
Shiga Toxin 2 Induces Macrophage-Granulocyte Colonies from Cells
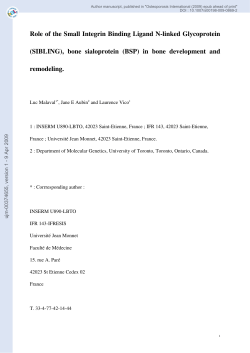
Shiga Toxin 2 Induces Macrophage-Granulocyte Colonies from Human Bone Marrow and Cord Blood Stem Cells Shin Chiyoda, Tae Takeda and Yosuke Aoki Infect. Immun. 2002, 70(9):5316. DOI: 10.1128/IAI.70.9.5316-5318.2002. These include: REFERENCES CONTENT ALERTS This article cites 21 articles, 1 of which can be accessed free at: http://iai.asm.org/content/70/9/5316#ref-list-1 Receive: RSS Feeds, eTOCs, free email alerts (when new articles cite this article), more» Information about commercial reprint orders: http://journals.asm.org/site/misc/reprints.xhtml To subscribe to to another ASM Journal go to: http://journals.asm.org/site/subscriptions/ Downloaded from http://iai.asm.org/ on June 11, 2014 by guest Updated information and services can be found at: http://iai.asm.org/content/70/9/5316 INFECTION AND IMMUNITY, Sept. 2002, p. 5316–5318 0019-9567/02/$04.00⫹0 DOI: 10.1128/IAI.70.9.5316–5318.2002 Copyright © 2002, American Society for Microbiology. All Rights Reserved. Vol. 70, No. 9 Shiga Toxin 2 Induces Macrophage-Granulocyte Colonies from Human Bone Marrow and Cord Blood Stem Cells Shin Chiyoda,1 Tae Takeda,2 and Yosuke Aoki3* Nagasaki Red Cross Blood Center, Nagasaki,1 and Department of Infectious Diseases Research, National Children’s Medical Research Center,2 and Department of Food and Health Sciences, Faculty of Human Life Sciences, Jissen Women’s University,3 Tokyo, Japan Received 23 April 2002/Returned for modification 17 May 2002/Accepted 27 May 2002 into ␣-medium (Flow Lab) with a Pasteur pipette and made into single-cell suspensions by repeated pipetting. Umbilical cord blood was obtained at the time of delivery after uncomplicated full-term pregnancy. Buffy coat cells obtained from umbilical cord blood were suspended in ␣-medium. Informed consent was obtained from all subjects. Methylcellulose culture was carried out according to the method of Iscove et al. (13). One milliliter of culture mixture containing 2 ⫻ 105 nucleated bone marrow cells or 2 ⫻ 105 to 4.5 ⫻ 105 cord blood mononuclear cells, ␣-medium, 1.35% methylcellulose, 30% fetal bovine serum, 1% deionized bovine serum albumin, 10⫺4 M 2-mercaptoethanol, growth factors, and various amounts of Stx was plated on each 35-mm culture dish. Cultures were incubated at 37°C in a humidified 4.6% CO2 air incubator for 16 days. All cultures were conducted in triplicate. Distinct groups of cells containing 40 cells or more were counted as colonies. Individual colonies were stained using the May-Giemsa method to identify cell types within each colony. Granulocyte-macrophage (GM) colonies were defined as those containing mainly granulocytes, and macrophage (M⌽) colonies contained M⌽ almost exclusively. HL-60 cells (established from human acute myelogenous leukemia cells) and Jurkat cells (established from human acute lymphocytic leukemia cells) were cultured in RPMI 1640 medium (104 cells/ml) in the presence or absence of Stx1 or Stx2 for 72 h, and the proliferation status of each cell line was determined by the Celltiter 96 aqueous nonradioactive cell proliferation assay method (Promega Co. Ltd.). Experiments were each conducted at least three times, with similar results. Statistical analysis was performed with Student’s t test. As shown in Table 1, adding Stx2 in culture resulted in the appearance of both GM and M⌽ colonies, with predominantly M⌽ colonies. In contrast, adding granulocyte colony-stimulating factor (G-CSF), interleukin-1 (IL-1), or IL-3 with stem cell factor (SCF) induced GM colonies more predominantly than M⌽ colonies. Adding G-CSF to the bone marrow cell culture containing Stx2 markedly increased the number of GM colonies above that in the culture containing only Stx2 or G-CSF alone (P ⬍ 0.001). Almost the same synergistic effect In 10 to 14% of patients infected with Escherichia coli O157: H7, hemolytic uremic syndrome (HUS) develops 1 week after the onset of diarrhea (8, 9, 14, 17). HUS is an acute, mainly pediatric illness characterized by acute hemolytic anemia with typical fragmented red blood cells, thrombocytopenia, and neuropathy. Highly elevated granulocytosis has been documented in many cases (15), including four cases seen by Gasser et al. (10), who first reported HUS in 1955. The occurrence of granulocytosis is not surprising, because many patients with bacterial infections such as those from E. coli, Shigella, Salmonella, or pneumococci usually show a rising granulocyte count in the peripheral blood. The level of granulocytosis in patients with E. coli O157:H7 infection, however, is extraordinarily high and correlates well with the severity of the illness. Among E. coli O157:H7 virulence factors, Shiga toxin (Stx) is a major pathogenic factor in HUS development. Using a mouse model, we demonstrated that injecting Stx2 into the peritoneal cavity of mice caused marked (sevenfold) granulocytosis in the peripheral blood. Elevated granulopoiesis and suppressed erythropoiesis have been observed in the bone marrow of mice injected with Stx2 (5). In order to clarify the mechanism behind granulocytosis in HUS, we studied the direct effect of Stx’s on bone marrow stem cell differentiation by using human bone marrow cell culture. The effect on stem cells in the cord blood was also examined. Stx2 was purified from a recombinant strain carrying the Stx2 gene by a method described elsewhere (21). Stx1 was purified from E. coli O157:H7 by the method of Noda et al. (16). The amount of lipopolysaccharide in the Stx preparations, which was determined by using a Limulus amebocyte lysate (Pregel-M; Teikokuzoki Co. Ltd., Tokyo, Japan), was less than 2.5 pg in 1 ng of purified Stx. Bone marrow cells were obtained by sternal puncture with a heparinized plastic syringe from a healthy volunteer and centrifuged at 170 ⫻ g for 10 min. Buffy coat cells were aspirated * Corresponding author. Mailing address: Faculty of Human Life Sciences, Jissen Women’s University, Osakaue 4-1-1, Hino-city, Tokyo, Japan 191-8510. Phone: 81-42-585-8892. Fax: 81-42-585-8892. E-mail: [email protected]. 5316 Downloaded from http://iai.asm.org/ on June 11, 2014 by guest Addition of Shiga toxin 2 to human bone marrow or cord blood cell culture induced macrophage-granulocyte colonies. Although Shiga toxin 2 alone induced colonies mainly composed of macrophages, it induced colonies mainly consisting of granulocytes when combined with physiological doses of interleukin-1, granulocyte colony-stimulating factor, or stem cell factor with interleukin-3. VOL. 70, 2002 NOTES TABLE 1. Effect of Stx’s on colony formation from human bone marrow stem cells M No addition Stx1 (10) Stx1 (50) Stx1 (100) Stx2 (10) Stx2 (50) Stx2 (100) G-CSF (100) G-CSF (100) ⫹ Stx1(50) Stx2 (50) ⫹ G-CSF (100) Stx2 (50) ⫹ G-CSF (100) ⫹ Stx1 (50) SCF (5,000) ⫹ IL-3 (500) Stx2 (50) ⫹ SCF (5,000) ⫹ IL-3 (500) IL-1 (100) Stx2 (50) ⫹ IL-1 (100) IL-1␣ (50) Stx2 (50) ⫹ IL-1␣ (50) 0 0 0 0 0 2.3 ⫾ 2.0 3.7 ⫾ 0.6 15 ⫾ 3.0 17 ⫾ 2.0 26 ⫾ 3.5 25 ⫾ 2.5 16 ⫾ 2.5 25 ⫾ 4.2 2.3 ⫾ 0.7 15 ⫾ 1.7 1.3 ⫾ 1.0 1.3 ⫾ 1.0 0 0 0 0 7.7 ⫾ 1.5 12 ⫾ 1.5 12 ⫾ 2.5 5.0 ⫾ 2.0 5.7 ⫾ 0.6 2.0 ⫾ 1.0 1.3 ⫾ 1.5 1.7 ⫾ 0.6 3.3 ⫾ 2.3 1.3 ⫾ 0.6 3.3 ⫾ 0.6 1.3 ⫾ 1.0 2.0 ⫾ 1.0 Cytokine or Stx added (pg/dish) No addition Stx1 (10) Stx1 (50) Stx1 (100) Stx2 (10) Stx2 (50) Stx2 (100) G-CSF (100) Stx2 (10) ⫹ G-CSF (100) SCF (5,000) ⫹ IL-3 (500) Stx2 (50) ⫹ SCF (5,000) ⫹ IL-3 (500) IL-1 (100) Stx2 (50) ⫹ IL-1 (100) IL-1␣ (50) Stx2 (50) ⫹ IL-1␣ (50) a No. of colonies/disha GM 0 0 0 0 4.0 ⫾ 0 6.0 ⫾ 1.0 9.3 ⫾ 0.6 14 ⫾ 1.0 23.7 ⫾ 2.1 12 ⫾ 1.0 28 ⫾ 2.0 4.3 ⫾ 0.8 21 ⫾ 1.2 0.7 ⫾ 0.6 1.3 ⫾ 1.0 M 0 0 0 0 10 ⫾ 2.0 20 ⫾ 0.6 17 ⫾ 1.2 4.7 ⫾ 1.2 3.0 ⫾ 1.0 11 ⫾ 2.3 8.0 ⫾ 2.6 1.3 ⫾ 0.6 2.7 ⫾ 1.2 0.7 ⫾ 0.6 1.0 ⫾ 0 Results are the mean ⫾ standard deviation of triplicate experiments. Results are the mean ⫾ standard deviation of triplicate experiments. was obtained when IL-1 was added to culture containing Stx2 (P ⬍ 0.001) or IL-3 with SCF instead of IL-1 (P ⬍ 0.05), as shown in Table 1. Addition of cytokines and Stx2 had almost the same effect on colony formation of human cord blood stem cells as for human bone marrow stem cells (Table 2). Addition of IL-1␣ alone to bone marrow or cord blood stem cell culture caused negligible colony formation, and the colony-stimulating effect of Stx2 was rather inhibited by IL-1␣. No colonies developed when various amounts of Stx1 were added to the culture (Tables 1 and 2). Addition of Stx1 to the culture containing G-CSF failed to change the number of colonies induced by G-CSF, and the presence of Stx1 in the culture containing both Stx2 and G-CSF did not alter the number of colonies induced by both Stx2 and G-CSF (Table 1). The culture containing Stx1(100 pg/dish) failed to increase the number of dead cells compared with controls. The proliferation status of both HL-60 and Jurkat cells did not change with the addition of Stx1 or Stx2 (Fig. 1). These results indicate that Stx1 has no toxic effect on bone marrow stem cells. Heat- denatured Stx2 (boiled for 10 min) had no colony-stimulating activity in either human bone marrow or cord blood cell cultures. Recently, it was shown showed that intraperitoneal injection of sublethal doses of Stx2 into mice caused marked granulocytosis in peripheral blood (5). Accordingly, we assayed in vitro colony formation to analyze the direct effect of Stx2 on human bone marrow and cord blood stem cells. We found that adding Stx2 to human bone marrow cell culture induced mainly M⌽ colonies. We further found that it induced a large number of GM colonies when cytokines such as G-CSF, IL-1, or SCF plus IL-3 were added. These results strongly suggest that Stx2 induces granulocytosis in the peripheral blood by directly or indirectly stimulating bone marrow stem cells to develop into GM colonies in vivo. Elevated granulocytosis in patients with bacterial infections is believed due to endotoxin (lipopolysaccharide), which is a cell wall pleiotropic component. However, no report has, to our knowledge, postulated the possibility that bacterial exotoxin (protein) is a factor in granulocytosis. This is the first report that Stx2 stimulates granulopoiesis directly or in FIG. 1. Effects of Stx1 and -2 on the proliferation status of bone marrow-derived cells. Jurkat cells (white) and HL-60 cells (gray) were cultured in the presence of Stx1 (A) or Stx2 (B). Bars indicate the standard deviation (n ⫽ 3). Downloaded from http://iai.asm.org/ on June 11, 2014 by guest GM a TABLE 2. Effect of Stx’s on colony formation from cord blood stem cells No. of colonies/disha Cytokine and/or Stx added (pg/dish) 5317 5318 NOTES INFECT. IMMUN. REFERENCES 1. Aoki, Y. 1986. The mechanism of activation of human natural killer cells by medullasin. Jpn. J. Cancer Res. 77:1018–1026. Editor: J. T. Barbieri 2. Aoki, Y., and R. Machinami. 1982. Medullasin and inflammation. Asian Med. J. 26:15–37. 3. Aoki, Y., and R. Machinami. 1983. Role of medullasin in granulocytes in the development of inflammation. I. Phlogistic activity and the effect on functions of macrophages and granulocytes. Arthritis Rheum. 26:1002–1010. 4. Aoki, Y., M. Sumiya, and Y. Oshimi. 1982. Medullasin enhances human natural killer cell activity. J. Clin. Investig. 69:1223–1230. 5. Aoki, Y., Y. Yoshida, and T. Takeda. 1999. Shiga toxin 2 promotes the stem cell differentiation into granulocytes in the bone marrow causing granulocytosis in the peripheral blood. J. Infect. 39:97–98. 6. Boerlin, P., S. A. Mcween, F. Boerlin-Petzold, J. B. Wilson, R. P. Johnson, and C. L. Glyles. 1999. Associations between virulence factors of Shiga toxin-producing Escherichia coli and disease in humans. J. Clin. Microbiol. 37:497–503. 7. Bolande, R. P., and B. S. Kaplan. 1985. Experimental studies on the hemolytic uremic syndrome. Nephron 39:228–236. 8. Carter, A. O., A. A. Borczyk, A. A. K. Carlson, B. Harvey, J. A. Hockin, M. A. Karmali, C. Krishman, D. A. Korn, and H. L. Lior. 1987. A severe outbreak of Escherichia coli O157:H7-associated hemorrhagic colitis in a nursing home. N. Engl. J. Med. 317:1496–1501. 9. Fong, J. C. S., J.-P. de Chadere’vian, and B. S. Kaplan. 1982. The hemolytic uremic syndrome: current concept and management. Pediatr. Clin. North Am. 29:835–856. 10. Gasser, C., E. Gauthier, A. Steck, R. E. Sieberman, and R. Oechslir. 1955. Hemolytic uremic syndrome: bilateral renal cortex necrosis by acute acquired hemolytic anemia. Schweiz. Med. Wochenenschr. 38:905–909. 11. Gianantonio, C. A., M. Vitacco, F. Mendilahazu, A. Ruffy, and J. Mendilahazu. 1964. The hemolytic uremic syndrome. J. Pediatr. 64:478–491. 12. Hase-Yamazaki, T., and Y. Aoki. 1995. Stimulation of human lymphocytes by cathepsin G. Cell. Immunol. 160:24–32. 13. Iscove, N. N., F. Sieber, and K. H. Winterhalter. 1974. Erythroid colony formation in cultures of mouse and human bone marrow: analysis of the requirement for erythropoietin by gel filtration and affinity chromatography on agarose-concanavalin A. J. Cell. Physiol. 83::309–320. 14. Kaplan, B. S., P. D. Thompson, and J.-P. de Chadare’vian. 1976. The hemolytic uremic syndrome. Pediatr. Clin. North Am. 23:761–777. 15. Martin, D. S., I. Walters, U. Matthei, J. Mitchel, T. Dillon, and M. Barrat. 1989. Polymorphonuclear leukocyte count in childhood hemolytic uremic syndrome. Pediatr. Nephrol. 3:130–134. 16. Noda, M., T. Yotsudo, N. Nakabayashi, T. Hirayama, and Y. Takeda. 1987. Purification and some properties of Shiga toxin from Escherichia coli O157:H7 that is immunologically identical to Shiga toxin. Microb. Pathol. 2:339–349. 17. Ostroff, S. M., J. M. Kobayashi, and J. A. Lewis. 1989. Infections with Escherichia coli O157:H7 in Washington state. JAMA 262:355–359. 18. Shumwy, C. N., K. L. Telplan, C. F. Piel, and R. H. Philibbs. 1966. The hemolytic uremic syndrome. Pediatr. Clin. North Am. 13:295–314. 19. Vedanarayanan, V. V., B. S. Kaplan, and J. C. S. Fong. 1987. Neutrophil function in an experimental model of hemolytic uremic syndrome. Pediatr. Res. 21:252–256. 20. Yamazaki, T., and Y. Aoki. 1998. Cathepsin G enhances human natural killer cell activity. Immunology 93:115–121. 21. Yotsudo, T., N. Nakabayashi, T. Hirayama, and Y. Takeda. 1987. Purification and some properties of a vero toxin from Escherichia coli O157:H7 that is immunologically unrelated to Shiga toxin. Microb. Pathol. 3:21–30. Downloaded from http://iai.asm.org/ on June 11, 2014 by guest combination with cytokines such as G-CSF, IL-1, or SCF plus IL-3, causing marked granulocytosis in the peripheral blood Leukocytes contain several agents that damage tissue, especially vascular endothelial cells. Infiltration of neutrophils in the kidney was mentioned in early reports on HUS (11, 18). Bolande and Kaplan (7) studied leukocytes in the buffy coat of patients with HUS soon after onset and noted that, in some cases, a tactile relationship existed between leukocyte cell processes and altered red blood cell walls and that leukocytes had abnormal morphologies with cytoplasmic projections. Vedanarayanan et al. (19) reported neutrophil function in an experimental rabbit model using an endotoxin-derived modified generalized Schwartzman reaction to understand the role of neutrophils in HUS. They speculated that neutrophil activation may be a mechanism of renal injury in this model. Characteristic functions of granulocytes are derived from proteases in lysozomes. In addition to bactericidal activity and tissue destruction in inflammation, granulocyte proteases, especially neutral proteases, have a broad spectrum of functions. Both medullasin and cathepsin G enhance DNA synthesis of human lymphocytes (2, 12). They also enhance human NK cell activity (1, 4, 20). Medullasin induces inflammation by injuring endothelial cells in vessels and accumulating both M⌽ and granulocytes when injected into rabbit or guinea pig skin (3). Intraperitoneal injection of Stx2 into mice enhanced medullasin levels in granulocytes (unpublished data), and so elevated medullasin in granulocytes would appear to be an important risk factor for HUS. Surprisingly enough, Stx1 did not show the same functions as Stx2. We previously believed that Stx1 and Stx2 have similar functions, although one paper reported that Stx2 had more potent toxicity than Stx1 (6). Our results suggest differences in the pathogenic mechanism between these two toxins. The primary structures of both have 55% homology in the A and B subunits. The responsive structure of Stx2 in granulocytosis is to be analyzed in a future study.









© Copyright 2026