
Contains Video DBT-Enhanced Cognitive Behavioral Therapy for Adolescent Trichotillomania:
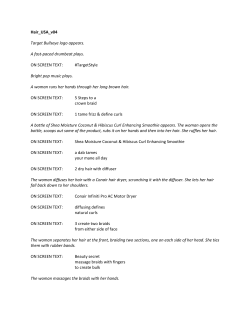
CBPRA-00405; No of Pages 11: 4C Available online at www.sciencedirect.com Cognitive and Behavioral Practice xx (2012) xxx-xxx www.elsevier.com/locate/cabp Contains Video 1 DBT-Enhanced Cognitive Behavioral Therapy for Adolescent Trichotillomania: An Adolescent Case Study Stacy Shaw Welch and Junny Kim, Anxiety and Stress Reduction Center of Seattle (Evidence Based Treatment Centers of Seattle), University of Washington Results and a case study for a DBT-enhanced habit reversal treatment (HRT) for adult trichotillomania (TTM) (Keuthen & Sprich, 2012) is adapted for use with adolescents. Trichotillomania in adolescence is a very important but understudied problem. Onset often occurs in adolescence, and yet very little treatment research exists. DBT-enhanced habit reversal has shown promise in adult samples (Keuthen et al., 2008) and may prove useful as a model for further study in adolescents. Here, we provide a case study using DBTenhanced HRT with an adolescent girl. The treatment emphasizes traditional CBT for TTM and also includes a focus on emotion regulation, mindfulness, and distress tolerance to help manage both focused and automatic pulling. R ESULTS and a case study for a dialectical behavior therapy (DBT)–enhanced CBT treatment for adult trichotillomania (TTM) (Keuthen & Sprich, 2012) is applied here to the treatment of adolescents. DBTenhanced CBT is aimed at improving outcomes and maintenance of gains beyond those typically found to date for TTM sufferers. In adult studies of CBT, complete abstinence from hair pulling is rarely achieved and relapse following treatment is a significant clinical problem (Diefenbach, Tolin, Hannan, Maltby, & Crocetto, 2006; Lerner, Franklin, Meadows, Hembree, & Foa, 1998; Mouton & Stanley, 1996). While the adult TTM literature is certainly in need of more attention, the child and adolescent treatment literature is almost nonexistent. This gap in the treatment literature is quite concerning given the potential importance of this developmental period to the onset, maintenance, and chronicity of TTM. Given the pressing need and lack of data, innovation is sorely needed. The encouraging results from Keuthen et al. (2010) inspired an adaptation of the protocol for use with adolescents. This case study describes the protocol as used to treat an adolescent presenting with TTM who was treated by the first author. 1 Video patients/clients are portrayed by actors. Keywords: trichotillomania; hair pulling; habit reversal; dialectical behavior therapy; adolescent 1077-7229/11/xxx-xxx$1.00/0 © 2012 Association for Behavioral and Cognitive Therapies. Published by Elsevier Ltd. All rights reserved. Trichotillomania in Adolescence Adolescence is a time characterized by rapid developmental change and many psychiatric disorders have their onset during this phase of life. This is true for TTM, which usually develops in late childhood or adolescence. The mean age of onset of cases reported in the literature is 8 years for males and 12 years for females; median age is 6 for males and 12 for females (Graber & Arndt, 1993). The lifetime prevalence of the disorder in adolescents has been estimated to be 1% (Hanna, 1997). The majority of studies find a much higher percentage of females than males in samples of children and adolescents (Hanna, 1997; Mancini, Van Ameringen, Patterson, Simpson, & Truong, 2009). However, at least one epidemiological study found a higher percentage of males. King, Scahill, et al. (1995) conducted a study with a sample of 794 consecutive 17-yearold Jewish Israeli adolescents (369 male, 425 female). The subjects were screened using a questionnaire and interview for current and past hair-pulling and comorbid psychopathology. The study found that males slightly outnumbered females in prevalence, by 5 to 3. Adapting TTM Treatment for Adolescents: Can We Adapt From Adult Models? Given the almost total lack of data on treatment for adolescents with TTM, clinicians are faced with a difficult situation when teenagers and their families present for help with this problem. Adapting a treatment that has been researched with adults, as we have done here, assumes that at least some basic elements of TTM in adolescents are similar to those in adults. Though data are Please cite this article as: Welch & Kim, DBT-Enhanced Cognitive Behavioral Therapy for Adolescent Trichotillomania: An Adolescent Case Study, Cognitive and Behavioral Practice (2012), doi:10.1016/j.cbpra.2011.11.002 2 Welch & Kim limited, the available findings suggest that there are significant similarities and overlap between adult and adolescent TTM. There appear to be enough similarities in how people pull and the function of their pulling to justify an adaptation of the basic principles of adult treatment models for evaluation of their effectiveness with youth. The topography of TTM appears to be similar in adolescents and adults. Although studies of children tend to show less endorsement of the pattern of “rising tension/relief” associated with hair pulling, older children/ teens endorse this symptom more similarly to adults (Hanna, 1997; King, Zohar, et al., 1995; Reeve, Bernstein, & Christenson, 1992). Pulling sites are also similar between adolescents and adults (see Franklin & Tolin, 2007, for a review of studies). Adolescents tend to pull primarily from the scalp, followed by eyelashes and eyebrows, and then hair from other areas of the body (e.g., pubic hair). Many pull from multiple areas (Hanna). Routines associated with the hair once it is pulled are also common (eating it, stroking the lip or mouth, inspecting it, lining it up, biting or popping the root, etc.). Additionally, pulling severity appears similar across age groups (Flessner, Woods, Franklin, Keuthen, & Piacentini, 2009). Psychiatric comorbidity tends to be high among adults with TTM, especially mood and anxiety disorders (Christenson, Ristvedt, & Mackenzie, 1993; Franklin et al., 2008; Reeve et al., 1992). Though data are more limited, the same appears to be true for adolescents, with around half to two-thirds meeting criteria for a comorbid psychiatric disorder, most typically anxiety and/or depression (Hanna, 1997; Lewin et al., 2009). The recent Child and Adolescent Trichotillomania Impact Project (CA-TIP), an Internet-based study, found high rates of comorbidity with depression and anxiety in a sample of 113 youth with TTM ages 10–17. Adolescents reported more of these symptoms than children (close to half of the teens in the sample compared to 17% of children). Depressive symptoms appeared to partly mediate the relationship between TTM symptoms and functional impairment (socially, academically, and interpersonally), and this was not related to duration of illness. The authors concluded that, “taken together, development of TTM during adolescence, a common age of onset, appears to be particularly devastating” (Lewin et al., p. 525). Automatic and Focused Pulling in Adolescence A major research finding in the TTM field in the early 1990s was that there may be two primary types of hair pulling behavior with different cues and reinforcers: automatic/habitual pulling and pulling that functions to regulate emotions (Christenson & Mackenzie, 1994). For instance, approximately 75% of adults with TTM endorse “automatic” pulling (i.e., pulling out of aware- ness), often accompanying sedentary, contemplative activities (Christenson & Mackenzie, 1994). Others pull in a more “focused” manner associated with a more compulsive quality. Here, pulling is often cued by negative emotions, intense thoughts or urges, or attempts to create symmetry (Diefenbach, Mouton-Odum, & Stanley, 2002; Flessner et al., 2009). Focused pulling appears to function more as emotion regulation behavior. It appears that many TTM sufferers have both patterns, though different patterns may accompany different episodes. A recent survey found this pattern in both adults and children/adolescents (Flessner et al., 2007) as have other smaller studies (Hanna, 1997). Of particular relevance to the treatment of adolescents are the results of a recent large cross-sectional study of 1,471 females with TTM ages 10–69 (Flessner et al., 2008). Results indicated a dramatic rise in the incidence of focused pulling at age 13, corresponding to the age of the beginning of puberty. This study also found increases in focused pulling in women of perimenopausal age, followed by a decrease postmenopause. Both developmental epochs are characterized by well-known exacerbations in mood and anxiety related to hormonal changes. Additionally, the Flessner study documented increases in functional impairment that increased over time. Younger children showed mild to moderate social and interpersonal impairment related to their TTM, which steadily increased into late adulthood, when impairment was moderate to severe. Less than 1% of the variance was related to duration of illness. These findings underscore the importance of developing effective treatments for teenagers living with TTM. Treatments for Adolescents With TTM Tolin, Franklin, Diefenbach, Anderson, and Meunier (2007) published an open trial for youth with TTM and have recently completed the first randomized controlled trial for TTM in youth (Franklin et al., 2007). Their open trial included eight biweekly meetings after active treatment concluded for the purpose of helping prevent relapse. Data from the open trial indicated significant reductions in hair pulling as rated by clinicians on the CGI; 77% were classified as “treatment responders” and 32% as “excellent responders.” At 6-month follow-up these ratings were 63% and 32%. Self-report of depression and anxiety showed decreases during treatment as well. Interestingly, none of the patients who achieved an excellent response relapsed. If the strength of initial treatment response/achievement of abstinence predicts future maintenance of gains, this may be an important finding and would be similar to findings in other disorders, such as depression and OCD (Frank et al., 1990; Hiss et al., 1994; Vittengl et al., 2009). The results are an extremely important first step in developing Please cite this article as: Welch & Kim, DBT-Enhanced Cognitive Behavioral Therapy for Adolescent Trichotillomania: An Adolescent Case Study, Cognitive and Behavioral Practice (2012), doi:10.1016/j.cbpra.2011.11.002 DBT2Enhanced CBT for Adolescent TTM treatments for youth with TTM. This treatment is comprehensive, state-of-the-art CBT, a major step forward in the field, and includes strategies to prevent relapse. Still, the results suggest that further innovation in how we provide CBT would be welcome. These results are more modest than hoped for in terms of helping more children stop pulling, and many children who did not achieve excellent results during the active treatment phase relapsed. CBT appears to be a good treatment; but we still need to do better for these youth. Improving Treatment for TTM DBT-enhanced CBT was developed in an attempt to improve and build upon the current state of the art by adding specific skills to more comprehensively address specific styles/functions of pulling. Recently, many researchers have suggested that the treatment for TTM might be improved if interventions were more specifically matched to the various functions of hair pulling (see Flessner et al., 2008). It has been hypothesized that traditional CBT interventions have had modest outcomes to date as they may be effective primarily with the “automatic” rather than the “focused” style of pulling (which appears more related to emotion regulation and is related to hair pulling severity). This may be especially important in adolescence, when focused pulling increases. Another goal in developing DBT-enhanced CBT was to increase the options available to help deal with negative or dysregulated mood states, very relevant for youth. Adolescence is a time of intensified emotion and a rich developmental period of learning emotion regulation skills generally. Youth who have the additional struggle of TTM may have even greater emotional vulnerability due to either the difficulty of coping with the disorder, existing psychiatric vulnerability, or both. Whether mood symptoms comprise a risk profile for the disorder or occur as a result of the disorder is unclear. Either way, it makes sense that adding a more specific focus on emotion regulation may be helpful to achieve better results from treatment and maintain them over time. This seems especially important in light of other data suggesting that unremitting, comorbid depressive symptoms negatively mediate treatment outcome in TTM in adults (Keijsers et al., 2006; Keuthen et al., 1998). While the specific mechanisms between negative affective states and pulling behavior remain unknown, it seems clear that adding an emphasis on coping with and reducing negative emotion states could have a major impact on treatment efficacy. DBT-Enhanced CBT for TTM As described by Keuthen and Sprich (2012), the treatment includes the core components of CBT for trichotillomania, including psychoeducation, self-monitoring, habit reversal, stimulus control, and relapse prevention. It also includes skills to improve mindfulness, emotion regulation, and distress tolerance, with specific application to TTM. We hoped that the addition of mindfulness training would complement and improve the focus on increasing awareness and decreasing impulsive pulling, which is essential for patients with automatic pulling behaviors. We also hoped that the additional emotion regulation and distress tolerance skills would provide a context for patients to improve emotion regulation generally, as well as tolerate difficult urges to pull that do not go away immediately and are very difficult to tolerate. The initial data in adult pilot samples have so far been encouraging. In an open pilot trial with 10 adults who met DSM-IV-TR criteria for TTM, significant improvements from baseline in both hair pulling severity and emotion regulation were reported at all study time points, though some worsening occurred on some measures during the follow-up period. Significant correlations were reported between hair pulling severity and emotion regulation throughout follow-up (Keuthen et al., 2010). No data are currently available for adolescents with TTM, although we hope there may be opportunity for further study. The protocol has been modified for use with adolescents in three main ways. First, important issues related to therapeutic style were considered. In our experience working with teens with TTM, overly formal, rigid, or clinical approaches are generally less effective. We believe that communicating expertise about TTM while coming across as an approachable person the teen can relate to helps build a strong interpersonal relationship. Without that, we have found it difficult to progress in therapy with a disorder like TTM, where both the disorder and treatments are hard, long, and sometimes very disappointing in the lack of an easier answer to manage pulling urges. Readers can observe some of this style in the videos contained in this article (see Video 1: Psychoeducation About Trichotillomania; Video 2: Chain Analysis; Video 3: Mindfulness; Video 4: Emotion Regulation; and Video 5: Distress Tolerance). Essentially, a more casual/friendly tone was used. Care was taken not to use professional jargon. Warm engagement was emphasized and opportunities to communicate experience with TTM and also to validate the teen's experience were taken whenever they arose. Much of the style—while not formalized in this adaptation—was borrowed from elements of DBT used to engage clients who have been burned out in some way on the mental health system. For different reasons, this may be relevant to teens with TTM, many of whom have had less than optimal experiences with clinicians who did not recognize or understand their hair pulling behaviors. The second adaptation to the protocol was the inclusion of parents. Parents are often confused, upset, Please cite this article as: Welch & Kim, DBT-Enhanced Cognitive Behavioral Therapy for Adolescent Trichotillomania: An Adolescent Case Study, Cognitive and Behavioral Practice (2012), doi:10.1016/j.cbpra.2011.11.002 3 4 Welch & Kim and frustrated by the ongoing pulling they observe. It is very common for power struggles over the hair pulling to ensue, and frustrations build up over why the teen can't “just stop” and why the parent can't “just stop saying anything about it.” Both struggles are challenging, and in our opinion, must be met with compassion and attention. The struggle of teens, who must live with sometimes constant urges to pull and the frustration of a disorder that impacts their physical appearance, is intense. Additionally, many teens feel that no one understands what they are going through, including their own parents (at best) and are criticized and humiliated for something they wish desperately they could control, but can't (at worst). The struggle of parents is also tremendous; in addition to the normal challenges of parenting a teen, they must find ways to support their child and sometimes accept ongoing hair pulling that is highly distressing to them, especially when they see it happening right in front of them. It can be difficult to understand and very hard to move towards a stance of silent support, as the therapy sometimes requires. We took a case-by-case approach to determine what level would be the best to include parents. The parents were always seen during the initial assessment and it was then determined whether it made more sense to include them in an ongoing way (at the beginning and end of sessions, for instance) or to have private “check-in” meetings where their efforts to support their teen could be discussed. Sometimes, we thought parents needed a private place where they could work through difficult feelings and say things that would be better not said in front of their child. Occasionally, this would require an additional therapist just for the parents, if the teen was not open to the therapist having parental contact or there were more in-depth issues that needed work (i.e., a more formal behavioral parent training approach if there were other issues such as oppositional behavior). The third major area of modification included going through the worksheets, forms, and handouts to make sure they were developmentally appropriate and would appeal to teens. At times, the amount of worksheets, forms, and formal homework was decreased, depending on the age and developmental needs of the teen. Skills presented were revised slightly to ensure that they were developmentally appropriate (for instance, a list of pleasant events in the emotion regulation module was revised to include activities typical of adolescents). Care was taken to use examples relevant to teens, and at times forms were created in session with the teen, as opposed to using a more standard worksheet. Otherwise, the protocol was delivered as it has been implemented and studied with adults. Here, we provide a case example of an extension of these treatment principles to therapy with an adolescent girl who presented for treatment of TTM. Key details have been changed to protect her confidentiality. Case Study 2 Molly was a 15-year-old typically developing female. She presented to treatment following earlier successful treatment for an anxiety disorder at around age 10 with the same therapist. Molly and her parents reported that she had at least one episode of pulling early in life, around the age of 5, when she pulled out most of her eyelashes one day while sitting down watching television. They were unsure if she pulled hair following this episode. Following this episode, Molly frequently pulled her eyelashes as they grew back, usually when trying to go to sleep, during long car rides, and during sedentary activities. They reported a long pattern of other body-focused repetitive behaviors throughout childhood, most notably twirling her hair, stating that “her fingers are almost always in her hair” and they remembered that almost always having been the case. Throughout childhood, Molly would often bite her nails, chew on the inside of her cheek, and pick at any scabs or flaking skin that she found on her body, lips, scalp, or face. This pattern is similar to that of many children who report multiple body-focused repetitive behaviors (BFRBs) in childhood, and then find that the number of different BFRBs decreases into adolescence and adulthood. Molly and her parents reported that at some point in middle childhood, she stopped pulling her eyelashes over the summer, although she continued to exhibit many other BFRBs. At around the age of 13, Molly began pulling more scalp hair and some eyebrow hair. She was unaware of any particular event that prompted her increase in pulling. She noted that she pulled both when she was sitting and bored as well as when she felt stressed and upset, such as when she had tests or was nervous about an upcoming social interaction. She was also bothered by the extent to which she picked at the skin on her lips and fingers/cuticles, which would sometimes bleed and cause her social embarrassment. Molly was given the following assessment measures: Trichotillomania Scale for Children (TSC), Screen for Child Anxiety Related Disorders (SCARED), Difficulty in Emotion Regulation Scale (DERS), and Moods and Feelings Questionnaire (MFQ). The TSC measures the severity, distress, and impairment associated with TTM (Tolin et al., 2008). The total score ranges from 0 to 2 with lower scores indicating less severity and impairment. The SCARED measures symptom severity linked to anxiety disorders (Muris et al., 2007). The total score ranges from 0 to 82 with scores equal to or greater than 25 indicating the possible presence of an anxiety disorder and scores equal to or greater than 30 indicating the likely presence of an anxiety disorder. The DERS measures clinically 2 Details about the case have been modified to protect the identity of the client. Please cite this article as: Welch & Kim, DBT-Enhanced Cognitive Behavioral Therapy for Adolescent Trichotillomania: An Adolescent Case Study, Cognitive and Behavioral Practice (2012), doi:10.1016/j.cbpra.2011.11.002 DBT2Enhanced CBT for Adolescent TTM 5 TSC Measure Scores 2 1.8 1.6 1.4 Score 1.2 TSC-C TSC-P 1 0.8 0.6 0.4 0.2 0 TSC-C TSC-P Baseline Mid-treatment 2 1.71 1.57 1.2 Post-treatment 0.3 0.5 Followup 0.5 0.5 Timepoint Figure 1. Hair pulling severity and impairment scores (TSC) at baseline, midtreatment, posttreatment, and follow-up. relevant problems related to emotion dysregulation (Gratz & Romer, 2004). The total score ranges from 36 to 180. Lower scores indicate fewer problems with emotion regulation. The MFQ measures depressive symptom severity (Costello & Angold, 1988). The total score ranges from 0 to 26. Higher scores indicate more severe depressive symptoms. Molly's scores on these measures are presented in Figures 1, 2, and 3. Course of Treatment Session 1: Psychoeducation and Assessment Video 1. Psychoeducation about Trichotillomania: Therapist provides psychoeducation to the client about the model and treatment of trichotillomania. The first stage of treatment involved educating Molly and her parents about hair pulling and skin picking. A behavioral model was presented that emphasized TTM as a biologically driven behavior with a strong learning component. Care was taken to validate the difficulty of stopping, as well as to instill hope that new skills could be learned to help decrease pulling behaviors. Molly and her parents reported feeling relieved by the model presented, as both she and her family had worried that her hair pulling might represent some form of self-mutilation or a deep expression of psychological trauma. They all noted a positive reaction to the idea that TTM is not anyone's fault, and that Molly's inability to “just stop” was normal. Another important part of the psychoeducation for the family was the idea that their frequent, occasionally frustrated reminders to her to stop pulling when they observed the behavior were not helpful, and were actually agitating Molly. Early on in treatment, we engaged in a conversation about what would be the best way for Molly's family to support her in treatment around this issue. She asked them to simply say “looks like trich is bugging you, anything you want my help with?” one time, and after that to refrain from commenting. Molly's father expressed a high degree of anxiety about this, and privately expressed to the therapist that he didn't know if he could do this because he had been collecting hairs under Molly's bed for quite some time as a means of monitoring her pulling behaviors. Motivational enhancement strategies were used with Molly, as well as her parents, to help increase their readiness to engage in the requirements of the Please cite this article as: Welch & Kim, DBT-Enhanced Cognitive Behavioral Therapy for Adolescent Trichotillomania: An Adolescent Case Study, Cognitive and Behavioral Practice (2012), doi:10.1016/j.cbpra.2011.11.002 Welch & Kim 6 DERS, SCARED, and MFQ Measure Scores 90 80 70 Score 60 50 DERS SCARED-C MFQ 40 30 20 10 0 Baseline Mid-treatment Post-treatment Followup DERS 82 67 55 49 SCARED-C 50 40 32 27 MFQ 27 25 23 20 Timepoint Figure 2. Emotion regulation (DERS), anxiety (SCARED), and depressive (MFQ) symptom severity scores at baseline, midtreatment, posttreatment, and follow-up. treatment. Molly agreed that if her parents would “back off” to some degree, and follow the therapist's suggestions, she would be open to a weekly check-in with her parents during the therapy sessions to discuss progress and let them know more about how she was doing. This arrangement worked well throughout the course of treatment. Both Molly and her father reported that as her father increased supportive and validating statements Weekly Hair Pulling Frequency 200 180 160 Frequency 140 120 100 wkly hair pulling 80 60 40 20 0 wkly hair pulling Baseline Mid-treatment 180 65 Post-treatment 4 Followup 7 Timepoint Figure 3. Weekly hair pulling scores at baseline, midtreatment, posttreatment, and follow-up. Please cite this article as: Welch & Kim, DBT-Enhanced Cognitive Behavioral Therapy for Adolescent Trichotillomania: An Adolescent Case Study, Cognitive and Behavioral Practice (2012), doi:10.1016/j.cbpra.2011.11.002 DBT2Enhanced CBT for Adolescent TTM about the difficulty involved with changing pulling behaviors, Molly became more open with him outside of the therapy sessions. Chain Analysis and Self-Monitoring During an early session, Molly and the therapist completed a chain analysis of her most recent pulling episode. A behavioral chain analysis is a strategy used by behavior therapists to obtain a moment-by-moment sequence of events; this has been operationalized for clinical use and termed “chain analysis” by Linehan in DBT (Linehan, 1993). Molly's chain, which she thought was typical of some of her pulling patterns, involved a busy, stressful week at school, feeling anxious about how much she had to get done academically, and social strain with a peer. She recalled having strong urges to pull while she was at drama practice, sitting in the theatre watching others go through some scenes. She resisted the urges to pull because she was too embarrassed to pull in front of others. She began pulling while she was in the car going home from practice. She then put on the hood of her sweatshirt and tried not to pull her hair while at dinner with her family because she knew that they would notice and call attention to the pulling. She had to stay up late writing a paper, and again worked hard not to pull her hair, even taking a shower at one point because she knew getting her hair wet would help. She had to stay up very late working on her paper, however, and at one point became highly frustrated and anxious about the work; at that point she noted that she had thoughts about giving up and mounting urges to pull and pulled her hair intermittently while staring at her computer screen. She recalled feeling terrible after pulling and then picked at skin on her lip until it hurt/bled. In addition to details about the environmental context of hair pulling (the “what” and “when”), the chain anal- Video 2. Chain Analysis: Therapist conducts a chain analysis with client to figure out what led to a recent pulling episode. ysis included details about the specific components of Molly's hair-pulling patterns (the “how”). Like many hair pullers, Molly would begin by fingering her hair and scalp, looking for hairs that were slightly different in some way (thicker, more wiry, or shorter). She would then isolate the hair and tug it. Following the pull, she would examine the hair and bite the bulb, or “root” of the hair. She would often stroke her lips with the hair, and then release it. She did not eat the hair. After conducting the chain analysis, Molly was asked to monitor all hair pulling using forms provided by the therapist. Through the chain analysis and self-monitoring, she and the therapist identified high-risk situations where she was likely to pull her hair: in the car, studying by herself late at night, going to sleep, getting ready for a date or important social interaction she was nervous about, math class (which she found both boring and anxiety-producing), watching TV, and when very angry at her parents. Session 2: Habit Reversal and Stimulus Control Habit reversal is a technique to help patients use a competing response to help tolerate urges to pull/control the behavior. Substituting a “competing response,” or a motor behavior that is incompatible with hair pulling, helps the individual shift to a new habit. Ideally, the competing response can be maintained for at least 90 seconds, be as inconspicuous as hair pulling, be easy to do, and produce increased awareness of the behavior. Sometimes, people find it useful to employ the same muscles that would have been used to pull hair. Muscle tension is produced and held, which may help “burn out” the urge to pull. Molly was taught to make tight fists and hold them for 90 seconds. She was taught to use this strategy if she had an urge to pull or was in a high-risk situation for pulling. She and the therapist also came up with multiple other competing responses, including squeezing a squishy/koosh ball, holding pens hard during schoolwork, squeezing the mouse on her computer, and holding her books or phone with both hands and squeezing her fingers together. She and her father worked out a system where they would buy a dozen small items to use for competing responses at a time, and then rotate them every few days. Molly reported that the novelty seemed to help increase their use. She also found it useful to pop bubble wrap, or bite the bubble wrap, blow and bite bubbles with gum, and pick out alfalfa sprouts out of a box and bite the “bulb” of the sprout. Other orally stimulating activities were used such as pop rocks or hard candy, gummy worms that she could play with, rub on her lips, and bite, and popping bath beads between her fingers/rubbing the oil from the beads on her hands to moisturize them. This also helped her avoid skin picking on her hands, as well as avoid hair pulling because she did not want to get her hair oily. Please cite this article as: Welch & Kim, DBT-Enhanced Cognitive Behavioral Therapy for Adolescent Trichotillomania: An Adolescent Case Study, Cognitive and Behavioral Practice (2012), doi:10.1016/j.cbpra.2011.11.002 7 Welch & Kim 8 Stimulus control Stimulus control techniques are strategies implemented by the client to decrease pulling by (a) providing cues to maintain awareness, (b) reducing the stimulation provided by pulling, or (c) interfering with or preventing pulling. To apply these strategies, Molly and the therapist discussed how she could apply specific strategies to help her through high-risk situations for pulling. Molly obtained permission to wear a hat at school during her math class and she tried wearing bandages around her fingers so that it would be difficult to isolate a hair and pull it. At night when going to bed, she wore moisturizing gloves (used with lotion) when falling sleep. While studying, she tried wetting down her hair and applying conditioner, which she left in her hair for hours. She also kept her nails cut very short and her father agreed to schedule some manicures for her as a reward for using her strategies. She also put notes on her computer and sent messages to herself on her cell phone during highrisk times to remind her to use her strategies. began practicing mindful awareness during the day and started reporting that she noticed more times when she pulled. She also said that the mindfulness exercises helped her notice when she was picking at the skin on her lip, an activity that she did primarily out of awareness. This dramatically reduced the amount that she picked the skin in that area. She found the pulling on her scalp to be more difficult to decrease. Molly initially reported that mindfulness of her scalp pulling seemed to make it more difficult to stop. She and the therapist worked on using her mindfulness skills to help her focus on making mindful choices about what strategy to use when she was aware of urges. She noted that the mindfulness practice helped her work on practicing different strategies to decrease pulling, as opposed to relying on a single skill all/most of the time. She reported this was helpful and she noted that she was using many more strategies on a regular basis than she had at first. Sessions 6–8: Emotion Regulation Molly was introduced to mindfulness and stated that this was a new concept for her. Although she had done yoga in her PE class and she noted that mindfulness seemed somewhat similar to the breathing exercises she had done there, she reported that she had not previously thought about the idea of the practice of being aware of the moment and nonjudgmental observation. She and the therapist reviewed the DBT concepts of states of mind (wise mind, emotion mind, reasonable mind) and discussed where pulling fit into these. She and the therapist discussed the concept of practicing increased awareness, and began engaging in different mindfulness practices during the beginning of each session, such as awareness of the breath, or observation of thoughts. Molly The emotion regulation module consists of a wide range of skills that draw from an evidence base about (a) regulating emotions more generally and (b) regulating emotions in response to events that are emotionally difficult. Upon review with clients, skills that seem particularly relevant to pulling are selected to work on with more focus. Molly's general emotion regulation strategies were good; she exercised, had good social relationships, and regularly used strategies she had learned in her earlier course of CBT to help regulate emotion (progressive muscle relaxation, cognitive restructuring). She and the therapist talked about her general tendency to be doing something all the time as something that made her more vulnerable to becoming dysregulated and pulling. They worked on planning breaks so she could relax, especially on nights when she had a lot of Video 3. Mindfulness: Therapist teaches the client mindfulness, practicing and demonstrating the skill in session. Video 4. Emotion Regulation: Therapist teaches the client emotion regulation skills. Sessions 3–5: Mindfulness Please cite this article as: Welch & Kim, DBT-Enhanced Cognitive Behavioral Therapy for Adolescent Trichotillomania: An Adolescent Case Study, Cognitive and Behavioral Practice (2012), doi:10.1016/j.cbpra.2011.11.002 DBT2Enhanced CBT for Adolescent TTM studying to do. She found that planning a few 10-minute breaks as opposed to taking “pulling breaks” was extremely helpful. Molly and the therapist also worked on the skill of “opposite action” (exposure) to anxiety in math class. This involved talking, answering questions, or asking questions in class early on during the hour. She found that if she did this toward the beginning of the class she was less agitated and this seemed to help decrease pulling. Sessions 9–10: Distress Tolerance Distress tolerance skills help patients find ways to tolerate distress without pulling, including tolerating strong and difficult urges to pull. Molly was already making very strong efforts to avoid pulling, but mostly just told herself not to do it. In this module of therapy, she and the therapist worked on identifying other ways she could get herself through a “crisis,” which in Molly's case was simply the incredibly strong urge to pull her hair. She developed a number of strategies, including self-soothing (listening to her favorite music, eating chocolate, shopping online, and snuggling with a childhood blanket while watching TV). It took some work for Molly to realize that these strategies were not designed to make her urges go away, but to help her coexist with the urges without resorting to pulling. She and the therapist also worked on the skill of “radical acceptance”—specifically, accepting that she had TTM and continued to experience urges to pull, even though she had done very well in treatment. This was very difficult for her and would sometimes make her want to give up and pull. She worked hard on taking a nonjudgmental stance toward her urges and pulling, and this was useful to help her focus more frequently on making mindful choices about what to do in response to her urges. Video 5. Distress Tolerance: Therapist teaches client distress tolerance skills to help in situations where there are urges to pull. Parent Training Molly's parents, her father in particular, were involved throughout treatment. At the beginning and end of each session, a brief check-in was done with her parents. Often, Molly taught the skills she had learned in session to her father, and then her father was coached in how he could support Molly during the week. Often, he was coached simply to withhold comments about pulling. Parental involvement at this level is not always possible with adolescents, who sometimes do not wish their parents to be actively involved in their treatment, but in this case it was useful and appeared to help make Molly's relationship to her parents closer. Molly's father agreed to support her by not talking about the hair pulling/skin picking and by buying all tools to help Molly when requested. In addition, her father participated in several sessions with the therapist to help support his efforts to not say anything about the pulling and encourage the rest of the family to do this as well, which was extremely difficult for him. He responded well to praise by therapist and also engaged in his own effort to stop a difficult behavior (overeating) by using some of the strategies that Molly was using in therapy. Both Molly and her father said that the bond between them improved as a result. Other behavioral parent training interventions were also taught during sessions with her father, such as attending to positive behavior, validation and encouragement, and differential reinforcement of other behaviors. Session 11–16: Relapse Prevention and Booster Sessions Towards the end of therapy, Molly worked on a relapse prevention plan with the therapist, identifying what had worked in treatment and how she could keep working on her hair pulling. She and the therapist also discussed the “abstinence violation effect” and how she could avoid a Video 6. Parent Training: Therapist provides education to client’s father about trichotillomania and advises ways that father can be helpful. Please cite this article as: Welch & Kim, DBT-Enhanced Cognitive Behavioral Therapy for Adolescent Trichotillomania: An Adolescent Case Study, Cognitive and Behavioral Practice (2012), doi:10.1016/j.cbpra.2011.11.002 9 Welch & Kim 10 full relapse when inevitable slips occurred. Booster sessions were then spaced out every few weeks. Molly's pulling decreased substantially over the course of treatment (see Figure 1). It did increase slightly posttreatment (see Figure 1) but both Molly and her family reported that the pulling was not contributing to noticeable hair loss or significant distress. While Molly said that she wished trich could go away completely, she felt that she had control over hair pulling and that the skills she had learned were helping her deal with other stressful situations in her life. Discussion Adolescence is an important time in terms of the development of TTM. As reviewed above, TTM often onsets in adolescence. Important patterns of pulling often begin during the teen years, such as the beginning of “focused” pulling that may serve to regulate emotions (Christenson et al., 1993). Adolescence may be a particularly important time for treatment of TTM, and the possibility of preventing the kind of chronic, difficult-to-treat disorder seen in adults is an exciting propect. However, the child and adolescent treatment data are even more sparse than the adult data, with only one published open trial to date (see Tolin et al., 2007), and no RCTs yet published (Bloch, 2009). The case study described here details an adaptation of a new treatment package for TTM, DBT-enhanced CBT (Keuthen et al., 2010). The treatment is an attempt to improve existing CBT treatments through the addition of skills to target specific pulling styles and has been reviewed elsewhere (Keuthen & Sprich, 2012) and has some promising, if preliminary, data (Keuthen et al., 2010). Given the importance of emotion regulation and the emergence of focused pulling in adolescence, we hoped that adapting the DBT-enhanced CBT protocol for use with teens might prove useful and pave the way for more rigorous study. Although the results of any case study must be interpreted cautiously, we were encouraged by the response of the teen described here. Our clinical impression was that the DBT skills did appear to enhance her response to the typical CBT skills. We observed that the mindfulness and distress tolerance skills, in particular, seemed very useful. The mindfulness skills appeared to help Molly increase her awareness generally of her pulling, in a way that actually increased her use of the more traditional CBT skills, such as habit reversal and stimulus control. The distress tolerance skills also appeared to help Molly live with the distressing, uncomfortable urge to pull long enough to employ the CBT techniques. She also seemed to be more engaged with using them even when they did not result in an immediate reduction in her pulling urges. The positive results from these clinical innovations and this case study are encouraging and we hope that further research will demonstrate the efficacy of this approach in treating teens with TTM. Supplementary materials related to this article can be found online at doi:10.1016/j.cbpra.2011.11.002. References Bloch, M. H. (2009). Trichotillomania across the life span. Journal of the American Academy of Child & Adolescent Psychiatry, 48, 879–883. Christenson, G., & Mackenzie, T. (1994). Trichotillomania. In M. Hersen, R. T. Ammerman (Eds.), Handbook of prescriptive treatments for adults (pp. 217–235). New York, NY US: Plenum Press. Christenson, G. A., Ristvedt, S. L., & Mackenzie, T. B. (1993). Identification of trichotillomania cue profiles. Behaviour Research and Therapy, 31, 315–320. Costello, E. J., & Angold, A. (1988). Scales to assess child and adolescent depression: Checklists, screens, and nets. American Academy of Child and Adolescent Psychiatry, 27, 726–737. Diefenbach, G. J., Mouton-Odum, S., & Stanley, M. A. (2002). Affective correlates of trichotillomania. Behaviour Research and Therapy, 40, 1305–1315. Diefenbach, G. J., Tolin, D. F., Hannan, S., Maltby, N., & Crocetto, J. (2006). Group treatment for trichotillomania: Behavior therapy versus supportive therapy. Behavior Therapy, 37, 353–363. Flessner, C. A., Woods, D. W., Franklin, M. E., Cashin, S. E., & Keuthen, N. J. (2008). The Milwaukee Inventory for Subtypes of Trichotillomania-Adult Version (MIST-A): Development of an instrument for the assessment of 'focused' and 'automatic' hair pulling. Journal of Psychopathology and Behavioral Assessment, 30, 20–30. Flessner, C. A., Woods, D. W., Franklin, M. E., Keuthen, N. J., & Piacentini, J. (2009). Cross-sectional study of women with trichotillomania: A preliminary examination of pulling styles, severity, phenomenology, and functional impact. Child Psychiatry and Human Development, 40, 153–167. Flessner, C. A., Woods, D. W., Franklin, M. E., Keuthen, N. J., Piacentini, J., Cashin, S. E., . . . TLC-SAB (2007). The Milwaukee Inventory for Styles of Trichotillomania-Child Version (MIST-C): Initial development and psychometric properties. Behavior Modification, 31, 896–918. Frank, E., Kupfer, D. J., Perel, J. M., & Cornes, C. (1990). Three-year outcomes for maintenance therapies in recurrent depression. Archives of General Psychiatry, 47, 1093–1099. Franklin, M. E., Cahill, S., Roth Ledley, D., Cardona, D., & Anderson, E. (2007). Presentation given at Word Congress in Barcelona, Spain. Franklin, M. E., Flessner, C. A., Woods, D. W., Keuthen, N. J., Piacentini, J., Moore, P., . . . TLC-SAB (2008). The Child and Adolescent Trichotillomania Impact Project: Descriptive psychopathology, comorbidity, functional impairment, and treatment utilization. Journal of Developmental and Behavioral Pediatrics, 29, 493–500. Franklin, M. E., & Tolin, D. F. (2007). Treating trichotillomania: Cognitivebehavioral therapy for hairpulling and related problems. New York: Springer. Graber, J., & Arndt, W. (1993). Trichotillomania. Comprehensive Psychiatry, 34, 340–346. Gratz, K. L., & Romer, L. (2004). Multidimensional assessment of emotion regulation and dysregulation: Development, factor structure, and initial validation of the difficulties in emotion regulation scale. Journal of Psychopathology & Behavioral Assessment, 26, 41–54. Hanna, G. (1997). Trichotillomania and related disorders in children and adolescents. Child Psychiatry and Human Development, 27, 255–268. Hiss, H., Foa, E. B., & Kozak, M. J. (1994). Relapse prevention program for treatment of obsessive-compulsive disorder. Journal of Consulting and Clinical Psychology, 62(4), 801–808. Keijsers, G. P. J., van Minnen, A., Hoogduin, C. A. L., Klaassen, B. N. W., Hendriks, M. J., & Tanis-Jacobs, J. (2006). Behavioural treatment of trichotillomania: Two-year follow-up results. Behaviour Research and Therapy, 44, 359–370. Please cite this article as: Welch & Kim, DBT-Enhanced Cognitive Behavioral Therapy for Adolescent Trichotillomania: An Adolescent Case Study, Cognitive and Behavioral Practice (2012), doi:10.1016/j.cbpra.2011.11.002 DBT2Enhanced CBT for Adolescent TTM Keuthen, N. J., O'Sullivan, R. L., Goodchild, P., Rodriguez, D., Jenike, M., & Baer, L. (1998). Retrospective review of treatment outcome for 63 patients with trichotillomania. The American Journal of Psychiatry, 155, 560–561. Keuthen, N. J., Rothbaum, B. O., Welch, S. S., Taylor, C., Falkenstein, M., Heekin, M., . . . Jenike, M. A. (2010). Pilot trial of Dialectical Behavior Therapy-enahnced habit reversal for trichotillomania. Depression and Anxiety, 27, 953–959. Keuthen, N. J., & Sprich, S. E. (2012). Utilizing DBT skills to augment traditional CBT for trichotillomania: An adult case study. Cognitive and Behavioral Practice, 19, xx-xx. doi:10.1016/j.cbpra.2011.02.004. King, R. A., Scahill, L., Vitulano, L. A., Schwab-Stone, M., Tercyak, K. P. Riddle, M. A. (1995). Childhood trichotillomania: Clinical phenomenology, comorbidity, and family genetics. Journal of the American Academy of Child & Adolescent Psychiatry, 34, 1451–1459. King, R. A., Zohar, A. H., Ratzoni, G., Binder, M., Kron, S., Dycian, A., . . . Apter, A. (1995). An epidemiological study of trichotillomania in Israeli adolescents. Journal of the American Academy of Child & Adolescent Psychiatry, 34, 1212–1215. Lerner, J., Franklin, M. E., Meadows, E. A., Hembree, E., & Foa, E. B. (1998). Effectiveness of a cognitive behavioral treatment program for trichotillomania: An uncontrolled evaluation. Behavior Therapy, 29, 157–171. Lewin, A. B., Piacentini, J., Flessner, C. A., Woods, D. W., Franklin, M. E., Keuthen, N. J., et al. (2009). Depression, anxiety, and functional impairment in children with trichotillomania. Depression and Anxiety, 26, 521–527. Linehan, M. M. (1993). Skills Training Manual for Treating Borderline Personality Disorder. New York, NY: Guilford Publications. Mancini, C., Van Ameringen, M., Patterson, B., Simpson, W., & Truong, C. (2009). Trichotillomania in youth: A retrospective case series. Depression and Anxiety, 26, 661–665. Mouton, S. G., & Stanley, M. A. (1996). Habit reversal training for trichotillomania: A group approach. Cognitive and Behavioral Practice, 3, 159–182. Muris, P., Merckelback, H., Schmidt, H., & Mayer, B. (2007). The revised version of the Screen for Child Anxiety Related Emotional Disorders (SCARED-R): Factor structure in normal children. Personality and Individual Differences, 26, 99–112. Reeve, E. A., Bernstein, G. A., & Christenson, G. A. (1992). Clinical characteristics and psychiatric comorbidity in children with trichotillomania. Journal of the American Academy of Child & Adolescent Psychiatry, 31, 132–138. Tolin, D. F., Diefenbach, G. J., Flessner, C. A., Franklin, M. E., Keuthen, N. J., Moore, P., . . . TLC-SAB (2008). The trichotillomania scale for children: Development and validation. Child Psychiatry and Human Development, 39, 331–349. Tolin, D. F., Franklin, M. E., Diefenbach, G. J., Anderson, E. Meunier, S. A. (2007). Pediatric trichotillomania: Descriptive psychopathology and an open trial of cognitive behavioral therapy. Cognitive Behaviour Therapy, 36, 129–144. Vittengl, J. R., Clark, L. A., & Jarrett, R. B. (2009). Continuation-phase cognitive therapy's effects on remission and recovery from depression. Journal of Consulting and Clinical Psychology, 77(2), 367–371. Address correspondence to Junny Kim, University of Washington, Anxiety and Stress Reduction Center of Seattle, 1200 5th Ave., Suite 800, Seattle, WA 98101; e-mail: [email protected]. Received: December 3, 2010 Accepted: November 5, 2011 Available online xxxx Please cite this article as: Welch & Kim, DBT-Enhanced Cognitive Behavioral Therapy for Adolescent Trichotillomania: An Adolescent Case Study, Cognitive and Behavioral Practice (2012), doi:10.1016/j.cbpra.2011.11.002 11









© Copyright 2026