorporated serum inhibin A and ultrasonographic NT measurements in the first trimester, with subsequent quadruple maternal biochemical marker assays in the second trimester (AFP, uE3, hCG, and inhibin A). They estimated that this test would show DR=94 per cent for FPR=5 per cent (Wald et al 1999). The authors asserted that: • the integrated test makes use of the fact that different screening markers are best used at different times during the pregnancy to take full advantage of the full discriminatory power of such testing; • the procedure’s accuracy could not be established if results from first trimester tests were conducted independently of second trimester tests; and • giving pregnant women different estimates of risk at different times of the pregnancy would lead to confusion. The approach has been criticised on the grounds that it undermines patient choice and defeats the purpose of the screening test as a means of providing meaningful guidance to pregnant women (Jenkins and Wapner 1999). It introduces an unacceptable delay that arises from combining the results of the screening test over two trimesters (Jenkins and Wapner 1999, Reynolds et al 1999). The combination of NT and maternal biochemical screening has not been assessed in a single large group of pregnant women (Malone et al 1999). Table 26 shows the estimated detection rates for variations of the integrated test. Table 26 Estimated detection rate for a fixed false positive rate of 5 per cent for variations of the “integrated test” Detection rate (%) Per cent increase over second trimester triple test DRb Second trimester triple test alone 69 – Second trimester quadruple test alone 76 10.1 Test variationa First trimester NT and serum inhibin A 85 23.2 First trimester serum inhibin A and second trimester quadruple test 85 23.2 First trimester NT and second trimester quadruple test 92 33.3 First trimester NT and serum inhibin A, and second trimester quadruple test 94 36.2 DR = detection rate; NT = nuchal translucency a The second trimester triple test includes serum alpha-fetoprotein (AFP), unconjugated oestriol (uE3), and human chorionic gonadotrophin (hCG). The second trimester quadruple test includes all triple test markers plus inhibin A. b Calculated as (DRVariation – DRTriple Test)/DRTriple Test × 100 Source: Wald et al (1999) Kadir and Economides (1997) reported that adding first trimester NT screening for trisomy 21 to second trimester maternal biochemical screening with AFP and free βhCG in a population of “low-risk” women produced a combined DR of 87.5 per cent (seven of eight affected fetuses) at an FPR of 9.1 per cent. Similar results for DR were reported by Thilaganathan et al (1997) although no estimates on FPR were provided. Nuchal translucency measurement in the first trimester of pregnancy 57 First trimester nuchal translucency plus first trimester maternal biochemical markers The combined use of sonographic and biochemical measurements increases sensitivity over the level attained by the use of each test alone (Cuckle and van Lith 1999). This is illustrated in Table 27. With the use of NT screening, the detection rate of biochemical screening increases by as much as 85 per cent over original values. When the serum test using all four biochemical markers is used, the DR increases from 70.1 per cent to about 88 per cent, an increase of 26 per cent. Gestational age-dependent estimates of sensitivity are similarly increased. Table 27 Estimated detection rate for a 5 per cent false positive rate for the combined use of NT and selected biochemical markers and combinations of markers measured from 9 to 11 weeks of gestation Detection rate (%) Serum alonea Biochemical marker NT alone Serum with NT Increase over serum aloneb Single markers: Free β-hCG 41.8 *72.7 77.7 85.9 PAPP-A 52.2 *72.7 81.2 55.6 64.6 *72.7 86.4 33.7 PAPP-A, free β-hCG and AFP 66.6 *72.7 87.2 30.9 PAPP-A, free β-hCG and uE3 68.6 *72.7 87.9 28.1 70.1 *72.7 88.3 26.0 Double markers: PAPP-A and free β-hCG Triple markers: Quadruple markers: PAPP-A, free β-hCG, AFP and uE3 AFP = alpha-fetoprotein; DR = detection rate; hCG = human chorionic gonadotrophin; NT = nuchal translucency; PAPP-A = pregnancy-associated plasma protein-a; uE3 = unconjugated oestriol a From Table 23 b Calculated as (DR Serum with NT – DRSerum Alone)/ DRSerum Alone × 100 * Please note that NT detection rate was calculated from a meta-analysis by Cuckle and van Lith (1999) Source: Cuckle and van Lith (1999) 58 Nuchal translucency measurement in the first trimester of pregnancy Summary of data on the effectiveness of screening using nuchal translucency measurement and maternal biochemical tests Table 28 presents point estimate ranges for the detection rates and FPRs of various screening techniques and combinations of techniques. Table 28 Estimated detection and false positive rates for combinations of screening modalities Range of point estimates (%) Screening technique Detection rate False positive rate 77–82* 5–8 30–52 65 67–69 70 5 5 5 5 36–44 45–58 57–64 63–68 5 5 5 5 78–81 86 87–88 88 5 5 5 5 See Table 27 and discussion for details 88 92 9.1 5 See Table 27 and discussion for details Comments Single modalities Nuchal translucency measurement in the first trimester CRL-adjusted cutoff levels used. Reference tests were CVS, amniocentesis or pregnancy outcome. See Table 19 and discussion for details. Maternal biochemical markers in the first trimester Single marker Double markers Triple markers Quadruple markers Maternal biochemical markers in the second trimester Single marker Double markers Triple markers Quadruple markers Estimates arising from systematic reviews of specific biochemical markers and combinations of markers. See Tables 21, 23 and discussion for details. Combination modalities First trimester nuchal translucency and first trimester maternal biochemical measurement NT plus single marker NT plus double markers NT plus triple markers NT plus quadruple markers First trimester nuchal translucency and second trimester maternal biochemical measurement NT plus double markers NT plus quadruple markers CRL = crown-to-rump length; CVS = chorionic villus sampling; NT = nuchal translucency * NT detection rate was calculated from primary studies identified by literature search that met inclusion criteria (Table 19) Nuchal translucency measurement in the first trimester of pregnancy 59 What are the economic considerations? Review of the literature In addition to the electronic databases in Table 12 and Internet sites listed under ‘Literature search’ in the section ‘Approach to assessment’, searched economic databases included EconLit, HEED and DARE. Only studies with a formal economic evaluation of screening for trisomy 21 by ultrasound were included. Neverteheless the summary of results (Appendix H) includes a study of biochemical markers for the detection of trisomy 21 in the UK, as it forms the basis of the modelling method adopted in this report. A comparison across studies of the cost-effectiveness of ultrasound screening in pregnancy is limited by the major differences in assumptions about detection rates, FPRs, rates of diagnostic procedures, procedure-induced fetal losses and unit costs across countries. While most studies report an average cost per case detected, the differing scale of the programs (i.e. number of screened pregnancies) makes an assessment of the incremental cost compared with existing practice vary from country to country (even where the technology has the same effectiveness). The incremental cost per extra case detected depends on the number of cases detected, even where there are no economies of scale in the screening program. A further difficulty is the lack of a standardised outcome measure. Studies often report a cost per trisomy 21 pregnancy detected but the cost per outcome is not constant over the level of outcome. As the detection rate rises (with the risk cutoff falling), the cost per case detected rises from a certain point due to the number of false positives. In addition, the meaning of a single outcome is questionable if the rate of procedureinduced fetal losses rises as the detection rate rises. It is conceivable that two strategies could have the same cost per case detected, even with different: • numbers of cases detected; • procedure-induced fetal loss rates; and • rates of unnecessary procedures. Where we are concerned with both cases detected and the consequences of false positive screens, we either have to consider both outcomes together or keep one constant. In one approach, Wald et al (1997b) kept the detection rate constant across interventions and thus the number of cases detected was the same in each strategy for a given sized group of women. Such an approach allows the use of an average cost-effectiveness ratio as a guide to decision making. An alternative is to keep the FPR constant and to calculate the extra cost per case detected for a given number of procedure-induced fetal losses. Another option which is common in the literature, is to present the trade-off between cost, detection and fetal losses. The last approach is more difficult to implement and makes decision making more difficult. While there is clinical trial evidence of the effectiveness of ultrasound screening for trisomy 21 in the first trimester, either on its own or in combination with first trimester biochemical screening, there remains some uncertainty about the effectiveness of this strategy in practice. 60 Nuchal translucency measurement in the first trimester of pregnancy Wald et al (1997b) have suggested a number of areas of concern that would affect the economics of ultrasound screening. In particular: • Evidence to date suggests only a small difference in detection rates between first and second trimester. However, the overall cost difference in screening is likely to be substantial if the uptake is higher, and the cost of combined ultrasound and biochemical screening is more than three times the cost of biochemical screening alone. • Screening performance is operator-dependent and involves repeated measurement, especially where there is a failure to obtain a measurement. The cost of providing ultrasound screening is therefore uncertain, not only because of the time taken for the scan, but also because of sonographer training and quality control. • While women prefer early screening, the benefits of providing the option of an earlier, less physically traumatic, termination are reduced by the fact that about a quarter of trisomy 21 pregnancies miscarry between 10 and 15 weeks of gestation. Thus, this proportion of women will be offered an induced abortion when they would have miscarried spontaneously in the next few weeks. • Serum testing in the first trimester will not detect neural tube defects. Therefore, if a screening strategy restricts serum screening to the first trimester, the opportunity for AFP screening in the second trimester will be lost. Screening for neural tube defects would then be based on ultrasound, performed either in association with an NT screen or as part of the second trimester ultrasound scan that checks for fetal abnormality. This strategy may result in a fall in the overall detection of neural tube defects. An alternative strategy, involving serum screening in both the first and second trimesters to pick up neural tube defects, would require additional funding. • It may be that the introduction of first trimester NT screening would reduce the rate of diagnostic tests in higher risk pregnant women. This would lead to a cost saving with some reduction in detection but a reduction in procedure related fetal losses. On the other hand some high-risk women may have amniocentesis in the second trimester irrespective of the results of early screening. Once a screening policy is in place it may not be possible to distinguish screening and non-screening ultrasound in the first trimester. Since many of these women currently have an ultrasound in the first trimester for other purposes (e.g. for dating of pregnancy), replacing a dating ultrasound with a NT ultrasound in this group of women could increase costs without improving detection. There are a number of options for ultrasound screening in pregnancy: • first trimester ultrasound for all pregnant women; • first trimester biochemical screening for all pregnant women; • second trimester biochemical screening for all pregnant women; • combined first trimester biochemical screening and ultrasound for all pregnant women; or • application of an age cutoff to any of the above. Nuchal translucency measurement in the first trimester of pregnancy 61 In order to provide some guidance on the likely costs and outcomes associated with some of these options, the next section presents a modelled decision analysis of ultrasound and biochemical screening for trisomy 21 in pregnancy, based on Australian data. Cost-effectiveness: a modelled decision analysis This section presents estimate of the potential cost-effectiveness of the widespread introduction of NT ultrasound screening of pregnant women for trisomy 21 compared with alternative screening practices in Australia. In principle, the cost-effectiveness of NT screening in the first trimester should be calculated as the incremental costeffectiveness ratio compared with current practice. That is to say (Ca − Cb ) (Oa − Ob ) where: Ca and Cb are the cost of ultrasound screening and current practice respectively, and Oa and Ob are the outcomes of ultrasound screening and current practice respectively. Outcomes reported in all analyses are cases of trisomy 21 detected and number of losses of unaffected fetuses. While ultrasound may be able to detect other congenital abnormalities, this evaluation has focussed on alternatives to biochemical screening for trisomy 21 alone, as this is the most common cause of intellectual disability. Nevertheless, to the extent that ultrasound screening may be capable of detecting other abnormalities, the estimates of cost-effectiveness are underestimated. The estimation of cost-effectiveness is done with a simple decision analysis similar to that used in Wald et al (1998), in a Microsoft Excel spreadsheet. Cost-effectiveness analysis in a decision analytic framework allows consideration of the potential cost-effectiveness of a technology in the absence of either high quality randomised controlled trial evidence of effectiveness or high quality prospective cost data. It allows identification of a range of potential costs and outcomes associated with screening strategies and the uncertainties associated with each. While the results of the analysis remain subject to considerable uncertainty given the quality of the underlying clinical and economic data, they nevertheless provide the basis for an assessment of the potential for the technology to provide health gains at an acceptable cost. Three screening strategies are considered in the following analyses: 1. NT in the first trimester followed by CVS for those with a positive test; 2. NT and biochemical screening in the first trimester, followed by CVS for those with a positive test; and 3. NT and biochemical screening for high-risk women (applying a lower age cutoff) in the first trimester, with biochemical screening in the second trimester for other women. 62 Nuchal translucency measurement in the first trimester of pregnancy The appropriate comparator is current screening practice. This is difficult to model since it consists of a combination of ultrasound screening and biochemical screening that takes into account age and other risk factors, followed by diagnostic testing (particularly for those over the age of 35). It is unclear how much of each of these parts of screening activity is being done currently and the likely degree of substitution if NT screening were to be implemented. Accordingly, the analysis begins with a simple comparison of universal screening, with each modality compared with no screening. The sensitivity analysis considers variations on key assumptions including detection rates, uptake and the extent of substitution of NT screening for dating ultrasound scans and diagnostic tests in those at higher risk. There are a number of possible outcomes of a screening program. The main aim of screening in pregnancy is to provide women with information on fetal status. Information prior to birth may in itself be valuable to women and may also allow them to make a choice on whether or not to continue with a pregnancy. However, increased information comes at a cost, both in terms of resources associated with screening and the trade-off between improved information from the test and negative consequences such as anxiety from a positive screen and the risk of inducing the loss of unaffected fetuses. For all the screening options, an increase in the rate of detection leads to an increase in the rate of false positive results and therefore procedure-related miscarriage in follow-up diagnostic tests. The primary outcome of interest in this assessment is the number of cases of trisomy 21 detected. However, the report takes the view that any consideration regarding the resource implications of providing screening for women should take into account downstream costs such as subsequent diagnostic tests and terminations. Accordingly, the number of diagnostic procedures and their outcomes have been calculated to provide the total cost of screening. As a secondary outcome measure, the number of live births with trisomy 21 is also calculated for each strategy. Some studies have gone further and calculated the lifetime extra cost of care for infants born with trisomy 21. For example Gill et al (1987) estimated the lifetime care cost in the United Kingdom as equivalent to about US$500,000. Since there are no reliable estimates of the money value of a life with or without trisomy 21, including just the cost of care provides a distorted picture of the cost-effectiveness of screening. Therefore the analysis does not consider the lifetime cost of care. Cost-effectiveness analysis is designed to consider a single outcome such as cost per case of trisomy 21 detected. Where there is a trade-off between outcomes (e.g. trisomy 21 cases detected versus procedure-induced fetal losses), cost-effectiveness analysis cannot provide a single number to compare strategies. In this case analysis is further compounded by the nature of the test, which does not provide a definitive result but rather provides a risk assessment. Reducing the risk threshold of the test increases both the detection rate and the FPR. As discussed above, one approach is to compare strategies at a given detection rate (Wald et al 1997b). Since the primary outcome of interest is the number of cases detected, a second strategy is to compare tests at a given FPR (specificity) with detection rates then varying across tests. The third approach, of comparing tests at the trial reported levels of sensitivity and specificity, is likely to be potentially misleading and open to manipulation, particularly in the absence of the known quality of the screening program in practice. Nuchal translucency measurement in the first trimester of pregnancy 63 The analysis can be further complicated if comparing strategies at different risk thresholds and consequent detection and FPRs. This led Wald et al (1998) to argue that average ratios are appropriate to compare strategies and that incremental analysis should be restricted to determining the cost-effectiveness of different risk thresholds within a given strategy (e.g. whether the risk threshold for biochemical screening should be 1:250 or 1:300). The authors of this review believe that in comparing mutually exclusive strategies for detecting cases of trisomy 21, it is appropriate to keep the FPR constant and use the incremental cost per case detected to aid decision making. Even with the same FPR, the actual number of fetal losses will differ across strategies if either the uptake of screening or the diagnostic procedure varies across strategies. However, the use of an incremental cost-effectiveness ratio (ICER) is complex when the ICER is not monotonic (i.e. it does not always move in the same direction as you increase the number screened). In this case one needs to know what the total expenditure on screening would be under each strategy. A number of possible strategies are simulated in a decision analytic model, and the incremental cost per case detected compared with the next best alternative screening strategy determined. The total costs and outcomes of each strategy are also reported. There are about 260,000 births in Australia each year. It is unknown what the prevalence of trisomy 21 would be without any screening program. Assuming an underlying prevalence of 1.6 per 1,000 live births (Jane Halliday, Manager, Victorian Perinatal Data Collection Unit, Department of Human Services, Victoria, personal communication, 2000), there would be approximately 416 trisomy 21 births each year. As shown in Table 29, the prevalence of trisomy 21 increases with maternal age. Table 29 Prevalence of trisomy 21 per 1,000 live births by age Maternal age (years) <30 <35 >30 >35 Prevalence of trisomy 21 births 0.6 0.9 2.6 3.2 Source: Jane Halliday, Manager, Victorian Perinatal Data Collection Unit, Department of Human Services, Victoria, personal communication, 2000. There is a high spontaneous rate of miscarriage of trisomy 21 fetuses. Between the first trimester and term, the rate is reported to be 40-48 per cent and between the second trimester and term, 23-30 per cent (Snijders et al,1995 Cuckle et al, 1990). This suggests that the rate of trisomy 21 pregnancies screened in the first trimester would be 2.7 to 3.1 per 1,000 compared with 2.1–2.3 per 1,000 in the second trimester. These data are not precise and do not accord exactly with the dates of NT and biochemical screening. For the purposes of the primary modelled analysis, the assumption was a 40 per cent rate of spontaneous miscarriage of trisomy 21 between the time at which NT screening would occur and term. The rate of fetal loss between the time when a second trimester biochemical screen would be done and term was assumed to be 23 per cent. This suggests a prevalence of 693 affected pregnancies when first trimester NT screening would be done and 540 in the second trimester when biochemical screening would be done. 64 Nuchal translucency measurement in the first trimester of pregnancy Current practice The number of women screened, the test type used and the timing of screening varies across Australia. In some States, NT ultrasound screening in the first trimester is part of current practice. However, a common practice, and the one funded by Medicare, is a combination of maternal age and biochemical marker screening in the second trimester. The detection rate for triple marker biochemical screening in the second trimester (AFP, total hCG and inhibin A) has been estimated at no more than 64 per cent (Table 21). Those at an increased risk of fetal abnormality (primarily based on age) are advised to consider a diagnostic test. There are no complete data on the extent of screening, but between October 1999 and September 2000 there were 41,410 claims for biochemical screening (Medicare item 66740), which represents about 16 per cent of all pregnant women. In Victoria some 30 per cent of pregnant women had a biochemical screen in 2001 (Halliday, 2002). South Australia has reported rates of biochemical screening in excess of 80 per cent. Some women currently have an ultrasound screen that includes NT measurement. It has been suggested that Victorian rates of NT screening may already be in excess of 25 per cent. CVS or amniocentesis is offered to those who have a risk in excess of 1:250 in second trimester and 1:300 in first trimester. Such risk assessments are based on screening results that take into account maternal age. An amniocentesis has been reported to have a procedure-related fetal loss rate of 0.9 per cent (95% CI=1.2 per cent, 0.6%) in the second trimester of pregnancy (Wald et al 1997b). The current uptake of amniocentesis among women with a positive screen has been reported to be 85 per cent (SABDR 1998). Ninety per cent of women with a diagnosis of a chromosomal abnormality terminate the pregnancy. Nuchal translucency screening Screening for trisomy 21 using ultrasound is possible in the first or second trimester. The primary cost-effectiveness analysis considers universal NT ultrasound screening for all pregnant women in the first trimester. While the current rate of ultrasound in the first trimester is unknown, between April and September 2000 there were 32,633 claims on Medicare item 55704 (pregnancy ultrasound between 12 and 16 weeks of gestation) and 70,130 claims for Medicare item 55706 (pregnancy ultrasound between 17 and 22 weeks of gestation). These represent 24 per cent and 54 per cent of pregnancies respectively. However, these item numbers only became available in 2000 and service providers may not yet charge against the appropriate Medicare item number. Moreover, many women use non Medicare providers of antenatal care, and the number of Medicare funded ultrasound services in the first trimester is likely to be a substantial underestimate of the total. Overall, the number of pregnancy ultrasounds claimed under Medicare was 243,345 in the six months from April to September 2000. Some women may have 3 or 4 scans during a pregnancy while others have none, but the available data suggests that the mean number of scans per woman during pregnancy was greater than two. NT ultrasound screening may substitute for the current use of ultrasound in the first trimester, with considerable implications for the cost-effectiveness of ultrasound screening. Nuchal translucency measurement in the first trimester of pregnancy 65 The extra cost of NT screening over current ultrasound examinations at either less than 12 weeks (MBS item number 55700 - $60) or 12-16 weeks (MBS item number 55704 $70) may be $30-40 rather than $100 (the fee applying to MBS item number 55706 genetic defect screening ultrasound 17-22 weeks). While the primary analysis assumes there will be no substitution for current first trimester ultrasound, the sensitivity analysis considers an 80 per cent substitution in the first trimester at a marginal cost of $40. Evidence from Snijders et al (1998) suggests that with a FPR of 5 per cent, the sensitivity of NT screening for trisomy 21 is 77 per cent (95% CI=72%, 82%). A figure of 77 per cent has been used for the detection rate of NT ultrasound screening in the primary modelled cost-effectiveness analysis. A combination of NT ultrasound, double biochemical markers and age screening might raise the detection rate to 86.4 per cent. Based on Table 27, double markers on their own would give a 64.6 per cent detection rate. Women who screen positive are assumed to be offered CVS or amniocentesis. The uptake of diagnostic testing following a positive screen is assumed to be 85 per cent with a 100 per cent detection rate and a procedure-related rate of fetal loss of 0.9 per cent irrespective of the test. The sensitivity analysis considers alternative assumptions about the detection rate and target risk group. Model construction The cost and outcomes associated with each strategy are calculated using a decision analytic model. The underlying assumptions about the natural history of trisomy 21 pregnancies and the characteristics of screening assumed in the primary analysis are presented in Tables 30 and Table 31 respectively. The economic assumptions are presented in Table 32. Table 33 shows the structure of the primary model with respect to NT ultrasound screening while Table 34 explains the model as it applies to biochemical screening. Variations on the assumptions of the primary model, including the age of women screened, are described and analysed in Appendix H. Table 30 Natural history of trisomy 21 pregnancy and screening characteristics assumed in primary analysis Factor in analysis Rate of trisomy 21 births Spontaneous loss of fetus from time of NT to term Spontaneous loss of fetus from time of second trimester biochemical screen to term NT ultrasound detection rate NT ultrasound false positive rate Second trimester biochemical screening detection rate Serum testing false positive rate Combined NT ultrasound and first trimester biochemical screening detection rate Occurrence (%) 0.16 40 23 77 5 64 5 86 NT = nuchal translucency 66 Nuchal translucency measurement in the first trimester of pregnancy Table 31 Screening and diagnostic test characteristics assumed in primary analysis Level of uptake / fetal losses associated with test Uptake of antenatal diagnostic test Amniocentesis procedure-induced fetal loss rate CVS procedure-induced fetal loss rate Termination of affected pregnancy Screening coverage with biochemical markers Screening coverage with ultrasound Occurrence (%) 85 0.9 0.9 90 100 100 CVS = chorionic villus sampling Table 32 Unit cost assumptions in primary analysis Resource type Unit cost Source $54.50 Fee applying to MBS item number 66740 (second trimester biochemical test) NT ultrasound screening cost per woman $100.00 Fee applying to MBS item number 55706 (second trimester ultrasound) Antenatal diagnosis cost first trimester CVS $683.00 MBS costs of ultrasound and karyotyping Antenatal diagnosis cost second trimester amniocentesis $782.90 MBS costs of ultrasound and karyotyping Biochemical screening cost per woman (first or second trimester) Additional counselling for positive screens who do not have a diagnostic procedure $20.00 Estimate based on expert opinion Dating first trimester ultrasound $60.00 Fee applying to MBS item number 55700 (first trimester ultrasound) $1,016.00 DRG based costs from National Hospital Cost Database $905.00 DRG based costs from National Hospital Cost Database Cost of termination Cost of procedure-induced fetal loss CVS = chorionic villus sampling; DRG = diagnostic related group; MBS = Medicare Benefits Schedule; NT = nuchal translucency The decision analysis framework is identical for both NT ultrasound and serum screening, with changes only in the probability of detection and associated costs. The framework is very similar to previous models in the literature. In particular, the formal methods of calculation are identical to Wald et al (1997b) in calculating the cost per trisomy 21 pregnancy detected. However in the current model no explicit calculation of the cost per trisomy 21 birth avoided has been undertaken. Note that, given the high rate of natural miscarriage in trisomy 21 pregnancies, the cost per case detected gives more emphasis to early risk information and less to the actual outcome at birth. The earlier the screening, the lower the cost per affected fetus detected, compared with the cost per future trisomy 21 birth detected. For each strategy, the model starts with a cohort of births and calculates the number of affected and unaffected births screened in a given trimester. An assumed spontaneous fetal loss rate allows the model to calculate the number of affected and unaffected pregnancies screened. The calculation of the number of trisomy 21 pregnancies detected would be (the number of affected pregnancies screened) × (detection rate). The number of trisomy 21 births prevented is (the number of affected births screened) × (detection rate) × (uptake of antenatal diagnosis) × (uptake of termination). Nuchal translucency measurement in the first trimester of pregnancy 67 The cost of pre-test information and counselling, including any dating ultrasound scan, is assumed to be the same for each screening modality and is therefore excluded from the primary analysis. In the sensitivity analysis the assumption that NT screening will substitute the dating ultrasound to some extent is incorporated by limiting the cost of NT screening (to the excess over a dating ultrasound). The cost of screening affected pregnancies must include not only the cost of the test, but for those who have a positive screen, the cost of counselling and for a proportion, the cost of antenatal diagnosis, an additional ultrasound scan and, for some, termination of the pregnancy. The NT ultrasound screen may involve post-test counselling at the time of the screen for those who screen positive, given the immediacy of the results. Biochemical screening will probably involve an additional visit to discuss the results. Nevertheless, it may be that there is little difference in the actual time spent counselling, and, in this analysis, any differences have been ignored. Given the comparatively small number of positive cases, this is unlikely to have any significant impact on the economic analysis. Those who decline further diagnosis are likely to receive additional counselling, and a cost of $20 has been included for this. For those who accept the diagnostic test, there is the risk of loss of an unaffected fetus. For those affected and who test positive, there is the risk of an “unnecessary” termination if the pregnancy would have resulted in spontaneous miscarriage. The cost of that termination is offset against the resource cost of a miscarriage. Table 33 NT ultrasound screening for trisomy 21 for all pregnant women (260,000 live births) Trisomy 21 pregnancies NT screening 12 weeks Detection rate CVS Decline Accept 77 15 85 No. of women Cost per woman 693 $100 Unaffected pregnancies $69,333 534 80 No. of women Total cost FPR 5% $20 $1,602 Decline 15% 85% 454 $626 $283,980 Accept Termination 90% 408 $905 $369,609 Fetal loss 0.9% Spontaneous miscarriage 40% 114 $905 $103,143 Live trisomy 21 births Total cost Cost per woman Total cost 259,584 $100 $25,958,400 1,947 $20 $38,938 $626 $6,904,026 $905 $89,858 99 171 $827,667 Total cost of screening $32,991,222 $33,818,889 CVS = chorionic villus sampling; FPR = false positive rate; NT = nuchal translucency 68 Nuchal translucency measurement in the first trimester of pregnancy Table 34 Biochemical screening for trisomy 21 for all pregnant women (260,000 live births) Trisomy 21 pregnancies No of women 1st trimester Cost per woman Unaffected pregnancies Total cost No of women Cost per woman Total cost 259,584 $54.50 $14,147,328 693 Miscarriage rate 22% 2nd trimester 153 540 $905 $54.50 $138,532 $29,444 – Biochemical screen Detection rate 64% 346 – Amniocentesis Decline 15% 52 $20 $1,037 Decline 1,947 $20 $38,938 Accept 85% 294 $581 $170,698 Accept 11,032 $581 $6,407,571 Termination 90% 265 $1,016 $268,743 Fetal loss 99 $905 $89,858 Spontaneous miscarriage 23% 63 $905 $57,397 Live trisomy 21 births 12,979 212 Total cost $665,851 $20,683,695 Total cost of screening $21,349,547 Results In the absence of screening or diagnosis in a population of 260,000 live births, 693 trisomy 21 pregnancies could be expected at 11 weeks, with 540 cases at 16 weeks and 416 live trisomy 21 births. Table 35 suggests that second trimester biochemical screening will detect 346 cases of trisomy 21 per year at a cost of $21.4million ($61,746 per case detected). If NT ultrasound screening is introduced, it will add an additional $12.5 million but detect a further 188 cases. If universal NT ultrasound screening was implemented and combined with biochemical screening in the first trimester, the extra cost would be $14.3 million but there would be 65 additional cases detected. If we only consider NT ultrasound screening plus biochemical screening in the first trimester compared with biochemical screening in the second trimester, the extra cost is $26.7 million with an extra 253 cases detected ($105,484 per extra case detected). The likely number of trisomy 21 births with second trimester biochemical screening, NT ultrasound, or a combination of NT and biochemical screening in the first trimester would be 212, 171 and 141, respectively. Table 35 Primary cost-effectiveness analysis of pregnancy screening strategies for trisomy 21 compared with next best strategy: cost per trisomy 21 case detected Number of cases detected Total cost ($) Cost per case detected ($) ∆ cases detected ∆ cost ($)a ∆ cost per case detected ($)a Biochemical screening (second trimester) 346 21,349,547 61,746 346 21,349,547 61,746 NT ultrasound screening 534 33,818,889 63,347 188 12,469,342 66,291 NT ultrasound screening + first trimester biochemical testing 599 48,065,939 80,238 65 14,247,051 218,602 ∆ = incremental; NT = nuchal translucency a Rounded to the nearest whole number Nuchal translucency measurement in the first trimester of pregnancy 69 The economic analysis of NT ultrasound screening has been limited by the nature of the data on the true detection rate for ultrasound screening. The primary analysis has assumed that ultrasound screening boosts detection compared with biochemical screening in the second trimester from 64.0 per cent to 77 per cent, while maintaining a 5 per cent FPR. If NT ultrasound is combined with first trimester biochemical screening, a detection rate of 86.4 per cent has been assumed. This key assumption is subject to considerable uncertainty given the quality of the trial data and the operator dependent characteristics of NT ultrasound screening in practice. While there is training and quality assurance in place, it is always unclear what level of detection is achieved in clinical practice. The modelling exercise has by necessity made a number of other assumptions on utilisation, costs and risk. The reviewers have made the best assumptions from the data available but there remains considerable uncertainty surrounding the parameters of the model. The results should therefore be viewed as only indicative of the range of likely costs and outcomes of alternative screening modalities. Figure 14: Cost effectiveness of universal screening options with 100% take up 60 NT and serum screening in 1st trimester 50 $ million 40 NT 30 Serum screening in 2nd trimester 20 10 0 0 100 200 300 400 500 600 cases detected Figure 14 illustrates the comparative costs and outcomes for the three screening options considered in the main analysis. The results of the modelling exercise suggest that if a difference in detection rate of 20 percentage points between combined screening with NT ultrasound plus biochemical markers in the first trimester and biochemical screening in the second trimester can be maintained in a universal NT screening program, then the former may cost an extra $26.7 million per year, with 253 more trisomy 21 cases detected and 71 fewer trisomy births a year. The incremental costs are $105,484 per extra case detected (see Appendix H; Table H-3). 70 Nuchal translucency measurement in the first trimester of pregnancy If screening was restricted to women aged 30 years or over, then the cost per case detected would be one third less. If screening was restricted to women aged 35 years or over, then the cost per case detected would be halved. With a high level of substitution of NT ultrasound screening for dating ultrasound in pregnancy and a reduction in the total amount of biochemical screening, it would be possible to achieve a resource saving. However, this is an unlikely scenario as most observers expect that NT screening would be combined with biochemical screening and is unlikely to replace more than half of dating ultrasound scans. The main analysis has not taken account of the current level of diagnostic testing in those 35 or over. Taking into account the conservative estimate that a third of women aged 35 years or more have an amniocentesis in the second trimester because of the risk associated with their age, one would expect to see 56 cases detected at a cost in excess of $9 million. Screening is less expensive than amniocentesis, with a lower detection rate. If done earlier in pregnancy it could, however, detect a higher absolute number of cases of trisomy 21 (a proportion of which would have resulted in spontaneous abortion) than amniocentesis. Provided that the take up of screening exceeded 43 per cent, and the detection rate was at least 86 per cent, the combination of NT and biochemical screening would dominate testing with amniocentesis (see Appendix H). In other words screening 43 per cent of women would save money and detect more cases compared to testing a third of women aged over 35 with amniocentesis. Taking account of the current rate of amniocentesis would improve the overall cost effectiveness of NT screening compared to current screening and diagnostic testing. It needs to be said, however, that screening by amniocentesis and CVS is already falling as a consequence of increased levels of biochemical screening and it is not known if a greater use of NT screening will lead to a reduction in diagnostic testing in women aged over 35. Although NT screening may offer greater direct visual reassurance to women, it may be that those at higher risk of an abnormal pregnancy may prefer to have the certainty of amniocentesis or CVS and may not be willing to accept the results of ultrasound and biochemical screening tests. If that is a common view, there might be little substitution in this age group. Sensitivity analysis around the main parameters of uncertainty suggests that, depending on the true detection rate in practice and the extent of substitution for dating ultrasound, the incremental cost per extra case detected would be in the range of $43,825 - $141,664. While considerable doubt remains about both its comparative effectiveness and its true comparative cost in clinical practice, it seems likely that the substitution of universal NT ultrasound screening for universal biochemical screening for trisomy 21 would lead to an extra cost of at least $11 million per year (with see Appendix H; Table H-7) and possibly closer to $27 million (Table 35). This estimate does not take into account the range of current screening practices in Australia. It is based on a subsidised screening test without consideration of the costs or outcomes of a coordinated population screening program with either maternal biochemical testing or ultrasonography. In addition, it should be noted that in calculating these figures no attempt has been made to take account of the social value of trisomy 21 births, in terms of either their potential future social contribution or costs of care. Nuchal translucency measurement in the first trimester of pregnancy 71 Relative cost-effectiveness has been calculated on the basis of costs per case detected. These are taken as proxies for the range of outcomes of screening. An important outcome is an increase in the quality and improvement in the timing of information of a potential fetal abnormality as this allows women to have an earlier, less physically (and perhaps emotionally) traumatic termination if they so choose. However, for others there would be an increase in unnecessary anxiety, invasive procedures and terminations of affected fetuses that would have otherwise miscarried before second trimester biochemical screening was done. The economic analysis suggests that the combination of NT ultrasound and biochemical screening in the first trimester when compared with biochemical screening in the second trimester, would lead to 155 “less traumatic” terminations, but also 44 additional terminations that would have otherwise resulted in a fetal loss before 16 weeks. 72 Nuchal translucency measurement in the first trimester of pregnancy Conclusions Safety The literature focusing on the safety of ultrasound in pregnancy is not of high quality. However, the ubiquitousness of the procedure and the fact that no major adverse events have come to light suggests that ultrasound in pregnancy is safe. Several professional organisations have issued recommendations about the use of specific types of ultrasonic imaging modalities based on indication, maternal and fetal characteristics and the potential for teratogenic or other adverse outcomes. These support the prudent use of the technology, stressing the importance of minimum output levels and exposure times. Effectiveness When used as a single modality, screening by measurement of NT in the first trimester has a detection rate for trisomy 21 of approximately 77-82 per cent at a false positive rate (FPR) of 5-8 per cent. For maternal biochemical screening, the comparable detection rate using double markers (PAPP-A and free β-hCG) in the first trimester of pregnancy is 65 per cent at an FPR of 5 per cent. For maternal biochemical screening during the second trimester using the triple marker test, the detection rate is 57-64 per cent and using the quadruple marker test the detection rate is 63-68 per cent. If used in combination in the first trimester, the detection rate with a 5 per cent FPR is 86 per cent for NT screening plus double markers (PAPP-A and free β-hCG), 87 and 88 per cent for NT plus triple markers PAPP-A, free β-hCG, AFP and PAPP-A, free βhCG, uE3 respectively and 88 per cent for NT plus quadruple markers (PAPP-A, free βhCG, AFP and uE3). Cost-effectiveness A universal maternal biochemical screening program in the second trimester with 100 per cent uptake by pregnant women would cost $21.3m. If a screening program of NT ultrasound plus maternal biochemical markers in the first trimester could achieve a 20 percentage point improvement in the detection rate of trisomy 21 compared with biochemical screening in the second trimester, then the modelled evaluation suggests that it may cost $26.7 million more per year, with 253 more trisomy 21 cases detected. The incremental cost is $105,484 per extra case detected. If screening was restricted to women aged 30 years or over, then the cost per case detected would be one third less. If screening was restricted to women aged 35 years or over, then the cost per case detected would be halved. Sensitivity analysis around the main parameters of uncertainty suggests that, depending on the true detection rate in practice and the extent of substitution for dating ultrasound and diagnostic tests in high risk pregnancies, the incremental cost per extra case detected would be in the range of $43,825 - $141,664. Nuchal translucency measurement in the first trimester of pregnancy 73 If a comparison is made between NT ultrasound in first trimester and biochemical screening in the second trimester then the additional cost is $12.5m with 188 extra cases detected. None of these cost effectiveness ratios considers the social value or cost of care for a trisomy 21 birth. Recommendations The MSAC considers that nuchal translucency screening (NTS), and NTS in conjunction with first trimester maternal biochemical screening (T1MBS), are safe and effective where provided by individuals with appropriate expertise in NTS. Hence NTS providers need to be appropriately accredited. However, the MSAC recommends that public funding should not be supported for NTS or NTS in conjunction with T1MBS as stand alone services, due to their poor cost-effectiveness. Consideration should be given to public funding of NTS or NTS in conjunction with T1MBS by incorporating, as far as possible, provision of the services into existing services provided in early pregnancy. The Minister for Health and Ageing accepted these recommendations on 16 October 2002. 74 Nuchal translucency measurement in the first trimester of pregnancy Appendix A MSAC terms of reference and membership The MSAC's terms of reference are to: • advise the Minister for Health and Ageing on the strength of evidence pertaining to new and emerging medical technologies and procedures in relation to their safety, effectiveness and cost-effectiveness and under what circumstances public funding should be supported; • advise the Minister for Health and Ageing on which new medical technologies and procedures should be funded on an interim basis to allow data to be assembled to determine their safety, effectiveness and cost-effectiveness; • advise the Minister for Health and Ageing on references related either to new and/or existing medical technologies and procedures; and • undertake health technology assessment work referred by the Australian Health Ministers’ Advisory Council (AHMAC) and report its findings to the AHMAC. The membership of the MSAC comprises a mix of clinical expertise covering pathology, nuclear medicine, surgery, specialist medicine and general practice, plus clinical epidemiology and clinical trials, health economics, consumer affairs and health administration and planning: Member Expertise or Affiliation Dr Stephen Blamey (Chair) general surgery Professor Bruce Barraclough general surgery Professor Syd Bell pathology Dr Paul Craft clinical epidemiology and oncology Professor Ian Fraser reproductive medicine Professor Jane Hall health economics Dr Terri Jackson health economics Ms Rebecca James consumer health issues Professor Brendon Kearney health administration and planning Mr Alan Keith Assistant Secretary, Diagnostics and Technology Branch, Commonwealth Department of Health and Ageing Associate Professor Richard King internal medicine Dr Ray Kirk health research Dr Michael Kitchener nuclear medicine Mr Lou McCallum consumer health issues Emeritus Professor Peter Phelan paediatrics Dr Ewa Piejko general practice Dr David Robinson plastic surgery Professor John Simes clinical epidemiology and clinical trials Nuchal translucency measurement in the first trimester of pregnancy 75 76 Member Expertise or Affiliation Professor Richard Smallwood Chief Medical Officer, Commonwealth Department of Health and Ageing Dr Robert Stable Representing the Australian Health Ministers’ Advisory Council Professor Bryant Stokes neurological surgery Professor Ken Thomson radiology Dr Douglas Travis urology Nuchal translucency measurement in the first trimester of pregnancy Appendix B Supporting committee Supporting committee for MSAC Reference 04a – Nuchal translucency measurement in the first trimester of pregnancy for screening of trisomy 21 and other autosomal trisomies Dr Paul Hemming (Chair) MB, ChB, FRACGP, FRCGP, FAMA President Royal Australian College of General Practitioners member of the MSAC Dr Matthew Andrews MBBS (Hons), MMed, FRANZCR Radiologist, Linacre Private Hospital, Hampton nominated by the Royal Australian and New Zealand College of Radiologists Associate Professor Lachlan de Crespigny MD, BS, FRCOG, FRANZCOG, DDU, COGU Honorary Fellow Murdoch Children’s Research Institute, Melbourne; Department of Obstetrics and Gynaecology University of Melbourne nominated by the Australian Association of Obstetrical and Gynaecological Ultrasonologists Professor David A Ellwood MA, DPHIL (Ocon), FRANZCOG, DDU Associate Dean, Canberra Clinical School University of Sydney; Professor of Obstetrics & Gynaecology Director of Fetal Medicine Unit The Canberra Hospital nominated by the Royal Australian and New Zealand College of Obstetricians and Gynaecologists Dr Peter Garcia-Webb MBBS, MD, FRCPA, FAACB Head, Department of Clinical Biochemistry Mayne Health, Western Diagnostic Pathology nominated by the Pathology Services Advisory Committee Associate Professor Eric Haan BMedSc, MBBS, FRACP Clinical Geneticist and Head South Australian Clinical Genetics Service Women's and Children's Hospital, North Adelaide co-opted clinical geneticist Ms Dell Horey BAppSc, MMedSc Convenor, Maternity Alliance consumer representative Dr John Primrose MB, BS (Hons), FRANZCR Senior Medical Adviser Health Access and Financing Division Department of Health and Ageing Medical Advisor to the MSAC Nuchal translucency measurement in the first trimester of pregnancy 77 Dr Amanda Sampson MBBS, DObstRCOG, FRANZCOG, DDU, COGU Ultrasonologist Women's Imaging Centre Freemasons Hospital Medical Centre East Melbourne nominated by the Royal Australian and New Zealand College of Obstetricians and Gynaecologists Dr Peter Warren MB, ChB, Dip Obst, FRANZCR, DDU Director of Medical Imaging Royal Hospital for Women, Randwick nominated by the Royal Australian and New Zealand College of Radiologists Ms Linda Marshall BSc, BA, MBA MSAC Project Manager Diagnostics and Technology Branch Department of Health and Ageing 78 Nuchal translucency measurement in the first trimester of pregnancy Appendix C Table C-1 Studies included in the review General characteristics of studies on NT measurement meeting entry criteria Location Date of enrolment Cases Maternal agea Quality criteria (ABCDE)b UK 1992 to 1993 3 29.8c Y1YNY Borrell et al (1996, 1997) Spain 1991 to 1993 47 ? Y2YNY A or CVS Brambati et al (1995) Italy 1992 to 1993 26 ? Y2YNY CVS Austria 1993 to 1994 4 26 Y2NNY A Australia 1989 to 1993 5 35c Y1YNY A or CVS Hyett et al (1995) UK ? 36 ? Y2NUY CVS Hyett et al (1996) UK 1993 to 1995 70 ? Y2NNY CVS Kornman et al (1996) The Netherlands 1994 7 38 Y2YNY A or CVS Martinez et al (1997) Spain ? 9 38 Y2YNY CVS Nicolaides et al (1994, Pandya et al (1994) UK 1990 to 1994 61 35 Y1YYY A or CVS Pandya et al (1995b) UK 1990 to 1994 101 35 Y2NNY A or CVS Salvoldelli et al (1993) Switzerland 1985 to 1991 28 ? Y2YNY CVS Schwarzler et al (1999) UK 1996 to 1997 12 29.4c Y1YNY Karyotyping, pregnancy outcome Scott et al (1996) Australia 1993 to 1995 8 38c Y2YNY CVS UK ? 326 31 Y2YNY A or CVS Szabo et al (1995) Hungary ? 31 ? Y2YNY CVS, cordocentesis Thilaganathan et al (1999) UK 1994 to 1998 21 28.6c Y5NUY CVS France 1988 to 1991 9 ? Y2YNY A or CVS Reference Bewley et al (1995), Roberts et al (1995) Hafner et al (1995) Hewitt (1993) Snijders et al (1998) Ville et al (1992) Population Reference test Karyotyping, pregnancy outcome A = amniocentesis; CVS = chorionic villus sampling; N = no; Y = yes; ? = unknown or unstated a Values are medians unless otherwise stated b Quality criteria are listed in Table 16 c Mean Nuchal translucency measurement in the first trimester of pregnancy 79 Appendix D Existing recommendations US National Institutes of Health Consensus Development Programs Following an earlier Consensus Development Conference convened by the US National Institutes of Health (NIH) in 1984 (Anonymous 1984), the Routine Antenatal Diagnostic Imaging with Ultrasound Study (RADIUS) Group conducted a randomised controlled trial on the routine use of ultrasound screening for women at low risk of poor pregnancy outcomes (Ewigman et al 1993, LeFevre et al 1993, Crane et al 1994). The study examined the experience of more than 15,000 women over several years with results published in the early 1990s. One of the substudies focused on fetal anomalies, examining the impact of detection on management and survival. It found that while ultrasonography detected more than three times as many anomalous fetuses, it did not significantly influence the management or outcome of pregnancies complicated by congenital malformations. In addition, ultrasonography had no significant impact on survival rates among infants with potentially treatable, life threatening anomalies despite the opportunity to take precautionary measures such as delivery in a tertiary centre (Crane et al 1994). Reanalysis of the RADIUS results by other authors raised concerns that the main findings were predicated on a certain level of operator skill or that there were system-wide differences in detection rates for the screening of malformed fetuses. Romero (1993) found that the detection rate in six European centres was 7.5 per 1,000 compared with about 6.8 per 1,000 in tertiary centres participating in the US study. Tertiary centres in Europe were found to be 4.4 times (95% CI=2.1, 9.5) more likely to identify a structural malformation than centres in the RADIUS Group (OR=3.9; 95% CI=1.6, 9.8) (Romero 1993). Extending this argument, DeVore suggested that reimbursement by third-party payers which is dependent on the diagnostic skill of the operator, will produce a favourable cost-effectiveness profile for the screening procedure (DeVore 1994). In 1993, the NIH Technology Assessment Workshop was convened to discuss the impact of the results on public health and reimbursement policies. It did not reach a policy position. Canadian Task Force on the Periodic Health Examination The Canadian Guide to Clinical Preventive Health Care was released by the Canadian Task Force on the Periodic Health Examination in 1994. It states that there is “fair evidence” to support offering triple marker screening (alpha-fetoprotein, human chorionic gonadotrophin and unconjugated oestriol) to women under 35 years of age when a comprehensive screening and prenatal diagnosis program (with education, interpretation and follow-up) is available. Screening with maternal biochemical markers outside a fully coordinated program is deemed undesirable. Triple marker screening followed by prenatal diagnosis may be offered to women over 35 years of age as an alternative to prenatal diagnostic techniques alone. 80 Nuchal translucency measurement in the first trimester of pregnancy Ultrasonographic screening using nuchal translucency (NT) is not recommended for trisomy 21 as part of the periodic health examination of pregnant women due to concerns about measurement reliability and generalisability. US Preventive Services Task Force The Guide to Clinical Preventive Services is a series of recommendations from the US Preventive Services Task Force (USPSTF) that is intended to provide clinicians with information on the effectiveness of different clinical preventive services and the quality of evidence on which recommendations are made. The second edition of the Guide, published in 1996, recommends offering screening for trisomy 21 using multiple maternal biochemical markers at 15-18 weeks of gestation to all pregnant women although it does not recommend a particular marker combination. It suggests patients have access to counselling and follow-up services, skilled high-resolution ultrasound and amniocentesis capabilities, and reliable and standardised laboratories. The Guide states that there is insufficient evidence to recommend for or against routine ultrasound examination as a screening test for trisomy 21. Royal College of Obstetrics and Gynaecology In 1997, the Royal College of Obstetrics and Gynaecology Study Group on Screening for Down Syndrome in the First Trimester published the following findings (RCOG 1997): 1) Although there appeared to be insufficient evidence to recommend routine screening for trisomy 21 in the first trimester by biophysical and biochemical markers: a) there were sufficient data to consider screening for trisomy 21 by the measurement of NT at 10-14 weeks gestation an acceptable procedure. Preliminary reports indicated that the detection rate for a given FPR are at least similar, if not superior, to biochemical screening with multiple markers at 15-22 weeks gestation. However NT screening should only be conducted where: i) centres had staff with a high level of ultrasound competence and had been certified by an external agency and subjected to external quality control procedures; and ii) centres had high standard precision equipment, clinical protocols and external systems of quality assurance and ongoing audit. Nuchal translucency measurement in the first trimester of pregnancy 81 b) there were sufficient data to consider that specific biochemical markers for trisomy 21 at 9-13 weeks gestation (notably pregnancy-associated plasma protein-a and beta human chorionic gonadotrophin) were as effective as those biochemical markers in established use at 15-22 weeks gestation. There may be additional biochemical markers that will become applicable in the first trimester. The introduction of biochemical markers in first trimester screening for trisomy 21 should only be considered when: i) robust assay kits, which meet international standards, were available; ii) centres demonstrated that their staff had expertise and experience in the use of these tests; and iii) centres had clinical protocols and systems of quality assurance and ongoing audit. c) the combined use of screening with NT and biochemical markers in the first trimester (9-13 weeks gestation) might have a detection rate for trisomy 21 superior to either biochemical markers or NT screening alone. 2) As screening for trisomy 21 in the first trimester with biochemical and ultrasound markers requires the active participation of the health professions in the community as well as institutions, the following issues need to be addressed: a) education and training of health professions such as family doctors, midwives, obstetricians and health visitors; b) increased provision of information to health professionals and pregnant women; c) expansion of counselling services; d) expansion of expertise on regularly performed diagnostic tests such as chorionic villus sampling (CVS) and early amniocentesis. This may require a policy of centralisation of these services until the safety of these techniques is demonstrated by clinicians intending to provide these interventions. Recommendation of minimum numbers of cases to be performed is important; e) a revision in the provision of therapeutic abortion services; f) central quality assurance of a continuing audit of counselling, information and education as well as biochemical and biophysical tests; g) a recommendation regarding the advisability of nationwide screening for trisomy 21; and h) evaluation of the cost implications of the introduction of a national policy of screening for trisomy 21. 82 Nuchal translucency measurement in the first trimester of pregnancy Particularly for Point 1 and its subpoints, three members of the study group held a dissenting opinion. They raised the following points (see RCOG 1997): • it has not been shown that NT measurement is a better screening test than second trimester screening using four biochemical markers (refer to Point 1a); • NT measurement required quality control, but they did not agree that a case had been made to limit NT measurement to centres certified by an external agency (refer to Point 1ai); • first trimester biochemical screening was, on current evidence, not as effective as second trimester screening using four markers (refer to Point 1b); • since the results of first trimester biochemical and ultrasound testing were not correlated, their combination must be more effective than either alone, although the precise method of combining these two tests was still being developed (refer to Point 1c); and • further research was needed to compare the performance of first and second trimester screening to determine which should be recommended for use in routine screening practice. In 1998, RCOG convened a working group to recommend a standard format for ultrasound scans conducted in the 20th week of gestation. In its report, the working group concluded that current evidence suggested that scanning for NT was an effective way of determining babies at risk of trisomy 21 and was best performed at 10-14 weeks. Whether NT screening was preferable to serum testing remained to be decided and it was most likely that a combination of serum testing and NT measurement would produce the highest sensitivity for the lowest FPR. However, whether or not NT screening would be introduced was a funding issue (see RCOG 2000). Human Genetics Society of Australasia A policy endorsed by the Human Genetics Society of Australasia (HGSA) in 1997 made the following recommendations: • The increasing indications for prenatal diagnosis make it necessary to have available a specialised team for prenatal diagnosis of birth defects and genetic diseases. This team should consist of clinical and laboratory services; • Each State requires at least one specialised prenatal diagnostic service that may be a discrete unit or a group of collaborating health professionals working in a coordinated service. Such clinical units should be located in tertiary obstetric facilities; • Each such clinical service requires the services of a clinical geneticist, genetic counsellor or nurse specialising in prenatal diagnosis, obstetrician (skilled in antenatal diagnosis and ultrasound), social worker, clinic coordinator and secretarial assistance. Some services also have another clinician skilled in antenatal ultrasound (ultrasonologist) as well as the obstetrician; Nuchal translucency measurement in the first trimester of pregnancy 83 84 • Each prenatal diagnosis service should have an expert ultrasound team led by a subspecialty trained medical specialist (obstetrician or radiologist) who is well versed in fetal and obstetric ultrasound. Ultrasonologists should have the qualifications of Certification in Obstetric and Gynaecological Ultrasound (COGU), Certification in Maternal-Fetal Medicine (CMFM) or the equivalent in experience and knowledge. If sonographers are used, they should also have special training in fetal anomaly detection and obstetric ultrasound and be appropriately supervised. The units should use modern, high-resolution ultrasound equipment; • Clinical management where a fetal anomaly is found and the implications are unclear should include seeking further opinions from relevant specialists (e.g. clinical geneticist, paediatric surgeon or neurosurgeon). A multidisciplinary group discussion to consider options for management should be encouraged; • Amniocentesis, CVS and fetal blood sampling should be performed in a prenatal diagnosis service where the operator(s) have sufficient training and annual experience of the procedure to keep the complication rates as low as possible. There is evidence that fetal loss rate for CVS is operator and experience-dependent. Prenatal diagnosis services that do not perform large numbers of specific procedures per year should be encouraged to refer their cases to a prenatal diagnostic service that does. Each prenatal diagnosis service should be expected to monitor its own performance of prenatal diagnosis procedures and make available statistics about its sampling success rate, proportion of abnormalities detected, fetal loss rate and other complications; • The prenatal diagnostic service should be closely associated with clinical genetic and diagnostic facilities in each State to allow effective counselling of the extended family if required; • Maternal biochemical screening for trisomy 21 and neural tube defects should be considered an accepted prenatal diagnostic option. Laboratories offering maternal biochemical screening should have sufficient throughput to maintain standards and audit results. The maternal biochemical screening service should be part of a well organised program which coordinates laboratory testing, education of patients and doctors, and counselling of patients. The prenatal diagnosis and ultrasound investigations should be the responsibility of the prenatal diagnostic service; • Facilities for prenatal diagnosis should be available at least for the following: – all women of 37 years and over (some States offer prenatal diagnosis at the age of 35 years and over, and this policy statement is not meant to alter this practice, but states 37 years as a minimum standard); – all women who have previously had a child with a neural tube defect or been determined to be at increased risk for such, in light of a serum alpha-fetoprotein test; – all women who have had a biochemical screening test for trisomy 21 that suggests the chromosome abnormality risk is greater than the accepted cutoff being used in the protocol; and – all other women who have a high risk of a fetus with a diagnosable defect, (e.g. ultrasound-detected abnormality, inborn error of metabolism, DNA-identifiable condition). Nuchal translucency measurement in the first trimester of pregnancy • The choice between CVS, amniocentesis, biochemical screening and ultrasound should be on the basis of informed consent that takes into consideration the test risks, timing, accuracy and method of termination (if affected); • Couples should receive appropriate counselling, ideally well before the diagnostic procedures are performed. This must include at least discussion of the risk of recurrence, the benefits and risks of the procedure, and the couple’s intended response to an abnormal result. Educational material should be supplied. • Interpretation of results should be a team responsibility. The results should be communicated to the referring doctor and patient as soon as possible and in a manner that ensures clear understanding. • The action to be taken on the basis of abnormal results is a decision for the couple concerned, based on the information given with full counselling support. Where termination of pregnancy is undertaken, it should be on the basis of a written diagnostic report. • The outcome of all pregnancies where prenatal diagnosis has taken place should be monitored in a standard manner. Each prenatal diagnostic unit should monitor the outcome of all CVS, amniocentesis and fetal blood sampling at regular intervals. The pathological examination of the aborted fetus and placenta should be done by a pathologist experienced in fetal pathology with due regard to confirmation of the amniocentesis result. This should include fetal radiography, cytogenetic analysis and any appropriate biochemical investigation. In October 2000, draft guidelines were made available for comment. Royal Australian and New Zealand College of Obstetricians and Gynaecologists A statement endorsed in June 2000 by the Royal Australian and New Zealand College of Obstetricians and Gynaecologists (RANZCOG) makes the following “best practice” recommendations: • Women who are considered to be at increased risk for aneuploidy, based on clinical history (advanced maternal age or previous affected pregnancy), should be offered the choice of screening by nuchal translucency screening or second trimester maternal biochemical screening, or diagnostic testing (either CVS or amniocentesis). All procedures should be performed by experienced operators who have had appropriate training. Access to consultation with a clinical geneticist should be available. General counselling support for women and their families should also be available as part of the prenatal diagnosis service; • Women who are not considered to be at increased risk should be made aware of the availability of screening tests for trisomy 21 and other chromosomal abnormalities. This should include NT screening and second trimester maternal biochemical testing. The relative advantages and disadvantages of the available screening tests should be discussed, as well as performance information based on the audit figures of local providers of the screening services. Regional variations in access to different forms of testing should also be taken into account when recommending a screening test to individual women; Nuchal translucency measurement in the first trimester of pregnancy 85 86 • NT screening should only be performed by trained operators, using a risk assessment program that incorporates NT, crown-to-rump length (CRL) and maternal age. This test should be done when the fetus has a CRL of 45-84 mm, which corresponds to 1113 weeks; • The second trimester biochemical screen should usually be done between 15 and 18 weeks gestation and a risk assessment performed incorporating maternal age and weight, using a software package developed for that purpose. Some programs may offer a wider gestational age range, and referring practitioners should be aware of local guidelines; • Sequential testing (e.g. NT screening followed by second trimester biochemical screening) is not currently recommended as a population screening method. However, it should be recognised that some women may choose to have a number of different screening tests and accept that this may increase their chance of a high-risk result; • All women who choose to have an antenatal screening test for trisomy 21 and other fetal aneuploidy should have appropriate pre-test counselling, including the provision of written information to ensure they have a complete understanding of the test and its accuracy. All women receiving a high-risk test result should be provided with adequate post-test counselling. The level of counselling support needed may vary with the type of result and the resources of the referring practitioner to deal with the issues surrounding an abnormal result. Abnormal screening test results should be treated as urgent clinical problems requiring early referral to an individual or centre able to provide both counselling and diagnostic procedures for prenatal diagnosis; • All providers of biochemical and ultrasound based screening tests for trisomy 21 and other fetal aneuploidy should maintain comprehensive records and appropriate followup of cases so they know their own screening test characteristics. They should maintain a continuing audit of their screening practice and be able to provide the users of their service with accurate and current information on the numbers of pregnancies screened, the detection rate and the screen positive rate. Ideally, providers should contribute data to a central body to facilitate pooling of data and allow for external scrutiny of results; and • Women’s understanding of, and satisfaction with, the screening methods should be assessed so that appropriate information and education can be offered. Nuchal translucency measurement in the first trimester of pregnancy Appendix E Ongoing primary studies Serum, Urine and Ultrasound Screening Study The UK National Health Service (NHS) Research and Development Health Technology Assessment Programme, through the National Coordinating Centre for Health Technology Assessment (NCCHTA), commissioned a study to assess the individual and combined performance of serum, urine and ultrasound markers in the first trimester of pregnancy. The study – called the Serum, Urine and Ultrasound Screening Study (SURUSS) (NHS 2000) – started in 1996 and is expected to involve 52,000 women recruited from 15 centres. Ultrasound nuchal translucency (NT) measurements will be taken at 10-12 weeks gestation and serum and urine samples collected at this time and also at the time of routine screening (about 16 weeks gestation). The study is also expected to specify the organisational arrangements necessary for the implementation of the most effective screening method. Results are expected to be released in early 2001. First and Second Trimester Screening Study The First and Second Trimester (FaST) Screening Study is an Australian project that commenced in 1998, involving Monash University and Monash Medical Centre. It is funded jointly by Monash University and the Victorian State Government through the Department of Human Services (Anonymous 2000). The study is attempting to assess the relative merits of screening for trisomy 21 in a multiracial Australian population by enrolling up to 15,000 pregnant women. The study is expected to be completed in late 2001. The specific aims of FaST are: • to evaluate NT as a prenatal screening marker for trisomy 21 in an Australian population; • to evaluate free beta human chorionic gonadotrophin (β-hCG) and pregnancyassociated plasma protein as first trimester biochemical markers for trisomy 21 in an Australian population; • to evaluate urinary β-core fragment and hyperglycosylated hCG as prenatal screening markers for trisomy 21 in an Australian population in both the first and second trimesters of pregnancy; • to define the optimum second trimester biochemical marker combination of inhibin A, free α-hCG, free β-hCG, alpha-fetoprotein (AFP) and unconjugated oestriol (uE3) in an Australian population; • to assess the relationships between the above markers and to evaluate the usefulness of the various combinations, comparing these to current second trimester “quadruple screening” (free β-hCG, free α-hCG, AFP, uE3); Nuchal translucency measurement in the first trimester of pregnancy 87 • to provide cost analyses, in terms of cost per trisomy 21 pregnancy identified, for each of the above screening strategies, alone and in combination, to describe the optimal, most cost-effective prenatal screening strategy for trisomy 21 in an Australian population; • to record women’s preferences for the timing of, and approach to, trisomy 21 screening; and • to define preferences and screening uptake rates by ethnicity. First and Second Trimester Evaluation of Risk Trial The First and Second Trimester Evaluation of Risk (FaSTER) Trial is funded under a US$10 million three year grant from the National Institutes of Health (NIH) and the US National Institute of Child Health and Human Development (NICHHD). The study is a multicentre, non randomised longitudinal study enrolling concurrent controls. It uses a non interventional trial design to compare the accuracy of first and second trimester non invasive screening methods for trisomy 21 and other chromosomal abnormalities versus diagnosis at delivery or fetal loss. The study is in the early stages of recruiting, through participating obstetric centres, pregnant women between the ages of 16 and 45 years; measurements will be taken before 10-14 weeks gestation, with a minimum sonographic fetal crown-to-rump length (CRL) of 38-84 mm. FaSTER is expected to enrol 62,000 patients in 11 centres across the United States. Participating centres include the New England Medical Center, Tufts University School of Medicine, Boston; Women and Infants Hospital, Brown University School of Medicine, Providence; Mount Sinai Medical Center, Montefiore Medical Center, Albert Einstein College of Medicine, New York; Intermountain HealthCare System, University of Utah School of Medicine, Salt Lake City; William Beaumont Hospital, Royal Oak; University of Texas Medical Branch, Galveston; University of Colorado Health Sciences Center, Denver; and the Swedish Hospital Medical Center, Seattle. As of April 2000, all staff training and software development had been completed and first semester laboratory norms established. About 2,600 women had been recruited. An interactive FaSTER trial website has been established (http://www.firsttrimester.org). It assists patients in establishing their due date and deciding on their eligibility for enrolment in the FaSTER trial. 88 Nuchal translucency measurement in the first trimester of pregnancy Appendix F Summary of meta-analysis of studies on nuchal translucency measurement in the detection of trisomy 21 applying set cutoff measures Table F-1 summarises the diagnostic test characteristics of nuchal translucency (NT) measurement according to cutoff value. Most studies used a sonographic transducer of 3.5 MHz or above, although five studies failed to report this information. Reported sensitivities ranged from 13.8 per cent (Ville et al 1992) to 100 per cent (Hewitt 1993), although most fell between 40 and 70 per cent. Only about half the studies reported a value for specificity. In these studies, the probability of the test correctly detecting people without disease ranged from 68 per cent (Martinez et al 1997, Kornman et al 1996, Scott et al 1996) to close to 100 per cent. A meta-analysis was performed on six studies that gave results for both sensitivity and specificity at a cutoff of ≥ 3 mm. Application of a random effects model to the data resulted in a pooled measure of sensitivity and specificity of 62 per cent (95% CI=40, 80%) and 93 per cent (95% CI=79, 98%), respectively. A likelihood ratio of 8.8 is computed from pooled results, implying that a positive test result is 8.8 times more likely to occur in pregnancies affected with trisomy 21 compared with those without trisomy 21. Nuchal translucency measurement in the first trimester of pregnancy 89 Table F-1 Performance characteristics of nuchal translucency measurements in collected studies, arranged according to cutoff values Ultrasound characteristics Route Age of gestation (weeks)b Detection rate (%) False positive rate (%) Likelihood ratio 5 TA 12 50.0 1.2 41.7 Borrell et al (1996, 1997), Comas et al (1995) 3.5 TA 13-18c 40.4d 3.7 10.9 Martinez et al (1997) 6.5 TV 11 44.4 d NA NA 5 TA 12 72.8 d NA NA 3.5, 5 TA 10–13 c 50.0 NA NA Scott et al (1996) 5 TA 10–13 c 37.5 d NA NA Bewley et al (1995), Roberts et al (1995) 3.5, 5 ? 11 33.3 6.1 5.4 Brambati et al (1995) 3.5, 5 TA/TV 8-15 c 26.9 3.2 8.4 Hyett et al (1995) ? ? 10–13 c 69.4 d NA Pandya et al (1995b) 5 TA 12 76.0 d 31.4 2.4 Szabo et al (1995) 3.5, 6.5 TA/TV 9-12 c 90.3 d 6.8 32.2 Pandya et al (1994), Nicolaides et al (1994) 5 TA 11 73.8 d 31.6 2.3 Ville et al (1992) ? TA/TV 9–14 c 13.8 NA Hewitt (1993) ? ? 11w 4de 100.0 NA NA Savoldelli et al (1993) 2.5, 3.75 TA 9w 3d – 12w 5d c 53.6 NA NA Referencea Transducer (MHz) 2.5 mm cutoff: Hafner et al (1995) 3.0 mm cutoff: Hyett et al (1996) Kornman et al (1996) 4.0 mm cutoff: NA NA NA CRL = crown-to-rump length; d = days; NA = not available; TA = transabdominal; TV = transvaginal; w = weeks; ? = unknown or unstated a Studies shaded and in bold type are included in a meta-analysis of diagnostic test characteristics b Values are medians unless otherwise stated c Figures presented are ranges d Indicates that while various cutoffs are presented, the results for a thickness of ≥ 3 mm are given e Figures presented are mean 90 Nuchal translucency measurement in the first trimester of pregnancy Appendix G Summary of comparative studies of cost-effectiveness in screening for trisomy 21 using NT ultrasound, biochemical and age screening Roberts et al (1998) Choosing options for ultrasound screening in pregnancy and comparing cost effectiveness: a decision analysis approach Country: UK Screening strategy and comparators: Ultrasound screening alternatives including ultrasound screening in the first trimester compared with no screening. Comments: Assumes that ultrasound screening has an expected detection rate of 5085 per cent for trisomy 21 and 10-30 per cent for other lethal abnormalities. The average cost for ultrasound screening in the first trimester in 1996 pounds was £30,583-217,099 per 1,000 women, with 1.58 cases detected and 8.93 cases missed. This suggests a cost per case detected of £19,356-255,410. False positives and procedure-related miscarriages appear to have been costed but the numbers are not reported. A cost per malformation avoided is not reported either. The study does not appear to take account of the natural rate of miscarriage and assumes a pregnancy prevalence of trisomy 21 of 1.5 per 1,000 (rather than a birth prevalence). It therefore underestimates the costs of screening and diagnosis and bases the number of cases detected as the number of cases detected at term. Serra-Pratt et al (1998) Trade-offs in prenatal detection of Down syndrome Country: Spain Screening strategy and comparators: Eight options were considered: 1. Do nothing. 2. Offer amniocentesis to all women (average 50 per cent uptake). 3. Offer amniocentesis to pregnant women aged over 35 and ultrasound screening to others. 4. Triple test biochemical screening for all women, applying a 1:250 risk cutoff. 5. As above, with a 1:100 risk cutoff. 6. Offer amniocentesis to women aged over 38, triple biochemical screening to others and, if the risk is above 1:270, offer ultrasound screening. 7. Offer triple biochemical screening to all women aged over 30 with a risk threshold of 1:250 and ultrasound screening to those aged under 30. 8. As 7, but with a 1:100 risk cutoff. Comments: Compares eight screening strategies in the second trimester. Baseline detection rates in strategies 3 and 4 are 52.1 per cent and 43.8 per cent respectively, with a 5 per cent FPR. Results are very sensitive to the assumed detection and false positive rates. Option 6 had the highest number of cases detected but also the highest cost per case detected. The baseline cost per case detected for options 2–8 is 19.75, 4.62, 3.45, 3.06, 4.8, 2.63 and 2.68 million pesetas. Nuchal translucency measurement in the first trimester of pregnancy 91 The results are insensitive to uptake rates. The assumed costs appear to be low and ultrasound is assumed to have zero cost. According to the reviewers’ calculations, the incremental cost-effectiveness ratio (ICER) for strategy 3 compared with strategy 4 is 10.2 million pesetas. Cusick and Vintzileos (1999) Fetal Down syndrome screening: a cost effectiveness analysis of alternative screening programs Country: United States Screening strategy and comparators: Five age stratified screening strategies in the second trimester of pregnancy, as follows: 1. Amniocentesis for women 35 years and older. 2. Triple marker biochemical screening for women aged under 35 followed by amniocentesis for those with positive results. Amniocentesis for women 35 years and older. 3. Triple marker biochemical screening for all women followed by amniocentesis for those with positive results. 4. For women under 35, triple marker biochemical screening followed by genetic sonogram where positive. Amniocentesis where the sonogram is positive. For women 35 years and older, triple marker biochemical screening followed by amniocentesis for those with positive results. 5. Triple marker biochemical screening for all women followed by genetic sonogram where positive and amniocentesis if this is also positive. Comments: Compares five programs. The second program is currently a common screening protocol. In the base case scenario it was assumed that the sensitivity of ultrasound was 70 per cent and the FPR was 13 per cent. The five screening programs were estimated to identify 30.0 per cent, 68.5 per cent, 62.3 per cent, 50.7 per cent and 35.8 per cent of all cases respectively. The screen positive rates (using an outcome of increased risk of trisomy 21 in women with normal pregnancies) were 8.4 per cent, 14.9 per cent, 8.3 per cent, 2.7 per cent and 1.2 per cent for strategies 1 to 5, respectively. The number of normal pregnancies lost due to amniocentesis in the five programs was 56, 100, 55, 17 and 7. The costs per trisomy 21 case detected in the five programs were estimated to be US$181,000, US$203,000, US$162,000, US$151,000 and US$194,000, respectively. The total costs of these screening programs for 167,654 pregnant women (8.4% of whom would be aged over 34 years) were calculated to be US$14.1 million, US$36.1 million, US$26.1 million, US$20.0 million and US$18.0 million. The following costs were used in the analysis: maternal biochemical triple screen - US$80; ultrasound exam - US$200; amniocentesis - US$1,000. Programs 4 and 5, which use sonography, appear to be the most favourable options, with the cost per case detected comparable to that of program 3 but with much lower screen positive rates, fewer losses due to amniocentesis and a considerably lower number of amniocentesis procedures required to identify cases of trisomy 21. The variance in detection rate affected the costeffectiveness of the intervention. For instance at 50 per cent, the cost per case detected for program 4 would be US$178,000, although FPRs and losses due to amniocentesis would remain much lower than in program 3. However, with a sensitivity rate of 90 per cent, program 5 would be the most favourable protocol, with a cost per case detected of US$131,000. 92 Nuchal translucency measurement in the first trimester of pregnancy The authors suggest that it is cost-effective to offer genetic sonogram prior to amniocentesis following a positive biochemical test if the ultrasound detection rate is at least 70 per cent. While biochemical screening alone costs more, it detects more cases of trisomy 21. According to the reviewers’ calculations, the ICER for triple screening over triple screening followed by ultrasound, is US$117,391 per case detected at a 70 per cent detection rate for the screening program incorporating ultrasound. In addition, the fetal loss per case detected is 34 per cent compared with 7 per cent. Wald et al (1997b) Antenatal screening for Down syndrome Country: United Kingdom Screening strategy and comparators: Triple marker biochemical screening comparing first and second trimester and a range of markers. Comments: Estimates the safety and financial cost-effectiveness of screening using different combinations of biochemical markers in screening women with a 1.3 per 1,000 risk of a trisomy 21 birth. The calculation of costs for screening in the first trimester, using maternal age with human chorionic gonadotrophin (hCG) and pregnancy-associated plasma protein-a (PAPP-A), is based on a detection rate of 62 per cent, 5 per cent FPR, fetal loss rate of 0.9 per cent and chorionic villus sampling (CVS) screen cost of £250. This was estimated to be £31,600 per trisomy 21 birth avoided. This is more expensive than any form of second trimester biochemical screening. The cost per trisomy 21 birth avoided for second trimester screening is said to be in the range of £23,000–34,000, based on followup diagnostic amniocentesis costing £150. Additionally, first trimester screening precludes screening for neural tube defects, whereas second trimester screening offers this additional benefit. Nuchal translucency screening in combination with biochemical testing in the first trimester is discussed in the expanded report, but is not judged to warrant economic evaluation. Vintzileos et al (1998) An economic evaluation of second trimester genetic ultrasonography for prenatal detection of Down syndrome Country: United States Screening strategy and comparators: First trimester genetic sonography versus universal CVS in women aged 35 years and over. Comments: Varies the detection and FPRs for first trimester ultrasound screening for women who are 35 years old or more with a prevalence of trisomy 21 of 1:100 to achieve break even cost with universal CVS. Benefits are defined as financial savings associated with a reduction in trisomy 21 births. The lifetime cost of neonates born with trisomy 21 is assumed to be US$500,000. The CVS fetal loss rate is 1:100 and the uptake of ultrasound and CVS is assumed to be the same (53 per cent of pregnancies). CVS has been assumed to be 100 per cent accurate. The results include a FPR of 5 per cent, which requires a sensitivity of at least 72 per cent for the financial benefits of screening to outweigh the costs. This is estimated for all possible FPRs. A review of eight published studies detailing the sensitivity and specificity of genetic sonography in the first trimester revealed that five studies produced diagnostic accuracy compatible with net benefits. Nuchal translucency measurement in the first trimester of pregnancy 93 When first trimester genetic ultrasound followed by CVS for those with abnormal results is compared with universal CVS (applying a sensitivity and false positive rate for genetic sonography of 77 per cent and 10 per cent respectively and a procedure-related fetal loss rate of 1:250), savings of approximately US$22 million and 1,785 fetal lives per year would be expected. It should be noted that this implies that universal CVS in this age group would cost an extra US$80,000 per trisomy 21 birth avoided and lead to an extra 1,785 fetal losses compared with ultrasound screening in the first trimester. Based on data in the paper, for a 77 per cent detection rate and 10 per cent FPR, the reviewers estimate that, ignoring the lifetime cost of care, the cost per case detected for universal CVS is US$240 million/2,000 = US$120,000 and for ultrasound screening, US$80 million/0.7× 2,000 = US$57,000. In addition, universal CVS would lead to an additional 1,785 fetal losses. The ICER for CVS based on these assumptions is US$160 million/600 = US$267,000 per extra case detected with an additional 1,785 fetal losses. Vintzileos et al (2000) Cost-benefit analysis of prenatal diagnosis for Down syndrome using the British or the American approach Country: United States Screening strategy and comparators: First trimester ultrasound screening versus second trimester screening by age and biochemical marker testing. More specifically: 1. First trimester ultrasound screening in all pregnant women followed by CVS for positive screens and second trimester ultrasound for those found to have normal CVS results; compared to 2. Second trimester biochemical screening with amniocentesis for those screening positive and all pregnant women over 35 years of age. Comments: Cost-effectiveness analysis with benefits defined as live births with trisomy 21 avoided. Trisomy 21 births are attributed a cost of lifetime care of US$500,000. Best case and worst case scenarios are presented for ultrasound screening with an 80 per cent detection rate and 5 per cent FPR assumed for the former; and a 50 per cent detection rate and 10 per cent FPR assumed for the latter. Seventy five per cent of women are said to be screened by ultrasound. Sixty six per cent of women under 35 are screened by maternal biochemical screening with an overall detection rate in all ages of 60 per cent applying a risk threshold of 1:150. Ultrasound examination costs US$200 compared with biochemical screening at US$70, counselling sessions are valued at US$100 and CVS or amniocentesis at US$1,200.There is a 70 per cent uptake of invasive diagnostic procedures among screen positive women. In a population of four million pregnancies the best case for ultrasound screening is said to have a cost of US$1,995 million, preventing 1,779 trisomy 21 births while resulting in 1,370 procedure-related fetal losses. The worst case is said to cost US$2,439 million, prevent 1,212 trisomy 21 births and result in 2,420 fetal losses. In contrast, the biochemical and age screening approach is costed at US$1,904 million, with 1,411 trisomy 21 births prevented and 1,680 fetal losses. The introduction of first trimester ultrasound screening for pregnant women in the US is predicted to cost at least US$91 million more per year than the biochemical and age screening strategy, but to reduce by almost one half, the number of invasive procedures and also reduce the number of fetal losses by 310. The results are sensitive to the assumed detection rates, the fetal loss rate and the cost of ultrasound. The results are also likely to be sensitive to the assumed uptake of screening in each strategy, although this is not reported. 94 Nuchal translucency measurement in the first trimester of pregnancy Appendix H Modelled economic evaluation of nuchal translucency ultrasound screening under various alternative assumptions The primary analysis of the cost effectiveness of nuchal translucency (NT) ultrasound screening is based on the assumptions in Tables 30–32. The following eight scenarios provide analyses of the cost effectiveness of NT ultrasound screening under a variety of alternative assumptions. Alternative scenario 1: screening for those at higher risk only (age-related) This assumes that screening is offered only to those women aged 35 years or over. The prevalence of trisomy 21 in this age group is assumed to be 3.2 per 1,000 (Fletcher et al 1995), with an expected 252 cases at 12 weeks and 131 live trisomy 21 births. All other assumptions are as in the primary analysis. The results are shown in Table H-1. In women who are 35 years or older (with twice the incidence of trisomy 21 compared with all women), the incremental cost per extra case detected by NT ultrasound screening compared with biochemical screening alone is $44,117, which is about half the cost per case detected for women of any age. Clearly, targeting a high-risk group reduces the costs per case detected in proportion to the relative risk. The number of cases detected for biochemical screening in the first trimester, NT ultrasound alone and a combination of NT ultrasound and biochemical screening in the first trimester would be 109, 157 and 188 respectively. The number of live trisomy 21 births would be 67, 54 and 44 respectively. Table H-1 Cost per trisomy 21 case detected in women aged 35 years or overa Number of cases detected Total cost ($) Biochemical screening (second trimester) 109 3,330,627 30,625 109 3,330,627 30,625 NT ultrasound screening 157 5,440,522 34,746 48 2,109,895 44,117 NT ultrasound screening + first trimester biochemical testing 188 7,693,263 40,830 32 2,252,740 70,753 Cost per case detected ($) ∆ cases detected ∆ cost ($) ∆ cost per case detected ($) ∆ = incremental; NT = nuchal translucency a Costs are rounded to the nearest whole number Another option is to offer screening to women who are 30 years or older (with a relative risk of 1.63 compared with all women (Fletcher et al 1995)). Table H-2 shows the costeffectiveness of screening if this age cutoff were to be applied. Nuchal translucency measurement in the first trimester of pregnancy 95 Table H-2 Cost per trisomy 21 case detected in women aged 30 years or overa Number of cases detected Total cost ($) Biochemical screening (second trimester) 253 9,480,178 37,531 253 9,480,178 37,531 NT ultrasound screening 364 15,349,567 42,207 111 5,869,389 52,841 NT ultrasound screening + first trimester biochemical testing 438 21,745,350 49,690 74 6,395,783 86,488 Cost per case detected ($) ∆ cases detected ∆ cost ($) ∆ cost per case detected ($) ∆ = incremental; NT = nuchal translucency a Costs are rounded to the nearest whole number With respect to screening of women aged 30 years or older (with two thirds the incidence of trisomy 21 compared to all women), the incremental cost per extra case detected by ultrasound compared with biochemical screening alone is $52,841, which is about two thirds of the cost per case detected for all women. The number of trisomy 21 live births would be 155, 125, and 103 for second trimester biochemical screening, first trimester NT ultrasound screening alone and first trimester biochemical screening plus NT ultrasound, respectively. The comparative results for other strategies in terms of cost per case detected are again in proportion to the relative prevalence of trisomy 21 by maternal age. Victorian and South Australian data suggest that in 1998 and 1999, 41-44 per cent of women over the age of 34 had a diagnostic test, with 80 per cent of these based on an indication of age alone (SABDR 1998; Jane Halliday, Manager, Victorian Perinatal Data Collection Unit, Department of Human Services, Victoria, personal communication). Assuming that a third of women aged 35 years or more currently have an amniocentesis in the second trimester solely on the basis of age-related risk, one would expect to see 56 cases detected at a cost in excess of $9 million. If ultrasound and biochemical screening could achieve a higher rate of uptake, even with a detection rate of only 86 per cent, there would be more cases detected at a lower total cost. As long as uptake is greater than 43 per cent, the combination of ultrasound and biochemical screening with a detection rate of 86 per cent would dominate testing with amniocentesis where it involved 33 per cent of pregnant women aged 35 years or over. It needs to be stated, however, that high rates of diagnostic testing by amniocentesis and CVS have persisted in spite of the existence of biochemical screening. It may be that women at higher risk of an abnormal pregnancy may prefer to have the certainty of amniocentesis or CVS and may not be willing to accept the results of ultrasound and biochemical screening tests. If that is a common view, there might be little substitution in this age group. While the total cost of ultrasound screening would be lower, the costeffectiveness ratios in Table H-1 may be a reasonable approximation of reality. Alternative scenario 2: ultrasound screening + biochemical screening in first trimester compared with serum screening in second trimester Women may well have ultrasound screening and, if negative, have further biochemical testing in the first or second trimester. Tables H-1–3 show the cost-effectiveness of ultrasound screening plus biochemical screening compared with biochemical screening alone. 96 Nuchal translucency measurement in the first trimester of pregnancy The combination of ultrasound and biochemical screening would add $25.0 million to the cost of screening but detect an extra 345 cases. The incremental cost-effectiveness is therefore $72,424 per additional case detected. The number of trisomy 21 live births would be 212 for second trimester biochemical screening and 141 for the combination of first trimester biochemical screening and NT ultrasound. Table H-3 Cost-effectiveness analysis of ultrasound screening plus biochemical screening compared with biochemical screening alone: cost per trisomy 21 case detecteda Number of cases detected Total cost ($) Cost per case detected ($) ∆ cases detected ∆ cost ($) ∆ cost per case detected ($) Biochemical screening (second trimester) 346 21,349,547 61,746 346 21,349,547 61,704 NT utrasound screening + first trimester biochemical screening 599 48,065,939 80,238 253 26,716,392 105,484 ∆ = incremental; NT = nuchal translucency a Costs are rounded to the nearest whole number Table H-4 shows the incremental cost-effectiveness of combined NT ultrasound and biochemical screening in the first trimester compared with biochemical screening alone for three age groups: 30 years and over, 35 years and over, and all ages. As expected, the comparative cost-effectiveness of screening is proportional to the prevalence of trisomy 21 in each age group. However, in each age group the extra costs per trisomy 21 case detected are greater for combined NT ultrasound and biochemical screening than for biochemical screening compared with no screening. While the incremental cost-effectiveness ratio for combined NT ultrasound and biochemical screening may represent good value for money, it is greater than the average cost-effectiveness of second trimester biochemical screening currently subsidised under Medicare, even for those aged 35 and over. Table H-4 Incremental cost-effectiveness of ultrasound and biochemical screening compared with biochemical screening alone by age groupa Age 30 and over Age 35 and over All ages 37,531 30,625 61,704 54,763 105,598 Biochemical screening (second trimester) Incremental cost per extra case detected ($) NT ultrasound screening + first trimester biochemical screening 66,298 Incremental cost per extra case detected ($) NT = nuchal translucency a Incremental costs are rounded to the nearest whole number Alternative scenario 3: 100 per cent uptake of ultrasound screening or ultrasound screening plus biochemical screening in the first trimester, compared to an assumed 50 per cent for biochemical screening in second trimester If one assumes a higher uptake for ultrasound screening than first trimester biochemical screening, the cost-effectiveness of ultrasound screening improves. If one assumes that 50 per cent of all pregnant women were to have biochemical screening (based on current levels and future growth), and that the introduction of NT ultrasound screening increases the rate of screening to 100 per cent, then the incremental cost for NT ultrasound screening compared with biochemical screening is $64,111 per extra case detected (see Table H-5). This is not very different from the primary analysis. Nuchal translucency measurement in the first trimester of pregnancy 97 Both scenarios are hypothetical with the uptake now probably lower than 50 per cent, and unlikely to ever reach 100 per cent with NT. Nevertheless, the calculations illustrate the impact of a large increase in uptake. If the uptake of screening doubles with NT ultrasound screening, so does the cost and the number of cases detected. The incremental cost per extra case detected for NT ultrasound screening compared with biochemical screening is not sensitive to uptake levels although total costs of course increase proportionately. Table H-5 Cost-effectiveness where NT ultrasound screening increases the uptake of screening to 100% compared with 50% for biochemical screeninga Number of cases detected Total cost ($) Cost per case detected ($) ∆ cases detected Diagnosisrelated fetal losses ∆ cost ($) Biochemical screening (second trimester) 173 10,674,773 61,704 173 50 10,674,773 61,704 NT ultrasound screening 534 33,818,889 63,331 361 99 23,144,115 64,111 48,065,939 80,238 65 99 14,247,051 219,051 NT ultrasound screening + first trimester biochemical testing 599 ∆ = incremental; NT = nuchal translucency a Costs are rounded to the nearest whole number ∆ cost per case detected ($) Alternative scenario 4: nuchal translucency ultrasound screening substitutes for dating ultrasound scanning in 80 per cent of pregnancies It may be that NT ultrasound screening would substitute for dating ultrasound scanning in the first trimester. This might result in an increase in the cost of ultrasound but by less than the full $100 for a NT ultrasound screen. On the other hand, a previous early ultrasound scan to determine the exact date of gestation increases the detection rate of biochemical screening and might reduce the difference in detection rates between ultrasound, biochemical screening and the combination of both. Given that a first trimester ultrasound scan has an MBS fee of $60 (item number 55700), it is estimated that the increase in cost would only be $40. Table H-6 reports the results of the scenario where NT ultrasound screening substitutes for another first trimester ultrasound scan in 100 per cent of pregnancies. The effect is to reduce the cost of NT ultrasound screening below that of biochemical screening in the second trimester. Provided that ultrasound screening is at least as effective as biochemical screening in detecting cases, it would dominate biochemical screening on this assumption. If more than one third of women substituted NT ultrasound screening for a dating ultrasound scan in the first trimester, followed by second trimester biochemical screening, the result would be a financial saving. Provided there was no difference in screening uptake and the extra cost of NT ultrasound screening over dating ultrasound did not exceed $40, offering NT ultrasound screening as a substitute for biochemical screening and an early scan that would have occurred between weeks 9 and 11, would most likely be costeffective. 98 Nuchal translucency measurement in the first trimester of pregnancy Table H-6 Cost per trisomy 21 case detected where nuchal translucency ultrasound screening substitutes for first trimester dating ultrasound in 100 per cent of pregnanciesa Number of cases detected Total cost ($) Cost per case detected ($) ∆ cases detected ∆ cost ($) ∆ cost per case detected ($) Biochemical screening (second trimester) 346 21,349,547 60,213 346 21,349,547 61,746 NT ultrasound screening 534 18,202,249 38,479 188 18,202,249 Dominant NT ultrasound screening + first trimester biochemical testing 32,449,299 52,654 65 32,449,299 218,602 599 ∆ = incremental; NT = nuchal translucency a biochemical detection rate is assumed to be a weighted average of 64–74 per cent, where the weights are the percentage of women who have an early scan. The cost of nuchal translucency ultrasound screening is $40 for the percentage who substitute an early scan. Costs are rounded to the nearest whole number However, if a combination of ultrasound and biochemical screening is adopted as common practice, there will not be financial savings at this level of substitution and cost. The incremental cost per extra case detected is $43,825 for a combination of ultrasound and biochemical screening in the first trimester compared with biochemical screening in the second trimester. This is based on an 80 per cent substitution for early ultrasound scanning. However, the incremental cost per case detected by the combination of ultrasound and biochemical screening is considerably lower than the cost per case detected for biochemical screening alone. If the community is willing to pay $61,746 per case detected for the 346 trisomy 21 cases detected, then paying $43,825 for an extra case detected might be regarded as value for money. The cost-effectiveness of NT ultrasound screening is sensitive to the extent of substitution that might take place. Table H-7 shows the incremental cost per case detected at various levels of substitution of NT screening for the dating ultrasound. With 50 per cent substitution of early ultrasound scanning, universal NT ultrasound screening has an incremental cost (cost per extra case detected) of $33,181, which is less than half that of biochemical screening in the second trimester ($69,050). Table H-7 Cost-effectiveness analysis of NT ultrasound screening plus biochemical screening in the first trimester compared with biochemical screening in the second trimester with varying levels of substitution for early ultrasound scanninga Level of substitution for early ultrasound Total cost 100% substitution 43,825.1 11,099,752.4 80% substitution 56,156.9 14,223,080.4 60% substitution 68,488.8 17,346,408.4 40% substitution 80,820.6 20,469,736.4 93,152.4 23,593,064.4 20% substitution No substitution a Incremental cost per extra case detected ($) 105,484 26,716,392.4 The cost for nuchal translucency ultrasound screening is $40 for the percentage that substitute for a dating scan. Incremental costs are rounded to the nearest whole number. Nuchal translucency measurement in the first trimester of pregnancy 99 Alternative scenario 5: varying the screening detection rate In the primary analysis, the sensitivity of biochemical screening, NT ultrasounds and the combination of NT and biochemical screening in first trimester is assumed to be 0.64, 0.77 and 0.86 respectively. As Table 26 shows, there is considerable uncertainty around these values. In order to examine the robustness of the cost effectiveness results to variation in the detection rates for the three screening modalities, a probabilistic sensitivity (Monte Carlo) analysis has been carried out. Rather than take a single point estimate of the detection rates, this analysis assumes a probability distribution for each of the detection rates and samples from that distribution 1000 times in order to produce a distribution of mean incremental cost per case detected. Given that we do not have any strong evidence that any of the values in the literature are more likely than any other, we have assumed a uniform distribution for each of the detection rates in the range outlined in Table 26. The results are shown in Table H-8. The results suggest that the estimates used in the primary analysis, of the cost effectiveness of each strategy, are relatively robust with, for example, a coefficient of variation of 10 for the combination strategy when compared to biochemical screening in the second trimester. The only strategy that has very wide confidence intervals is the combination strategy compared to NT alone. There is a widespread view that if NT and serum screening were both reimbursed, the combination strategy would be the most likely practice to be adopted. In this case the relevant ICER for the combination strategy is $121,554 (95% CI $104,109 $141,664) compared to biochemical screening in the second trimester. Table H-8 Probabilistic sensitivity analysis of the cost-effectiveness of screening options with uniform distribution of detection rates as reported in Table 26 Comparator Screening option Biochemical screening (second trimester) NT ultrasound screening NT ultrasound screening + first trimester biochemical testing No screening Mean ∆ cost per case detected (95% CI) 60,388 (58,384 62,459) Biochemical screening (second trimester) 71,462 (59,643 84,953) NT ultrasound screening alone 345,104 (-1,139,504 1,423,280) NT ultrasound screening + first Biochemical screening trimester biochemical testing (second trimester) NT = nuchal translucency Incremental costs are rounded to the nearest whole number 121,554 (104,109 141,664) Alternative scenario 6: varying the chorionic villus sampling procedure-induced fetal loss rate The primary analysis assumes that the procedure-related rate of loss associated with both CVS and amniocentesis in each trimester is the same at 9 in 1,000. However, there is some suggestion in the literature that CVS has a higher procedure-related loss rate (Alfirevic et al 2000), although the general view is that with experienced operators the rates are similar. The results of assuming a 2.5 per cent procedure-related fetal loss for CVS compared with a one per cent loss for amniocentesis are considered here. This variation makes little difference to the cost per trisomy 21 case detected but results in an almost threefold increase in the number of diagnosis-related fetal losses with NT ultrasound screening. 100 Nuchal translucency measurement in the first trimester of pregnancy Alternative scenario 7: cost of ultrasound screening $80 compared to $100 in primary analysis Table H-9 shows the cost effectiveness of NT screening if a price of $80 is assumed rather than the equivalent second trimester ultrasound cost of $100. Table H-9 Cost effectiveness of NT with cost of $80 for NT ultrasound in first trimester Biochemical screening (second trimester) NT ultrasound screening NT ultrasound screening + first trimester biochemical testing Number of cases detected Total cost ($) Cost per case detected ($) ∆ cases detected ∆ cost ($)a ∆ cost per case detected ($)a 346 21,349,547 61,746 346 21,349,547 61,746 534 28,613,342 53,596 188 7,263,795 38,617 599 42,860,392 71,548 65 14,247,051 218,602 NT = nuchal translucency Incremental costs are rounded to the nearest whole number If the cost of a NT ultrasound is reduced to $80 then the incremental cost per additional case detected for NT when compared to second trimester biochemical screening is $38,617. For a combination of NT and first trimester biochemical screening compared to second trimester biochemical screening, the cost per extra case detected is $84,931. Alternative scenario 8: combinations of assumptions favourable to ultrasound screening The primary cost-effectiveness analysis is reasonably conservative with respect to the costeffectiveness of ultrasound screening. This alternative examines a combination of assumptions favourable to NT screening and reports the incremental cost-effectiveness by age group. The assumptions are as follows: • 48 per cent natural fetal loss from week 12 to term; • 50 per cent screening with biochemical markers and 100 per cent with NT ultrasound; • 80 per cent substitution for early dating ultrasound; • NT ultrasound and biochemical screening used in combination in the first trimester; • detection rate of 64 per cent for biochemical screening; and • a detection rate of 86.4 per cent for the combination of NT ultrasound and biochemical screening in the first trimester. Nuchal translucency measurement in the first trimester of pregnancy 101 The results in Table H-10 demonstrate that under an optimistic set of assumptions, the cost of detecting an extra case of trisomy 21 in pregnancy through the combination of NT ultrasound and biochemical screening in the first trimester is less than that of biochemical screening in the second trimester. The relationship between maternal age, the prevalence of trisomy 21 and the cost-effectiveness of screening remains as in the primary analysis. If screening is limited to those in older age groups, there is a substantial improvement in the cost-effectiveness ratios. Table H-10 Incremental cost-effectiveness of combined nuchal translucency ultrasound plus biochemical screening and biochemical screening alone under optimistic assumptions by age groupa Age 35 and over All ages 43,171 126 35,666 54 69,050 173 29,370 505 24,204 217 47,185 691 Age 30 and over Biochemical screening (second trimester) Incremental cost per extra case detected ($) Number of cases detected NT ultrasound screening plus first trimester biochemical screening Incremental cost per extra case detected ($) Number of cases detected NT = nuchal translucency a Incremental costs are rounded to the nearest whole number 102 Nuchal translucency measurement in the first trimester of pregnancy Appendix I Contact details for Australian centres accredited by the Fetal Medicine Foundation New South Wales Location Bankstown Bankstown-Lidcombe Hospital Ultrasound Department Locked Mail Bag 1600 Bankstown NSW 2200 Phone: 02 9722 8194 Fax: 02 9722 8197 Bankstown Mayne Health Diagnostic Imaging 50 Kitchener Pde Bankstown NSW 2200 Phone: 02 9708 4066 Fax: 02 9708 1114 Baulkham Hills The Hills Ultrasound for Women Hills Hospital 499 Windsor Road Baulkham Hills NSW 2153 Phone: Belmont Hunter Health Imaging Service Belmont Hospital Croudace Bay Rd Belmont NSW 2280 Phone: 02 4923 2219 Fax: 02 4923 2178 Blacktown Kempsey St Specialist Centre 3 Kempsey St Blacktown NSW 2148 Phone: 02 9831 1644 Fax: 02 9672 1319 Bondi Junction Sydney Ultrasound for Women 17th Floor, Westfield Towers 500 Oxford St Bondi Junction NSW 2026 Phone: 02 9388 0955 Fax: 02 9388 0933 Contact Registered Practitioners Mr Lambros Wassef Mr Lambros Wassef Dr Stephen Mackie Dr Stephen Mackie Dr Linda Atkins Dr Linda Atkins Dr Criton Kasby Shona England Shona England Dr Criton Kasby Dr Criton Kasby Dr Andrew McLennan Dr Andrew McLennan Nuchal translucency measurement in the first trimester of pregnancy 103 Burwood Sydney Ultrasound for Women Suite 3, 29 Belmore Street Burwood NSW 2134 Phone: 02 9745 4054 Fax: 02 9744 8854 Burwood Suite 25, Level 4 12 Railway Parade Burwood NSW 2134 Phone: 02 9744 7240 Fax: 02 9744 7260 Campbelltown MacArthur Diagnostic Imaging 14 Warby Street Campbelltown NSW 2560 Phone: 02 4626 1257/ 02 4625 3900 Fax: 02 4628 4975 Camperdown King George V Memorial Hospital Department Ultrasound & Fetal Medicine Missenden Road Camperdown NSW 2050 Phone: 02 9515 6042 Fax: 02 9515 6579 Campsie Mayne Health Diagnostic Imaging Campsie Imaging Centre 308-312 Beamish Street Campsie NSW 2194 Phone: 02 9922 3018 Fax: 02 9955 0039 Chatswood Sydney Ultrasound for Women Level 1, 56 Neridah Street Chatswood NSW 2067 Phone: 02 9413 9196 Fax: 02 9413 3863 Dee Why Pittwater Radiology Dee Why X-Ray 812 Pittwater Road Dee Why NSW 2099 Phone: 02 9982 4911 Fax: 02 9981 4457 104 Dr Andrew McLennan Dr Andrew McLennan Dr Viola Gabriel Dr Viola Gabriel Ms Cathy Nelson Dr Michael Meyerson Dr Michael Meyerson Prof Janet Vaughan Prof Janet Vaughan Dr Robert Ogle Kim Brinsmead Dr Philippa Ramsay Dr Peter Hunter Dr Peter Hunter Dr Andrew McLennan Dr Andrew McLennan Ms M Lucas Dr Alan Farrell Ms Mandy Finlay Mrs Belinda Smith Mrs Leanne Ippolito Dr Alan Farrell Dr Alan Gunn Nuchal translucency measurement in the first trimester of pregnancy Eastwood North West Radiology Ryde Medical Centre 247 Ryedale Road Eastwood NSW 2122 Phone: 02 9858 4266 Fax: 02 9874 7022 Gosford Coast Ultrasound Hills Street Medical Centre Suite 6, 16-18 Hills Street Gosford NSW 2250 Phone: 02 4325 7541 Fax: 02 4324 2770 Hamilton RBR Diagnostic Ultrasound Service 20 Devon St Hamilton NSW 2303 Phone: 02 4997 0673 Hornsby Northside Imaging 53 Palmerston Rd Hornsby NSW 2077 Phone: 02 9476 3388 Fax: 02 9477 7873 Hornsby Hornsby Ku-Ring-Gai Hospital Palmerston Road Hornsby NSW 2077 Kingswood Penrith Ultrasound for Women Suite 7, 1A Barber Avenue Kingswood NSW 2747 Phone: 02 4721 2195 Fax: 02 4732 3922 Kogarah St George's Hospital Women's and Children's Health Level 2, Pritchard Wing, Gray St Kogarah NSW 2217 Phone: 02 9350 3635 Fax: 02 9350 3901 Lambton Women's Health and Ultrasound Suite 2, 25 Morehead Street Lambton NSW 2299 Phone: 02 4957 3899 Fax: 02 4957 4083 Dr Sonja Borsky Dr Sonja Borsky Dr Malcolm Catt Dr Robert B Richardson Dr Robert B Richardson Ms Linda Walford-Smith Ms Linda Walford-Smith Ms Jodi Trace Ms Beverley Barraclough Ms Beverley Barraclough Dr Linda Atkins Dr Linda Atkins Mr David Fauchon Mr Brendan Mein Ms Narelle Kennedy Dr Lucy Bowyer Dr Lucy Bowyer Dr Steve Raymond Dr Steve Raymond Dr Stephen O’Callaghan Ms Susan Cowie Ms Veronica McDougall Nuchal translucency measurement in the first trimester of pregnancy 105 Lismore North Coast Radiology 17 Orion Street Lismore NSW 2480 Phone: 02 6621 2085 Fax: 02 6622 4780 Liverpool Feto-Maternal Unit Liverpool Hospital Department of Obstetrics Feto-Maternal Unit Caroline Chisholm Building Liverpool NSW 2170 Phone: 02 9828 4145 Fax: 02 9828 5672 Liverpool Sydney Ultrasound for Women Suite 205, 161 Bigge Street Liverpool NSW 2170 Phone: 02 9822 8447 Fax: 02 9822 7761 Maitland Maitland Hospital X-Ray Department 550-560 High St Maitland NSW 2320 Phone: 02 4939 2000 Mona Vale Pittwater Radiology 6/60 Barrenjoey Rd Mona Vale NSW 2103 Phone: 02 9997 4504 / 02 9982 4911 Fax: 02 9981 4457 New Lambton Hunter Imaging Group PO Box 192 New Lambton NSW 2305 Phone: 02 4952 8457 Fax: 02 4956 2884 Newcastle John Hunter Hospital Hunter Regional Mail Centre Locked Bag 1 Newcastle NSW 2310 Phone: 02 4921 4385 Fax: 02 4921 4394 106 Mr Peter Murphy Mr Peter Murphy Dr John Smoleniec Dr John Smoleniec Ms Ann Quinton Mr Robert Ogle Dr Andrew McLennan Dr Andrew McLennan Ms Kristine Louise Morris Ms Kristine Louise Morris Dr Amanda Woodward Dr Amanda Woodward Professor Warwick B Giles & Dr Stephen O'Callaghan Professor Warwick B Giles Dr Stephen O'Callaghan Dr Steve Raymond Dr Stephen Cole Nuchal translucency measurement in the first trimester of pregnancy Newtown Sydney Ultrasound for Women RPAH Medical Centre 404/100 Carillon Avenue Newtown NSW 2042 Phone: 02 9516 2064 Fax: 02 9550 6257 Newtown Specialised Ultrasound for Women 412/100 Carillon Avenue Newtown NSW 2042 Phone: 02 9519 0999 Fax: 02 9519 0606 North Sydney Mater Imaging Mater Hospital Rocklands Road North Sydney NSW 2060 Phone: 02 9955 4466 Fax: 02 9955 7523 Orange Orange Base Hospital Sale Street Orange NSW 2800 Phone: 02 6362 1411 Pennant Hills Pennant Hills Diagnostic Centre 12 Fisher Ave, Pennant Hills NSW 2120 Phone: 02 9875 2911 Fax: 02 9484 1089 Penrith Nepean Hospital Perinatal Ultrasound P.O Box 63, Somerset Road Penrith NSW 2751 Phone: 02 4724 2578 Fax: 02 4724 3206 Randwick Royal Hospital for Women Department for Medical Imaging PO Box 788 Randwick NSW 2031 Phone: 02 9382 6800 Fax: 02 9382 6806 Dr Andrew McLennan Dr Andrew McLennan Dr Philippa Ramsay Dr Philippa Ramsay Dr Linda Atkins Ms Sally Quinn & Peter Stevenson Mr Peter Stevenson Ms Stephanie Martin Ms Jackie Spurway Ms Jackie Spurway Mr Paul O'Keefe Dr Louis Shulman Ms Anita Giga Professor Ron Benzie Professor Ron Benzie Mr Brendan Mein Ms Frances Miceli Ms Alison Webb Dr Henry Murray Mr David Fauchon Dr Glen McNally Dr Peter Warren Dr Glen McNally Dr Peter Warren Nuchal translucency measurement in the first trimester of pregnancy 107 Randwick Hay Street Centre 2 Hay St Randwick NSW 2031 Phone: 02 9326 4001 Fax: 02 9326 4111 Randwick Sydney Ultrasound for Women Randwick Specialist Medical Centre 135 Belmore Street Randwick NSW 2031 Phone: 02 9399 9255 Fax: 02 9399 9153 St Leonards Department of Maternal Fetal Medicine Royal North Shore Hospital St Leonards NSW 2065 Phone: 02 9926 7099 Fax: 02 9906 6742 St Leonards North Shore Obstetric & Gynaecologic Ultrasound North Shore Private Hospital Suite 8, Level 3 Westbourne Street St Leonards NSW 2065 Phone: 02 9487 9800 Fax: 02 9487 9803 Sydney Sydney Ultrasound for Women 4 O'Connell Street Sydney NSW 2000 Phone: 02 9221 8099 Fax: 02 9235 3968 Wagga Wagga PO Box 5215 Wagga Wagga NSW 2650 Phone: 02 6925 8844 Fax: 02 6925 8866 Wahroonga SAN Ultrasound for Women Sydney Adventist Hospital 185 Fox Valley Road Wahroonga NSW 2076 Phone: 02 9487 9800 Fax: 02 9487 9803 108 Dr Wendy Cox Dr Andrew McLennan Dr Andrew McLennan Mr Jonathan Morris Mr Jonathan Morris Dr Andrew McLennan Ms Suzanne Connard Ms Beverley Barraclough Ms Beverley Barraclough Dr Andrew McLennan Dr Andrew McLennan Dr George Angus Dr George Angus Dr Philippa Ramsay Dr Philippa Ramsay Ms Jo Lennox Nuchal translucency measurement in the first trimester of pregnancy Westmead Suite 1 1A Ashley Lane Westmead NSW 2145 Westmead University of Sydney & Westmead Hospital Department of Obstetrics and Gynaecology Westmead Hospital Hawkesbury Road Westmead NSW 2145 Phone: 02 9845 6800 Fax: 02 9845 7793 Westmead Nuclear Medicine and Ultrasound Associates Suite 35, 1A Ashley Lane Westmead NSW 2145 Phone: 02 9831 3055 Windsor Sydney Pregnancy & Women’s Ultrasound Services 10/251 George Street PO Box 291 Windsor NSW 2756 Phone: 02 4587 8575 Fax: 02 4577 6834 Wollongong South Coast Ultrasound 363 - 367 Crown St Wollongong NSW 2500 Phone: 02 4228 9711 Fax: 02 4228 9118 Stephanie The Stephanie The Professor Brian Trudinger Professor Brian Trudinger Ms Lyn Ryder Ms Cherie Drinkwalter Ms Cherie Drinkwalter Ms Nicole Short Ms Lisa Kench Dr Henry Murray Dr Henry Murray Dr Michael Peek Prof Ron Benzie Ms Narelle Kennedy Mr David Fauchon Dr Warren Davis Ms Anne Oliver Dr Warren Davis Ms Anne Oliver Dr Patricia McPherson Nuchal translucency measurement in the first trimester of pregnancy 109 Victoria Ballarat Ballarat Health Services Drummond Street North PO Box 577 Ballarat VIC 3353 Phone: 03 5320 4000 Fax: 03 5320 4828 Ballarat St John of God Health Care Department of Nuclear Medicine & Ultrasound PO Box 20 Ballarat VIC 3353 Phone: 03 5320 2121 Fax: 03 5320 2194 Ballarat Radsonic Diagnostic 801 Mair Street Ballarat VIC 3350 Phone: Ballarat West Lake Imaging PO Box 42W Ballarat West VIC 3350 Phone: 03 5331 4899 Fax: 03 5333 2083 Berwick Women's Imaging Centre Suite 2, 1/8 Langmore Lane Berwick VIC 3806 Phone: 03 9769 9499 Fax: 03 9769 9599 Boronia Radclin Medical Imaging 154 Boronia Road Boronia VIC 3155 Phone: 03 9762 1822 Fax: 03 9762 8102 Carlton Royal Womens Hospital Ultrasound Department 132 Grattan Street Carlton VIC 3052 Phone: 03 9344 2147 110 Dr Jim Mullany Mr Greg Murray Dr Jim Mullany Mr Greg Murray Dr Gary Gill Dr Gary Gill Dr Peter Graham Dr Jim Mullany Dr Jim Mullany Mr Greg Murray Dr Jim Mullany Mr Greg Murray Dr Jacqui Oldham Dr Jacqui Oldham Dr Debbie Nisbet Dr Paul Shekleton Dr Andrew Ngu Mrs Julie Koska Mrs Julie Koska Ms Yvonne Gray Dr Amanda Sampson Dr Amanda Sampson Nuchal translucency measurement in the first trimester of pregnancy Carlton Melbourne Ultrasound for Women Level 1, 62 Lygon Street Carlton VIC 3053 Phone: 03 9663 3999 Fax: 03 9663 3555 Carlton Women’s & Children’s Ultrasound Centre 96 Grattan Street Carlton VIC 3053 Phone: 03 9347 6030 Fax: 03 9347 7645 Clayton Dr James Grimwade Pty Limited 14 -16 Dixon Street Clayton VIC 3168 Phone: 03 9562 8423 Fax: 03 9562 7079 Clayton Monash Medical Centre 246 Clayton Rd Clayton VIC 3168 Phone: 03 9594 5303 Fax: 03 9594 6389 Dandenong North 53 Brady Road Dandenong North VIC 3175 Phone: 03 9790 0333 Fax: 03 9701 1422 Darling South PO Box 13 Darling South VIC 3145 Phone: Doncaster East COGUS 12 Happy Valley Court Doncaster East VIC 3109 Phone: 03 9840 7199 Fax: 03 9841 0910 Dr Lachlan de Crespigny Dr Lachlan de Crespigny Dr Victor Hurley Dr Nicole Woodrow Dr Michael Bethune Ms Ann Kennett Ms Maria Maxfield Ms Dorothy McGinnes Ms Braidy Davies Ms Nafissa Akhounova Dr F Rex Betheras Dr Charles Siles Dr F Rex Betheras Dr Charles Siles Dr James Grimwade Dr James Grimwade Dr E M Wallace Dr Sheila Mulvey Dr Sheila Mulvey Dr Paul Shekleton Dr Jacqui Oldham Dr James Grimwade Dr Graeme Atchison Dr Nicole Woodrow Dr Peter Lee Dr Peter Lee Helen Denise Phillips Helen Denise Phillips Dr Steven L S Chow Dr Steven L S Chow Nuchal translucency measurement in the first trimester of pregnancy 111 East Melbourne Women's Imaging Centre Freemasons Suite 6, 320 Victoria Parade East Melbourne VIC 3002 Phone: 03 9417 6788 Fax: 03 9416 1084 East Melbourne Mercy Hospital for Women Medical imaging Department Clarendon Street East Melbourne VIC 3002 Phone: 03 9827 4065 Fax: 03 6419 0656 Epping Mayne Health Diagnostic Imaging 185 Cooper Street Epping VIC 3076 Phone: 03 9888 5400 Fax: 03 9836 4498 Fitzroy Central Melbourne Medical Imaging 55 Victoria Parade Fitzroy VIC 3065 Phone: 03 9473 1000 Fax: 03 9473 1005 Footscray MIA Victoria, Taft Diagnostic Imaging Western Private Hospital Cnr Eleanor and Marion Streets Footscray VIC 3011 Phone: 03 9317 8777 Fax: 03 9317 0106 Geelong Barwon Medical Imaging Geelong Hospital Ryrie Street PO Box 281 Geelong VIC 3226 Phone: 03 5226 7758 Fax: 03 5246 5149 112 Dr Amanda Sampson Dr Amanda Sampson Dr Andrew Ngu Dr Hugh Robinson Dr Jacqui Oldham Dr Debbie Nisbet Dr Christine Acton Dr Christine Acton Ms Braidy Davies Ms Nafissa Akhounova Ms Gabrielle Fedai Dr Simon Meagher Ms Clare Lee Dr C M Blecher Dr C M Blecher Ms Anna Kennett Marc Hull Marc Hull Mrs Helen Magee Mrs Helen Magee Dr Charles Siles Mr John Bell Ms Yvonne Gray Ms Margaret Condon Mr Marc Hull Ms Sandra Buckley Ms Sandra Buckley Ms Sharon Stafford Dr Kay Wilson Nuchal translucency measurement in the first trimester of pregnancy Geelong Geelong Radiological Clinic Obstetric Service St John of God Health Care PO Box 1087 Geelong VIC 3220 Phone: 03 5221 3300 Fax: 03 5222 5781 Hoppers Crossing MIA Victoria Taft Diagnostic Imaging 267 Heaths Road Hoppers Crossing VIC 3029 Malvern Womens Ultrasound Malvern Suite 2, 147 Wattletree Road Malvern VIC 3144 Phone: 03 9509 8811 Fax: 03 9509 8711 Melton Melton X-Ray Centre 390-392 High Street Melton VIC 3337 Phone: 03 9743 5633 Fax: 03 9743 3650 Mildura 4 Healthscope Court Private Bag 876 Mildura VIC 3500 Phone: 03 5021 4404 Fax: 03 5021 4405 Morwell Gippsland Diagnostic Services 4 Hoyle St Morwell VIC 3840 Phone: 03 5133 9933 Fax: 03 5133 9971 Mulgrave Obstetric and Gynaecological Ultrasound 441 Police Road Mulgrave VIC 3170 Phone: 03 9790 1766 Fax: 03 9790 1100 Mr Russell Artis Mr Russell Artis Ms Julie Dew Ms Michelle Appleford Dr Kay Wilson Ms Doxia Bryce Ms Doxia Bryce Ms Lyn Lavan Ms Margaret Condon Ms Yvonne Gray Mrs Helen Magee Dr Amanda Sampson Dr Amanda Sampson Dr Jacqui Oldham Dr Paul Shekleton Dr Debbie Nisbet Dr Jim Mullany Robyn Marshman Dr Jim Mullany Dr J.D.P Bowditch Dr J.D.P Bowditch Dr R Brownlee Dr R Brownlee Dr Simon Meagher Dr Simon Meagher Dr Shawn Choong Nuchal translucency measurement in the first trimester of pregnancy 113 Noble Park Mayne Health Diagnostic Imaging South Eastern Private Hospital 313 Princes Highway Noble Park VIC 3175 Phone: 03 9562 3433 Fax: 03 9558 5731 Richmond Monash Ultrasound for Women Epworth Hospital Level 4, 89 Bridge Road Richmond VIC 3121 Phone: 03 9427 7610 Fax: 03 9427 9232 Werribee MIA Victoria Taft Diagnostic Imaging Werribee Mercy Hospital 300 Princess Highway Werribee VIC 3030 Phone: 03 9748 3200 Fax: 03 9748 0249 Ms Vicki Truelove Ms Vicki Truelove Dr Simon Meagher Dr Simon Meagher Ms Doxia Bryce Ms Doxia Bryce Mrs Helen Magee Dr Charles Siles Mr John Bell Ms Margaret Condon Ms Lyn Lavan Ms Yvonne Gray Queensland Auchenflower The Wesley Fetal Medicine Unit Wesley Medical Centre Suite 15, Chasely Street Auchenflower QLD 4066 Phone: 07 3371 4933 Fax: 07 3870 3936 Brisbane Brisbane Ultrasound for Women Ballow Chambers 121 Wickham Tce Brisbane QLD 4000 Phone: 07 3831 1777 Fax: 07 3831 1788 Brisbane Watkins Medical Centre 225 Wickham Terrace Brisbane QLD 4000 Phone: 07 3831 0658 Fax: 07 3831 3711 114 Dr Francis Carmody Dr Gary Pritchard Dr Gary Pritchard Ms Helen Gofton Mr Neil Pennell Ms Sue Williams Ms Margo Harkness Ms Paula Sivyer Dr F M McMahon Dr F M McMahon Nuchal translucency measurement in the first trimester of pregnancy Buderim Mayne Health Diagnostic Imaging - QLD 9 Vista Park Drive Buderim QLD 4556 Phone: 07 5444 5877 Fax: 07 5444 7098 Burleigh Waters Gold Coast Medical Imaging Treetops Specialist Medical Cntr Classic Way Burleigh Waters QLD 4220 Phone: 07 5593 6955 Fax: 07 5593 6059 Castletown Queensland X-Ray Mater Hospital PO Box 674 Castletown Townsville QLD 4812 Phone: 07 4759 2800 Fax: 07 4779 7402 Herston Royal Womens Hospital Brisbane Butterfield Street Herston QLD 4029 Phone: 07 3636 7849 Fax: 07 3255 0880 Ipswich Clarke & Robertson Radiology 2 Pring Street Ipswich QLD 4305 Phone: 07 3281 1099 Fax: 07 3812 3154 Mermaid Beach South Coast Radiology 5 Markeri St Mermaid Beech QLD 4218 Phone: 07 556 90 416 Mobile: 041 9313 529 Noosaville Mayne Health Diagnostic Imaging Noosa Hospital 111 Goodchap St Noosaville QLD 4566 Phone: 07 5455 9393 Fax: 07 5449 1131 Mr Ian Stewart Mr Ian Stewart Mrs Anna Galea Mrs Anna Galea Ms Susan Boyd Ms Susan Boyd Dr Stephen Sinnott Dr Stephen Sinnott Dr Carol Portmann Dr Geoff Stieler Dr Geoff Stieler Mr Reginald Viney Mr Reginald Viney Ms Jessica Nilsen Ms Jessica Nilsen Nuchal translucency measurement in the first trimester of pregnancy 115 South Brisbane Mater Mother's Hospital Centre for Maternal Fetal Medicine Raymond Terrace South Brisbane QLD 4101 Phone: 07 3840 8844 Fax: 07 3840 1949 South Brisbane Queensland X-Ray The Women's Diagnostic Centre Mater Private Clinic 550 Stanley St South Brisbane QLD 4101 Phone: 07 3840 6208 Fax: 07 3844 4277 Southport Gold Coast Medical Imaging 123 Nerang St Southport QLD 4215 Phone: 07 5591 5422 Fax: 07 5506 7835 / 7855 Spring Hill Diagnostic Imaging for Women Ground floor 75, Astor Terrace (corner Cousins St) Spring Hill QLD 4000 Phone: 07 3839 8666 Fax: 07 3839 8333 Sunnybank Queensland X-Ray The Women's Diagnostic Centre Suite 15, McCullough Centre 259 McCullough St Sunnybank QLD 4109 Phone: 07 3345 2033 Fax: 07 3345 2635 Toowoomba St Vincent's Medical Centre Scott Street Toowoomba QLD 4350 Phone: 07 4688 5470 Fax: 07 4688 5469 Tweed Heads Tweed Heads District Hospital Medical Imaging Department Florence Street Tweed Heads QLD 2485 Phone: 07 5536 0419 Fax: 07 5506 7835 116 Prof Fung Yee Chan Prof Fung Yee Chan Ms Donna Amaraddio Dr Lisa Begg Dr Robert Cincotta Ms Alison Lee-Tannock Dr Kerry McMahon Dr Kerry McMahon Dr Bronwyn Rogers Dr Matthew Lee Mrs Anna Galea Mrs Anna Galea Ms Karen Doust Ms Karen Doust Ms Paula Sivyer Dr Bronwyn Rogers Dr Bronwyn Rogers Dr Kerry McMahon Dr Anthony Cerqui Dr Anthony Cerqui Dr Matthew Lee Mrs Anna Galea Mrs Anna Galea Nuchal translucency measurement in the first trimester of pregnancy Warwick Warwick Hospital X-ray Department PO Box 1155 Warwick QLD 4370 Phone: 07 4661 6892 Mr Mark Yuile Mr Mark Yuile Dr Karen Shand Dr Karen Shand Ms Maureen Pachulicz Dr Christina Hayward Dr Kevin Williams Dr Kevin Williams Mrs Kerry Thoirs Ms Maureen Pachulicz Ms Maureen Pachulicz Dr Meegan Gun Ms Maria Mavrogiorgis South Australia Ashford Ultrasound Specialists for Women Ashford Specialist Centre Suite 29, 57-59 Anzac Highway Ashford SA 5035 Phone: 08 8293 8880 Fax: 08 8293 8591 Modbury Benson Radiology Modbury Hospital Smart Road Modbury SA 5092 Phone: 08 8265 5100 Fax: 08 8265 5151 North Adelaide Women's & Children's Hospital Perinatal Imaging 72 King William Road North Adelaide SA 5006 Phone: 08 8204 7750 Fax: 08 8204 7749 Woodville South The Queen Elizabeth Hospital Ultrasound Dept 28 Woodville Rd Woodville South SA 5011 Phone: 08 8222 6894 Fax: 08 8222 6040 Western Australia Balcatta Perth Radiological Clinic Joondalup Radiology 217 Wannerou Rd Balcatta WA 6021 Phone: 08 9300 2855 Fax: 08 9345 0367 Dr Susan Lamp Dr Susan Lamp Nuchal translucency measurement in the first trimester of pregnancy 117 Bunbury Imaging the South South West Health Campus Bunbury WA 6230 Phone: 08 97266999 Fax: 08 97266900 Joondalup Mayne Health Diagnostic Imaging Joondalup Health Campus PO Box 242 Joondalup WA 6919 Phone: 08 9400 9030 Fax: 08 9400 9033 Joondalup Joondalup Medical Campus Perth WA 6027 Kalgoorlie Kalgoorlie Regional Hospital PMB 7 Kalgoorlie WA 6430 Phone: 08 90 805 644 Fax: 08 90 805 777 Kalgoorlie X Ray West PO Box 513 Kalgoorlie WA 6430 Phone: 08 9021 5044 Fax: 08 9091 1571 Karratha Pilbara Radiology PO Box 1399 Karratha WA 6714 Phone: 08 91 44 19 22 Fax: 08 91 44 26 90 Mandurah Imaging The South 5 Randell St Mandurah WA 6210 Phone: 08 95 35 54 44 Fax: 008 95 35 70 69 Murdoch St John of God Medical Clinic Suite 15/16 100 Murdoch Drive Murdoch WA 6150 Phone: 08 9366 1771 Fax: 08 9366 1766 118 Sarah Court Sarah Court Ms Michelle Pedretti Ms Michelle Pedretti Mr Paul Stefanetti Dr Bev Hewitt Dr Bev Hewitt Kerry Harvey Kerry Harvey Ms Kerry Harvey Ms Kerry Harvey Dr Leila Dekker Dr Leila Dekker Ms Eleanor Snell Ms Eleanor Snell Mr Paul Stefanetti Ms Sarah Court Dr Peter J Hugo Dr Peter J Hugo Ms Karen Lines Ms Rae roberts Ms Sarah court Dr Anthony Murphy Nuchal translucency measurement in the first trimester of pregnancy Quinns Rocks Quinns Medical Imaging PO Box 97 Quinns Rocks WA 6030 Phone: 08 9305 8606 Fax: 08 9305 8609 Subiaco Perth Ultrasound 442 Barker Road Subiaco WA 6008 Phone: 08 9382 1500 Fax: 08 9382 1927 Subiaco Ob/Gyn Ultrasound St John of God Health Care Suite 309, 25 McCourt Street PO Box 1144 Subiaco WA 6008 Phone: 08 9388 1340 Fax: 08 9388 1351 Subiaco King Edward Memorial Hospital for Women Ultrasound Department 374 Bagot Road Subiaco WA 6008 Phone: 08 9340 2710 Fax: 08 9340 2747 Wembley Obstetric and Gynecological Ultrasound - Wembley 166 Cambridge Street Wembley WA 6014 Phone: 08 9380 4744 Fax: 08 9388 8331 West Perth Park Ultrasound 11 Ventnor Avenue Suite 7 West Perth WA 6005 Phone: 08 9481 4008 Fax: 08 9481 4080 West Perth SKG Radiology 30 Ord Street West Perth WA 6005 Phone: 08 9322 4966 Dr Walter Harmer Mr Paul Stefanetti Dr John Phillips Dr John Phillips Ms Karen Lines Ms Dawn Voges Dr Anthony Murphy Dr Anthony Murphy Dr Jan Dickinson Dr Jan Dickinson Dr Peter Hugo Dr John Newnham Ms Dawn Voges Ms Rae Roberts Dr John Phillips Mr Nevile Phillips Mr Nevile Phillips Dr Bev Hewitt Dr Bev Hewitt Mrs Gillian Kaye Ms Kym Webb Dr Sue Ulreich Dr Sue Ulreich Ms Samantha Ward Ms Tricia Duggin Nuchal translucency measurement in the first trimester of pregnancy 119 Tasmania Hobart Royal Hobart Hospital 48 Liverpool St Hobart TAS 7000 Phone: 03 6231 4457 Fax: 03 6231 4457 Launceston Launceston Ultrasound for Women Suite 7, 7 High St Launceston TAS 7250 Phone: 03 6331 3999 Fax: 03 6331 3666 Dr Peter Davies Dr Peter Davies Dr Susan James Dr Susan James Ms Maree Eastley Australian Capital Territory Bruce Canberra Imaging Group Dr Wes Cormick Dr Wes Cormick Calvary Clinic Mary Potter Court Bruce ACT 2617 Deakin Canberra Imaging Group Dr Wes Cormick Dr Wes Cormick John James Hospital Strickland Cres Deakin ACT 2600 Phone: 02 6285 1173 Fax: 02 6282 4252 Garran The Canberra Hospital Professor David Ellwood Professor David Ellwood Fetal Medicine Unit Ms Jan Curren Ms Jan Curren Garran ACT 2605 Phone: 02 6244 3079 Fax: 02 6244 3154 Woden National Capital Diagnostic Ms Pam Cooke Ms Pam Cooke Imaging Corinna Chambers, PO Box 303 Woden ACT 2696 Phone: 02 6282 2888 Fax: 02 6281 4261 Source: Ann Robertson, Special Projects Officer, RANZCOG, personal communication, August 2002. 120 Nuchal translucency measurement in the first trimester of pregnancy Abbreviations AFP AIUM ALARA ASUM CA-125 CI CMFM COGU CRL CVS DR DS EFSUMB FaST FaSTER FDA FMF FN FP FPR hCG HGSA ICER ISUOG IUGR LR MBS MI MoM MSAC NCCHTA NHMRC NHS NICHHD NIH NPV NT NTS alpha-fetoprotein American Institute of Ultrasound in Medicine as low as reasonably achievable Australasian Society for Ultrasound in Medicine cancer antigen 125 confidence interval Certification in Maternal-Fetal Medicine Certification in Obstetric and Gynaecological Ultrasound crown-to-rump length chorionic villus sampling detection rate; syn. sensitivity Down syndrome European Federation of Societies for Ultrasound in Medicine and Biology First and Second Trimester Screening Study First and Second Trimester Evaluation of Risk trial Food and Drug Administration (United States) Fetal Medicine Foundation false negative false positive false positive rate human chorionic gonadotrophin Human Genetics Society of Australasia incremental cost-effectiveness ratio International Society for Ultrasound in Obstetrics and Gynaecology intrauterine growth retardation likelihood ratio Medicare Benefits Schedule mechanical index multiple of the median Medical Services Advisory Committee National Coordinating Centre for Health Technology Assessment (United Kingdom) National Health and Medical Research Council National Health Service (United Kingdom) National Institute of Child Health and Human Development (United States) National Institutes of Health (United States) negative predictive value nuchal translucency nuchal translucency screening Nuchal translucency measurement in the first trimester of pregnancy 121 ODS OMFL OR PAPP-A PPV RADIUS RANZCOG RCOG RCT RD Sen SP1 Spe sROC SURUSS T1MBS T2MBS TI TN TP uE3 USPSTF WFUMB 122 output display standard oromandibulofacial limb hypogenesis odds ratio pregnancy-associated plasma protein-a positive predictive value Routine Antenatal Diagnostic Imaging with Ultrasound Study Royal Australian and New Zealand College of Obstetricians and Gynaecologists Royal College of Obstetrics and Gynaecology randomised controlled trial risk difference Sensitivity; syn. detection rate schwangerschaftsprotein 1 specificity summary receiver operator characteristic Serum, Urine and Ultrasound Screening Study First trimester maternal biochemical screening Second trimester maternal biochemical screening thermal index true negative true positive unconjugated oestriol US Preventive Services Task Force World Federation of Ultrasound in Medicine and Biology Nuchal translucency measurement in the first trimester of pregnancy References AIUM, 2000, Official statements and reports [Online]. American Institute of Ultrasound in Medicine, Available from: http://www.aium.org/stmts.htm [Accessed 22 September 2000]. Alfirevic, Z., Gosden, C., and Neilson J. ‘Chorion villus sampling versus amniocentesis for prenatal diagnosis’. In: The Cochrane Library, Issue 2, 2000 Update Software, Oxford. Anonymous, 1984. ‘The use of diagnostic ultrasound imaging during pregnancy’ [consensus statement]. Journal of the American Medical Association 252. 669-672. Anonymous, 1998a. ‘Clinical safety statement’. European Federation of Societies for Ultrasound in Medicine and Biology Newsletter. 11. Anonymous, 1998b. ‘Conclusions and recommendations on thermal and non-thermal mechanisms for biological effects of ultrasound’. European Federation of Societies for Ultrasound in Medicine and Biology Newsletter. Vol 12 (1). Anonymous, 2000. FaST (First and second trimester) Study 2000. [Internet] Available from: www.med.monash.edu.au/ob-gyn/Fast.html> [Accessed 20 September 2000]. ASUM, 1998. ‘Safety statements’. In: Australian Society for Ultrasound in Medicine, Willoughby, New South Wales. American Institute of Ultrasound in Medicine. Australian Bureau of Statistics, 2000. Population by age and sex. Canberra: 2000: 28–30. Baird, P.A. and Sadovnick, A.D.. 1987. ‘Life expectancy in Down syndrome’. Journal of Pediatrics 110: 849–854. Baird, P.A. and Sadovnick A.D. 1989. ‘Life tables for Down syndrome’. Human Genetics 82: 291–292. Barnett, S.B., Ter Haar, G.R., Ziskin, M.C., Rott, H.D., Duck, F.A. and Maeda, K. 2000. ‘International recommendations and guidelines for the safe use of diagnostic ultrasound in medicine’. Ultrasound in Medicine and Biology 26: 355–366. Bartels, I. and Lindemann, A. 1988. ‘Maternal levels of pregnancy-specific beta-1glycoprotein (SP-1) are elevated in pregnancies affected by Down syndrome’. Human Genetics 80: 46-48. Benacerraf, B.R. 1998. Ultrasound of Fetal Syndromes. Churchill Livingstone, Philadelphia. Benacerraf, B.R., Barss, V.A. and Laboda, L.A. 1985. ‘A sonographic sign for the detection in the second trimester of the fetus with Down syndrome’. American Journal of Obstetrics and Gynecology 151: 1078–1079. Bernardino, F., Cardoso, R., Montenegro, N., Bernardes, J. and de Sa, J.M. 1998. ‘Semiautomated ultrasonographic measurement of fetal nuchal translucency using a computer software tool’. Ultrasound in Medicine and Biology 24: 51–54. Bevis, D. 1952. ‘The antenatal prediction of haemolytic disease of the newborn’. Lancet 1: 295–298. Nuchal translucency measurement in the first trimester of pregnancy 123 Bewley, S., Roberts, L.J., Mackinson, A.M. and Rodeck, C.H. 1995. ‘First trimester fetal nuchal translucency: problems with screening the general population’. 2. British Journal of Obstetrics and Gynaecology 102: 386–388. Biagiotti, R., Periti, E., Brizzi, L., Vanzi, E. and Cariati, E. 1997. ‘Comparison between two methods of standardization for gestational age differences in fetal nuchal translucency measurement in first-trimester screening for trisomy 21’. Ultrasound in Obstetrics and Gynecology 9: 248–252. Blakemore, K.J. 1998. ‘Nuchal translucency’. Ultrasound in Obstetrics and Gynecology 11: 388– 390. Bogart, M.H., Pandian, M.R. and Jones, O.W. 1987. ‘Abnormal maternal serum chorionic gonadotrophin levels in pregnancies with fetal chromosome abnormalities’. Prenatal Diagnosis 7: 623-630. Booth, T. 1985. ‘Labels and their consequences’. In: Lane, D. and Stratford, B. (eds)., Current Approaches to Down’s Syndrome, Rinehart and Winston, London. Borrell, A., Costa, D., Martinez, J.M., Delgado, R.D., Casals, E., Ojuel, J. and Fortuny, A. 1996. ‘Early midtrimester fetal nuchal thickness: effectiveness as a marker of Down syndrome’. American Journal of Obstetrics and Gynecology 175: 45–49. Borrell, A., Costa, D., Martinez, J.M., Delgado, R.D., Farguell, T. and Fortuny, A. 1997. ‘Criteria for fetal nuchal thickness cut-off: a re-evaluation’. Prenatal Diagnosis 17: 23–29. Borrell, A., Costa, D., Martinez, J.M., Farre, M.T., Cararach, J. and Fortuny, A. 1998. ‘Natural evolution of nuchal thickness in trisomy-21 fetuses’. Obstetrics and Gynecology 91: 78–81. Braithwaite, J.M. and Economides, D.L. 1995. ‘The measurement of nuchal translucency with transabdominal and transvaginal sonography – success rates, repeatability and levels of agreement’. British Journal of Radiology 68: 720–723. Braithwaite, J.M., Kadir, R.A., Pepera, T.A., Morris, R.W., Thompson, P.J. and Economides, D.L. 1996. ‘Nuchal translucency measurement: training of potential examiners’. Ultrasound in Obstetrics and Gynecology 8: 192–195. Braithwaite, J.M., Morris, R.W. and Economides, D.L. 1996. ‘Nuchal translucency measurements: frequency distribution and changes with gestation in a general population’. British Journal of Obstetrics and Gynaecology 103: 1201–1204. Brambati, B. 1992. ‘Genetic diagnosis through chorionic villus sampling’. In: Milunsky, A. (ed)., Genetic Disorders and the Fetus: Diagnosis, Prevention, and Treatment, University Press, Baltimore, MD, USA. Brambati, B., Cislaghi, C., Tului, L., Alberti, E., Amidani, M., Colombo, U. and Zuliani, G. 1995. ‘First-trimester Down’s syndrome screening using nuchal translucency: a prospective study in patients undergoing chorionic villus sampling’. Ultrasound in Obstetrics and Gynecology 5: 9–14. Brambati, B., Lanzani, A. and Tului, L. 1990. ‘Transabdominal and transcervical chorionic villus sampling: efficiency and risk evaluation of 2,411 cases’. American Journal of Medical Genetics 35: 160–164. 124 Nuchal translucency measurement in the first trimester of pregnancy Brambati, B., Tului, L., Simoni, G. and Travi, M. 1991. ‘Genetic diagnosis before the eighth gestational week’. Obstetrics and Gynecology 77: 318–321. Brizot, M., Theodoropoulos, P., Snijders, R. and Nicolaides, K. 1994. ‘First trimester fetal nuchal translucency’. In: Grudzinskas, J., Chard, T., Chapman, M and Cuckle, H. (eds)., Screening for Down’s Syndrome, Cambridge University Press, Cambridge. Brookes, M.E. and Alberman, E. 1996. ‘Early mortality and morbidity in children with Down syndrome diagnosed in two regional health authorities in 1989’. Journal of Medical Screening 3: 7–11. Buyse, M.L. 1990. The Birth Defects Encyclopedia. Blackwell Scientific Publications, Boston. Campbell, J.D., Elford, R.W. and Brant, R.F. 1993. ‘Case-control study of prenatal ultrasonography exposure in children with delayed speech’. Canadian Medical Association Journal 149: 1435–1440. Canick, J.A., Knight, G.J., Palomaki, G.E., Haddow, J.E., Cuckle, H.S. and Wald, N.J. 1988. ‘Low second trimester maternal serum unconjugated oestriol in pregnancies with Down syndrome’. British Journal of Obstetrics and Gynaecology 95: 330-333. Cartwright, R.A., McKinney, P.A., Hopton, P.A., Birch, J.M., Hartley, A.L., Mann, J.R., Waterhouse, J.A., Johnston, H.E., Draper, G.J. and Stiller, C. 1984. ‘Ultrasound examinations in pregnancy and childhood cancer’. Lancet 2: 999–1000. Chew, S., Anandakumar, C. and Ratman, S.S. 1995. ‘Maternal serum markers for Down’s syndrome pregnancies’. Singapore Medical Journal 36: 417-423. Cicero, S., Curcio, P., Papageorghiou, A., Sonek, J. and Nicolaides, K. 2001. ‘Absence of nasal bone in fetuses with trisomy 21 at 11-14 weeks of gestation: an observational study’. Lancet 358: 1665-67. Clarke, M. and Oxman, A. 1999. Cochrane Reviewer’s Handbook 4.0 [updated July 1999]. The Cochrane Collaboration, Oxford, England. Cochrane Methods Group on Systematic Reviews of Screening and Diagnostic Tests 1996, Recommended methods [Online]. Available from: http://som.flinders.edu.au/fusa/cochrane/ [Accessed on: 7 March 2000]. Comas, C., Martinez, J.M., Ojuel, J., Casals, E., Puerto, B., Borrell, A. and Fortuny, A. 1995. ‘First-trimester nuchal edema as a marker of aneuploidy’. Ultrasound in Obstetrics and Gynecology 5: 26–29. Commonwealth Department of Health and Aged Care 1999. Medicare Benefits Schedule 1 November 1999 with 1 February 2000 and 1 May 2000 supplements [Online]. Available from: http://www.health.gov.au/pubs/mbs/mbs5/default.htm [Accessed on: 20 September 2000]. Crane, J.P., LeFevre, M.L., Winborn, R.C., Evans, J.K., Ewigman, B.G., Bain, R.P., Frigoletto, F.D. and McNellis, D. 1994. ‘A randomized trial of prenatal ultrasonographic screening: impact on the detection, management, and outcome of anomalous fetuses’. American Journal of Obstetrics and Gynecology 171: 392–399. Nuchal translucency measurement in the first trimester of pregnancy 125 Canadian Task Force on the Periodic Health Examination (Canadian Task Force on the Periodic Health Examination) 1994. The Canadian Guide to Clinical Preventive Health Care. Canada Communication Group, Ottawa, Canada, Cuckle, H.S. et al. 1990. ‘Screening for Down’s syndrome’. In: Lilford, R. (ed). Prenatal Diagnosis and Prognosis. Butterworth, London. Cuckle, H. 1994. ‘Risk estimation in Down’s syndrome screening policy and practice’. In: Grudzinkas, J., Chard, T., Chapman, M. and Cuckle, H. (eds)., Screening for Down’s Syndrome. Grudzinskas J, Chard T, Chapman M and Cuckle H, Cambridge University Press, Cambridge. Cuckle, H. 1998. ‘Antenatal screening for Down’s syndrome’. Lancet 352: 1144–1145. Cuckle, H.S. and van Lith, J.M. 1999. ‘Appropriate biochemical parameters in firsttrimester screening for Down syndrome’. Prenatal Diagnosis 19: 505–512. Cuckle, H.S., Wald, N.J. and Thompson, S.G. 1987. ‘Estimating a woman’s risk of having a pregnancy associated with Down’s syndrome using her age and serum alpha-fetoprotein level’. British Journal of Obstetrics and Gynaecology 94: 387–402. Cullen, M.T., Gabrielli, S., Green, J.J., Rizzo, N., Mahoney, M.J., Salafia, C., Bovicelli, L. and Hobbins, J.C. 1990. ‘Diagnosis and significance of cystic hygroma in the first trimester’. Prenatal Diagnosis 10: 643–651. Cusick, W. and Vintzileos, A.M. 1999. ‘Fetal Down syndrome screening: a cost effectiveness analysis of alternative screening programs’. Journal of Maternal-Fetal Medicine 8 (6), 243–248. de Crespigny, L. and Dredge, R. 1997. Which Tests for my Unborn Baby? Ultrasound and Other Prenatal Tests. Oxford University Press, Melbourne. de Grouchy, J. and Turleau, C. 1983. ‘Autosomal Disorders’. In: Principles and Practice of Medical Genetics. Churchill Livingston, Edinburgh. Department of Human Services, 2000a. Down syndrome and your family [Online]. Department of Human Services, Australia. Available from: http://www.betterhealth.vic.gov.au/4A2566CF001EE13F/(LevelFour)/B47E212BC6456 39F4A25684E0015DB12?OpenDocument [Accessed 8 September 2000]. Department of Human Services, 2000b. Parents need information about their child’s disabilities [Online]. Department of Human Services, Australia Available from: http://www.betterhealth.vic.gov.au/4A2566CF001EE13F/(LevelFour)/ED2D50AE8C68 ACEF4A256744000BCC4D?OpenDocument [Accessed 8 September 2000]. DerSimonian, R. and Laird, N. 1986. ‘Meta-analysis in clinical trials’. Controlled Clinical Trials 7: 177–188. DeVore, G.R. 1994. ‘The Routine Antenatal Diagnostic Imaging with Ultrasound Study: another perspective’. Obstetrics and Gynecology 84: 622–626. DiMaio, M.S., Baumgarten, A., Greenstein, R.M., Saal, H.M. and Mahoney, M.J. 1987. ‘Screening for fetal Down’s syndrome in pregnancy by measuring maternal serum alphafetoprotein levels’. New England Journal of Medicine 317: 342–346. 126 Nuchal translucency measurement in the first trimester of pregnancy Down, L. 1866. ‘Some observations on an ethnic classification of idiots’. Clinical Lectures and Reports 3: 259–262. Drugan, A., Greb, A., Johnson, M.P., Krivchenia, E.L., Uhlmann, W.R., Moghissi, K.S. and Evans, M.I. 1990. ‘Determinants of parental decisions to abort for chromosome abnormalities’. Prenatal Diagnosis 10: 483–490. Drugan, A., Syner, F.N., Greb, A. and Evans, M.I. 1988. ‘Amniotic fluid alpha-fetoprotein and acetylcholinesterase in early genetic amniocentesis’. Obstetrics and Gynecology 72: 35–38. Dupont, A., Vaeth, M. and Videbech, P. 1986. ‘Mortality and life expectancy of Down’s syndrome in Denmark’. Journal of Mental Deficiency Research 30: 111–120. Eisenberg, V.H. and Schenker, J.J. 1997. ‘The moral aspects of prenatal diagnosis’. European Journal of Obstetrics, Gynecology and Reproductive Biology 72: 35–45. Ekwo, E.E., Kim, J.O. and Gosselink, C.A. 1987. ‘Parental perceptions of the burden of genetic disease’. American Journal of Medical Genetics 28: 955–963. Evans, M.I., Bottoms, S.F., Critchfield, G.C., Greb, A. and LaFerla, J.J. 1990. ‘Parental perceptions of genetic risk: correlation with choice of prenatal diagnostic procedures’. International Journal of Gynaecology and Obstetrics 31: 25–28. Evans, M.I., Koppich, F.Cd., Nemitz, B., Quigg, M.H. and Zador, I.E. 1988. ‘Early genetic amniocentesis and chorionic villus sampling. Expanding the opportunities for early prenatal diagnosis’. Journal of Reproductive Medicine 33: 450–452. Evans, S., Newnham, J., MacDonald, W. and Hall, C. 1996. ‘Characterisation of the possible effect on birthweight following frequent prenatal ultrasound examinations’. Early Human Development 45: 203–214. Ewigman, B.G., Crane, J.P., Frigoletto, F.D., LeFevre, M.L., Bain, R.P. and McNellis. D. 1993. ‘Effect of prenatal ultrasound screening on perinatal outcome’. RADIUS Study Group. New England Journal of Medicine 329: 821–827. FMF 2000. [Online]. The Fetal Medicine Foundation, Australia. Available from: http://www.fetalmedicine.com [Accessed 15 September 2000]. Fletcher, J. 1979. ‘Prenatal diagnosis, selective abortion, and the ethics of withholding treatment from the defective newborn’. Birth Defects: Original Article Series 15: 239–254. Fletcher, J., Hicks, N.R., Kay, J.D. and Boyd, P.A. 1995. ‘Using decision analysis to compare policies for antenatal screening for Down’s syndrome’. British Medical Journal 311: 351–356. Fort, P., Lifshitz, F., Bellisario, R., Davis, J., Lanes, R., Pugliese, M., Richman, R., Post E.M. and David, R. 1984. ‘Abnormalities of thyroid function in infants with Down syndrome’. Journal of Pediatrics 104: 545–549. Fost, N. 1992. ‘Ethical issues in genetics’. Pediatric Clinics of North America 39: 79–89. Franceschi, M., Comola, M., Piattoni, F., Gualandri, W. and Canal, N. 1990. ‘Prevalence of dementia in adult patients with trisomy 21’. American Journal of Medical Genetics 7 (Suppl): 306–308. Nuchal translucency measurement in the first trimester of pregnancy 127 Fuchs, F. and Riis, P. 1956. ‘Antenatal sex determination’. Nature 117: 330–335. Gill, M., Murday, V. and Slack, J. 1987. ‘An economic appraisal of screening for Down’s syndrome in pregnancy using maternal age and serum alpha fetoprotein concentration’. Social Science and Medicine 24: 725–731. Goel, V., Glazier, R., Summers, A. and Holzapfel, S. 1998. ‘Psychological outcomes following maternal serum screening: a cohort study’. Canadian Medical Association Journal 159: 651–656. Gordis, L. 2000. Epidemiology. W.B. Saunders Company, Philadelphia. Gordon, J.W. 1995. ‘The morality of prenatal diagnosis’. Human Reproduction 10: 767–768. Grisso, J.A., Strom, B.L., Cosmatos, I., Tolosa, J., Main, D. and Carson, J. 1994. ‘Diagnostic ultrasound in pregnancy and low birthweight’. American Journal of Perinatology 11: 297–301. Gross, R.H., Cox, A., Tatyrek, R., Pollay, M. and Barnes, W.A. 1983. ‘Early management and decision making for the treatment of myelomeningocele’. Pediatrics 72: 450–458. Hackshaw, A.K., Wald, N.J. and Haddow, J.E. 1996. ‘Down’s syndrome screening with nuchal translucency’. Lancet 348: 1740. Haddow, J.E. 1998. ‘Antenatal screening for Down’s syndrome: where are we and where next?’ Lancet 352: 336–337. Haddow, J.E., Palomaki, G.E., Knight, G.J., Foster, D.L. and Neveux, L.M, 1998. ‘Second trimester screening for Down’s syndrome using maternal serum dimeric inhibin A’. Journal of Medical Screening 5:115-199. Haddow, J.E., Palomaki, G.E., Knight, G.J., Williams, J., Miller, W.A. and Johnson, A. 1998. ‘Screening of maternal serum for fetal Down’s syndrome in the first trimester’. New England Journal of Medicine 338: 955–961. Haddow, J.E., Palomaki, G.E., Knight, G.J., Williams, J., Pulkkinen, A., Canick, J.A., Saller, D.N. (Jr) and Bowers, G.B. 1992. ‘Prenatal screening for Down’s syndrome with use of maternal serum markers’. New England Journal of Medicine 327: 588–593. Hafner, E., Schuchter, K. and Philipp, K. 1995. ‘Screening for chromosomal abnormalities in an unselected population by fetal nuchal translucency’. Ultrasound in Obstetrics and Gynecology 6: 330–333. Hahnemann, N. 1974. ‘Early prenatal diagnosis; a study of biopsy techniques and cell culturing from extraembryonic membranes’. Clinical Genetics 6: 294–306. Hall, S., Bobrow, M. and Marteau, T.M. 2000. ‘Psychological consequences for parents of false negative results on prenatal screening for Down’s syndrome: retrospective interview study’. British Medical Journal 320: 407–412. Halliday, J. 2002. Annual report on prenatal diagnosis in Victoria 2001. Murdoch Children’s Research Institute, Melbourne 128 Nuchal translucency measurement in the first trimester of pregnancy Hayes, C., Johnson, Z., Thornton, L., Fogarty, J., Lyons, R., O’Connor, M., Delany, V. and Buckley, K. 1997. ‘Ten-year survival of Down syndrome births’. International Journal of Epidemiology 26: 822–829. Health Insurance Commission 1999. Medicare Benefits Schedule (MBS) Item Statistics Reports [Online]. Available from: http://www.hic.gov.au/statistics/dyn_mbs/forms/mbs_tab4.shtml [Accessed on: 1 February 2001]. Hennekens, C. and Buring, J. 1987. Epidemiology in Medicine. Little, Brown and Company, Boston. Herman, A., Dreazen, E., Samandarov, A., Bukovsky, Y., Weinraub, Z. and Maymon, R. 2000. ‘On-to-on versus on-to-out nuchal translucency measurements’. Ultrasound in Obstetrics and Gynecology 15: 126–130. Herman, A., Maymon, R., Dreazen, E., Caspi, E., Bukovsky, I. and Weinraub. Z. 1998. ‘Nuchal translucency audit: a novel image-scoring method’. Ultrasound in Obstetrics and Gynecology 12: 398–403. Hewitt, B. 1993. ‘Nuchal translucency in the first trimester’. Australian and New Zealand Journal of Obstetrics and Gynaecology 33: 389–391. HGSA 1997. Prenatal diagnosis: HGSA policies [Online]. Human Genetics Society of Australasia, Australia. Available from: http://www.hgsa.com.au/policy/pd.html [Accessed 29 November 2000]. Hogdall, C.K., Hogdall, E.V.S., Arends, J., Norgaard-Pedersen, B., Smidt-Jensen, S. and Larsen, S.O. 1992. ‘CA125 as a maternal serum marker for Down’s syndrome in the first and second trimesters’. Prenatal Diagnosis 12: 223-237. Hook, E.B. and Chambers, G.M. 1977. ‘Estimated rates of Down syndrome in live births by one year maternal age intervals for mothers aged 20–49 in a New York State study – implications of the risk figures for genetic counselling and cost–benefit analysis of prenatal diagnosis programs’. Birth Defects Original Article Series 13: 123–141. Horwell, D.H., Loeffler, F.E. and Coleman, D.V. 1983. ‘Assessment of a transcervical aspiration technique for chorionic villus biopsy in the first trimester of pregnancy’. British Journal of Obstetrics and Gynaecology 90: 196–198. Hurst, T., Shafir, E., Day, P. and Lancaster, P. 1999. ‘Congenital malformations Australia, 1995 and 1996’. Australian Institute of Health and Welfare, National Perinatal Statistics Unit, Sydney. Hyett J, Perdu M, Sharland S, Snijders R, Nicolaides KH. 1999. ‘Using fetal nuchal translucency to screen for major congenital cardiac defects at 1014 weeks of gestation:population based cohort study’. British Medical Journal 318: 81-85. Hyett, J.A., Moscoso, G. and Nicolaides, K.H. 1995. ‘First-trimester nuchal translucency and cardiac septal defects in fetuses with trisomy 21’. American Journal of Obstetrics and Gynecology 172: 1411–1413. Nuchal translucency measurement in the first trimester of pregnancy 129 Hyett, J.A., Sebire, N.J., Snijders, R.J. and Nicolaides, K.H. 1996. ‘Intrauterine lethality of trisomy 21 fetuses with increased nuchal translucency thickness’. Ultrasound in Obstetrics and Gynecology 7: 101–103. Irwig, L., Tosteson, A.N., Gatsonis, C., Lau, J., Colditz, G., Chalmers, T.C. and Mosteller, F. 1994. ‘Guidelines for meta-analyses evaluating diagnostic tests’. Annals of Internal Medicine 120: 667–676. Janicki, M.P., Dalton, A.J., Henderson, C.M. and Davidson. P.W. 1999. ‘Mortality and morbidity among older adults with intellectual disability: health services considerations’. Disability and Rehabilitation 21: 284–294. Jauniaux, E., Brown, R., Snijders, R.J., Noble, P. and Nicolaides, K.H. 1997. ‘Early prenatal diagnosis of triploidy’. American Journal of Obstetrics and Gynecology 176: 550–554. Jenkins, T.M. and Wapner, R.J. 1999. ‘Integrated screening for Down’s syndrome’. New England Journal of Medicine 341: 1935; discussion 1936. Johnson, M.P., Johnson, A., Holzgreve, W., Isada, N.B., Wapner, R.J., Treadwell, M.C., Heeger, S. and Evans, M.I. 1993. ‘First-trimester simple hygroma: cause and outcome’. American Journal of Obstetrics and Gynecology 168: 156–161. Kadir, R.A. and Economides, D.L. 1997. ‘The effect of nuchal translucency measurement on second-trimester biochemical screening for Down’s syndrome’. Ultrasound in Obstetrics and Gynecology 9: 244–247. Kaufman, M.H. and Chang, H.H. 2000. ‘Studies of the mechanism of amniotic sac puncture-induced limb abnormalities in mice’. International Journal of Interventional Biology 44: 161–175. Keenan, K.L., Basso, D., Goldkrand, J. and Butler, W.J. 1991. ‘Low level of maternal serum alpha-fetoprotein: its associated anxiety and the effects of genetic counselling’. American Journal of Obstetrics and Gynecology 164: 54–56. Khalid, L., Price, S.M. and M. B. 1994. ‘Attitudes of midwives to maternal serum screening for Down’s syndrome’. Public Health 108: 131–136. Kidd, J., Cook, R. and Marteau, T.M. 1993. ‘Is routine AFP screening in pregnancy reassuring?’ Journal of Psychosomatic Research 37: 717–722. Kieler, H., Ahlsten, G., Haglund, B., Salvesen, K. and Axelsson, O. 1998a. ‘Routine ultrasound screening in pregnancy and the children’s subsequent neurologic development’. Obstetrics and Gynecology 91: 750–756. Kieler, H., Axelsson, O., Haglund, B., Nilsson, S. and Salvesen, K.A. 1998b. ‘Routine ultrasound screening in pregnancy and the children’s subsequent handedness’. Early Human Development 50: 233–245. Kieler, H., Haglund, B., Waldenstrom, U. and Axelsson, O. 1997. ‘Routine ultrasound screening in pregnancy and the children’s subsequent growth, vision and hearing’. British Journal of Obstetrics and Gynaecology 104: 1267–1272. Kinnier Wilson, L.M. and Waterhouse, J.A. 1984. ‘Obstetric ultrasound and childhood malignancies’. Lancet 2: 997–999. 130 Nuchal translucency measurement in the first trimester of pregnancy Korenberg, J., Pulst, S. and Gerwehr, S. 1992. ‘Advances in the understanding of chromosome 21 and Down syndrome’. In: Lott, I. and McCoy. E. (eds)., Down Syndrome: Advances in Medical Care John Wiley and Sons, Inc., New York. Kornman, L.H., Morssink, L.P., Beekhuis, J.R., De Wolf, B.T., Heringa, M.P. and Mantingh, A. 1996. ‘Nuchal translucency cannot be used as a screening test for chromosomal abnormalities in the first trimester of pregnancy in a routine ultrasound practice’. Prenatal Diagnosis 16: 797–805. Kullander, S. and Sandahl, B. 1973. ‘Fetal chromosome analysis after transcervical placental biopsies during early pregnancy’. Acta Obstetrica et Gynecologica Scandinavica 52: 355–359. Kuppermann, M., Goldberg, J.D., Nease, R.F. (Jr)., and Washington, A.E. 1999. ‘Who should be offered prenatal diagnosis? The 35-year-old question’. American Journal of Public Health 89: 160–163. Kurman, R.J., Young, R.H., Norris, H.K., Main, C.S., Lawrence, W.D. and Scully, R.E. 1984. ‘Immunocytochemical localization of placental lactogen and chorionic gonadotropin in the normal placenta and trophoblastic tumours, with emphasis on intermediate trophoblast and the placental site trophoblastic tumour’. International Journal of Gynecological Pathology 3:101-21. LeFevre, M.L., Bain, R.P., Ewigman, B.G., Frigoletto, F.D., Crane, J.P. and McNellis, D. 1993. ‘A randomized trial of prenatal ultrasonographic screening: impact on maternal management and outcome’. American Journal of Obstetrics and Gynecology 169: 483–489. Lejeune, J., Gautier, M. and Turpin, R. 1959a. ‘Human chromosomes in tissue culture’. Comptes Rendus de l’Academie des Sciences 248: 602–606. Lejeune, J., Gautier, M. and Turpin,R. 1959b. ‘Studies of the somatic chromosomes of nine Mongoloid children’. Comptes Rendus de l’Academie des Sciences 248: 1721–1728. Lippman, A., Tomkins, D.J., Shime, J. and Hamerton, J.L. 1992. ‘Canadian multicentre randomized clinical trial of chorion villus sampling and amniocentesis’. Prenatal Diagnosis 12: 385–408. Loncar, J., Barnabei, V.M. and Larsen, J.W. Jr., 1995. ‘Advent of maternal serum markers for Down syndrome screening’. Obstetrics and Gynecological Survey 50: 316–320. Lustig, L., Clarke, S., Cunningham, G., Schonberg, R. and Tompkinson, G. 1988. ‘California’s experience with low MS-AFP results’. American Journal of Medical Genetics 31: 211–222. Macdonald, W., Newnham, J., Gurrin, L. and Evans, S. 1996. ‘Effect of frequent prenatal ultrasound on birthweight: follow up at 1 year of age’. Western Australian Pregnancy Cohort (Raine) Working Group. Lancet 348: 482. Malone, F.D, Berkowitz, R.L., Canick, J.A. and D’Alton, M.E. 2000. ‘First-trimester screening for aneuploidy: research or standard of care?’ American Journal of Obstetrics and Gynecology 182: 490–496. Malone, F.D., D’Alton, M.E. and Berkowitz, R.L. 1999. ‘Integrated screening for Down’s syndrome’. New England Journal of Medicine 341: 1935–1936; discussion 1937. Nuchal translucency measurement in the first trimester of pregnancy 131 Mange, A.P. and Mange, E.J. 1990. Genetics: Human Aspects. Sinauer Associates, Massachusetts. Marteau, T.M., Cook, R., Kidd, J., Michie, S., Johnston, M., Slack, J. and Shaw, R.W. 1992a. ‘The psychological effects of false-positive results in prenatal screening for fetal abnormality: a prospective study’. Prenatal Diagnosis 12: 205–214. Marteau, T.M., Kidd, J., Cook, R., Michie, S., Johnston, M., Slack, J. and Shaw, R.W. 1991. ‘Perceived risk not actual risk predicts uptake of amniocentesis’. British Journal of Obstetrics and Gynaecology 98: 282–286. Marteau, T.M., Slack, J., Kidd, J. and Shaw, R.W. 1992b. ‘Presenting a routine screening test in antenatal care: practice observed’. Public Health 106: 131–141. Martinez, J.M., Borrell, A., Antolin, E., Puerto, B., Casals, E., Ojuel, J. and Fortuny, A. 1997. ‘Combining nuchal translucency with umbilical Doppler velocimetry for detecting fetal trisomies in the first trimester of pregnancy’. British Journal of Obstetrics and Gynaecology 104: 11–14. Maymon, R., Herman, A., Dreazen, E., Tovbin, Y., Bukovsky, I. and Weinraub, Z. 1999. ‘Can nuchal cord cause transient increased nuchal translucency thickness?’ Human Reproduction 14: 556–559. McVicker, R.W., Shanks, O.E. and McClelland, R.J. 1994. ‘Prevalence and associated features of epilepsy in adults with Down’s syndrome’. British Journal of Psychiatry 164: 528– 532. Merkatz, I.R., Nitowsky, H.M., Macri, J.N. and Johnson, W.E. 1984. ‘An association between low maternal serum alpha-fetoprotein and fetal chromosomal abnormalities’. American Journal of Obstetrics and Gynecology 148: 886–894. Merrick, J. 2000. ‘Incidence and mortality of Down syndrome’. Israel Medical Association Journal 2: 25–26. Miller, M.W., Brayman, A.A. and Abramowicz, J.S. 1998. ‘Obstetric ultrasonography: a biophysical consideration of patient safety – the ‘rules’ have changed’. American Journal of Obstetrics and Gynecology 179: 241–254. Mohr, J. 1968. ‘Foetal genetic diagnosis: development of techniques for early sampling of foetal cells’. Acta Pathologica et Microbiologica Scandinavica 73: 73–77. Mol, B.W., Lijmer, J.G., van der Meulen, J., Pajkrt, E., Bilardo, C.M. and Bossuyt, P.M. 1999. ‘Effect of study design on the association between nuchal translucency measurement and Down syndrome’. Obstetrics and Gynecology 94: 864–869. Mol, B.W., Pajkrt, E., van Lith, J.J. and Bilardo, C.M. 1996. ‘Screening for fetal trisomies by maternal age and fetal nuchal translucency thickness at 10 to 14 weeks of gestation’. British Journal of Obstetrics and Gynaecology 103: 1051–1052. Monni, G., Zoppi, M.A., Ibba, R.M. and Floris, M. 1997. ‘Fetal nuchal translucency test for Down’s syndrome’. Lancet 350: 1631–1632. 132 Nuchal translucency measurement in the first trimester of pregnancy Morgan, F.J., Birken, S. and Canfield, R.E. 1975. ‘The amino acid sequence of human chorionic gonadotrophin. The alpha subunit and beta subunit’. Journal of Biological Chemistry 250: 5247-58 Mori, M., Brambati, B. and Tului, L. 1995. ‘The current ethical controversy over reproductive medicine: prenatal diagnosis’. Human Reproduction 10: 765–766. Morris, J.K., Mutton, D.E., Ide, R., Alberman, E. and Bobrow, M. 1994. ‘Monitoring trends in prenatal diagnosis of Down’s syndrome in England and Wales, 1989–92’. Journal of Medical Screening 1: 233–237. Medical Research Council 1991. ‘Medical Research Council European trial of chorion villus sampling’. Lancet 337: 1491–1499. Muller, F. and Bussieres, L. 1996. ‘Maternal serum markers for fetal trisomy 21 screening’. European Journal of Obstetrics, Gynecology and Reproductive Biology 65: 3–6. Mulvey, S. and Wallace, E.M. 2000. ‘Women’s knowledge of and attitudes to first and second trimester screening for Down’s syndrome’. British Journal of Obstetrics and Gynaecology 107: 1302–1305. Nadel, A., Bromley, B. and Benacerraf, B.R. 1993. ‘Nuchal thickening or cystic hygromas in first- and early second-trimester fetuses: prognosis and outcome’. Obstetrics and Gynecology 82: 43–48. Nadler, H.L. 1968. ‘Antenatal detection of hereditary disorders’. Pediatrics 42: 912–918. Naumburg, E., Bellocco, R., Cnattingius, S., Hall, P. and Ekbom, A. 2000. ‘Prenatal ultrasound examinations and risk of childhood leukaemia: case-control study’. British Medical Journal 320: 282–283. NHS HTA, 2000. SURUSS (serum, urine and ultrasound screening program) [Online]. National Health Service Health Technology Assessment, England. Available from: http://www.hta.nhsweb.nhs.uk/projdets/932505.htm [Accessed 20 September 2000]. Newnham, J.P., Evans, S.F., Michael, C.A., Stanley, F.J. and Landau, L.I. 1993. ‘Effects of frequent ultrasound during pregnancy: a randomised controlled trial’. Lancet 342: 887–891. NHMRC, 2000. ‘How to Use the Evidence: Assessment and Application of Scientific Evidence’. National Health and Medical Research Council, Canberra. NICHHD (National Institute of Child Health and Human Development) Study Group 1976. ‘Midtrimester amniocentesis for prenatal diagnosis. Safety and accuracy’. Journal of the American Medical Association 236: 1471–1476. NICHHD 1979. ‘Antenatal diagnosis: report of a consensus development conference’. National Institute of Child Health and Human Development, Bethesda, MD, USA. Nicolaides, K., Sebire, N. and Snijders, R. 1999b. ‘Nuchal translucency and chromosomal effects’. In: Nicolaides, K., Sebire, N. and Snijders, R. (eds)., The 11–14-week Scan: The Diagnosis of Fetal Abnormalities. Parthenon Publishing Group, London. Nicolaides, K., Sebire, N. and Snijders, R. 1999a. The 11–14 week Scan: The Diagnosis of Fetal Abnormalities. Parthenon Publishing Group, New York. Nuchal translucency measurement in the first trimester of pregnancy 133 Nicolaides, K.H., Azar, G., Byrne, D., Mansur, C. and Marks, K. 1992. ‘Fetal nuchal translucency: ultrasound screening for chromosomal defects in first trimester of pregnancy’. British Medical Journal 304: 867–869. Nicolaides, K.H., Brizot, M.L. and Snijders, R.J. 1994. ‘Fetal nuchal translucency: ultrasound screening for fetal trisomy in the first trimester of pregnancy’. British Journal of Obstetrics and Gynaecology 101: 782–786. O’Callaghan, S.P., Giles, W.B., Raymond, S.P., McDougall, V., Morris, K. and Boyd, J. 2000. ‘First trimester ultrasound with nuchal translucency measurement for Down syndrome risk estimation using software developed by the Fetal Medicine Foundation, United Kingdom –- the first 2000 examinations in Newcastle, New South Wales, Australia’. Australian and New Zealand Journal of Obstetrics and Gynaecology 40: 292–295. Pajkrt, E., de Graaf, I.M., Mol, B.W., van Lith, J.M., Bleker, O.P. and Bilardo, C.M. 1998. ‘Weekly nuchal translucency measurements in normal fetuses’. Obstetrics and Gynecology 91: 208–211. Palomki, G.E. and Haddow, J.E. 1987. ‘Maternal serum alpha-fetoprotein, age and Down’s syndrome risk’. American Journal of Obstetrics and Gynecology 156: 460-3. Pandya, P.P., Altman, D.G., Brizot, M.L., Pettersen, H. and Nicolaides, K.H. 1995a. ‘Repeatability of measurement of fetal nuchal translucency thickness’. Ultrasound in Obstetrics and Gynecology 5: 334–337. Pandya, P.P., Brizot, M.L., Kuhn, P., Snijders, R.J. and Nicolaides. K.H. 1994. ‘Firsttrimester fetal nuchal translucency thickness and risk for trisomies’. Obstetrics and Gynecology 84: 420–423. Pandya, P.P., Kondylios, A., Hilbert, L., Snijders, R.J. and Nicolaides, K.H. 1995b. ‘Chromosomal defects and outcome in 1015 fetuses with increased nuchal translucency’. Ultrasound in Obstetrics and Gynecology 5: 15–19. Pastore, L.M., Hertz-Picciotto, I. and Beaumont, J.J. 1999. ‘Risk of stillbirth from medications, illnesses and medical procedures’. Paediatric and Perinatal Epidemiology 13: 421– 430. Penrose, L. 1934. ‘The relative aetiological importance of birth order and maternal age in mongolism’. Proceedings of the Royal Society of London 115: 431–450. Phillips, O.P., Elias, S., Shulman, L.P., Andersen, R.N., Morgan, C.D. and Simpson, J.L. 1992. ‘Maternal serum screening for fetal Down syndrome in women less than 35 years of age using alpha-fetoprotein, hCG, and unconjugated estriol: a prospective 2-year study’. Obstetrics and Gynecology 80: 353–358. Pueschel, S.M. 1991. ‘Ethical considerations relating to prenatal diagnosis of fetuses with Down syndrome’. Mental Retardation 29: 185–190. RANZCOG, 2000. Antenatal screening for Down syndrome and other fetal aneuploidy [Online]. Royal Australian and New Zealand College of Obstetricians and Gynaecologists, Australia. Available from: http://www.racog.edu.au/open/statements/2-2b.pdf [Accessed 14 September 2000]. 134 Nuchal translucency measurement in the first trimester of pregnancy RCOG, 1997. ‘Recommendations arising from the Study Group on Screening for Down Syndrome in the First Trimester’. Report of the Study Group. Royal College of Obstetrics and Gynaecology, London. RCOG, 2000. ‘Routine ultrasound screening in pregnancy: protocols, standards and training’. Supplement to Ultrasound Screening for Fetal Abnormalities: Report of the RCOG Working Party. Royal College of Obstetrics and Gynaecology, London. Reed, B.D., Ratcliffe, S. and Sayres, W. 1988. ‘Maternal serum alpha-fetoprotein screening’. Journal of Family Practice 27: 20, 22, 26. Reynolds, T.M. 1998. ‘Antenatal screening for Down’s syndrome’. Lancet 352: 1145. Reynolds, T., Zimmermann, R. and Wright, E. 1999. ‘Integrated screening for Down’s syndrome’. New England Journal of Medicine 341: 1935; discussion 1936. Roberts, L.J., Bewley, S., Mackinson, A.M. and Rodeck, C.H. 1995. ‘First trimester fetal nuchal translucency: problems with screening the general population’. British Journal of Obstetrics and Gynaecology 102: 381–385. Roberts, T., Mugford, M., Piercy, J. 1998. ‘Choosing options for ultrasound screening in pregnancy and comparing cost effectiveness: a decision analysis approach’. British Journal of Obstetrics and Gynaecology 105: 960–970 Roelofsen, E.E., Kamerbeek, L.I., Tymstra, T.J., Beekhuis, J.R. and Mantingh, A. 1993. ‘Women’s opinions on the offer and use of maternal serum screening’. Prenatal Diagnosis 13: 741–747. Romero, R. 1993. ‘Routine obstetric ultrasound’. Ultrasound in Obstetrics and Gynecology 3: 303–307. Rothman, K. and Greenland, S. 1998. Modern Epidemiology. Lippincott-Raven, Philadelphia. Royston, P. and Thompson, S.G. 1992. ‘Model-based screening by risk with application to Down’s syndrome’. Statistics in Medicine 11: 257–268. SABDR, 1998. ‘1997 Annual Report of the South Australian Birth Defects Register’. South Australia Birth Defects Register, Adelaide, Australia. Sadler, M. 1997. ‘Serum screening for Down’s syndrome: how much do health professionals know?’ British Journal of Obstetrics and Gynaecology 104: 176–179. Salvesen, K.A. and Eik-Nes, S.H. 1999a. ‘Ultrasound during pregnancy and birthweight, childhood malignancies and neurological development’. Ultrasound in Medicine and Biology 25: 1025–1031. Salvesen, K.A. and Eik-Nes, S.H. 1999b. ‘Ultrasound during pregnancy and subsequent childhood non-right handedness: a meta-analysis’. Ultrasound in Obstetrics and Gynecology 13: 241–246. Salvesen, K.A., Bakketeig, L.S., Eik-Nes, S.H., Undheim, J.O. and Okland, O. 1992. ‘Routine ultrasonography in utero and school performance at age 8–9 years’. Lancet 339: 85–89. Nuchal translucency measurement in the first trimester of pregnancy 135 Santalahti, P., Latikka, A.M., Ryynanen, M. and Hemminki, E. 1996. ‘Women’s experiences of prenatal serum screening’. Birth 23: 101–107. Savoldelli, G., Binkert, F., Achermann, J. and Schmid, W. 1993. ‘Ultrasound screening for chromosomal anomalies in the first trimester of pregnancy’. Prenatal Diagnosis 13: 513–518. Schafer, D., Arnemann, J., Brude, E. and Baumann, R. 1995. ‘Society must decide about prenatal diagnosis’. Human Reproduction 10: 768–769. Schuchter, K., Wald, N., Hackshaw, A.K., Hafner, E. and Liebhart, E. 1998. ‘The distribution of nuchal translucency at 10–13 weeks of pregnancy’. Prenatal Diagnosis 18: 281–286. Schwarzler, P., Carvalho, J.S., Senat, M.V., Masroor, T., Campbell, S. and Ville, Y. 1999. ‘Screening for fetal aneuploidies and fetal cardiac abnormalities by nuchal translucency thickness measurement at 10–14 weeks of gestation as part of routine antenatal care in an unselected population’. British Journal of Obstetrics and Gynaecology 106: 1029–1034. Scott, F., Wheeler, D., Sinosich, M., Boogert, A., Anderson, J. and Edelman, D. 1996. ‘First trimester aneuploidy screening using nuchal translucency, free beta human chorionic gonadotrophin and maternal age’. Australian and New Zealand Journal of Obstetrics and Gynaecology 36: 381–384. Sebire, N.J., Snijders, R.J., Brown, R., Southall, T. and Nicolaides, K.H. 1998. ‘Detection of sex chromosome abnormalities by nuchal translucency screening at 10–14 weeks’. Prenatal Diagnosis 18: 581–584. Serra-Prat, M., Gallo, P., Jovell, A.J., Aymerich, M., Estrada, M.D. 1998. ‘Trade-offs in prenatal detection of Down syndrome’. American Journal of Public Health 88 (4): 551–7. Sherod, C., Sebire, N.J., Soares, W., Snijders, R.J. and Nicolaides, K.H. 1997. ‘Prenatal diagnosis of trisomy 18 at the 10–14-week ultrasound scan’. Ultrasound in Obstetrics and Gynecology 10: 387–390. Shu, X.O., Jin, F., Linet, M.S., Zheng, W., Clemens, J., Mills, J. and Gao, Y.T. 1994. ‘Diagnostic X-ray and ultrasound exposure and risk of childhood cancer’. British Journal of Cancer 70: 531–536. Shulman, L.P., Emerson, D.S., Felker, R.E., Phillips, O.P., Simpson, J.L. and Elias, S. 1992. ‘High frequency of cytogenetic abnormalities in fetuses with cystic hygroma diagnosed in the first trimester’. Obstetrics and Gynecology 80: 80–82. Shuttleworth, G. 1909. ‘Mongolian imbecility’. British Medical Journal 2: 661–665. Silver, R.K., MacGregor, S.N., Sholl, J.S., Hobart, E.D. and Waldee, J.K. 1990. ‘An evaluation of the chorionic villus sampling learning curve’. American Journal of Obstetrics and Gynecology 163: 917–922. Smith, D.K., Shaw, R.W. and Marteau, T.M. 1994. ‘Informed consent to undergo serum screening for Down’s syndrome: the gap between policy and practice’. British Medical Journal 309: 776. 136 Nuchal translucency measurement in the first trimester of pregnancy Smith, D.K., Shaw, R.W., Slack, J. and Marteau, T.M. 1995. ‘Training obstetricians and midwives to present screening tests: evaluation of two brief interventions’. Prenatal Diagnosis 15: 317–324. Smith, G.F. and Berg, J.M.B. 1976. Down’s Anomaly. Edinburgh, Churchill Livingstone. Snijders, R.J. Noble, P., Sebire, N., Souka, A. and Nicolaides, K.H. 1998. ‘UK multicentre project on assessment of risk of trisomy 21 by maternal age and fetal nuchal-translucency thickness at 10–14 weeks of gestation’. Lancet 352: 343–346. Snijders, R.J. Sebire, N.J. and Nicolaides. K.H. 1995. ‘Maternal age and gestational agespecific risk for chromosomal defects’. Fetal Diagnosis and Therapy 10: 356–367. Snijders, R.J., Sebire, N.J., Nayar, R., Souka, A. and Nicolaides, K.H. 1999a. ‘Increased nuchal translucency in trisomy 13 fetuses at 10–14 weeks of gestation’. American Journal of Medical Genetics 86: 205–207. Snijders, R.J., Sundberg, K., Holzgreve, W., Henry, G., Nicolaides, K.H. 1999b. ‘Maternal age- and gestation-specific risk for trisomy 21’. Ultrasound in Obstetrics and Gynecology 13: 167–70. Spencer, K. and Carpenter, P. 1993. ‘Prospective study of prenatal screening for Down’s syndrome with free beta human chorionic gonadotrophin’. British Medical Journal 307: 764– 769. Staples, A.J., Sutherland, G.R., Haan, E.A. and Clisby, S. 1991. ‘Epidemiology of Down Syndrome in South Australia, 1960–89’. American Journal of Human Genetics 49: 1014–1024. Statham, H. and Green, J. 1993. ‘Serum screening for Down’s syndrome: some women’s experiences’. British Medical Journal 307: 174–176. Steele, M.W. and Breg, W.R. Jr., 1966. ‘Chromosome analysis of human amniotic-fluid cells’. Lancet 1: 383–385. Stewart, T.L. and Malone, F.D. 1999. ‘First trimester screening for aneuploidy: nuchal translucency sonography’. Seminars in Perinatology 23: 369–381. Stranc, L.C., Evans, J.A. and Hamerton, J.L. 1997. ‘Chorionic villus sampling and amniocentesis for prenatal diagnosis’. Lancet 349: 711–714. Suchet, I.B., van der Westhuizen, N.G. and Labatte, M.F. 1992. ‘Fetal cystic hygromas: further insights into their natural history’. Canadian Association of Radiologists Journal 43: 420– 424. Szabo, J. and Gellen, J. 1990. ‘Nuchal fluid accumulation in trisomy-21 detected by vaginosonography in first trimester’. Lancet 336: 1133. Szabo, J., Gellen, J. and Szemere, G. 1995. ‘First-trimester ultrasound screening for fetal aneuploidies in women over 35 and under 35 years of age’. Ultrasound in Obstetrics and Gynecology 5: 161–163. Tabor, A., Philip, J., Madsen, M., Bang, J., Obel, E.B. and Norgaard-Pedersen, B. 1986. ‘Randomised controlled trial of genetic amniocentesis in 4606 low-risk women’. Lancet 1: 1287–1293. Nuchal translucency measurement in the first trimester of pregnancy 137 Taipale, P. and Hiilesmaa, V. 1999. ‘Ultrasonographic screening for fetal chromosomal abnormalities in early pregnancy’. Acta Obstetricia et Gynecologica Scandinavica 78: 563–572. Thase, M.E. 1982. ‘Longevity and mortality in Down’s syndrome’. Journal of Mental Deficiency Research 26: 177–192. Thilaganathan, B., Sairam, S., Michailidis, G. and Wathen, N.C. 1999. ‘First trimester nuchal translucency: effective routine screening for Down’s syndrome’. British Journal of Radiology 72: 946–948. Thilaganathan, B., Slack, A. and Wathen, N.C. 1997. ‘Effect of first-trimester nuchal translucency on second-trimester maternal serum biochemical screening for Down’s syndrome’. Ultrasound in Obstetrics and Gynecology 10: 261–264. Thornton, J.G., Hewison, J., Lilford, R.J. and Vail, A. 1995. ‘A randomised trial of three methods of giving information about prenatal testing’. British Medical Journal 311: 1127– 1130. USPSTF 1996. Guide to Clinical Preventive Services. US Preventive Services Task Force,Williams and Wilkins, Baltimore, Maryland. Van Blerk, M., Smitz, J., De Catte, L., Kumps, C., Van Der Elst, J. and Van Steirteghem, A.C. 1992. ‘Second-trimester cancer antigen 125 and Down’s syndrome’. Prenatal Diagnosis 12: 1062-1026. Valenti, C., Schutta, E.J. and Kehaty, T. 1968. ‘Prenatal diagnosis of Down’s syndrome’. Lancet 2: 220. Van Lith, J.M.M., Pratt, J.J., Beekhuis, J.R. and Mantingh, A. 1992. ‘Second-trimester maternal serum immunoreactive inhibin as a marker for fetal Down’s syndrome’. Prenatal Diagnosis 12: 801-816. van Zalen-Sprock, R.M., van Vugt, J.M. and van Geijn, H.P. 1992. ‘First-trimester diagnosis of cystic hygroma – course and outcome’. American Journal of Obstetrics and Gynecology 167: 94–98. Ville, Y., Lalondrelle, C., Doumerc, S., Daffos, F., Frydman, R., Oury, J. and Dumez, Y. 1992. ‘First-trimester diagnosis of nuchal anomalies: significance and fetal outcome’. Ultrasound in Obstetrics and Gynecology 2: 314–316. Vintzileos, A.M., Ananth, C.V., Fisher, A.J., Smulian, J.C., Day-Salvatore, D., Beazoglou, T., Knuppel, R.A. 1998. ‘An economic evaluation of second-trimester genetic ultrasonography for prenatal detection of Down syndrome’. American Journal of Obstetrics and Gynecology 179’(5): 1214–1219. Vintzileos, A.M., Ananth, C.V., Smulian, J.C., Day-Salvatore, D.L., Beazoglou, T. and Knuppel, R.A. 2000. ‘Cost-benefit analysis of prenatal diagnosis for Down syndrome using the British or the American approach’. Obstetrics and Gynecology 95: 577–583. Wald, N.J., Cuckle, H.S., Densem, J.W., Nanchahal, K., Royston, P., Chard, T., Haddow, J.E., Knight. G.J. Palomaki, G.E. and Canick, J.A. 1988. ‘Maternal serum screening for Down’s syndrome in early pregnancy’. British Medical Journal 297: 883–887. 138 Nuchal translucency measurement in the first trimester of pregnancy Wald, N.J., Densem, J.W., George, L., Muttukrishna, S. and Knight, P.G. 1996a. ‘Prenatal screening for Down’s syndrome using inhibin-A as a serum marker’. Prenatal Diagnosis 16: 143–153. Wald, N.J., Densem, J.W., George, L., Muttukrishna, S., Knight, P.G., Watt, H., Hacksaw, A. and Morris, J.K. 1997a. ‘Inhibin-A in Down’s syndrome pregnancies: revised estimate of standard deviation’. Prenatal Diagnosis 17: 285–290. Wald, N.J., Densem, J.W., Smith, D. and Klee, G.G. 1994. ‘Four-marker serum screening for Down’s syndrome’. Prenatal Diagnosis 14: 707–716. Wald, N.J., Hackshaw, A.K., Huttly, W. and Kennard, A. 1996b. ‘Empirical validation of risk screening for Down’s syndrome’. Journal of Medical Screening 3: 185–187. Wald, N.J., Kennard, A. and Hackshaw, A.K. 1995. ‘First trimester serum screening for Down’s syndrome’. Prenatal Diagnosis 15: 1227–1240. Wald, N.J., Kennard, A., Hackshaw, A. and McGuire, A. 1997b. ‘Antenatal screening for Down’s syndrome’. [published erratum appears in Journal of Medical Screening 1998; 5 (2):110 and 1998;5(3):166]. Journal of Medical Screening 4: 181–246. Wald, N.J., Kennard, A., Hackshaw, A. and McGuire, A. 1998. ‘Antenatal screening for Down’s syndrome’. Health Technology Assessment 2: 1–112. Wald, N.J., Watt, H.C. and Hackshaw, A.K. 1999. ‘Integrated screening for Down’s syndrome on the basis of tests performed during the first and second trimesters’. New England Journal of Medicine 341: 461–467. Watson, W.J., Katz, V.L. and Thorp, J.M. Jr., 1991. ‘Spontaneous resolution of fetal nuchal cystic hygroma’. Journal of Perinatology 11: 213–215. Webley, C. and Halliday, J. 2000. Report on prenatal diagnostic testing in Victoria, 1999. Perinatal Data Collection Unit, Murdoch Children’s Research Institute, Melbourne. White-van Mourik, M.C., Connor, J.M. and Ferguson-Smith, M.A. 1992. ‘The psychosocial sequelae of a second-trimester termination of pregnancy for fetal abnormality’. Prenatal Diagnosis 12: 189–204. Whitlow, B.J. and Economides, D.L. 1998. ‘The optimal gestational age to examine fetal anatomy and measure nuchal translucency in the first trimester’. Ultrasound in Obstetrics and Gynecology 11: 258–261. Whitlow, B.J., Chatzipapas, I.K. and Economides, D.L. 1998. ‘The effect of fetal neck position on nuchal translucency measurement’. British Journal of Obstetrics and Gynaecology 105: 872–876. WHO and PAHO, 1999. ‘Evaluation of chorionic villus sampling safety: World Health Organization and Pan American Health Organization consultation on CVS’. Prenatal Diagnosis 19: 97–99. Williamson, P., Harris, R., Church, S., Fiddler, M. and Rhind, J. 1996. ‘Prenatal genetic services for Down’s syndrome: access and provision in 1990–1991’. British Journal of Obstetrics and Gynaecology 103: 676–683. Nuchal translucency measurement in the first trimester of pregnancy 139 Ziskin, M.C. 1999. ‘Intrauterine effects of ultrasound: human epidemiology’. Teratology 59: 252–260. 140 Nuchal translucency measurement in the first trimester of pregnancy

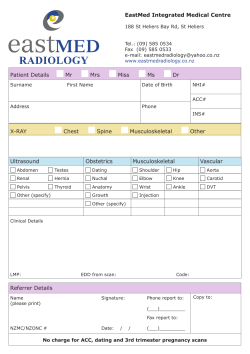








© Copyright 2026