
ICD Coding Newsletter June 2001 Distribution List
ICD Coding Newsletter (incorporating Special Edition features) June 2001 Distribution List Health Information Manager/s (HIMS) Clinical Coders Information Technology (IT) Interested Others ..................................................................................... ..................................................................................... ..................................................................................... The ICD Coding Newsletter supports the clinical coding function performed in Victoria by Health Information Managers and Clinical Coders, by providing relevant information for these professionals and their associates. The newsletter, prepared by the Victorian ICD Coding Committee in conjunction with the Department of Human Services, seeks to: • Ensure the standardisation of coding practice across the state • Provide a forum for resolution of coding queries • Address topical coding education issues • Inform on national and state coding issues from the Victorian perspective. The scope of the newsletter includes coding feature articles, selected coding queries and responses, and various information updates including feedback on the quality and uses of coded data (as reported to the Victorian Admitted Episodes Dataset). Should you have any queries or comments regarding the ICD Coding Newsletter, contact Nicolette Thein: Telephone 9616 8141 Fax 9616 7629 Email [email protected] Website www.dhs.vic.gov.au/ahs/hdss Notification of change of address or requests regarding the mailing list may be directed to any of the above contacts. An electronic coding query form can be completed at: www.dhs.vic.gov.au/ahs/hdss/icdquery.htm May be reproduced ICD Coding Newsletter – June 2001 i Contents Coding Features...................................................................................................... 1 Additional Diagnoses – Queries and Responses ................................................................... 1 Minor Trauma Coding............................................................................................................... 4 ACS 0031 Anaesthesia ............................................................................................................... 7 HIMAA Education Seminar................................................................................. 9 List of Selected ICD-10-AM Coding Queries................................................. 10 Coding Corkboard ............................................................................................... 37 Coding Newsletter Mailing List............................................................................................. 37 Health Funds and Australian Coding Standards ................................................................ 38 Websites..................................................................................................................................... 39 Information Updates ........................................................................................... 40 Data Quality .............................................................................................................................. 40 Audits of VAED Data .......................................................................................................... 40 A review of Newborns – Qualified but no condition coded .......................................... 42 Dual Coding Study Results................................................................................................. 47 Reporting To The VAED ......................................................................................................... 49 AR-DRG Modifications (2001-2002)................................................................................... 49 VAED Schedule Requirements 2001–2002........................................................................ 52 ICD-10-AM Library File for use in Victoria – 1.7.2001 .................................................... 56 NCCH Language of Health conference 2001 ........................................................................... 60 Coding Standards Advisory Committee............................................................................... 61 Coding Calendar of Events ................................................................................ 63 Victorian ICD Coding Committee.................................................................... 64 Member Profile – Evelyn Robinson ....................................................................................... 64 Members as at 1 June 2001 ...................................................................................................... 66 Next Meetings........................................................................................................................... 66 On a Lighter Note ................................................................................................ 67 Alphabetic Index to Victorian ICD-10-AM Coding Advice: July 1999 – June 2001 ................................................................................................................ 68 Abbreviations ....................................................................................................... 79 May be reproduced ICD Coding Newsletter – June 2001 ii Coding Features Additional Diagnoses – Queries and Responses The following three queries were omitted from publication in the previous Newsletter awaiting finalisation by the Victorian Coding Committee. A complete list of queries answered via the DHS ‘Additional Diagnoses Help Desk’ facility can also be accessed at: www.dhs.vic.gov.au/ahs/hdss/clincode.htm Query 10 - Neonates There are often conditions documented on the Newborn Examination record, such as birth traumas, including cephalhaematomas due to vacuum extraction or injuries from forcep blades, birthmarks; and other abnormalities such as talipes, large for dates, etc. If these are observations alone, that is no specific care is instituted, should they be coded? Answer Additional Assign Code Condition (Yes/No) Conditions Yes Reason for assigning/not assigning code The Additional Diagnosis standard does not documented on the deal very well with conditions noted on the Newborn Newborn Examination record, and similar Examination documents in newborn records. record, such as birth trauma, However, it is the opinion of the Victorian birthmarks, other ICD Coding Committee that neonatal abnormalities. conditions, such as congenital anomalies and effects of birth trauma, are all actively evaluated during the birth episode, and that they should therefore be coded. This instruction applies to the birth episode only (for newborns admitted at birth or during the mother’s delivery episode of care). May be reproduced ICD Coding Newsletter – June 2001 1 Query 13 – Histology Findings Patient admitted for total abdominal hysterectomy and bilateral salpingooophorectomy for endometrial hyperplasia due to Tamoxifen. Histology shows: endometrial hyperplasia, small endometrial leiomyomata, low grade chronic endometritis, atrophic ovaries, focal mild adenofibromatous change on surface of left ovary. Obviously the endometrial hyperplasia will be coded. Should the other findings be coded? Answer Additional Condition Assign Code Reason for assigning/not assigning code (Yes/No) Endometrial Yes hyperplasia As the patient is admitted for treatment of endometrial hyperplasia, this finding supports the admission diagnosis and would be coded as principal diagnosis Other findings on Yes histology. • Even though ACS 0010, Abnormal findings, indicates that these conditions should not be Small coded unless their significance is indicated by endometrial the treating doctor and they meet ACS 0002, leiomyomata it is the opinion of the Victorian ICD Coding Committee that the conditions noted on • Low grade histology should be coded. chronic endometritis Histology results are not well dealt with by ACS 0010 as they usually provide definitive • Atrophic information that does not require clinical ovaries interpretation (although they may require clinical evaluation). That is, these conditions • Focal mild either exist or they don’t, as opposed to a adenofibroma- microbiology finding of an organism that tous change on may or may not be indicative of an infection. surface of left ovary Although this example is quite specific, it is more common for patients to present with a general symptom, and in these cases all the 2 ICD Coding Newsletter - June 2001 May be reproduced findings may be contributory factors in the patient’s condition and would all be actively evaluated in respect to the patients final diagnosis (this evaluation may occur on review of the histopathology during or after the patient’s admission). In this particular example, although the reason for admission is the endometrial hyperplasia and this is supported by the histology result, it is felt that the other conditions would be actively evaluated in the context of the patient’s admission and determination of the final diagnosis. The Department of Human Services, via the Victorian ICD Committee will work with the NCCH to get clarification of ACS 0010. Query 16 - Obstetrics In relation to obstetric cases and the associated conditions standard do we code placental abnormalities? For example, placental infarct. Answer Additional Assign Code Condition (Yes/No) Placental anomalies Yes • Reason for assigning/not assigning code The Additional Diagnosis standard does not placental deal very well with conditions noted on the infarct delivery summary form, and similar • knot in cord documents in obstetric records. • true knot However, it is the opinion of the Victorian ICD Coding Committee that these conditions are ‘actively evaluated’ during this episode of care, and that they should therefore be coded. May be reproduced ICD Coding Newsletter – June 2001 3 Minor Trauma Coding Kylie Holcombe, St Vincent’s Hospital These notes have been compiled to assist with the coding of minor trauma, for which there are no actual documented injuries. It was identified in the 1999–2000 round of the VAED audit that there were some problems in coding these types of cases and that the correction of coding often resulted in a DRG change. When a patient presents to Accident and Emergency due to trauma and there are no physical signs of injury such as lacerations, contusions or fractures, the patient may still have signs of having suffered an injury, such as presence of pain at the injured site. Coders should apply the following guidelines: a) Where pain is documented as due to an external cause but no specific injury is documented, code as injury NOS of the site and the External Cause. b) Where a patient presents with pain but no external cause relationship is documented, code the pain only. Do not code an external cause code, as it is not related to the pain. It is also very important to remember in what way codes may be used for research and statistical purposes. If a clinician wished to do research on chest trauma it would make sense to pull out all the cases that have an injury code relating to the chest, but not necessarily to look at chest pain cases as well. Many statistics are also drawn from the codes that are assigned - pain codes would not interest those conducting research on injury or trauma; however, even an unspecified injury code would enable more accurate injury and trauma statistics. The following scenarios have been provided to assist assignment of appropriate codes for minor trauma admissions. 4 ICD Coding Newsletter - June 2001 May be reproduced SCENARIO 1 A ninety year old patient is sent into hospital from her nursing home having fallen onto her left side from her bed whilst resting. The patient is complaining of severe pain in her left hip and is unable to weight bear on this leg. The hip is x-rayed and no fracture is detected. The patient also has a small graze on her left elbow that is cleaned and dressed. The patient is returned to the nursing home later in the afternoon. This patient’s main problem is the fact that she cannot weight bear, and the hip pain. From the notes provided it is clear that the patient has suffered a trauma. It would not make sense to code hip pain as M25.55 indicates a chronic or spontaneous hip pain. To capture the correct ‘picture’ of this patient’s trauma, it should be coded as follows: S79.9 Unspecified injury of hip and thigh S50.81 Abrasion of forearm W06 Fall involving bed (Injury, - hip) Y92.22 Health service area Y93.4 While resting, sleeping, eating or engaging in other vital activities SCENARIO 2 A twenty year old man, who is the driver in a motor vehicle accident involving a collision with a bus, is brought into Accident and Emergency complaining of chest pain. The chest is tender on palpation where he hit the steering wheel, but the patient is having no difficulty breathing and his chest x-ray reveals that no ribs have been fractured. The man is given Panadol for the pain and sent home. As in Scenario One, the patient has pain at the site of impact and therefore has suffered an injury. If chest pain is coded, it would give the impression of a spontaneous or chronic problem. Although additional external cause codes would indicate the cause of the pain, the patient has suffered a trauma which should be reflected in the coding: S29.9 Unspecified injury of thorax V44.5 Driver injured in collision with heavy transport vehicle or bus Y92.4 Street and highway Y93.9 Unspecified activity May be reproduced ICD Coding Newsletter – June 2001 5 SCENARIO 3 An eighteen year old female who was a passenger in a two-car collision is brought into Accident and Emergency. She is visibly distressed but is conscious and not complaining of any pain or injury. Examination reveals no injuries. In this scenario the patient is experiencing no pain and has no other injury. Whilst this case would probably not meet the criteria for admission, if the admission were clinically justified, it would be coded as: Z04.1 Examination and observation following transport accident V43.6 Passenger injured in collision with car, pick-up truck or van Y92.4 Street and highway Y93.9 Unspecified activity SCENARIO 4 A fifty-five year old male presents to Accident and Emergency with a severe headache. The patient claims that one week ago he fell off a ladder and struck his head on a post. The patient has an old contusion on his scalp but a brain CT reveals no internal injury. The patient is given pain relief and three hours later states he had no headache at all. He is discharged home. In this scenario there is no evidence that the headache is related to the injury incurred one week before. If the headache had been present since the injury this may be different, but would need to be clarified with the treating clinician. In this instance the headache would be coded, but not the trauma, as follows: R51 Headache 56001-00 [1952] CT brain without contrast 6 ICD Coding Newsletter - June 2001 May be reproduced SCENARIO 5 A twenty-two year old male presents with a painful ankle four days after twisting the ankle in a basketball game. Examination and x-ray reveal no apparent damage. The clinician documents ankle pain secondary to basketball injury. In this scenario the clinician has related the ankle pain to the trauma, therefore it should be coded as a traumatic injury. It has not been specified as a sprain so it should be coded as an ankle injury NOS: S99.9 Unspecified injury of ankle and foot X50 Overexertion and strenuous or repetitive movements Y92.3 Sports and athletics area Y93.05 Basketball The assignment of codes should always tell the story. When you have finished coding a trauma case, look at the codes and determine if you can tell what happened to the patient by the codes alone. As per the Clinical Coders’ Creed you will ‘..need to make decisions which are based on (your) experience and common sense’. ACS 0031 Anaesthesia Anaesthetic Procedure Codes The NCCH intends to include a simplified range of anaesthetic procedure codes in the Third Edition of ICD-10-AM. It is recognised that unwarranted time has been spent by coders searching for specific anaesthetic information and that coders have gone to great lengths to comply with ACS 0031. The Department of Human Services recommends that the default codes from ACS 0031 Anaesthesia be used for the coding of all anaesthetics for 2001-2002 separations, in preparation for the reduced range of anaesthetic codes that will be available in the Third Edition. This means coders only need to identify the type of anaesthetic (e.g. GA, epidural, caudal, spinal or sedation), rather than search for detail of drugs or gases used, for episodes from 1 July 2001 Please refer to June 2001 Coding Matters for background information to these forthcoming changes. May be reproduced ICD Coding Newsletter – June 2001 7 Therefore, the following default codes are to be used: General anaesthesia combined with major regional anaesthesia (epidural, caudal or spinal) 92502-03 [1910] General anaesthesia combined with major regional anaesthesia General anaesthesia 92502-02 [1910] Intravenous and inhalational general anaesthesia Major regional 18209-05 [32] Epidural injection of local anaesthetic, combined preoperative, intraoperative and postoperative 18209-02 [34] Caudal injection of local anaesthetic, combined preoperative, intraoperative and postoperative 18209-08 [36] Spinal injection of local anaesthetic, combined preoperative, intraoperative and postoperative Note: the advice to default to the assignment of injection, was previously advised in Victorian ICD Coding Newsletter, November 2000, page 16. Sedation 92503-00 [1911] Intravenous sedation, anaesthetist controlled Anaesthesia and sedation for dental procedure For sedation 97942-00 [487] Intravenous sedation for dental procedure For general anaesthesia 97949-00 [487] General anaesthesia for dental procedure Anaesthesia during labour 90486-02 [1333] 1 8 Epidural injection of other therapeutic substance during labour 1 Extracted from NCCH ICD-10-AM, July 2000, General Standards for Procedures. ICD Coding Newsletter - June 2001 May be reproduced HIMAA Education Seminar Evelyn Robinson, Peninsula Health The HIMAA Victorian Branch Education Sub-Committee held a very successful education session on 23 March 2001 at The Centre, Ivanhoe, titled ‘Working with Coding’. The first half of the program was a Coding Workshop conducted by Jennie Shepheard that focused on Associated Conditions, Post-operative Complications and Diabetes. Participants were sent the workbooks in advance, so they could come prepared with their answers for discussion. This session was very helpful as it reinforced a lot of the difficult areas when applying these Standards. The afternoon session included a panel discussion with speakers from various hospitals, discussing motivating, auditing and training in a Coding Service. Ruth Rundell (Geelong Hospital), Patricia Savino (Northern Hospital), Andrea Groom (Southern Health) and Kathy Wilton (Royal Children’s Hospital) each described the Coding Service at their hospital. This informative session gave us many ideas on Coding Allocation and EFT, internal auditing methods, education of coders and training of new coding staff. Andrea Groom gave us a brief taste of the ‘Clever Coders’ Cup’ that is held each month at Southern Health. Participants were split into teams and quiz questions posed on various coding topics, such as the ‘10-AM Commandments’ section of ‘Coding Matters’ and the Australian Coding Standards. Other speakers presented examples of the uses of coding and casemix information, including Adverse Events, Injury Surveillance and Clinical Costing. Dr Mark Stokes, Director of Victorian Injury Surveillance Systems explained the use of Victorian Emergency Minimum Dataset data to assist in epidemiological research for injury prevention. Linda Butcher from the Mercy Hospital for Women discussed clinical costing and revenue model analysis using ICD-10-AM data. This education seminar proved very valuable for those Health Information Managers working in the coding environment and we look forward to future events. May be reproduced ICD Coding Newsletter – June 2001 9 List of Selected ICD-10-AM Coding Queries The ICD Coding Committee is an advisory body to Victorian clinical coders and the Department of Human Services. The Committee does not have the authority to establish coding standards but offers advice, based on the combined knowledge and experience of the members and/or the NCCH, in response to individual coding queries. The Committee’s advice printed in this section of the newsletter can be adopted immediately unless an introduction date is stated. The implementation of this guidance is advisable as it sets a precedent for good coding practice. Unless otherwise stated, there is no expectation that coders should go back to similar episodes already coded differently and change the coding. It is acknowledged that this might result in a year’s data containing episodes coded in a non-standard way. #1622 ACS 1002 Asthma................................................................................ 12 #1636 Colonoscopy: Investigation or finding? ......................................... 13 #1638 Low birth weight................................................................................. 14 #1641 Retained products of conception ..................................................... 16 #1642 Post-infarction angina ........................................................................ 17 #1644 Mechanical complication of ventricular shunt ............................. 17 #1648 Chemotherapy & device loading ..................................................... 18 #1650 Post-procedural complications ......................................................... 18 #1651 Laparoscopic cholecystectomy to open cholecystectomy with exploration of CBD ............................................................................. 20 #1654 Autologous chondrocyte implantation (ACI)................................ 21 #1658 Smoking related COPD ..................................................................... 22 #1659 ACS 0226 Prostatic cancer.................................................................. 23 #1661 Principal diagnosis in obstetrics ...................................................... 24 #1662 ACS 2103 Admission for Convalescence/ Aftercare..................... 25 #1663 Palliative Care...................................................................................... 25 #1664 Musculoskeletal chest pain............................................................... 27 #1665 Anaesthetic procedures...................................................................... 27 #1669 External cause code - scooters ........................................................... 28 10 ICD Coding Newsletter - June 2001 May be reproduced #1671 Osseous metaplasia and Solar lentigo.............................................29 #1676 Follow-up gastroscopy........................................................................30 #1677 Grouping of laparoscopy codes ........................................................30 #1680 Low K+...................................................................................................32 #1682 Underlying condition .........................................................................33 #1685 Ethanol injection..................................................................................33 #1689 ACS 0012 suspected condition (perforation)..................................34 #1691 ACS 0909 Additional procedures performed in conjunction with CABGs ...................................................................................................35 #1693 Bilateral maxilla and mandible osteotomies with internal fixation ...................................................................................................36 May be reproduced ICD Coding Newsletter – June 2001 11 #1622 ACS 1002 Asthma ICD-10-AM 1st Edition had a statement within ACS 1002 Asthma - ‘When asthma and bronchitis are documented for one episode of care, assign only the code for asthma’. There is no such statement in the 2nd Edition. Case scenario Principal diagnosis – 59 year old male admitted with acute bronchitis – infective cause. Additional conditions – patient also has mild asthma. Treated with antibiotics and Ventolin. Does the above statement still apply? There is no entry for ‘Bronchitis – with asthma’. There is an entry for ‘Bronchitis – asthmatic’, but this is not the diagnosis supplied, is it the same condition as a patient with bronchitis and asthma (the dictionary does not seem to help)? This patient has ‘acute bronchitis and asthma’. There is no further breakdown under ‘Bronchitis – acute, asthmatic’ or ‘with asthma’. The code for acute bronchitis: Acute bronchitis J20 has no exclusion notes for asthma. The index entry ‘Asthma – bronchitis’ takes us to: J45.9 Asthma, unspecified. Chronic asthma and chronic bronchitis seem well covered by ACS 1008 Chronic Obstructive Pulmonary Disease (COPD), but I would like some advice on the coding of ‘Bronchitis NOS with asthma’ and ‘Bronchitis – acute with asthma’. Do you code it to bronchitis or asthma? NCCH Response: The statement ‘When asthma and bronchitis are documented for one episode of care, assign only the code for asthma’ has been removed in the second edition due to problems with interpretation. In the case cited assign J20.x Acute Bronchitis as the principal diagnosis and J45.x Asthma as an additional diagnosis. If a causative organism is documented, this should also be coded. If a patient has both asthma and bronchitis then both the conditions should be coded. For example a patient with asthma may get viral bronchitis. The index entry ‘Bronchitis, asthmatic’ will be reviewed for the third edition of ICD-10-AM. 12 ICD Coding Newsletter - June 2001 May be reproduced #1636 Colonoscopy: Investigation or finding? Patient admitted for colonoscopy for investigation of anaemia. Colonoscopy found adenocarcinoma of the colon (sigmoid). What should be the principal diagnosis: anaemia or cancer? If the cancer should be the principal diagnosis, then can you use: D63.0 Anaemia in neoplastic disease instead of D64.9 Anaemia, unspecified Please advise which of the following coding options would be assigned, or alternatives if appropriate. Option 1: C18.7 Malignant neoplasm of colon, sigmoid colon M8140/3 Adenocarcinoma NOS D63.0 Anaemia in neoplastic disease 32090-01 [911] Fibreoptic colonoscopy to caecum with biopsy 92503-00 [1911] Intravenous sedation, anaesthetist controlled Option 2: D64.9 Anaemia, unspecified C18.7 Malignant neoplasm of colon, sigmoid colon M8140/3 Adenocarcinoma NOS 32090-01 [911] Fibreoptic colonoscopy to caecum with biopsy 92503-00 [1911] Intravenous sedation, anaesthetist controlled May be reproduced ICD Coding Newsletter – June 2001 13 Coding Matters Volume 6, Number 1, June 1999, page 13, stated that when a patient has both anaemia and a neoplasm, a cause and effect does not need to be documented; the words ‘in’, ‘with’ or ‘due to’ neoplastic disease are sufficient in order to assign: D63.0* Anaemia in neoplastic disease Because this is an asterisk code, the underlying cause (dagger code) is the principal diagnosis as in your Case 1. #1638 Low birth weight Premature male baby delivered at 31 weeks gestation, weight 940gms; small for gestational age (SGA) due to placental insufficiency. Coded as: P07.3 Other preterm infants P05.1 Small for gestational age P02.2 Fetus and newborn affected by other and unspecified morphological and functional abnormalities of placenta. Should code: P07.1 Other low birth weight be coded as well as small for gestational age? Noting the exclusion note under: Disorders related to short gestation and low birth weight, P07 NEC [Excludes: low birth weight due to slow fetal growth and fetal malnutrition (P05.-)], only P05.1 Small for gestational age is assigned. Does ACS 0033 Conventions Used in the Tabular List of Diseases, Volume 5 page 15, Type 2 Exclusion apply to this case? 14 ICD Coding Newsletter - June 2001 May be reproduced There are various permutations of prematurity and low birth weight: a baby could be one or the other or both. Therefore, if both were relevant, two codes would be used, selecting one from each of the following groups: P07.2 Extreme immaturity OR P07.3 Other preterm infants and P07.0 Extremely low birth weight OR P07.1 Other low birth weight OR P05.- Slow fetal growth and fetal malnutrition In the case given, the two appropriate codes are: P07.3 Other preterm infants P05.1 Small for gestational age Because the baby’s low weight problem is adequately indicated by P05.1, there would be no reason to add P07.1 (no additional information provided by it). Because the cause and effect have been documented, it would also correct to add: P02.2 Fetus and newborn affected by other and unspecified morphological and functional abnormalities of placenta May be reproduced ICD Coding Newsletter – June 2001 15 #1641 Retained products of conception Patient admitted in a previous episode with diagnosis of ‘Missed Abortion’ and underwent ’Suction Curettage’. Two weeks later, the patient was admitted with continuous PV bleeding, diagnosis was ‘Retained products of conception (RPOC)’ and underwent a D & C. Histopathology revealed RPOC. We have coded as follows: O04.1 Medical abortion, incomplete, complicated by delayed or excessive haemorrhage O09.1 5-13 completed weeks 35643-00 [1267] Evacuation of contents of gravid uterus 92502-00 [1910] Intravenous general anaesthesia ACS 1544, page184 tells us to code as ‘a complication of a current, incomplete abortion (O03-O06 with a fourth character of .0-.4)’. We are unsure which of these codes to use: O03.1 Spontaneous abortion, incomplete, complicated by delayed or excessive haemorrhage O04.1 Medical abortion, incomplete, complicated by delayed or excessive haemorrhage We rejected the following code because of the Exclusion note under it (excludes: retained products of conception O03-O06): O08 Complications following abortion and ectopic and molar pregnancy As the patient is still suffering from a ‘missed abortion’ (and not a complication of abortion), the principal diagnosis should reflect the original episode’s diagnosis: O02.1 Missed abortion It would be useful if ACS 1544 Complications following Abortion and Ectopic and Molar Pregnancy also covered coding of missed abortions. The Victorian ICD Coding Committee has sent a request to the NCCH that ACS 1544 is amended to include this information. 16 ICD Coding Newsletter - June 2001 May be reproduced #1642 Post-infarction angina Question 1 If a patient is re-admitted with post-infarction angina one or two weeks after the original AMI, should the AMI or the post-infarction angina be sequenced first? Question 2 ACS 0940 states, ‘if the patient develops postinfarction angina, I20.0 Unstable angina may be sequenced as an additional code’. Does this line apply only to this happening in the same episode of care? In this case, the post-infarction angina was treated and was the reason for the admission. Question 1 The post-infarction angina would be the principal diagnosis as it was the reason for admission. Because this is still within four weeks of the AMI, the AMI would also be coded (see Inclusion note with I21) to: I21.- Acute myocardial infarction Question 2 The quotation from ACS 0940, page 141, applies only when coding the same episode of care in which the acute myocardial infarction was initially treated. #1644 Mechanical complication of ventricular shunt A 52 year old male is admitted with a mechanical complication of his ventricular shunt and has it revised at the distal peritoneal site. The codes used were: T85.0 Mechanical complication of ventricular intracranial (communicating) shunt Y83.1 Surgical operation with implant of artificial internal device Y92.22 Health Service Area 90330-00 [1001] Revision of cerebrospinal fluid shunt at peritoneal site 92502-02 [1910] Intravenous and inhalation general anaesthetic These codes seem fine but it is grouping to 901Z Extensive O.R procedure unrelated to principal diagnosis. Is this a grouping anomaly, as the principal diagnosis does relate directly to the procedure? May be reproduced ICD Coding Newsletter – June 2001 17 The Commonwealth has been advised of this anomaly, however notification was too late for inclusion into AR-DRG Version 4.2. This will be considered for version 5 and in the interim, DRG 901Z is inevitable. #1648 Chemotherapy & device loading Should code: Z45.- Adjustment and management of implanted device still be assigned as the principal diagnosis if a patient was admitted to the Chemotherapy Ward as a same day patient for flushing of vascular access device when chemotherapy is not administered during the same admission. If the patient meets the criteria for admission and the only treatment is flushing of the device, then the principal diagnosis would be: Z45.- #1650 Adjustment and management of implanted device Post-procedural complications I am writing for further clarification of coding post-procedural complications mainly in relation to the following statements taken from ACS 1904: ‘... a post procedural complication is defined as: A condition or injury that is related to a surgical/procedural intervention rather than being related to the patients disease process.’ An example is a patient admitted for a femoral-popliteal bypass and common femoral artery endarterectomy. The patient has a past history of ischaemic heart disease (IHD), having had an AMI 12 months ago with no further chest pain since. The patient underwent the above procedure and developed angina post-procedurally (on the day of the procedure) which was treated with Anginine. The patient will now be followed up by Cardiology. Clinician has documented post-op angina. Would this be coded as a post-procedural complication? 18 ICD Coding Newsletter - June 2001 May be reproduced I97.8 Other postprocedural disorders of circulatory system, not elsewhere classified I20.9 Angina pectoris, unspecified Y83.2 Surgical operation with anastomosis, bypass or graft Y92.22 Health service area (Place of occurrence) as it is not an expected outcome of this procedure? OR is this an expected outcome because the procedure and complication involve the same body system (circulatory) and therefore coded only to: I20.9 Angina pectoris, unspecified If this is the case, if the patient underwent a hernia repair instead would we then code it as a post-procedural complication: I97.8 Other postprocedural disorders of circulatory system, not elsewhere classified I20.9 Angina pectoris, unspecified Y83.8 Surgical operation and other surgical procedures as the cause of abnormal reaction of the patient, or of later complication, without mention of misadventure at the time of the procedure, Other surgical procedure Y92.22 Health service area (Place of occurrence) OR is this considered an exacerbation of a previously existing condition (IHD) and therefore only coded as: I20.9 Angina pectoris, unspecified That is, ‘related to the patients disease process’. If this is the case, does this mean that all patients with pre-exiting IHD will never have post-procedural angina coded as a postprocedural complication? A clinician’s documentation of ‘post op’ does not necessarily mean that the condition is a complication of the operation (see ACS 1904 Procedural complications). ACS 1904 does not instruct coders to make decisions based on ‘expected outcomes’; rather, it states a ‘procedural complication’ is ‘A condition or injury which is related to a surgical/procedural intervention rather than being related to the patient’s disease May be reproduced ICD Coding Newsletter – June 2001 19 process’. In this case, the angina is most likely a progression of the pre-existing disease process even if the angina had not been diagnosed previously. The correct code is therefore: Angina pectoris, unspecified I20.9 #1651 Laparoscopic cholecystectomy to open cholecystectomy with exploration of CBD Laparoscopic cholecystectomy converted to open cholecystectomy and then exploration of the common bile duct. After examining the codes under cholecystectomy, there is no code that describes all the three features of the surgery. I then decided to code: 30446-00 [965] Laparoscopic cholecystectomy proceeding to open cholecystectomy For the exploration of the CBD, I decided to add: 30454-00 [963] Choledochotomy But it has an exclusion note that if the exploration is with a cholecystectomy it must be coded from [965]. My only choice is to use two codes from [965] to reproduce all the elements of my operative statements but the string of codes reads that I have coded two cholecystectomies. In order to capture all information, both codes are required despite the apparent repeat of one part of the surgery. This has been confirmed by the NCCH’s answers to NCCH Queries #374 and #471 and in the workbook for the Post Implementation Education Workshops, March 1999, where arthroscopy for removal of loose bodies requires: 49561-01 [1517] Arthroscopic meniscectomy of knee with debridement, osteoplasty or chondroplasty 49561-02 [1511] Arthroscopic removal of loose bodies with debridement, osteoplasty or chondroplasty Note, the Victorian ICD Coding Committee has submitted a request to NCCH for creation of a Standard that covers this type of double coding. 20 ICD Coding Newsletter - June 2001 May be reproduced #1654 Autologous chondrocyte implantation (ACI) A new procedure, referred to as ACI is being performed at our hospital. Question 1 Which code do we use for harvesting of cartilage? Question 2 Which code do we use for the re-implantation? At present, we are coding the harvesting of cartilage to: 90577-00 [1565] Procurement of muscle or fascia for graft 90574-01 [1561] Excision of joint, not elsewhere classified. We are coding the re-implantation to: 90598-00 [1520] Other repair of knee 14203-01 [1906] Direct living tissue implantation. We are coding the disease to one or other of these: M22.8 Other disorders of patella M23.89 Other internal derangements of knee, unspecified ligament or unspecified meniscus For this patient, the correct procedure code for the harvesting of cartilage is: 48558-00 [1503] Arthroscopic debridement of knee If not performed during a debridement of the knee, harvesting of cartilage could be coded to: 49557-01 [1502] Arthroscopic biopsy of knee If the hospital would like to be able to separately identify these patients, code as an additional diagnosis: Z51.4 Preparatory care for subsequent treatment, not elsewhere classified. The re-implantation of the cartilage is coded to: 49503-02 [1520] Chondroplasty of knee 14203-01 [1906] Direct living tissue implantation May be reproduced ICD Coding Newsletter – June 2001 21 A chondroplasty is a plastic repair of the knee. The above code can be located by: Chondroplasty -knee (open) 49503-02 [1520] and Repair - knee NEC - - by - - - chondroplasty – see Chondroplasty The diagnosis code for ‘chondral defect’ could be: M22.9 Disorder of patella, unspecified This code should be used only if there is no further information about the defect available. The coder should make an attempt to obtain further information. It may be that the actual diagnosis is ‘chondromalacia’, in which case the diagnosis code would be: M22.4 Chondromalacia patellae. A very useful diagram and explanation of this procedure can be found at www.thaxter.com/implantation.gif #1658 Smoking related COPD Instead of writing, ‘smoking related COPD’ our clinicians sometimes draw an arrow after the COPD and put smoker or ex-smoker. Alternatively, they write the smoking status of the patient next to the diagnosis of COPD. Is this sufficient enough to assign codes: J44.x Other chronic obstructive pulmonary disease F17.1 Mental and behavioural disorders due to use of tobacco – harmful use Or does the exact causal relationship between COPD and smoking have to be documented? 22 ICD Coding Newsletter - June 2001 May be reproduced Before COPD can be coded, it must meet ACS 0002 for additional diagnoses. The Committee considered that the above illustration would be sufficient indication that the condition was due to smoking. Sufficient indication of relationship Not an indication of relationship • COPD/smoker • COPD • HT • HT • CCF • CCF • Smoker • COPD/smoker • CCF COPD/CCF/AF/DM/Smoker COPD ← smoker Smoker →COPD #1659 ACS 0226 Prostatic cancer Just wishing to confirm that, following the deletion of ACS 0226 Prostatic Cancer from 2nd edition ACS, that any history of prostate cancer (meeting additional diagnosis standards, of course) would now be coded to: Z85.4 Personal history of malignant neoplasm of genital organs regardless of previous surgery type. NCCH Query #1341 answer states that ACS 0226 Prostate cancer (1st edition) is still clinically relevant. Therefore, prostate cancer patients who have had a non-radical prostatectomy/TURP should be assigned code C61 Malignant neoplasm of prostate, not a Z85.- code, as these patients still have prostate cancer in the remaining prostate tissue. The NCCH will consider the reintroduction of a similar ACS. May be reproduced ICD Coding Newsletter – June 2001 23 #1661 Principal diagnosis in obstetrics This is a general query regarding determination of the principal diagnosis in obstetric cases, but an example to illustrate is: Prolonged pregnancy for medical and surgical induction, progresses to vacuum extraction due to compound presentation, followed by suture of 1st degree perineal laceration. Should the principal diagnosis be the prolonged pregnancy (reason for admission) or the compound presentation (reason for vacuum extraction)? There is variation amongst coders about the choice for principal diagnosis. Some coders sequence conditions in chronological order, whilst others identify the major procedure and then match the principal diagnosis to that. We note the HIMAA coding course textbook instructs that the principal diagnosis is that related to the actual delivery itself (presumably in our example above, the compound presentation and vacuum extraction). There are two queries on the NCCH database that deal with this issue. Query #174 and #877 that state there are no strict rules with regard to assigning principal diagnosis unless the patient is admitted antenatally. The sequence of diagnosis codes is not significant for grouping, however coders should ensure that important diagnosis codes are transmitted to the VAED, if there are a large number of codes for one patient. The most significant procedure should be sequenced first. 24 ICD Coding Newsletter - June 2001 May be reproduced #1662 ACS 2103 Admission for Convalescence/ Aftercare I seek clarification on application of ACS 2103 Admission for Convalescence/Aftercare, in cases of aftercare following medical (as against surgical) treatment for a condition. Sample case: Patient transferred back to our hospital following overnight treatment in a larger hospital Accident and Emergency department for fractured vertebra post MVA. Medical investigation only at larger hospital, 4 weeks medical treatment at our hospital. Is the principal diagnosis the aftercare or the medical condition? ACS 2103 has been modified in the 2nd edition, but this was not highlighted in the Education Workshops (Appendix B, Workbook list of changed Standards does not mention ACS 2103). The change affects coding of cases of aftercare following medical (as against surgical) treatment of a condition, with the changed wording suggesting that the condition is coded as an additional diagnosis now whereas the first edition instruction was ‘assign the code for the condition…’ for these cases. As the patient was clearly given medical treatment at your hospital, this is not an admission for convalescence or aftercare, but rather an acute medical admission. Therefore ACS 2103 does not apply in this case. #1663 Palliative Care What is the principal diagnosis for each of the following admissions to our palliative care unit? Case One 77 y.o female with stage 3 ovarian cancer presented with 4/52 upper abdominal pain for ‘symptom control’ (in one place in the record) and ‘investigation and treatment’ (in another). May need endoscopy, +/- CT abdo to elucidate cause of pain. Previously started on Ranitidine because of dyspepsia. Investigations not carried out, and patient’s pain settled over a few days. May be reproduced ICD Coding Newsletter – June 2001 25 Case Two 35 y.o. male with metastatic (lung and spinal cord) psoas muscle sarcoma presenting with increasing pain for symptom control. Quadriplegic due to spinal cord compression from mets. This admission, presents with low back pain, constipation, increased right arm weakness and twitching, and partially treated E. Coli UTI. Deteriorating condition. Treated with morphine, Clonazepan and Augmentin. Case Three 45 y.o. male with frontal oligodendroglioma, admitted with nausea and vomiting and increasing debility for symptom control. Increasing nausea probably due to increased intracranial pressure. Has had dizziness, nausea, occasional headache, unsteady on feet for months. Treated with Maxolon, steroids, ranitidine, haloperidol. Case Four 43 y.o. male with metastatic thymic carcinoid tumour (extensive secondaries in bone – pelvis, ribs, sternum, orbits, thoracic and lumbar spine and brain) presents with severe low back and hip pain for treatment/symptom control. Also dehydrated and constipated. Treated with pain control medications. ACS 0224 Palliative Care states ‘A principal diagnosis code should be assigned which reflects the diagnosis resulting in the relatively shortened prognosis’, thus for patients admitted to a Palliative Care Unit (and therefore admitted specifically for palliative care) the diagnosis should be the terminal condition. As this is a palliative care unit, it is easy to determine that the patient has been admitted for palliative care. When a terminally ill patient is admitted to an acute setting, care should be taken to determine the reason for admission. If the intent for the admission is for palliative care, ensure that ACS 0224 is followed. If the admission is for symptomatic care, ensure that ACS 0001 is followed when assigning the principal diagnosis. 26 ICD Coding Newsletter - June 2001 May be reproduced #1664 Musculoskeletal chest pain How should we code musculoskeletal chest pain? R07.4 Chest pain, unspecified R07.3 Other chest pain M79.18 Myalgia, other The correct code for musculoskeletal chest pain is: R07.3 Other chest pain Although the Index at Pain – chest does not give a code for ‘Other’, reference to the Tabular indicates that R07.3 is a better code than R07.4 as this chest pain is specified as musculoskeletal’. The Index also provides: Pain - muscle M79.1- chest - - anterior wall R07.3 #1665 Anaesthetic procedures Would we code both epidural and spinal anaesthesia, in this case given for elective LUSCS (no anaesthesia during labour)? According to our anaesthetists, this is being done more often for ‘better anaesthetic cover’. ACS 0031 Anaesthesia (page 35) gives a hierarchy for coding anaesthesia but epidural, spinal and cannula are on the same level (iii). Query #1294 on the NCCH Query Database advises that both codes are assigned. The spinal anaesthesia provides fast pain relief while the epidural provides longer relief. May be reproduced ICD Coding Newsletter – June 2001 27 #1669 External cause code - scooters The patient had a fall from an ‘unmotorised scooter’. We have currently coded this to W02 Fall involving ice-skates, skis, roller-skates or skateboards Owing to its proximity to a skateboard. We have checked the Coding Query Database and tried all the index possibilities but have come up with no further clarification. It appears that accidents involving people riding scooters are not automatically assigned to W02. The term ‘pedestrian’ in Definitions Related to Transport Accidents (vol 1, page 444) includes a person riding a scooter as a user of a ‘pedestrian conveyance’. It was noted that, if the person falls from the scooter, the correct code is: W02 Fall involving ice-skates, skis, roller-skates or skateboards If the fall results from collision with another person, the correct code is: W03 Other fall on same level due to collision with, or pushing by, another person Includes: fall due to collision of pedestrian (conveyance) with another pedestrian (conveyance) However, the Table of Land Transport Accident (vol 2, page 420), under pedestrians, provides the following External Cause codes: For a person on a scooter colliding with another person: W51 Striking against or bumped into by another person For a person on a scooter striking a stationary object: W22 28 Striking against or struck by other objects ICD Coding Newsletter - June 2001 May be reproduced #1671 Osseous metaplasia and Solar lentigo I need advice on how to code: 1. Osseous metaplasia 2. Solar Lentigo I have used the following codes: L98.9 Other specified disorders of skin and subcutaneous tissue L81.4 Other melanin hyperpigmentation Please review ACS 0033 and 0034 for the use of modifiers and inclusion terms. Osseous metaplasia is a bone condition (histology report would indicate this). Follow the index: Disorder - bone - - specified type NEC and use code M89.8- Other specified disorders of bone. Solar Lentigo is coded to: L81.4 Other melanin hyperpigmentation. Inclusion terms are not exhaustive, and coding convention permits the use of general terms to describe a condition if there is no essential modifier present to further clarify the term. May be reproduced ICD Coding Newsletter – June 2001 29 #1676 Follow-up gastroscopy A patient comes in for follow-up gastroscopy to check on ulcerative oesophagitis and hiatus hernia. Patient had been treated with Losec. On follow-up gastroscopy, only hiatus hernia is found. Would I use the new standard ACS 2111 Screening for Specific Disorders and code the appropriate: Z09.- Follow-up examination after treatment for conditions other than malignant neoplasms then the hiatus hernia code or would I just code the condition found. Investigation by the Coding Committee indicates that the Losec would be given for treatment of the ulcerative oesophagitis. As the follow-up gastroscopy was to check the resolution of the ulcerative oesophagitis, which had resolved, the principal diagnosis code should be: Z09.8 Follow up examination after other treatment for other conditions. Other codes to use are: Z87.18 Personal history of other digestive system disease K44.9 Diaphragmatic hernia and the appropriate endoscopy procedure code. ACS 2111 cannot be applied in this case, as ‘screening is the testing or examination for disease or disease precursors in asymptomatic individuals’, and ‘codes….should be assigned as the principal diagnosis when a patient is examined for a particular disease or disorder when the disease for which the patient is being screened is not detected or has never been detected’ (ACS 2111). As this patient has a known past history of a condition this standard does not apply. #1677 Grouping of laparoscopy codes Patient admitted with duodenal obstruction caused by cancer of pancreatic body diagnosed on CT, for gastrojejunostomy. Surgeon performed laparoscopy first and then converted to an open procedure. 30 ICD Coding Newsletter - June 2001 May be reproduced For grouping, when procedure codes include laparoscopy: • H05A Hepatobiliary diagnostic procedures with Catastrophic/Severe CC [mean LOS 10.8, weight 3.3610]. Without laparoscopy: • H06Z Other hepatobiliary & pancreas OR procedures [mean LOS 17.0, weight 5.1595]. Diagnosis codes were: C25.1 Malignant neoplasm of body of pancreas M8140/3 Adenocarcinoma NOS K56.6 Other and unspecified intestinal obstruction E87.6 Hypokalaemia C83.3 Diffuse non-Hodgkin’s lymphoma, large cell (diffuse) M9680/3 Malignant lymphoma, large cell, diffuse, NOS D56.8 Other thalassemia Groups to H06Z Other hepatobiliary & pancreas OR procedures without laparoscopy: 30515-00 [881] Gastro-enterostomy Groups to H05A Hepatobiliary diagnostic procedures with catastrophic/Severe CC with laparoscopy: 30515-00 [881] Gastro-enterostomy 30390-00 [984] Laparoscopy Laparoscopic code takes grouping to diagnostic procedures, which is incorrect. Do we need a new code for "converted from? to.. " or separate laparoscopic code for gastrojejunostomy? Which codes do I use for now? This problem exists in several areas of the grouper logic (for example MDC 13, female reproductive system) and in cases of long stay medical patients who have a minor diagnostic procedure during their stay. The problem occurs because of the surgical hierarchy. May be reproduced ICD Coding Newsletter – June 2001 31 Because there are not enough patients having gastroenterostomy to justify a specific DRG for gastroenterostomy, these patients are allocated to the ‘other’ DRG. On the other hand there are many patients who have a diagnostic procedure and the creation of a DRG for these patients is justified. Consequently, when a patient who would otherwise be allocated to the ‘other’ DRG has a procedure that is listed for any one of the specific DRGs, the case will move into the more specific DRG. Most of the time, this works in favour of the hospitals. The diagnostic DRG is often the exception. This logic can be easily studied in the flow charts at the beginning of the MDC 7 chapter in Volume 1, page 250 of the version 4.1 definitions manual. The Department of Human Services has sent a submission to the Commonwealth for consideration. In the interim, your suggested codes are correct. #1680 Low K+ Is the documentation (recorded by the clinician) of ‘Low K+’ sufficient for coding: E87.6 Hypokalaemia Patient was admitted for closure of ileostomy, ‘Low K+’ documented and patient commenced on Slow K. This is an accepted medical abbreviation. As the patient has been put on medication for this condition, the hypokalaemia may be coded. The term ‘low’ is acceptable terminology indicating hypokalaemia. This could also be indicated by a down pointing arrow. Similarly the term ‘high’ or an up pointing arrow are acceptable terminology. 32 ICD Coding Newsletter - June 2001 May be reproduced #1682 Underlying condition Do you code the underlying condition when the condition being coded is not the principal diagnosis? ACS 0001 instructs to assign the underlying condition in addition when you are coding the ‘problem’ – but this is for principal diagnosis. Two examples are for patients admitted for other conditions but have End Stage Renal Failure due to reflux nephropathy and liver failure due to cirrhosis. The nephropathy and cirrhosis do not meet ACS 0002, on their own. Only code those that meet the definition of ACS 0001 and ACS 0002. Except where the specialty Coding Standards override, coders should not code ‘packages’ of diseases. If the components are active and are being actively treated, these may be coded, otherwise code only the treated conditions. #1685 Ethanol injection Please advise on how to code endoscopic ethanol injections of a non-bleeding angiodysplastic stomach lesion. I have coded this as: 30473-00 [1005] Panendoscopy to duodenum 92193-00 [1885] Injection or infusion of other therapeutic or prophylactic substance 92503-00 [1911] Intravenous sedation, anaesthetist controlled This groups to: G45B Other gastroscopy – Non major digestive disease, same day If I were to use code: 30478-07 [870] Endoscopic sclerosing injection of bleeding gastric or duodenal lesions May be reproduced ICD Coding Newsletter – June 2001 33 this would group (I believe inappropriately) to: G41B Complex therapeutic gastroscopy – Non major digestive disease, same day I do not believe the code is correct as the lesion is not, and has not been bleeding. I cannot find a code that accurately reflects this procedure. There is no code for injection of non-bleeding lesion of the stomach and I am also unsure if ethanol is considered a sclerosing agent. On investigation, we find that ethanol is a sclerosing agent, therefore the Coding Committee recommends the use of code: 30478-07 [870] Endoscopic sclerosing injection of bleeding gastric or duodenal lesions The Coding Committee will lodge a public submission to the NCCH suggesting the removal of the term ‘bleeding’ from the code descriptor, or the creation of a new code for injection of non-bleeding lesions. It was noted that the index for injection of varices leads to ‘non-bleeding’ for oesophagus and oesophago-gastric sites whilst it leads to ‘bleeding’ for gastric and duodenal sites. #1689 ACS 0012 suspected condition (perforation) 7/9/00: Colonoscopy with biopsy performed for diarrhoea for investigation; Outcome: mild colitis – Discharged home. 8/9/00: Presented with abdominal pain, post colonoscopy and fever (perforation??) Settled with IV antibiotics – Discharged home 9/9/00 with script for Keflex. Suggested code: K52.9 34 Colitis ICD Coding Newsletter - June 2001 May be reproduced We reviewed ACS 0012 Suspected Conditions ‘if treatment is initiated, and investigation results are inconclusive, assign a code for the suspected condition’ and ACS 1904 Procedural Complications ‘some transient conditions occur in the post procedural period but are not regarded as post procedural complications.’ Suggested codes for 7/9/00: K52.9 Noninfective gastroenteritis and colitis, unspecified 32090-01 [911] Fibreoptic colonoscopy to caecum, with biopsy Anaesthetic code as appropriate Suggested codes for 8/9/00 (on the basis of the above information) R10.4 Other and unspecified abdominal pain R50.9 Fever, unspecified The documentation (as quoted) does not support the coding of perforation of colon. The Keflex is more likely to be treatment for the colitis or fever and not necessarily a standard treatment for colon perforation. #1691 ACS 0909 Additional procedures performed in conjunction with CABGs Should Swan-Ganz catheterisation and intra-operative transoesophageal echocardiogram (TOE) be coded in conjunction with a CABG procedure? Are they a routine part of a CABG procedure and as such are codes not required for these components? In view of ACS 0909 Coronary artery bypass grafts that says not to code other routine procedures performed with CABGs, the Committee considers that these are a part of the CABGs procedure and therefore should not be coded. May be reproduced ICD Coding Newsletter – June 2001 35 #1693 Bilateral maxilla and mandible osteotomies with internal fixation It appears there are two possible ways of coding bilateral maxilla and mandible osteotomies with internal fixation. Example 1 45722-01 [1706] Osteotomy of maxilla with internal fixation, bilateral/Le Fort osteotomy with internal fixation 45722-00 [1706] Osteotomy of mandible with internal fixation, bilateral Example 2 45746-00 [1708] Osteotomies or ostectomies of mandible and maxilla, 4 procedures with internal fixation I believe Example 1 provides a greater level of specificity as to where the procedures were actually performed, that is, how many osteotomies were performed on the maxilla versus how many were performed on the mandible. Confusion also arises in the counting of the procedures. Are we only counting the number of osteotomies and ostectomies? Are there other procedures that we should be counting as well (eg genioplasty, bone grafts) if performed? In the above case there are no other procedures to count except the number of osteotomies, so what codes are to be used? The Committee recommends following the index entry: Osteotomy - maxilla - - multiple procedures - - - with - - - - multiple ostectomies or osteotomies of mandible, in combination — see block [1707] 36 ICD Coding Newsletter - June 2001 May be reproduced Coding Corkboard Coding Newsletter Mailing List Currently the Victorian Coding Newsletter is freely distributed to hospitals. As it is planned that the hard-copy printing and posting of the Newsletter will be phased out, we are seeking your help to update our ‘mailing list’. Once our mailing lists have been updated, it is our intention to post only one hard copy newsletter to each Victorian hospital. If you have a special need to receive a hard copy newsletter, please send your request to the Secretary, Victorian Coding Committee via fax or email as detailed below. The Newsletter will still be available via the Health Data Standards and Systems Unit website http://www.dhs.vic.gov.au/ahs/hdss/newslett.htm however you will now have the opportunity to receive your own copy via email. For each person wishing to receive their own electronic copy of the Coding Newsletter, please email your contact details to the Secretary, Victorian Coding Committee: [email protected] Alternatively, please fax the ‘Coding Newsletter Email Subscriber Form’ (enclosed inside back cover of this Newsletter) to the Secretary, Victorian Coding Committee on: (03) 9616 7629 May be reproduced ICD Coding Newsletter – June 2001 37 Health Funds and Australian Coding Standards The Victorian ICD Coding Committee requests that hospitals send details of any instance of a health fund requiring a hospital to provide ICD codes in a format that does not follow the Australian Coding Standards (for example, requesting codes in a different sequence or not accepting a Z code as principal diagnosis). We will refer instances to the National Centre for Classification in Health; ultimately, these matters will be taken up with the Australian Health Insurance Association (AHIA). For each instance, please provide the Secretary of the Victorian Coding Committee with the following details: • Name of contact and contact details (for example, email address) • Name of hospital • UR Number and separation date of episode • Name of health fund (and, if possible, name or title of employee) • Description of unresolved problem with health fund [email protected] Secretary, Victorian ICD Coding Committee 38 ICD Coding Newsletter - June 2001 May be reproduced Websites New Zealand Health www.nzhis.govt.nz/publications/coders-current.html Information Service (nzhis) (Previous issues available via a link at the top of each Coders’ Update issue) Just Coding - a US web site www.justcoding.com with useful articles, quizzes, etc RxList - an internet drug index www.rxlist.com Australian Institute of Health www.aihw.gov.au and Welfare (AIHW). In particular, a range of publications using hospital data: AIHW’s newsletter Access is www.aihw.gov.au/publications/health.html available at this site. Handbook of Medical www.mihandbook.stanford.edu/handbook/home.htm Informatics (UK) – contains coding quiz in Q&A section May be reproduced ICD Coding Newsletter – June 2001 39 Information Updates Data Quality Audits of VAED Data 1999–2000 The Final Report for the 1999–2000 audit of VAED data was posted to the DHS website in January. It is password protected. All public hospitals were notified of access codes in a letter sent to CEOs in January, which also advised of the commencement of the 2000–2001 audits. 2000–2001 The audit of 2000–2001 VAED data commenced in December 2000. This is a Year one audit within the two year audit cycle, and as such will provide a statewide audit result, as hospitals will be selected from all groups, and metropolitan and rural locations. Methodology will be consistent with that used in the previous two years of this project, updated to the second edition of ICD-10-AM, AR-DRG v4.1 and WIES8. Data will mostly be drawn from the first three quarters of 2000–2001, however data from the final quarter of the 1999–2000 financial year have been reviewed at some sites, and data from the final quarter of 2000–2001 will be used at others. In all instances, the most recent available data will again be examined. Hospital Selections - Random, Follow-up, Supplementary - and Targets Some 7,700 episodes will be reviewed at the 56 sites randomly selected for audit of an ‘annual’ sample. Four sites audited in 1999–2000 had results warranting ‘follow-up’ audit in this round. Sample sizes at these four sites will be larger, and designed to achieve statistically significant results, with a total of 1,830 episodes to be assessed. Of the 12 sites where follow-up audits were conducted last year, results at seven remained outside previously set parameters, and ‘supplementary’ audits (as provided for in the Policy and Funding Guidelines) will be conducted on 700 episodes at these sites. In addition, two target audit topics have been identified: coding of 500 ‘sick neonate’ episodes will be examined across 14 sites, while the results of the Dual Coding Study will 40 ICD Coding Newsletter - June 2001 May be reproduced be verified at nine sites. These target sites may be involved in the audit either as ‘annual’, ‘follow-up’ or ‘supplementary’ sites, or may just be selected for one or both audits of target data. By mid April, about 26 sites had been audited of the 71 sites to be involved in the audit of 2000–2001 VAED data. A further 25 sites should be completed by the end of June, with the remainder to be audited before mid September, when visits are scheduled to be completed. Queries Any queries about the VAED audits should be directed to Joanne McLachlan (9616 7710) or Mark Gill (9616 7456), rather than HMA or auditors. May be reproduced ICD Coding Newsletter – June 2001 41 A review of Newborns – Qualified but no condition coded Irene Kearsey, Department of Human Services Purpose of data study Some newborn episodes in the Victorian Admitted Episode Dataset (VAED) are reported as acute but with no condition coded (the only diagnosis code being for birth outcome). Whether the newborn is Qualified or Unqualified makes no difference to the casemix payment the hospital receives. However, there are two important reasons why the Department needs the Qualification Status (and therefore the Care Type) to be correct: • Put simply, the Department reports Acute Care episodes to the Commonwealth to secure Victoria’s share of Medicare funding and does not report Unqualified episodes; the Department can be audited and must be seen to make every attempt to provide accurate data. • If the postcode for an Acute Care episode is interstate, the Department bills the relevant interstate health authority for that admission; if the coding seems to indicate there was no justification for an “admission” (for example, a newborn with no code that indicates a diagnosis), an interstate health authority will not pay and the Department cannot recover costs. There are three criteria for a newborn to be Qualified: • Second or subsequent live born of a multiple birth • Admitted to a Neonatal Intensive Care Unit/Special Care Nursery • Remains in hospital without the mother The Z38.- code can indicate a multiple birth and an additional diagnosis code can indicate the absence of the mother in certain circumstances. In almost every circumstance, the reason for time in a Neonatal Intensive Care Nursery/Special Care Nursery (NICU/SCN) can be indicated by a diagnosis code. The only explanation for the absence of such a diagnosis code would be if the newborn had a condition that caused him/her to be moved to the NICU/SCN but this could not be coded because the circumstances did not justify coding it according to ACS 1615 Specific interventions for the sick neonate. 42 ICD Coding Newsletter - June 2001 May be reproduced Details of data search Using the 2000-2001 VAED (December Consolidation), I extracted all newborn episodes where the only diagnosis code is Z38.0 Singleton, born in hospital but the Care Type is 4 Acute (rather than U Unqualified newborn). I sent each hospital reporting any such episodes a list of the records and asked for an investigation and report back on the circumstances. I also looked at the Criterion for Admission because, if the diagnosis coding were correct (for example, the baby had no problem), the Criterion for Admission should be U Unqualified newborn. If the mother left the hospital before the baby (that is, during the episode, the baby became qualified causing the Care Type to became Acute), the Criterion for Admission should remain U (rather than be N Qualified newborn). Results – Summary The initial extract of episodes containing a Z38 Newborn code produced 18,808 records (remember, this was the December consolidation so less than half a year’s records were coded). Of these, 18,221 were Z38.0 Singleton, born in hospital. The final extract found 151 records with Care Type 4 Acute where the only diagnosis code was Z38.0 Singleton, born in hospital (0.8%). Although this is a tiny percentage, action to correct anomalies is still worthwhile. The following table summaries the numbers of records per hospital: Hospitals with records Records each found in this extract 6 1 3 2 4 3 1 5 1 6 2 9 2 10 1 30 1 48 Total hospitals 21 Total records 151 May be reproduced ICD Coding Newsletter – June 2001 43 Of the 151 records, 4 records (2.6%) had Criterion for Admission U Unqualified newborn at admission. The other 147 records (97.4%) had Criterion for Admission N Qualified newborn (ie, Qualified at time of birth rather than becoming qualified because, for example, the mother had left the hospital). After the initial mail-out and one follow-up, four hospitals did not respond, representing 1 record, 3 records, 5 records, and 48 records respectively (57 records in all). Seventeen hospitals that did respond represented 94 records. The 94 records were identified as those with incorrect Care Type and those with missing diagnosis code, according to the hospitals’ responses: Incorrect Care Type 13 13.8% Missing diagnosis 81 86.2% Total 94 Some hospitals did not indicate what the additional diagnosis was, just that the newborn had been in the Special Care Nursery. For 89 records, the hospital indicated the missing diagnosis. No hospital reported an episode where the explanation was that the mother left the hospital before the newborn. Results – Care Type Generally, the allocation of qualification status for newborns is outside the control of the Health Information Manager but this review gave hospitals the chance to discuss the issue with those who do record this. For three hospitals, incorrect Care Type was the explanation for all their problem records. One episode (total length of stay four days) ended, at the patient’s request, with two days of Hospital in the Home. When the hospital transferred the mother and her (Unqualified) baby to HITH, the hospital changed the baby’s Care Type to Acute because the in-house system had no account code for Unqualified HITH. This is an incorrect change. The hospital should create an account code (or separate the baby from the date of leaving the hospital – although the circumstances, as given to me, would justify reporting the HITH days for the baby). See ‘Purpose of data study’ above for reasons why the Department needs the Care Type to be accurate. 44 ICD Coding Newsletter - June 2001 May be reproduced Results – Diagnosis coding Of the records with missing diagnosis codes, the following summarises the conditions that had been overlooked in a number of the records (with the Australian Coding Standard, where one applies). Maternal diabetes Look at ACS 1602 Neonatal complications of maternal diabetes If the laboratory report and the clinician confirm the newborn had at least a transient decrease in blood sugar that can be attributed to the maternal condition, you should assign, with the Z38 code, one of the following: P70.1 Syndrome of infant of a diabetic mother P70.0 Syndrome of infant of mother with gestational diabetes Baby needs more care than normal because of some maternal cause Look at ACS 1609 Maternal causes of perinatal morbidity and mortality and Coding Matters Volume 7, Number 3, December 2000 Newborns affected by maternal causes If a baby requires more care than normal because of a maternal cause, you should assign, with the Z38 code, a code from the following plus a code for the effect on the newborn (sequenced first): P00 Fetus and newborn affected by maternal conditions that may be unrelated to the present pregnancy P01 Fetus and newborn affected by maternal conditions of pregnancy P02 Fetus and newborn affected by complications of placenta, cord and membranes P03 Fetus and newborn affected by other complications of labour and delivery P04 Fetus and newborn affected by noxious influences transmitted via placenta or breast milk Observed post-caesarean – no ill-effect Look at ACS 1609 Maternal causes of perinatal morbidity and mortality If a baby is observed post-caesarean but suffers no ill-effect, you should assign, with the Z38 code: Z76.2 Health supervision and care of other [than foundling] healthy infant and child May be reproduced ICD Coding Newsletter – June 2001 45 Observed for suspected condition, such as sepsis Look at ACS 1611 Observation and evaluation of newborn for suspected condition not found If an otherwise healthy newborn is suspected to be at risk of an abnormal condition but, after examination and observation, there is no need for further treatment or medical care, you should assign, with the Z38 code: Z03.8 Observation for other suspected diseases and conditions Mother not able to care for baby Look at ACS 1615 Specific interventions for the sick neonate – Maternal illness/incapacity to care: If the newborn is exclusively dependent on nursing care for more than 24 consecutive hours, you should assign, with the Z38 code, a code to indicate the reason for the baby requiring care. Examples include: Z02.8 Other examinations for administrative purposes [baby for adoption] Z76.2 Health supervision and care of other [than foundling] healthy infant and child [mother transferred to ICU or to another hospital, causing the baby to be cared for in SCN] Of the other conditions that had been overlooked, the following were mentioned by more than one hospital: • Prematurity • Respiratory distress Summary Some hospitals commented on the exercise: • “We have … spoken to the Resident Doctors about the diagnosis and to give a reason why the baby was in Special Care Nursery. I hope this will eliminate cases of this kind in the future.” • “This proved to be a very useful exercise and promoted much discussion amongst our coding team. Please continue with this type of feedback.” This hospital is also investigating an internal mechanism for checking this on a routine basis within the hospital. 46 ICD Coding Newsletter - June 2001 May be reproduced Action for preventing this from occurring • Liaise with NICU/SCN clinicians to ensure comprehensive documentation. • Liaise with administrative staff responsible for assigning Care Type to ensure rules are followed. Acknowledgement I thank the hospitals for their efforts in reviewing their records and reporting back. Because the VAED is still ‘live’ for these episodes, hospitals have been able to revise their data (which would have increased WIES in some episodes). For all of these episodes, the hospital’s PRS/2 Control Report would have given Warning message 403 Qualified newborn without justification. This exercise demonstrates that it is unwise to ignore warning messages. Dual Coding Study Results Additional Diagnoses and Post Procedural Complications Mark Gill, Department of Human Services Throughout this financial year a Dual Coding Study has been conducted to assess the impact of two significant changes to Australian Coding Standards (ACS) 0002 Additional Diagnosis and 1904 Procedural Complications. The Department recognised that these revised coding standards could adversely affect the funding of Victorian public hospitals through significant numbers of episodes grouping to ‘non-CC’ DRGs, when previously they would have grouped to ‘with CC’ DRGs. The Dual Coding Study was designed to identify and manage this effect and the Department indicated it would not penalise hospitals for failing to reach agreed WIES8 levels where the shortfall could reasonably be attributed to the effect of modified ACS 0002 and ACS 1904. The Victorian Advisory Committee on Casemix Data Integrity (VACCDI) has overseen the Dual Coding Study which has involved nine volunteer hospitals (the Alfred, Monash, St Vincent’s, Ballarat, Warrnambool, Wangaratta, Goulburn Valley, Stawell and Kyabram) coding 2000-2001 separations in accordance with both the 1999-2000 and 2000May be reproduced ICD Coding Newsletter – June 2001 47 2001 applications of the coding standards. This data were then matched to data held by the Department to simulate funding differences and to derive WIES8 reduction factors. The Dual Coding Study has confirmed that WIES8 has been reduced by the modification to coding standards. Based on the initial results from four hospitals (A1, B1, C1, C2), Coding Standards WIES8 Adjustment Factors were set at 1.025 for A hospitals, 1.0125 for B hospitals and 1.007 for C,D,E hospitals. The Department gathered information from five more hospitals and together the results show significant differences between hospitals from the same hospital group. There are two main reasons for this: (i) statistical analysis from the VAED Audit suggests high sampling variability in regard to WIES; and (ii) differences in hospital coding in regard to these standards, particularly before, and possibly after the modifications. More information will be available on the latter effect, and any reconsideration of the factors will occur, after the Dual Coding Study results have been examined within the 2000-2001 phase of the VAED audit. The Dual Coding Study results are shown below: DUAL CODING STUDY, VICTORIA, 2000-2001 (modified additional diagnoses and post procedural complications coding standards) HOSPITAL BY GROUP RECORDS DUAL CODED % DRG CHANGE % WIES CHANGE A1 900 7.3 -2.84 A2 500 3.2 -0.76 A3 1349 2.8 -0.81 B1 741 2.1 -0.92 B2 500 3.8 -2.45 B3 500 3.8 -1.60 B4 457 3.5 -1.95 C1 254 1.6 -0.70 C2 269 0.7 -0.24 48 ICD Coding Newsletter - June 2001 May be reproduced Reporting To The VAED AR-DRG Modifications (2001-2002) As notified in HDSS Bulletin 20, Victoria will move to AR-DRG Version 4.2 for casemix funding of Victorian Public Hospitals for separations occurring on or after 1 July 2001. A list of the changes between Version 4.1 and Version 4.2 is available from the Commonwealth Department’s website at: www.health.gov.au/casemix/dev42.htm Details of software availability are located at: www.health.gov.au/casemix/grouper1.htm The new AR-DRG Version 4.2 Manual consists of the existing three-volume AR-DRG Version 4.1 Manual, plus a new Volume 4, which can be ordered from the National Centre for Classification in Health. The following is an excerpt from the Victoria — Public Hospitals Policy and Funding Guidelines 2001–2002: In 2001-2002, hospitals will assign diagnoses and procedure codes using the 2nd edition of the ICD-10-AM classification. For funding purposes, these codes will be grouped using AR-DRG Version 4.2 (no mapping required). As in previous years, some adjustments are to be made to the original AR-DRG4 (Version 4.2) grouping utilising the VIC-DRG4 field, prior to the calculation of WIES9. Some of the AR-DRG Version 4.1 adjustments applied in WIES8 (bilateral hip replacement and bilateral knee replacement; hook needle localisation of breast lesion; retained placenta and membranes without haemorrhage; paraurethral injection; care of lactating mother; and post natal depression) are no longer necessary as the anomalies have been rectified in AR-DRG Version 4.2. The VIC-DRG4s for WIES8 for Peritoneal dialysis, Radiotherapy, Bone Marrow Transplants and Admission weight remain for WIES9. The VIC-DRG4s for Nasopharyngeal intubation and Arteriovenous fistula have been modified for WIES9. May be reproduced ICD Coding Newsletter – June 2001 49 Peritoneal dialysis In recognition of cost differences between peritoneal and haemodialysis, episodes with a principal diagnosis of peritoneal dialysis (ICD-10-AM code Z49.2) are to be assigned a VIC-DRG4 of L61Y Admit for peritoneal dialysis. Radiotherapy Victorian Coding Standard 0229 states that non-same day patients receiving radiotherapy should have the malignant condition sequenced first, followed by the radiotherapy code (ICD-10-AM code Z51.0). Same day radiotherapy admissions, which follow the Australian Coding Standard, have Z51.0 assigned as the principal diagnosis followed by the malignancy code. To maintain funding equity, a VIC-DRG4 of R64Z Radiotherapy will be assigned for non-same day, non-surgical episodes that include a radiotherapy diagnosis code (grouped as if the radiotherapy code is the principal diagnosis). Bone Marrow Transplants In recognition of cost differences between allogeneic and autologous bone marrow transplants, AR-DRG4 A04Z Bone marrow transplant is split into VIC-DRG4 A04A Allogenic bone marrow transplant and A04B Non-allogenic bone marrow transplant. Any cases grouped to AR-DRG4 A04Z with ICD-10-AM 2nd edition procedure codes of 13706-00, 13706-06, 13706-09, or 13706-10 are allocated to VIC-DRG4 A04A and all other cases originally grouped into AR-DRG4 A04Z are allocated to VIC-DRG4 A04B. Admission weight In AR-DRG Version 4.2, admission weight must be between 400 and 9999 grams otherwise the episode will be assigned to AR-DRG 960Z Ungroupable. The Department has been notified of live births where the baby weighs significantly less than 400 grams. Episodes with an admission weight between 125 and 399 grams are assigned an admission weight of 400 grams for grouping to an appropriate VIC-DRG4. 50 ICD Coding Newsletter - June 2001 May be reproduced Nasopharyngeal intubation For 2000-2001, new 2nd edition procedure codes were introduced for nasopharyngeal intubation (90179-02 Nasopharyngeal intubation and 90179-05 Management of nasopharyngeal intubation). In AR-DRG Version 4.2, these codes are valid only for MDC 22 Burns. These codes will be mapped to 92035-00 Other intubation of respiratory tract, so that episodes with either of these codes will group to an appropriate VIC-DRG4. Arteriovenous fistula In AR-DRG Version 4.1, procedure codes for surgical formation of arteriovenous fistula of lower limb (34509-00) and upper limb (34509-01), were not included in the lists of procedures relevant to MDC 11 Diseases and disorders of kidney and urinary tract. AR-DRG Version 4.2 has amended the allocation of procedure code 34509-01 arteriovenous anastomosis of upper limb but has not been amended for procedure code 34509-00 arteriovenous formation of lower limb. The procedure code for formation of arteriovenous fistula in lower limb (34509-00) will be mapped to 34509-01 arteriovenous anastomosis of upper limb, for grouping to an appropriate VIC-DRG4. May be reproduced ICD Coding Newsletter – June 2001 51 VAED Schedule Requirements 2001–2002 A hospital may transmit data via its nominated PRS/2 system as frequently as desired, but must meet requirements set out below according to hospital type. Public hospitals The following will be included in the Victoria—Public Hospitals Policy and Funding Guidelines 2001–2002 in Section B: Conditions of Funding: Acute Health. Transmission of Admitted Patient Data. The hospital will transmit data to the Victorian Admitted Episodes Dataset (VAED) via PRS/2 according to the timelines detailed in clauses (a) and (b). a) Admission and separation details for any month are to be transmitted in time for the VAED file consolidation on the 21st day of the following month (see (d) below for processing schedule). b) Diagnosis and procedure and sub-acute details in any month are to be transmitted in time for the VAED file consolidation on the 21st day of the second month following (see (d) below for processing schedule). c) Data for the financial year should be completed in time for the VAED file consolidation on 21 August 2002. Any corrections must be transmitted before finalisation of the VAED database on 21 September 2002. d) It is the hospital's responsibility to ensure that data are transmitted to the VAED to meet the processing schedule for inclusion in the Allegiance Systems file consolidation on the 21st of each month. Because of the various methods of transmission used by hospitals, and Allegiance Systems’ processing schedules, data must be transmitted by the PRS/2 feeder systems to the VAED by, at the latest, the 17th day of each month; however, weekends or public holidays may bring the effective deadline forward to the 14th day. 52 ICD Coding Newsletter - June 2001 May be reproduced e) WIES9, multi-purpose services and sub-acute payments will be: 1) fully paid for data originally submitted in accordance with the deadlines specified in clauses (a) and (b) above, even if data is subsequently amended; or 2) paid at a reduced rate (50 percent), or not recognised for payment, according to Schedules 2.1 and 2.2 located at the end of this section if the data has not been submitted in accordance with either deadline specified in clauses (a) and (b) above; or 3) not recognised for payment, if data has not been submitted in accordance with both deadlines specified in clauses (a) and (b) above. This clause applies to all account classes including DVA. f) If difficulties are anticipated in meeting the relevant data transmission timeframes for either admission and separation data, or diagnosis and procedure details, the hospital or multi-purpose service must write to the Department, indicating the nature of the difficulties, remedial action being taken, and the expected transmission schedule. Exemptions for one-off late submission of data will generally only be considered for computer system problems that are beyond the control of the hospital or multipurpose service. (Hospitals or multi-purpose services undertaking the PRS/2 data submission testing process are automatically exempted.) Exemptions for late submission of admission and separation data will also be considered for staffing problems that are beyond the control of the small rural hospitals or multi-purpose services. Exemptions for late submission of admission and separation data will be automatically granted to hospitals or multi-purpose services maintaining a consistently high level of timely data submission. g) Data should be reconciled after each transmission against the hospital or multipurpose service’s in-house computer or manual systems and against the Monthly Return-Admitted Patients and any required corrections transmitted with data for the subsequent period. Private hospitals Private hospitals are expected to adhere to the same timelines as Public hospitals (indicated above). May be reproduced ICD Coding Newsletter – June 2001 53 Schedule 2.1 Timelines for the Receipt of Admission and Separations Details (E2) VAED Consolidation Date Month of Separation 2001/2002 July 21 Aug Full Rate August 21 Sept Half Rate Full Rate September 21 Oct Nil 21 Nov Nil 21 Dec Nil 21 Jan Nil 21 Feb Nil Half Rate Full Rate Nil Nil Nil Nil Half Rate Full Rate Nil Nil Nil Half Rate Full Rate Nil Nil Half Rate Full Rate Nil October November December January Half Rate Full Rate VAED Consolidation Date Month of Separation 2001/2002 December 21 Mar Nil 21 Apr Nil 21 May Nil 21 Jun Nil 21 Jul Nil 21 Aug Nil 21 Sep Nil January Half Rate Full Rate Nil Nil Nil Nil Nil Nil Half Rate Full Rate Nil Nil Nil Nil Nil Half Rate Full Rate Nil Nil Nil Nil Half Rate Full Rate Nil Nil Nil Half Rate Full Rate Nil Nil Half Rate Nil February March April May June 54 ICD Coding Newsletter - June 2001 May be reproduced Schedule 2.2 Timelines for the Receipt of Diagnoses and Procedure (X2, Y2) and Sub-Acute Details (S2) VAED Consolidation Date Month of Separation 2001/2002 July 21 Sept Full Rate August 21 Oct Half Rate Full Rate September 21 Nov Nil 21 Dec Nil 21 Jan Nil 21 Feb Nil 21 Mar Nil Half Rate Full Rate Nil Nil Nil Nil Half Rate Full Rate Nil Nil Nil Half Rate Full Rate Nil Nil Half Rate Full Rate Nil October November December Half Rate VAED Consolidation Date Month of Separation 2001/2002 December January February March April May June May be reproduced 21 Mar Half Rate Full Rate 21 Apr Nil 21 May Nil 21 Jun Nil 21 Jul Nil 21 Aug 21 Sep Half Rate Full Rate Nil Nil Nil Nil Nil Half Rate Full Rate Nil Nil Nil Nil Half Rate Full Rate Nil Nil Nil Half Rate Full Rate Nil Nil Half Rate Full Rate Nil Half Rate ICD Coding Newsletter – June 2001 55 ICD-10-AM Library File for use in Victoria – 1.7.2001 As the move to AR-DRG v4.2 requires some revisions to the ICD Library File, the opportunity has been taken to make a few other minor revisions. These are set out in the table below. Each hospital has two options: • Download the new ICD Library File that is available from the Department’s web site (VAED downloadable files). This is password protected. Please contact the Help Desk to obtain the password. • Make the changes listed in the table below to their existing ICD Library File. Changes to ICD-10-AM Library File for use in Victoria for separations on and after 1.7.2001 Key to this table * Change [column] = the column of the Library File § Auth = Authority for change: DRG = revised in AR-DRG v4.2 (some edits in the Victorian file are more strict than those specified in v4.2) Vic = Victorian decision Code Indication of Diagnosis Code Title Change* Specification Auth§ I15.0 Renovascular hypertension First [Age] Insert DRG 40015 I15.1 M35.2 Hypertension sec to other renal First [Age] Insert disorder 40015 Behcet’s disease DRG First [Age] Remove edit DRG [Area] Remove edit Vic N39.3 Stress incontinence [Sex] Remove edit DRG N99.0 Postprocedural renal failure First [Age] Insert DRG 40015 N99.1 Postprocedural urethral stricture First [Age] Insert DRG 40015 N99.4 Postproc pelvic adhesions First [Age] Insert DRG 40015 56 ICD Coding Newsletter - June 2001 May be reproduced Code Indication of Diagnosis Code Title Change* Specification Auth§ N99.5 Malfunction stoma First [Age] Insert DRG 40015 N99.8 Other postproc GU system First [Age] Insert DRG 40015 N99.9 Postproc GU NOS First [Age] Insert DRG 40015 T31.00 Burns – body surface area [Code] Insert 1 DRG T31.10 Burns – body surface area [Code] Insert 1 DRG T31.11 Burns – body surface area [Code] Insert 1 DRG T31.20 Burns – body surface area [Code] Insert 1 DRG T31.21 Burns – body surface area [Code] Insert 1 DRG T31.22 Burns – body surface area [Code] Insert 1 DRG T31.30 Burns – body surface area [Code] Insert 1 DRG T31.31 Burns – body surface area [Code] Insert 1 DRG T31.32 Burns – body surface area [Code] Insert 1 DRG T31.33 Burns – body surface area [Code] Insert 1 DRG T31.40 Burns – body surface area [Code] Insert 1 DRG T31.41 Burns – body surface area [Code] Insert 1 DRG T31.42 Burns – body surface area [Code] Insert 1 DRG T31.43 Burns – body surface area [Code] Insert 1 DRG T31.44 Burns – body surface area [Code] Insert 1 DRG T31.50 Burns – body surface area [Code] Insert 1 DRG T31.51 Burns – body surface area [Code] Insert 1 DRG T31.52 Burns – body surface area [Code] Insert 1 DRG T31.53 Burns – body surface area [Code] Insert 1 DRG T31.54 Burns – body surface area [Code] Insert 1 DRG T31.55 Burns – body surface area [Code] Insert 1 DRG T31.60 Burns – body surface area [Code] Insert 1 DRG T31.61 Burns – body surface area [Code] Insert 1 DRG T31.62 Burns – body surface area [Code] Insert 1 DRG T31.63 Burns – body surface area [Code] Insert 1 DRG T31.64 Burns – body surface area [Code] Insert 1 DRG T31.65 Burns – body surface area [Code] Insert 1 DRG T31.66 Burns – body surface area [Code] Insert 1 DRG T31.70 Burns – body surface area [Code] Insert 1 DRG T31.71 Burns – body surface area [Code] Insert 1 DRG T31.72 Burns – body surface area [Code] Insert 1 DRG May be reproduced ICD Coding Newsletter – June 2001 57 Code Indication of Diagnosis Code Title Change* Specification Auth§ T31.73 Burns – body surface area [Code] Insert 1 DRG T31.74 Burns – body surface area [Code] Insert 1 DRG T31.75 Burns – body surface area [Code] Insert 1 DRG T31.76 Burns – body surface area [Code] Insert 1 DRG T31.77 Burns – body surface area [Code] Insert 1 DRG T31.80 Burns – body surface area [Code] Insert 1 DRG T31.81 Burns – body surface area [Code] Insert 1 DRG T31.82 Burns – body surface area [Code] Insert 1 DRG T31.83 Burns – body surface area [Code] Insert 1 DRG T31.84 Burns – body surface area [Code] Insert 1 DRG T31.85 Burns – body surface area [Code] Insert 1 DRG T31.86 Burns – body surface area [Code] Insert 1 DRG T31.87 Burns – body surface area [Code] Insert 1 DRG T31.88 Burns – body surface area [Code] Insert 1 DRG T31.90 Burns – body surface area [Code] Insert 1 DRG T31.91 Burns – body surface area [Code] Insert 1 DRG T31.92 Burns – body surface area [Code] Insert 1 DRG T31.93 Burns – body surface area [Code] Insert 1 DRG T31.94 Burns – body surface area [Code] Insert 1 DRG T31.95 Burns – body surface area [Code] Insert 1 DRG T31.96 Burns – body surface area [Code] Insert 1 DRG T31.97 Burns – body surface area [Code] Insert 1 DRG T31.98 Burns – body surface area [Code] Insert 1 DRG T31.99 Burns – body surface area [Code] Insert 1 DRG Z06 Infection w drug rest microorg. [Code] Insert 1 DRG Z11.0 Spec screening [Code] Remove 1 DRG Z11.1 Spec screening [Code] Remove 1 DRG Z11.2 Spec screening [Code] Remove 1 DRG Z11.3 Spec screening [Code] Remove 1 DRG Z11.4 Spec screening [Code] Remove 1 DRG Z11.5 Spec screening [Code] Remove 1 DRG Z11.6 Spec screening [Code] Remove 1 DRG Z11.8 Spec screening [Code] Remove 1 DRG Z11.9 Spec screening [Code] Remove 1 DRG Z12.0 Spec screening [Code] Remove 1 DRG Z12.1 Spec screening [Code] Remove 1 DRG Z12.2 Spec screening [Code] Remove 1 DRG 58 ICD Coding Newsletter - June 2001 May be reproduced Code Indication of Diagnosis Code Title Change* Specification Auth§ Z12.3 Spec screening [Code] Remove 1 DRG Z12.4 Spec screening [Code] Remove 1 DRG Z12.5 Spec screening [Code] Remove 1 DRG Z12.6 Spec screening [Code] Remove 1 DRG Z12.8 Spec screening [Code] Remove 1 DRG Z12.9 Spec screening [Code] Remove 1 DRG Z13.0 Spec screening [Code] Remove 1 DRG Z13.1 Spec screening [Code] Remove 1 DRG Z13.2 Spec screening [Code] Remove 1 DRG Z13.3 Spec screening [Code] Remove 1 DRG Z13.4 Spec screening [Code] Remove 1 DRG Z13.5 Spec screening [Code] Remove 1 DRG Z13.6 Spec screening [Code] Remove 1 DRG Z13.7 Spec screening [Code] Remove 1 DRG Z13.81 Spec screening [Code] Remove 1 DRG Z13.82 Spec screening [Code] Remove 1 DRG Z13.83 Spec screening [Code] Remove 1 DRG Z13.84 Spec screening [Code] Remove 1 DRG Z13.85 Spec screening [Code] Remove 1 DRG Z13.86 Spec screening [Code] Remove 1 DRG Z13.88 Spec screening [Code] Remove 1 DRG Z13.9 Spec screening [Code] Remove 1 DRG Z30.5 IUD First [Age] Replace with Vic 30011 Second [Age] Replace with 41214 Z34.0 Z34.8 Z34.9 Supervision pregnancy Supervision pregnancy Supervision pregnancy [Code] [Code] [Code] Remove 1 DRG Insert 2 Vic Remove 1 DRG Insert 2 Vic Remove 1 DRG Insert 2 Vic Z35.0 Supervision pregnancy [Code] Remove 1 DRG Z35.1 Supervision pregnancy [Code] Remove 1 DRG Z35.2 Supervision pregnancy [Code] Remove 1 DRG Z35.3 Supervision pregnancy [Code] Remove 1 DRG Z35.4 Supervision pregnancy [Code] Remove 1 DRG May be reproduced ICD Coding Newsletter – June 2001 59 Code Indication of Diagnosis Code Title Change* Specification Auth§ Z35.5 Supervision pregnancy [Code] Remove 1 DRG Z35.6 Supervision pregnancy [Code] Remove 1 DRG Z35.7 Supervision pregnancy [Code] Remove 1 DRG Z35.8 Supervision pregnancy [Code] Remove 1 DRG Z35.9 Supervision pregnancy [Code] Remove 1 DRG Insert 2 Vic Z51.5 Palliative care [Code] Insert 1 DRG Z76.1 Supervision healthy infant [Code] Remove 2 Vic Z76.2 Supervision other healthy infant [Code] Remove 2 Vic Z97.5 IUD Second [Age] Replace with Vic 41214 Code Indication of Procedure Code Title Change* Specification Auth§ 35506-01 Removal IUD First [Age] Change to Vic 30011 Second [Age] Change to Vic 41214 45548-01 Removal breast tissue expander [Sex] Change to Vic 4 NCCH Language of Health conference 2001 Several Victorian coders gave papers at the recent NCCH conference – did Victoria proud – and DHS is particularly pleased they are all part of the Victorian Coding Committee. Congratulations to: • Andrea Groom • Kylie Holcombe • Jennie Shepheard • Kathy Wilton 60 ICD Coding Newsletter - June 2001 May be reproduced Coding Standards Advisory Committee Irene Kearsey, Department of Human Services The Coding Standards Advisory Committee (CSAC) was established by the National Centre for Classification in Health (then the National Coding Centre) in 1994. A summary of how CSAC fits into the coding process could be useful to newer readers. The Coding Standards Advisory Committee comprises representatives of the public and private health sectors (a representative of each State/Territory health authority, one from the Commonwealth authority and from the Australian Institute of Health and Welfare, and one from the Australian Private Hospitals Association), the Health Information Management Association of Australia Ltd and the Clinical Coders’ Society of Australia, and a representative of the New Zealand health authority. CSAC’s main function is to authorise the introduction of new and amended ICD-10-AM codes and Australian Coding Standards (ACSs). However, CSAC also: • Advises on activities and products relating to coding and coding quality measures. • Reports to and from organisations and jurisdictions represented on the committee. • Ensures that standards of definition and convention are maintained when ratifying changes to ICD-10-AM and the ACSs. • Reviews public submissions for changes to ICD-10-AM. • Receives feedback from users of coded data on the impact of standards and codes on current data collections. • Ratifies coding advice from the NCCH before publication in Coding Matters. • Recommends future changes to the AR-DRG classification system, as they relate to coding, to departments of health. • Recommends the national adoption of ICD-10-AM modifications on a biennial basis to the National Health Information Management Group. • Provides input to relevant authorities on morbidity and mortality coding related issues such as data edits, coding quality measurement, design or data collection systems. • Provides coding advice on definitions related to relevant classification items in the National Health Data Dictionary to the National Health Data Committee. May be reproduced ICD Coding Newsletter – June 2001 61 • Provides advice on the relationship between ACSs for morbidity coding and rules for cause of death coding to NCCH and the Australian Bureau of Statistics. • Provides advice on other relevant health classification systems. Apart from contributing to the revision process of the classification system, CSAC work also flows into the education process and thus to all coders in Australia and New Zealand. Meetings are usually quarterly and (so far) have been held in the capital cities of the eastern seaboard. Each meeting takes one (long) day but, between meetings, there is a considerable amount of email traffic involving documents for comment. As Victoria’s representative, I consult the Victorian ICD Coding Committee members for advice on my response to CSAC issues and I report back to the Committee on the outcome of CSAC meetings and decisions. From a personal point of view, one valued outcome of CSAC is that we each get to know our opposite numbers in the other health authorities and can contact them on non-coding matters for information and advice. And, of course, the fact that we get to know NCCH staff, and they get to know us, helps resolve issues. As the Department of Human Services’ representative, I can observe how influential a single coder can be in the development of ICD-10-AM: a submission to NCCH can achieve a change if the problem is clearly described, any relevant information is provided, and a clear solution is set out. Coders who find problems in the classification should not think ‘I just have to put up with that’ – they should prepare a submission. While NCCH has a set time for accepting submissions, your ideas should be worked up at the time you find a problem, ready for submission. If you would like a sounding-board, send draft submissions to the Victorian Coding Committee at any time for comment. Because some problems can be fixed between editions of ICD-10-AM, send draft submissions to the Committee at any time and we can forward it to NCCH immediately if appropriate. 62 ICD Coding Newsletter - June 2001 May be reproduced Coding Calendar of Events Date Event Details 29-31 July 2001 HIC 2001: Health Information National Convention Centre, and Health Informatics Canberra Conference Discounted registration for HIMAA members www.hisa.org.au 17-19 August Casemix Conference 2001 Singapore 2001 – A Journey Begins 16-19 September 13th National Casemix 2001 Conference March 2003 NCCH Biennial conference Tan Tock Seng Hospital, Singapore www.ttsh.gov.sg Hobart, Tasmania www.health.gov.au/casemix Victoria For a comprehensive list of health information events, see: www.himaa.org.au/Calendar.html May be reproduced ICD Coding Newsletter – June 2001 63 Victorian ICD Coding Committee Member Profile – Evelyn Robinson Brief Work History After graduating in 1997 from Queensland University of Technology, my first position was as a Regional Health Information Manager at Warrnambool Base Hospital. This position included working at Camperdown and Timboon Hospitals. Following this role, I was employed at Southern Health for approximately two years. After leaving Southern, I worked at Cabrini for a brief period, before commencing my current position as Coding Coordinator at Peninsula Health. In my ‘spare time’ I also work one day a week at The Alfred Hospital. Why did you join the Coding Committee? I found I enjoyed coding and wanted to broaden my own experience and knowledge of ICD coding through being a Committee member. I enjoy trying to solve coding queries, researching difficult topics and helping others with coding problems, and felt I could make a contribution as a Coding Committee member to assist other Victorian coders. What do you see as the challenges for the Coding Committee in the future? To ensure queries are responded to in a timely manner. Endeavouring to keep up with clinical advances in technology, in order to respond to coding queries. Developing and maintaining an electronic format of Coding Committee queries. 64 ICD Coding Newsletter - June 2001 May be reproduced Name your most unusual possession My husband Clive, who is a Furniture Designer, designed and made a very unusual wine rack, which now takes pride of place in our home. How do you cope with stress? Stress + → Coffee Stress +++ → Strong coffee What is your most annoying habit? I asked Clive this and he said there were far too many annoying habits to document here!! Finish this sentence: Never attempt to? Say yes to completion of a ‘Member Profile’ article! From your experience, what hints can you provide to Coders on achieving and maintaining a high level of clinical coding competence? Try to keep up as much as possible with reading all the relevant literature about coding and clinical information. Also, regular liaison with clinicians can prove very useful in improving clinical knowledge. Family Husband Clive. I also come from a large family, having seven sisters and numerous nephews and nieces. Interests Football (Go Bombers!), Cricket and Rugby Union. I also enjoy travelling, both in Australia and overseas, when I can find the time. May be reproduced ICD Coding Newsletter – June 2001 65 Members as at 1 June 2001 Irene Kearsey Convener (Department of Human Services) Nicolette Thein Secretary (Department of Human Services) Sharon Brown Latrobe Regional Hospital Moira Cameron Cabrini Hospital Rhonda Carroll The Alfred Hospital Glenda Cunningham Royal Talbot Rehabilitation Centre Andrea Groom Southern Health Kylie Holcombe St Vincent’s Hospital Susan Peel Yarra Ranges Health Service Evelyn Robinson Peninsula Health Ruth Rundell Barwon Health - The Geelong Hospital Jennie Shepheard La Trobe University representative Kathy Wilton Royal Children’s Hospital Committee’s representative on VACCDI: Pauline Cripps, Box Hill Hospital Next Meetings Department of Human Services, 10.00 am, 555 Collins Street, Melbourne: • Tuesday 3 July 2001 • Tuesday 7 August 2001 66 ICD Coding Newsletter - June 2001 May be reproduced On a Lighter Note After discharging the last patient in the ER, I started for the sleep room at about 2am. The nurse told me a moderately intoxicated man was coming in with a stuck contact lens. She offered to take it out with a suction lens remover and have me sign the chart in the morning. Half an hour later the ringing telephone at the bedside told me she hadn’t succeeded. Examination of the patient’s eyes produced an immediate explanation: Neither eye had a contact lens in it. The patient had tried unsuccessfully to remove his cornea with his fingernails, and the nurse had failed to improve the situation with the suction cup. Unpersuaded by the facts, the patient repeatedly grasped his cornea between his thumb and middle fingernails and pulled until his grip slipped off the tented membrane. Each attempt produced the same exclamation, ‘Damn, that hurts. See I can get it out to here but it always pops back.’ Finally, I asked to see his contact lens case. I showed him the lenses in his case and asked, ‘Whose lenses are these?’ Only then did he reluctantly admit he must have taken them out and forgotten. Two Tylenol 3’s got him through the night. A follow up exam the next day revealed normal vision, healing corneal abrasions, a large subconjunctival haemorrhage, and an ugly hangover. May be reproduced ICD Coding Newsletter – June 2001 67 Alphabetic Index to Victorian ICD-10-AM Coding Advice: July 1999 – June 2001 ACS Australian Coding Standard CF Coding Feature CT Coding Tip HDSS # - MM/YY HDSS Bulletin Vic Addition Victorian Additions to Australian Coding Standards *Please refer to the original source for the page number of a query Advice Descriptor Source ID -A#1485 Ablation, radiofrequency, liver November 1999 #1572 Ablation, percutaneous transluminal myocardial septal August 2000 #1612 Abscess, abdominal wall November 2000 #1482 Abscess, submandibular, incision and drainage of May 2000 #1494 Abstraction guidelines, general ACS 0010 February 2000 #1479 ACS 0002 Additional diagnoses November 1999 Item 13.1 ACS 0002 Additional diagnoses (VAED) HDSS 13 - 07/00 (replaces HDSS 2 - 07/99) #1494 ACS 0010 General abstraction guidelines February 2000 #1529 ACS 0012 Suspected Conditions May 2000 #1689 ACS 0012 Suspected Condition (perforation) June 2001 CF ACS 0031 Anaesthetics November 2000 #1659 ACS 0226 Prostatic Cancer June 2001 #1468 ACS 0237 Recurrence of primary malignancy & 0234 February 2000 Contiguous sites & (NCCH query 884) 68 ICD Coding Newsletter - June 2001 May be reproduced Advice Descriptor Source ACS 0909 Additional procedures performed in June 2001 ID #1691 conjunction with CABGs #1622 ACS 1002 Asthma June 2001 #1662 ACS 2103 Admission for convalesce/aftercare June 2001 #1580 Acute pulmonary oedema November 2000 #1479 Additional diagnoses, ACS 0002 November 1999 Item 13.1 Additional diagnoses, ACS 0002 (VAED) HDSS 13 – 07/00 (replaces HDSS 2 - 07/99) #1691 Additional procedures performed in conjunction with June 2001 CABGs, ACS 0909 #1507 Adjustment, ureteric memokath February 2000 #1662 Admission for convalescence/aftercare, ACS 2103 June 2001 CF Admissions principally for a specific treatment for February 2000 which there is a Z code #1472 Alcohol dependence, past history February 2000 #1564 Amplatzer duct occluder, insertion of August 2000 #1520 Amputation and open fractures May 2000 #1517 Amputation, distal 3rd and 4th fingers with May 2000 reattachment #1466 Anaemia, post operative February 2000 CF Anaesthesia, ACS 0031 November 2000 #1665 Anaesthetic procedures June 2001 CF Anaesthetics June 2000 #1562 Angiograms, CT August 2000 #1490 Apraxia, senile gait May 2000 CF Assigning code prefixes June 2000 #1622 Asthma, ACS 1002 June 2001 #1654 Autologous Chondrocyte Implantation (ACI) June 2001 -B#1470 Biopsy, transjugular liver May be reproduced May 2000 ICD Coding Newsletter – June 2001 69 Descriptor Source CF Blood transfusions June 2000 #1499 Brachytherapy and radiotherapy November 1999 #1480 Brachytherapy, intraluminal November 1999 #1585 Brachytherapy, intra-coronary August 2000 #1615 Breast lesion, wide local excision of November 2000 #1568 Bypass using vein, ilio-femoral (PTFE) August 2000 Advice ID -C#1478 Calciphylaxis November 1999 CF Cancelled surgery June 2000 #1601 Cancer site codes November 2000 #1558 Capsulectomy of shoulder August 2000 #1571 Carbon fibre resurfacing August 2000 #1589 Chemotherapy November 2000 #1648 Chemotherapy and device loading June 2001 Item 6.1 Chemotherapy - admission for HDSS 6 -10/99 #1537 Chemotherapy cancelled due to URTI August 2000 CF Chemotherapy, intraperitoneal August 1999 CF Cochlear implant procedure May 2000 CF Coding idiosyncratic episodes February 2000 CF Coding of clinical information recorded by clinicians August 2000 other than medical officers #1541 Coffin-Lowry syndrome May 2000 #1636 Colonoscopy: investigation or finding June 2001 #1532 Conscious state, decreased May 2000 CF Continuous ventilatory support August 2000 0029 Contracted procedures, coding of Vic Addition #1624 COAD and pneumonia, sequencing of November 2000 #1538 COPD, infective exacerbation of, with emphysema May 2000 #1492 Coronary artery disease in stent and transplanted heart November 1999 70 ICD Coding Newsletter - June 2001 May be reproduced Descriptor Source #1510 Coroner’s report/Post mortem coding February 2000 #1562 CT Angiograms August 2000 #1613 Cyst, mullerian November 2000 #1515 Cystadenoma of ovary (borderline malignancy) February 2000 Advice ID -D#1532 Decreased conscious state May 2000 #1472 Dependence, alcohol, past history February 2000 #1618 Dependence, opioid November 2000 #1551 Dependency, benzhexol May 2000 #1513 Depression, postnatal February 2000 CF Diabetes November 2000 #1597 Diabetes – periungual telangiectasia November 2000 CT Diabetes with diarrhoea November 2000 (replaces CF June 2000) CF Diabetes with multiple complications August 1999 #1548 Diastasis recti post delivery May 2000 #1539 Diathermy of penile wart May 2000 #1566 Dimple, sacral May 2000 #1542 Disorder, schizoaffective, hypomanic May 2000 #1625 Drainage, cyst, liver, ultrasound guided (percutaneous) November 2000 #1484 Dysplasia, Otospondylomegaepiphyseal August 2000 -E#1538 Emphysema with infective exacerbation of COPD May 2000 #1593 Epidural during labour November 2000 #1555 Epilepsy and status epilepticus August 2000 #1685 Ethanol injection June 2001 #1560 Excision/removal of osteophytes August 2000 #1615 Excision, wide local, breast lesion November 2000 #1584 Excision, wide, of neoplasm August 2000 May be reproduced ICD Coding Newsletter – June 2001 71 Advice Descriptor Source External cause code - Scooters June 2001 ID #1669 -F#1676 Follow-up gastroscopy June 2001 #1520 Fractures, open and amputation May 2000 #1540 Fundoplication, Nissen (laparoscopic), revision of May 2000 -G#1489 GAMP (ACS 1912 Sequelae of injuries, poisonings, toxic November 1999 effects and other external causes and 1906 Current and old injuries) #1530 Gastric lap bands November 2000 #1462 Geriatric Evaluation and Management Program coding November 1999 #1501 Group B strep. status, (unknown) February 2000 #1563 Group B strep. carrier in pregnancy August 2000 #1677 Grouping of laparoscopy codes June 2001 -H#1578 Hemicolectomy and LUSCS August 2000 #1599 Hepatic portal vein pressure/post pressure studies November 2000 #1582 Hepatitis B vaccinations in newborns August 2000 #1573 Hepatitis B vaccine August 2000 #1609 Hernia, ventral or epigastric November 2000 #1623 Hysterectomy, vaginal, laparoscopically assisted November 2000 -I#1621 I24.0, use of code November 2000 #1568 Ilio-femoral bypass using vein (PTFE) August 2000 #1500 Impacted tooth, surgical removal November 1999 #1476 Implant, breast, re-inflation of May 2000 CF Implant, cochlear May 2000 #1546 Implant, facial, removal of November 2000 #1569 Implant, iridium, insertion of August 2000 72 ICD Coding Newsletter - June 2001 May be reproduced Descriptor Source #1495 Implant, loop recorder February 2000 #1552 Implant, nose (silicon), removal of May 2000 #1579 Implant, silastic, thyroplasty August 2000 #1482 Incision and drainage of submandibular abscess May 2000 CF Infusion, isolated limb November 1999 #1565 Infusion pump for pain management August 2000 #1564 Insertion of amplatzer duct occluder August 2000 #1569 Insertion of iridium implant August 2000 #1598 Insertion of pleuroperitoneal shunt November 2000 #1567 Insertion, transfemoral aortic stent August 2000 #1585 Intra-coronary brachytherapy August 2000 CF Intraocular lens guide November Advice ID 2000 (replaces CF August 2000) #1575 Intravascular ultrasound August 2000 -L#1475 Lacerated bowel and bladder during LUSCS May 2000 #1651 Laparoscopic cholecystectomy to open cholecystectomy June 2001 with exploration of CBD #1677 Laparoscopy codes, grouping of June 2001 #1504 Lavage, arthroscopic, of shoulder February 2000 #1493 LeFort Osteotomy November 1999 #1615 Lesion, breast, wide local excision of November 2000 #1638 Low birthweight June 2001 #1680 Low K+ June 2001 #1578 LUSCS and hemicolectomy August 2000 -M#1600 Meconium in liquor November 2000 #1644 Mechanical complication of ventricular shunt June 2001 #1543 Melanotic macule, lip-labial May 2000 May be reproduced ICD Coding Newsletter – June 2001 73 Descriptor Source #1587 Mesocaval shunt, thrombectomy of August 2000 #1545 Metastatic spread May 2000 CF Minor Trauma Coding June 2001 0233 Morphology Vic Addition #1664 Musculoskeletal chest pain June 2001 #1473 Myelodysplastic syndrome with anaemia November 1999 Advice ID -N#1584 Neoplasm, wide excision of August 2000 #1540 Nissen fundoplication, laparoscopic, revision of May 2000 -O#1661 Obstetrics, principal diagnosis June 2001 #1519 Obstruction, upper airway February 2000 #1580 Oedema, acute pulmonary November 2000 #1618 Opioid dependence November 2000 0030 Organ procurement Vic Addition #1671 Osseous metaplasia and solar lentigo June 2001 #1560 Osteophytes, excision/removal of August 2000 #1693 Osteotomies with internal fixation (bilateral maxilla and June 2001 mandible) #1484 Otospondylomegaepiphyseal dysplasia August 2000 #1496 Overwarfarinisation/stabilisation of INR February 2000 -P#1620 Pacemaker recall November 2000 #1663 Palliative Care June 2001 #1572 Percutaneous transluminal myocardial septal ablation August 2000 #1597 Periungual telangiectasia in diabetes November 2000 #1486 Photodynamic therapy (PDT) May 2000 CF Place of occurrence June 2000 #1598 Pleuroperitoneal shunt insertion November 2000 74 ICD Coding Newsletter - June 2001 May be reproduced Descriptor Source #1624 Pneumonia and COAD, sequencing of November 2000 CF Poisoning and adverse effects of drugs August 2000 #1642 Post infarction angina June 2001 #1650 Post-procedural complications June 2001 #1510 Post mortem/Coroner’s report coding February 2000 #1527 Pre-admission tests May 2000 CF Prefixes, assignment of June 2000 Prefix.1 Prefixes for diagnoses Vic Addition Prefix.2 Prefixes for obstetric codes Vic Addition #1583 Pregnancy following tubal ligation August 2000 #1561 Premature labour, patient transferred to another hospital November 2000 #1661 Principal diagnosis in Obstetrics June 2001 #1628 Principal procedure selection November 2000 #1659 Prostatic Cancer, ACS 0226 June 2001 #1568 PTFE (ilio-femoral bypass using vein) August 2000 #1599 Pressure/portal pressure studies, hepatic portal vein November 2000 #1580 Pulmonary oedema, acute November 2000 Advice ID -R#1485 Radiofrequency ablation of liver November 1999 0229 Radiotherapy Vic Addition #1499 Radiotherapy and brachytherapy November 1999 #1518 Reattachment of finger February 2000 #1517 Reattachment, amputated distal 3rd and 4th fingers May 2000 #1468 Recurrence of primary malignancy (ACS 0237) & 0234 February 2000 Contiguous sites & (NCCH query 884) 2104 Rehabilitation Vic Addition #1476 Re-inflation of breast implant May 2000 #1552 Removal of silicon implant from nose May 2000 #1535 Removal, bath drain from fingers May 2000 May be reproduced ICD Coding Newsletter – June 2001 75 Descriptor Source #1560 Removal/excision of osteophytes August 2000 #1546 Removal, facial implants November 2000 #1511 Repair AAA with endoluminal bifurcation graft February 2000 #1516 Replacement of progesterone ‘IUD’ February 2000 #1571 Resurfacing, carbon fibre August 2000 #1641 Retained products of conception June 2001 #1540 Revision of a laparoscopic Nissen Fundoplication May 2000 Advice ID -S#1542 Schizoaffective disorder, hypomanic May 2000 #1544 Schizophrenia, chronic May 2000 #1669 Scooters - External cause code June 2001 CF Screening for specific disorders August 2000 #1628 Selection principal procedure November 2000 CF Sequencing guidelines June 2000 #1624 Sequencing of COAD and pneumonia November 2000 #1587 Shunt, mesocaval, thrombectomy of August 2000 #1598 Shunt, pleuroperitoneal, insertion of November 2000 #1579 Silastic implant thyroplasty August 2000 #1658 Smoking related COPD June 2001 #1671 Solar lentigo and osseous metaplasia June 2001 #1555 Status epilepticus and epilepsy August 2000 #1487 Stenosis, lumbar spinal November 1999 #1506 Stent, endobronchial February 2000 #1567 Stent, transfemoral aortic, insertion of August 2000 #1465 Sternal wires May 2000 #1501 Strep. Group B status, (unknown) February 2000 #1563 Strep. Group B carrier in pregnancy August 2000 #1599 Studies, pressure/portal pressure, hepatic protal vein November 2000 #1559 Study, WADA August 2000 76 ICD Coding Newsletter - June 2001 May be reproduced Descriptor Source #1463 Sudden cardiac death November 1999 #1529 Suspected conditions, ACS 0012 May 2000 #1689 Suspected condition (perforation), ACS 0012 June 2001 #1541 Syndrome, Coffin-Lowry May 2000 Advice ID -T#1553 Tamoxifen for breast cancer May 2000 #1597 Telangiectasia, periungual in diabetes November 2000 #1527 Tests, pre-admission May 2000 #1486 Therapy, photodynamic May 2000 #1587 Thrombectomy of mesocaval shunt August 2000 #1503 Thrombophlebitis, post operative February 2000 #1579 Thyroplasty, silastic implant August 2000 CF Tracheostomy June 2000 CF Transfusions, blood June 2000 #1470 Transjugular liver biopsy May 2000 -U#1625 Ultrasound guided percutaneous drainage liver cyst November 2000 #1575 Ultrasound, intravascular August 2000 Item 14.3 Unacceptable obstetric diagnosis combination HDSS 14 – 07/00 (replaces CF June 2000) #1682 Underlying condition June 2001 #1501 Unknown Group B. strep status February 2000 -V#1582 Vaccination, Hepatitis B in newborns August 2000 #1573 Vaccine, Hepatitis B August 2000 CF Ventilatory support, continuous August 2000 0029 VIC Addition - Coding of contracted procedures Vic Addition 0233 VIC Addition - Morphology Vic Addition 0030 VIC Addition - Organ procurement Vic Addition May be reproduced ICD Coding Newsletter – June 2001 77 Descriptor Source Prefix.1 VIC Addition - Prefixes for diagnoses Vic Addition Prefix.2 VIC Addition - Prefixes for obstetric codes Vic Addition 0229 VIC Addition - Radiotherapy Vic Addition 2104 VIC Addition - Rehabilitation Vic Addition Advice ID -W#1559 WADA study August 2000 #1539 Wart, penile, diathermy of May 2000 #1471 Warts, vulval, vaginal and perianal warts May 2000 #1584 Wide excision of neoplasm August 2000 -X#1576 Xanthelasma August 2000 -ZCF 78 Z codes – Admissions principally for a specific treatment February 2000 ICD Coding Newsletter - June 2001 May be reproduced Abbreviations ACS Australian Coding Standard ADX Additional Diagnosis AN-DRG Australian National Diagnosis Related Groups AR-DRG Australian Refined Diagnosis Related Groups CABG Coronary Artery Bypass Graft D&C Dilation and Curettage DHS Department of Human Services GA General Anaesthetic HDSS Health Data Standards and Systems HIMAA Health Information Management Association of Australia HMA Healthcare Management Advisors Pty Ltd ICD-9-CM International Classification of Diseases - 9th Revision – Clinical Modification ICD-10-AM Statistical Classification of Diseases and Related Health Problems, 10th Revision, Australian Modification LUSCS Lower Uterine Segment Caesarean Section NCCH National Centre for Classification in Health RPOC Retained Products of Conception TOE Transoesophageal Echocardiogram VAED Victorian Admitted Episodes Dataset VEMD Victorian Emergency Minimum Dataset VICC Victorian ICD Coding Committee May be reproduced ICD Coding Newsletter – June 2001 79

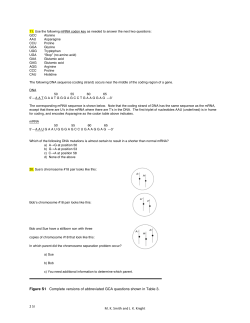








© Copyright 2026