
Methamphetamine Abuse
Methamphetamine Abuse
This course has been awarded
one (1.0) contact hour.
This course expires on January 24, 2015.
Copyright © 2006 by RN.com.
All Rights Reserved. Reproduction and distribution
of these materials are prohibited without the
express written authorization of RN.com.
First Published: January 10, 2006
Revised: January 10, 2009
Revised: January 24, 2012
Material protected by Copyright ©AMN Healthcare
Acknowledgements
RN.com acknowledges the valuable contributions of…
...Nadine Salmon, RN, BSN, IBCLC is the Clinical content Specialist for RN.com. Nadine earned her
BSN from the University of the Witwatersrand, Johannesburg, South Africa. She worked as a midwife
in Labor and Delivery, an RN in Postpartum units and Antenatal units, before moving to the United
Kingdom, where she worked as a Medical Surgical Nurse. After coming to the US in 1997, Nadine
worked in obstetrics and became a Board Certified Lactation Consultant. Nadine was the Clinical Pre
Placement Manager for the International Nurse Staffing division before joining RN.com. When not
writing courses and other educational materials, Nadine is currently pursuing her master’s degree in
Nursing Leadership.
…Susan Herzberger, RN, MSN, original course author.
Disclaimer
RN.com strives to keep its content fair and unbiased.
The author(s), planning committee, and reviewers have no conflicts of interest in relation to this
course. Conflict of Interest is defined as circumstances a conflict of interest that an individual may
have, which could possibly affect Education content about products or services of a commercial
interest with which he/she has a financial relationship.
There is no commercial support being used for this course. Participants are advised that the
accredited status of RN.com does not imply endorsement by the provider or ANCC of any commercial
products mentioned in this course.
There is no "off label" usage of drugs or products discussed in this course.
You may find that both generic and trade names are used in courses produced by RN.com. The use
of trade names does not indicate any preference of one trade named agent or company over another.
Trade names are provided to enhance recognition of agents described in the course.
Note: All dosages given are for adults unless otherwise stated. The information on medications
contained in this course is not meant to be prescriptive or all-encompassing. You are encouraged to
consult with physicians and pharmacists about all medication issues for your patients.
Purpose and Objectives
The purpose of Methamphetamine Abuse is to inform healthcare professionals about the acute and
chronic problems associated with methamphetamine abuse and to prepare them to intervene with
patients using methamphetamine.
After successful completion of this continuing education course, participants will be able to:
1. Describe the effects of methamphetamine.
2. Identify the populations most vulnerable to methamphetamine (meth) abuse.
3. List the hazards associated with clandestine meth labs.
4. Prepare a strategy to minimize the risk of meth-related violence.
5. Match interventions with meth-related medical emergencies.
6. State the prognosis for meth addicts in recovery.
Material protected by Copyright ©AMN Healthcare
Introduction
The expression “speed kills” comes from the 1960s and reflects the dangerous reputation of
methamphetamine at that time. Unfortunately, the majority of meth addicts did not live through that
time, so public awareness of the inherent dangers of this illicit drug requires persistent attention. In
this course, you will learn about the methamphetamine problem from several different perspectives.
You are likely to encounter patients with meth-related problems in all healthcare environments:
Emergency departments
Hospital wards
Primary care facilities
School health services
Pediatric clinics
Long-term facilities
Your “meth” patients may not be methamphetamine users, though. They may be first-responders to a
crisis, casualties of domestic exposure to meth, or meth laboratory clean-up crew members. Please
click on the glossary icon for a full list of slang words for methamphetamine.
Statistics
According to the National Institute on Drug Abuse [NIDA], (2011), approximately 13 million people 12
years and older have abused methamphetamine in their lifetimes. In 2010, approximately 353,000
were current users (NIDA, 2011).
A survey conducted in 2010 by the NIDA found that the abuse rate among 8th, 10th, and 12th
graders has declined significantly between 1999 and 2007, and remains unchanged since then.
Retrieved from NIDA, 2012
http://www.drugabuse.gov/publications/topics-in-brief/methamphetamine-addiction-progress-need-to-remain-vigilant
Abuse remains noteworthy in certain areas of the country with indicators suggesting particular
problems in Hawaii, the West Coast, and the Midwest.
After marijuana, methamphetamine and other amphetamine-type stimulants are the most widely used
Material protected by Copyright ©AMN Healthcare
illicit drugs worldwide (Urbina & Jones in Clark, 2008).
The potent addiction liability and destructive health and social consequences make the abuse
of methamphetamines particularly dangerous.
Methamphetamine Abuse
Methamphetamine is a psychostimulant used to treat attention-deficit disorder, narcolepsy, and
morbid obesity (Clark, 2008). It's also a Schedule II drug, meaning that it has a high potential for
abuse.
For many drug addicts, methamphetamine is the street drug of choice because it's less expensive
and has longer-lasting effects than crack cocaine (Clark, 2008). While cocaine is metabolized rapidly,
methamphetamine has a longer duration of action, producing extended euphoria.
Test Yourself:
Q: Substance abuse and __________ are strongly linked.
A: Mental Illness
Sources of Methamphetamine
Meth is easily available and affordable, compared to other illicit drugs. One hit of meth is about a
quarter of a gram and will cost a user about $25 (Frontline, 2012). However, the price of meth is
volatile, and depends on the drug's purity, the amount and where it is sold.
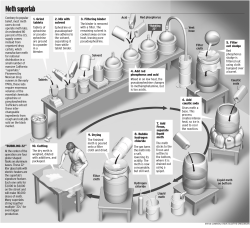
Illicit users of meth obtain the drug from imported sources or local clandestine labs. Local “mom &
pop” laboratories sprung up throughout the country when recipes for making meth out of OTC
ingredients became available over the Internet.
An epidemic began in the Midwest states and law enforcement systems became overburdened with
locating and seizing clandestine labs that increased tenfold in numbers over a decade (Markovich,
2005; ONDCP, 2004; NIDA, 2004b). People discovered that manufacturing meth is a lucrative
business that turns over a profit five to twenty times that of initial start-up costs. State legislative
efforts to control meth precursors such as pseudoephedrine and anhydrous ammonia are starting to
have a good effect now.
Law enforcers are now able to redirect their efforts to curb the Mexico-based drug trafficking
that provides the major supply of meth (ONDCP, 2005).
Test Yourself:
Q: Methamphetamine is manufactured using over the counter (OTC) medications such as:
A: A) Natamycin
B) Acetaminophen C) Pseudoephedrine D) Anhydrous chlorine
Material protected by Copyright ©AMN Healthcare
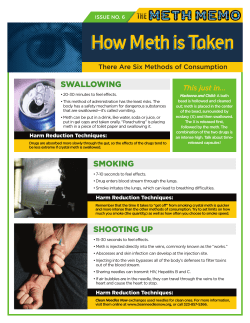
How Methamphetamine Is Used
Methamphetamine is a Schedule II narcotic that comes in 3 major forms:
Powder
Tablets
Chunks:Can be heated in a glass pipe and their fumes inhaled
Methamphetamine Powder.
Methamphetamine tablets.
Ice Meth chunks and pipe.
Images provided courtesy of the US DEA(Drug Enforcement Agency), 2012.
Meth can be smoked, snorted, injected, or ingested. Smoking is the most popular route among users
now (SAMHSA, 2005a).
Did You Know?
When methamphetamine is injected, the effects are usually felt within 3 to 5 minutes.
Action of Meth On The Brain
Methamphetamine acts by increasing the release of dopamine in the brain, which leads to feelings of
euphoria. However, this surge of pleasure is followed by a “crash” that often leads to repeated use of
the drug and eventually to difficulty feeling any pleasure at all, especially from natural rewards.
Long-term methamphetamine abuse also results in many damaging physical and psychiatric effects,
such as:
Addiction
Violent Behavior
Anxiety
Confusion
Insomnia
Psychotic symptoms (e.g. paranoia, hallucinations, delusions)
Cardiovascular problems (e.g. rapid heart rate, irregular heartbeat, increased blood pressure,
stroke)
(NIDA, 2012)
Patterns of Use
People take meth to feel euphoria and well-being, to increase their energy and stamina, to stay
awake, to be empowered, to lose weight, and to demonstrate assertiveness.
The onset of effect varies according to the route. The effects are felt within three to five minutes when
Material protected by Copyright ©AMN Healthcare
the meth is smoked, injected, or snorted. The effects from ingestion take 15 to 20 minutes. The
effects of meth last over twelve hours, compared to the effects of cocaine that last about half an hour.
Patterns of use among meth users vary widely. Some may use meth on occasion without becoming
dependent, and may still function normally within society. However, tolerance to meth builds quickly
and the extreme addictive potential of this drug makes almost all users vulnerable to its dangers.
Many meth users try to prevent a crash by taking just enough meth to stay functional. Others try to
recapture the initial euphoric rush they experienced the first time by bingeing on meth over several
days. The most intolerable time comes at the end of a binge, in a state called “tweaking.” Addicts feel
irritable, paranoid, and volatile (Markovich, 2005). This poses a danger for anyone attempting to
confront or curtail their actions.
Signs & Symptoms of Meth Abuse
These are some of the clinical signs and symptoms of methamphetamine abuse that you can assess:
Immediate Effects
↑ Heart rate and BP
↑ Body temperature
Hyper-vigilance
↑ Respirations
↓ Appetite
Poor impulse control
↑ Wakefulness
Tremors
Impaired judgment
↑ Physical activity
Egocentricity
Effects of Intoxication or Overdose
Dyspnea
Cardiac arrhythmias
Stroke
Tachycardia
Convulsions
Paranoia
Hyperthermia
Cardiovascular collapse
Aggressive behavior
Signs & Symptoms of Meth Intoxication
Since methamphetamines primarily affect the cardiovascular and central nervous
systems, the following signs and symptoms of meth intoxication can be observed below:
Insomnia
Tremors
Increased alertness
Loss of appetite
Hyperthermia
Increased body
movement / physical
Paranoia
Euphoria
activity
Tachycardia
Hallucinations
Restlessness
Hyperreflexia
(Clark 2008)
Presentation of a Meth High
Individuals who abuse methampetamines may not have outward physical signs, but those who do
can present with hypertension, tachycardia, tremors, and
Material protected by Copyright ©AMN Healthcare
weight loss (Gettig, Grady & Nowosadzka, 2006).
Individuals who chronically abuse meth usually have poor school and job performance, as well as
difficulties with interpersonal relationships.
Users may also experience:
Tremors
Agitation
Restlessness
Insomnia
Feelings of power, increased energy, aggression and alertness
(Gettig et al., 2006)
Excitement
Decreased appetite
Since methamphetamines have a very lengthy half-live, highs are generally intense and
lengthy (Gettig et al., 2006).
Presentation of a Meth Crash
Following a high, the user ultimately experiences an unpleasant "crash," which may last for a few
weeks (Gettig et al., 2006).
The withdrawal symptoms are essentially the opposite of what is experienced during the euphoric
stages of meth abuse.
Symptoms during the crash usually include:
Depression
Fatigue
Lack of energy
Hunger
Cravings for the drug
The combination of the high experience with the desire to avoid withdrawal
symptoms places addicts at risk for using the drug repeatedly, creating a vicious cycle of destruction
(Gettig et al., 2006).
Withdrawal Effects & Effects of Chronic Usage
Withdrawal Effects
Anxiety
Extreme frustration
Nightmares
Suicidal depression
Cognitive impairment
Insomnia followed by
hypersomnia
Agitated paranoia
Perceptual dullness
Dehydration + chills
Anhedonia (inability to
experience pleasure)
Fatigue
Effects of Chronic Usage
Weight loss
Rhabdomyolysis
Weakened immunity
Acute lead poisoning
Material protected by Copyright ©AMN Healthcare
Repetitive motor
activity
Violent speech and
behavior
Skin disorders + hair loss
Restlessness + irritability
Dental deterioration
Insomnia
Psychotic delusions
Long-Term Effects of Meth Abuse
As addiction to methamphetamine worsens, users develop tolerance to the drug. To achieve the
desired "high," depending on their personal sensitivity, they may need to increase the amount of meth
used or change the route of administration, and often embark on a "binge and crash" cycle (Gettig et
al., 2006). The lack of sleep and nourishment that accompanies such episodes can lead to paranoia,
psychosis, and unpredictable, violent, or risk-taking behavior.
Chronic meth abuse can also permanently alter brain chemistry, with resultant developement of
chronic psychiatric illnesses such as depression and schizophrenia is increased (Gettig et al., 2006).
Long-term abusers of meth may also develop insomnia and movement disorders Gulien, in Gettig et
al., 2006).
The most common complication of meth abuse is addiction, which has grave emotional, physical, and
financial complications (Hardman &t Limbird, in Gettig et al., 2006).
Methamphetamine-induced paranoia and hallucinations can lead to rage, domestic violence,
child abuse, murder, and suicide.
Neurological Damage
Methamphetamine targets the central nervous system (CNS) by stimulating the
release of dopamine and, in lesser amounts, norepinephrine and serotonin, and inhibits their reuptake
(Clark, 2008).
Dopamine is a neurotransmitter that causes CNS excitation. It elevates mood, creates feelings of
euphoria, and enhances body movement and reflexes. However, high doses of methamphetamine
damage nerve terminals in areas of the brain (Clark, 2008).
Life-threatening medical complications can occur with a dose of any size. Tachycardia, hypertension,
and increased metabolism commonly occur, but more serious effects, such as hyperthermia,
seizures, MI, stroke, and even death, are possible (Clark, 2008).
Brain abnormalities will show up on MRIs and PET scans that resemble those seen in dementia and
schizophrenia (Thompson, 2004).
Did You Know?
Even with meth abstinence, only partial reversal of the neurotoxic damage is expected, although
some symptoms may slowly resolve as the brain adapts and compensates for permanent deficits
(Wang, et al., 2004).
Material protected by Copyright ©AMN Healthcare
Changes In Body Image
Chronic methamphetamine abuse can have devastating physical as well as psychosocial
consequences.
Changes in body image occur not only from malnutrition and poor hygiene, but also from selfdestructive urges to purge the body of imagined "meth bugs". Methampphetamine abusers develop a
crawling sensation on their skin, as if a bug is tunneling under the skin. In response to this sensation,
user pick incessantly at the skin, causing skin wounds, infections, scabs, and scars (Clark, 2008).
Even though users may be aware that there is nothing on the skin, they will continue to scratch and
pick at the skin, and sometimes use needles, glass, or other sharp objects to "dig out," or get rid of,
the sensation (Clark, 2008). This practice may reduce the distress, but puts the user at risk for
disease, infection, and altered body image.
Chronic methamphetamine use also damages the teeth and gums, resulting in a condition commonly
referred to as "meth mouth." This is often caused by dental caries and periodontal disease that occur
as a result of poor oral hygiene, poor nutrition and xerostomia (dry mouth), caused by chronic
exposure to the chemicals that make up methamphetamines (Clark, 2008).
Meth abusers are also at increased risk for blast-related trauma, chemical and thermal burns, and
inhalation injury from exposure to the chemicals used in meth labs (Clark, 2008).
Image of a person with dermatillomania (also known as
pathologic skin picking), that results in skin sores due to
self-inflicted skin picking on arms, shoulders and chest.
Image provided by Wikipedia (2012) in the Public Domain.
This is a case of suspected meth mouth with a close-up
shot of the lower right posterior teeth. This patient was
treated at the University of Tennessee Health Science
Center: College of Dentistry in Memphis, TN. Image
provided by GNU Free Documentation License, 2012.
Intoxication & Overdose
Emergency department care for meth intoxication focuses on managing life-threatening
symptoms and/or psychotic behavior.
There is no antidote available for methamphetamine intoxication.
Supportive measures include:
Treat hyperthermia with cooling measures, such as an ice bath.
Take standard measures to control convulsions and cardiovascular events. Benzodiazepines
are sometimes used for extreme anxiety.
Short- term neuroleptics (anti-psychotics) and admission to a psychiatric department may be
needed for toxic psychosis.
Material protected by Copyright ©AMN Healthcare
This individual has the potential to become violent; do you observe any
potential weapons?
Yes. Her cell phone and the chair.
Management For Potential For Violence
The potential for violence to erupt in a meth-intoxicated, binging, or tweaking patient is something to
think about before you are in the midst of danger.
These are some ways to lower your risk of harm (DHHS, 2011):
Orient the patient by identifying yourself and your purpose
Call the patient by name
Take the patient to a quiet, spacious place with minimal stimuli
Remain non-confrontational
Acknowledge the patient’s agitation and distress
Remove potential weapons
Have a back-up plan for a team approach to managing any violence that may occur, if
necessary
Toxic Exposures
People exposed to toxic chemicals from a clandestine meth lab have symptoms of respiratory and
eye irritation, headache, dizziness, nausea and vomiting, and shortness of breath (ONDCP, 2005;
Markovich, 2005). A variety of chemicals may be used in the manufacturing of meth, including
corrosives, solvents, and respiratory irritants (Colorado Drug Endangered Children Organization,
2005). Ammonia or hydrogen chloride is a standard ingredient that presents a significant danger and
risk of fatality.
Possible damaging effects of ammonia & hydrogen chloride:
(Source: Agency for Toxic Substances and Disease Registry, 2004)
Material protected by Copyright ©AMN Healthcare
There is no antidote for these chemical exposures. Inducing emesis is not advised if the chemicals
have been ingested, but diluting stomach contents with water or milk may be helpful.
Once the patients have been decontaminated with a total body and hair washing and the eyes
irrigated, treatment is supporting of basic respiratory and cardiovascular functions.
Thermal Burns
The chemicals used to make meth are highly volatile, and patients arriving from a meth lab may also
have thermal burns from an explosion.
Whether the burns are caused by flames or chemicals or a combination of these, you will need to
evaluate what percentage of the body is burned and identify the depth or degree of the burns.
Document your findings on a body map. If over 30% of the total body surface area is burned, expect a
systemic inflammatory response.
Test Yourself:
Q: If over _____ of the total body surface area is burned, expect a systemic inflammatory response.
A: 30%
Children Removed From Meth Lab Sites
Adults without symptoms who are involved in a meth lab seizure will not show up for medical care but
all children removed from the situation will require a complete medical evaluation within 24 hours
(CDEC, 2005). Children are at greater risk for toxicity than adults because of a proportionately larger
lung surface area and closer proximity to the ground where vapors tend to collect (ATSDR, 2004).
You might think that a pungent, disagreeable odor would naturally keep children from wandering into
a dangerous environment, but olfactory fatigue occurs when the chemical exposure is prolonged,
dismantling the natural protective sense.
Evaluate children for effects of recent chemical exposure as well as for CNS depression due to
chronic exposure to chemicals. Some may have a strong odor resembling cat urine, associated with
meth production (Markovich, 2005). Note any signs and symptoms of child abuse, such as
emaciation, lack of grooming and hygiene, noticeable fatigue, bruises or injuries, and odd behavior.
Some studies show that over half of the children removed from meth labs test positive for meth
(CDEC, 2005). In some states you will be asked to collect a urine drug specimen for the purpose of
assisting with prosecution.
Treatment
Currently, the most effective treatments for methamphetamine addiction are comprehensive
cognitive-behavioral interventions. An example of such an intervention is the use of the Matrix Model,
which is a behavioral treatment approach that combines behavioral therapy, family education,
individual counseling, 12-step support, drug testing, and encouragement for non drug-related
activities.
Contingency management interventions, which provide tangible incentives in exchange for engaging
in treatment and maintaining abstinence, have also been shown to be effective (NIDA, 2010).
Material protected by Copyright ©AMN Healthcare
There are no medications at this time approved to treat methamphetamine addiction; however, this is
an active area of research for NIDA (NIDA, 2010).
The combination of predictable relapses and harsh setbacks in achieving treatment goals
explains the resistance meth addicts have to entering treatment.
Prevention & Screening
Some ways you can work preventatively to reduce the methamphetamine problem are:
Routinely screening your patients for substance use
Enhancing your awareness of vulnerable populations
Educating patients and the public about meth
Supporting those legislative efforts proven to work
Screening for substance abuse should be as routine as asking about prescription medications. It can
be as direct and simple as an adapted version of the CAGE questionnaire (See Appendix One):
Have you ever felt the need to cut down on your alcohol or drug habits?
Are you annoyed by criticism from others over these habits?
Have you ever felt bad about this issue?
Have you ever had to have an alcohol or drug fix in the morning?
Prevention & Screening
Screening for substance use should not be done when patients are obviously under the influence of
alcohol or drugs. If the patient is “under the influence” expect poly-drug use, asking about specific
daily amounts being used and the last time they were used.
Using street terms and expressing a nonjudgmental attitude may increase the patient’s willingness to
disclose information. Tests for screening of specific substances may be useful for planning treatment
but if blood alcohol levels and urine drug screens are done, obtain the patient consent first (National
Guidelines Clearinghouse, 2005).
Vulnerable People
People who fall into a high-risk category for meth abuse are identified by demographic statistics and
constitutional vulnerability. Demographic groups at risk are:
Young adults between 20 and 30
People whose occupations require physical stamina
People trying to lose weight
People wanting to enhance their physical, mental, or sexual performance
Those with a constitutional vulnerability suffer from chronic depression, low energy, and low
self-esteem. For them, the first experience of what they consider well-being may have come with their
first use of meth. They cannot recapture that experience because repeated usage is less and less
satisfying, but the addiction to trying is extremely powerful.
Material protected by Copyright ©AMN Healthcare
Test Yourself:
Q: People who fall into a high-risk category for meth abuse are sometimes identified by:
A: A) Class B) Income C) Ethnicity D) Demographic statistics
Patient Education
Your efforts to teach patients and the public about meth can make a measurable difference. Since
1999, public education campaigns actively confronting the meth problem have produced a decline in
meth use among youth (University of Michigan, 2004).
Parents today tend to underestimate the presence and influence of drugs in their adolescents’ lives
though (Partnership for a Drug-Free America, 2005). This points to a need for more parental
education.
Research shows that decreasing usage of a particular drug is directly connected to how widely that
drug is perceived to be dangerous (NIDA, 2004a). Research also shows that public memory of a
drug’s dangers fades over the decades. As a nurse, you can be alert to the public’s need for
information.
Test Yourself:
Q:What are the warning signs of a Clandestine Meth Lab?
A: A strong, pungent odor of solvents, ammonia, or ether; a residence with blacked-out windows; a lot
of night activity; excessive trash (Source: Division of Narcotics Enforcement, Iowa Department of
Public Safety, 2005.)
Conclusion
Among the many illicit drugs in circulation, methamphetamine is especially threatening to health. This
is because of meth’s powerful addictive potential and the extreme neurological consequences.
Meth addiction not only blocks enjoyment of life but tragically steals years of normal productivity from
many people in their first decade of adulthood.
Having studied the problem, you will be ready to intervene against these odds as you work with
patients who have abused methamphetamines.
Appendix One: The CAGE Questionnaire
The CAGE questionnaire, the name of which is an acronym of its four questions, is a widely used
method of screening for alcoholism.
It is not valid for diagnosis of other substance use disorders, although somewhat modified versions of
the CAGE are frequently implemented for such a purpose.
Two or more “yes” responses indicate that further evaluation is needed.
Material protected by Copyright ©AMN Healthcare
Scoring: Responses on the CAGE are scored 0 for "no" and 1 for "yes," with a higher score an
indication of alcohol problems. A total score of 2 or greater is considered clinically significant.
Source: Ewing, J. A. (1984). Detecting alcoholism: The CAGE Questionnaire. Journal of the American Medical Association, 252,
1905–1907.
Glossary of Terms
Bathtub crank: poor quality methamphetamine; methamphetamine produced in bathtubs
Beannies: methamphetamine
Bikers coffee: methamphetamine and coffee
Black beauty: methamphetamine
Blade: crystal methamphetamine
Blue devils: methamphetamine
Box labs: small, mobile, clandestine labs used to produce methamphetamine
Brown: marijuana; heroin; methamphetamine
Chalk: Crack Cocaine; amphetamine; methamphetamine
Christmas tree meth: green methamphetamine produced using Drano crystals
Chrome: crystal methamphetamine
Cinnamon: methamphetamine
Cook: drug manufacturer; mix heroin with water; heating heroin to prepare it for injection
Cooker: to inject a drug; person who manufactures methamphetamine
CR: methamphetamine
Crank: Crack Cocaine; heroin; amphetamine; methamphetamine; methcathinone
Crankster: someone who uses or manufactures methamphetamine
Crink: Methamphetamine
Cristina (Spanish): methamphetamine
Material protected by Copyright ©AMN Healthcare
Croak: crack mixed with methamphetamine; methamphetamine
Crossles: methamphetamine
Crush and rush: method of methamphetamine production in which starch is not filtered out of the ephedrine
or pseudoephedrine tablets.
Crypto: methamphetamine
Crystal glass: crystal shards of methamphetamine
Crystal meth: methamphetamine
Crystal: Cocaine; amphetamine; methamphetamine; PCP
Desogtion: methamphetamine
Dropping: wrapping methamphetamine in bread and then consuming it
Elbows: one pound of methamphetamine
Fast: methamphetamine
Fire: Crack and methamphetamine; to inject a drug
Five-way: combines snorting of heroin, cocaine, methamphetamine, ground up flunitrazepam pills, and
drinking alcohol
Geep: methamphetamine
Geeter: methamphetamine
Getgo: methamphetamine
Getting glassed: to snort methamphetamine
Glass: heroin; amphetamine; hypodermic needle; methamphetamine
Go-fast: methcathinone; crank; methamphetamine
Half elbows: pound of methamphetamine
Hiropon: smokable methamphetamine
Holiday meth: green methamphetamine produced using Drano crystals
Hot Ice: smokable methamphetamine
Hot rolling: liquefying methamphetamine in an eye dropper and then inhaling it
Hotrailing: to heat methamphetamine and inhale the vapor through nose using a plastic tube
Hugs and Kisses: combination of methamphetamine and methylenedioxymethamphetamine (MDMA)
Ice: cocaine; crack cocaine; smokable methamphetamine; methamphetamine;
methylenedioxymethamphetamine (MDMA); phencyclidine (PCP)
Jet fuel: PCP; methamphetamine; methamphetamine combined with PCP (phencyclidine)
L.A. glass: smokable methamphetamine
L.A. ice: smokable methamphetamine
Lemon drop: methamphetamine with a dull yellow tint
Load of Laundry: Methamphetamine
Maui-wowie: marijuana; methamphetamine
Meth head: methamphetamine regular user
Meth monster: one who has a violent reaction to methamphetamine
Meth speed ball: methamphetamine combined with heroin
Meth: Methamphetamine
Mexican crack: methamphetamine with the appearance of crack; methamphetamine
Mexican speedballs: crack and methamphetamine
Nazimeth: methamphetamine
OZs: methamphetamine
P and P: methamphetamine used in combination with MDMA (methylenedioxymethamphetamine) and Viagra
Material protected by Copyright ©AMN Healthcare
Paper: a dosage unit of heroin; one-tenth of a gram or less of the drug ice or methamphetamine
Party and play: methamphetamine used in combination with MDMA (methylenedioxymethamphetamine) and
Viagra
Pink elephants: methamphetamine
Pink hearts: amphetamine; methamphetamine
Pink: methamphetamine
Po coke: methamphetamine
Poor man's coke: methamphetamine
Quill: cocaine; heroin; methamphetamine
Red: under the influence of drugs; methamphetamine
Redneck cocaine: methamphetamine
Rock: methamphetamine
Shabu: combination of powder cocaine and methamphetamine; crack cocaine; methamphetamine;
methylenedioxymethamphetamine (MDMA)
Sketch: methamphetamine
Soap dope: methamphetamine with a pinkish tint
Spackle: methamphetamine
Sparkle: methamphetamine that has a somewhat shiny appearance
Speed freak: habitual user of methamphetamine
Speed: Crack Cocaine; amphetamine; methamphetamine
Speedballing: to shoot up or smoke a mixture of cocaine and heroin; ecstasy mixed with ketamine; the
simultaneous use of a stimulant with a depressant
Spoosh: methamphetamine
Stove top: crystal methamphetamine; methamphetamine
Super ice: smokable methamphetamine
The five way: heroin plus cocaine plus methamphetamine plus Rohypnol (flunitrazepam) plus alcohol
Tic: PCP in powder form; methamphetamine
Tina: methamphetamine; crystal methamphetamine; methamphetamine used with Viagra
Trash: methamphetamine
Tweek: methamphetamine-like substance
Twisters: Crack and methamphetamine
Wash: methamphetamine
Water: blunts; methamphetamine; PCP; a mixture of marijuana and other substances within a cigar; Gamma
hydroxybutyrate (GHB)
Wet: blunts mixed with marijuana and PCP; methamphetamine; marijuana cigarettes soaked in PCP
("embalming fluid") and dried
White Cross: amphetamine; methamphetamine
Working man's cocaine: methamphetamine
Ya Ba: a pure and powerful form of methamphetamine from Thailand; "crazy drug"
Yellow bam: methamphetamine
Yellow jackets: depressants; methamphetamine
References
Agency for Toxic Substances and Disease Registry (ATSDR). (2004). Medical management guidelines. Retrieved
10/08/05, from http://www.atsdr.cdc.gov/
Material protected by Copyright ©AMN Healthcare
Clark, J. (2008). The Danger Next Door: Methamphetamine. RN Web.com.
Colorado Drug Endangered Children (CDEC) Organization (2005). Clandestine methamphetamine labs frequently asked
questions. Retrieved 10/08/05, from http://www.colodec.org.
Department of Health & Human Services (DHHS), (2011). Treatment of stimulant use disorders. Quick guide for clinicians.
Based on TIP 33. Publication SMA 01-3598.
Division of Narcotics Enforcement. Iowa Department of Public Safety. (2005). Clandestine laboratories. Retrieved
10/06/05, from http://www.dps.state.ia.us/DNE/clanlab.shtml
Frontline (2012). The Meth Epidemic: Frequently Asked Questions. Retrieved January 4, 2012
from:http://www.pbs.org/wgbh/pages/frontline/meth/faqs/#12
Gettig, J., Grady, S. & Nowasadzka, I. (2006). Methamphetamines: Putting The Brakes On Speed. The Journal of School
Nursing, 22(2), p. 66-73.
Herzberger, S. (2005). Meth addiction. Advance for Nurses. Retrieved 10/05/05, from http://www.advanceweb.com.
Markovich, K. (2005). Methamphetamine abuse. Advance for Nurse Practitioners. Retrieved 4/03/05, from
http://nurse-practitioners.advanceweb.com.
National Guidelines Clearinghouse. (2005). Screening and ongoing assessment for substance use. Retrieved 10/06/05,
from http://www.hivguidelines.org.
National Institute on Drug Abuse [NIDA], 2010. Info Facts: Methamphetamine Abuse.Retrieved January 4, 2012 from:
http://www.drugabuse.gov/publications/infofacts/methamphetamine
NIDA. (2004a). Monitoring the Future: National results on adolescent drug use. Retrieved 7/12/05, from
http://www.monitoringthefuture.org.
NIDA. (2004b). NIDA InfoFacts: Methamphetamine. Retrieved 7/23/05, from http://www.nida.nih.gov.
Partnership for a Drug-Free America. (2005). Partnership Attitude Tracking Study 2004. Retrieved 7/12/05, from
http://www.drugfree.org.
Substance Abuse and Mental Health Services Administration [SAMHSA], (2005a). Smoked
methamphetamine/amphetamines: 1992-2002. The DASIS Report, January 7. 2005.
SAMHSA. (2005b). Youth drug use continues to decline. Retrieved 9/14/05, from http://www.samhsa.gov.
Thompson, P. (2004). Structural abnormalities in the brains of human subjects who use methamphetamine. The Journal
of Neuroscience, 24(26): 6028-6036.
United States Drug Enforcement Administration (DEA), 2012. Methamphetamine Images. Retrieved January 4, 2012
from: http://www.justice.gov/dea/images_methamphetamine.html
University of Michigan. (2004). Overall teen drug use continues gradual decline; but use of inhalants rises. Retrieved
7/12/05, from http://www.monitoringthefuture.org.
Wang, G. et al. (2004). Partial recovery of brain metabolism in methamphetamine abusers after protracted abstinence.
American Journal of Psychiatry, 161(2): 242-248.
At the time this course was constructed all URL's in the reference list were current and accessible. RN.com is
committed to providing healthcare professionals with the most up to date information available.
© Copyright 2006, AMN Healthcare, Inc.
Please Read:
This publication is intended solely for the use of healthcare professionals taking this course, for credit, from RN.com. It is
Material protected by Copyright ©AMN Healthcare
designed to assist healthcare professionals, including nurses, in addressing many issues associated with healthcare. The
guidance provided in this publication is general in nature, and is not designed to address any specific situation. This
publication in no way absolves facilities of their responsibility for the appropriate orientation of healthcare professionals.
Hospitals or other organizations using this publication as a part of their own orientation processes should review the
contents of this publication to ensure accuracy and compliance before using this publication. Hospitals and facilities that
use this publication agree to defend and indemnify, and shall hold RN.com, including its parent(s), subsidiaries, affiliates,
officers/directors, and employees from liability resulting from the use of this publication. The contents of this publication
may not be reproduced without written permission from RN.com.
Material protected by Copyright ©AMN Healthcare








© Copyright 2026