
Detection of overweight and obesity in a national sample of
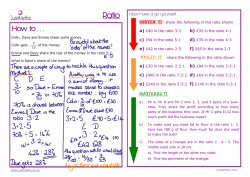
Detection of overweight and obesity in a national sample of 6 –12-y-old Swiss children: accuracy and validity of reference values for body mass index from the US Centers for Disease Control and Prevention and the International Obesity Task Force1–3 Michael B Zimmermann, Carolyn Gu¨beli, Claudia Pu¨ntener, and Luciano Molinari KEY WORDS Body mass index, skinfold thickness, anthropometry, percentage of body fat, sensitivity, specificity, children, Switzerland INTRODUCTION Measurement of body mass index (BMI; in kg/m2) is a practical and reproducible method for classifying overweight in adults (1, 2) and is increasingly recommended for screening overweight in children and adolescents (3–5). New growth charts from the US Centers for Disease Control and Prevention (CDC) include age- and sex-specific BMI reference values for children and adolescents aged 2–20 y (6). The International Obesity Task 838 Force (IOTF) has also published age- and sex-specific BMI criteria for children and has proposed them as international reference values (5). Because these 2 sets of reference criteria differ, they may produce different estimates of overweight and obesity (7–9). Moreover, BMI is an expression of weight, not adiposity, and the accuracy of these reference values in classifying adiposity in children has not yet been validated in most countries (10). Many methods available to measure body fatness, including dual-energy X-ray absorptiometry (DXA), underwater weighing, and total body potassium, are limited by their complexity and cost to research settings (11–14). In clinical and public health settings, body fatness has traditionally been estimated from skinfold thicknesses (SFTs) (1, 15, 16). Although single SFT measurements have only limited precision (17, 18), reproducibility is improved by using multisite measurements integrated into validated prediction equations (18, 19). Schaefer et al (18) reported an intraobserver CV of 2%, which corresponded to 0.4% of fractional fat mass, with the use of multisite SFTs in children. SFT measurements can accurately predict percentage of body fat (%BF) in childhood (13, 18, 20). In the present study, we compared the new CDC and IOTF sex-specific BMI-for-age reference values to %BF values estimated from multisite SFTs in screening for overweight and obesity in a nationally representative sample of 6 –12-y-old Swiss schoolchildren. SUBJECTS AND METHODS A probability-proportionate-to-size cluster sampling based on current census data was used to obtain a representative national sample of 2600 Swiss children aged 6 –12 y. This represents 앒1 1 From the Laboratory for Human Nutrition, Institute for Food Science and Nutrition (MBZ), and the Institute for Pharmaceutical Science (CG and CP), Swiss Federal Institute of Technology Zu¨rich, Switzerland; and the Department of Growth and Development, University Childrens’ Hospital, Zu¨rich, Switzerland (LM). 2 Supported by the Swiss Foundation for Nutrition Research, Zu¨rich, Switzerland, and the Swiss Federal Institute of Technology, Zu¨rich, Switzerland. 3 Reprints not available. Address correspondence to MB Zimmermann, Laboratory for Human Nutrition, Swiss Federal Institute of Technology Zu¨rich, PO Box 474, Seestrasse 72, CH-8803 Ru¨schlikon, Switzerland. E-mail: [email protected]. Received May 30, 2003. Accepted for publication October 22, 2003. Am J Clin Nutr 2004;79:838 – 43. Printed in USA. © 2004 American Society for Clinical Nutrition Downloaded from ajcn.nutrition.org by guest on October 6, 2014 ABSTRACT Background: For defining overweight in children, reference values for body mass index (BMI) are available from the US Centers for Disease Control and Prevention (CDC) and the International Obesity Task Force (IOTF). However, these 2 sets of reference criteria differ, and their accuracy in classifying adiposity has not yet been validated in most countries. Objective: We compared BMI criteria from the IOTF and the CDC with percentage of body fat (%BF) from multisite skinfold thicknesses (SFTs) for identification of overweight in 6 –12-y-old Swiss children. Design: In a representative sample (n ҃ 2431), weight, height, and 4 SFTs were measured. Regression and receiver operating characteristic (ROC) curves were used to evaluate BMI as an indicator of adiposity. Results: BMI and %BF were well correlated (r2 ҃ 0.74), and the areas under the ROC curves for overweight and obesity were 0.956 – 0.992. The sensitivity and specificity of the IOTF and CDC overweight criteria and of the CDC obesity criteria were high. The sensitivity of the IOTF obesity criteria was only 48% and 62% in boys and girls, respectively. Overall, the performance of the CDC criteria was superior. With the use of the CDC criteria, the prevalence of overweight in girls and boys was 19.1% and 20.3%, respectively. Conclusions: BMI is an excellent proxy measure of adiposity in 6 –12-y-old children. In Swiss children, both BMI criteria accurately predict overweight, but the sensitivity of the IOTF obesity criteria is poor. They failed to detect one-half of the children identified as obese on the basis of %BF from SFTs. Am J Clin Nutr 2004;79: 838 – 43. DETECTION OF OVERWEIGHT IN SWISS CHILDREN %BF ⫽ 兵562 ⫺ 4.2关age (y) ⫺ 2兴其/D ⫺ 兵525 ⫺ 4.7关age (y) ⫺ 2兴其 (1) For boys D (g/mL) ⫽ 1.169 ⫺ 0.0788 ⫻ log (sum of 4 SFTs) (2) For girls D (g/mL) ⫽ 1.2063 ⫺ 0.0999 ⫻ log (sum of 4 SFTs) (3) The mean regression coefficients (SEs in parentheses) for prediction of %BF from log (sum of 4 SFTs) with the use of these equations in prepubertal boys and girls are 26.56 (3.00) and 29.85 (3.25), respectively (23). Statistical analysis was performed by using SPLUS 2000 (Insightful, Seattle), EXCEL 97 (Microsoft, Redmond, WA), and PRISM3 (GraphPad, San Diego). Interobserver and intraobserver variations in SFT measurements were expressed as CVs. Analysis of variance and analysis of covariance (ANCOVA) were used to study sex differences. The 85th and 95th percentiles of %BF-for-age were calculated separately for boys and girls by quantile regression (24). A square root transformation of %BF resulted in a near linear age dependency of the percentiles. Overweight and obesity were defined as values above the 85th and 95th percentiles, respectively, for %BF-for-age. BMI was calculated as weight (in kg) divided by height2 (in m). The BMI values of the children were compared with the IOTF reference data (10) and with reference data from the CDC (11). Children with a BMI at or above the age-specific cutoffs were defined as overweight or obese. For the calculation of the prevalence of overweight and obesity, the sample was divided into 3 age groups (6 – 8, 9 –10, and 11–12 y). Prevalence data were expressed as percentages and were compared by using chi-square tests. Because BMI does not follow a Gaussian distribution, a shifted logarithmic transformation, log (x Ҁ 11), was done to make the age-dependent distribution of BMI nearly Gaussian, as judged by its negligible skewness and kurtosis. Regression of BMI on %BF by sex was done to describe their relation. Receiver operating characteristic (ROC) curves were used to assess the performance of BMI in detecting overweight and obesity. Because the distribution of BMI is age dependent, BMI SD scores (BMI-SDS), which were adjusted for age, were used. The reference values necessary to calculate SDS were obtained from the sample itself; after the shifted logarithmic transformation, means and SDs by age were linear for boys and quadratic, with minimal curvature, for girls. The ROC curves for BMI-SDS were constructed by calculating the specificity and sensitivity (percentages) generated by using the percentile cutoffs for the screening indexes. The series of sensitivities were then plotted against the corresponding values of 100 Ҁ specificity. The area under the ROC curve (AUC) was calculated to provide a numerical summary of the indicator’s performance. The SE of the AUC was obtained by bootstrapping (25). An AUC of 0.95 implies that a randomly selected overweight (or obese) child has a BMI-SDS greater than that of a randomly selected normal-weight child 95% of the time (26). The sensitivity and specificity of the IOTF and CDC BMI reference values for overweight and obesity, as defined by the 85th and 95th percentiles of %BF-SDS, were calculated. P values 쏝 0.05 were considered significant. RESULTS At the schools, 3413 children were invited to participate, and 2672 accepted. Of these, 64 were absent on the day of measurement. The overall response rate was 76.4%. Two percent of the subjects participated in the weight and height measurement but declined the SFT measurements. After removing subjects with incomplete data and a small number of subjects aged 욷13 y, a sample of 2431 subjects (1235 girls and 1196 boys) remained. The descriptive characteristics of the sample are shown in Table 1. The interobserver and intraobserver CVs for measurement of SFTs were 3.1% and 1.8%, respectively. The prevalence of overweight and obesity in the sample by age and sex according to the IOTF and CDC BMI reference values is shown in Table 2. There were no significant differences between the sexes in the prevalence of overweight and obesity, although the prevalence of overweight, as assessed on the basis of the IOTF cutoffs, was higher in the girls than in the boys for all age groups. There was no significant effect of age on the prevalence of either overweight or obesity. Downloaded from ajcn.nutrition.org by guest on October 6, 2014 in 250 children in this age group in Switzerland (21). Sixty communities and schools across Switzerland were identified by stratified random selection. Three or 4 classrooms were then randomly selected from each school, and all students from the selected classrooms were invited to participate. The average sample size at each school was 45 students, and the number varied according to the size of the classrooms. Ethical approval for the study was obtained from the Swiss Federal Institute of Technology, Zu¨ rich, Switzerland. Written informed consent was obtained from the school physician, the teachers, and the parents of the children. For the measurements, the subjects removed their shoes, emptied their pockets, and wore light indoor clothing. Height and weight were measured by using standard anthropometric techniques (1). Body weight was measured to the nearest 0.1 kg by using a Tanita digital scale (HD-313; Tanita, Tokyo) calibrated with standard weights. Height was measured to the nearest 0.1 cm by using a pull-down, metal measuring tape (personcheck REF 44 444, Medizintechnik KaWe; Kirchner & Wilhelm, Asperg, Germany). SFTs were measured by 2 trained examiners (CG and CP) using a Harpenden Skinfold Caliper (HSK-BI; British Indicators, West Sussex, United Kingdom) with a constant spring pressure of 10 g/mm2 and a resolution of 0.2 mm. SFTs were measured at the triceps, biceps, subscapular, and suprailiac sites (22). For the triceps, the midpoint of the back of the upper arm between the tips of the olecranal and acromial processes was determined by measuring with the arm flexed at 90°. With the arm hanging freely at the side, the caliper was applied vertically above the olecranon at the marked level. Over the biceps, the SFT was measured at the same level as the triceps, with the arm hanging freely and the palm facing outwards. At the subscapular site, the SFT was picked up just below the inferior angle of the scapula at 45° to the vertical along the natural cleavage lines of the skin. The suprailiac SFT was measured above the iliac crest, just posterior to the midaxillary line and parallel to the cleavage lines of the skin, with the arm lightly held forward. All sites were measured on the right site of the body in duplicate. For each site, 10% of the SFT measurements were repeated by a second examiner to calculate interobserver variation. With the use of mean values from repeated SFT measurements, body density (D) and %BF were calculated according to the following equations from Deurenberg et al (23): 839 840 ZIMMERMANN ET AL TABLE 1 Descriptive characteristics of the national sample of 6 –12-y-old Swiss children1 Age (y) Weight (kg) Height (cm) BMI (kg/m2) Body fat (%) Boys (n ҃ 1196) Girls (n ҃ 1235) 9.80 앐 1.77 34.7 앐 9.7 139.1 앐 11.5 17.6 앐 2.8 17.1 앐 8.3 9.84 앐 1.80 35.0 앐 10.4 138.8 앐 12.4 17.8 앐 2.9 19.3 앐 9.6 1 All values are x 앐 SD. There were no significant differences between the boys and the girls. FIGURE 1. The 85th and 95th percentiles (P85 and P95, respectively) for percentage of body fat (%BF) from the Deurenberg equation, as calculated by quantile regression in a national sample of 6 –12-y-old Swiss boys and girls (n ҃ 2431). DISCUSSION Although measurement of BMI is practical and reproducible, the correlation coefficient between BMI and %BF by DXA or densitometry in children varies between 0.4 and 0.9 according to age, ethnicity, and sex (27, 28). We measured adiposity by using multisite SFTs to judge the performance of BMI as an indicator of overweight in our sample. Studies have shown that %BF values calculated from SFTs have high reproducibility (18) and correlate well with %BF values measured by DXA in children (13, 20). Using ROC curve analysis to compare the accuracy of SFTs and BMI with that of DXA in 10 –15-y-old children, Sardinha et al (20) reported that the AUC for SFTs was equal to or greater than the AUC for BMI. We found a strong and age-independent association between BMI and %BF calculated from SFTs. By regression, 74% of the variability in %BF was explained by BMI in both the boys and the girls. The boys and the girls differed significantly in the slope of TABLE 2 The prevalence of overweight and obesity in a national sample of 6 –12-y-old Swiss children by age and sex according to BMI criteria from the International Obesity Task Force (IOTF) and the US Centers for Disease Control and Prevention (CDC)1 IOTF criteria Age group 6–8 y Boys (n ҃ 450) Girls (n ҃ 446) 9–10 y Boys (n ҃ 381) Girls (n ҃ 398) 11–12 y Boys (n ҃ 365) Girls (n ҃ 391) All Boys (n ҃ 1196) Girls (n ҃ 1235) 1 CDC criteria Overweight Obese Overweight Obese 16.4 앐 1.7 19.7 앐 1.9 4.00 앐 0.93 4.26 앐 0.96 21.8 앐 1.9 20.0 앐 1.9 8.00 앐 1.28 6.73 앐 1.19 19.2 앐 2.0 19.6 앐 2.0 4.46 앐 1.06 3.27 앐 0.89 21.8 앐 2.1 18.8 앐 2.0 8.40 앐 1.42 4.77 앐 1.07 14.0 앐 1.8 17.9 앐 1.9 3.01 앐 0.89 3.58 앐 0.94 16.2 앐 2.1 18.4 앐 2.0 6.08 앐 1.39 6.14 앐 1.21 16.6 앐 1.1 19.1 앐 1.1 3.85 앐 0.56 3.72 앐 0.54 20.3 앐 1.2 19.1 앐 1.1 7.63 앐 0.79 5.91 앐 0.67 All values are percentage 앐 SE. There were no significant differences between the sexes (chi-square test). Downloaded from ajcn.nutrition.org by guest on October 6, 2014 The 85th and 95th percentiles for %BF by age from the Deurenberg equation, as calculated by quantile regression for boys and girls, are shown in Figure 1. The regression of BMI on %BF for boys and for girls is shown in Table 3. The boys and the girls differed significantly in the slope of the regression (P 쏝 0.001, ANCOVA). In the boys, age was not a significant predictor of BMI after %BF was controlled for (P ҃ 0.6, ANCOVA). In the girls, age was a significant predictor of BMI (P ҃ 0.001, ANCOVA), although it enhanced the multiple correlation only minimally, from 0.742 to 0.744. The ROC curves of BMI-SDS for prediction of overweight in the boys and the girls on the basis of the 85th percentile for %BF, as well as the positions on the curves of the CDC and IOTF BMI reference values for overweight, are shown in Figure 2. The ROC curves of BMI-SDS for prediction of obesity in the boys and the girls on the basis of the 95th percentile for %BF, as well as the position on the curves of the CDC and IOTF BMI reference values for obesity, are shown in Figure 3. The areas under the ROC curves of BMI-for-age for prediction of overweight and obesity in the boys and the girls on the basis of the 85th and 95th percentiles of %BF, respectively, are shown in Table 4. The sensitivity and specificity of the IOTF and CDC reference cutoffs for overweight and obesity in the boys and the girls are shown in Table 5. 841 DETECTION OF OVERWEIGHT IN SWISS CHILDREN TABLE 3 Regression of log (BMI Ҁ 11) on percentage of body fat for boys and for girls in a national sample of 6 –12-y-old Swiss children1 Boys Intercept Slope Residual SE R2 P Girls 2 1.148 (0.013) 0.039 (0.001) 0.196 0.74 쏝 0.0001 1.136 (0.013) 0.036 (0.001)3 0.204 0.74 쏝 0.0001 n ҃ 2431. Regression coefficient; SE in parentheses (all such values). 3 Significantly different from the boys, P 쏝 0.001 (analysis of covariance). 1 2 FIGURE 3. The receiver operating characteristic (ROC) curves of BMI SD scores for prediction of obesity in boys and girls on the basis of the 95th percentile of percentage of body fat calculated from skinfold thicknesses in a national sample of 6 –12-y-old Swiss children (n ҃ 2431). The position of the BMI reference values for obesity from the US Centers for Disease Control and Prevention (CDC) and the International Obesity Task Force (IOTF) on the ROC curves is shown, and the area under the curve (AUC; 앐SE) is indicated for the boys and the girls. ROC curve (Figure 2). The CDC reference value for obesity had a higher sensitivity and specificity than did the IOTF reference. The sensitivity of the IOTF reference value for obesity was poor, and the false negative rate was 38% for the boys and 52% for the girls. This was reflected in the better position of the CDC reference values on the ROC curve for obesity (Figure 3). Reilly et al (7) compared the sensitivity and specificity of the 1990 UK reference values with those of the IOTF reference values for detecting adiposity (쏜95th percentile for %BF) measured by bioelectrical impedance in 7-y-old children in the United Kingdom. The sensitivity of the IOTF reference values was low and differed significantly between boys (46%) and girls (72%). Flegal et al (8) used the new CDC and IOTF criteria to compare the prevalence of overweight and obesity in 6 –11-y-old US children in the NHANES III (1988 –1994). Compared with the CDC criteria, the IOTF criteria gave lower prevalence estimates for overweight and obesity in boys and for obesity in girls. The differences in prevalence were not systematic, and some were large, up to 10% for overweight and up to 50% for obesity. Kain et al (9) reported that in 6-y-old Chilean children, the CDC and IOTF criteria generated comparable prevalence estimates for overTABLE 4 Areas under the receiver operating characteristic curves of BMI SD scores for prediction of overweight and obesity in boys and girls on the basis of the 85th and 95th percentiles of percentage of body fat (%BF), respectively, in a national sample of 6 –12-y-old Swiss children1 Overweight Age group FIGURE 2. The receiver operating characteristic (ROC) curves of BMI SD scores for prediction of overweight in boys and girls on the basis of the 85th percentile for percentage of body fat calculated from skinfold thicknesses in a national sample of 6 –12-y-old Swiss children (n ҃ 2431). The position of the BMI reference values for overweight from the US Centers for Disease Control and Prevention (CDC) and the International Obesity Task Force (IOTF) on the ROC curves is shown, and the area under the curve (AUC; 앐SE) is indicated for the boys and the girls. 6–8 y 9–10 y 11–12 y Total 1 2 Obesity Boys Girls Boys Girls 0.97 앐 0.02 0.96 앐 0.01 0.97 앐 0.01 0.97 앐 0.01 0.96 앐 0.01 0.94 앐 0.01 0.96 앐 0.01 0.96 앐 0.01 0.99 앐 0.003 0.99 앐 0.003 0.99 앐 0.003 0.99 앐 0.02 0.98 앐 0.01 0.95 앐 0.01 0.98 앐 0.01 0.97 앐 0.012 All values are x 앐 SE; n ҃ 2431. Significantly different from the boys, P 쏝 0.001. Downloaded from ajcn.nutrition.org by guest on October 6, 2014 the regression (P 쏝 0.001). However, this difference appeared to be physiologically irrelevant because the use of a common slope of 0.374 for the boys and the girls in the regression equation left the residual SE practically unchanged at 0.20 (Table 3). The areas under the ROC curves for the girls and the boys were 0.956 and 0.967, respectively, for overweight (NS) and 0.970 and 0.992, respectively, for obesity (P 쏝 0.001; Table 4). This suggests that the accuracy of BMI in predicting adiposity was greater in the boys than in the girls. In 6 –11-y-old US children in the third National Health and Nutrition Examination Survey (NHANES III), the correlation coefficients between BMI-for-age and the average of the triceps and subscapular SFTs in boys and girls were 0.88 and 0.85, respectively (29). Mei et al (29) determined the performance of area under the ROC curve of BMI-for-age as defined by the average of the triceps and subscapular SFTs at the cutoffs for overweight (쏜85th percentile) from the NHANES III. For children aged 6 –11 y, the mean AUC was 0.973, which is similar to the value obtained in the present study. In our sample, the CDC and IOTF reference values for overweight showed fairly high sensitivity and high specificity in both sexes (Table 5). The CDC and IOTF cutoffs for the boys and the girls were close together and were well placed on the bend of the 842 ZIMMERMANN ET AL TABLE 5 Sensitivity and specificity of the age- and sex-specific BMI reference values for overweight and obesity from the International Obesity Task Force (IOTF) and the US Centers for Disease Control and Prevention (CDC) in a national sample of 6 –12-y-old Swiss children1 Overweight Obesity Boys Age group 6–8 y IOTF CDC 9–10 y IOTF CDC 11–12 y IOTF CDC Total IOTF CDC 1 Sensitivity Girls Specificity Sensitivity 83.6 93.4 94.1 89.5 78.6 81.4 Boys Specificity Sensitivity 91.7 91.7 91.5 91.2 94.2 91.6 76.4 75.0 72.9 79.2 95.0 94.0 78.8 85.1 94.4 91.5 Girls Specificity Sensitivity 68.0 100 99.1 96.3 68.4 84.2 98.6 96.7 92.9 93.6 61.2 91.3 99.4 96.9 30.0 54.0 98.1 97.6 84.9 84.9 92.6 92.6 60.7 76.5 100 97.7 47.6 59.1 98.9 97.6 83.8 82.8 92.3 92.4 62.4 91.4 99.5 96.9 48.3 67.9 98.6 97.3 % % % Specificity % n ҃ 2431. We thank the teachers and children at the participating schools for their cooperation and P Ballmer (Canton Hospital Winterthur, Switzerland) for technical advice. Each of the authors made substantial contributions to the study design, data collection, data analyses, and the writing or editing of the manuscript. None of the authors had any personal or financial interests, including advi- sory board affiliations, in the companies or organizations sponsoring this research. REFERENCES 1. World Health Organization. Physical status: the use and interpretation of anthropometry. Report of a WHO Expert Committee. World Health Organ Tech Rep Ser 1995;854:1– 452. 2. Garrow JS, Webster JD. Quetelet’s index (W/H2) as a measure of fatness. Int J Obes Relat Metab Disord 1985;9:147–53. 3. Dietz WH, Robinson TN. Use of the body mass index as a measure of overweight in children and adolescents. J Pediatr 1998;132:191–3. 4. Barlow SE, Dietz WH. Obesity evaluation and treatment: Expert Committee recommendations. The Maternal and Child Health Bureau, Health Resources and Services Administration and the Department of Health and Human Services. Pediatrics [serial online] 1998;102:e29. Internet: http://pediatrics.aappublications.org/cgi/content/full/102/3/e29 (accessed 15 October 2003). 5. Cole TJ, Bellizzi MC, Flegal KM, Dietz WH. Establishing a standard definition for child overweight and obesity worldwide: international survey. BMJ 2000;320:1240 –3. 6. Kuczmarski RJ, Ogden CL, Grummer-Strawn LM, et al. CDC growth charts: United States. Adv Data 2000;8:1–27. 7. Reilly JJ, Dorosty AR, Emmett PM, and the ALSPAC Study Team. Identification of the obese child: adequacy of the body mass index for clinical practice and epidemiology. Int J Obes Relat Metab Disord 2000; 24:1623–7. 8. Flegal KM, Ogden CL, Wei R, Kuczmarski RL, Johnson CL. Prevalence of overweight in US children: comparison of US growth charts from the Centers for Disease Control and Prevention with other reference values for body mass index. Am J Clin Nutr 2001;73:1086 –93. 9. Kain J, Uauy R, Vio F, Albala C. Trends in overweight and obesity prevalence in Chilean children: comparison of three definitions. Eur J Clin Nutr 2002;56:200 – 4. 10. Reilly JJ. Assessment of childhood obesity: national reference data or international approach? Obes Res 2002;10:838 – 40. 11. Fomon SJ, Haschke F, Ziegler EE, Nelson SE. Body composition of reference children from birth to age 10 years. Am J Clin Nutr 1982;35: 1169 –75. 12. Goran MI, Toth MJ, Poehlman ET. Assessment of research-based body composition techniques in healthy elderly men and women using the 4-compartment model as a criterion method. Int J Obes Relat Metab Disord 1998;22:135– 42. 13. Gutin B, Litaker M, Islam S, Manos T, Smith C, Treiber F. Bodycomposition measurement in 9 –11-y-old children by dual-energy X-ray absorptiometry, skinfold-thickness measurements, and bioimpedance analysis. Am J Clin Nutr 1996;63:287–92. Downloaded from ajcn.nutrition.org by guest on October 6, 2014 weight, but the IOTF reference value for obesity generated an 앒50% lower prevalence estimate than did the CDC reference value. The CDC and IOTF BMI criteria were generated by using different data sets and smoothing methods, and their approaches to setting cutoffs were different (8). The CDC criteria were based on the BMI distribution of representative samples of US children (6). The IOTF criteria, on the other hand, were not related to a reference population distribution; they were instead extrapolated from adult BMI cutoffs for overweight and obesity and are based on the assumption that children with those BMI values have inherent health risks (5). For ages 6 –12 y, the IOTF BMI cutoffs are generally higher than are the CDC reference values. For boys, the mean differences between the CDC and IOTF reference values for overweight and obesity are 앒0.5 and 1.5–2.0 BMI units, respectively. For girls, the 2 sets of reference values are similar for overweight, but the IOTF cutoffs are 앒1.0 BMI unit higher (8). These differences explain both the lower prevalence estimate that was obtained in our sample with the IOTF reference values for overweight in boys than with the CDC reference values and the sharply lower prevalence estimate for obesity in boys and girls that was obtained with the IOTF reference values (Table 2). Our data indicate that BMI is an excellent proxy measure of adiposity in 6 –12-y-old Swiss children. Although both the IOTF and CDC age- and sex-specific BMI criteria accurately predict overweight, the IOTF criteria for obesity are insensitive and failed to identify 40 –50% of obese children in our sample. Overall, the performance of the CDC reference values was superior, and they provided more accurate estimates of adiposity. Although the IOTF reference values have been proposed for international use, before they are widely adopted to detect childhood adiposity, their validity should first be tested in other countries around the world. DETECTION OF OVERWEIGHT IN SWISS CHILDREN 14. Goran MI, Driscoll P, Johnson R, Nagy TR, Hunter G. Cross-calibration of body-composition techniques against dual-energy X-ray absorptiometry in young children. Am J Clin Nutr 1996;63:299 –305. 15. Himes JH. Anthropometric assessment of nutritional status. New York: Wiley-Liss, Inc, 1991. 16. Brook CGD. Determination of body composition of children from skinfold measurements. Arch Dis Child 1971;46:182– 4. 17. Roche AF, Sievogel RM, Chumlea WC, Webb P. Grading body fatness from limited anthropometric data. Am J Clin Nutr 1981;34:2831– 8. 18. Schaefer F, Georgi M, Zieger A, Scha¨ rer K. Usefulness of bioelectrical impedance and skinfold measurements in predicting fat-free mass derived from total body potassium in children. Pediatr Res 1994;35:617–24. 19. Hammond J, Rona RJ, Chinn S. Estimation in community surveys of total body fat of children using bioelectrical impedance or skinfold measurements. Eur J Clin Nutr 1994;48:164 –71. 20. Sardinha LB, Going SB, Teixeira PJ, Lohman TG. Receiver operating characteristic analysis of body mass index, triceps skinfold thickness, and arm girth for obesity screening in children and adolescents. Am J Clin Nutr 1999;70:1090 –5. 21. Federal Department of Statistics. Statistical yearbook of Switzerland. Zu¨ rich, Switzerland: Verlag NZZ, 2000. 843 22. Gibson RS. Nutritional assessment: a laboratory manual. Oxford, United Kingdom: Oxford University Press, 1993:79 –100. 23. Deurenberg P, Pieters JJ, Hautvast JG. The assessment of the body fat percentage by skinfold thickness measurements in childhood and young adolescence. Br J Nutr 1990;63:293–303. 24. Koenker R, Bassett G. Regression quantiles. Econometrica 1978;46:33–50. 25. Davison AC, Hinkley DV. Bootstrap methods and their application. Cambridge, United Kingdom: Cambridge University Press, 1997. 26. Zweig MH, Campbell G. Receiver operating characteristic plots: a fundamental evaluation tool in clinical medicine. Clin Chem 1993;39: 561–77. 27. Dietz WH, Bellizzi MC. Introduction: the use of body mass index to assess obesity in children. Am J Clin Nutr 1999;70(suppl):123S–5S. 28. Pietrobelli A, Faith MS, Allison DB, Gallagher D, Chiumello G, Heymsfield SB. Body mass index as a measure of adiposity among children and adolescents: a validation study. J Pediatr 1998;132:204 –10. 29. Mei Z, Grummer-Strawn LM, Pietrobelli A, Goulding A, Goran MI, Dietz WH. Validity of body mass index compared with other bodycomposition screening indexes for the assessment of body fatness in children and adolescents. Am J Clin Nutr. 2002;75:978 – 85. Downloaded from ajcn.nutrition.org by guest on October 6, 2014









© Copyright 2026