ABC
docz
Explore
Log in
Create new account
Download
Report
No category
Signs and symptoms of urinary system diseases. The urinary
SureStep LH Ovulation Test Guide
Essentials of Pathophysiology CHAPTER 25 DISORDERS OF RENAL FUNCTION
UROLOGY ASSOCIATES OF KINGSPORT, P.C.
Clinical assessment tool for children 0-5 years
Celebrate World Kidney Day 12 March 2015
INTRODUCTION AND CLINICAL MANIFESTATIONS OF RENAL DISEASE (1)
iCassette - TigerOfficer.com
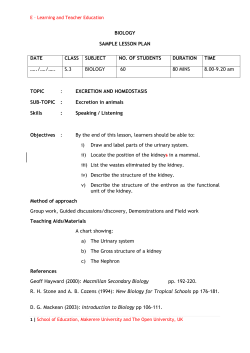
BIOLOGY SAMPLE LESSON PLAN DATE CLASS SUBJECT
HISTORY TAKING OF RENAL PROBLEMS RENAL COLIC
Non-specific Urethritis Syndrome: A Clinical Puzzle
© Copyright 2026
About abcdocz
DMCA / GDPR
Report