
Titan Total Shoulder System Fracture Surgical Technique
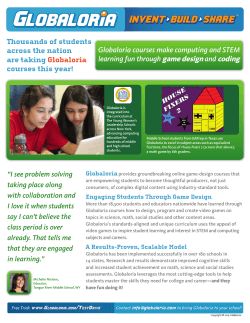
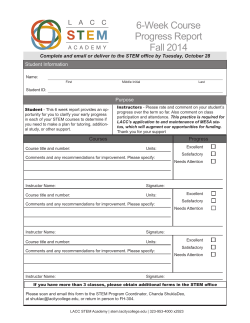
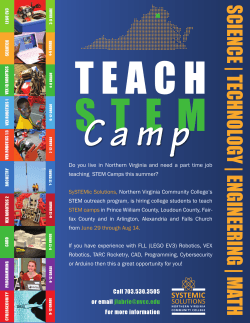
Integra® Titan™ Total Shoulder System FRACTURE SURGICAL TECHNIQUE Table of Contents Design Rationale........................................................................................................................................................................................................02 Indications/Contraindication/Warnings/Precautions.........................................................................................................................................03 Surgical Technique.................................................................................................................................................................................................... 04 Step 1: Preoperative Templating & Patient Positioning.......................................................................................................................................05 Step 2: Exposure.........................................................................................................................................................................................................05 Step 3: Head Excision and Sizing............................................................................................................................................................................ 06 Step 4: Humeral Canal Preparation........................................................................................................................................................................ 06 Step 5: Distal Trial Stem and Proximal Trial Body Insertion................................................................................................................................ 06 Step 6: Head Trialing and Restoring Humeral Height..........................................................................................................................................07 Step 7: Trial Reduction...............................................................................................................................................................................................07 Step 8: Diaphysis Preparation for Tuberosity Repair..............................................................................................................................................08 Step 9: Prosthesis Assembly and Implantation.................................................................................................................................................... 08 Step 10: Bone Grafting and Tuberosity Repair...................................................................................................................................................... 09 Step 11: Closure.......................................................................................................................................................................................................... 09 Revision Procedure.................................................................................................................................................................................................... 10 Long Stem Option...................................................................................................................................................................................................... 10 Essential Product Information.................................................................................................................................................................................. 11 Instrumentation..........................................................................................................................................................................................................13 Implant Catalog Numbers & Dimensions.............................................................................................................................................................. 19 Design Rationale Titan Proximal Humerus Fracture Solution The Titan Total Shoulder System provides a unique way to address what may be seen as a difficult procedure. Titan’s modular stem design allows the surgeon to mix component sizes to best fit patient anatomy. The ability to press-fit the hemiarthroplasty humeral prosthesis to address proximal humerus fractures gives an advantage of intraoperative height adjustment without need for jigs or the use of cement. • Interchangeable proximal bodies and distal stems to accommodate varying patient anatomy. • Multiple fixation options (press-fit vs. cemented) to address varying bony quality. • Bone impaction humeral preparation technique to preserve bone stock. • Well-fixed stem provides an intraoperative building platform and a pathway for revision. Heads 26 Eccentric & Concentric Humeral Heads in Various Heights • Optimal osteotomy coverage and soft tissue balancing Bodies Textured Modular Bodies in 3 Heights • Allow for intraoperative height adjustment • Smaller proximal body size promotes tuberosity consolidation and increased union opportunity • Addresses varying patient anatomy • Promotes initial and long-term bone fixation Concentric Head Eccentric Head Body Screw Fracture Body Cemented Stem Press-Fit Stem Polished Suture Holes and Groove • For added bone and soft tissue fixation • May reduce suture abrasion Height Lines • To help simplify replication of trial to definitive prosthesis height placement Stems Press-Fit Stem Option • No need to remove cement in case of revision • Bone impaction humeral preparation to preserve bone stock • 12 splines on stem contribute to enhanced press fit and anti-rotation for a well fixed stem Cemented Stem and Cemented Long Stem Options to Address Varying Bone Quality • Smooth, fluted stem allows for optimal cement fixation and rotational control • 5 stem diameters ranging from 6-14 mm to address varying humeral sizes • Long Stems in 8, 10 and 12mm diameter options; all available in 125mm and 165mm lengths • Tapered, polished distal stem for ease of insertion Titan Total Shoulder System was developed in collaboration with: Joseph Abboud, M.D. Phillip Duke, MB.BS, FRACS, FA(ORTH)A William Geissler, M.D. Sanford Kunkel, M.D. Anand Murthi, M.D. Matthew Ramsey, M.D. Mark Ross, MB.BS.FRACS(ORTH) 2 Indications For Use Total Shoulder Arthroplasty or Hemiarthroplasty is indicated for: • Severely painful and/or disabled joint resulting from osteoarthritis, traumatic arthritis or rheumatoid arthritis. • Fracture-dislocations of the proximal humerus where the articular surface is severely comminuted, separated from its blood supply or where the surgeon’s experience indicates that alternative methods of treatment are unsatisfactory. • Other difficult clinical problems where shoulder arthrodesis or resection arthroplasty are not acceptable (e.g. – revision of a failed primary component). Shoulder Hemiarthroplasty is also indicated for: • Ununited humeral head fractures. • Avascular necrosis of the humeral head. • Rotator cuff arthropathy. • Deformity and/or limited motion. The humeral component is intended for cemented or un-cemented use. The glenoid component is intended for cemented use only. Contraindications The following conditions are contraindications for total shoulder arthroplasty and hemiarthroplasty: • Active local or systemic infection. • Inadequate bone stock in the proximal humerus or glenoid fossa for supporting the components. • Poor bone quality, such as osteoporosis, where there could be considerable migration of the prosthesis and/or a chance of fracture of the humerus or glenoid. • Absent, irreparable or nonfunctional rotator cuff or other essential muscles. • Pregnancy. • Muscular, neurologic, or vascular deficiencies that compromise the affected extremity. • Known metal allergies. Warnings The use of a glenoid prosthesis in patients with cuff tear arthropathy could increase the risk of glenoid component loosening due to non-anatomic loading conditions. The following conditions tend to adversely affect shoulder replacement implants; • Excessive patient weight • High levels of patient activity • Likelihood of falls • Poor bone stock • Metabolic disorders • Disabilities of other joints Precautions • Do not reuse this device. Reuse of this product may result in infection or other systemic complication that may affect the patient’s overall health. Additionally, the reuse of this product could adversely affect function of the device. Any implant that has been damaged, mishandled, or removed from the sterile field may have surface damage that could result in implant fracture and/or particulate and should be discarded. • The MR environment presents risks to patients with metal implants. Review of the available literature documents that metal implants may heat resulting in tissue damage and may migrate out of position. They may also cause artifact affecting image quality. Physicians should take these risks into consideration when recommending MRI imaging for patients with metal implants. Note: The Titan Reverse Shoulder System and Titan Total Shoulder System have not been evaluated for safety and compatibility in the MR environment. Neither the Titan Reverse Shoulder System nor the Titan Total Shoulder System has been tested for heating or migration in the MR environment. 3 Surgical Technique As the manufacturer of this device, Integra does not practice medicine and does not recommend this or any other surgical technique for use on a specific patient. The surgeon who performs any implant procedure is responsible for determining and using the appropriate techniques for implanting the device in each patient. Proper surgical procedures and techniques are the responsibility of the medical professional. Individual surgeon evaluation of the surgical technique should be performed based on his or her personal medical training and experience. This essential product information does not include all of the information necessary for selection and use of a device. Please see full labeling on package insert for all necessary information. The goal of hemiarthroplasty for fracture is to replace the humeral head with a prosthetic component, reconstruct the rotator cuff, and repair the tuberosities by securing to both the humeral shaft and the prosthesis. Introduction A hemiarthroplasty is indicated when salvage of the native humeral head is not possible. This is the case in most head-splitting fractures of the humeral head, and in impression fractures involving more than 40% of the head. In a typical or “classic” four-part fracture, the humeral head fragment is separate from the shaft and both tuberosities, and is dislocated out of the glenoid. Figure 1. The greater and lesser tuberosities are separated from the head fragment, and may be separated from each other. The head is devoid of all soft-tissue attachment, creating a high probability of avascular necrosis. For this reason, a hemiarthroplasty is typically used in older patients. In younger patients, especially those with a “valgus impacted” pattern, internal fixation may be preferred. Description Displaced 4-Part Fracture Of Proximal Humerus The pathophysiology of displaced 4-part fractures involves each muscle or muscle group pulling fragments in various directions. Figure 2. The diaphysis (1) is drawn medially by the pectoralis major and latissimus dorsi muscles and is separated from the epiphysis at the surgical neck. The lesser tuberosity (2) is retracted anteromedially by the subscapularis. The greater tuberosity (3) is retracted medially, superiorly and posteriorly by the supraspinatus, infraspiratus and teres minor. The tuberosities may remain intact or be fragmented, and may be separated or remain in continuity with one another (impacted type). The humeral articular surface (4) is no longer in contact with the glenoid. It is separated from the tuberosities and may undergo varus or valgus displacement, usually resulting in devascularization. It may present an impacted fracture or a displaced fracture. 1 2 3 4 2 1 4 Step 1 • Preoperative Templating and Patient Positioning 3 Preoperative evaluation of the humerus using the modular total shoulder x-ray templates helps determine the size of the prosthesis and proper height restoration. Hemiarthroplasty for proximal humerus fracture can be performed using general anesthesia, regional anesthesia (i.e., interscalene block), or a combination. Place the patient in beach chair position, Figure 3. This position would have the patient supine with the hips flexed approximately 30°, knees bent approximately 30° and back elevated approximately 30°. Specialized headrests, such as the Mayfield or the McConnell, arm mounts or operating tables with breakaway side panels can facilitate further access to the top and back of the shoulder. 4 Step 2 • Exposure A deltopectoral approach is used to provide exposure to the anterior aspect of the glenohumeral joint, the upper humeral shaft and the humeral head. The initial incision line runs from the mid-clavicle, over the top of the coracoid and extends in a straight line down the anterior aspect of the arm, Figure 4. It should follow the path of the cephalic vein along the interval between the deltoid and the pectoralis major. The length of the initial incision along this line can vary, depending on the exposure needed to provide adequate access and visualization of the joint, and is determined by patient body habitus. 5 Once the initial incision is made, expose, incise and release the fascia. Locate the cephalic vein at the deltopectoral interval. Separate the deltoid and pectoralis major muscles so that the deltoid muscle is completely free from its origin to its insertion, especially along its deep surface. Abduct and externally rotate the arm. Gently retract laterally the cephalic vein along with the deltoid muscle. Incise the clavipectoral fascia lateral to expose the conjoined tendon. If needed, release the upper 25% of the pectoralis major tendon from its insertion on the humerus, using an electrocautery cutting blade. Figure 5. Place a Hohmann retractor over the top of the humeral head, pulling the upper part of the deltoid posteriorly. Check that the rotator cuff tendons are intact. Introduce self-retaining Weitlander or Kobel retractors underneath the conjoined tendon and underneath the middle deltoid. It is important to always save or preserve the coracoacromial ligament. 6 Isolate, clamp and ligate or coagulate the anterior humeral circumflex vessels lying across the anterior/inferior third of the subscapularis tendon. In Fracture cases it is important to be aware of the musculocutaneous nerve, which penetrates the coracobrachialis muscle 3-5 cm distally from the coracoid. The nerve may not be palpable within the surgical field, but note its proximity to the conjoined tendon. Figure 6. Introduce a Hohmann retractor and carefully retract the Axillary nerve along with the latissimus dorsi tendon. This is especially important as it will protect the axillary nerve, define and expose the inferior capsule. Locate the biceps tendon, it can be used to identify the area between the lesser and greater tuberosity. Using scissors dissect the sheath of the biceps tendon and divide the transverse humeral ligament. Figure 7. 5 7 Step 2 • Exposure (continued) 8 Release the Biceps tendon from the bicipital groove and along the rotator interval down to its glenoid attachment. Resect the long head of the biceps at the origin of the superior glenoid at the transverse humeral ligament. Step 3 • Head Excision and Sizing With the tuberosities retracted out of the way via stay sutures or retractors, use a towel clip or bone hook to remove the humeral head and all fractured pieces. Figure 8. Measure the removed humeral head on the Head Sizing Gauge, Figure 9. Once size has been determined harvest any cancellous bone out of the humeral head you may need for grafting later in the procedure. 9 Step 4 • Humeral Canal Preparation Attach the 6mm Humeral Stem Trial to the Stem Trial Handle. With the arm in adduction, external rotation and extension begin sequential trialing starting with the 6mm Humeral Stem Trial. Follow the path created through the intramedullary canal and increase the Stem Trial diameter in 1mm increments until the Stem Trial fits securely in the humerus. Figure 10. Note the final Humeral Stem Trial diameter. This will determine the size of the Humeral Stem implant. Reduce the tuberosities around the Stem Trial Handle. Using the laser lines, estimate the body height needed. Step 5 • Distal Trial Stem and Body Insertion Attach the selected Stem Trial to the standard size Fracture Body Trial. Attach the Body/ Stem Trial construct to the Fracture Trial Inserter/Extractor. 10 11 Affix the Version Rod to the Fracture Trial Inserter/Extractor to ensure proper version. The Version Rod is aligned parallel with the patient’s forearm and initially sets the trial in 30° of retroversion. Using the Slotted Mallet, carefully drive the Body/Stem Trial into the proximal humerus so that the Body/Stem Trial is in line with the long axis. Seat the Body/ Stem Trial until the desired fit is achieved, Figure 11. 6 Step 5 • Distal Trial Stem and Body Insertion (continued) The Body/Stem Trial should be positioned at the correct height to preserve the anatomic reconstruction of the tuberosities. If the Fracture Body Trial is too short, the prosthesis will not allow space for the anatomic reconstruction of the tuberosities. Figure 12. If this happens remove the Standard Fracture Body Trial and replace with the Large Fracture Body Trial. This will increase the overall prosthesis height and allow for more surface area and proper reconstruction of the tuberosities. Figure 13. If the overall prosthesis is too proud with the Standard Fracture Body Trial, replace it with the Small Fracture Body Trial. Placing the prosthesis at the proper level will allow space for anatomic reconstruction of the tuberosities. If more height is desired after increasing to a Large Fracture Body Trial, increasing stem diameter will result in a higher seated prosthesis. A slight overlap of the tuberosities on the prosthesis is desirable. 12 Incorrect Height 13 Remove the Inserter/Extractor. STEP 6: Head Trialing and Restoring Humeral Height Place the Taper Adapter onto the Fracture Body Trial using the Taper Adapter Shaft and attach the previously selected size Head Trial to the fracture body, Figure 14. This size was selected after removal and sizing of the humeral head (Table below shows head options). WIDTH HEIGHT 38 14* 40 15* 42 16 44 16, 19 46 14, 17, 20 48 15, 18, 21 50 19, 22 52 20 Correct Height 14 15 *Only Eccentric Head Option STEP 7: Trial Reduction Note the height etchings on the side of the Fracture Body Trial to replicate height of final implant. Figure 15. Perform a trial reduction and range of motion test. Ensure that the humeral head remains in the glenoid fossa and does not ride too high. Also ensure there is free motion with no undue tightness. Adjust Fracture Body Trial height or Head Trial if there is any height or soft tissue balance issues. Figure 16. Reduce the tuberosities to ensure they will fit around the prosthesis and can be attached to one another. A towel clip or reduction forcep can be utilized to hold the tuberosities around the prosthesis. Check soft tissue tensioning by performing a gentle range of motion test. 7 16 Step 8 • Diaphysis Preparation for Tuberosity Repair 17 Drill two suture holes, one on each side of the bicipital groove, into the humeral shaft to assist in repair of the tuberosities. Place two heavy non-absorbable sutures through the drill holes before proceeding with prosthesis implantation. Figure 17. Step 9 • Prosthesis Assembly and Implantation Body Stem Assembly Select and remove from their packaging the final sized Fracture Body and Humeral Stem that corresponds to the trials. Seat and secure the Fracture Body implant onto the Stem Impaction Stand. Place the Humeral Stem implant onto the Humeral Body with finger pressure. Place the Stem Impactor over the tip of the humeral stem and engage the tapers with a few mallet strikes. Figure 18A. 18A 18B Remove the final Fracture Body/Stem implant construct from the Stem Impaction Stand and place the implant into the Head Impaction Stand with the appropriate size Head Impaction Stand Insert. The Head Impaction Stand should match the size of your Body Trial (SML, STD, LRG) Figure 18B. Tighten the knob on the side of Head Impaction Stand to secure the implant. Remove the Humeral Body Screw from its packaging and insert into the Humeral Body with the Driver Handle, Torque Limiter and 1/8 Hex Driver. Tighten the screw until the torque limiter clicks. Figure 18B. Cemented Stem Thoroughly irrigate the medullary canal to remove debris. Use either a small piece of cancellous bone or utilize a cement restrictor and place 1-2 cm below distal stem to prevent cement from extruding to the elbow. Use either a medium or high viscosity cement, place cement down the humeral canal using finger pressure. Figure 19. Cemented Stem options are available in 2 mm increments (6-14 mm). A definitive prosthesis sized 1-2 mm smaller than Stem Trial used should be selected to allow for adequate cement mantle. Attach the final prosthesis to the Fracture Implant Inserter/ Extractor. Affix the Version Rod to the Inserter/Extractor to ensure proper version and use hand pressure to insert prosthesis. The Version Rod is aligned parallel with the patient’s forearm and sets the prosthesis in 30° of retroversion. Figure 20. Note the etchings on the side of the Fracture Body to replicate humeral height from the trial reduction. Remove any excessive cement from around the fracture body and suture holes. Allow the cement to dry before proceeding. Press-fit Stem Attach the Fracture Implant Inserter/Extractor to the final prosthesis. Attach the Version Rod to Inserter/Extractor to ensure proper version and use light taps with a mallet to seat the implant. The Version Rod is aligned parallel with the patient’s forearm and initially sets the prosthesis in 30° of retroversion. FIGURE 20. Note the etchings on the side of fracture body; they should replicate humeral height from the trial reduction. 19 20 8 Step 9 • Prosthesis Assembly and Implantation (continued) 21 Humeral Head Re-trialing of the humeral head is now possible but not required. Once humeral head is selected, place it on the trunion of the stem. Impact the implant using the Head Impactor with a few strikes from a mallet, Figure 21. Step 10 • Bone Grafting and Tuberosity Repair Impact in the direction of the trunion axis Utilizing the bone graft removed earlier from the humeral head, graft the area around the humeral shaft and Fracture Body. Figure 22. 22 Place two heavy non-absorbable sutures through each of the holes on the medial side of the prosthesis. Figure 23. Place the arm in neutral position and reduce the greater tuberosity to its anatomical position. Take one of the sutures in the superior hole and wrap it around the greater tuberosity superiorly and secure it down. Figure 24. Repeat using one of the inferior sutures to wrap around inferiorly and secure the greater tuberosity. Figure 25. Take the remaining two sutures and place one superiorly and one inferiorly into the subsacpularis near the insertion into the lesser tuberosity. The opposite ends of the sutures will wrap around the implant and greater tuberosity which will allow the sutures to reduce and secure the lesser tuberosity. Figure 26. Use the sutures in the humeral shaft to tension the tuberosities. Place one suture anteriorly from the subscapularis to the supraspinatus, and the second suture posteriorly from the supraspinatus to the infraspinatus, to secure tuberosities to the humeral shaft. Figure 27. 23 The biceps tendon can now be relocated into the bicipital groove and a biceps tenodeses performed using a modified Kessler stitch into the supraspinatus. Note The above tuberosity repair technique is modeled after Dr. Pascal Boileau’s published cerclage technique.* 24 Step 11 • Closure Thoroughly irrigate the wound with antibiotic solution. If a regional anesthetic is not used then infiltrate the soft tissue with a local anesthetic that will last six to eight hours. A wound drainage system is recommended to prevent formations of postoperative hematoma. The wound may be closed according to surgeon preference. *Boileau P, Walch G, Krishnan S. Tuberosity Osteosynthesis and Hemiarthroplasty for Four-Part Fractures of the Proximal Humerus. Techniques in Shoulder and Elbow Surgery 2000; 1(2): 96-109. 9 25 Step 11 • Closure (continued) 26 Careful attention to wound closure will result in a cosmetically acceptable incision. After the dressing and shoulder immobilizer are in place, the use of a cold wrap is recommended. The combination of regional anesthetic or local anesthetic and the immediate cooling seems to decrease the amount of postoperative pain. Revision Procedure Removal of the humeral head and/or proximal humeral body during revision surgery can be achieved without disturbing a well-fixed distal stem. Removing the Humeral Head The Humeral Head can be removed using the Head Extractor. Place the two prongs of the Extractor between the Humeral Head and the osteotomy surface so that the prongs will advance in each side of the linking component, Figure 28. Lift the head off the proximal humeral body taper by impacting the end of the Extractor with the Slotted Mallet. Removing the Proximal Humeral Body The proximal humeral body can be removed using the Body Separator. Disengage the locking screw and remove using the 1/8 Hexdriver and Driver Handle. Thread the Body Separator into proximal humeral body. The pre-designed gap between the tines of the Body Separator will disengage the morse taper between the Humeral Body and the Humeral Stem without disruption to a well-fixed Humeral Stem. Remove the Humeral Body that is threaded to the Body Separator. Figure 29. 27 28 Long Stem Option The surgical technique for implanting a Titan Long Stem differs slightly from the standard length stems. Attach the T-Handle to the Starter Awl and create a 6mm pilot hole the humerus. Continue progressively reaming using cylindrical reamers of increasing diameter to 8, 10, or 12mm in either the 125mm or 165mm stem length options. The canal is reamed until cortical chatter is present and inserted to the depth of the laser mark associated with the desired height of humeral body. It is important to prepare the medullary canal over its total length. The final reamer used will correlate to the proper trial stem selected. The reamer, trial, and implant are line to line; minimizing cement to the stem flutes and within the surrounding trabecular bone. If a greater cement mantle is desired, choose an long stem implant diameter smaller than the reamer and trial stem diameter used for preparation. 29 The Body Trials from the Total Shoulder System Humeral Tray 1 Base can be used with the Trial Cemented Stems to determine proper prosthesis height. The Definitive Stem Primary Body Trials can be used with the definitive long stem implants once cemented in place to reassess desired humeral head height. Notes The long stems are for cemented use only. The long reamers are a special order item and do not come with the standard TSS and RSS instrumentation set. 10 Essential Product Information Indications For Use Total Shoulder Arthroplasty or Hemiarthroplasty is indicated for: • Severely painful and/or disabled joint resulting from osteoarthritis, traumatic arthritis or rheumatoid arthritis. • Fracture-dislocations of the proximal humerus where the articular surface is severely comminuted, separated from its blood supply or where the surgeon’s experience indicates that alternative methods of treatment are unsatisfactory. • Other difficult clinical problems where shoulder arthrodesis or resection arthroplasty are not acceptable (e.g. – revision of a failed primary component). Shoulder Hemiarthroplasty is also indicated for: • Ununited humeral head fractures. • Avascular necrosis of the humeral head. • Rotator cuff arthropathy. • Deformity and/or limited motion. The humeral component is intended for cemented or un-cemented use. The glenoid component is intended for cemented use only. Contraindications The following conditions are contraindications for total shoulder arthroplasty and hemiarthroplasty: • Active local or systemic infection. • Inadequate bone stock in the proximal humerus or glenoid fossa for supporting the components. • Poor bone quality, such as osteoporosis, where there could be considerable migration of the prosthesis and/or a chance of fracture of the humerus or glenoid. • Absent, irreparable or nonfunctional rotator cuff or other essential muscles. • Pregnancy. • Muscular, neurologic, or vascular deficiencies that compromise the affected extremity. • Known metal allergies. 11 Warnings The use of a glenoid prosthesis in patients with cuff tear arthropathy could increase the risk of glenoid component loosening due to non-anatomic loading conditions. The following conditions tend to adversely affect shoulder replacement implants; • Excessive patient weight • High levels of patient activity • Likelihood of falls • Poor bone stock • Metabolic disorders • Disabilities of other joints Precautions • Do not reuse this device. Reuse of this product may result in infection or other systemic complication that may affect the patient’s overall health. Additionally, the reuse of this product could adversely affect function of the device. Any implant that has been damaged, mishandled, or removed from the sterile field may have surface damage that could result in implant fracture and/or particulate and should be discarded. • The MR environment presents risks to patients with metal implants. Review of the available literature documents that metal implants may heat resulting in tissue damage and may migrate out of position. They may also cause artifact affecting image quality. Physicians should take these risks into consideration when recommending MRI imaging for patients with metal implants. Note: The Titan Reverse Shoulder System and Titan Total Shoulder System have not been evaluated for safety and compatibility in the MR environment. Neither the Titan Reverse Shoulder System nor the Titan Total Shoulder System has been tested for heating or migration in the MR environment. Sterility This implant has been sterilized by gamma radiation and is sterile in the unopened, undamaged package. If either the implant or the package appears damaged or has been opened, or if sterility is questioned for any reason, the implant should not be used. Do not resterilize this product. Adverse Events • Potential adverse events include early or late postoperative infection, allergic reaction, intraoperative or postoperative bone fracture and/or postoperative pain. • Intraoperative bone perforation or fracture may occur, particularly in the presence of poor bone stock caused by osteoporosis, bone defects from previous surgery, bone resorption, or while inserting the device. • Loosening or migration of the implants can occur due to loss of fixation, trauma, malalignment, bone resorption, and/or excessive activity. • Surgical intervention may be required to treat adverse effects. • MDR Reporting Reminder: Medical device manufacturers and users are required by law and regulation to report serious injuries and death. Product Information Disclosure Integra has exercised reasonable care in the selection of materials and the manufacture of these products. Integra excludes all warranties, whether expressed or implied, including but not limited to, any implied warranties of merchant ability or fitness for a particular purpose. Integra shall not be liable for any incidental or consequential loss, damage, or expense, directly or indirectly arising from use of this product. Integra neither assumes nor authorizes any person to assume for it any other or additional liability or responsibility in connection with these products. Surgical Procedure A Surgical Technique brochure is available which outlines the basic procedure for device implantation and use of the specialized surgical instrumentation. It is the responsibility of the surgeon to be familiar with the procedure before use of these products. Each surgeon must evaluate the appropriateness of the surgical technique used based on personal medical training and experience. Meticulous preparation of the implant site and selection of the proper size implant increase the potential for successful reconstruction. A complete set of instruments for each type of implant is available to aid bone preparation and reduce the operative time. It is suggested that the proper size implant be removed from its sterile package only after the implant site has been prepared and properly sized. Training Surgeons may obtain training from a qualified instructor prior to implanting the Titan Total Shoulder System to ensure thorough understanding of the implantation techniques and the instrumentation. 12 Instrumentation CEMENTED LONG STEM BASE 2 3 1 1 Reamers 2 Slap Hammer 3 Adapters 13 Catalog No. Description RMR-0950-025-08125 RMR-0950-025-10125 RMR-0950-025-12125 RMR-0950-025-08165 RMR-0950-025-10165 RMR-0950-025-12165 ADA-0950-040-501 ADA-0950-040-502 SLP-1002-519 Reamer Cemented Long Stem, 8mm x 125mm Reamer Cemented Long Stem, 10mm x 125mm Reamer Cemented Long Stem, 12mm x 125mm Reamer Cemented Long Stem, 8mm x 165mm Reamer Cemented Long Stem, 10mm x 165mm Reamer Cemented Long Stem, 12mm x 165mm Trial Adaptor Stem Adaptor Slap Adaptor QTY 1 1 1 1 1 1 1 1 1 CEMENTED LONG STEM INSERT 2 1 This area to remain empty during sterilization 1 Trial Cemented Long Stems 2 Definitive Stem Primary Body Trials Catalog No. Description TRL-0950-025-08125 TRL-0950-025-10125 TRL-0950-025-12125 TRL-0950-025-18165 TRL-0950-025-10165 TRL-0950-025-12165 TRL-0920-120-08STD TRL-0920-120-10SML TRL-0920-120-10STD TRL-0920-120-10LRG TRL-0920-120-12STD TRL-0920-120-14SML TRL-0920-120-14STD TRL-0920-120-14LRG TRL-0950-120-08SML TRL-0950-120-08STD TRL-0950-120-08LRG Trial Cemented Long Stem, 8mm x 125mm Trial Cemented Long Stem, 10mm x 125mm Trial Cemented Long Stem, 12mm x 125mm Trial Cemented Long Stem, 8mm x 165mm Trial Cemented Long Stem, 10mm x 165mm Trial Cemented Long Stem, 12mm x 165mm Definitive Stem Primary Body Trial - 08 Std Definitive Stem Primary Body Trial - 10 Sml Definitive Stem Primary Body Trial - 10 Std Definitive Stem Primary Body Trial - 10 Lrg Definitive Stem Primary Body Trial - 12 Std Definitive Stem Primary Body Trial - 14 Sml Definitive Stem Primary Body Trial - 14 Std Definitive Stem Primary Body Trial - 14 Lrg Definitive Stem Primary Body Trial - 08 Sml Definitive Stem Primary Body Trial - 08 Std Definitive Stem Primary Body Trial - 08 Lrg QTY 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 14 Instrumentation HUMERAL TRAY 1: INSERT 2 1 4 3 5 6 7 8 This area to remain empty during sterilization 9 15 1 Head Resection Guide 5 Pin Puller 2 Starter Awl 6 Fixation Pins 3 T-Handle 7 Cutting Templates & Handle 4 Version Rods 8 Cutting Depth Gauge Catalog No. Description SET189-A001 AWL-0920-042-001 G108352_B SET189-D007 3020 PIN-0920-051-001 TMP-0920-040-001R TMP-0920-040-001L ROD-0920-040-002 GAU-0920-058-001 HSG-0920-041-001 HSG-0920-041-002 Head Cutting Guide Starter Awl T-Handle w/Lg AO Version Rod Pin Puller Fixation Pin Head Cutting Template, Right Head Cutting Template, Left Head Cutting Template, Handle Head Cutting Depth Gauge Head Sizing Gauge, 38-46 Head Sizing Gauge, 48-52 QTY 1 1 1 2 1 3 1 1 1 1 1 1 9 Head Sizing Gauge HUMERAL TRAY 1: BASE 2 1 6 7 9 8 1 Stem Trial Handles 5 Calcar Planers 2 Fracture Trial Inserter/Extractor 6 Taper Adapters 3 Body Trials & Body Screws 7 Cutting Templates & Handle 4 Stem Trials 8 Taper Adapter Handle Catalog No. Description HDL-0920-043-001 INS-0950-046-001 TRL-0920-020-08STD TRL-0920-020-10SML TRL-0920-020-10STD TRL-0920-020-10LRG TRL-0920-020-12STD TRL-0920-020-14SML TRL-0920-020-14STD TRL-0920-020-14LRG TRL-0950-020-08SML TRL-0950-020-08STD TRL-0950-020-08LRG BSW-0920-021-01 TRL-0920-025-06 TRL-0920-025-07 TRL-0920-025-08 TRL-0920-025-09 TRL-0920-025-10 TRL-0920-025-11 TRL-0920-025-12 TRL-0920-025-13 Stem Trial Handle Fracture Trial Inserter/Extractor Body Trial, 8 Standard Body Trial, 10 Small Body Trial, 10 Standard Body Trial, 10 Large Body Trial, 12 Standard Body Trial, 14 Small Body Trial, 14 Standard Body Trial, 14 Large Fracture Body Trial, 8 Small Fracture Body Trial, 8 Standard Fracture Body Trial, 8 Large Body Screws Humeral Stem Trial, 6mm Humeral Stem Trial, 7mm Humeral Stem Trial, 8mm Humeral Stem Trial, 9mm Humeral Stem Trial, 10mm Humeral Stem Trial, 11mm Humeral Stem Trial, 12mm Humeral Stem Trial, 13mm 3 4 5 QTY 3 1 1 1 1 1 1 1 1 1 1 1 1 2 1 1 1 1 1 1 1 1 9 Humeral Trial Inserter/Extractor Catalog No. Description TRL-0920-025-14 TRL-0920-025-15 TRL-0920-025-16 INS-0920-046-001 RMR-0920-050-001 RMR-0920-050-002 ADT-0920-065-001 TMP-0920-040-001R TMP-0920-040-001L ROD-0920-040-002 SCR-0920-066-001 INS-0950-045-001 Humeral Stem Trial, 14mm Humeral Stem Trial, 15mm Humeral Stem Trial, 16mm Humeral Trial Inserter/Extractor Calcar Planer, Small Calcar Planer, Large Taper Adapter Head Cutting Template, Right Head Cutting Template, Left Head Cutting Template, Handle Taper Adapter Shaft Fracture Implant Inserter/Extractor QTY 1 1 1 1 1 1 4 1 1 1 1 1 16 Instrumentation HUMERAL TRAY 2: INSERT 4 1 2 3 5 17 1 Ratcheting Screw Driver Handle 2 Eccentric Head Trial Hex Driver 3 Osteotomy Sizing Discs 4 Eccentric Head Trials Catalog No. Description G107992_B SCR-0920-060-001 HSP-0920-070-001E HSP-0920-070-002E HSP-0920-070-003 HSP-0920-070-004 HSP-0920-070-005 HSP-0920-070-006 HSP-0920-070-007 HSP-0920-070-008 TRL-0920-010-3814E TRL-0920-010-4025E TRL-0920-010-4216E TRL-0920-010-4416E TRL-0920-010-4419E TRL-0920-010-4614E TRL-0920-010-4617E TRL-0920-010-4620E TRL-0920-010-4815E TRL-0920-010-4818E TRL-0920-010-4821E TRL-0920-010-5019E Driver Handle w/Sm AO 1/8 Hexdriver Head Sizing Plate, 38mm Head Sizing Plate, 40mm Head Sizing Plate, 42mm Head Sizing Plate, 44mm Head Sizing Plate, 46mm Head Sizing Plate, 48mm Head Sizing Plate, 50mm Head Sizing Plate, 52mm Head Trial, Eccentric, 38x14mm Head Trial, Eccentric, 40x15 mm Head Trial, Eccentric, 42x16mm Head Trial, Eccentric, 44x16mm Head Trial, Eccentric, 44x19mm Head Trial, Eccentric, 46x14mm Head Trial, Eccentric, 46x17mm Head Trial, Eccentric, 46x20mm Head Trial, Eccentric, 48x15mm Head Trial, Eccentric, 48x18mm Head Trial, Eccentric, 48x21mm Head Trial, Eccentric, 50x19mm 5 Concentric Head Trials QTY 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 Catalog No. Description TRL-0920-010-5022E TRL-0920-010-5220E TRL-0920-010-4216C TRL-0920-010-4416C TRL-0920-010-4419C TRL-0920-010-4614C TRL-0920-010-4617C TRL-0920-010-4620C TRL-0920-010-4815C TRL-0920-010-4818C TRL-0920-010-4821C TRL-0920-010-5019C TRL-0920-010-5022C TRL-0920-010-5220C Head Trial, Eccentric, 50x22mm Head Trial, Eccentric, 52x20mm Head Trial, Concentric, 42x16mm Head Trial, Concentric, 44x16mm Head Trial, Concentric, 44x19mm Head Trial, Concentric, 46x14mm Head Trial, Concentric, 46x17mm Head Trial, Concentric, 46x20mm Head Trial, Concentric, 48x15mm Head Trial, Concentric, 48x18mm Head Trial, Concentric, 48x21mm Head Trial, Concentric, 50x19mm Head Trial, Concentric, 50x22mm Head Trial, Concentric, 52x20mm QTY 1 1 1 1 1 1 1 1 1 1 1 1 1 1 HUMERAL TRAY 2: BASE 2 1 3 5 4 6 7 8 9 11 10 1 Head Impactor 5 Head Impaction Stand 9 2 Body Screw Hex Driver 6 Body/Stem Separator 10 Body/Stem Impaction Handle 3 Torque Limiter 7 Final Implant Inserter/Extractor 11 Slotted Mallet 4 Head Extractor 8 Head Impaction Stand Adapters Catalog No. Description IMP-0920-079-501 SCR-0920-060-002 G207153 SET188-A001 STD-0920-071-001 SEP-0920-068-001 INS-0920-045-001 INS-0920-071-SML INS-0920-071-STD INS-0920-071-LRG SIS-0920-054-001 IMP-0920-055-001 G107991_B Head Impactor 3/32 Hexdriver Torque Limiter Head Extractor Head Impaction Stand, Base Assembly Body Separator Humeral Implant Inserter/Extractor Head Impaction Stand Insert, Small Head Impaction Stand Insert, Standard Head Impaction Stand Insert, Large Stem Impaction Stand Stem Impactor Slotted Mallet Body/Stem Impaction Stand QTY 1 1 1 1 1 1 1 1 1 1 1 1 1 18 Catalog Numbers And Implant Dimensions Press-Fit Stem Dimensions (mm), Ti Diameter A Diameter B Humeral Head Dimensions (mm), CoCr Diameter C Height Cemented Stem Dimensions (mm), CoCr Width A B C Spherical Diameter Ø Length PRESS-FIT STEM CATALOG NO. LENGTH DIAMETER A DIAMETER B DIAMETER C SPLINE DEPTH NO. OF SPLINES HUMERAL HEAD CATALOG NO. HEIGHT WIDTH SPHERICAL DIAMETER Ø OFFSET (ECCENTRIC)CONCENTRIC STEM-0920-025-06 90.4 11.6 6.8 4.61 12 MHH-0920-010-3814X 14 38 41 2.5 No Option STEM-0920-025-07 90.412.4 7.6 5.3 1 12 MHH-0920-010-4015X 15 40 43 2.5 No Option STEM-0920-025-08 90.413.7 9.0 6.61 12 MHH-0920-010-4216X 1642 45 4 C STEM-0920-025-09 90.414.4 9.9 7.41 12 MHH-0920-010-4416X 1644 48 4 C STEM-0920-025-10 90.415.410.9 8.51 12 MHH-0920-010-4419X 1944 45 4 C STEM-0920-025-11 90.416.5 12.1 9.51 12 MHH-0920-010-4614X 1446 54 4 C STEM-0920-025-12 90.4 17.5 13.210.61 12 MHH-0920-010-4617X 1746 49 4 C STEM-0920-025-13 90.418.5 14.2 11.61 12 MHH-0920-010-4620X 2046 4 C 47 STEM-0920-025-14 90.419.5 15.3 12.61 12 MHH-0920-010-4815X 1548 56 4 C STEM-0920-025-15 90.420.5 16.4 13.5 1 12 MHH-0920-010-4818X 1848 51 4 C STEM-0920-025-16 90.421.5 17.4 14.7 1 12 CEMENTED STEM CATALOG NO. LENGTH DIAMETER A DIAMETER B DIAMETER C NO. OF FLUTES STEM-0950-025-06 90.4 9.6 6.1 4.64 STEM-0950-025-08 90.411.6 8.1 6.74 STEM-0950-025-10 90.413.4 9.9 8.54 STEM-0950-025-12 90.415.4 11.9 10.64 STEM-0950-025-14 90.4 17.5 14.0 12.64 CEMENTED LONG STEM CATALOG NO. LENGTH DIAMETER A DIAMETER B DIAMETER C NO. OF FLUTES MHH-0920-010-4821X 2148 49 4 C MHH-0920-010-5019X 1950 53 4 C MHH-0920-010-5022X 2250 51 4 C MHH-0920-010-5220X 2052 55 4 C Fracture Body Dimensions (mm), Ti Trunnion Offset Max Length STEM-0950-025-08125 125 11.5 8.0 6.04 Height STEM-0950-025-08165 165 11.5 8.0 6.04 STEM-0950-025-10125 125 13.5 10.0 8.0 4 STEM-0950-025-10165 165 13.5 10.0 8.04 STEM-0950-025-12125 125 15.5 12.0 10.04 Max Width STEM-0950-025-12165 165 15.5 12.0 10.04 Base Diameter FRACTURE BODY CATALOG NUMBER HEIGHT MAX LENGTH MAX WIDTH BASE DIAMETER TRUNNION OFFSET BOD-0950-020-08SML 30 16.711.611.6 8 BOD-0950-020-08STD 35 16.911.611.6 8 BOD-0950-020-08LRG 40 17.111.611.6 8 BSW-0920-021-01 19 Body Screw 20 Integra® Titan Total Shoulder System ™ For more information or to place an order, please contact: United States, Canada, Asia, Pacific, Latin America USA 877-444-1122 866-800-7742 fax Outside USA 609-936-5400 609-750-4259 fax integralife.com 0086 n n Europe, Middle-East, Africa International: +33 (0)4 37 47 59 50 +33 (0)4 37 47 59 25 fax Benelux: +32 (0)2 257 4130 +32 (0)2 253 2466 fax France: +33 (0)4 37 47 59 10 +33 (0)4 37 47 59 29 fax Switzerland: +41 (0)22 721 23 00 +41 (0)22 721 23 99 fax United Kingdom: +44 (0)1 264 345 781 +44 (0)1 264 363 782 fax integralife.eu n n n EC REP Ascension Orthopedics, Ltd. BioPark Broadwater Road Welwyn Garden City Herts. AL7 3AX United Kingdom n n Manufacturer: Ascension Orthopedics, Inc. 8700 Cameron Road Austin, Texas 78754 Availability of these products might vary from a given country or region to another, as a result of specific local regulatory approval or clearance requirements for sale in such country or region. Always refer to the appropriate instructions for use for complete clinical instructions. Non contractual document. The manufacturer reserves the right, without prior notice, to modify the products in order to improve their quality. Warning: Applicable laws restrict these products to sale by or on the order of a physician. n n n Additional information for EMEA Customers only: Products mentioned in this document are CE class I, IIa, IIb or III devices. Contact Integra should you need any additional information on devices classification. All the medical devices mentioned on this document are CE marked according to European council directive 93/42/EEC on medical devices and its relatives, unless specifically identified as “NOT CE MARKED”. Integra and the Integra logo are registered trademarks of Integra LifeSciences Corporation or its subsidiaries in the United States and/or other countries. Titan is a trademark of Integra LifeSciences Corporation or its subsidiaries. ©2014 Integra LifeSciences Corporation. All rights reserved. Printed in USA. 0278440-1-EN LC-0927-002 Rev C





© Copyright 2026