
Polymorphous Light Eruption
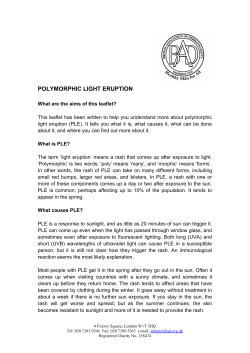
Polymorphous Light Eruption Erhard Holzle, M.D., Gerd Plewig, M.D., Renate von Kries, M.D., Percy Lehmann, M.D. Department of Dermatology, University of Diisseldorf, Diisseldorf, F. R. G. Polymorphous light eruption (PLE) is a common photo dermatosis of unknown etiology. It affiicts mainly fair skinned patients, with a preponderance of young females. There is, however, no absolute restriction as to age, sex, or race. Clinical variants include the papular, vesiculo-bullous, and hemorrhagic variety, as well as plaque, erythema mul tiforme-like, and insect bite (strophulus)-like types. Skin lesions appear only in certain exposed areas hours or a few days after intense sunshine, and are nearly always mono morphous in the same patient. The rash subsides sponta neously within several days without leaving scars. The histopathologic picture is characteristic and shows a perivascular lymphocytic inftltrate in the upper and mid dle corium with subepidermal edema, vacuolization of basal cells, and spongiosis in the lower epidermis. The most important differential diagnoses are solar urticaria, pho tosensitive erythema multiforme, and lupus erythemato sus. The action spectrum of PLE is under debate. Repro duction of skin lesions has been reported with UVB, UVA, and, rarely, visible light, with UVA probably being the most effective part of the spectrum. More important than treatment of PLE is prophylaxis. UVA- and UVB-effective sunscreens are of some help. Phototherapy and especially photochemotherapy (psoralen + UVA; PUVA) offer effective ways to decrease light sensitivity. Systemic treatment with chloroquine or f3-car otene has been disappointing. ] Invest Dermatol 88:325-385, t was recognized in the early 19th century that certain ecze matous reactions were caused by sunlight. Willan [1] was the first to use the term "eczema solare." In 1879 Sir Jonathan Hutchinson [2] presented 14 patients under the diagnosis "summer prurigo. " There is reason to believe that "prurigo aestivalis," "prurigo adolescentium," and "acne prurigo" syn onymously designated similar sun-induced skin disorders. Rasch, in 1900 [3], simplified the terminology by introducing the term "polymorphous light eruption (PLE). " This designation was widely accepted to characterize urticarial, papular, vesicular, and ecze matous reactions precipitated by light [4]; however, it did not clarify the nosology of photodermatoses. A variety of sunlight-evoked eruptions, such as solar urticaria, hydroa vacciniforme, porphyrias, photoallergic dermatitis, pho tosensitive erythema multiforme, and lupus erythematosus (LE) fell under this diagnosis. It was only during the past decades that these differential diagnoses have been separated and polymor phous light eruption has been defmed as a clinical entity [5-8). Until now, however, it remains difficult, if not impossible, to distinguish in certain patients between polymorphous light erup tion and light-induced subacute or discoid cutaneous lupus ery thematosus, or photosensitive erythema multiforme. This review describes the growing knowledge about PLE. We put forward our concept of the disease as a distinct entity with several morphologic variants. O ur experience is based on obser vations in more than 250 patients in the years from 1977 to 1985 [8-11). 1987 I CLINICAL FEATURES Polymorphous light eruption is a very common photodermatosis, but the true prevalence among the population is not known. In a survey of 271 apparently healthy subjects, 10% gave a history consistent with PLE [12]. Many persons are aware of a transient "sun allergy" but never visit a dermatologist because they know how to manage the problem by themselves. Individual suscep tibility varies greatly, and only the most severely afflicted patients are seen by physicians. In many patients, PLE appears during the first days of vacationing on the beach or in high altitudes. When the patient returns home the eruption has resolved spontaneously and the pliysician who is asked for help can only conceive a diagnosis by the patient's history. Polymorphous light eruption seems to occur most frequently among fair-skinned populations. Large series are reported from Scandinavian countries [13,14], but the eruption is not confmed to a certain race or skin color [7]. It has been reported in Blacks, O rientals, and in Native North and Latin Americans [15,16]. Among the latter, the familial occurrence is a characteristic fea ture. This peculiar photodermatosis might represent an entity different from PLE observed in whites [17]. Inheritance in an autosomal-dominant mode with a reduced penetrance has been reported in 56% of patients evaluated in Finland [18] and in 75% of Canadian Inuit patients [19]. In other series, genetic predis position ranged from 3-45%. Jansen [18] suggested that patients in other reports might not have been questioned as thoroughly and, therefore, genetic predisposition in general might be under estimated. There is agreement that the time of onset is most commonly during the early adult life [7,13], but the eruption may also start in childhood. In children the face and ears frequently are involved. Similar cases have been described under the designation ''juvenile Reprint requests to: Prof. Dr. E. Holzle, Universitatshautklinik, Moor enstr. 5, D-4000 Diisseldorf 1, F.R.G. Abbreviations: DLE: discoid lupus erythematosus LE: lupus erythematosus MED: minimal erythemal dose PLE: polymorphous light eruption PUVA: photochemotherapy (psoralen + UVA) SCLE: subacute cutaneous lupus erythematosus UVA: ultraviolet A UVB: ultraviolet B 0022-202X/87/S03.50 Copyright © 1987 by The Society for Investigative Dermatology, Inc. 32s VOL. 88, NO. 3 MARCH SUPPLEMENT POLYMORPHOUS LIGHT ERUPTION 1987 spring eruption" [20,21], which is probably part of the PLE spec trum. Actinic prurigo [22,23], however, is in our view a separate disorder that bears resemblance to the hereditary variant of PLE among North, Central, and South American Natives (18,24]. Features that distinguish these disorders from PLE are involve ment of non-sun-exposed areas, lack of complete clearing during the winter season, and presence of chronic eczematous lesions. In our experience, 90% of PLE patients are women. This is in accordance with the findings of Clorius and Jung [6] and Jansen [13]. Others have found a preponderance of men [25,26] or an equal sex distribution [27,28]. The reason that, in some studies, women are more commonly afflicted is not well understood. It is possible diat the preponderance of females does not reflect the true prevalence, which might be equal, but rather might reflect a higher rate of reporting of the rash by women. Lesions of PLE are confined to sun-exposed body sites. In contrast to others [5,7,13] we have neither observed lesions on areas covered by clothing nor a tendency of the eruption to gen eralize. In our experience, PLE is confined to certain sites of predilection even when large areas are sun-exposed. In order of decreasing frequency of involvement, these sites are: V-neck, dorsal forearm and back of hands, upper arms, face, shoulders, thighs, and lower legs. Variations among different patients occur. In exquisitely sensitive individuals larger parts of the trunk are involved, too. Jansen [13] notes that lips and eyes are frequently involved, and reports that patients experience general symptoms, like chills, headache, fever, and nausea after sun exposure. The reaction is of a delayed type. Lesions appear from several hours to a few days after intense sun exposure. A characteristic sequence of events is reported by most patients, and the dynamics ofthe lesions can be observed when PLE is experimentally evoked by phototesting. Itching occurs first; it is followed by patchy erythema. Finally, distinct lesions emerge, which may coalesce. The sequence from itchy, patchy erythema to sparsely distributed and then densely aggregated skin lesions requires increasing amounts ofradiation energy. Lesions are present for hours or several days and resolve spontaneously without residues when further sun exposure is avoided. Scaling, hyperkeratosis, lichenification, or scarring are not primary lesions in PLE. These changes may occur secondarily due to rubbing or scratching and prolonged sun ex posure. Also the clinical picture might be altered by a concomitant sunburn reaction. The majority of patients experience seasonal recurrences over many years, with decreasing sensitivity after repeated sun exposures. Finally, the problem may resolve spon taneously after many years [13,29]. Many patients experience the elicitation of skin lesions by sun light through window glass, e.g., in airplanes, cars, and trains. This was already observed by early authors [25] and indicates that the action spectrum is not confined to sunburn radiation. MORPHOLOGIC VARIANTS Most authors agree that there are different morphologic variants, with the papular variety being the dominant type [13,28,30]. Lamb et al [31] and Epstein [32,33] in their series distinguished plaque, prurigo-like, and erythema multiforme-like types from the papular, eczematous, and erythematous variety. The latter was designated erythema solare perstans. In his review [7] Epstein refers to small papules, large papules that may coalesce and form plaques, papulovesicular lesions, erythema multiforme-like le sions, prurigo-like nodules, and an eczematous response that may become secondarily lichenified by rubbing and scratching. Re cently, a vesiculobullous variant of PLE was described [34,35]. In our view, diffuse erythematous response, eczematous re actions, and prurigo-like nodules are not part of the PLE spec trum. These lesions characterize separate light-induced disorders, which comprise differential diagnoses of PLE. Widespread diffuse erythema following sun exposure might occur in systemic LE or in the presence of a phototoxic photosensitizer. Eczema in ex posed areas is a feature of photoallergy, photosensitive eczema, persistent light reaction, light-aggravated atopic eczema, or air- 33$ borne contact dermatitis. Prurigo associated with sun exposure might by seen in actinic prurigo, which represents an entity sep arate from PLE. The reason we do not observe eczematous lesions in our patients might be the lack of chronic exposure to high intensity solar radiation. In the F. R. G. the summer season is short and longer periods of sunny weather conditions are rare. In our patients [8,11] the papular type, along with the hem orrhagic and insect bite (strophulus)-like varieties, the plaque type, the vesiculobullous type, and an erythema multiforme-like type make up the spectrum of PLE. We do not share the opinion that the clinical picture might be polymorphous in the same in dividual [5,6] or that combination or transition between the var ious types might occur [7]. In our series skin lesions were mon omorphous in any one patient. Papular Type It is the most common type of PLE. Small papules or papulovesicles are disseminated or densely aggregated on a patchy erythema (Figs lA,2A). Hemorrhagic Type rhagic. Rarely, the papular lesions are hemor Insect bite (Strophulus)-like Type This is a peculiar, rare variety of the papular type. The lesions are few, scattered, and consist of small urticarial papules topped by a tiny vesicle. Plaque Type This is the second most common variety in our patients. It occurs frequently on the face [7] and resembles sub acute cutaneous lupus erythematosus (SCLE), with its sharply demarcated, erythematous, elevated, often urticarial plaques. Erythema Multiforme-like Type sions and occurs less frequently. It shows typical target le Vesiculobullous Type It consists of tense vesicles and small bullae on an erythematous base. It seems to be frequent among North American women vacationing to Hawaii [34]. In Europe it is very rarely observed [35]. HISTO PATHOLOGY AND IMMUNOHISTO PATHOLOGY In 1960 Wright and Winer [36] gave a description of the histo pathologic pattern seen in PLE that has gained wide acceptance. They found parakeratosis, subepidermal edema, vascular dilata tion, and lymphocytic infiltration. Sometimes acanthosis, liq uefaction degeneration of the basal layer, and diminished elastic fibers were observed. McGrae and Perry [5] stressed the similar ities to lymphocytic infiltration Jessner. Lamb et al [26], as well as Lever and Schaumburg-Lever [37] distinguished the plaque type of PLE from LE by absence of vacuolar alteration of basal cells, a view that did not hold true [7,8,38]. The main features characteristic for PLE are observed in the common papular type [7,8]. In other morphologic variants, this basic pattern is also prominent, but certain features might be pronounced or addi tional features superimposed. The pattern of PLE, seen in the papular type, shows a superficial and deep perivascular lymphocytic infiltrate with an interstitial component in the upper dermis. There are subepidermal edema and vacuolization of basal cells, exocytosis of lymphocytes, and focal spongiosis. Sunburn cells are notably absent or sparse (Figs lB,2B). In the plaque type the infiltrate tends to be lichenoid, subepi dermal edema is pronounced, and spongiosis is widespread, in volving the lower epidermis. The erythema multiforme-like type exhibits a prominent su bepidermal edema sometimes forming a blister, and few extra vasated erythrocytes. Epidermal necrosis may or may not be present. In the vesiculobullous type spongiotic vesicles and subepider mal blisters are formed. The insect bite (strophulus)-like type shows focal necrosis in the upper malpighian layer, and in the hemorrhagic type there is notable extravasation of erythrocytes. Figure 1. PLE, papular type, genuine lesions. A, Papules scat tered on chest 48 h after sun exposure; B, Histopathology from another patient with similar lesions shows perivascular and in terstitial lymphocytic infiltrate in the upper corium with subep idermal edema, vacuolization of basal cells, and spongiosis. Figure 2. PLE, papular type, experimentally induced lesions. A, Urticarial papules that coalesce emerged in the moderately pigmented test area on the upper arm 24 h after irradiation with toO J/cm2 UVA (UVASUN 3000); B, Superficial and deep per ivascular lymphocytic infiltrate with subepidermal edema, vac uolization of basal cells, and spongiosis. A B 345 VOL. 88, NO. 3 MARCH SUPPLEMENT 1987 POLYMORPHOUS LIGHT ERUPTION 3Ss Neutrophils and eosinophils are only present in a few cases [7]. We have noted them only in the vesiculobullous type. This is, however, inconsistent with other reports [34]. Using monoclonal antibodies to defme subsets of infiltrating mononuclear cells in papular PLE, Muhlbauer et al [39] found that the perivascular infiltrate was predominandy composed of T cells with a slight but inconsistent preponderance of cyto toxic/suppressor cells over helper/inducer cells. Macrophages represented less than 5% of the infiltrating cells. Langer hans/indeterminate cells were found to be increased in number. The same group [40] studied PLE by direct immunofluores cence technique and detected intervascular and focal perivascular deposition·of fibrin. In some patients, C3 and IgM was found in the walls of venules. The lupus band test was negative in all subjects. Recendy, Moncada et al [41] found a predominance of T helper cells and Ia + cells in the dermal infiltrate of PLE. evoked by sun exposure through window glass while patients are riding on trains, airplanes, or in cars. Furthermore, sunburn is not a prominent feature in PLE, neither clinically nor micro scopically. The question as to whether erythemal or pigmentary responses to solar radiation may differ from normal reactions in patients with PLE has stimulated research that produced confticting. ex perimental data. Thune [14] as well as others[54] found the MED of sunburn radiation lowered in patients with PLE. In contrast, Jansen [55] reported normal values, perhaps with a slighdy de layed fading of the erythema; pigmentary responses were also found to be normal. We could not discern any differences in MED-UVB or pig mentary reactions induced by UVA between patients with PLE and normal controls [9]. Others, too, have questioned the use fulness of MED-UVB as a diagnostic parameter [7]. ACTION SPECTRUM DIFFERENTIAL DIAGNOSIS The action spectrum ofPLE is not known. There have been many debates about the wavelength and energy requirements for elic iting skin lesions. Experimental results are conflicting and some times contradictory. Factors that may relate to the reported var iability include differences in individual susceptibility, seasonal variations, differences in test sites, light sources, and interpreta tion of test results, as well as the clinical variety ofPLE, including geographic differences. Many investigators report the induction of skin lesions with sunburn radiation between 280 and 320 om [32,33,42,43,44]. Most of these authors used radiation from high pressure mercury or xenon lamps or carbon arc sources with appropriate filters. In some instances responses to UVC were noted [33]. On the other hand, Langhof and Sprossig [45], Wiskemann and Wulf[46], and Gschnait et al [47] were able to reproduce skin lesions ofPLE with long-wave UV light (UVA). In a multitude of experimental studies, various authors came to the conclusion that the action spectrum might range from UVB, to UVA, and into visible light[14,27,44,48-51]. In some instances, an additive effect of infrared radiation was observed [13,14]. During the years from 1977 to 1985 we tried to induce skin lesions experimentally in more than 250 patients. Until 1982, 180 patients were tested by using various procedures [8]. Monochro matic light, both UVA and UVB, as well as polychromatic UVA in doses up to 40 J/cm2 failed to elicit PLE. When UVA from a high-intensity apparatus (UVASUN 3000; Mutzhas, Munich, FRG) [52] was given in doses of 60-100 J/cm2, up to 90% of patients developed lesions ofPLE if stringent requirements were met (Ta ble I). Adhering to the same experimental procedure but using polychromatic UVB in minimal erythemal doses (MED) up to 4, we were unable to reproducePLE at that time; however, only a few patients were tested. Recendy, we have extended our experience to another 90 pa tients. These were tested with UVA and UVB (UV 800 equipped with fluorescent bulbs, Philips TL 12; Waldmann, Villingen Schwenningen, FRG) on a contralateral or adjacent skin site, fol lowing the method described (Table I). About 60% of patients showed lesions ofPLE; out of this group 75% revealed sensitivity to UVA, 10% to UVB, and 15% reacted to both UVA and UVB [11]. The smaller yield of positive reactions compared with the previous study [8] might be due to the fact that some patients were tested in summer or fall, at a time when their skin was less UV sensitive due to hardening. Similar results were found by Ortel et al [53], who were able to reproduce skin lesions in 50% of 142 patients. In 56% the eliciting wavelengths were found in the UVA range, in 17% in the UVB spectrum, and in 26% in both. In view of these data it appears that, in the majority of PLE patients, long-wave UV is most effective in eliciting skin lesions. A small subgroup of patients shows additional sensitivity to UVB or may react to UVB exclusively. These findings are in accord ance with the observation that eruptions of PLE are frequendy The diagnosis of PLE is based on a patient's histo.ry and clinical features of lesions. The time course of PLE, with its onset hours after intense sun exposure and spontaneous fading (without res idue) of lesions within hours or days is very characteristic. It aids in establishing the diagnosis when the patient presents without skin lesions. A diagnosis can be made almost with certainty when the patient presents with a typical rash or whenPLE is reproduced by phototesting in the laboratory. Biopsies of genuine or exper imentally induced lesions may confirm the diagnosis, if other differential diagnoses cannot be excluded clinically. Staining with hematoxylin and eosin suffices; special stains are of little help, perhaps with the exception of direct immunofluorescence tech nique, if lupus erythematosus is suspected. It is our belief that chronic skin lesions with pronounced epi dermal changes are not part of the PLE spectrum. Thus, light induced disorders showing eczematous lesions, e.g., photoallergic dermatitis, photosensitive eczema, and persistent light reaction are excluded from PLE by their morphology. Solar urticaria may mimic the plaque type ofPLE. Time course of whealing and the reproduction of typical hives using low doses of electromagnetic radiation are characteristic for solar urticaria. Photosensitive erythema multiforme is a rare condition[56]. It is difficult to separate this disorder from the erythema multiforme type ofPLE. Clinical and histologic pictures are very similar[57]. The following features may help to differentiate light-sensitive erythema multiforme fromPLE: (1) The former occurs 1-14 days after sun exposure. (2) Immune complexes may be detected in the initial stage, and the lymphohistiocytic infiltrate is perivascular and interstitial in the upper corium. (3) Sometimes eosinophils and extravasated erythrocytes are prominent, and the epidermis shows focal necrosis. The deposition of immune complexes in venules of the skin triggered by UV erythema has been discussed as the underlying pathogenetic mechanism in photosensitive erythema multiforme [58]. Lupus erythematosus is the most important differential diag nosis, clinically and histologically. Subacute cutaneous lupus er ythematosus and the tumid type of discoid LE (DLE) may present with lesions very similar to the plaque type ofPLE. In LE, how ever, waxing and waning of lesions are not as closely correlated to sun exposure as in PLE. Lesions usually persist for several weeks or months even without further UV exposure. When LE lesions are induced by experimental UV irradiation [59] it takes at least several days, in most cases 1-2 weeks or longer, for lesions to appear. This prolonged time course differs from PLE. Histologically, the lymphocytic infiltrate in LE frequendy ex tends perivascularly and around the adnexa in the deeper corium. There might be mucin deposition between collagen bundles[60]. Subepidermal edema is not pronounced, and liquefaction degen eration, if present, is confined to the epidermal basal cell layer. Spongiosis is absent. Sometimes neutrophils are seen in vessels of the superficial plexus. In most cases of PLE the perivascular 36$ HOLZLE ET AL Table I. THE JOURNAL OF INVESTIGATIVE DERMATOLOGY Recommendations for Provocative Photo testing in PLE Test time Test site Size of test area Light source UV dose Before the PLE season starts Previously involved body areas. Avoid pigmented skin No less than 5 x 10 cm Use polychromatic UV in large doses UVA: 60-100 J/cm2 UVB: 2 MED Repeat irradiations on day 2 and 3, if necessary lymphocytic infiltrate reaches only into the mid-dermis. Subep idermal edema is a prominent feature. Vacuolization accompanied by spongiosis occurs in the 2 or 3 suprabasal cell layers. Intra cellular and intercellular edema of the lower part of the epidermis, in combination with subepidermal edema, gives the dermoepi dermal interface a spongy appearance. The histopathologic dif ferences mentioned are prominent only in fully developed lesions. In the initial stage of LE or PLE it is extremely difficult, sometimes impossible, to distinguish between the two diseases on histo pathologic grounds. Direct and indirect immunofluorescence are of limited value because they may yield negative results in early stages of LE or may be found positive in some patients with PLE who, however, do not meet other criteria of LE [29]. It is our impression that there might be a subgroup of patients that cannot be separated clearly either from DLE, SCLE, or PLE. It is con ceivable that these patients eventually progress into LE. This view is, however, not substantiated by follow-up studies [29,30], in which PLE patients were not found to develop LE. THERAPY AND PROPHYLAXIS Some patients may experience a cooling and beneficial subjective effect by local application of zinc lotion in acute-stage PLE. Top ical or systemic steroids may ameliorate inflammation or itching and shorten the eruption. In few patients eruptions of PLE can be suppressed by prophylactic systemic steroid treatment. Con trolled trials are lacking and it seems inappropriate to treat this chronic, intermittent, self-limited, and benign disease with sys temic steroids. More important than therapy of the acute eruption seems the prevention of further attacks by prophylactic measures. Light protection, phototherapy, photochemotherapy and, to some extent, systemic drugs offer ways to decrease UV sensitivity. Sun protection by protective clothing or staying in the shade may prevent PLE. The usefulness of topical sunscreens is limited, although sun blockers have been found effective in UVB-sensitive patients [62], and broad-band screens (UVB plus UVA) or phys ical sunscreens may be beneficial in other patients [8,51,63,64]. Systemic treatment with J3-carotene yielded different results. Some authors found only modest improvement of UV tolerance not sufficient to enable the patient to perform normal outdoor activities [65,66], while others report complete remission [14,67] (uncontrolled studies). J3-Carotene was also used in combination with canthaxanthin [68], a combination recently banned by the German Federal Department of Health. In controlled trials[69,70] J3-carotene was ineffective in many cases. The same holds true for chloroquine [68], although antimalarials, mainly chloroquine and quinacrine, have been commonly used to treat PLE[61,71,72]. Results have been unimpressive. Some authors [73,74] assume that the underlying mechanism in PLE is a disturbance in the tryptophan metabolism, with ac cumulation of kynurenic acid, which may act as a photosensitizer. They advocate treatment with high doses of nicotinamide to re duce the level of kynurenic acid and report good therapeutic results [74]. There is no proof of this hypothesis. In actinic prurigo [75] and PLE [76], thalidomide was helpful, but is obsolete in view of the teratogenic effect and neurotoxic side effects. Ketoprofen, a nonsteroidal anti-inflammatory agent, was shown to be ineffective [69]. Phototherapy and photochemotherapy provide a good protec- tive effect. Patients with PLE frequently show "hardening" with decreasing UV sensitivity during spring or early summer. It seems worthwhile to induce this protective mechanism by controlled exposures to sunlight [77] or artificial UV sources [78-80]. Also, PUVA treatment was used to prevent further attacks of PLE [47,81-84], and was found to be superior to phototherapy [53,62,83,85]. Until more is known about the long-term hazards of PUVA therapy, patients should be monitored carefully, al though the number of exposures and the cumulative UVA doses are quite small. We do not advocate PUVA therapy in PLE as the treatment of first choice, but inform our patients about the benign nature of PLE and recommend sun-protective measures in combination with skin "hardening" using natural sunlight. If this fails, phototherapy is used. O nly those patients who are exquisitely sensitive to UV are treated with PUVA therapy in our department. The mechanism by which phototherapy or pho tochemotherapy induce protection is not completely understood. Besides increased melanization and thickening of epidermis and stratum corneum, factors that enhance UV absorption in the ep idermis and provide a protecting shield for the underlying dermis, immunologic mechanisms cannot be excluded. HYP O THESES ON ETIOLOGY AND PATHOGENESIS OF PLE Apart from the fact that PLE is induced by electromagnetic ra diation emanating from the sun, nothing is known about its etiol ogy, despite many investigative studies. In their search for an endogenous photosensitizer, European authors focused on gastrointestinal abnormalities in PLE patients [45,86]. Also urinary excretion of an indole derivative, called "Kimmig's light band" [87] was described but was not found to be specific for PLE [88]. O thers [73,74] put forward the hypoth esis that disturbances in the tryptophan metabolism might be the cause of photosensitization. None of these theories account for the pathomechanism of PLE. Many investigators hold the view that PLE is related to a cell mediated immunologic reaction [7]. The time course of the re action, with a delay after the initiating sun exposure, the clinical picture, and histopathologic findings bear similarities to the ecze matous reaction of delayed-type hypersensitivity. A relevant pho toallergen has not been identified. Functional disturbances of lym phocytes have been found only inconsistently. Horkay and Meszaros [89] described UV-induced lymphocyte transformation in PLE. Also, a defect in the excision repair mechanism in lymphocytes of PLE patients was reported [90], but was not confirmed by others [91,92]. In recent studies on cell-mediated immunity in PLE, a transient decrease [93] as well as an increase[41] in number of lymphocytes was found; no inhibition of leukocyte migration was detected [94]. The number of peripheral T cells and response of peripheral lymphocytes to phytohemagglutinin, concanavalin A, and pu rified protein derivative of tuberculin was found normal before and after PUVA treatment [95]. This argues against the distur bance in lymphocyte function as a cause of PLE. REFERENCES 1. 2. 3. 4. 5. 6. Bateman T: A Practical Synopsis of Cutaneous Diseases According to the Arrangement of Dr. Willan. Philadelphia, Collins & Croft, 1817, pp 251-253 Hutchinson J: Lectures on Clinical Surgery: On Certain Rare Dis eases of the Skin. Volt. London, Churchill, 1879 Rasch C: Om et polymorft (erytematost, vesikulost og ekzematoidt) lysudslet. Hospitalstid 43:478-480, 1900 Hausmann W, Haxthausen H: Die Lichterkrankungen der Haut. Strahlentherapie, Sonderbande Bd 11, Berlin, Urban & Schwar zenberg, 1929, pp 62-71 McGrae JD, Perry HO: Chronic polymorphic light eruption. Acta Derm Venereol (Stockh) 43:364-379, 1963 Clorius R, Jung EG: Die polymorphe Lichtdermatose. Ergebnis bericht. Zentralbl Haut Geschlechtskr 133:291-298, 197411975 VOL. 88, NO. 3 MARCH SUPPLEMENT 1987 POLYMORPHOUS LIGHT ERUPTION 37$ 7. Epstein JH: Polymorphous light eruption. J Am Acad Dermatol 3: 329-243, 1980 36. Wright ET, Winer LH: Histopathology of allergic solar dermatitis. J Invest Dermatol 34:103-106, 1960 8. Hiilzle E, Plewig G, Hofmann C, Roser-MaaB E: Polymorphous light eruption. Experimental reproduction of skin lesions. J Am Acad Dermatol 7:111-125, 1982 37. Lever WF, Schaumburg-Lever G: Histopathology of the Skin. 6th ed. Philadelphia, Lippincott, 1983, pp 211-212 9. Plewig G, Hofmann C, Hiilzle E: Polymorphe Lichtdermatose, Fort schritte der Praktischen Dermatologie und Venerologie, Band 9. Edited by 0 Braun-Falco, HH Wolff. Springer, Berlin, 1979, pp 117-127 38. Ackerman AB: Histologic Diagnosis ofInflammatory Skin Diseases. Philadelphia, Lea & Febiger, 1978, pp 289-291 39. Muhlbauer JE, Bhan AK, Harrist TJ, Bernhard JD, Mihm MC: Papular polymorphic light eruption: An immunoperoxidase study using monoclonal antibodies. Br J Dermatol 108:153-162, 1983 40. Muhlbauer JE, Mihm MC, Harrist T]: Papular polymorphous light eruption. Fibrin, complement, and immunoglobulin deposition. Arch Dermatol 120:866-868, 1984 41. Moncada B, Gonzalez-Amaro R, Baranda ML, Coredo C, Urbina R:Immunopathology of polymorphous light eruption. J Am Acad Dermatol 10:970-973, 1984 42. Blum HF: Photodynamic Action and Diseases Caused by Light. New York, Reinhold, 1941, pp 211-250 43. Cahn MM, Levy EJ, Shaffer B: Experimentally induced reactions to ultraviolet light. I. Polymorphous light eruption and photo toxicity to drugs. J Invest DermatoI32:355-361, 1959 44. Magnus IA: Studies with a monochromator in the common idio pathic photodermatoses. Br J Dermatol 76:245-264, 1964 45. Langhof H, Spriissig M: Zur Pathogenese und Therapie des Lich tekzems. Arch Dermatol Syph 197:303-321, 1954 46. Wiskemann A, Wulf K: Untersuchungen tiber den ausliisenden Spektralbereich und die direkte Lichtpigmentierung bei chron ischen und akuten LichtausschHigen. Arch Klin Exp Dermatol 209: 443-453, 1959 10. Plewig G, Hiilzle E, Roser-MaaB E, Hofmann C: Photoallergy, New Trends in Allergy. Edited by J Ring, G Burg. Springer, Berlin, 1981, PP 152-169 11. Hiilzle E, Lehmann P, von Kries R, Plewig G: Polymorphous light eruption. A destinct entity with morphological variants. 44th An nual Meeting of Am Acad Dermatol, Las Vegas, Nevada, Dec 7-12, 1985 12. Morison WL, Stem RS: Polymorphous light eruption. A common reaction uncommonly recognized. Acta Derm Venereol (Stockh) 62:237-240, 1982 13. Jansen CT: The natural history of polymorphous light eruptions. Arch Dermatol 115:165-169, 1979 14. Thune P: Chronic polymorphic light eruption. Particular wavebands and the effect of carotene therapy. Acta Derm Venereol (Stockh) 56:127-133, 1976 15. Fusaro RM, Johnson JA: Hereditary polymorphic light eruption in American Indians. Photoprotection and prevention of streptococ cal pyoderma and glomerulonephritis. JAMA 244:1456-1459, 1980 16. Everett MA, Crockett W, Lamb JH, Minor D: Light-sensitive erup tions in American Indians. Arch Dermatol 83:243-248, 1961 17. Hojyo-Tomoka MT, Dominguez-Soto L: Clinical and epidermiol ogical characteristics of polymorphous light eruption in Mexico. Castellanian 3:21-23, 1975 47. Gschnait F, Hiinigsmann H, Brenner W, Fritsch P, Wolff K: In duction of UV light tolerance by PUVA in patients with poly morphous light eruption. Br J Dermatol 99:293-295, 1978 18. Jansen CT: Heredity of chronic polymorphic light eruptions. Arch Dermatol 114:188-190, 1978 48. Rottier PB: Testing of the skin for reactions to ultraviolet radiation. Dermatologica 127:260-266, 1963 19. Orr PH, Birt AR: Hereditary polymorphic light eruption in Ca nadian Inuit. Int J Dermatol 23:472-475, 1984 49. Verhagen ARHB: Light tests and pathogenetic wavelengths in chronic 20. Anderson D, Wallace HJ, Howes ETB: Juvenile spring eruption. Lancet ;:755-756, 1954 50. Frain-Bell W, Dickson A, Herd J, Sturrock I: The action spectrum in polymorphic light eruption. Br J Dermatol 89:243-249, 1973 21. Baran R, Civatte J: La photodermatose printaniere juvenile. Ann Dermatol Venereol (Paris) 107:537-541, 1980 51. 22. Calnan CD, Meara RH: Actinic prurigo (Hutchinson's summer pru rigo). Clin Exp Dermatol 2:365-371, 1977 Nordlund JJ, Klaus SN, Mathews-Roth MM, Pathak MA: A new therapy for polymorphous light eruption. Arch Dermatol 108: 710-712, 1973 52. 23. Aoki T, Fujita M: Actinic prurigo: A case report with successful induction of skin lesions. Clin Exp Dermatol 5:47-52, 1980 24. Birt AR, Davis RA: Hereditary polymorphous light eruption of American Indians. Int J DermatoI14:105-111, 1975 Mutzhas ME, Hiilzle E, Hofmann C, Plewig G: A new apparatus with high radiation energy between 320-460 nm: Physical de scription and dermatological applications. J Invest Dermatol 76: 42-47, 1981 53. 25. Lamb JH, Shelmire B, Cooper Z, Morgan Iq, Keaty C: Solar der matitis. Arch DermatoI62:1-27, 1950 Ortel B, Tanew H, Hiinigsmann H, Wolff K: Polymorphous light eruption. Action spectrum and photoprotection. J Am Acad Der matol 14: 748-753, 1986 26. Lamb JH, Jones PE, Maxwell TB: Solar dermatitis. Arch Dermatol 75:171-180, 1957 54. 27. Rottier PB, Baart de la Faille H: MED-action spectra in polymorphic light eruption and in porphyria compared with model normal spectra. Acta Derm Venereol (Stockh) 57(suppl 77):3-35, 1977 Stevanovic DV: Polymorphous light eruption. Br J Dermatol 72: 261-270, 1960 55. 28. EpsteinJH: Polymorphous light eruption. Ann Allergy 24:397-405, 1966 Jansen CT: Erythemal and pigmentary phototest reactions in polymorphous light eruptions. Acta Derm Venereol (Stockh) 59: 499-503, 1979 29. Jansen CT, Karvonen ]: Polymorphous light eruption. A seven-year follow-up evaluation of 114 patients. Arch DermatoI120:862-865, 1984 56. Fitzpatrick JE, Thompson PB, Ading JL, Huff C: Photosensitive recurrent erythema multiforme. J Am Acad Dermatol 9:419-423, 1983 30. Frain-Bell W, Mackenzie LA, Witham E: Chronic polymorphic light eruption (A study of 25 cases). Br J Dermatol 81:885-896, 1969 57. Galosi A, Plewig G, Hiilzle E, Dorn M: Lichtinduziertes poster petisches Erythema exsudativum multiforme. Hautarzt 37:494498, 1986 31. Lamb JH, Jones PE, Morgan RJ, Everett MA, Penrod IN: Further studies in light-sensitive eruptions. Arch Dermatol 83:568-583, 1961 58. Wuepper KD, Watson PA, Kazmierowski JA: Immune complexes 32. Epstein JH: Polymorphous light eruptions. Wavelength dependency and energy studies. Arch Dermatol 85:82-88, 1962 59. 33. Epstein JH: Polymorphous light eruptions. Phototest technique studies. Arch Dermatol 85:502-504, 1962 Lehmann P, Holzle E, Kind P, Goerz G, Plewig G: Experimental reproduction of skin lesions in lupus erythematosus by UVB and UVA radiation. Scientific exhibit, 45th Annual Meeting of Am Acad Dermatol, New Orleans, Louisiana, Dec. 6-11, 1986 34. EJpern DJ, Morison WL, Hood AF: Papulovesicular light eruption. A defined subset of polymorphous light eruption. Arch Dermatol 121:1286-1288, 1985 60. Panet-Raymond G, Johnson WC: Lupus erythematosus and poly morphous light eruption. Arch Dermatol 108:785-787, 1973 61. 35. Lehmann P, Hiilzle E, Plewig G: Vesikulobulliise Form der poly morphen Lichtdermatose. Allergologie 9:32-53, 1986 Cahn MM, Levy EZ, Shaffer B: Polymorphous light eruption. A ten-year follow-up and evaluation. Arch Dermatol 86:756-758, polymorphous light dermatosis. Dermatologica 133:302-312, 1966 in erythema multiforme and the Stevens-Johnson syndrome. J Invest Dermatol 74:368-371, 1980 1963 38s 62. 63. HOLZLE ET AL Gschnait F, Schwarz T, Ladich I: Treatment of polymorphous light eruption. Arch Dermatol Res 275:379-382, 1983 1ppen H, Kolmel K: Lichtschutz gegen Ultraviolett A. Arztliche THE JOURNAL OF INVESTIGATIVE DERMATOLOGY 81. Becker SW: Prevention of sunburn and light allergy with methox alen. General Practitioner 19:115-117, 1959 82. Parrish JA, Levine Mj, Morison WL, Gonzalez E, Fitzpatrick TB: Comparison of PUV A and beta-carotene in the treatment of polymorphous light eruption. Br J DermatoI100:187-198, 1979 83. Holzle E, Roser-Maap E, Hofmann C, Plewig G: Photochemoth erapie von Photodermatosen: Lichturtikaria, persistierende Lich treaktion und polymorphe Lichtdermatose. Hautarzt 32(suppl V): 404-406, 1981 Kosmetologie 10:219-226, 1980 64. McFadden N: UV-A sensitivity and topical protection in polymor phous light eruption. Photodermatology 1:76-78, 1984 65. Swanbeck G, Wennersten G: Treatment of polymorphous light eruption with beta-carotene. Acta Derm Venereol (Stockh) 52: 462-466, 1972 66. Mathews-Roth MM, Pathak MA, Fitzpatrick TB, Harber LC, Kass EM: Beta-carotene therapy for erythropoetic protoporphyria and other photosensitivity diseases. Arch Dermatol 113:1229-1232, 1977 67. Jansen CT: Beta-carotene treatment of polymorphous light eruption. Dermatologica 149:363-373, 1974 68. Suhonen R, Plosila M: The effect of beta-carotene combination with canthaxanthin, Ro 8-8427 (PhenoroR), in the treatment of poly morphous light eruption. Dermatologica 163:172-176, 1981 69. Corbett MF, HawkJL, Herxheimer A, Magnus IA: Controlled ther apeutic trials in polymorphous light eruption. Br J Dermatol 107: 571-581, 1982 70. Jansen CT: Oral carotinoid treatment in polymorphous light erup tion: A cross-over comparison with oxychloroquine and placebo. Photodermatology 2:166-169, 1985 84. Jansen CT, Karvonen J, Malmiharju T: PUV A therapy for poly morphous light eruptions: Comparison of systemic methoxsalen and topical trioxsalen regimens and evaluation of local protective mechanisms. Acta Derm Venereol (Stockh) 62:317-320, 1982 85. Plewig G, Holzle E, Lehmann P: Phototherapy for photodermatoses. Curr Probl Derm 15. Therapeutic Photomedicine. Edited by LH Honigsmann, G Sting!. Basel, Karger, 1986, pp 254-264 86. Wulf K, Bramstedt F, Lindenschmidt TO: Storungen der Ei weiBverdauung, ein haufiger Befund bei chronisch polymorphen Lichtausschlagen. Medizinische Welt 1:525-528, 1955 87. Kimmig J: Lichtdermatosen und Lichtschutz. Arch Dermatol Syph 200:68-85, 1955 88. Wulf K: Beitrag zur A tiologie der Lichtdermatosen. Mit experi mentellem Nachweis endogen gebildeter photodynamisch wirk samer Urinsubstanzen unter besonderer Beriicksichtigung der chronis chen polymorphen Lichtausschlage. Arch Dermatol Syph 197:209-225, 1954 71. Christiansen JV, Brodthagen H: The treatment of polymorphous light eruption with chloroquine. Br J Dermatol 68:204-208, 1956 89. 72. Woodburne AR, Philpott OS, Philpott JA: Quinacrine (Atabrine) in treatment of solar dermatoses. Arch Dermatol 70:116-118, 1964 Horkay I, Meszaros C: A study on lymphocyte transformation in light dermatoses. Acta Derm Venereol (Stockh) 51:268-27, 1971 90. 73. Bonafe JL, Chap H: Lucite polymorphe et perturbations du metab olisme du tryptophanne (Voie de la cynurenine). Ann Dermatol Venereol (Paris) 107:89-90, 1980 Horkay I, Tamasi P, Csongor J: UV-Iight induced DNA damage and repair in lymphocytes in photodermatoses. Acta Derm Ve nereol (Stockh) 53:105-108, 1973 91. 74. Neumann R, Rappold E: Therapie der polymorphen Lichtdermatose mit Nicotinamid. Zentralbl Haut Geschlechtskr 150:628, 1985 Raffle E, MacLeod TM, Hutchinson F: In vitro lymphocyte studies in chronic polymorphous light eruption. BrJ DermatoI 89:143-148, 1973 75. Lovell CR, Hawk JCM, Calnan CD, Magnus IA: Thalidomide in actinic prurigo. Br J Dermatol 108:467-471, 1983 76. Saul A, Flores 0, Novales J: Polymorphous light eruption: Treat ment with thalidomide. AustralasJ DermatoI17:17-21, 1976 77. Johnson KJ: Light sensitivity treated by hyposensitization. Ann Al lergy 19:891-893, 1961 78. Van der LeunJC, Van Weelden H: Light-induced tolerance to light in photodermatoses. J Invest Dermatol 64:280(abstr), 1975 79. Morison WL, Momtaz K, Mosher DB, Parrish JA: UV-B photo therapy and prophylaxis of polymorphous light eruption. Br J Dermatol 106:231-233, 1982 80. Meffert H, Sonnichsen N: Photokonditionierung bei polymorpher Lichtdermatose. Dermatol Monatsschr 170:274-276, 1984 92. Jung EG, Bonert E: Chronisch polymorphe Lichtdermatose. Un tersuchungen an Lymphozyten in vitro. Dermatologica 148:209-212, 1974 93. Horkay I, KrajczarJ, Bodolay E, Debreczeni M, Begany A: A study on cell-mediated immunity in polymorphic light eruption. Der matologica 166:75-80, 1983 94. Jansen CT, Helander I: Cell-mediated immunity in chronic poly morphous light eruptions. Leukocyte migration inhibition assay with irradiated skin as antigen. Acta Derm Venereol (Stockh) 56: 121-125, 1976 95. Karvonen J, Viander M, lIonen J, Jansen CT: PUVA photohypo sensitization in polymorphous light eruption: Evaluation of sys temic immunological factors. Acta Derm Venereol (Stockh) 62: 497-500, 1982










© Copyright 2026