
Pectus Excavatum An informational brochure for
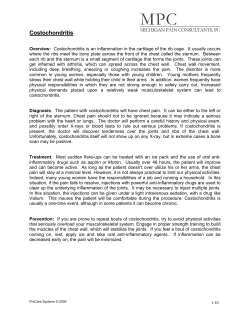
Pectus Excavatum An informational brochure Patients and Families with "caved-in" chest for Learn about the treatment of this congenital chest wall malfonnation. This brochure contains the answers to frequently asked questions about Pectus Excavatum Andre. Hebra. M.D. Chief, Division of Pedw/ric Swgery Professor of SlIIgery and Peaia/rics Pediatl'ics Surgery 96 Jonathan Lucas Street Suite418CSB PO Box 250613 Charleston· SC 29425 Ph (843) 792-3851 1-800-424-6872 Pager (843) 792-2123 E-Mail: [email protected] FREQUENTLY ASKED QUESTIONS ABOUT CORRECTIVE SURGERY FOR PECTUS EXCAVATUM USING THE MINIMALLY INVASIVE TECHNIQUE (ALSO KNOWN AS THE NUSS OPERATION): 1) How does the minimally-invasive differ from the old surgical repair? approach The Minimally Invasive Operation for repair of Pectus Excavatum, also known as the NUSS OPERATION, is a completely different surgery from what it used to be. The open Ravitch operation required making an incision in the anterior chest - the front of the chest - and then removing segments of all the ribs affected by the pectus. The outer layer of the cartilage ribs (perichondrium) is preserved in order to allow the ribs to grow back. The sternum must be fractured in at least one area to allow for it to be bent in the appropriate position. Complications of the open operation include bleeding, infection, injury to the lungs and pleura, and possible need for placement of chest drains. The end result is rated as very good but it does leave a long scar on the chest. With the new technique (known as the Nuss operation or the minimally invasive repair), it is not necessary to create any large incisions or to remove/fracture any ribs or cartilage, or sternum. The surgeon is able to approach the chest with small lateral chest wall incisions and, using a special camera (thoracoscope), the surgeon can visualize the inside of the chest so that a stainless steel bar can be placed in order to correct the deformity. Again, this is accomplished without cutting anything, without breaking bones, without removing any cartilage. The duration of the entire operation is much shorter. With the open repair, the operation may take 4 to 5 hI'S. With the Nuss technique, the operation is typically completed in just about an hour. 2) What type of patient should be considered for this operation? What are the indications for surgery? What is the chest index? Is it a cosmetic operation? Patients must be carefully evaluated prior to surgery. The things that we look for are -#1 - how severe is the deformity (one must determine the chest index). #2, what kind of physiologic impairment it is causing to the patient. #3, what is the psychosocial impact of the deformity. The chest index is a measurement taken on the CT scan of the chest in which a ratio is obtained between the lateral and anterior-posterior diameter of the chest wall. A normal chest index is 2.5. Patients with an index greater than 3.2 have a fairly pronounced and severe pectus excavatum and will typically need operative correction. Even if asymptomatic, those patients usually benefit form the corrective surgery. Many patients with mild to moderate pectus excavatum will not report any significant shortness of breath. However, upon further questioning, one may find that the child can't keep up with their peers in the same physical activities that they used to. They get tired more easily. Or, as summer comes around, they don't want to take their shirt off for sports, swimming, or around other children. Typically affected children always leave their shirt on if they're in the pool. Clearly such patients would benefit from the surgery. A parallel comparison can be made with children born with Cleft Lip & Palate - that repair could be considered a cosmetic repair. However, no one would allow a child to go on in life with a cleft lip deformity. Pectus deformity is no different. The only difference is that you can hide it under a shirt. But it's still a deformity of the sternum and the chest that deserves to be corrected if it is causing significant concerns to the patient & family. 3) Is there an ideal age group for the new operation? The ideal age for the minimally invasive operation is between 812 years. The main reason for that is that the child should be old enough to understand what's ahead, to understand reasons for surgery, to understand what's involved in recovery from surgery. Moreover, between 8-12 years, the ribs and cartilage are still soft enough so that the surgeon can repair the deformity using the pectus-bar easily. The recovery from surgery at that age is much easier than it is for teenagers. However, age by itself is not considered a contraindication for surgery. As a matter of fact, many adult patients have undergone the Nuss operation with excellent results. Treatment of Pectus Excavatum 4) How does the Minimally Invasive operation work? The Minimally Invasive operation (Nuss technique) is done through 2 small lateral chest wall incisions -- one on each side of the chest, lateral to the nipple area. A small 5 mm camera is also inserted into the chest. This will allow the surgeon to have direct visualization of the placement of the bar and all the important structures inside your chest (such as the heart, blood vessels, and lungs). The surgeon will know exactly where to place the bar. Through these small lateral chest wall incisions, a special curved stainless steel bar (also known as the LORENZ pectus bar) is passed behind the sternum. The bar comes in different length according to age and patient size. Then the bar is selected at the time of surgery and is bent by the surgeon after certain measurements of the chest are taken. The bar will have a smooth concave shape to it in order to allow for its placement behind the sternum. The bar is passed through the small lateral chest wall incision, under the sternum, in front of the heart, all the way to the other side of the chest. The bar is than flipped, such that the sternum is raised and the entire chest wall is remodeled. The entire maneuver is done under thoracoscopic visualization. Essentially, what the operation is like placing an internal "brace". The brace (pectus bar) will displace the ribs and the sternum forward, keeping it in that position until complete remodeling of the chest wall has occurred. This process typically takes two years. Fort that reason, the bar is left in place for at least two years. The bar is kept in secure position by sutures that attach it to the chest wall muscle fascia. In addition, a lateral stabilizer (a type of T-connector) is attached to the sides of the bar for extra points of fixation. Finally, a third point of fixation (an extra stitch that is placed around a rib and around the bar itself) can be used to hold it in place right next to the sternum. The operation is done under general anesthesia. thoracic epidural should be considered. In addition, a The thoracic epidural requires placement of a little catheter in the epidural space (mid-back) by the anesthesiologist. This technique is similar to the one employed for delivering babies. The epidural catheter can remain in place for several days after surgery, allowing doctors from the pain team to deliver certain types of pain medications to facilitate the management of pain & discomfort after surgery. The medications will have a numbing effect, so that the child is essentially numb and with minimal pain from about the nipple level down. The catheter can be left in place for about 3 days after surgery. It is important to remember that anytime a patient receives a thoracic epidural, it will be necessary to place a Foley catheter -a catheter to drain the bladder. The reason for that is because those patients who have an epidural will have trouble voiding. With the Foley, the patient can void normally into a bag. Once the epidural is removed, the Foley catheter is removed as well. Patients typically will be discharged home with oral-pain medicine. Typically, a narcotic pain medication like Tylenol with codeine or Percocet will be necessary for 1 to 2 weeks. Additionally, an anti-inflammatory medication (like Motrin, Alive or Advil) is also utilized. 7) How long will the bar stay in place? When and how is it removed? The bar stays in place for about 2 years and most studies have shown that this will give the chest enough time to remodel itself and assume a new "normal" shape. The operation for bar removal is relatively simple. It is usually done as an outpatient procedure. It does require general anesthesia. The surgeon will reopen one or two of the small lateral incisions and essentially pull the bar out. The incision is closed and the whole procedure takes just a few minutes. Patients usually go home shortly after surgery, on the same day. i /-/i " Jl . _,_., - - /' I PP.C't.us Bar CT Scan appearance Excavatum of the chest in a patient with Pectus 8) Are there common problems or complications associated with this procedure? The most common problems and complications related to surgery have changed since the operation was first reported in 1996. In the initial series of several hundred patients it was found that the most common complications were bar displacement, pneumothorax, and infection. However, as the technique has improved, the complication rate has dramatically decreased. For instance, bar displacement -which was reported in almost 10% of the patents - IS now reported in about 1%. Other problems such as Infection and pneumothorax are very rare. The use of thoracoscopy has also helped in making this a safer operation. Occasionally we may see patients that have an initial excellent cosmetic result but the chest may change and the ribs may do funny things. Some patients may experience different growth rate of the ribs on the left and right side of the chest (this is particularly a concern in patients with severe asymmetry of the chest prior to any corrective surgery). It has been reported before that ribs and cartilage can grow in an unusual way that you didn't expect. This may result in an asymmetric appearance of the chest even after a successful operation using the minimally invasive technique. Unfortunately the surgeon cannot control the rate of bone and cartilage growth in a developing child. 10) How long does the patient stay in the hospital after surgery? Immediately after surgery, the patient is taken to the recovery room and than to a general care floor in the hospital. Usually there is no need for critical care monitoring or leu admission. The room is fairly typical for most hospitals; nurses come in and check on the patient frequently. Other services that will be involved in the patient's care include the pain management, child life and physical & occupational therapy. All providers will concentrate specifically on the needs of the pectus repair patients. The average length of stay varies between 5-7 days. As a rule, the younger child will stay less and the older child and young adults will stay longer. Again, if the ribs are soft and the repair is very easy, odds are that the patent will stay in the hospital just a few days. Patients and families are advised to pick a vacation time to have the surgery done - usually around summertime - because most children will have to stay out of school for about 2 weeks after surgery to be observed closely at home. Physical activities will be limited and patients will not be able to lift up their book bags for almost one month after surgery. Patients are instructed not to lift more than about 10 pounds after surgery, which, as most parents know, is lighter than the average book bag these days. Also, patients can't return to either PE or sports until cleared by their surgeon. Typically patients are seen back in the surgeon's office 2 weeks after discharge from the hospital and, at that time, it is determined, based on the individual patient's progress, when they can go back to physical activities. Generally speaking, most patients will return to sports and normal physical activities 4 - 6 weeks after surgery. However, contact sports (which include soccer and football) should be avoided for at least 6 months. Despite such initial restrictions, after approximately 4 - 6 weeks, the patient should be fully recovered and should become very, very active. It is important to build up muscle. It is important to regain strength. Thus patients should be participating in sports, running, swimming, biking, and especially weight-lifting. It is desirable that children recovering from pectus surgery should build their pectoralis (chest), deltoid (shoulder), and abdominal muscles. Workingout with weights is very important after cleared by the surgeon. 12) How do the kids who have had the Nuss repair feel about it? This operation has truly revolutionized the way pectus excavatum has been managed. The operation is well accepted by patients and parents as well as the community in general and the pediatricians. It is less invasive, less traumatic, and it gives patients an excellent functional and cosmetic result. The majority of patients are well informed about their surgical options and they will seek surgical treatment using the minimally invasive technique. The overall satisfaction rate with the procedure has been rated as excellent or very good by more than 90% of patients. The Nuss procedure usually seems to be quite a life-changing operation. Most parents and the children just cannot believe the difference it has made in their lives - something that they probably would not admit to prior to surgery has caused them to have a whole new outlook on their futures as well as their perception of themselves and their own wellbeing. Additional information about corrective surgery for Pectus Excavatum can be found at the following website: emedicine.com (search words: Pectus Excavatum) An informational brochure for Patients and Families with "caved-in" chest Pediatrics Surgery 96 Jonathan Lucas Street Suite418CSB PO Box 250613 Charleston· SC 29425 Ph (843) 792 -3851 1-800-424-6872 Pager (843) 792-2123 E-Mail: [email protected] After Minimally Invasive Repair











© Copyright 2026