ABC
docz
Explore
Log in
Create new account
Download
Report
No category
Plan Review Application - Flathead City
Mobile Food Service - Flathead City
Flathead City-County Health Department Food Establishment Plan
Form - Single Window System
The Orissa Shops and Commercial Establishment Rules, 1958
STRATA CLEANING
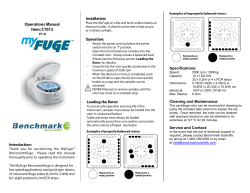
C1012 MyFuge Operations Manual - BE/CS 196a
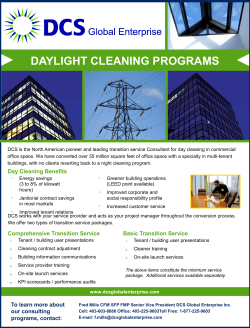
Daylight Cleaning Services Brochure
INEC AD-HOC STAFF FOR 2015 GENERAL ELECTIONS
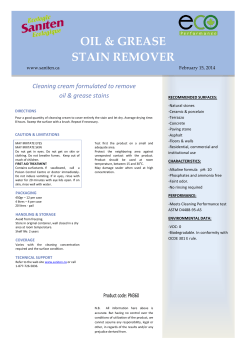
Cleaning cream formulated to remove oil & grease stains RECOMMENDED SURFACES:
Tile & Grout Care Special - Applied Products Australia
ServSafe Chapter 10 Sanitary Facilities and Equipment
© Copyright 2026
About abcdocz
DMCA / GDPR
Report