
Efficacy of magnetic resonance imaging in deciding the
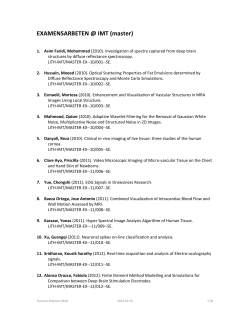
Miki Fujii, MD, PhD1 David G. Armstrong, DPM, MD, PhD2, Efficacy of magnetic resonance imaging in deciding the appropriate surgical margin in diabetic foot osteomyelitis ABSTRACT The best therapy for diabetic foot osteomyelitis (DFO) is controversial. However, identification of the precise localization of DFO is essential for appropriate treatment. AIM To ascertain the efficacy of magnetic resonance imaging (MRI) in the diagnosis of DFO, and to select the appropriate surgical margin. Hiroto Terashi, MD, PhD3 1Department of Plastic and Reconstructive Surgery, Kitaharima Medical Center, Ono, Japan 2Southern Arizona Limb Salvage Alliance, University of Arizona College of Medicine, Tucson, AZ, USA 3Department of Plastic and Reconstructive Surgery, Kobe University Hospital, Kobe, Japan Correspondence to: [email protected] Conflicts of interest: None METHODS Preoperative MRI findings were compared with the results of histopathological examinations of resected bones, and the margins of the resected bones were analysed by histopathology. A total 149 bones from 28 foot ulcers in 26 patients were examined. All ulcers were classified into 4 types according to the main etiological factors. RESULTS In 14 neuropathic ulcers, all 55 bones, even those with severe infection, were fully and accurately diagnosed with the use of MRI. In 14 ischemic ulcers, only 9 of 94 bones evaluated by MRI after revascularization were diagnosed accurately. Of 32 bone margins that showed bone marrow oedema, 28 healed, and 4 did not heal, displaying severe infection or ischemia. CONCLUSIONS MRI is effective in the diagnosis of neuropathic ulcers, but not as effective in the diagnosis of ischemic ulcers. This study suggested that the appropriate surgical margin should be defined in the area of the bone marrow oedema, but diligence should be exercised in cases with severe infection or ischemia. 8 INTRODUCTION The best therapy for diabetic foot osteomyelitis (DFO), whether primarily medical or primarily surgical, is a subject of contention. Each has its potential advantages and disadvantages1. Recent guidelines2 have recommended that the presence and amount of residual dead or infected bone and soft tissue should determine the duration of antibiotic therapy. Besides the choice of primary therapy, identification of the precise localization of DFO is essential for appropriate treatment. Guidelines2,3 recommend the use of plain radiographs as a first-line investigative tool for diagnosing DFO, and further note that although magnetic resonance imaging (MRI) has been recognized as the most accurate imaging modality for detecting DFO, it is not always necessary for diagnosing or managing DFO. Plain radiographs, however, show only destruction of bone, and not actual bone infection or inflammation. We have previously demonstrated the efficacy of MRI in the diagnosis of DFO in ulcers with different aetiologies 4,5. In the present report, we describe our study of additional cases, and propose a means of defining the appropriate surgical margin for remission based on MRI and histopathological findings. METHODS First, preoperative MRI findings were compared with the results of histopathological examination of the resected bones. Second, bone margins of the resected bones were analysed by histopathology. The records of 26 patients with diabetic foot ulcers (20 men and 6 women; mean age, 66.8 years; range, 42−85 years of age) who were suspected of having osteomyelitis and had undergone surgery from 2008−2014 were examined. All patients had been diagnosed with type 2 diabetes, according to the classification of the World Health Organization. The ulcers were classified into 4 types according to the main aetiological factors: type I, neuropathic ulcers; type II, ischemic ulcers (critical limb ischemia [CLI]); type III, neuropathic ulcers with infection; and type IV, ischemic EWMA Journal 2015 vol 15 no 1 Science, Practice and Education ulcers with infection4-6. Peripheral neuropathy (PN) was assessed by touch sensation using the Ipswich touch test7. Peripheral arterial disease (PAD) was suspected by the absence of pulsation and/or sound from the dorsalis pedis artery and the posterior tibial artery assessed by Doppler stethoscope, an ankle-brachial index < 0.9, and skin perfusion pressure < 40 mmHg. Patients with suspected PAD were evaluated with the use of computed tomographic angiography, duplex ultrasonography, and angiography. Infection was assessed by the following: general conditions such as high fever, chills, or malaise; clinical findings such as redness, warmth, swelling, or purulent secretions; the results of laboratory tests. DFO was suspected in patients with a positive probe-to-bone test, swollen foot, sausage toe, unexplained high leukocyte count or inflammatory markers, and plain foot radiographic findings3. Preoperative MRI was carried out with 1.5 T MR scanners (3 mm slice thickness, T1-weighted images, conventional spin echo, repetition time/echo time of 460 ms/13 ms, fat-suppressed T2-weighted images, short-tau inversion-recovery images, short T1 inversion recovery, and repetition time/echo time/inversion time of 3,401 ms/80 ms/150 ms). All MRI findings were checked by M.F and H.T with consensus interpretation. The affected bone marrow was compared with the adjacent normal fatty marrow, and low intensity signals on T1-weighted images and high intensity signals on fat-suppressed T2-weighted images were attributed to osteomyelitis. Incomplete or hazy signals or reticulated patterns were attributed to reactive bone marrow oedema. Normal bone marrow signals were considered indicative of areas clear of disease (8). All bones were marked according to the presence of osteomyelitis (OM), bone marrow oedema (BME), or normal bone (N) (Fig. 1). Surgery after the MRI diagnosis included resection of Figure 1: MRI diagnosis of case 1, left 2nd toe b) b) C) a) a) b) c) c) b) c) a) Osteomyelitis (OM) (T1WI: low intensity, fat-suppressed; T2WI: high intensity) b) Bone marrow edema (BME) (incomplete or hazy signals or reticulated patterns) c) Normal bone marrow signal (N) MRI diagnosis: Distal phalanges (c): Normal bone (N) Middle phalanges (b, a): bone marrow edema/ osteomyelitis (BME/ OM) Proximal phalanges (a, b, c): osteomyelitis/bone marrow edema/ normal bone (OM/BME/N) EWMA Journal 2015 vol 15 no 1 the infected bones and gangrenous tissue, amputation, or disarticulation. The area of resection was estimated preoperatively (from the MRI findings, blood flow, and area of soft tissue infection) and confirmed intraoperatively. A definitive diagnosis was then made from the histopathological examination of 5 mm thick sections of formalinfixed and paraffin-embedded bones stained with haematoxylin and eosin. Only bone marrow oedema or infiltration of inflammatory cells, or both was considered indicative of reactive bone marrow oedema. However, these 2 conditions, together with the presence of osteonecrosis, granulation tissue, and/or fibrosis, were considered indicative of osteomyelitis (Fig. 2). The diagnosis from the preoperative MRI findings was compared with the definitive diagnosis from the histopathological findings (Fig. 3). Bone margins of the resected bones were examined by histopathology. Figure 2: Histopathological diagnosis (haematoxylin & eosin staining, 40×) Osteomyelitis (OM) Bone marrow edema (BME) (H&E; 40 ) Bone marrow edema Inflammatory cells Osteonecrosis Granulation Fibrosis (H&E; 40 ) Bone marrow edema Inflammatory cells Informed consent was obtained from each patient, and the study protocol conformed to the ethical guidelines of the Declaration of Helsinki as reflected in the approval by the institution’s human research review committee. RESULTS A total of 28 ulcers from 26 patients, including 2 patients with 2 different types of ulcers each, were classified into 4 types according to the main aetiological factors as follows: type I, neuropathic ulcers (n=3); type II, ischemic ulcers (n=3); type III, neuropathic ulcers with infection (n=11); and type IV, ischemic ulcers with infection (n=11) (Table 1). The 26 patients underwent a total of 30 MRI examinations before surgery (Table 2). The average interval between the MRI examinations and surgery was 16.7 (range 2−48) days. All ischemic ulcers (type II and type IV) were revascularised by bypass or endovascular treatment before surgery. MRI was carried out as follows: 3 examinations for 3 type I ulcers; 3 before revascularisation for 3 type II ulcers; 1 after revascularisation for 1 type II ulcers; 11 for 9 Figure 3: Histopathological diagnosis of case 1, left 2nd toe. OM N BME) OM) BME BME) N) N) BME Histopathological features of bone marrow in the resected bones correspond to the MRI findings. Table 1. Classification of ulcers OM Main aetiologic factors Classification* Ulcers (n) Neuropathic ulcers Type I 3** Ischemic ulcers ( CLI ) Type II 3** Neuropathic ulcers Type III 11** ½ (H&E; 40 ) with infection CLI with infection Type IV 11** Total 28** *Terashi H. et al Keio Osteomyelitis J Med 2011; 6 0:17-‐21, * *Two (OM), bone marrow edema (BME), normal marrow (N) patients, had two types obone f ulcers each. N different OM Table Table 1 1. . C Classification lassification o of f u ulcers lcers Table 2. Details of MRI examinations Main aaetiologic etiologic ffactors actors Classification* Classification* Ulcers Ulcers ((n) n) Main Neuropathic u lcers Type I 3** Neuropathic ulcers Type I 3** Ischemic u lcers ( C LI ) Type I I 3** Ischemic ulcers ( CLI ) Type II 3** Neuropathic u lcers Type I II 11** ½ Neuropathic ulcers Type III 11** ½ with i nfection with infection CLI 11** CLI w with ith iinfection nfection Type Type IIV V 11** Total 28** Total 28** *Terashi H . e t a l K eio J M ed 2 011; 6 0:17-‐21, * *Two *Terashi H. et al Keio J Med 2011; 60:17-‐21, **Two patients, h had ad ttwo wo d different ifferent ttypes ypes o of f u ulcers lcers eeach. ach. patients, Type I Type II MRI 3* 4* Pre-‐revascularization: 3 Post-‐revascularization: 1 Type III 11 11* Type IV 11 12* Pre-‐revascularization: 6 Post-‐revascularization: 6 Total 28 30* Average interval between MRI and surgery: 16.7 days. *One ulcer of Type II (Case 5) underwent both pre-‐ and post-‐ revascularization MRI. Table Table 2 2. . D Details etails o of f M MRI RI e examinations xaminations 11 type III ulcers; and 6 before and 6 after revascularisation Ulcers MRI MRI post-revascularisation for type IV Ulcers ulcers. Pre- and MRI Type I 3 3* Type I for 23 patients who 3* underwent was done 2 surgeries, 1 for Type 3 4* Type III I 3 4* Pre-‐revascularization: Pre-‐revascularization: 3 3 type II ulcer and 1 for type IV ulcer. Post-‐revascularization: Post-‐revascularization: 1 1 A total of 149 bone specimens (39 distal phalanx, 29 Type I II 11 11* Type III 11 11* Type 11 12* Pre-‐revascularization: 6 middle 34 metatarsal bone, Type IIV V phalanx, 11 46 proximal 12* phalanx, Pre-‐revascularization: 6 Post-‐revascularization: 6 and from 57 toes as follows: 1 cuboid bone were obtained Post-‐revascularization: 6 Total 28 30* Total 28 from 3 ulcers), 30* type II (40 bones from 3 type I (11 bones Average iinterval b etween M RI a nd ssurgery: 1 d Average nterval b etween M RI a nd urgery: 16.7 6.7 and days. ays. ulcers), typeof III (44II (bones from 11 ulcers), typeost-‐ IV *One u lcer T ype Case 5 ) u nderwent b oth p re-‐ *One ulcer of Type II (Case 5) underwent both pre-‐ aand nd p post-‐ (54 bones from 11 ulcers) (Table 3). revascularization revascularization M MRI. RI. Histologic analysis of all bone specimens revealed the Table Table 3 3: : SSpecification pecification o of f b bone one sspecimens pecimens iin n e each ach u ulcer lcer ttype ype Ulcers Ulcers (n) Toes ((n) n) (n) Toes Type I 3 4* Type I 3 4* Type I I 3 12* Type II 3 12* Type I II 11 19* Type III 11 19* Type I V 11 22* Type IV 11 22* Total 28 57* Total 28 57* *Four t oes a nd a c uboid bone one *Four toes and a cuboid b 10 Bones Bones ((n) n) 11 11 40 40 44 44 54 54 149 149 Distal Distal phalanx phalanx ((n) n) 3 3 12 12 13 13 11 11 39 39 Ulcers 3 3 presence of osteomyelitis, bone marrow oedema, normal bone, or gangrene. The histopathological features of bone Table 3: in Specification of bbones one specimens in each ype marrow the resected corresponded toulcer the tMRI findings for ulcers of types I and III in every localisationMiddle (Table 4). Osteomyelitis was detected in 41 bones, Ulcers Distal withphalanx (n) specificity Toes (n) of Bones phalanx (n) (n) a sensitivity and 100%.(n) In type II ulcers, Type I 3 4* 11 3 however, none of the 40 bones was accurately diagnosed 3 Type II because 3 of unclear 12* or equivocal 40 12 (Table 9 by MRI images Type III 11 19* 44 13 5). Of 40 bones from type II ulcers, 27 showed dry gan- 7 Type IV 11 22* 54 11 10 grene. Only28 9 bones from type149 IV ulcers examined by 29 Total 57* 39 post-revascularisation *Four toes and a cuboid MRI bone were accurately diagnosed. Middle Middle phalanx phalanx (n) (n) 3 3 9 9 7 7 10 10 29 29 Proximal Proximal phalanx phalanx Metatarsal Metatarsal (n) (n) (n) (n) 3 1 3 1 11 8 11 8 14 10 14 10 18 15 18 15 46 34 46 34 Cuboid Cuboid (n) (n) 1 1 1 1 EWMA Journal 2015 vol 15 no 1 Science, Practice and Education Table 4. MRI and histopathological diagnosis of neuropathic ulcers (Type I; Neuropathic ulcers, Type III; neuropathic ulcers with infection) MRI diagnosis (n) Histopathological diagnosis (n) Type Ulcers(n) Bones(n) Correct Incorrect OM OM/BME OM/BME/N BME I 3 11 11 0 6 4 0 1 III 11 44 44 0 17 12 2 10 Total 14 55 55 0 Osteomyelitis (OM), bone marrow edema (BME), normal bone (N) N 0 3 The other 45 bones still could not be diagnosed because clinical outcomes of nonsurgical treatments have been of unclear or equivocal images. demonstrated with long-term courses of antibiotics2. If conservative surgery is chosen, the surgeon needs to know Histopathological analysis revealed osteomyelitis in 27 bones of type IV ulcers, but only 9 bones were correctly the precise area of osteomyelitis. If medical therapy were Table 5. MRI nd histopathological diagnosis ischemic ulcers (CLI) chosen, the duration of antibiotic therapy would depend diagnosed byapost-revascularisation MRI,of with a sensitiv(Type II; CLI, Type IV; CLI with infection) ity of 29.6%. on the presence and amount of residual dead or infected Margins of 49 bones wereGroup examined by histopathology bone2. Besides choosing primary therapy, identification of A; Pre-‐revascularization MRI diagnosis (Table 6). Of 37 bone margins of healed ulcers, 9 were the precise localization of DFO is therefore essential for MRI d iagnosis Histopathological diagnosis normal and 28 displayed bone marrow oedema. Of 12 appropriate treatment. OM/ OM/ bone margins of unhealed ulcers, 4 showed bone marrow MRI is a valuable tool for diagnosing osteomyelitis, Type Ulcers Bones Correct Incorrect* OM BME BME/N OM/G BME BME/N G N oedema and II 3** 8 were 33 gangrenous. 0 Of the 33 32 bone 4 margins 0 0 as well as 0 for defining 1 the 1 presence 27 and 0 anatomy of deep 3 with marrow the 4 0 soft displaying IV bone 5** 14 oedema, 0 28 healed 14 (87.5%) 3 and 5 tissue 1 infections 2 . Its2 efficacy 1 in accurately 0 that did not heal were from 2 patients with type III ulcers the extent of DFO of different aetiological types of ulcers Table 4. MTable Table RI and 44. . hM M istopathological RI RI aand nd hhistopathological istopathological diagnosis dodiagnosis oof f nneuropathic europathic ulcers uulcers lcers involving severe soft tissue infection and f iagnosis 2neuropathic patients with is not definitively known. Our previous studies4,5 have Group Post-‐revascularization MRI iagnosis (Type I; Neuropathic (Type (Type II; ; NNeuropathic europathic ulcers, Type uulcers, lcers, III; nBeuropathic TT; ype ype IIII; II; nneuropathic europathic ulcers with uulcers ilcers nfection) w wdith ith iinfection) nfection) type IV ulcers involving severe soft tissue infection and demonstrated the efficacy of MRI in diagnosing DFO ischemia. 8 gangrenous bone margins from of different aetiological types of ulcers, showing that for dMRI diagnosis MRI MRI d(dn) iagnosis iagnosis (Histopathological (n) n) Histopathological Histopathological diagnosis iagnosis iagnosis n) The MRI iagnosis 2 patients dHistopathological iagnosis d(dn) ((n) Type type Type Ulcers(n) Type Ulcers(n) Ulcers(n) Bones(n) Bones(n) Bones(n) Correct Correct Correct Incorrect Incorrect OM OM/ OM/BME OM OM OM/BME OM/BME OM/BME/N OM/BME/N OM/BME/N BME I, III), BME BME N DFO N N was reliably disOM/ with II ulcers could not be diagnosed by MRIIncorrect because neuropathic ulcers (type I Ulcers I I 3 Bones 3 3 11 11 11 11 11 11 0 OM BME 0 0 6 BME/N tinguishable 6 6 4 OM/G 4 4 0 from 0 0 BME/N 1 bone 0 1 1 oedema N 0 0 at any location, Correct Incorrect* BME G ofType severe ischemia. reactive 11 III III 7 11 11 44 44 44 7 44 44 0 0 0 0 17 0 17 17 12 12 2 4 2 2 10 2 3 10 10 0 1 3 3 II III 1** 44 0 0 12 in the presence of severe infection. Total 6** Total Total 14 40 14 14 55 55 55 -‐ 55 55 0 1 0 0 1 even 0 However, MRI IV 55 9 6 0 1 0 0 useful in1 diagnosing Osteomyelitis Osteomyelitis Osteomyelitis b one OM), marrow b-‐ bone one m marrow arrow (BME), eedema dema (12 (BME), BME), bone n4 normal ormal ( N) bbone one ( (N) N) not 3 (OM), ((OM), edema 31 normal 1 was 1 ischemic 9 0 ulcers (type II, IV) DISCUSSION because Osteomyelitis (OM), Bone marrow edema (BME), Normal bone (N), Gangrene (G) of insufficient interstitial fluid. Taken together, our *Because of unclear equivocal MRI findings, **One ulcer of Type II uprevious nderwent bconclusions oth pre-‐ and phave ost-‐ been confirmed by additional Positive results haveor been shown with conservative surgery vascularization MRI. combined with antibiotics9,10, and additional satisfactory cases in the present study. Table 5. M RI and istopathological diagnosis dodiagnosis f iagnosis ischemic lcers (CLI) Table Table 55. . h M M RI RI aand nd hhistopathological istopathological oof f uiischemic schemic uulcers lcers ((CLI) CLI) (Type II; CLI, Type with infection) (Type (Type III; I; CICV; LI, LI, C TLI Type ype IIV; V; CCLI LI w with ith iinfection) nfection) Group A; PGroup Group re-‐revascularization AA; ; PPre-‐revascularization re-‐revascularization MRI diagnosis M MRI RI ddiagnosis iagnosis Histopathological Histopathological iagnosis Histopathological diagnosis ddiagnosis OM/ OM/ OM/ OM/ OM/ OM/ Type Ulcers Incorrect* Incorrect* OM BME OM/G OM/G BME G N G Type Type Bones Ulcers Ulcers Correct Bones Bones Correct Correct Incorrect* OM OM BME/N BME BME BME/N BME/N OM/G BME/N BME BME BME/N BME/N G N N II 3** II II 33 3** 3** 33 33 0 0 0 33 33 4 33 0 4 4 0 0 0 0 0 0 1 0 0 1 1 1 27 1 1 0 27 27 0 0 IV 5** IV IV 14 5** 5** 14 14 0 0 0 14 14 3 14 5 3 3 0 5 5 0 0 1 2 1 1 2 2 2 1 2 2 0 1 1 0 0 MRI MRI MRI ddiagnosis iagnosis diagnosis Group B; PGroup Group ost-‐revascularization BB; ; PPost-‐revascularization ost-‐revascularization MRI diagnosis M MRI RI ddiagnosis iagnosis Histopathological diagnosis ddiagnosis Histopathological Histopathological iagnosis OM/ OM/ OM/ OM/ OM/ OM/ Type Ulcers Incorrect* Incorrect* OM BME OM/G OM/G BME G N G Type Type Bones Ulcers Ulcers Correct Bones Bones Correct Correct Incorrect* OM OM BME/N BME BME BME/N BME/N OM/G BME/N BME BME BME/N BME/N G N N II 1** II II 1** 1** 7 7 7 0 0 0 7 7 0 7 0 0 0 0 0 0 0 0 0 4 0 0 2 4 4 0 2 2 1 0 0 1 1 IV 6** IV IV 40 6** 6** 40 40 9 9 9 -‐ 1 -‐ -‐ 6 1 1 1 6 6 1 1 0 1 0 0 0 1 1 0 0 0 0 0 0 0 0 -‐ -‐ -‐ 31 31 12 31 4 12 12 1 4 4 1 1 3 1 3 3 1 1 1 9 1 1 0 9 9 0 0 Osteomyelitis Osteomyelitis Osteomyelitis (OM), Bone ((OM), OM), marrow BBone one edema m marrow arrow (BME), eedema dema Normal ((BME), BME), bone NNormal ormal (N), G bbone angrene one ((N), N), GG (G) angrene angrene ((G) G) *Because *Because o*Because f unclear ooof f r uuenclear quivocal RI findings, *f*One ulcer of Type II uoonderwent b oth pre-‐ babnd ppp ost-‐ nclear oor r eM equivocal quivocal M MRI RI findings, indings, ***One *One uulcer lcer f f TType ype III I uunderwent nderwent oth oth re-‐ re-‐ aand nd ppost-‐ ost-‐ vascularization MRI. vascularization vascularization M MRI. RI. EWMA Journal diagnosis MRI MRI MRI ddiagnosis iagnosis 2015 vol 15 no 1 11 Table 6. Histopathological examinations of the bone margin Bone margins (n) Healed ulcers 37 Unhealed ulcers 12 Total 49 Histopathological diagnosis Normal Bone marrow edema Bone marrow edema Gangrene Currently, the appropriate surgical margin for full remission of DFO is not known. In the present study, we examined 49 bone margins by histopathology and demonstrated that when the bone margin was set in the area of bone marrow oedema, the chances of cure were high, and that diligence was essential with cases of severe soft tissue infection or ischemia. We propose an appropriate surgical strategy based on MRI and histopathology. In neuropathic ulcers (type I and III), the localisation of osteomyelitis is identified by MRI and the surgical margins are determined on the MR images of the bone (in the area of bone marrow oedema), and the range of soft tissue infection. Because no methods are currently available for diagnosing the range of soft tissue infections, it has to be defined, in part, empirically. Type II ulcers, CLI, are of dry gangrene caused by ischemia, and preoperative MRI is not effective for diagnosis, therefore the site of resection has to be determined based on the sufficiency of blood supply after revascularisation. Type IV ulcers, CLI with infection, are the most difficult to treat because of the decision regarding which to carry out first, revascularisation for ischemia or debridement for infection. Except for cases requiring emergency debridement for infection, we advocate evaluation of osteomyelitis using MRI after revascularisation and setting of the bone margin in the area of bone marrow oedema. Thus, the appropriate surgical margin should be based on not only the range of osteomyelitis, but also on the range of soft tissue infection or the sufficiency of blood supply. Toes in each type(n) I 0 4 0 0 4 II 2 2 0 8 12 III 2 8 2 0 12 IV 5 14 2 0 21 Total 9 28 4 8 49 Our study has several limitations. First, the definitive diagnosis of DFO requires both histopathological findings and isolation of bacteria from bone samples2. To show the localisation of osteomyelitis, we used histopathological findings in the diagnosis. Second, our bone samples were from toes, metatarsals, and a cuboid bone. Although the forefoot is not the only site of diabetic foot ulcers, it is the most common11. Third, the classification6 chosen for categorizing ulcers is not universal. Our Kobe classification7, a hybrid of the University of Texas11 and the Wagner classification12, have recently been used in Japan. In Asia, type 2 diabetes is becoming epidemic, characterized by rapid rates of increase within a short period, onset at a relatively young age, and a low body mass index13. A distinct discipline of podiatric medicine such as that in United States or Europe is not available in Asia; therefore, the establishment of a classification system that is more relevant to Asian populations is necessary. In conclusion, although the present study comprised a limited number of patients, we were able to recommend an appropriate surgical margin and strategy based on MRI and histopathology. These continuing studies are therefore aimed at salvaging as much of the diabetic foot as possible. REFERENCES 1 Lipsky BA. Treating diabetic foot osteomyelitis primarily with surgery or antibiotics: have we answered the question? Diabetes Care 2014;37(3):593-5. 5 Fujii M, Armstrong DG, Terashi H. Efficacy of Magnetic Resonance Imaging in Diagnosing Diabetic Foot Osteomyelitis in the Presence of Ischemia. J Foot Ankle Surg 2013;52: 717-23. 2 Lipsky BA, Berendt AR, Cornia PB, Pile JC, Peters EJ, Armstrong DG et al. Infectious Diseases Society of America. 2012 Infectious Diseases Society of America clinical practice guideline for the diagnosis and treatment of diabetic foot infections. Clin Infect Dis 2012:54:e132-73. 6 Terashi H, Kitano I, Tsuji Y. Total management of diabetic foot ulcerations-Kobe classification as a new classification of diabetic foot wounds. Keio J Med 2011;60:17-21. 3 Lipsky BA, Peters EJG, Senneville E, Berendt AR, Embil JM, Lavery LA et al. Expert opinion on the management of infections in the diabetic foot. Diabetes Metab Res Rev 2012;28(1):163–78. 4 Fujii M, Terashi H, Tahara H. Efficacy of Magnetic Resonance Imaging in Diagnosing Osteomyelitis in Dabetic Foot Ulcers. J Am Podiatr Med Assoc 2014;104(1):24-9. 12 7 Rayman G, Vas PR, Baker N, Taylor CG Jr, Gooday C, Alder AI et al. The Ipswich Touch Test: A simple and novel method to identify inpatients with diabetes at risk of foot ulceration. Diabetes Care 2011;34:1517-8. 8 Morrison WB, Schweitzer ME, Batte WG, Radack DP, Russel KM. Osteomyelitis of the foot: relative importance of primary and secondary MR imaging signs. Radiology 1998;207:625-32. 9 Aragón-Sánchez J. Treatment of diabetic foot osteomyelitis: A surgical critique. Int J Low Extrem Wounds 2010;9:37-59. 10 Ha Van G, Siney H, Danan JP, Sachon C, Grimaldi A. Treatment of osteomyelitis in the diabetic foot. Contribution of conservative surgery. Diabetes Care 1996;19:1257-60. 11 Armstrong DG, Lavery LA, Harkless LB. Validation of a diabetic wound classification system: the contribution of depth, infection, and ischemia to risk of amputation. Diabetes Care 1998;21:855–9. 12 Wagner FW. The dysvascular foot: a system for diagnosis and treatment. Foot Ankle 1981;2:64–122. 13 Chan JC, Malik V, Jia W, Kadowaki T, Yajnik CS, Yoon KH, Hu FB. Diabetes in Asia: epidemiology, risk factors, and pathophysiology. JAMA 2009;301:2129– 40. EWMA Journal 2015 vol 15 no 1









© Copyright 2026