
Pregnancy in a Patient With Adrenal Carcinoma Literature
S P E C I A L
C l i n i c a l
C a s e
F E A T U R E
S e m i n a r
Pregnancy in a Patient With Adrenal Carcinoma
Treated With Mitotane: A Case Report and Review of
Literature
Liana Tripto-Shkolnik, Zeev Blumenfeld, Moshe Bronshtein, Asher Salmon,
and Anat Jaffe
Diabetes and Endocrinology Unit (L.T.S., A.J.), Hillel Yaffe Medical Center, Hadera 38100, Israel;
Reproductive Endocrinology (Z.B.), Department of Obstetrics and Gynecology, RAMBAM Health Care
Campus, Rappaport Institute and Faculty of Medicine, Technion-Israel Institute of Technology, Haifa
31097, Israel; Faculty of Social Welfare and Health Sciences (M.B.), University of Haifa, Haifa 31095,
Israel; and Sharett Institute of Oncology (A.S.), Hadassah University Hospital, Jerusalem 91120, Israel
Context: Adrenocortical carcinoma (ACC) affects patients in a broad age group, including young
women. Mitotane, an adrenolytic agent, is the mainstay of treatment after surgical removal of the
tumor. There is extreme paucity of information regarding the effect of mitotane on childbearing
potential and pregnancy outcome.
Objective: The aim of the study was to describe and discuss the case of an ACC patient who
conceived while on mitotane treatment. Current literature is reviewed.
Patient and Methods: A 33-year-old woman received mitotane treatment for 4 years due to metastatic ACC. Despite nearly therapeutic blood levels of the drug, the patient had regular menstruation and was able to conceive. Mitotane was stopped at gestation week 6. Although the drug
continued to be detected in considerable amounts, the fetus developed normally, including morphologically intact adrenal glands. At gestation week 21, pregnancy was terminated due to ACC
recurrence. Mitotane levels were undetectable in fetal cord blood and amniotic fluid.
Conclusion: Our report suggests that mitotane, despite its action as an endocrine disruptor, does
not affect normal gonadal function or an ability to conceive. The concern of placental transfer by
this hydrophobic compound is not supported by our findings. However, we do not recommend
drawing conclusions regarding the safety of mitotane in pregnancy, based on 1 or several case
reports. Until more data are available, pregnancy should be avoided in women being treated with
mitotane for ACC. (J Clin Endocrinol Metab 98: 443– 447, 2013)
he patient first presented in 2005, at the age of 29
years, with rapid development of facial and ankle
edema, hirsutism, supraclavicular fat pads, and easy bruising. Cushing’s syndrome was diagnosed by 9 times the
upper limit of normal urinary free cortisol and abnormal
overnight dexamethasone suppression test. ACTH was undetectable. Abdominal computer tomography revealed a
right adrenal mass measuring 7.5 cm in its longest diameter,
with baseline Hounsfield unit density of 30, undergoing contrast enhancement to 66 and no contrast washout on late
T
10-minute scan. According to the above parameters, adrenal
carcinoma was suspected. No metastases were seen on abdominal and lung computer tomography scan and on fluorodeoxyglucose (FDG)-positron emission tomography
(PET). Electrolytes were normal at presentation, but over a
period of 10 days, hypokalemia evolved, indicating overt
hypercortisolism. It responded to treatment with aldospirone. At this point, ketoconazole was administered.
Urinary free cortisol had fallen from 1018 to 313 mg/d
after 2 days of therapy and to 130 mg/d after 4 days.
ISSN Print 0021-972X ISSN Online 1945-7197
Printed in U.S.A.
Copyright © 2013 by The Endocrine Society
doi: 10.1210/jc.2012-2839 Received July 22, 2012. Accepted November 28, 2012.
First Published Online December 28, 2012
Abbreviations: ACC, Adrenal cortical carcinoma; FDG, fluorodeoxyglucose; PET, positron
emission tomography; US, ultrasound.
J Clin Endocrinol Metab, February 2013, 98(2):443– 447
jcem.endojournals.org
The Endocrine Society. Downloaded from press.endocrine.org by [${individualUser.displayName}] on 11 June 2014. at 14:43 For personal use only. No other uses without permission. . All rights reserved.
443
444
Tripto-Shkolnik et al
Pregnancy on Mitotane Treatment
The patient underwent surgery and the mass, measuring 8 ⫻ 6 ⫻ 5 centimeters and weighing 165 grams, was
excised. The pathologist concluded that the lesion was
adrenocortical carcinoma (ACC) with abundant necrosis,
vascular invasion, and Ki-67 of 30 – 40%.
The patient started mitotane treatment immediately after surgery and continued treatment at a dose of 1.5–3 g/d
with plasma mitotane level monitoring (Table 1). Plasma
levels were measured by Lysosafe service provided by HPA
Pharma (www.lysosafe.com).
Further dose escalation was prevented by gastrointestinal intolerance.
One year after the surgery, follow-up FDG-PET scan
revealed disseminated disease with lung, liver, and lymph
node metastases.
The patient started chemotherapy according to EDP
(etoposide, doxorubicin, and cisplatin) protocol (1). Prior
to chemotherapy initiation, and monthly for the duration,
GnRH analog treatment was given for fertility preservation (2, 3).
After 4 courses of chemotherapy, the patient preferred
to stop the treatment. She continued mitotane, glucocorticoid and mineralocorticoid replacement, and oral contraceptive pills.
Mitotane level reached the therapeutic target after 18
months of therapy (Table 1).
Serial FDG-PET scans were negative.
One and a half years after cessation of chemotherapy,
the patient chose to stop oral contraceptives, regular menstrual periods were resumed, and hormonal profile was of
the ovulating type.
After 3 months the patient learned that she was
pregnant.
At this point she was strongly advised to terminate the
pregnancy. The patient was determined to continue.
The patient decided to stop mitotane at 6-week gestation due to her desire not to harm the fetus. Blood levels
TABLE 1. Mitotane Level Monitoring During Treatment
and After Drug Withdrawal
Clinical Context
Treatment started
First recurrence
EDP chemotherapy
Serial FDG-PET negative
Contraceptive stopped
6 wk pregnanta
Second recurrence
Pregnancy terminated
Mitotane
Dose, g/d
2.5–3
3.5
3
1.5–3
1.5
1.5
0
0
Mitotane
Level,
mg/L
1.6 – 6.6
7.8
13.4
13.2–20.6
13.2
9.8
5.99
4.2
Abbreviation: EDP, etoposide, doxorubicin, and cisplatin.
a
Mitotane stopped at 6 weeks gestation.
Months
After
Diagnosis
2–11
12
17
20 –27
34
40
42
45
J Clin Endocrinol Metab, February 2013, 98(2):443– 447
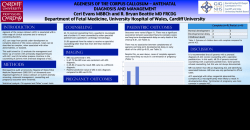
Figure 1. Prenatal US showing longitudinal, parasagittal axis of the
fetus, clearly visualizing normal-sized left adrenal.
were monitored (Table 1). Those continued to be measurable 5 months after discontinuation. She continued
glucocorticoid supplementation with hydrocortisone.
Change of supplemental glucocorticoid to dexamethasone
was considered, in the face of possible placental transfer of
mitotane and, thus, fetal hypoadrenalism that might have
been addressed with dexamethasone replacement.
Fetal ultrasound (US) at week 16 revealed a morphologically normal female fetus, no intrauterine growth retardation, and normal appearing adrenals (Figure 1).
At gestation week 18, the patient presented with a clinical picture compatible with rapid evolvement of Cushing’s syndrome. Hypercortisolism was biochemically confirmed—loss of diurnal variation, and urinary free cortisol
elevated to 9 times normal.
Abdominal US and magnetic resonance imaging demonstrated a large 8-centimeter liver metastasis, and lung
computer tomography revealed a 2-centimeter metastasis
of left lung base.
Since the patient preferred the effort to spare the pregnancy, right hepatectomy was attempted but was unsuccessful due to profuse bleeding from a severely congested
liver.
At 21-week gestation, the pregnancy was terminated.
Prior to the procedure, amniotic fluid and fetal cord blood
were drawn for mitotane level; in both samples, the drug
was undetectable. Blood levels 2 weeks before the procedure and 10 days afterward were 5.99 and 4.2 mg/L,
respectively.
The patient resumed chemotherapy, and the liver mass
shrank but remained detectable on imaging.
Six months after the pregnancy termination, the patient
underwent surgery to remove the liver lesion. Immediately
after the procedure, the patient suffered a refractory
shock. As part of resuscitation efforts, reexploration of the
The Endocrine Society. Downloaded from press.endocrine.org by [${individualUser.displayName}] on 11 June 2014. at 14:43 For personal use only. No other uses without permission. . All rights reserved.
J Clin Endocrinol Metab, February 2013, 98(2):443– 447
jcem.endojournals.org
surgery site was undertaken, but no bleeding was found.
The patient died on the operating table. It was suspected
that she might have suffered a massive pulmonary embolism, but a postmortem investigation was not performed.
Discussion
ACC is a rare neoplasm with a high mortality rate. The
disease has bimodal age distribution with a first peak in
childhood and a second peak in ages 40s and 50s. ACC is
slightly more prevalent in women (4). More than half of
the cases are hormone secreting—most commonly cortisol
and androgens (5).
Mitotane [o,p’ dichlorodiphenyl dichloroethane (o,p’
DDD)] (Lysodren; HRA Pharma, Paris, France; Bristol
Meyers Squibb, New York, New York) is a derivate of p,p’
dichlorodiphenyl trichloroethane (p,p’ DDT), a common
insecticide.
Mitotane’s adrenolytic activity has been known since
the late 1950s and has been used in the treatment of endogenous hypercortisolism and adrenal carcinoma (6).
Recent data suggest that treatment with mitotane might
prolong recurrence-free survival in patients with ACC (7).
Blood level monitoring is recommended. The target blood
concentration is 14 –20 mg/L (4). Given the young age of
diagnosis in some patients and the need for prolonged if
not lifelong treatment, questions do arise concerning the
445
feasibility of pregnancy on mitotane therapy as well as
mutagenic potential of the compound.
ACC diagnosed during pregnancy has been reported
with grave maternal and fetal outcomes; several reports
have been published recently (8 –10).
There is an extreme paucity of data regarding the effect
of mitotane on the human fetus. The suspicion of the ability of this hydrophobic compound to cross the placenta
comes from the observation that p,p’ DDT, the morphologically similar insecticide, is found in cord blood of infants in DDT-exposed areas (11). Given the adrenolytic
activity of the drug, teratogenic effect is feared.
However, very few reports regarding humans address
this issue. Those are summarized in Table 2.
In 1973, Luton et al (12) published a paper describing
several patients treated with mitotane for Cushing’s disease. Among them, one patient gave birth to a normal
infant after being treated throughout her pregnancy.
In 1978, Leiba et al (13) reported a case of a 38-year-old
woman treated with mitotane 5 g/d for 100 days for hypercortisolism due to Cushing’s disease 8 years before
pregnancy. She delivered a normal female baby.
In 1989, Leiba et al (14) reported a case of a 30-year-old
woman treated with mitotane 1.5– 4 g/d (1.5 g during
month 1 of pregnancy). Mitotane was stopped on week 4,
and the pregnancy was terminated on week 6. Histopathological examination of the embryo revealed a dysmorpho-
TABLE 2. Mitotane Treatment Before or During Pregnancy: Summary of Published Case Reports
Authors
Year of
Publication
Patient’s
Age
Luton et al (12)
1973
ND
CD
Leiba et al (13)
1978
38
CD
5 g/d
ND
Continued throughout
pregnancy
8 y before pregnancy
Leiba et al (14)
1989
30
CD
1.5 g/d
ND
4 wk gestation
Gerl et al (15)
1992
28
CD
1–1.5 g/d
3.9 – 4.7 mg/L
34 wk gestation
Baszko-Blaszyk
et al (16)
2011
28
ACC
ND
12.5 mg/L on
conception
Kojori et al (17)
2011
28
ACC
1 g/d
Current case
2012
33
ACC
1.5 g/d
Diagnosis
Mitotane
Dose
Blood Level
Monitoring
During
Pregnancy
ND
ND
Timing of Mitotane
Cessation
Fetal Outcome
Patient’s
Outcome
Normal infant
ND
Normal female
infant
Pregnancy
termination on
wk 6
Healthy male
infant on wk
38
ND
Continued
Spontaneous
abortion on wk
10, twins
ND
Continued throughout
pregnancy
9.8 – 4.2 mg/L
6 wk gestation
Premature delivery
on wk 31 due
to maternal
HELLP
syndrome, no
evidence of AI
Pregnancy
termination on
wk 21 due to
dramatic ACC
recurrence
6 mo later,
no
evidence
of ACC
ACC recurred
shortly
after
delivery
Additional
Information
ND
Pycnotic sympathoblasts
in cortical primordia
ND
Cord blood mitotane
1.4 mg/L, equal to
maternal blood at
birth
Passed away
6 mo later
Normal child’s growth
and development at
1 y follow-up
Visualization of fetal
adrenal on US,
morphologically
normal fetus,
mitotane ⬍1 mg/L in
cord blood or AF
Abbreviations: CD, Cushing’s disease; ND, no details; HELLP, hemolytic anemia, elevated liver enzymes, and low platelet count; AI, adrenal
insufficiency; AF, amniotic fluid.
The Endocrine Society. Downloaded from press.endocrine.org by [${individualUser.displayName}] on 11 June 2014. at 14:43 For personal use only. No other uses without permission. . All rights reserved.
446
Tripto-Shkolnik et al
Pregnancy on Mitotane Treatment
genic event in the cortical primordia characterized by pycnotic sympathoblasts.
Among the very few references mentioning mitotane
treatment during pregnancy in more detail is a German
publication by Gerl et al (15) reporting a case of a 28year-old woman with Cushing’s syndrome treated by 1.5
g/d for 18 months before pregnancy. Dose was reduced to
1 g/d during pregnancy. Mitotane blood levels were 3.9 –
4.7 mg/L. Mitotane was stopped at 34 weeks, and delivery
was at 38 weeks. Cord blood mitotane concentration at
birth was 1.4 mg/L— equal to maternal blood level.
This patient delivered a healthy baby boy. The newborn’s ACTH measured 3 hours postpartum was 1533
pg/ml (10 times higher than normal), yet the baby’s blood
cortisol was normal (15).
The two most recent reports, and the only two discussing patients with ACC, were published in 2011 by Polish
(16) and Canadian (17) groups. In the report by BaszkoBłaszyk et al (16), a 27-year-old patient with a virilizing
adrenal carcinoma was treated with surgical excision in
2008 and subsequently with mitotane. The patient conceived twins while on mitotane, with a blood level of 12.5
mg/L. On week 10 gestation, spontaneous abortion occurred (16). Kojori et al (17) presented a patient of the
same age with ACC who became pregnant while treated
with mitotane and hydrocortisone replacement. She was
switched to dexamethasone on gestation week 17. Mitotane blood level monitoring was not reported. On the 29th
week, US demonstrated normal fetal growth but suggested
hypoplastic adrenal glands. Despite that, the baby had
intact adrenal function at birth and was growing and developing normally at 1-year follow-up (17).
It is important to note that the mother presented with
disease recurrence shortly after birth.
Our report contributes several discussion points, bearing in mind natural limitations since it is only based on one
case.
First, mitotane treatment at a dose achieving nearly
therapeutic blood level did not interfere with normal ovulatory gonadal function in our patient and her ability to
conceive. Second, although mitotane treatment was discontinued at gestation week 6, the blood concentration of
the drug continued to be measurable (Table 1). Despite
this, the fetus developed normally, including morphologically normal adrenals, viewed by sonography (Figure 1).
Previous experience supports the ability of high resolution
US to accurately diagnose adrenal pathology such as agenesia, tumors, hypoplasia, hyperplasia, and gross morphological abnormalities (18). It should be highlighted that
the pregnancy was terminated at week 21; thus, fetal
anomaly that might have occurred later cannot be excluded. Third, the patient received hydrocortisone sup-
J Clin Endocrinol Metab, February 2013, 98(2):443– 447
plementation, a substrate to placental inactivation by 11hydroxysteroid dehydrogenase. Thus, if mitotane had
caused fetal hypoadrenalism, and since the fetus did not
“receive” glucocorticoid replacement, one could expect
intrauterine growth retardation. This, however, was not
evident.
Fourth, fetal cord blood and amniotic fluid drug levels
were undetectable, whereas the patient’s blood concentration was between 4 and 6 mg/L, further supporting the
assumption that the placental transfer may be less than
expected from the compound’s chemical properties. The
lower detection limit of the assay is 1 mg/L, far below the
patient’s blood level at the time. Since fat serves as a reservoir for mitotane accumulation, it might have been useful to examine the drug presence in fetal fat tissue, but that
was not performed.
Fifth, the disease recurred drastically during pregnancy
in our patient. Pregnancy itself and mitotane withdrawal
could have been implicated as possible accelerators.
Thus, both the Canadian patient who experienced ACC
recurrence shortly after giving birth (despite being treated
with mitotane throughout the pregnancy) (17) and our
patient whose outcome was so grave should lead to the
conclusion that feasibility of pregnancy in an ACC patient
needs to be seriously weighed against the possible negative
effect on disease progression.
In summary, there are very few reports discussing pregnancy in patients on mitotane. This is a detailed case presentation of a patient with ACC who conceived while on
mitotane treatment and who maintained the pregnancy up
to week 21, with sonographic confirmation of a morphologically normal fetus, including intact adrenal glands visualization and no evidence of mitotane transfer to the
amniotic fluid and cord blood. However, we do not recommend, based on our case and the scant current literature, concluding that pregnancy is safe in women treated
with mitotane. Until further knowledge is available, effective contraception should be recommended to such patients, and pregnancy should be avoided.
Acknowledgments
This article is dedicated to D.S.P., a beautiful woman, a remarkable person, and an outstandingly courageous patient.
The authors thank Prof. David Schneider, Asaf Ha-Rofe
Medical Center, Sackler Faculty of Medicine, Tel Aviv University, for his help with the amniotic fluid and fetal cord blood
samples. We also thank Mrs. Ariela Ehrlich, MLS, for the revision and proofreading.
Address all correspondence and requests for reprints to: Liana
Tripto Shkolnik, MD, MMedSc, Diabetes and Endocrinology
The Endocrine Society. Downloaded from press.endocrine.org by [${individualUser.displayName}] on 11 June 2014. at 14:43 For personal use only. No other uses without permission. . All rights reserved.
J Clin Endocrinol Metab, February 2013, 98(2):443– 447
Unit, Hillel Yaffe Medical Center, POB 169, Hadera 38100,
Israel. E-mail: [email protected].
Disclosure Summary: The authors have nothing to disclose.
References
1. Fassnacht M, Terzolo M, Allolio B, et al. Combination chemotherapy in advanced adrenocortical carcinoma. N Engl J Med. 2012;
366:2189 –2197.
2. Jeruss JS, Woodruff TK. Preservation of fertility in patients with
cancer. N Engl J Med. 2009;360:902–911.
3. Blumenfeld Z, von Wolff M. GnRH-analogues and oral contraceptives for fertility preservation in women during chemotherapy. Hum
Reprod Update. 2008;14:543–552.
4. Allolio B, Fassnacht M. Clinical review: adrenocortical carcinoma:
clinical update. J Clin Endocrinol Metab. 2006;91:2027–2037.
5. Fassnacht M, Libe R, Kroiss M, Allolio B. Adrenocortical carcinoma: a clinician’s update. Nat Rev Endocrinol. 2011;7:323–335.
6. De Francia S, Ardito A, Daffara F, et al. Mitotane treatment for
adrenocortical carcinoma: an overview. Minerva Endocrinol. 2012;
37:9 –23.
7. Terzolo M, Angeli A, Fassnacht M, et al. Adjuvant mitotane treatment for adrenocortical carcinoma. N Engl J Med. 2007;356:2372–
2380.
8. Abiven-Lepage G, Coste J, Tissier F, et al. Adrenocortical carcinoma
and pregnancy: clinical and biological features and prognosis. Eur J
Endocrinol. 2010;163:793– 800.
9. Kotteas E, Ioachim E, Pavlidis N. A pregnant patient with adrenocortical carcinoma: case report. Onkologie. 2012;35:517–519.
jcem.endojournals.org
447
10. Homer L, Viatge M, Gayet FX, Laurent Y, Kerlan V. [Cushing
syndrome and pregnancy: a propos of a malignant adrenocortical
carcinoma]. Gynecol Obstet Fertil. 2012;40:e1– e4.
11. Foster W, Chan S, Platt L, Hughes C. Detection of endocrine disrupting chemicals in samples of second trimester human amniotic
fluid. J Clin Endocrinol Metab. 2000;85:2954 –2957.
12. Luton JP, Remy JM, Valcke JC, Laudat P, Bricaire H. [Recovery or
remission of Cushing’s disease following long term administration
of op’DDD in seventeen patients (author’s translation)]. Ann Endocrinol (Paris). 1973;34:351–376.
13. Leiba S, Kaufman H, Winkelsberg G, Bahary CM. Pregnancy in a
case of Nelson’s syndrome. Acta Obstet Gynecol Scand. 1978;57:
373–375.
14. Leiba S, Weinstein R, Shindel B, et al. The protracted effect of o,p’DDD in Cushing’s disease and its impact on adrenal morphogenesis
of young human embryo. Ann Endocrinol (Paris). 1989;50:49 –53.
15. Gerl H, Benecke R, Knappe G, Rohde W, Stahl F, Amendt P. Pregnancy and partus in Cushing’s disease treated with o,p’-DDD. Acta
Endocrinol (Copenh). 1992;126:133.
16. Baszko-Błaszyk D, Ochmańska K, Waśko R, Sowiński J. Pregnancy
in a patient with adrenocortical carcinoma during treatment with
mitotane—a case report. Endokrynol Pol. 2011;62:186 –188.
17. Kojori F, Cronin CM, Salamon E, Burym C, Sellers EA. Normal
adrenal function in an infant following a pregnancy complicated by
maternal adrenal cortical carcinoma and mitotane exposure. J Pediatr Endocrinol Metab. 2011;24:203–204.
18. Bronshtein M, Tzidony D, Dimant M, Hajos J, Jaeger M, Blumenfeld Z. Transvaginal ultrasonographic measurements of the fetal
adrenal glands at 12 to 17 weeks of gestation. Am J Obstet Gynecol.
1993;169:1205–1210.
Mark Your Calendar for the Reducing Health Disparities Summit,
March 22-23, 2013, Sheraton Baltimore Inner Harbor
www.endo-society.org
The Endocrine Society. Downloaded from press.endocrine.org by [${individualUser.displayName}] on 11 June 2014. at 14:43 For personal use only. No other uses without permission. . All rights reserved.









© Copyright 2026