
Document 136227
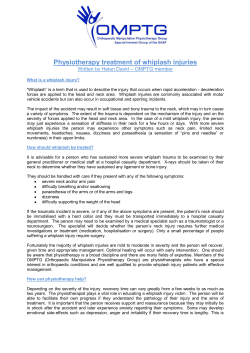
Journal of Orthopaedic & Sports Physical Therapy 2000;30(12):755-766 Cervicogenic Dizziness: A Review of Diagnosis and Treatment Diane M. Wrisley, MS, P7; NCS1 htrick J. Sparto, PhD, PT2 Susan I. Whitney, PhD, P7; ATC3 Joseph M. Furman, MD, PhD2 The diagnosis of cervicogenic dizziness is characterized by dizziness and dysequilibrium that is associated with neck pain in patients with cervical pathology. The diagnosis and treatment of an individual presenting with cervical spine dysfunction and associated dizziness complaints can be a challenging experience to orthopaedic and vestibular rehabilitationspecialists. The purpose of this article is to review the incidence and prevalence, historical background, and proposed pathophysiology underlying cervicogenic dizziness. In addition, we have outlined the diagnostic criteria, evaluation, and treatment of dizziness attributed to disorders of the cervical spine. The diagnosis of cervicogenic dizziness is dependent upon correlating symptoms of imbalance and dizziness with neck pain and excluding other vestibular disorders based on history, examination, and vestibular function tests. When diagnosed correctly, cervicogenic dizziness can be successfully treated using a combination of manual therapy and vestibular rehabilitation. We present 2 cases, of patients diagnosed with cervicogenic dizziness, as an illustration of the clinical decisionmaking process in regard to this diagnosis. ) Orthop Sports Phys Ther 2000;30:755-766. therapists must learn how to elicit a thorough history that will provide the information necessary to make decisions about treating the patient o r referring the patient to another health care practitioner. We borrow the definition of cervicogenic dizziness from Furman and Cassw: "a nonspecific sensation of altered orientation in space and dysequilibrium originating from abnormal afferent activity from the neck." Cervicogenic dizziness does not result from vestibular dysfunction and, therefore, Key Words: cervical vertigo, dysequilibrium, whiplash rarely results in true vertigo.'O Cervicogenic dizziness is most often associated with flexion-extension injuries and has been reported in he diagnosis and treatment of an individual presenting patients with severe cervical arthriwith cervical spine dysfunction and associated complaints tis, herniated cervical disks, and of dizziness can be a challenging experience to orthopaedhead tra~ma."J."~ In these paic and vestibular rehabilitation specialists. The differential tients, complaints of ataxia, undiagnosis may include cervicogenic dizziness, benign paroxsteadiness of gait, or postural imysmal positional vertigo, perilyrnphatic fistula, labyrinthine concussion, balance associated with neck pain, migraine-related vertigo, and central or peripheral vestibular dysfunclimited neck range of motion, or tion. The decision to treat the patient o r refer to another healthcare headache p r e d ~ m i n a t e . ' This ~ . ~ professional is essential to providing appropriate and timely care. Given article will focus on the incidence the potential seriousness of some of the causes of dizziness, physical and prevalence, historical background, and proposed pathophysiI Department of Physical Therapy, School of Health and Rehabilitation Sciences, University of Pittsology underlying cervicogenic dizburgh, Pittsburgh, Pd. ziness. In addition, we will address Department of Otolaryngology, School of Medicine, Department of Physical Therapy, School of Health and Rehabilitation Sciences, University of Pittsburgh, Pittsburgh, Pd. the diagnostic criteria, evaluation, I Department of Otolaryngology, School of Medicine, Department of Physical Therapy, School of and treatment of dizziness attribHealth and Rehabilitation Sciences, University of Pittsburgh, Pittsburgh, Pd; Center for Rehab Seruted to disorders of the cervical vices, Vestibular Rehabilitation Center, Pittsburgh, Pd. Send correspondence to: Pdtrick 1. Sparto, University of Pittsburgh, Department of Physical Therapy, spine. When diagnosed and treat6035 Forbes Tower, Pittsburgh, PA 15260. E-mail: [email protected] ed properly, the symptoms of cer- vicogenic dizziness can be reduced, resulting in improved function."" INCIDENCE AND PREVALENCE The concurrence of dizziness complaints and cervical spine dysfunction is commonly associated with flexionextension injuries (whiplash) acquired in a motor vehicle accident. It is estimated that every year 0.1% of the population experiences a whiplash inju~-y.~-@' Significant disability can result, with an estimated 20% of individuals who experience whiplash requiring greater than 20 weeks to return to work.@' Furthermore, a significant proportion of those who experience whiplash complain of neck pain months after the injury occurred? The primary symptom of whiplash is neck pain, which is reported by 62-100% of study participants in initial evaluations after the hipl lash.^^^^^^^^^^^^^ The next most common symptom is headache (primarily occipital in location), which occurs in 6 M 7 % of the study population^.^^.^^.^^^ Although dizziness, vertigo, and dysequilibrium d o not frequently occur at the initial presentation to the emergency department,".57 20-58% of individuals who have sustained a closed head or whiplash injury will experience these symp toms.58.64.71 Vestibular system disorders are included in the differential diagnosis of patients with dizziness associated with cervical spine dysfunction. For example, dizziness following neck injury may be due to vestibular system pathologies, brain injury, or cervicogenic dizz i n e s ~ . ~ Several ' . ~ . ~ groups have examined the occurrence of vestibular disorders following whip lash.21.24.4n..-.71 Table 1 provides operational definitions for frequently used terms regarding vestibular pathology that may be unfamiliar to the reader. Routine tests that are performed for the diagnosis of vestibular disorders are described in Table 2. Abnormalities have included deficits in smooth eye pursuit, normal or hypoactive caloric vestibular responses, spontaneous and positional nystagmus, and impaired postural ~ o n t r o l . ~ ~ ~ ~ . ~ ~ - ~ ~ Reports of dizziness with other types of neck dysfunction are certainly not as prevalent as with whip lash. However, several case reports have demonstrated dizziness in patients with cervical spine spondylosis and cervical muscle spasms. Ryan and CopeGSreported 3 cases of dizziness that they attributed to cervical spondylosis. The symptoms of 3 patients with dizziness and painful posterior cervical muscles reduced with an injection of anesthetic into the posterior neck m ~ s c l e s .Cervicogenic ~~.~ dizziness may be a result of whiplash injury, other forms of cervical spine dysfunction, o r spasms in the cervical muscles. 756 HISTORICAL BASIS AND PATHOPHYSIOLOGY OF CERVICOGENIC DIZZINESS Brown2" relates that the contribution of the cervical region to balance has been studied experimentally in animals for 150 years. Strong connections have been demonstrated between the cervical dorsal roots and the vestibular nuclei with the neck receptors (such as proprioceptors and joint receptors) playing a role in eye-hand coordination, perception of balance, and postural adjustments. Brownz0provides a comprehensive review of this literature. With strong connections between the cervical receptors and balance function, it is understandable that injury or pathology of the neck may be associated with a sense of dizziness or dysequilibri~m.~ Dizziness that is presumed to occur due to dysfunction in the cervical spine has been recognized since early in the 20th century. Symptoms of cervicogenic dizziness were thought to be due to abnormal input from cervical sympathetic nerves based on the work of Barrelo and Lieow% in the 1920's. They experimentally induced dizziness, tinnitus, and Horner's syndrome (constriction of the pupil, ptosis, ipsilateral loss of sweating) by injecting anesthetic into the upper cervical region. No sympathetic or vascular changes were subsequently identified that could account for these symptoms and this theory lost favor.m In the 1950's, there was a resurgence of interest in the idea that dizziness may be related to pathologies of the cervical r e g i ~ n Ryan . ~ and Cope" introduced the term "cervical vertigo" and although vertigo as defined in Table 1 is rarely a symptom, cervical vertigo has remained the most popular name for the focus of Ryan and Cope's paper. These authors theorized that cervicogenic dizziness was due to abnormal afferent input to the vestibular nucleus from damaged joint receptors in the upper cervical region. They described 3 types of patients that display this syndrome: patients with cervical spondylosis, patients treated with cervical traction, and patients following neck trauma. Graf4 found that he could relieve dizziness considered to be related to cervical muscle dysfunction by injecting anesthetic into the posterior cervical muscles. This finding supported Ryan and Cope's- theory that abnormal afferents from the cervical region caused dizziness and dysequilibrium. Others have experimentally produced a "reversible" lesion in the cervical region and observed deficits in balance and vision. CohenZJdescribed deficits in balance, orientation, and coordination in primates following injection of anesthetic in the upper 3 cervical dorsal roots. Biemond and de Jong15 reported that injection of anesthetic into the neck of rabbits induced positional nystagmus. Later, de Jong and colleaguesw found that injection of anesthetic around the dorsal roots of rabbits, cats, and primates J Orthop Sports Phys Ther-Volume 30-Number 129 December 2 0 0 TABLE 1. Definition of terms. Term Ataxia Dizziness Dysequilibrium Saccades Visual smooth pursuit Unsteadiness of gait Vertigo Labyrinthine concussion Mild brain injury Benign Paroxysmal Positional Vertigo (BPW) Perilymphatic fistula Whiplash Definition The inability to produce smooth, coordinated movements.12 A nonspecific term that describes an altered orientation in space. It may include sensations of light-headedness, heavy-headedness, faintness, giddiness, unsteadiness, imbalance, falling, waving, or fl~ating.~ The inability to maintain upright post~re.~ A rapid change in eye position, usually to shift gaze quickly from one object to an~ther.~'.~' The ability to maintain gaze on a moving object.75 Abnormal sway or gait pattern during amb~lation.~~ An illusory sensation of motion (rotational, translational, or tilting of the visual environment)of either self or surro~ndings.'~ A peripheral vestibular impairment caused by head trauma that usually is manifested by unilateral hearing loss and unilateral reduced peripheral vestibular function. Patients will typically complain of fluctuating vertigo and dysequilibrium.38 Injury to the brain characterized by brief loss of consciousness or coma less than 1 hour. A disorder caused by the presence of debris in the semicircular canal. Patients will typically complain of short episodes of vertigo when rolling over in bed, reaching up, or bending over. The Dix-Hallpike Maneuver is used to diagnose BPW. If present, the patient will present with nystagmus that begins 5-15 seconds after the patient is positioned and lasts for 30 seconds to 1 minute. Symptoms are usually worse in the morning and improve throughout the day." An abnormal connection between the middle and inner ear spaces. Patients typically present with symptoms of unilateral hearing loss, tinnitus, dizziness, dysequilibrium, and ~ertigo.'~ Injury to the cervical vertebrae or associated soft tissue caused by a sudden forward or backward acceleration of the vertebral co1umn.l TABLE 2. Common vestibular laboratory tests that may be performed on persons with cervicogenic dizziness. Vestibular test Description of the test Criteria for a normal result Oculomotor screening5J4 Patients are asked to sit in an otherwise darkened room, fixate on a target, and watch vertical lines move in front of them. The electronystagmography (ENG) electrodes that surround the eyes record eye movements. Abnormal responses may indicate central nervous system dysfunction. For horizontal canal testing, patients are placed in the supine position with their head flexed 30". Warm or cold air or water is placed in the ear canal alternately while the ENG electrodes record eye movements. This is the only test that can localize the side of the lesion in the ear. Patients are asked to lie supine with their head turned to the right and left and also to lie completely on their left and right sides. The eye movements are recorded in each position in darkness. Patients sit in a darkened room while they are moved slowly to the right and left in a rotating chair. Eye movements are recorded. This test assesses the vestibulo-ocular reflex. The accuracy and timing of the eye movements are compared with normative data. Caloric te~tirigsl~.~~ Positional testing5J4 Rotational testinpa P o ~ t u r o g r a p h y ~ ~ , ~ ~ ~ ~ ~ ~ ~ ~ ~ ~The patient stands on a forceplate during 6 increasingly complex visual and somato-sensory conditions (Sensory organization testing). The forceplate records the amount of sway that the patient experiences. Postural sway is also assessed during linear and angular perturbations of the platform. J Orthop Sports Phys Ther*Volurne 3O.Nurnber 12 December 2000 The symmetry and intensity of the eye movements are compared with normative data. Nystagmus is not normally seen in persons without vestibular dysfunction. The examiner determines the symmetry and intensity of the response from the recordings and compares it to normative data. Patient's scores are compared to age-related normative scores. 757 produced nystagmus and ataxia. In humans, injecting jects with whiplash-associated disorder or other cervianesthetic around the cervical dorsal roots caused dys- cal dysfunction has led some to consider using postuequilibrium, a strong sensation of imbalance and be- rography as a diagnostic t e ~ t . ~ . ~ . ~ ~ ~ ~ ~ ~ ~ " W o w e v e r , these tests cannot be performed in the clinic without ing pulled towards the side of the injection. Wap specialized equipment and have not been validated. neri4 discovered that the sensation of tilting or fallFurthermore, increased postural sway is a nonspecific ing could also be evoked by electrical stimulation to finding that is also evident in patients with vestibular the cervical muscles. Accordingly, the aberrant input injury.' from the cervical proprioceptors is considered to be The lack of a definitive diagnostic test increases related to muscle spasms in the sternocleidomastoid the challenge of diagnosing cervicogenic dizziness. and upper trapezius muscle^.^^.^.^.^^ Hence, this eviTherefore, the diagnosis of cervicogenic dizziness is dence leads to the current theory that cervicogenic dizziness results from abnormal input into the vestib- suggested by (1) a close temporal relationship beular nuclei from the proprioceptors of the upper cer- tween neck pain and symptoms of dizziness, including time of onset and occurrence of episodes, (2) vical region. Furthermore, the interconnections beprevious neck injury or pathology, and (3) eliminatween the cervical proprioceptors and the vestibular tion of other causes of dizziness.% It is important to nuclei may contribute to a cyclic att tern,^ such that take a detailed history and perform a comprehensive cervical muscle spasms contribute to dizziness and examination in order to eliminate other causes of dizziness contributes to muscle spasm, although the dizziness. The details of the history and physical excausal relationship is unclear. amination are discussed below. DIAGNOSTIC CRITERIA Cervicogenic dizziness is a diagnosis of exclusion (ie, the diagnosis is usually based on the elimination of the other competing diagnoses, such as vestibular or central nervous system pathologies). The develop ment of a robust clinical diagnostic test for cervicogenic dizziness has been elusive. The neck torsion nystagmus test, or head-fixed, body-turned maneuver is considered by some to identify cervicogenic dizziness." This test requires the head of the patient to be stabilized while the body is rotated underneath.!'"% Theoretically, the neck proprioceptors are stimulated while the inner ear structures remain at their resting ~ t a t eNystagmus .~ is elicited in a positive test. However, this test has not been demonstrated to be specific for cervicogenic dizziness. Oosterveld et alx' reported that 64% of 262 patients with neck pain who presented to an otolaryngology department post-whiplash had nystagmus elicited with the head-fixed, body-turned maneuver. On the other hand, it has been demonstrated that up to 50% of subjects without cervical spine pathology have also demonstrated nystagmus with the head-fixed, bodyturned m a n e ~ v e r . ~ ~ A, positive " ~ . ~ ~ response (nystagmus) may not indicate pathology, but may instead be a manifestation of the cervical ocular reflex.% Others have explored the use of vestibular and postural sway testing for the diagnosis of cervicogenic dizziness. Tjell and Rosenhallio examined smooth pursuit eye movements in patients with whiplash, acute vestibular pathology, or central nervous system dysfunction. Based on reduced velocity of eye movements during the tracking tasks when the subjects' heads were turned, the researchers were able to classify the individuals who had dizziness post-whiplash with a sensitivity of 90% and specificity of 91%. In addition, evidence of increased postural sway in s u b PHYSICAL THERAPY EVALUATION Patient History When a physician refers a patient to physical therapy, the referral may or may not provide a direction for the history taking. Certainly, a referral for "dizziness, evaluate and treat" by a primary care physician would not be as helpful as one for "cervicogenic dizziness, evaluate and treat" by an otolaryngologist or neurologist. Furthermore, one would expect a more thorough screening procedure for vestibular or central nervous system disorders by the physicians specializing in inner ear disorders. Since not all therapists have the benefit of receiving referrals from these specialists, this article assumes that the only information provided to the therapist is from the patient. Furthermore, because of the imprecise use of the terms dizziness and vertigo in the general community, we will approach the patient with no preconceived notions about the qualitative nature of the patient's symptoms. Obtaining a thorough history from a patient presenting with dizziness is critical to making a decision regarding the proper care of the patient. The first step is to ask the patient to describe their symptoms. Unfortunately, there are many words used to describe symptoms of dizziness and vertigo, and it is often difficult for a patient to provide specific descrip tions. Table 3 includes some typical ways that patients describe their symptoms. If a patient's descrip tion of their symptoms is consistent with vertigo, then a central or peripheral vestibular disorder is suspected. However, cervicogenic dizziness cannot be completely ruled out as a diagnosis. The duration and frequency of the symptoms, as well as their temporal relationship with the neck 1 Orthop Sports Phys Ther-Volume SO. Number 12. December 2000 TABLE 3. Common words used to describe symptoms of patients presenting with balance and vestibular disorders. Patient's words What the words suggest Dizziness Spinning Headache My neck hurts. People tell me that my head is not straight. I feel like I am going to fall. I can't walk straight. I am having trouble reading. I am tired. I feel like everything is moving when I am in a busy environment with motion and distractions. My vision is jumping. Swimming sensation in their head This is a nonspecific finding and could be either cewicogenic dizziness or a peripheral or central vestibular disorder. The patient could have a central or peripheral vestibular disorder, although spinning of short duration often suggests Benign Paroxysmal Positional Vertigo (BPPV) if there is no central nervous system dysfunction. Often patients complain of an occipital or bitemporal headache with cewicogenic dizziness. Tension headaches are more localized and are described as a ring around the head or in the frontal area. Migraines can be very severe, tend to be unilateral, and may cause sensitivity to light and motion. It is often seen in people with whiplash or labyrinthineconcussion disorders. This is more common in central vestibular disorders than peripheral disorders. This is often seen in ce~icogenicdizziness and also with head trauma. This is rarely seen in persons with peripheral vestibular disorders. This is common in both cewicogenic dizziness and in peripheral or central vestibular disorders. It is a nonspecific symptom. This could be seen in cewicogenic dizziness, with a peripheral vestibular disorder, or with central vestibular disorder. This is also a nonspecific symptom. It could be cewicogenic dizziness or a peripheral or central vestibular disorder. It might be helpful to test their eyes with a vision chart to see if there is any loss of acuity. If the problem exists only with head movement, it may suggest a vestibular abnormality. This is a very common complaint in persons with vestibular or balance disorders. This complaint of space and motion discomfort is common in persons with migraine, anxiety-panic, and in persons with peripheral vestibular disorders. The visual surroundings will jump with oscillopsia and it usually suggests a peripheral vestibular disorder of either 1 or both ears. Nonspecific but can suggest that there is central nervous system dysfunction. pain, can aid in the diagnosis of cervicogenic dizziness. The time (how long ago) and mode of onset (gradual, sudden, or associated with injury) should be determined. Symptoms resulting from cervicogenic dizziness typically are associated with injury or cervical spine disease, however, their onset may be sudden or gradual and occur days to years following the injury. Next, if the dizziness is episodic, the number of events per day or week and the duration of each event should be elicited by the therapist. Table 4 lists the frequency and duration expected for various causes of dizziness. Cervicogenic dizziness typically occurs in episodes lasting minutes to hours. Information regarding conditions that exacerbate or relieve the symptoms is also helpful. Symptoms resulting from cervicogenic dizziness will be increased with neck movements o r neck pain and decreased with in- terventions that relieve neck pain (modalities, analgesic, anti-inflammatory or muscle relaxant medication). Finally, the therapist should ask the patient for any history of balance difficulties and falls related to the symptoms. A similar type of history regarding neck pain should be obtained, including a specific description of symptoms, location, time and mode of onset, and aggravating factors. Dizziness related to active movement or changes in head position with or without neck pain may lead one to think that there is a cervical component. To entertain a diagnosis of cervicogenic dizziness, however, the therapist must be able to correlate the onset and duration of the dizziness symptoms with the neck dysfunction (ie, dizziness accompanied by neck pain or with head movements). In addition to the complaints about dizziness and TABLE 4. Duration and frequency . . of common causes of dizziness. Cause Common symptoms Frequency Duration Benign Paroxysmal Positional Vertigo4' Vertigo Episodic Seconds Cewicogenic d i z ~ i n e s s ~ ~ . ~ ~ Perilymphatic fistula16 Dizziness, dysequilibrium Dysequilibrium, vertigo Episodic Episodic Minutes to hours Seconds to minutes Labyrinthine concussion42 Central vestibular dysfuncti~n~~ Vertigo, dysequilibrium Dizziness, dysequilibrium Episodic More constant Hours to days Days to weeks J Orthop Sports Phys Ther.Volume SO. Number 12. December 2 0 0 Related factors Related to head position, usually worse in AM Related to head position Vertigo during Valsalva maneuver Increases with fatigue May be seen in combination with inner ear ~atholoeies 759 TABLE 5. The appropriate action to be taken by a physical therapist based on various additional symptoms in patients presenting with dizziness or vertigo. Unexplained or new onset of symptoms that may require immediate medical attention Constant vertigo Feeling of being pushed to one side Facial asymmetry Swallowing dysfunction Speech problems Oculomotor dysfunction (cranial nerves Ill, IV, VI) Rosis Vertical nystagmus Loss of consciousness Repeated, unexplained falls Changes in sensation Severe headache Upper motor neuron signs and symptoms Symptoms that require nonemergent referral to an otola~n~oloaist Constant dizziness Unilateral hearing loss New onset of tinnitus Aural fullness (stuffiness in ear) Ear pain Transient vertigo Symptoms that can be treated by a physical therapist Transient dizziness Cervical pain Limited cervical range of motion Radicular upper extremity symptoms Headache Balance complaints Jaw pain Visual sensitivity Nausealvomiting* Anxiety, fatigue* Although physical therapists may not provide direct intervention for these symptoms, reduction in dizziness may alleviate them. neck dysfunction, the therapist should be careful to ask further questions regarding other symptoms that may be perceived by the patient, as listed in Table 5. All the symptoms in the first column of Table 5 suggest a possible central nervous system pathology that may need immediate attention. It is always preferable to speak with the patient's primary care or referring physician before seeking emergent care. Symptoms listed in the second column of Table 5 (which are frequently reported after sustaining a whiplash injury) require a visit to an otolaryngologist because they are consistent with inner ear pathology. In our opinion, these symptoms d o not require urgent attention. Finally, the third column lists typical secondary symp toms that may be reported at the time of the initial evaluation. We believe that these symptoms are within the scope of physical therapist practice and thus may be addressed directly. If a patient experiences transient true vertigo, then a peripheral vestibular ailment or benign paroxysmal positional vertigo is more likely. The time course of the symptoms also may provide a clue to the pathology. Dizziness or vertigo due to perilymphatic fistula may have an onset 24-72 hours after head trauma and episodes may last minutes to hours.%." Nausea and vomiting are common signs of acute vestibular pathology. Benign paroxysmal positional vertigo may occur more than 2 weeks after head t r a ~ m a ;and ~ characteristically lasts less than a minute after a change in position.47 Cervicogenic dizziness may occur anywhere from days to months or longer after an injury of the head and neckFOwith a time course of minutes to hours per episode. Examination Once the history is complete, the therapist can proceed to rule in o r out the competing differential diagnoses. Note that the examination procedure presented here does not represent the complete exam a vestibular rehabilitation specialist would use for any patient presenting with nonspecific dizziness,'" nor does it represent the complete exam that an orthopaedic physical therapy specialist would use for a patient with nonspecific cervical dysf~nction.~%ther, it is an outline of a thorough - examination the authors would use to rule in or out a diagnosis of cervicogenic dizziness. The order in which the assessments are performed is at the discretion of the therapist, but an attempt was made to discuss the examination in a logical sequence. The flow chart (Figure) depicts the decision-making process that the physical therapist should go through to arrive at a diagnosis of cervicogenic dizziness or other pathology that may present similarly to cervicogenic dizziness. In the first step, the therapist determines if the patient with a chief complaint of dizziness or vertigo has neck pain, either at rest, with active neck movement, or with palpation of the neck musculature. This step is important because, by definition, a diagnosis of cervicogenic dizziness is excluded in a patient without neck pain.'" If the patient has dizziness with neck pain, a diagnosis of cervicogenic dizziness should be considered because cervicogenic dizziness might account for both the dizziness and the neck pain. However, there is a possibility that the patient may have neck pain as a secondary impairment due to a vestibular disorder or may have 2 s e p arate diagnoses, 1 to account for the dizziness and 1 to account for the neck pain. To help establish a diagnosis of cervicogenic dizziness, other vestibular disorders such as benign paroxysmal positional vertigo, Meniere's disease, labyrinthine concussion, and migraine-related vestibulopathy must be ruled out. Although the sensitivity and specificity of vestibular J Orthop Sports Phys Ther.Volume 30. Number 12. December 2000 / injury or patholog/ I no i PPV, vestibular disorder, andlor cewicogenic dini I I L-J Dix-Hallpike and refer to MD for no Vestibular disorder, andlor cewicogenic dizziness / ?-, 4 Canalith repositioning Maneuver normal results vestibular testing Vestibular disorder Co-treat (Case 1) FIGURE. Decision tree used for a ~atientwho Dresents with dizziness or vertigo and neck pain. BPW indicates benign paroxysmal positional vertigo; MD, medical doctor; VR-PT, vestibhar rehabilitition physical therapist. function tests are not very high,4.%14.17.X'-3'II~!l.40.7.9 the use of vestibular function tests in conjunction with history and clinical examination provides the clinician with a reasonable idea of the involvement of the vestibular system. In the early part of the examination, the therapist should measure the patient's active cervical range of motion, preferably while the patient is sitting. This is done for several reasons. The first is to simply measure any impairment in the range of motion. Second, the therapist should inquire about any symp toms of pain or dizziness elicited by the active movements. Changes in pain or dizziness can be quantified by comparing the patient's rating of these symptoms with the rating obtained before movement. Third, the active movement can be used to determine if the patient has adequate range of motion for subsequent tests that the therapist may perform, such as the Dix-Hallpike maneuver for benign paroxysmal positional vertigo (BPPV), which requires 30" of cervical extension and 45" of cervical rotation.:" J Orthop Sports Phys Ther.Volume 30-Numher 12eDecemher 2 0 With the patient sitting, the therapist may also perform vision tests and an upper quarter screening procedure (range of motion, manual muscle testing, accessory motion testing, sensation and reflex testing of the upper extremity and cervical region). The therapist may test for posterior semicircular canal BPPV using the Dix-Hallpike mane~ver.~-'"he therapist must make certain that the patient has adequate active range of motion, given that the cervical spine of the patient is placed in 45" of rotation and 30" of extension so that the posterior semicircular canal is stimulated in the vertical plane. The Dix-Hallpike maneuver is initiated by having the patient attain the long-sitting position while the therapist rotates the patient's head 45" to one side and brings the patient into supine quickly while extending the head 30". The patient is asked to report any symptoms while the therapist observes the patient's eyes for nystagmus. If the patient cannot tolerate a traditional Dix-Hallpike maneuver because of pain or decreased cervical range of motion, the position can be modi- ties, postural reeducation, active range of motion, fied by having the patient lie down to the side with massage, balance retraining, trigger point injection, the head turned so the back of the head is toward muscle relaxants, and use of a soft cervical collar the surface and the nose is pointing up. Tilt tables or mobilization tables can be used to put the patient during the acute phase.lfi.20.'2~26~27.M.44.5'.65.M~77 HOweVer, few controlled clinical trials have been performed in a position to stimulate the posterior semicircular to determine the effectiveness of these interventions. canal by having the patient rotate the head approxiThree clinical trials that propose intervention for mately 45' to the side and lowering the head of the cervicogenic dizziness are summarized in Table 6. bed into a trendelenberg position. A Dix-Hallpike These authors report that 7342% of patients receivmaneuver is said to be positive if the patient reports symptoms of spinning and rotational, upbeating nys- ing some form of manual therapy had a reduction in their symptom^.^"^'.^^ It is the authors' experience tagmus is observed with a latency of 5-15 seconds and a duration of 30 seconds to 1 minute. If the Dix- that patients may require both manual therapy and vestibular rehabilitation to achieve relief of both cerHallpike maneuver is positive, BPPV can be treated vical and vestibular symptoms. by performing a canalith repositioning maneuverw Two case reports will be used to illustrate the diagor by instructing the patient in Brandt-Daroff exercisnosis and treatment of suspected cervicogenic dizzies.'" A single treatment of the canalith repositioning maneuver has been reported to eliminate symptoms ness. One case report describes a patient who was in 72-78% of patients with BPPV, with complete ressuccessfully treated using a combination of both olution of 91% after 2 treatment^.^^.^^.^^.^^.^" However, manual therapy and vestibular rehabilitation (Case only one randomized controlled clinical trial has 1). The second case report describes a patient initialbeen performed." Brandt-Daroff exercises have been ly evaluated by an orthopaedic physical therapist and given cervical spine range of motion exercises and reported to result in a remission of symptoms in 98% of patients when performed over a 2-week perisubsequently treated with vestibular rehabilitation therapy alone (Case 2). od]" no randomized controlled clinic trial has been performed to confirm this. If the therapist is not skilled in these interventions, then referring the paCase 1 tient to a physical therapist o r physician specializing The first patient is a 49-year-old woman who prein balance disorders is appropriate. sented with complaints of dizziness, nausea, and dyseA negative Dix-Hallpike maneuver should lead to quilibrium 8 months after a motor vehicle accident. management of the neck impairments and referral She described fluctuating symptoms that occurred to a physician for vestibular testing. The diagnosis of cervicogenic dizziness is then made only after no ves- daily. The symptoms were exacerbated by head rnovements or with lying down and would last for hours. tibular abnormalities are found by the physician. She related that the symptoms were worse on days Considering either diagnosis, the therapist may dewhen the neck pain and headaches were worse. She cide to cotreat with, o r refer to, a vestibular rehabilidenied any tinnitus, aural fullness, or hearing loss. tation physical therapist. Vestibular function testing results including electronysPatients with cervicogenic dizziness may complain tagmography (ENG), calorics, positional testing and of poor balance. Balance disorders may be manifestrotational chair, provided by the physician, were nored by difficulties in standing with a narrow base of mal. support, walking with head turns, reaching outside On initial evaluation, she rated her neck pain as the base of support, turning and looking over one's 8-9/10 on a verbal analog scale with 0 meaning no shoulder, standing o r walking on compliant surfaces. decreased environmental lighting, and eye closure. A pain and 10 meaning the worst imaginable pain. Her cervical range of motion was not impaired; however, full balance assessment may include pen and paper any head or neck movements increased her symp tests such as the Activities-specific Balance Confitoms of dizziness. She presented with tenderness to dence scale?* as well as functional tests like the Dynamic Gait Indexm and the Berg Balance Test.13 The palpation and palpable trigger points (areas of increased pain) in her bilateral upper trapezius, scaleClinical Test for Sensory Interaction in Balance (CTSIB) is another popular test that is used to assess nes, and sternocleidomastoid muscles. She dernonstrated an inability to maintain focus on an object the patient's ability to use vestibular cues while conwhile turning her head (impaired functional use of flicting visual and proprioceptive cues are presentthe vestibular-ocular reflex) and complained of ined.'j7 creased nausea during activities that required head and eye movement. During static balance testing, she PHYSICAL THERAPY INTERVENTION was able to maintain stance with feet together for 6 Historically, the intervention for cervicogenic dizzi- seconds with her eyes open, but was unable to mainness has included manual therapy (mobilization and tain the position with her eyes closed. She was unable to maintain tandem stance (sharpened Romberg) manipulation), mechanical traction, physical modaliJ Orthop Sports Phys Ther .Volume SO. Number 12. December 2000 TABLE 6. Summary of articles that address outcome of treatment for cervicogenic dizziness. Study Subjects Wing and Hatgrave-Wilson, 1 974n 80 subjects with history of neck pain and vertigo, 46% with neck injury. Control group Type of study Neurodologic evaluation Intervention Frequency and duration None. Case series. 96% had normal ear, nose, and throat examination, 80% had normal electronystagmography examination including caloric and positional testing. Manipulation, immobilization in soft cervical collar, instruction in proper sleeping positions. Not specified. Karlberg et al, 199652 17 patients, mean age 37 years, with diagno- 50 patients with suspected cervisis of cervicogenic dizziness. Subjects rancogenic dizziness, 31 patients domized to receive immediate ~hvsical therapy or wait 2 months and i k a t e physical therapy. 17 healthy subjects. Prospective, randomized, clinical trial. Ear, nose, and throat and neurological exam excluded extra-cervical causes of dizziness. Soft tissue treatment, stabilization exercises of the trunk and cervical spine, passive and active range of motion exercises, relaxation techniques, home training programs, and minor ergonomic changes at work. 5-20 weeks with median number of visits = 13. Outcome measures Results Ear, nose, and throat with head flexed, extended or rotated with eyes open and closed; subjective report of symptom relief. 73% of patients demonstrated improvements in ear, nose, and throat with head and neck movements. 53% of patients reported complete relief of all symptoms. 36% had significant improvement and returned to normal activity without medication. Calm et al. 1998" Subjective intensity of neck pain; intensity and frequency of dizziness; variance of vibration and galvanic-induced body sway. There was no change in symptoms of neck pain or dizziness between the time when initially tested and just prior to beginning physical therapy, for the group that started treatment late. 82% of ~atientsre~orted improvement of dizzinks followi;lg physical therapy. 82% of patients reported improvement of neck symptoms. Postural performance significantly improved following phvsical theraw ( P < .05). or single limb stance without upper extremity s u p port. On the sensory organization test of computerized dynamic posturography, she demonstrated a pattern of multisensory dysfunction. Her composite score was 19/100 (normal for her age would be 70/ 100) with increased sway in conditions 1-3 and falls on all trials of conditions 4-43 (for additional information about posturography test conditions, refer to Furman"). She demonstrated ataxic gait with her eyes open and closed. The patient was given a diagnosis of cervicogenic dizziness based on the association between her symp toms of dizziness and neck pain, history of a flexionextension injury of the cervical region, and the exclusion of other peripheral vestibular pathology. She was initially seen weekly for physical therapy and treated with soft tissue massage, mobilization, and deep massage to her cervical musculature with emphasis on massaging the trigger points in the sternocleidomastoid muscle. She was instructed in a home exercise program of gentle range of motion exercises, followed by application of ice to be performed 24 times each day. In addition, she was provided a J Orthop Sports Phys Ther.Volume 30. Number 12. December 2 0 0 with cervical spine dysfunction (group A) and 19 patients without cervical spine dysfunction (group B). None. Case series. Ear, nose, and throat and neurological exam excluded extracervical causes of dizziness. Both groups treated with manual therapy. "Intensive outpatient physical therapy" for up to 3 months. Subjective improvement in dizziness. Group A: 77.4% reported improvement of symptoms of dizziness; 5 patients completely free of dizziness. Group B: 26.3% reported improvement of symptoms; none were completely free of symptoms. transcutaneous electrical nerve stimulation (TENS) unit and instructed in its use to provide pain relief and to decrease the spasms in the cervical muscles. She was also instructed to begin a progressive walking program and to perform simple balance activities such as standing with the eyes closed and standing feet together with small amounts of sway. At the end of 3 weeks, the patient reported that her pain level had decreased from 8-9/10 to 3/10 on a verbal analog scale more than 50% of time. She reported only a single episode of dizziness and nausea in the previous week. She demonstrated significant improvement in the static balance tests. She demonstrated no veering while walking with head turns or while walking with her eyes closed. Although she demonstrated significant improvements in pain control and balance, she continued to describe dizziness and nausea with head turns, standing or moving with her eyes closed, with movement in the environment or with conflicting visual cues (ie, walking in store aisles or in environments with busy patterns on the floor or walls). Due to these syrnp toms of dizziness and the finding of gaze instability at initial evaluation, it was decided to begin vestibular rehabilitation to decrease her reliance on visual and somatosensory cues and increase her use of vestibular cues for balance. The vestibular rehabilitation program consisted of eye exercises (VORxl and VORx2) to improve the efficacy of the vestibular-ocular reflex and balance exercises with graded exposure to varied sensory The patient was seen for 17 visits over a period of 5 months. At discharge, she reported that she was close to 100% of her premorbid function. She continued to complain of left occipital pain and mild dizziness with quick movements and visual conflict. She reported her pain level was less than 2/10 on a verbal analog scale 90% of the time. On evaluation, cervical range of motion and strength were not impaired and she was able to perform the static balance tests (Romberg, sharpened Romberg, and single limb stance) for at least 30 seconds with her eyes open and closed. Her computerized dynamic posturography score had also improved to within normal limits, with a composite score of 81/100 and normal amounts of sway on all 6 conditions of the sensory organization test. She was able to ambulate community distances (distances of 1-2 miles) without assistance and with no evidence of sway. Case 2 The patient is a 49-year-old female who experienced a motor vehicle accident that resulted in a flexionextension injury of the cervical region one year ago. She was referred to an outpatient orthopaedic clinic with a diagnosis of neck pain and dizziness. The patient's chief complaint was of dizziness and imbalance, which she related to changes in head position. She had only 25% of normal cervical flexion, extension, right side bending, and right rotation. She also had approximately 50% of normal range of motion for left side bending and left rotation. The orthopaedic therapist saw the patient for 1 visit and provided her with neck stretching exercises in an attempt to increase her range of motion and then referred her to vestibular rehabilitation. The patient stated that she previously had experienced an acute onset of vertigo but had not been vertiginous for several months. Her Activities-specific Balance Confidence scale (ABC) score was only 27%, indicating that the patient perceived that she was not confident with her balance (100% is the best score that can be achieved). The ABC is a tool used to assess confidence in 16 different activities of daily living and has been used with persons with vestibular dysf~nction.~" The patient's Dizziness Handicap Inv e n t o r y (DHI) score was 66. Scores range from zero to 100. A score of zero indicates no symptoms. The DHI measures perceived handicapping effects of dizziness. A score of 66, in our experience, reflects severe symptoms. The patient had normal strength, sensation, and deep tendon reflexes in all extremities. At baseline, the patient's dizziness symptoms were 50/100 based on a verbal analog scale (higher scores indicate greater perceived dizziness). She related a mild increase in symptoms during head movements with her eyes open and closed. Her dynamic posturography score was normal for the Sensory Organization Test. The patient's Dynamic Gait Index score was 20/24. A score of 24/24 would be considered normal for her age.m The therapist attempted to perform the DixHallpike maneuver in order to rule out BPPV, but the patient was unable to tolerate the position because of nausea. It was believed that the patient had symptoms consistent with cervicogenic dizziness based on her flexionextension injury, correlation of symptoms with head movements and neck pain and the exclusion of a peripheral vestibular diagnosis based on normal performance on vestibular function testing (electronystagmography, caloric, positional and rotational vestibular testing). Due to the patient's complaints of dizziness, dysequilibrium, and her lack of confidence in performing upright activities it was believed she would benefit from a rehabilitation program that would retrain her ability to use various balance strategies during functional activities. The patient was provided with a home exercise program that emphasized walking, standing and performing head movements, rolling to the right and left, and standing with eyes closed. She was seen for 2 additional visits, 2 weeks apart. During her fourth visit to physical therapy 2 months after her initial evaluation, her ABC score had increased to 70% and her DHI had decreased to 40/ 100. The patient was not complaining of any symp toms at baseline and the DGI increased to 23/24. However, she continued to have an increase in symp toms while shopping and in busy visual environments. She had no symptoms while working. The patient was satisfied with the outcome of her therapy and was discharged. CONCLUSION Cervicogenic dizziness is a diagnosis characterized by dizziness and dysequilibrium that is associated with neck pain in patients with cervical pathology. The current literature on this topic is limited with respect to the number and quality of the clinical uials reported. The diagnosis is dependent on correlating symptoms of imbalance and dizziness with neck pain and excluding other vestibular disorders on the basis of history, examination, and vestibular function tests. When diagnosed correctly, we believe that cervicogenic dizziness can be successfully treated using a J Orthop Sports Phys Ther-Volume SO. Number 12.December 2000 combination o f manual therapy and vestibular rehabilitation. Manual therapy is recommended treatment for cervicogenic dizziness directed at decreasing muscle spasms and trigger points o f pain in the cervical musculature. In the first case presented, although the patient's neck pain and balance appeared to improve with manual therapy, i t was n o t until she was also given vestibular rehabilitation exercises that the symptoms o f dizziness improved. In the second case, the patient improved with a home exercise program that addressed cervical range o f motion and balance. From o u r clinical experience, we recommend that cervicogenic dizziness be treated with manual therapy t o decrease the irritation o n the cervical proprioceptors f r o m muscle spasms and trigger points, and exercises with graded exposure t o sensory inputs to improve the patient's use o f vestibular and proprioceptive inputs for balance. In addition, we recommend eye exercises to improve the function o f the vestibular-ocular reflex. In order t o fully address all o f the patient's symptoms, i t may be necessary for the orthopaedic and vestibular specialists to treat the patient together. REFERENCES 1. Taber's Cyclopedic Medical Dictionary. Philadelphia, Pa: FA Davis; 1997. 2. Alund M, Larsson SE, Ledin T, Odkvist L, Moller C. Dynamic posturography in cervical vertigo. Acta Otolaryngo/ S~ppl.1991;481:601-602. 3. Alund M, Ledin T, Odkvist L, Larsson SE. Dynamic posturography among patients with common neck disorders. A study of 15 cases with suspected cervical vertigo. / Vesfib Res. 1993;3:383-389. 4. Assessment: posturography. Report of the therapeutics and technology assessment subcommittee of the American ~ c a d e m of y Neurology. Neurology. 1993;43:12611264. 5. Assessment: electronystagmography. Report of the therapeutics and technology assessment subcommittee of the American Academy of Neurology. Neurology. 1996;46: 1763-1 766. 6. Baloh RW. History 1: patient with dizziness. In: Baloh RW, Halmagyi GM, eds. Disorders of the Vestibular System. New York, NY: Oxford; 1996:157-170. 7. Baloh RW. Dizziness, Hearing Loss, and Tinnitus. Philadelphia, Pa: FA Davis; 1998. 8. Baloh RW, Sills AW, HonrubiaV. Impulsiveand sinusoidal rotatory testing: a comparison with results of caloric testing. Laryngoscope. 1979;89:646-654. 9. Barnsley L, Lord S, Bogduk N. Whiplash injury. Pain. 1994;58:283-307. 10. Barre ]A. Sur un syndrome sympathique cervcial posterieur et sa cause frequente: I'arthrite cervicale. Rev Neurol. 1926;45:1246-1253. 11. Barrett K, Buxton N, Redmond AD, JonesJM, Boughey A, Ward AB. A comparison of symptoms experienced following minor head injury and acute neck strain (whiplash injury). / Accid Emerg Med. 1995;12:173-176. 12. Benarroch EE, Westmoreland BF, Daube J, ReaganTJ, Sandok BA. Medical Neurosciences. Philadelphia, Pa: Lippincott Williams & Wilkins; 1999. J Orthop Sports Phrj Ther.Volume SO-Number 12mDecember 2000 13. Berg KO, Maki BE, Wiliams JI, Holliday PJ, Wood-Dauphinee SL. Clinical and laboratory measures of postural balance in an elderly population. Arch Phys Med Rehab. 1992;73:lO73-lO8O. 14. Bhansali SA, Honrubia V. Current status of electronystagmography testing. Otolaryngol Head Neck Surg. 1999; l20:419426. 15. Biemond A, de Jong JMBV. On cervical nystagmus and related disorders. Brain. 1969;92:417458. 16. Biesinger E. Vertigo caused by disorders of the cervical vertebral column: diagnosis and treatment. Adv Otorhinolaryngol. 1988;39:44-51. 17. Bowman CA, Mangham CA. Clinical use of moving platform posturography. Sem Hearing. 1989;10:161-169. 18. Brandt T. Somatosensory vertigo. In: Brandt T, ed. Vertigo: Its Multisensory Syndromes. London: Springer-Verlag; 1991:277-288. 19. Brandt T, Daroff RB. Physical therapy for benign paroxysmal positional vertigo. Arch Otolaryngol. 1980;106: 484-485. 20. Brown JJ. Cervical contributions to balance: cervical vertigo. In: Berthoz A, Vidal PP, Graf W, eds. The Head Neck Sensory Motor System. New York, NY: Oxford University Press; 1992 :644-647. 21. Chester JB. Whiplash, postural control, and the inner ear. Spine. 1991;16:716442. 22. Clendaniel RA. Cervical vertigo. In: Herdman SJ, ed. Vestibular Rehabilitation. Philadelphia, Pa: FA Davis; 2000: 494-594. 23. Cohen LA. Role of eye and neck proprioceptive mechanisms in body orientation and motor coordination. / Neurophysiology. 1961;24:1-11. 24. Compere WE. Electronystagmographic findings in patients with "whiplash" injuries. Laryngoscope. 1968;78:12261233. 25. Dal T, Ozluoglu LN, Ergin NT. The canalith repositioning maneuver in patients with benign positional vertigo. Eur Arch Otorhinolaryngol. 2000;257:133-136. 26. Davis D. A common type of veritog relieved by traction of the cervcial spine. Ann Intern Med. 1953;38:778. 27. de JongJMBV, Bles W. Cervical dizziness and ataxia. In: Bles W, and Brandt T, eds. Disorders of Posture and Gait. Amsterdam: Elsevier Science Publishers; 1986:185-206. 28. Deans GT, Magalliard JN, Kerr M. Neck sprain--a major cause of disability following car accidents. Injury. 1987; 18:lO-12. 29. deJong PTVM, de Jong JMBV, Cohen 6, Jongkees LBW. Ataxia and nystagmus induced by injection of local anesthetics in the neck. Ann Neurol. 1977;1:240-246. 30. Di Fabio RP. Sensitivity and specificity of platform posturography for identifying patients with vestibular dysfunction. Phys Ther. 1995;75:290-305. 31. Di Fabio RP. Meta-analysis of the sensitivity and specificity of platform posturography. Arch Otolaryngol Head Neck Surg. l996;l22:l5O-l56. 32. Di Fabio RP, Emasithi A, Paul S. Validity of visual stabilization conditions used with com~uterizeddvnamic ~ l a t form posturography. Acta ~tola'ryn~ol. 1998;118:449454. 33. Dix MR, Hallpike CS. The pathology, symptomatology, and diagnosis of certain common disorders of the vestibular system. Ann Otorhinolaryngol. 1952;6:987-1016. 34. Epley JM. The canalith repositioning procedure: for treatment of benign paroxysmal positional vertigo. Otolaryngo1 Head Neck Surg. 1992;107:399-404. 35. Fitz-Ritson D. Assessment of cervicogenic vertigo. / Manipulative Physiol Ther. 1991;14:193-198. 36. Fitzgerald DC. Persistent dizziness following head trauma 765 37. 38. 39. 40. 41. 42. 43. 44. 45. 46. 47. 48. 49. 50. 51. 52. 53. 54. 55. 56. 57. 58. and perilymphatic fistula. Arch Phys Med Rehab. 1995; 76:1017-1020. Fitzgerald DC. Head trauma: hearing loss and dizziness. / Trauma. 1996;40:488-496. Furman JM, Cass SP. Balance Disorders: A Case-Study Approach. Philadelphia, Pa: FA Davis; 1996. Furman JM. Role of posturography in the management of vestibular patients. Otolaryngol Head Neck Surg. 1995; 112:8-1 5. Furman JM, Kamerer DB. Rotational responses in patients with bilateral caloric reduction. Acta Otolaryngol. 1989; 108:355-361. Furman JM, Wall C Ill, Kamerer DB. Alternate and simultaneous binaural bithermal caloric testing: a comparison. Ann Otol Rhino1 Laryngol. 1988;97:359-364. Furman JM, Whitney SL. Central causes of dizziness. Phys Ther. 2000;80:179-187. Calm R, Rittmeister M, Schmitt E. Vertigo in patients with cervical spine dysfunction. Eur Spine 1. 1998;7:55-58. Gray LP. Extra labyrinthine vertigo due to cervical muscle lesions. / Laryngol. 1956;70:352-361. Hain TC, Helminski 10, Reis IL, Uddin MK.Vibration does not improve results of the canalith repositioning procedure. Arch Otolaryngol Head Neck Surg. 2000;126:617622. Herdman SJ. Assessment and treatment of balance disorders in the vestibular deficient patient. In: Duncan PW, ed. Balance: Proceedings of the APTA Forum. Alexandria, Va: APTA; 1990:87-94. Herdman SJ, Tusa RJ, Zee DS, Proctor LR, Mattox DE. Single treatment approaches to benign paroxysmal positional vertigo. Arch Otolaryngol Head Neck Surg. 1993; 119:450-454. Hildingsson C, Wenngren BI, Bring G, Toolanen G. Oculomotor problems after cervical spine injury. Acta Orthop Scand. 1989;60:513-516. Hohl M. Soft-tissue injuries of the neck in automobile accidents: factors influencing prognosis. / Boneloint Surg. 1974;56-Az1675-1682. Jacobson GP, Newman CW. The development of the dizziness handicap inventory. Arch Otolaryngol Head Neck Surg. 1990;116:424-427. Jongkees LBW. Cervical vertigo. Laryngoscope. 1969;79: 1473-1 484. Karlberg M, Magnusson M, Malmstrom EM, Melander A, Moritz U. Postural and symptomatic improvement after physiotherapy in patients with dizziness of suspected cervical origin. Arch Phys Med Rehabil. 1996;77:874-882. Karlberg M, Persson L, Magnusson M. Impaired postural control in patients with cervico-brachial pain. Acta Otolaryngol Suppl. 1995;520:440-442. Lieou YC. Syndrome sympathique cervicale posterieur et arthrite chronique de la colone vertebral cervciale, etude clinique et radiologique [Academic Thesis]. Strasbourg, 1928. Magee DJ. Orthopedic PhysicalAssessment. Philadelphia, Pa: WB Saunders; 1997. Norre ME. Cervical vertigo. Diagnostic and semiological problem with special emphasis upon "cervical nystagmus." Acta Otorhinolaryngol Belg. 1987;41:436-452. Norris SH, Watt I.The prognosis of neck injuries resulting from rear-end vehicle collisions. / Bone Joint Surg. 1983; 65-B:608-611. Oostendorp RAB, Van Eupen AAJM, Van Erp JMM, Elvers HWH. Dizziness following whiplash injury: a neuro-oto- 59. 60. 61. 62. 63. 64. 65. 66. 67. 68. 69. 70. 71. 72. 73. 74. 75. 76. 77. 78. 79. logical study in manual therapy practice and therapeutic implication. / Manual Manip Ther. 1999;7:123-130. Oosterveld WJ, Kortschot HW, Kingma GG, DeJong JMBV, Saatci MR. Electronystagmographic findings following cervical whiplash injuries. Acta Otolaryngol (Stockh). 1991;111:201-205. Padoan S, Karlberg M, Fransson PA, Magnusson M. Passive sustained turning of the head induces asymmetric gain of the vestibulo-ocular reflex in healthy subjects. Acta Otolaryngol. 1998;118:778-782. Phillipszoon AJ. Neck torsion nystagmus. Pract Oto-Rhino-Laryngologist. 1963;25:339-344. Powell LE, Myers AM. The activities-specific balance confidence (ABC) scale. / Gerontol. 1995;50A:M23-M34. Rubin AM, Woolley SM, Dailey VM, Goebel JA. Postural stability following mild head or whiplash injuries. Am / Otol. 1995;16:216-221. Rubin W. Whiplash with vestibular involvement. Arch Otolaryngol. 1973;97:85-87. Ryan MS, Cope S. Cervical vertigo. Lancet. 1955;2:13551358. Sandler B. Lesions of the neck and vertigo. In: Spector M, ed. Dizziness and Vertigo: Diagnosis and Treatment. New York, NY: Grune and Stratton; 1967:219-228. Shumway-Cook A, Horak FB. Assessing the influence of sensory interaction on balance. Phys Ther. 1986;66: 1548-1 550. Shumway-Cook A, Woolacott A. Motor Control: Theory and Practical Application. Baltimore, Md: Williams and Wilkins; 1995. Spitzer WO, Skovron ML, Salmi LR, et al. Scientific monograph of the Quebec Task Force on whiplash-associated disorders: redefining "whiplash" and its management. Spine. 1995;20:1 S-73s. Tjell C, Rosenhall U. Smooth pursuit neck torsion test: a specific test for cervical vertigo. Am / Otol, 1998;19:7681. Toglia JU. Acute flexion-extension injury of the neck: electronystagmographicstudy of 309 patients. Neurology. 1976;26:808-814. van de Calseyde P, Ampe W, Depondt M. ENG and the cervical syndrome. Adv Otorhinolaryngol. 1977;22:119124. Voorhees RL. The role of dynamic posturography in neurotologic diagnosis. Laryngoscope. 1989;99:995-lOOl. Wapner S, Werner H, Chandler KA. Experiments on the sensory-tonic field theory of perception: 1. Effect of extraneous stimulation of the visual perception of verticality. I Exp Psych. 1951;42:351-357. Whitney SL, Herdman SJ. Physical therapy assessment of vestibular hypofunction. In: Herdman SJ, ed. Vestibular Rehabilitation. Philadelphia, Pa: FA Davis; 2000:333372. Whitney SL, Hudak MT, Marchetti GF. The activities-specific balance confidence scale and the dizziness handicap inventory: a comparison. / Vestib Res. 1999;9:253259. Wing LW, Hargrave-Wilson W. Cervical vertigo. Aust NZ / Surg. 1974;44:275-277. Wolf IS, Boyev KP, Manokey BJ, Mattox DE. Success of the modified Epley maneuver in treating benign paroxysmal positional vertigo. Laryngoscope. 1999; 109:900903. Wolf M, Hertanu T, Novikov I, Kronenberg J. Epley's manoeuvre for benign paroxysmal positional vertigo: a prospective study. Clin Otolaryngol. 1999;24:43-46. J Orthop Sports Phys Ther *Volume SO. Number 12. December 2000











© Copyright 2026