
Nonoperative and Operative Treatments for Rotator Cuff Tears
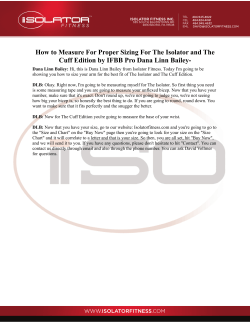
Review Annals of Internal Medicine Systematic Review: Nonoperative and Operative Treatments for Rotator Cuff Tears Jennifer C. Seida, MPH; Claire LeBlanc, MD; Janine R. Schouten, BSc; Shima S. Mousavi, MD; Lisa Hartling, PhD; Ben Vandermeer, MSc; Lisa Tjosvold, MLIS; and David M. Sheps, MD, MSc Background: Many approaches exist for managing rotator cuff tears. Purpose: To compare the benefits and harms of nonoperative and operative interventions on clinically important outcomes in adults with rotator cuff tears. Data Sources: 12 electronic databases (1990 to September 2009), gray literature, trial registries, and reference lists were searched. ate quality. Reported functional outcomes did not differ between open versus mini-open repair, mini-open versus arthroscopic repair, arthroscopic repair with versus without acromioplasty, or single-row versus double-row fixation. Earlier return to work was reported for mini-open repair versus open repair and for continuous passive motion with physical therapy versus physical therapy alone. Open repairs showed greater improvement in function than did arthroscopic debridement. Complication rates were low across all interventions. Study Selection: Controlled and uncontrolled studies that assessed nonoperative or operative treatments or postoperative rehabilitation for adults with confirmed rotator cuff tears were included. Operative studies in English-language publications and nonoperative and postoperative rehabilitation studies in English, French, or German were considered. Studies were assessed in duplicate. Limitations: Limited evidence, which was often of low quality, precluded conclusions for most comparisons. Language restrictions may have excluded some relevant studies, and selective outcome reporting may have introduced bias. Data Extraction: 2 reviewers assessed risk for bias by using the Cochrane Risk of Bias tool and the Newcastle–Ottawa Scale. One reviewer rated the evidence by using a modified GRADE (Grading of Recommendations Assessment, Development, and Evaluation) approach. Data were extracted by one reviewer and verified by another. Primary Funding Source: Agency for Healthcare Research and Quality. Data Synthesis: 137 studies met eligibility criteria. All trials had high risk for bias. Cohort and uncontrolled studies were of moder- T he rotator cuff comprises 4 muscle tendon units that stabilize the humeral head within the shoulder joint and aid in moving the upper extremity (1). “Rotator cuff tear” refers to partial or full discontinuation of 1 or more of these units due to traumatic injury or degeneration. Incidence increases with age. Approximately 54% of adults older than 60 years have a partial or complete rotator cuff tear, compared with only 4% of those aged 40 to 60 years (2). Symptoms include pain, weakness, and limitation of motion (1). Both nonoperative and operative treatments are used to relieve pain and restore movement and function of the shoulder (3). Most patients initially undergo 6 weeks to 3 months of nonoperative treatment, which may consist of Conclusion: Evidence on the comparative effectiveness and harms of various operative and nonoperative treatments for rotator cuff tears is limited and inconclusive. Ann Intern Med. 2010;153:246-255. For author affiliations, see end of text. This article was published at www.annals.org on 6 July 2010. www.annals.org combinations of oral medications and injections; rest from activity; passive and active exercise; and such therapies as heat, cold, or ultrasonography. Failing nonoperative treatment, the cuff may be surgically repaired by using an open, mini-open, or arthroscopic approach. Various postoperative rehabilitation programs can help restore range of motion, strength, and function. Earlier operative repair may result in better patient outcomes, earlier return to work, and decreased costs (4, 5). Patients and clinicians struggle with when to abort nonoperative treatment in favor of surgery. The relative effectiveness of the various nonoperative and operative treatment options for patients with rotator cuff tears remains uncertain. Our comparative effectiveness review examines the relative effectiveness and safety of all nonoperative and operative treatments for rotator cuff tears in adults. See also: Print Editors’ Notes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 247 Web-Only Appendix Tables CME quiz Conversion of graphics into slides 246 © 2010 American College of Physicians METHODS We prospectively developed and followed a research protocol. An external panel of content experts provided input in formulating the key questions and identifying interventions and outcomes of interest. The full evidence report, including search strategies and evidence tables, is available at www .effectivehealthcare.ahrq.gov/reports/final.cfm. Nonoperative and Operative Treatments for Rotator Cuff Tears We investigated early versus late surgical repair, operative interventions, nonoperative interventions, postoperative rehabilitation, and operative versus nonoperative treatments. We also examined complications and prognostic factors in all included studies. Data Sources and Searches We systematically searched MEDLINE, EMBASE, Evidence-Based Medicine Reviews, the Cochrane Library, AMED, CINAHL, SPORTDiscus with Full Text, Academic Search Elite, Health Source, Science Citation Index Expanded (via Web of Science), Scopus, BIOSIS Previews, CRISP, Current Controlled Trials, ClinicalTrials.gov, and the Nederlands Trial Register from January 1990 to September 2009. Appendix Table 1, available at www.annals .org, lists our MEDLINE search strategy. We also handsearched abstracts from recent scientific meetings and reference lists of relevant reviews to identify additional studies. No language restrictions were applied. Study Selection Trials, cohort studies, and prospective uncontrolled studies that evaluated any nonoperative or operative treatment or postoperative rehabilitation for adults with confirmed rotator cuff tears were eligible for inclusion. We defined uncontrolled studies as single-group studies that reported baseline and follow-up data. For the purposes of this review, we also considered cohort studies that compared the effectiveness of only 1 intervention across 2 patient populations (such as open repair in older versus younger patients) to be uncontrolled studies. Confirmed tears were defined as partial- or full-thickness lesions diagnosed by imaging or intraoperative findings. Studies were required to enroll a minimum of 11 participants and report at least 1 of the following outcomes: quality of life, function, time to return to work or activity, pain, range of motion, or strength. Operative studies were required to follow participants for at least 12 months; no follow-up criteria were set for nonoperative or postoperative rehabilitation studies. We included operative studies published in English only because of a lack of translation resources. We considered English-, German-, and French-language publications for studies that examined nonoperative treatments and postoperative rehabilitation, because the literature on these interventions was sparse. One reviewer screened titles, keywords, and abstracts for broad relevance. Two independent reviewers assessed the full publication of potentially relevant studies, and discrepancies were resolved by consensus. Data Extraction and Quality Assessment One reviewer extracted data by using a standardized form, and a second reviewer verified the data for accuracy and completeness. Reviewers resolved discrepancies by consensus or through a third party. Two reviewers independently assessed the methodological quality of included studies. We evaluated trials by using the Cochrane Risk of Bias tool (6) and observational www.annals.org Review Context Multiple therapies are available to treat rotator cuff tears. Contribution This systematic review of 137 studies found evidence that patients with rotator cuff tears experienced improvements in function after undergoing any of several operative procedures or nonoperative therapy. Few complications were seen with the surgical procedures. Sparse comparative data precluded recommendations for a superior treatment approach. Caution The amount and strength of available evidence was low for many therapies. Implication Several therapies might benefit patients with rotator cuff tears and are associated with a reasonably low risk for harm, but we do not yet know the most beneficial therapy. —The Editors analytic studies by using a modified Newcastle–Ottawa Scale (7). Uncontrolled studies were assessed for consecutive enrollment, complete outcome data, and standardized or independent approach to outcome assessment. The funding sources were recorded for all studies. One reviewer (Dr. Hartling) graded the strength of evidence according to published guidelines (8, 9) for the 4 key outcomes of quality of life, functional outcomes, time to return to work, and cuff integrity. Four domains were assessed: risk for bias (low, medium, or high), consistency (no inconsistency, inconsistency present, unknown, or not applicable), directness (direct or indirect), and precision (precise or imprecise). Data Synthesis and Analysis We summarized the included studies qualitatively. Controlled studies were combined by using meta-analysis if the study design, study population, interventions being compared, and outcomes were sufficiently similar. For continuous outcomes measured on different scales across studies, we calculated a standardized mean difference for the pooled estimate. Results were combined by using randomeffects models, and statistical heterogeneity was quantified by using the I2 statistic (10, 11). Role of the Funding Source The Agency for Healthcare Research and Quality funded this review and provided feedback on the question formulation and decision to submit for publication but was not involved in the searches, selection, data extraction, data analysis, or interpretation of the findings. 17 August 2010 Annals of Internal Medicine Volume 153 • Number 4 247 Review Nonoperative and Operative Treatments for Rotator Cuff Tears RESULTS We identified 5677 citations and included 137 studies in our review (Figure). Appendix Table 2, available at www.annals.org, lists included and excluded studies, along with the reasons for exclusion. Table 1 summarizes general study characteristics. Number of study participants ranged from 12 to 224 (median, 55; interquartile range [IQR], 33 to 93). Mean age ranged from 41.2 to 80 years. Appendix Table 3, available at www.annals.org, provides further study characteristics. Methodological Quality All randomized, controlled trials (RCTs) and controlled clinical trials had a high risk for bias. The most common sources of potential bias were inadequate blinding, inadequate allocation concealment, and incomplete outcome data. The methodological quality of the cohort studies was moderate, with a median score of 5 out of 8 stars (IQR, 4 to 6 stars). Limitations in study design included lack of independent, blinded outcome assessment Figure. Literature search and selection. Citations retrieved from electronic literature searches (n = 5677) References selected for further examination of titles and abstracts (n = 1008) Potentially relevant references identified by hand searches (n = 2) Not retrieved (n = 29) Articles retrieved and evaluated in full for inclusion (n = 981) Excluded (n = 844) Ineligible study design: 182 Not primary research: 153 Not confirmed rotator cuff tear: 107 No baseline data: 89 Non–English-language study: 79 Primary intention not treatment of rotator cuff tear: 59 Not intervention of interest: 47 No numeric outcome of interest: 39 Enrolled ≤10 participants: 34 Follow-up <12 mo: 23 Not population of interest: 15 Multiple publication: 13 Published before 1990: 4 Included (n = 137) 248 17 August 2010 Annals of Internal Medicine Volume 153 • Number 4 and failure to adequately control for potential confounders. Uncontrolled studies generally had moderate quality, with consecutive enrollment, adequate follow-up, and standardized outcome assessment reported in 63%, 77%, and 44% of studies, respectively. Funding sources were reported for only 49 studies (36%). Appendix Table 4, available at www.annals .org, details the methodological quality of each study. Early Versus Late Surgical Repair One RCT (12), which compared early versus late surgical repair after failed nonoperative treatment, found superior mean functional outcome scores with early repair but did not report the statistical significance of this difference. The groups did not significantly differ in cuff integrity. Overall, the evidence was too limited to make a conclusion. Table 2 summarizes the strength of the evidence for all comparisons. Operative and Postoperative Rehabilitation Interventions One hundred thirteen studies examined operative interventions, and 11 examined postoperative rehabilitation. Studies that assessed surgery were categorized as comparing an operative approach (such as open, mini-open, or arthroscopic), a technique (such as suture, anchor type, or configuration), or augmentation. Table 2 summarizes the strength of the evidence for these comparisons. Operative Approaches Operative approaches were evaluated in 32 controlled and 58 uncontrolled studies. The evidence on the specific comparisons from the trials and cohort studies is examined here. The uncontrolled studies consistently reported functional improvement from preoperative to postoperative scores, regardless of the approach (open, mini-open, or arthroscopic), sample size, or outcome measure. Open Versus Mini-open Repair. One RCT (13) and 2 retrospective cohort studies (14, 15) compared open with mini-open repair. Quality of life (13), function (13–15), cuff integrity (14, 15), and range of motion (13, 14) did not significantly differ between the groups. The cohort studies demonstrated statistically significant benefit from mini-open repairs, with patients returning to work or activity approximately 1 month earlier (mean difference, 1.08 months [95% CI, 0.63 to 1.52 months]) and having greater abduction strength (14). Mini-open Versus Arthroscopic Repair. Ten studies (1 controlled clinical trial [16], 2 prospective cohort studies [17, 18], and 7 retrospective cohort studies [19 –25]) compared mini-open with arthroscopic repair. Function did not significantly differ, either for the controlled clinical trial or the pooled estimate of 9 cohort studies (standardized mean difference, ⫺0.11 [CI, ⫺0.28 to 0.06]). Cuff integrity (20, 23), pain (16, 18, 23, 24), range of motion (16, 18, 20, 23, 24), and strength (16, 24) also did not differ. Open Versus Arthroscopic Repair. One prospective cohort study (26) and 2 retrospective cohort studies (27, 28) compared open versus arthroscopic rotator cuff repair. www.annals.org Nonoperative and Operative Treatments for Rotator Cuff Tears A pooled estimate showed no differences in function (standardized mean difference, ⫺0.49 [CI, ⫺1.12 to 0.13]); however, we found significant statistical heterogeneity among the 3 studies (I2 ⫽ 83%). Patient age, type of tear, and tear size did not seem to differ among the studies; the heterogeneity may be due to differences in the study design (prospective vs. retrospective) or length of follow-up. One study (28) found no difference in pain or cuff integrity but statistically significant differences in favor of arthroscopic repair for external rotation range of motion and strength and supraspinatus strength. Two prospective cohort studies that compared open or mini-open repair with arthroscopic repair found no difference in function (29, 30) or cuff integrity (29). Arthroscopic repair was favored for pain relief in one study (30), whereas open or mini-open repair was favored for external rotation in the other (29). Open Repair Versus Debridement. Two controlled clinical trials (31, 32) and 2 retrospective cohort studies (33, 34) compared open repair with debridement. Improvement in function was statistically significant for the repair groups (standardized mean difference for trials, 0.59 [CI, 0.15 to 1.03]; for cohort studies, 1.00 [CI, 0.11 to 1.90]); however, we found substantial heterogeneity among the cohort studies (I2 ⫽ 79%). The statistical heterogeneity among studies may be explained by the different study designs (prospective vs. retrospective) or tear sizes (small or medium tears vs. massive tears). The magnitude of the difference varied across studies from an absolute difference of 2.2 on a 35-point scale (32) to 11.5 on an 83-point scale (33). One cohort study (33) showed a statistically significant shorter time to maximum range of motion with arthroscopic debridement (3.2 vs. 6.8 months). Arthroscopic Repair Versus Acromioplasty. Two RCTs (35, 36) compared arthroscopic rotator cuff repair with acromioplasty versus repair without acromioplasty. One prospective cohort study (37) compared arthroscopic repair with acromioplasty alone. Function did not differ between the groups. Other Approaches. Seven studies compared different operative approaches: biceps tenotomy versus tenodesis (38), rotator cuff repair versus palliative treatment (39), arthroscopic rotator cuff repair plus superior labral anterior-to-posterior lesion repair versus arthroscopic rotator cuff repair plus biceps tenotomy (40), arthroscopic rotator cuff repair plus tenodesis with versus without proximal biceps detachment (41), arthroscopic debridement with versus without tenotomy (42), complete open repair versus partial open repair versus debridement (43), and open repair plus classic acromioplasty versus repair plus modified acromioplasty (44). We found few clinically important differences between groups across all studies. No differences in function were observed for 5 of the comparisons (38, 41– 44). One study (39) found a statistically significant difference in function that favored rotator cuff repair more than palliative treatment. Another (40) showed www.annals.org Review Table 1. Descriptive Characteristics of Included Studies Characteristic Study design Controlled Uncontrolled Publication type Peer-reviewed article Abstract Country of corresponding author United States Europe Asia Other Language of publication English German French Studies, n 66 (21 RCTs; 6 CCTs; 13 PCs; 26 RCs) 71 133 4 49 56 18 14 130 4 3 Questions* 1. Early vs. late surgical repair 2. Operative interventions 3. 4. 5. 6. 1 RCT† 113 (12 RCTs; 5 CCTs; 11 PCs; 22 RCs‡; 63 uncontrolled) Postoperative rehabilitation therapy 11 (6 RCTs; 1 CCT; 1 PC; 2 RCs; 1 uncontrolled) Nonoperative interventions 10 (1 RCT; 2 RCs‡; 7 uncontrolled) Nonoperative vs. operative interventions 5 (2 RCTs†; 1 PC; 2 RCs‡) Complications 85 Prognostic factors 72 CCT ⫽ controlled clinical trial; PC ⫽ prospective cohort study; RC ⫽ retrospective cohort study; RCT ⫽ randomized, controlled trial. * Questions were not mutually exclusive. All studies that examined complications or prognostic factors also addressed an effectiveness question (questions 1 to 4). † One study (12) addressed questions 1 and 4. ‡ One study (33) compared 4 treatment groups (2 operative and 2 nonoperative) and is presented for questions 2, 3, and 4. greater functional improvement with arthroscopic rotator cuff repair with biceps tenotomy than with arthroscopic rotator cuff repair plus superior labral anterior-to-posterior lesion repair. However, the absolute difference of 4 points on the 35-point scale is of questionable clinical importance. Range of motion (38, 41, 43) and strength (43) did not significantly differ. Operative Techniques Fifteen controlled studies examined operative techniques. Six studies (4 RCTs [45– 48] and 2 cohort studies [49, 50]) compared single-row suture anchor repairs with double-row repairs. For function, the pooled estimate showed statistically significant improvement that favored double-row fixation (standardized mean difference for trials, 0.55 [CI, 0.02 to 1.07]; for cohort studies, 0.78 [CI, 0.46 to 1.11]). We found considerable heterogeneity among the trials (P ⫽ 0.008; I2 ⫽ 75%) but not among the cohort studies. The studies were similar in design, patient age, and tear type; the heterogeneity may be attributable to tear size, which ranged from small in one study (45) 17 August 2010 Annals of Internal Medicine Volume 153 • Number 4 249 Review Nonoperative and Operative Treatments for Rotator Cuff Tears Table 2. Summary of Strength of Evidence for Nonoperative and Operative Interventions Comparison Studies, n Strength of Evidence Summary Early vs. late repair Operative approaches Open RCR vs. mini-open RCR 1 32 3 Low The evidence was too limited to make a conclusion. Moderate Moderate Low Moderate Low Moderate Moderate No difference for function. Some evidence for earlier return to work or activity (by approximately 1 month) with mini-open repairs. The evidence was too limited to make a conclusion for health-related quality of life or cuff integrity. No difference in function or cuff integrity. The evidence was too limited to make a conclusion. No difference in function. The evidence was too limited to make a conclusion for cuff integrity. Some evidence for greater improvement in function for open RCR. No difference in function. Low Low The evidence was too limited to make a conclusion. The evidence was too limited to make a conclusion. Moderate No clinically important difference for function and no difference for cuff integrity. No difference in cuff integrity. The evidence was too limited to make a conclusion for function. The evidence was too limited to make a conclusion. The evidence was too limited to make a conclusion. Low Mini-open RCR vs. arthroscopic RCR Open RCR vs. arthroscopic RCR Open or mini-open RCR vs. arthroscopic RCR Open RCR vs. debridement Arthroscopic RCR with acromioplasty vs. without acromioplasty Arthroscopic RCR vs. acromioplasty alone Other approaches Operative techniques Single-row vs. double-row suture anchor fixation Mattress locking vs. simple stitch Other techniques Operative augmentation Postoperative rehabilitation Continuous passive motion with PT vs. PT alone Other postoperative rehabilitation Nonoperative interventions Nonoperative vs. operative treatment 10 3 2 4 2 1 7 15 6 2 7 3 10 3 7 3 5 Moderate Low Low Low Moderate Low Low Low No clinical or statistical difference in function. Some evidence for earlier return to work with continuous passive motion. The evidence was too limited to make a conclusion. The evidence was too limited to make a conclusion. The evidence was too limited to make a conclusion. PT ⫽ physical therapy; RCR ⫽ rotator cuff repair. to massive in another (47). Although the meta-analysis showed statistical significance, the absolute differences in the change scores were small (5 points on a 100-point scale) (50) and therefore of questionable clinical relevance. For cuff integrity, the pooled risk ratio from 3 trials (45– 47) showed no difference between groups (risk ratio, 1.20 [CI, 0.86 to 1.68]). However, 1 cohort study (50) found a statistically significant difference that favored double-row fixation. Measures of health-related quality of life (45), return to work (46), range of motion (47), and strength (45, 48, 49) did not differ across techniques. Of the 2 studies that compared the effectiveness of mattress stitch versus simple stitch, 1 controlled clinical trial (51) favored mattress stitch for functional outcomes. A prospective cohort study showed no difference between groups (52). Cuff integrity (51, 52), pain (51, 52), and range of motion (51) did not differ. Each of the 7 remaining studies examined different technique comparisons, including bioabsorbable tacks versus suture tying (53), side-to-side versus tendon-tobone fixation (54), nonabsorbable versus absorbable suture (55), headed bioabsorbable corkscrew versus metal suture anchor (56), mattress versus single transosseous suture (57), ultrasonic suture welding versus hand-tied knots (58), and staple fixation versus side-to-side suture (59). The overall level of evidence was low for these techniques. All studies assessed function; 3 found statis250 17 August 2010 Annals of Internal Medicine Volume 153 • Number 4 tically significant differences (12 to 15 points on a 100point scale) between the groups examined (53, 54, 56). We noted a statistically significant difference in cuff integrity in 1 study (55) but could not assess the difference in 2 others because of incomplete data reporting (57, 59). Individual studies found statistically significant differences for range of motion (56) and strength (57) but not for pain (53, 55). Operative Augmentation Three small controlled and 5 uncontrolled studies assessed surgical augmentation. One RCT (60) and 1 retrospective cohort study (61) compared porcine small intestine submucosa xenografts with no augmentation. Function (60) and cuff integrity (60, 61) did not significantly differ. One study (61) found a slower rate of activityrelated pain resolution, an almost global loss of strength, and less sport participation in the augmentation group. One retrospective cohort study (62) compared patch graft with no augmentation and found no statistically significant difference in function. Range of motion for abduction was significantly improved with patch augmentation (40° difference between groups). Five uncontrolled studies evaluated different types of augmentations, and all showed improvement in functional scores. www.annals.org Nonoperative and Operative Treatments for Rotator Cuff Tears Postoperative Rehabilitation Ten controlled studies and 1 uncontrolled study evaluated postoperative rehabilitation. Three RCTs (63– 65) studied the addition of continuous passive motion to physical therapy. Overall, moderate evidence showed no difference in function or pain (pooled standardized mean differences, 0.08 [CI, ⫺0.37 to 0.52] and ⫺0.12 [CI, ⫺1.08 to 0.83], respectively). One study (63) found no statistically significant difference between groups for range of motion or strength. Another study (64) found that the time to return to work favored continuous passive motion with physical therapy over physical therapy alone (absolute difference of 12 and 21 days, respectively). Similarly, time to 90° abduction favored continuous passive motion. Continuous passive motion may improve recovery over the short term. Seven additional studies each reported on different postoperative rehabilitation comparisons: a land-based program with or without aquatic therapy (66), inpatient versus outpatient rehabilitation (67), individualized physical therapy plus home exercise versus home exercise alone (68), rehabilitation with progressive loading versus traditional loading (69), inpatient rehabilitation versus private outpatient rehabilitation with the Concept Global d’Epaule method (70), standardized versus nonstandardized physical therapy (71), and videotape-based versus therapist-based home exercise instruction (72). One study (71) demonstrated that patients who received standardized physical therapy showed statistically significant improvement in function compared with those who received nonstandardized treatment. Progressive loading showed a statistically significant reduction in pain versus traditional loading (69). Outpatient therapy with the Concept Global d’Epaule method reduced pain better than inpatient rehabilitation (70). Health-related quality of life (66), function (68, 70, 72), pain (67, 71), range of motion (66 – 68), and strength (68, 70) did not significantly differ across the remaining studies. We could not evaluate 1 study because the investigators did not report levels of significance for most outcomes (69). One uncontrolled study (73) demonstrated significant improvements in health-related quality of life and function after rehabilitation. Nonoperative Interventions Three controlled and 7 uncontrolled studies examined nonoperative interventions. One RCT (74) compared sodium hyaluronate with dexamethasone injections; however, no head-to-head comparison regarding the relative efficacy of these interventions was reported. A retrospective cohort study (75) compared rehabilitation that focused on protecting the cuff through reliance on other muscles (deltoid, pectoralis major, and latissimus dorsi) with no rehabilitation. Differences in function that favored the rehabilitation group were statistically significant and clinically important (absolute difference, 26.9 points on a 100-point scale). A second retrospective cohort study (33) compared www.annals.org Review administration of steroid injection with no steroid injection among participants undergoing physical therapy (treatment components not specified) and receiving oral medications (not specified). Function (absolute difference, 11 on an 83-point scale) and time to maximum range of motion (absolute difference, 4 months) significantly improved. For the uncontrolled studies, the degree of improvement in functional outcome scores varied considerably. The strength of evidence was too low to make conclusions for any of the nonoperative interventions (Table 2). Operative Versus Nonoperative Interventions Five studies compared nonoperative with operative treatments. Four studies (12, 33, 76, 77) included either physical therapy (treatment components not specified) or stretching and strengthening exercises, with or without the addition of steroid injections, oral medications, activity modification, or manual therapy. One study (78) examined the use of shock-wave therapy. Nonoperative treatments were compared with either open or mini-open repair. One study included a third comparison group that received arthroscopic debridement (33). All groups showed statistically significant improvements regardless of the intervention. All but 1 study (76) showed statistically significant differences in function that favored operative repair. One study (33) showed that patients who had arthroscopic debridement had a statistically significant shorter time to maximum range of motion (3.2 months) than did those in the nonoperative and open repair groups (6.8 months each). In general, the evidence was too limited to make conclusions regarding comparative effectiveness (Table 2). Complications Sixty-four studies provided data on 34 different complications, and an additional 21 studies reported no complications during follow-up. Five complications were identified a priori to be most clinically relevant. Generally, complications were uncommon (Appendix Table 5, available at www.annals.org). Recurrent tears occurred in a median of 3% of patients (IQR, 2% to 7%) in operative studies and 4% (IQR, 0% to 5%) in postoperative rehabilitation studies. In most operative studies, no patients had infections (IQR, 0% to 2%), whereas a median of 0.5% of patients (IQR, 1.3% to 6%) in postoperative rehabilitation studies reported infections. Stiffness occurred in a median of 2% of patients (IQR, 0% to 3%) in operative studies, whereas 2 nonoperative studies reported events in 4% and 7% of patients. Two percent of patients (IQR, 1.8% to 4.5%) in operative studies developed reflex sympathetic dystrophy, versus 0% and 7% in 2 postoperative rehabilitation studies. Neurologic injury was very rare (median, 0% [IQR, 0% to 0.1%]). Because of the low event rates, the benefit of receiving treatment for rotator cuff tears seems to outweigh the risk for associated harms. 17 August 2010 Annals of Internal Medicine Volume 153 • Number 4 251 Review Nonoperative and Operative Treatments for Rotator Cuff Tears Prognostic Factors Seventy-two of the 137 studies assessed the effect of known prognostic factors on patient outcomes. The number of prognostic factors examined across many different outcome measures and the inconsistency among the investigators’ conclusions limited our ability to identify predictors of good outcome for nonoperative and operative treatments of rotator cuff tears. Overall, older age, increased tear size, and greater preoperative symptoms were repeatedly found to be associated with recurrent tears. Sex, worker’s compensation board status, and duration of symptoms were not found to be associated with poorer outcomes in most studies that examined these variables. DISCUSSION Our comparative effectiveness review provides a current synthesis of the state of the evidence on nonoperative and operative interventions for rotator cuff tears. Sparse data are available for most comparisons, which precludes firm conclusions for a single approach or the optimal overall management of this condition. Patients experienced substantial improvements across all interventions. We found few clinically important differences when comparisons between interventions were available. Complications were rare, and we considered few to be clinically important. The benefit of receiving treatment for rotator cuff tears seems to outweigh the risk for associated harms. The strength of evidence was low for most interventions. This low grade was driven by the high risk for bias within individual studies and the lack of consistency and precision across studies. Many studies used weak study designs, failed to control for important sources of bias, and lacked an independent comparison group. Trials had a high risk for bias and frequently had inadequate blinding, insufficient allocation concealment, and incomplete outcome data. Although blinding is not always feasible because of the nature of the intervention, adequate allocation concealment is always possible in an RCT. Selective outcome reporting may also have introduced bias. The methodological quality was moderate for the cohort and uncontrolled studies. Many studies did not control for important potential confounders in their design or analysis. We could not assess the possibility of publication bias because of the small number of studies for each comparison. The lack of consistency and precision of results across the studies was primarily due to varied comparisons made across this body of literature; relatively few studies compared the same interventions. In addition, variation in the pathologic presentation of rotator cuff disease contributed to inconsistency among the studies. Although most patients had full-thickness tears, the size and configuration of the tears, degree of fatty infiltration, and number and type of comorbid conditions varied widely across the included studies. Both outcome measures and timing of measurements varied considerably across studies, which made com252 17 August 2010 Annals of Internal Medicine Volume 153 • Number 4 parisons difficult. The most common outcome was function, but 21 different tools were used for this purpose, and multiple tools were often used in the same study. The quality of reporting was poor and inconsistent, particularly in studies that evaluated nonoperative interventions. Physical therapy was often labeled as an intervention, with no description of treatment components or delivery. Studies rarely described the timing and frequency of intervention components, the training and experience of the staff who implemented the interventions, or any cointerventions, which leads to interpretive challenges. Our review differs from previously published reviews because it assesses the full range of nonoperative and operative treatment options, includes a broad range of study designs, and considers only studies that confirmed the presence of rotator cuff tears. One previous review (79), published in 2004, similarly examined all treatment methods in controlled and uncontrolled studies, but we have included the considerable literature published since then. One limitation of our review is the language restriction, which we applied because of a lack of translation resources. In addition, we could not retrieve 29 potentially relevant references. It is unlikely that these would have affected our results, because we identified many of these citations through searches of gray literature. Priorities for future research include studies that compare the effectiveness of early versus delayed surgery. Patients generally have surgery after several months of failed conservative treatment. Evidence is needed to determine whether surgery should be delayed and, if so, for how long and for whom. Evidence that compared the relative effectiveness of operative versus nonoperative treatments or compared the various nonoperative treatment options was sparse. Although most of the studies we reviewed focused on the comparative effectiveness of operative treatments, evidence for most individual treatment comparisons was sparse, which leaves many unanswered questions. For future research, investigators should use a streamlined approach when evaluating operative treatments that begins with assessing broad treatment questions before focusing on detailed procedures. They should use a comparative design and ensure that the diagnosis of rotator cuff tears is confirmed appropriately. Consensus on clinically important and patient-important outcomes, as well as choice of measurement tools, is needed to ensure consistency and comparability across studies. Detailed reporting of study methods and interventions is needed to allow appropriate interpretation of results and replication of treatments. The CONSORT (Consolidated Standards of Reporting Trials) (80) and STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) (81) statements provide guidance for minimizing the risk for bias when designing RCTs and cohort studies, respectively. We found moderate evidence for some interventions, but the data were too limited to make definite conclusions for most interventions examined. Few differences of cliniwww.annals.org Nonoperative and Operative Treatments for Rotator Cuff Tears cal importance were evident when we compared the relative effectiveness of the various treatments. Future studies, of high methodological quality, are needed to explore the relative effectiveness of early versus delayed surgery and of nonoperative versus operative treatment, as well as among the various nonoperative and operative interventions. From the University of Alberta, Edmonton, Alberta, Canada. Disclaimer: The authors of this report are responsible for its content. Statements in the report should not be construed as endorsement by the Agency for Healthcare Research and Quality or the U.S. Department of Health and Human Services. Grant Support: By the Agency for Healthcare Research and Quality, U.S. Department of Health and Human Services (contract 290-020023). Potential Conflicts of Interest: Ms. Seida, Dr. LeBlanc, Ms. Schouten, Dr. Mousavi, Mr. Vandermeer, and Dr. Sheps: Grants received (money to institution): Agency for Healthcare Research and Quality. Dr. LeBlanc: Consultancy: University of Alberta. Dr. Hartling: Other (money to institution): Agency for Healthcare Research and Quality. Dr. Sheps: Consultancy: Agency for Healthcare Research and Quality. Disclosures can also be viewed at www.acponline.org/authors/icmje/ConflictOfInterestForms .do?msNum⫽M10-0825. Corresponding Author: Jennifer C. Seida, MPH, Alberta Research Cen- tre for Health Evidence, University of Alberta, 11402 University Avenue, Edmonton, Alberta T6G 2J3, Canada; e-mail, [email protected]. Current author addresses and author contributions are available at www.annals.org. References 1. Crusher RH. Rotator cuff injuries. Accid Emerg Nurs. 2000;8:129-33. [PMID: 10893553] 2. Bartolozzi A, Andreychik D, Ahmad S. Determinants of outcome in the treatment of rotator cuff disease. Clin Orthop Relat Res. 1994:90-7. [PMID: 7955708] 3. Ghodadra NS, Provencher MT, Verma NN, Wilk KE, Romeo AA. Open, mini-open, and all-arthroscopic rotator cuff repair surgery: indications and implications for rehabilitation. J Orthop Sports Phys Ther. 2009;39:81-9. [PMID: 19194025] 4. Suenaga N, Minami A, Kaneda K. Postoperative subcoracoid impingement syndrome in patients with rotator cuff tear. J Shoulder Elbow Surg. 2000;9: 275-8. [PMID: 10979521] 5. Wittenberg RH, Rubenthaler F, Wo¨lk T, Ludwig J, Willburger RE, Steffen R. Surgical or conservative treatment for chronic rotator cuff calcifying tendinitis—a matched-pair analysis of 100 patients. Arch Orthop Trauma Surg. 2001;121:56-9. [PMID: 11195119] 6. Higgins J, Green SE. Cochrane Handbook for Systematic Reviews of Interventions, Version 5.0.1. The Cochrane Collaboration; 2008. 7. Wells G, Shea B, O’Connell B, Peterson J, Welch V, Losos M, et al. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomized studies in meta-analyses. Ottawa, Ontario, Canada: Department of Epidemiology and Community Medicine, University of Ottawa; 2009. 8. Owens DK, Lohr KN, Atkins D, Treadwell JR, Reston JT, Bass EB, et al. AHRQ series paper 5: grading the strength of a body of evidence when comparing medical interventions—agency for healthcare research and quality and the effective health-care program. J Clin Epidemiol. 2010;63:513-23. [PMID: 19595577] 9. Atkins D, Best D, Briss PA, Eccles M, Falck-Ytter Y, Flottorp S, et al; GRADE Working Group. Grading quality of evidence and strength of recomwww.annals.org Review mendations. BMJ. 2004;328:1490. [PMID: 15205295] 10. Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. 2002;21:1539-58. [PMID: 12111919] 11. Deeks JJ, Altman DG, Bradburn MJ. Statistical methods for examining heterogeneity and combining results from several studies in meta-analysis. In: Egger M, Smith GD, Altman DG, eds. Systematic Review in Health Care: Metaanalysis in Context 2nd ed. London: BMJ Publishing Group; 2001:285-312. 12. Moosmayer S, Lund G, Seljom U, Svege I, Hennig T, Tariq R, et al. Comparison between surgery and physiotherapy in the treatment of small and medium-sized tears of the rotator cuff: A randomised controlled study of 103 patients with one-year follow-up. J Bone Joint Surg Br. 2010;92:83-91. [PMID: 20044684] 13. Mohtadi NG, Hollinshead RM, Sasyniuk TM, Fletcher JA, Chan DS, Li FX. A randomized clinical trial comparing open to arthroscopic acromioplasty with mini-open rotator cuff repair for full-thickness rotator cuff tears: diseasespecific quality of life outcome at an average 2-year follow-up. Am J Sports Med. 2008;36:1043-51. [PMID: 18354140] 14. Baker CL, Liu SH. Comparison of open and arthroscopically assisted rotator cuff repairs. Am J Sports Med. 1995;23:99-104. [PMID: 7726359] 15. Hata Y, Saitoh S, Murakami N, Kobayashi H, Takaoka K. Atrophy of the deltoid muscle following rotator cuff surgery. J Bone Joint Surg Am. 2004;86-A: 1414-9. [PMID: 15252087] 16. Kim SH, Ha KI, Park JH, Kang JS, Oh SK, Oh I. Arthroscopic versus mini-open salvage repair of the rotator cuff tear: outcome analysis at 2 to 6 years’ follow-up. Arthroscopy. 2003;19:746-54. [PMID: 12966383] 17. Colegate-Stone T, Allom R, Tavakkolizadeh A, Sinha J. An analysis of outcome of arthroscopic versus mini-open rotator cuff repair using subjective and objective scoring tools. Knee Surg Sports Traumatol Arthrosc. 2009;17:691-4. [PMID: 19002667] 18. Pearsall AW 4th, Ibrahim KA, Madanagopal SG. The results of arthroscopic versus mini-open repair for rotator cuff tears at mid-term follow-up. J Orthop Surg Res. 2007;2:24. [PMID: 18053153] 19. Ko¨se KC, Tezen E, Cebesoy O, Karadeniz E, Guner D, Adiyaman S, et al. Mini-open versus all-arthroscopic rotator cuff repair: comparison of the operative costs and the clinical outcomes. Adv Ther. 2008;25:249-59. [PMID: 18363045] 20. Liem D, Bartl C, Lichtenberg S, Magosch P, Habermeyer P. Clinical outcome and tendon integrity of arthroscopic versus mini-open supraspinatus tendon repair: a magnetic resonance imaging-controlled matched-pair analysis. Arthroscopy. 2007;23:514-21. [PMID: 17478283] 21. Sauerbrey AM, Getz CL, Piancastelli M, Iannotti JP, Ramsey ML, Williams GR Jr. Arthroscopic versus mini-open rotator cuff repair: a comparison of clinical outcome. Arthroscopy. 2005;21:1415-20. [PMID: 16376228] 22. Severud EL, Ruotolo C, Abbott DD, Nottage WM. All-arthroscopic versus mini-open rotator cuff repair: A long-term retrospective outcome comparison. Arthroscopy. 2003;19:234-8. [PMID: 12627146] 23. Verma NN, Dunn W, Adler RS, Cordasco FA, Allen A, MacGillivray J, et al. All-arthroscopic versus mini-open rotator cuff repair: a retrospective review with minimum 2-year follow-up. Arthroscopy. 2006;22:587-94. [PMID: 16762695] 24. Warner JJ, Te´treault P, Lehtinen J, Zurakowski D. Arthroscopic versus mini-open rotator cuff repair: a cohort comparison study. Arthroscopy. 2005;21: 328-32. [PMID: 15756188] 25. Youm T, Murray DH, Kubiak EN, Rokito AS, Zuckerman JD. Arthroscopic versus mini-open rotator cuff repair: a comparison of clinical outcomes and patient satisfaction. J Shoulder Elbow Surg. 2005;14:455-9. [PMID: 16194734] 26. Ide J, Maeda S, Takagi K. A comparison of arthroscopic and open rotator cuff repair. Arthroscopy. 2005;21:1090-8. [PMID: 16171634] 27. Costouros JG, von Campe A, Gerber C. Arthroscopic rotator cuff repair leads to less postoperative fatty infiltration than open repair. Presented at the 20th Congress of the European Society for Surgery of the Shoulder and the Elbow (SECEC-ESSSE 2006), Athens, Greece, 20 –23 September 2006. 28. Millar NL, Wu X, Tantau R, Silverstone E, Murrell GA. Open versus two forms of arthroscopic rotator cuff repair. Clin Orthop Relat Res. 2009;467:96678. [PMID: 19184264] 29. Bishop J, Klepps S, Lo IK, Bird J, Gladstone JN, Flatow EL. Cuff integrity after arthroscopic versus open rotator cuff repair: a prospective study. J Shoulder Elbow Surg. 2006;15:290-9. [PMID: 16679227] 30. Buess E, Steuber KU, Waibl B. Open versus arthroscopic rotator cuff repair: a comparative view of 96 cases. Arthroscopy. 2005;21:597-604. [PMID: 15891728] 17 August 2010 Annals of Internal Medicine Volume 153 • Number 4 253 Review Nonoperative and Operative Treatments for Rotator Cuff Tears 31. Montgomery TJ, Yerger B. Management of rotator cuff tears: a comparison of arthroscopic debridement and surgical repair. J Shoulder Elbow Surg. 1994;3: 70-8. 32. Ogilvie-Harris DJ, Demazie`re A. Arthroscopic debridement versus open repair for rotator cuff tears. A prospective cohort study. J Bone Joint Surg Br. 1993;75:416-20. [PMID: 8496210] 33. Vad VB, Warren RF, Altchek DW, O’Brien SJ, Rose HA, Wickiewicz TL. Negative prognostic factors in managing massive rotator cuff tears. Clin J Sport Med. 2002;12:151-7. [PMID: 12011722] 34. Motycka T, Lehner A, Landsiedl F. Comparison of debridement versus suture in large rotator cuff tears: long-term study of 64 shoulders. Arch Orthop Trauma Surg. 2004;124:654-8. [PMID: 15372278] 35. Gartsman GM, O’connor DP. Arthroscopic rotator cuff repair with and without arthroscopic subacromial decompression: a prospective, randomized study of one-year outcomes. J Shoulder Elbow Surg. 2004;13:424-6. [PMID: 15220883] 36. Milano G, Grasso A, Salvatore M, Zarelli D, Deriu L, Fabbriciani C. Arthroscopic rotator cuff repair with and without subacromial decompression: a prospective randomized study. Arthroscopy. 2007;23:81-8. [PMID: 17210431] 37. Mullett H, Venkat V, Massoud S, Levy O, Copeland S. Small and medium rotator cuff tears: comparison of arthroscopic rotator cuff repair vs. arthroscopic subacromial decompression. Presented at the 20th Congress of the European Society for Surgery of the Shoulder and the Elbow (SECEC-ESSSE 2006), Athens, Greece, 20 –23 September 2006. 38. Boileau P, Baque´ F, Valerio L, Ahrens P, Chuinard C, Trojani C. Isolated arthroscopic biceps tenotomy or tenodesis improves symptoms in patients with massive irreparable rotator cuff tears. J Bone Joint Surg Am. 2007;89:747-57. [PMID: 17403796] 39. Favard L, Berhouet J, Colmar M, Boukobza E, Richou J, Sonnard A, et al. Massive rotator cuff tears in patients younger than 65 years: what treatment options are available? Orthop Traumatol Surg Res. 2009;95(4 Suppl):19-26. 40. Franceschi F, Longo UG, Ruzzini L, Rizzello G, Maffulli N, Denaro V. No advantages in repairing a type II superior labrum anterior and posterior (SLAP) lesion when associated with rotator cuff repair in patients over age 50: a randomized controlled trial. Am J Sports Med. 2008;36:247-53. [PMID: 17940144] 41. Franceschi F, Longo UG, Ruzzini L, Papalia R, Rizzello G, Denaro V. To detach the long head of the biceps tendon after tenodesis or not: outcome analysis at the 4-year follow-up of two different techniques. Int Orthop. 2007;31:537-45. [PMID: 16947053] 42. Klinger HM, Spahn G, Baums MH, Steckel H. Arthroscopic debridement of irreparable massive rotator cuff tears—a comparison of debridement alone and combined procedure with biceps tenotomy. Acta Chir Belg. 2005;105:297-301. [PMID: 16018524] 43. Moser M, Jablonski MV, Horodyski M, Wright TW. Functional outcome of surgically treated massive rotator cuff tears: a comparison of complete repair, partial repair, and debridement. Orthopedics. 2007;30:479-82. [PMID: 17598493] 44. Torrens C, Lo´pez JM, Verdier E, Marı´n M. Open anterior acromioplasty with preservation of the coracoacromial ligament: A modified surgical technique. J Shoulder Elbow Surg. 2003;12:9-14. [PMID: 12610479] 45. Burks RT, Crim J, Brown N, Fink B, Greis PE. A prospective randomized clinical trial comparing arthroscopic single- and double-row rotator cuff repair: magnetic resonance imaging and early clinical evaluation. Am J Sports Med. 2009;37:674-82. [PMID: 19204365] 46. Charousset C, Grimberg J, Duranthon LD, Bellaiche L, Petrover D. Can a double-row anchorage technique improve tendon healing in arthroscopic rotator cuff repair?: A prospective, nonrandomized, comparative study of double-row and single-row anchorage techniques with computed tomographic arthrography tendon healing assessment. Am J Sports Med. 2007;35:1247-53. [PMID: 17452513] 47. Franceschi F, Ruzzini L, Longo UG, Martina FM, Zobel BB, Maffulli N, et al. Equivalent clinical results of arthroscopic single-row and double-row suture anchor repair for rotator cuff tears: a randomized controlled trial. Am J Sports Med. 2007;35:1254-60. [PMID: 17554104] 48. Grasso A, Milano G, Salvatore M, Falcone G, Deriu L, Fabbriciani C. Single-row versus double-row arthroscopic rotator cuff repair: a prospective randomized clinical study. Arthroscopy. 2009;25:4-12. [PMID: 19111212] 49. Park JY, Lhee SH, Choi JH, Park HK, Yu JW, Seo JB. Comparison of the 254 17 August 2010 Annals of Internal Medicine Volume 153 • Number 4 clinical outcomes of single- and double-row repairs in rotator cuff tears. Am J Sports Med. 2008;36:1310-6. [PMID: 18413680] 50. Sugaya H, Maeda K, Matsuki K, Moriishi J. Functional and structural outcome after arthroscopic full-thickness rotator cuff repair: single-row versus dual-row fixation. Arthroscopy. 2005;21:1307-16. [PMID: 16325080] 51. Ko SH, Friedman D, Seo DK, Jun HM, Warner JJ. A prospective therapeutic comparison of simple suture repairs to massive cuff stitch repairs for treatment of small- and medium-sized rotator cuff tears. Arthroscopy. 2009;25:583-9, 589.e1-4. [PMID: 19501286] 52. Ko SH, Lee CC, Friedman D, Park KB, Warner JJ. Arthroscopic single-row supraspinatus tendon repair with a modified mattress locking stitch: a prospective, randomized controlled comparison with a simple stitch. Arthroscopy. 2008; 24:1005-12. [PMID: 18760207] 53. Bennett WF. Arthroscopic repair of anterosuperior (supraspinatus/subscapularis) rotator cuff tears: a prospective cohort with 2- to 4-year follow-up. Classification of biceps subluxation/instability. Arthroscopy. 2003;19:21-33. [PMID: 12522399] 54. Bigoni M, Gorla M, Guerrasio S, Brignoli A, Cossio A, Grillo P, et al. Shoulder evaluation with isokinetic strength testing after arthroscopic rotator cuff repairs. J Shoulder Elbow Surg. 2009;18:178-83. [PMID: 19111477] 55. Boehm TD, Werner A, Radtke S, Mueller T, Kirschner S, Gohlke F. The effect of suture materials and techniques on the outcome of repair of the rotator cuff: a prospective, randomised study. J Bone Joint Surg Br. 2005;87:819-23. [PMID: 15911666] 56. Cummins CA, Strickland S, Appleyard RC, Szomor ZL, Marshall J, Murrell GA. Rotator cuff repair with bioabsorbable screws: An in vivo and ex vivo investigation. Arthroscopy. 2003;19:239-48. [PMID: 12627147] 57. Matis N, Hu¨bner C, Aschauer E, Resch H. Arthroscopic transosseous reinsertion of the rotator cuff. Oper Orthop Traumatol. 2006;18:1-18. [PMID: 16534558] 58. McIntyre LF, Norris M, Weber B. Comparison of suture welding and hand-tied knots in mini-open rotator cuff repair. Arthroscopy. 2006;22:833-6, 836.e1. [PMID: 16904579] 59. Wilson F, Hinov V, Adams G. Arthroscopic repair of full-thickness tears of the rotator cuff: 2- to 14-year follow-up. Arthroscopy. 2002;18:136-44. [PMID: 11830806] 60. Iannotti JP, Codsi MJ, Kwon YW, Derwin K, Ciccone J, Brems JJ. Porcine small intestine submucosa augmentation of surgical repair of chronic two-tendon rotator cuff tears. A randomized, controlled trial. J Bone Joint Surg Am. 2006; 88:1238-44. [PMID: 16757756] 61. Walton JR, Bowman NK, Khatib Y, Linklater J, Murrell GA. Restore orthobiologic implant: not recommended for augmentation of rotator cuff repairs. J Bone Joint Surg Am. 2007;89:786-91. [PMID: 17403801] 62. Ito J, Morioka T. Surgical treatment for large and massive tears of the rotator cuff. Int Orthop. 2003;27:228-31. [PMID: 12827299] 63. Lastayo PC, Wright T, Jaffe R, Hartzel J. Continuous passive motion after repair of the rotator cuff. A prospective outcome study. J Bone Joint Surg Am. 1998;80:1002-11. [PMID: 9698005] 64. Michael JW, Ko¨nig DP, Imhoff AB, Martinek V, Braun S, Hu¨bscher M, et al. [Efficiency of a postoperative treatment after rotator cuff repair with a continuous passive motion device (CPM)]. Z Orthop Ihre Grenzgeb. 2005;143: 438-45. [PMID: 16118760] 65. Raab MG, Rzeszutko D, O’Connor W, Greatting MD. Early results of continuous passive motion after rotator cuff repair: a prospective, randomized, blinded, controlled study. Am J Orthop (Belle Mead NJ). 1996;25:214-20. [PMID: 8775698] 66. Brady B, Redfern J, MacDougal G, Williams J. The addition of aquatic therapy to rehabilitation following surgical rotator cuff repair: a feasibility study. Physiother Res Int. 2008;13:153-61. [PMID: 18548557] 67. Delbrouck C, Dauty M, Huguet D, Dubois C. [Rehabilitation after shoulder rotator cuff surgery: in-patient or day-hospitalization (about 76 cases)]. Ann Readapt Med Phys. 2003;46:207-13. [PMID: 12787979] 68. Hayes K, Ginn KA, Walton JR, Szomor ZL, Murrell GA. A randomised clinical trial evaluating the efficacy of physiotherapy after rotator cuff repair. Aust J Physiother. 2004;50:77-83. [PMID: 15151491] 69. Klintberg IH, Gunnarsson AC, Svantesson U, Styf J, Karlsson J. Early loading in physiotherapy treatment after full-thickness rotator cuff repair: a prospective randomized pilot-study with a two-year follow-up. Clin Rehabil. 2009; 23:622-38. [PMID: 19482895] 70. Marc T, Gaudin T, Teissier J. Rehabilitation after rotator cuff repairs: factors www.annals.org Nonoperative and Operative Treatments for Rotator Cuff Tears influencing functional outcome at two years [French]. Kinesitherapie Revue 2009;89:36-44. 71. Milroy DR, Marland JD, Parent EC, Brennan GP. Rotator cuff repair: the effect of a standardized post-operative physical therapy protocol versus a nonstandardized post-operative protocol. J Orthop Sports Phys Ther. 2008;38: A17-8. 72. Roddey TS, Olson SL, Gartsman GM, Hanten WP, Cook KF. A randomized controlled trial comparing 2 instructional approaches to home exercise instruction following arthroscopic full-thickness rotator cuff repair surgery. J Orthop Sports Phys Ther. 2002;32:548-59. [PMID: 12449254] 73. Boissonnault WG, Badke MB, Wooden MJ, Ekedahl S, Fly K. Patient outcome following rehabilitation for rotator cuff repair surgery: the impact of selected medical comorbidities. J Orthop Sports Phys Ther. 2007;37:312-9. [PMID: 17612357] 74. Shibata Y, Midorikawa K, Emoto G, Naito M. Clinical evaluation of sodium hyaluronate for the treatment of patients with rotator cuff tear. J Shoulder Elbow Surg. 2001;10:209-16. [PMID: 11408900] 75. Leroux JL, Thomas E, Azema MJ, Bonnel F, Blotman F. Functional pattern of 115 rotator cuff tears. Eur J Phys Med Rehabil. 1993;3:242-7. 76. Lunn JV, Castellanos-Rosas J, Tavernier T, Barthe´le´my R, Walch G. A ANNALS OF INTERNAL Review novel lesion of the infraspinatus characterized by musculotendinous disruption, edema, and late fatty infiltration. J Shoulder Elbow Surg. 2008;17:546-53. [PMID: 18372195] 77. Yamada N, Hamada K, Nakajima T, Kobayashi K, Fukuda H. Comparison of conservative and operative treatments of massive rotator cuff tears. Tokai J Exp Clin Med. 2000;25:151-63. [PMID: 11358030] 78. De Carli A, Vulpiani M, Russo A, Vadala A, Trovato P, Feretti A. Reparable rotator cuff tears: surgery vs shock wave therapy [Abstract]. J Orthopaed Traumatol. 2006;7:S51. 79. Grant HJ, Arthur A, Pichora DR. Evaluation of interventions for rotator cuff pathology: a systematic review. J Hand Ther. 2004;17:274-99. [PMID: 15162111] 80. Moher D, Schulz KF, Altman DG; CONSORT GROUP (Consolidated Standards of Reporting Trials). The CONSORT statement: revised recommendations for improving the quality of reports of parallel-group randomized trials. Ann Intern Med. 2001;134:657-62. [PMID: 11304106] 81. von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP; STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. J Clin Epidemiol. 2008;61:344-9. [PMID: 18313558] MEDICINE JUNIOR INVESTIGATOR AWARDS Beginning in 2010, Annals of Internal Medicine and the American College of Physicians will recognize excellence among internal medicine trainees and junior investigators with annual awards for original research and scholarly review articles published in Annals in each of the following categories: ● Most outstanding article with a first author in an internal medicine residency program or a general medicine or internal medicine subspecialty fellowship program ● Most outstanding article with a first author within 3 years following completion of training in internal medicine or one of its subspecialties Selection of award winners will consider the article’s novelty, methodological rigor, clarity of presentation, and potential to influence practice, policy, or future research. Judges will include Annals Editors and representatives from Annals’ Editorial Board and the American College of Physicians’ Education/Publication Committee. Papers published in the year following submission are eligible for the award in the year of publication. First author status at the time of manuscript submission will determine eligibility. Authors should indicate that they wish to have their papers considered for an award when they submit the manuscript, and they must be able to provide satisfactory documentation of their eligibility if selected for an award. Announcement of awards for a calendar year will occur in January of the subsequent year. We will provide award winners with a framed certificate, a letter documenting the award, and complimentary registration for the American College of Physicians’ annual meeting. Please refer questions to Mary Beth Schaeffer at mschaeffer@acponline .org. www.annals.org 17 August 2010 Annals of Internal Medicine Volume 153 • Number 4 255 Annals of Internal Medicine Current Author Addresses: Ms. Seida, Ms. Schouten, Drs. Mousavi and Hartling, and Mr. Vandermeer: Alberta Research Centre for Health Evidence, University of Alberta, Aberhart Center, 11402 University Avenue, Edmonton, Alberta T6G 2J3, Canada. Dr. LeBlanc: University of Alberta, Aberhart Center, 11402 University Avenue, Edmonton, Alberta T6G 2J3, Canada. Ms. Tjosvold: 2K3.28 Walter C. Mackenzie Health Sciences Center, University of Alberta, Edmonton, Alberta T6G 2R7, Canada. Dr. Sheps: 10839 124th Street, Edmonton, Alberta T5M 0H4, Canada. Author Contributions: Conception and design: J.C. Seida, C. LeBlanc, L. Hartling, D.M. Sheps. Analysis and interpretation of the data: J.C. Seida, C. LeBlanc, J.R. Schouten, L. Hartling, B. Vandermeer, D.M. Sheps. Drafting of the article: J.C. Seida, J.R. Schouten, S.S. Mousavi, L. Hartling, B. Vandermeer, L. Tjosvold, D.M. Sheps. Critical revision of the article for important intellectual content: J.C. Seida, C. LeBlanc, S.S. Mousavi, L. Hartling, B. Vandermeer. Final approval of the article: J.C. Seida, C. LeBlanc, L. Hartling, L. Tjosvold. Statistical expertise: B. Vandermeer. Obtaining of funding: L. Hartling. Administrative, technical, or logistic support: J.C. Seida, L. Tjosvold. Collection and assembly of data: J.C. Seida, J.R. Schouten, S.S. Mousavi, L. Hartling, L. Tjosvold. W-86 17 August 2010 Annals of Internal Medicine Volume 153 • Number 4 www.annals.org Copyright of Annals of Internal Medicine is the property of American College of Physicians and its content may not be copied or emailed to multiple sites or posted to a listserv without the copyright holder's express written permission. However, users may print, download, or email articles for individual use.









© Copyright 2026