
Seizures in encephalitis Usha Kant Misra , *C T Tan , Jayantee Kalita
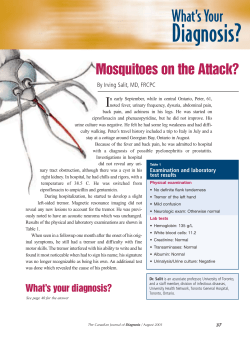
Neurology Asia 2008; 13 : 1 – 13 REVIEW ARTICLES Seizures in encephalitis Usha Kant Misra DM, *C T Tan MD, Jayantee Kalita DM Department of Neurology, Sanjay Gandhi PGIMS, Lucknow, India; *Department of Medicine, University of Malaya, Kuala Lumpur, Malaysia Abstract A large number of viruses can result in encephalitis. However, certain viruses are more prevalent in certain geographical regions. For example, Japanese encephalitis (JE) and dengue in South East Asia and West Nile in Middle East whereas Herpes simplex encephalitis (HSE) occurs all over the world without any seasonal or regional variation. Encephalitis can result in acute symptomatic seizures and remote symptomatic epilepsy. Risk of seizures after 20 years is 22% following encephalitis and 13% after meningitis with early seizures. Amongst the viruses, HSE is associated with most frequent and severe epilepsy. Seizures may be presenting feature in 50% because of involvement of highly epileptogenic frontotemporal cortex. Presence of seizures in HSE is associated with poor prognosis. HSE can also result in chronic and relapsing form of encephalitis and may be an aetiology factor in drug resistant epilepsy. Amongst the Flaviviruses, Japanese encephalitis is the most common and is associated with seizures especially in children. The frequency of seizures in JE is reported to be 6.9% to 46%. Associated neurocysticercosis in JE patients may aggravate the frequency and severity of seizures. Other flaviviruses such as equine, St Louis, and West Nile encephalitis can also produce seizures. In Nipah encephalitis, seizures are commoner in relapsed and late-onset encephalitis as compared to acute encephalitis (50% vs 24%). Other viruses like measles, varicella, mumps, influenza and enteroviruses may result in encephalitis and seizures. Status epilepticus can also occur in encephalitis. It may be refractory to medication and require aggressive treatment. Single or discrete seizures in encephalitis should be treated as any other acute symptomatic seizures. INTRODUCTION Encephalitis refers to acute inflammatory process affecting the brain. Viral infections are the most important cause of encephalitis. There are over 100 viruses that can result in encephalitis. The patients present with fever and varying degree of alteration in sensorium which may be associated with focal neurological signs or seizures. In such patients, malaria, bacterial meningitis and non infectious causes of encephalopathy must be carefully excluded. Viral encephalitis generally results in nonspecific clinical picture with some specific features of anatomical involvement such as behavioral changes, aphasia or partial complex seizure in herpes simplex encephalitis (HSE) because of characteristic frontotemporal involvement. There are numerous viruses responsible for viral encephalitis. While precise estimates about the incidence of encephalitis following these viral infections are not available; there are estimates that HSE is the most important cause of treatable viral encephalitis with an incidence of 1 case/million population/year. Certain viruses are prevalent in certain regions. Japanese encephalitis (JE) in South East Asia, West Nile encephalitis is Middle East, St. Luis encephalitis and equine encephalitis in America are some examples. Lately West Nile encephalitis from USA and Nipah virus encephalitis from Malaysia have been reported. The incidence of clinically diagnosable encephalitis is between 3.5-7.4/100,000 population/year; however in children the incidence is much higher. 1 Encephalitis may occur in sporadic or epidemic form. Establishing the diagnosis of viral encephalitis may be challenging. The likelihood of a virus depends upon the geographical location, timing of the epoch studied and method or rigor of investigation. In a recent study in Finland, cerebrospinal fluid (CSF) polymerase chain reaction (PCR) was used to diagnose over 3,000 Address for correspondence: U K Misra, Professor and Head, Department of Neurology, Sanjay Gandhi Post Graduate Institute of Medical Sciences, Raebareily Road, Lucknow- 226014, India. FAX: 091-0522-2668017, Email: [email protected], [email protected] Neurology Asia patients with CNS infections, such as encephalitis, meningitis and myelitis. In this study, Vericella zoster was the most common infection (29%), followed by herpes and entero viruses in 11% each, and influenza A virus in 7% of patients.2 This study suggests that HSV is probably over estimated and Varicella zoster underestimated. HSE however, remains a critical diagnosis because specific treatment is available for this encephalitis. In USA, the most important encephalitides are HSE and arbovirus encephalitides, but 73% encephalitis is of undetermined etiology.3 Encephalitis and meningoencephalitis are important causes of acute symptomatic seizures and remote symptomatic epilepsy. Long-term risk of seizures following CNS infection was studied in a large population based study. Twenty year risk of unprovoked seizures was 6.8%; 22% for encephalitis with early seizures, and 13% for bacterial meningitis with early seizures.4 In the present review, the seizures in HSE, Flavivirus (Japanese encephalitis, eastern equine and western equine, dengue), and other viruses including Nipah virus encephalitis will be discussed. HERPES SIMPLEX ENCEPHALITIS Herpes simplex virus is a neurotropic virus and is the most important cause of sporadic encephalitis in children above 6 months and in adults.5 No seasonal or gender related preference occurs in HSE. It has a high mortality of 70% if untreated and prognosis is poor. Only a minority of patients return to normal functions. There is a bimodal distribution of HSE with one third cases occurring before 20 years of age and half in those above 50 year of age. In a recent PCR study on 516 patients with clinical evidence of encephalitis, 7.4% patients were due to HSE and most of these HSE patients were above 40 year of age.6 The bimodal distribution of HSE may reflect primary HSV infection in younger age group and reactivation of latent HSV infection in older patients. In immunocompetent patients, more than 90% of HSE occurs due to infection with HSV-1 and the remainder due to HSV-2.7 More than two-third cases of HSE due to HSV1 infection appears to result from reactivation of endogenous latent HSV-1 infection in the individuals previously exposed to the virus. HSV-1 has remarkable capability for producing latency, persistent infection and for reactivation.8 Primary HSV1 infection results in axoplasmic transport to the trigeminal sensory ganglion where it establishes latency. Latent HSV1 virus is detectable in trigeminal ganglia of nearly all June 2008 seropositive individuals.8 Reactivation results in retrograde transport of virus resulting in herpes labialis amongst other clinical manifestations. However the pathway by which HSV reaches the CNS in humans to produce encephalitis remains unknown. In Primary infection, virus could invade the olfactory bulbs through the nose and spread via olfactory pathway to orbitofrontal and medial temporal lobes.9 Affinity of HSV-1 for basifrontal and medial temporal (limbic) cortex and sparing of the most other cortices, grey matter, nuclear masses and white matter is interesting and mysterious. The affinity for the specialized areas is attributed to intranasal inoculation and spread via olfactory nerve of HSV.9 Proximity of dural nerves to basifrontal and temporal lobes, virus lies dormant in anterior and middle cranial fossa which renders these areas more susceptible to HSV. The virus may travel by cell to cell contact across the meninges into adjacent cortices. The structures involved in HSE are part of limbic system and these boundaries are respected by HSV1.10 This affinity is attributed to distinctive anatomical, neurochemical and immunological properties of these cortices. Clinical spectrum The clinical manifestations of HSE in older children and adults are indicative of area of pathology in the brain. These include focal encephalitis with fever, altered sensorium, bizarre behavior and focal neurological signs. The focal neurological signs are related to fronto-temporal involvement including aphasia, personality change and focal seizures. Such focality however may be minimal in the acute stage and may not be diagnostic of a particular viral cause. It has recently been reported that about 20% HSE cases may be relatively mild and atypical without any focal feature.11 The EEG and MRI findings in HSE are consistent with frontotemporal involvement (Figure 1). However there are no characteristic series of findings pathognomonic of HSE. Seizures in HSE can be acute symptomatic or remote symptomatic. In a study on 29 survivors of 34 biopsy proven HSE patients with acyclovir therapy, who were evaluated 6 months to 11 year after HSE, the most common long term symptom was behavioral abnormality in 45% followed by seizures in 24.7%.12 Seizures were the presenting feature in 50% patients in the acute stage. Seizures are not only common in HSE but also have prognostic significance. In a study on children Figure 1A: Cranial MRI, T2 sequence of a patient with herpes simplex encephalitis shows hyper intensity in temporal lobes. with HSE where 47 patients were evaluated, 26 (65%) had good outcome and 14 (35%) had poor outcome. Seizures occurred at the time of presentation in 63% and 71% of them had poor outcome. Abnormal neuroimaging (79%) and EEG (92%) were more prevalent in patients with poor outcome group.13 Temporal and frontal cortices are highly epileptogenic compared to parietal and occipital cortex. Change in excitability of hippocampal A3 neuronal network and HSV1 induced neuronal loss results in mossy fiber reorganization which may play an important role in the generation of epileptiform activity.14 Clinical characteristics and prognosis of post encephalitic epilepsy in children were evaluated in 44 patients aged 21 mo to 17 year (mean 8.1 years) who were selected from 798 epilepsy children. Twenty had favorable and 24 poor outcome. Factors predicting a poor outcome in post encephalitic epilepsy were status epilepticus occurring during the first stage, slow background activity, multifocal spikes and HSE.15 Figure 1B: EEG of the same patients showing rhythmic slow waves both sides, and periodic lateralized epileptiform discharges (PLEDs) on the right. Neurology Asia Although HSE typically produces a monophasic illness, chronic encephalitis and relapsing encephalitis have also been reported rarely. A 66 year old immunocompetent man developed status epilepticus and died of pneumonia in the course of progressive hemiparesis, cognitive decline and brain atrophy over 9.5 year period after HSE. Autopsy confirmed active encephalitis consisting of necrosis and lymphocytic infiltration with intranuclear inclusions in neurons and glia and markedly edematous parenchyma of frontal and parietal lobes. HSV1 antigen was detected by immunohistochemistry, HSV-1 DNA by in situ hybridization and herpes virus nucleocapsid by electron microscopy. These findings suggest that direct viral reactivation might result in relapse of HSE causing progressive clinical deterioration associated with persistence of HSV1 in brain.16 In a long term follow up study of cognitive sequelae of HSE, 1 out of 8 adult patients with HSE experienced progressive clinical deterioration.17 In children with HSE progressive cognitive and behavioral deterioration for many years has also been reported.18,19 Most of these patients develop intractable seizures, slowly progressive hemiparesis and cognitive decline some years after contacting the disease. The histopathological changes are consistent with chronic active encephalitis. Intractable seizure disorders associated with chronic herpes infection are being reported when the pharmaco-resistant epilepsy patients were subjected to epilepsy surgery and resected brain tissue was subjected to histopathology and PCR. Three patients who developed HSV1 encephalitis diagnosed 6 months, 3 years and 7 months back, underwent surgical reaction 8.5 years, 6 years and 3 years respectively. Pathological examination confirmed chronic encephalitis in all 3 patients and PCR revealed HSV1 genome. These cases represent example of chronic herpes encephalitis manifesting with seizure disorder and presence of viral genome in brain long after initial episode of treated HSE.18 There was a case report of chronic persistent temporal lobe encephalitis following genital herpes by HSV-2 resulted in intractable partial complex seizure which necessitated temporal lobectomy. Immunohistochemistry of resected temporal lobe confirmed HSV2 infection. Post operative exacerbation of seizures was resistant to drugs and could be controlled after acyclovir therapy.20 Complicated febrile convulsions may also be the initial manifestation of HSV-1 encephalitis. In June 2008 a study on 151 children with febrile convulsions; 5 children with complicated febrile convulsion did not have HSV antibodies in serum and CSF, but CSF was positive for HSV PCR. The authors suggested that any patient with complicated febrile convulsion should be investigated for HSV PCR, to look for HSV encephalitis.21 These preliminary results do need further studies. Experimental studies on hippocampal excitability in herpes simplex encephalitis Corneal inoculation of mice with HSV-1 induces acute spontaneous behavioral and electroencephalographic seizures because of increased hippocampal excitability and seizure susceptibility. In slices from infected mice, the surviving hippocampal CA3 pyramidal neurons exhibited a more depolarizing resting membrane potential concomitant with an increase in membrane input resistance. They also had lower threshold for generating synchronized bursts and a decrease in amplitude after hyperpolarization (AHP) compared to controls. These results suggest that a direct change in the excitability of hippocampal CA3 neuronal network could play an important role in the development of acute seizure and subsequent epilepsy in HSV infection.22 Similar results were reported in another experimental study in which hippocampal cell culture on treatment with HSV-1 virus resulted in epileptiform activity, neuronal loss and increase in mossy fiber sprouting. Intracellular recording of CA3 pyramidal neurons revealed more depolarizing resting membrane potential, reduced threshold for generating synchronized burst and decreased amplitude of hyperpolarization compared to controls. These results show increase in CA3 neuronal excitability, neuronal loss and mossy fiber reorganization which may have a role in seizures and epilepsy following HSV infection.14 HSV strains vary with respect to their neurovirulence, +GC strains of HSV1 replicate to higher titers and expressed more abundant viral antigens then –GC strain. +GC strains spread more completely through out the brain to involve amygdela, nucleus accumbens, brainstem nuclei and locus ceruleus. +GC antigens has also been found in cerebral cortex layer 1 of animals that developed seizures. FLAVIVIRUS ENCEPHALITIS Several mosquito born neurotropic members of genus flavi virus family cause similar disease pattern across the globe. These viruses include St. Louis and equine encephalitis in USA, Rocio virus encephalitis in Brazil, Murray Valley encephalitis in Australia, New Guinea, and New Zealand. JE is the most important flavirus, which causes 30,000 to 50,000 cases of encephalitis and 10,000 deaths in Asia every year. West Nile virus is prevalent in Middle East and recently outbreaks have been reported from USA. Flavivirus genus also includes mosquito born virus that causes hemorrhagic fever (yellow fever, dengue fever and tick borne virus). Flavivirus is a small RNA virus with an envelop protein which is important for viral attachment and entry into the host. Epidemiology Epidemiology of flavivirus is governed by complex interplay between entomologic (vector), climatic, human behavior and viral factors that are not completely understood.23 Humans are dead end host because they don’t have sufficiently prolonged viremia to transmit the virus. However, West Nile virus can be transmitted to humans through blood products and organ transplantation because of relatively prolonged viremia. In Asia, pigs and birds are important natural hosts for JE virus because these animals are often kept close to human habitat. They serve as amplifying host and transmit virus to humans. In USA death of crows and blue jays may serve as warning that human disease is imminent.24,25 JE is mostly a disease of children where as West Nile encephalitis and St Louis encephalitis in USA affect adults. This paradox is attributed to intensity of viral transmission and to acquired immunity. Serological surveys reveal that in endemic areas almost everyone is infected by JE virus during childhood, however fever occurs in a minority (1 in 300) of the exposed persons and encephalitis occurs in even fewer. Thus JE does not occur in adults in endemic areas because adults are already immune to JE virus. However in a newly invaded JE virus area all the age groups are at risk of developing JE. Travelers to endemic area are also at risk of developing JE. Epidemiology of Murray valley encephalitis in Australia and West Nile in Africa follows a pattern similar to JE in Asia, though fewer cases of encephalitis occur in these areas. A pure febrile syndrome caused by Murray valley encephalitis virus is not seen. West Nile virus results in large out breaks of fever, arthralgia and rash but when it spread to new areas, it results in outbreaks of encephalitis. St Louis encephalitis is endemic in southern USA, but most of the population does not have pre-existing immunity because of low rate of transmission of virus to humans. However occasionally there has been outbreak of St Louis encephalitis as in 1975.26 Advance age is associated with greater severity of West Nile, St Louis and JE27,28, in which there is a second peak in the elderly. The exact reason for more severe disease in elderly though not known but impaired integrity of blood brain barrier (BBB) due to cerebrovascular disease or neurocysticercosis may be responsible.29 Prior infection with a flavivirus and cross reacting antibodies may affect the outcome of infection with a second flavivirus. For example, in JE, prior infection with dengue may protect against a severe illness.30 However, serial infection with different serotypes of dengue virus is associated with more severe illness; e.g. dengue hemorrhagic fever. The strain variation may also be important determinant of the severity of clinical picture in endemic area. Clinical features The neurological disease typically develops in patients after an incubation period of 3-15 days and a short nonspecific febrile illness. The neurological symptoms and signs depend on which part of the nervous system is predominantly affected. The involvement of meninges cause meningitis, brain parenchyma causes encephalitis and spinal cord causes myelitis. The most important manifestation which often overlap are impairment of consciousness and seizures occurring in about 85% patients with JE and Murray Valley encephalitis, and up to 10% in West Nile encephalitis. Japanese encephalitis JE is a severe form of endemic flavivirus encephalitis manifesting with features of encephalitis or encephalomyelitis. In a study on radiological changes in JE, CT scan was done in 38 and MRI in 31 patients. Thalamic involvement was present in 93.5% (Figure 2), basal ganglia in 35%, mid brain in 58%, pons in 26% and cerebral cortex in 19.4% of patients.31 Similar findings have been reported in earlier autopsy studies.32,33 Anterior horn cell involvement in JE has also been reported based on clinical, neurophysiological34,35 and neuropathological findings.32 Thalamus and basal ganglia involvement in JE is associated with high frequency of movement disorders, which may appear as transient form of parkinsonism Neurology Asia June 2008 and varying types of dystonia. Severe dystonia simulating status dystonicus have also been reported.34,36,37 Neurocysticercosis and JE coinfection has been reported from China and India.38,39,40 In a study on 163 JE patients, 37.4% had evidence of neurocysticercosis confirmed by antibodies in CSF, CT scan or autopsy.29 In MRI studies, similar observations have also been reported (Misra UK and Kalita J, Unpublished observation). The coexistence of JE and neurocysticercosis is attributed to the pivotal role of pig in the transmission of JE virus and Tenia solium. Pig is amplifying host of JE virus and intermediate host in the life cycle of Tenia solium. Neurocysticercosis may enhance the susceptibility of host to JE virus infection and could add to the seizure burden in JE patients. Seizures in Japanese encephalitis Figure 2A: Cranial MRI T1 sequence of a child with Japanese encephalitis and status epilepticus shows hyperintense lesion in thalamus bilaterally and frontoparietal cortical involvement. Seizures in JE have been noted by a number of investigators. These are partial motor or secondary generalized and appear at the onset or during the course of disease occurring more frequently in children. In a study, seizure was documented in 6.7% patients. 41 Isolated case report of Day 90 Figure 2B: EEG of the same child shows epileptiform discharges on the left side, some of which spread to right. diencephalic seizure has been reported in JE and are of interest because of involvement of thalamus and brain stem.42 In JE, seizures are less intractable then HSE.43 In a study, 30 out of 65 JE patients had seizures in the first week of encephalitis. The seizures were generalized tonic clinic in 17 and partial motor with secondary generalization in 13. Eleven patients had single seizure, 8 had two seizures and 11 had multiple seizures. Interictal EEG in the patients with seizure revealed theta to delta slowing in all and epileptiform discharges in 4 patients only. MRI carried out in 26 patients revealed bilateral thalamic lesion in 24, cortical in 7, basal ganglia in 8 and brainstem involvement in 3. In the seizure group, 3 patients died, 9 had poor, 8 partial and 9 complete recovery by 3 months. Presence of seizure in JE correlated with GCS score, focal weakness, EEG abnormality and cortical lesion on CT or MRI, though seizure was not associated with poor prognosis.44 Although seizure has been reported to be commoner in children41, in a comparative study of JE in adults and children, seizures were present 67.2% of adults and 56.7% of children, but this difference was not statically significant.46 The seizure was generally infrequent and easily controlled with phenytoin or carbamazepine monotherapy. 44 The experience of JE in children from Vietnam however was different. In a study on 144 JE patients, 134 children and 10 adults, 29% had seizures and 12% died. Of the 40 patients with witnessed seizures, 60% died or had severe sequelae compared to only 26% of 104 with no witnessed seizures. Patients with seizures were more likely to have elevated CSF opening pressure and signs of brain herniation.47 High frequency of seizure in Vietnamese study could be due to difference in the herd immunity as well as referral bias. The Indian study was from a tertiary care referral center where very sick patients with seizures could not have been referred.44,45 EEG changes in JE are nonspecific. In a study on 27 patients with JE, diffuse slowing of theta to delta range was the commonest (24), lateralized spike or spike wave discharges and alpha coma in 3 patients each. High frequency of slowing is attributed for thalamic involvement, lateralized epileptic discharges to cortical and alpha coma to the involvement of thalamus and brainstem, which is sufficient to produce loss consciousness but not enough to block the alpha activity. Alpha coma in JE may be common but its prognosis is not as bad as hypoxic coma or cardiac arrest. In 3 JE patients with alpha coma, 1 patient died and one each had partial and complete recovery.48 In another study on EEG in 56 patients revealed slowing of background activity in 35, unreactive slowing in 9, low amplitude in 1, burst suppression pattern in 1 and normal in 1 patient. Patients with grade 1 b had poor outcome compared to less severe EEG abnormality. Asymmetrical EEG pattern was not related to outcome. Seizures were documented in 20% of patients.47 Dengue Dengue is an important flavivirus with nearly 50 million cases occurring world wide mostly in Asia, Africa and South America. Most patients present with fever but some may have dengue hemorrhagic fever, dengue shock syndrome and dengue encephalopathy or encephalitis. Though dengue is regarded as a non neurotropic virus, a variety of neurological manifestations following dengue virus infection have been reported. Encephalopathy in dengue may be due to metabolic alterations, hypotension, hypoxia, hepatic or renal failure. Recently evidence of CNS invasion of dengue virus based on experimental, CSF antibody and PCR studies have been suggested.49,50 In a study on 24 dengue patients with neurological manifestations, 50% had altered sensorium; 5 of whom had seizures (generalized in 3, focal in one). In another study, 11 out of 17 patients had encephalopathy and 6 had acute flaccid paralysis (myositis). In the encephalopathy group 3 had seizures and one had myoclonus. CSF pleocytosis and EEG changes were present in 8 patients each. In the myositis group, creatinine kinase was raised in 5, electromyography (EMG) and muscle biopsy were consistent with myositis in one patient each. The patients with myositis improved completely within one month but in encephalopathy group 3 died and 1 had poor outcome. Dengue patients presenting with encephalopathy had more severe illness and worse outcome than those with myositis only. Dengue myositis may be an early or mild form of disease whereas encephalopathy may be a more severe form and some patients may have an overlapping clinical picture.51,52 The EEG changes in dengue virus infection are nonspecific; slowing occurs in 55% patients in a study on 24 dengue patients with neurological involvement. The EEG abnormality correlates with level of consciousness.51 St. Louis encephalitis St Louis encephalitis is one of the most common arboviral disease in USA in earlier series. It is spread by at least 3 different mosquitoes which Neurology Asia breed in stagnant water or irrigated fields, explaining both urban and rural distribution. It manifests with flu like illness followed by meningoencephalitis. Severity of disease and propensity of virus to infect the CNS increases with age.53 The disease often occurs in outbreaks and clinical manifestations are similar to West Nile encephalitis. Neurological sequelae are present in 5% of surviving patients. West Nile encephalitis West Nile encephalitis occurs in summer months. The most common neurological syndromes caused by West Nile Virus in New York city epidemic included encephalitis with muscle weakness (39%), aseptic meningitis (32%), encephalitis without muscle weakness (22%) and milder illness with fever and headache only (7%).54 Neuromuscular manifestations include polyradiculitis, axonal polyneuropathy simulating poliomyelitis or occasionally Guillain-Barre syndrome.55 Seizures is said to be uncommon in West Nile encephalitis..56 Eastern equine encephalitis Eastern equine encephalitis is a life threatening mosquito borne arboviral infection found mainly along the east and gulf coast of USA. Cases occur sporadically in small epidemics. Two hundred and twenty three cases were reported to Centers for Disease Control and Prevention during 1955 to 1993. It results in nonspecific clinical picture and diagnosis is based on CSF serology, PCR and brain tissue. The radiological findings are similar to JE. In a study on eastern equine encephalitis, MRI revealed thalamic and basal ganglia involvement in 71% each and brainstem in 43% patients. Cortical lesions, white matter changes and meningeal enlargement were less common. Seizures were reported in 18 patients (25%); 15 had generalized seizure; 3 had focal seizures with one secondary generalized and one had complex partial seizure. EEG revealed slowing except in 6 patients who had focal epileptiform discharges and periodic lateralized epileptiform discharges (PLEDs). Thirty six percent of patients died and 35% had moderate to severe sequelae.57 Nipah virus encephalitis Nipah virus is closely related to Hendra virus. Hendra virus was discovered in an outbreak in Australia in 1994. Nipah virus was first isolated in 1998-1999, where it resulted in an outbreak June 2008 of encephalitis in pig farmers of Malaysia and Singapore affecting about 300 patients.58 Nipah virus has high infection rate because half the patients have affected family members and for every 3 patients there was one asymptomatic infections. The reservoir of Nipah virus is fruit bat of Pteropus species. Half eaten fruits by bats may infect the pigs.59 Pig to pig transmission finally affects the human being working in pig farms. Outbreaks of Nipah virus encephalitis have also been reported from Siliguri, India and Bangladesh. The pathogenesis of Nipah virus encephalitis is thought to be due to vasculitis of medium and small sized vessels causing thrombosis and microinfarcts, and direct neuronal invasion.58 Nipah encephalitis affects all age groups; its incubation period is less than 2 weeks. The clinical manifestations are fever, headache, vomiting and altered sensorium. Brain stem involvement results in distinctive clinical features such as myoclonus, hypotonia, ataxia and autonomic changes. Segmental myoclonus occurs in onethird cases mostly in diaphragm and anterior neck muscles which is associated with high mortality. Nipah encephalitis has an unusual tendency for recurrence. About 10% patients suffer a second or even third episode months or years after recovery form the first attack (relapsed Nipah encephalitis). About 5% patients who either were asymptomatic or had a mild nonencephalitic illness may also develop late-onset Nipah encephalitis.60 Seizure is commoner in relapsed or late-onset Nipah encephalitis occurring in half the patients; however myoclonus is uncommon. The autopsy studies have revealed that relapsed / late-onset encephalitis is associated with presence of Nipah virus antigen detected by immuno-localization in brain with out vasculitis.61,62 In a study on 137 patients with Nipah encephalitis, 2.2% developed epilepsy in 8 years follow up. Risk of epilepsy is 1.8% in acute and 4% in late-onset Nipah encephalitis (Tan CT, unpublished observation). Cerebrospinal fluid shows pleocytosis and protein rise in 75% patients. IgM antibodies are present in all by 12 weeks and IgG by 4 weeks. Brain MRI in acute stage shows multiple disseminated small discrete hyperintense lesions best seen in FLAIR sequence particularly in sub-cortical and deep white matter suggesting microinfarct, which has been confirmed in postmortem studies.63 EEG abnormalities have been reported in 97% patients. It is commonly seen as continuous, diffuse symmetrical slowing of background with or without focal changes. The slowing corresponds to severity of illness. Bilateral periodic lateralized epileptiform discharges (BiPLEDs) are seen in 25% patients with acute encephalitis and correlated with coma and high mortality (all patients with BiPLEDs died by day 5).64 The mortality of Nipah encephalitis seems to be reduced by ribavirin.65 rate of 25%. Systemic manifestations such as coagulopathy and hepatic dysfunction are associated with high mortality. Influenza B is associated with seizures, PLEDs and focal temporal lobe abnormalities on MRI.71 MISCELLANEOUS VIRUSES Enteroviruses cause 40-60% of viral meningitis, most cases of acute flaccid paralytic and a small number of cases of encephalitis in children. With nearly successful eradication of poliovirus by vaccination, coxsackie and echo viruses are the responsible enteroviruses. Most enterovirus infections are asymptomatic. However, systemic manifestations include rash, respiratory symptoms, pleurodynia, carditis and diarrhea. Group A coxsackie virus causes herpengina. Coxsackie and echo virus is common cause of aseptic meningitis but occasionally causes encephalitis, cerebellitis, opsoclonus myoclonus syndrome and focal encephalitis.72 Rarely bilateral hippocampal lesions on MRI mimicking HSE have been reported.73 Enteroviruses can cause severe spinal and brainstem encephalitis in children.74 Seizure has been described in enterovirus 71 encephalitis.75 A number of other viruses can result in encephalitis and seizures. Some important viruses are briefly mentioned in the following section. Varicella zoster Chickenpox is a common self-limiting childhood infection. Sometimes in adults, chickenpox may be associated with encephalitis. Varicella zoster is also associated with uni-focal and multi-focal vasculopathy. Uni-focal large vessel vasculopathy usually affects elderly immuno-competent patients whereas muiti-focal vasculopathy affects elderly immuno-compromised patients. In the former, zoster is followed several weeks later by ipsilateral middle cerebral artery infarction due to retrograde spread of Varicella zoster via trigeminal system. Less typical presentation includes cerebral vasculopathy following remote site of infection e.g. sacral, progressive leucoencephalopathy or vasculitic optic neuropathy.66 Seizure is a feature of zoster encephalitis-vasculitis.67 The prognosis is good following acyclovir therapy. Mumps Mumps virus is a paramyxovirus and causes selflimiting febrile illness with parotitis. Neurological complications are common in mumps. CSF pleocytosis was present in 50% patients with uncomplicated parotitis who underwent lumbar puncture.68 Aseptic meningitis in mumps is self limiting and may persist up to one month. Before mumps vaccination, mumps encephalitis constituted 20-30% of encephalitis.69 Encephalitis generally occurs 1-2 weeks after the parotitis and manifests with fever, altered sensorium, seizures, focal weakness, abnormal movements and aphasia. Mumps encephalitis usually resolves by 1-2 weeks. The sequelae include focal weakness and seizures.69,70 Death occurs in 1-2% cases. Orchitis, parotitis and pancreatitis may or may not accompany CNS disease. Influenza Encephalitis is a rare complication of influenza A infection and is associated with mortality Enteroviruses Measles Measles is infrequently associated with encephalitis although subclinical form of CNS involvement demonstrated by EEG abnormalities in 50% cases.76 Measles encephalitis is usually nonfocal and presents during convalescence. Patients present with fever, seizures and altered mental state. Following measles encephalitis, although most patients survive, neurological sequelae are common. Diagnosis is usually on clinical grounds but can be confirmed serologically. Measles can also cause progressive sub-acute encephalitis in immune compromised patients77, acute disseminated encephalomyelitis (ADEM) and subacute sclerosing panencephalitis, which can also be associated with seizures. ACUTE DISSEMINATED ENCEPHALOMYELITIS (ADEM) Acute disseminated encephalomyelitis (ADEM) is a monophasic complication characterized by rapid onset of neurologic symptoms and signs following viral encephalitis in children and adults. ADEM occurs in 1 in 1000 measles infection with mortality as high as 25% and neurological sequelae in 25-40% of survivors.78 On the Neurology Asia other hand, the incidence of ADEM following varicella zoster and rubella infections are 1 in 10,000 and 1 in 20,000 respectively with lower occurrence of neurological sequelae compared to measles. In the tropical countries because of poor vaccination coverage, ADEM continues to be a common health problem. The important pathogens associated with ADEM include measles, herpes simplex, HIV, human herpes virus, mumps, influenza, Epstein Barr and coxsackie viruses. The frequency and severity of ADEM following viral infection is highly variable. ADEM has also been reported following Mycoplasma pneumoniae and Legionella, Cincinnatiensis. The neurologic signs and symptoms include paresthesia, pain, weakness, spasticity, incoordination, dysarthria and dysphagia. Seizure may occur in severe cases and its incidence ranges between 4% and 35%.79,80 Seizures in ADEM following measles infection may be as high as 50%. Some studies have reported high incidence (35%) of partial seizures and status epilepticus in ADEM.76 The management of seizures in ADEM is same as encephalitis. STATUS EPILEPTICUS IN ENCEPHALITIS Encephalitis is an important cause of refractory seizures and status epilepticus. There is paucity of systemic prospective study of status epilepticus in encephalitis. Herpes simplex, JE, West Nile, influenza, Papova virus have been reported to result in status epilepticus. In last 3 years, our studies on status epilepticus revealed 31 out of 101 cases (30%) were due to encephalitis, another 25% were from other CNS infection. The etiologies of the encephalitis were JE in 9, HSE in 1, dengue in 1, and in 17 patients no etiology agent could be established. Generalized convulsive status epilepticus was the commonest (21), followed by partial status epilepticus with secondary generalization (5) and nonconvulsive status epilepticus in 4 patients. The seizures were difficult to control. Nine of our patients had refractory status epilepticus, and 10 died. MRI changes and Glasgow Coma Scale were related to outcome. We concluded that status epilepticus in encephalitis requires aggressive therapy. (Misra UK, Kalita J, unpublished observations) MANAGEMENT OF SEIZURES IN VIRAL ENCEPHALITIS Seizures can occur at any stage of encephalitis, from being the presenting feature to late sequelae. Their severity, frequency and response to 10 June 2008 treatment are variable according to the etiology and other factors. There are limited large-scale studies on management of seizures in encephalitis. The recommendations on management of seizures related to encephalitis, including the section below are largely based on clinical experience, and experience from other causes of acute symptomatic seizures. General management Other than the use of antiepileptic drugs to arrest the seizures, other general measures including the use of antibiotic and antiviral drugs, electrolyte and fluid management, blood pressure monitoring, respiratory and other aspects of intensive care are equally important. Many antibiotics often used in co-existent infections such as quinolones, third or fourth generation cephalosporins and meropenem may precipitate or aggravate seizures. Urgency of seizure control and choice of antiepileptic drugs The significance of single seizure in encephalitis is obviously dependant on the type of infection, and the clinical status of the individual patient. Seizures are common in HSE and is associated with poor outcome.13 In a Vietnamese study on JE, seizures were again common, had high mortality, poor sequele as well as brain herniation.47 These argue for urgent measures even after first seizure in encephalitis. We have found in majority of JE, the seizures are easily controlled by phenytoin or carbamazepine monotherapy.44 However, when intravenous antiepileptic drugs are used, one should be aware of the potential deleterious effect of respiratory suppression, and lowering of blood pressure on the brain with high intracranial pressure. Management of status epilepticus As mentioned above, encephalitis is an important cause of status epilepticus, and is associated with high mortality. Diagnosis of convulsive seizures is easy, but subtle seizures and nonconvulsive seizures require EEG. The subtle seizures manifest with eye deviation, nystagmus, hyperventilation and subtle tremulous movement of fingers, chin, and eyelids. Management of status epilepticus in encephalitis is similar to status epilepticus from other causes. Prophylactic antiepileptic drug treatment In encephalitis from HSV and JE, where there is high incidence of seizures, which may contribute to the high mortality and morbidity, one may argue for the routine use of prophylactic antiepileptic drugs during acute encephalitis, without clinical seizures. However, the benefit of such a practice awaits confirmation from further studies. Duration of use of antiepileptic drug treatment In encephalitis with seizures that is easily controlled by antiepileptic drugs, there is no study to address the issue of the duration to continue the antiepileptic drugs. Based on the consideration that the seizures is related to acute pathology, the antiepileptic drugs should thus cover the duration of active pathology, which in most cases, is less than 3 months. ACKNOWLEDGEMENT We acknowledge Rakesh Kumar Nigam for secretarial help. REFERENCES 1. Johnson RT. Acute encephalitis. Clin Infect Dis 1996; 23: 219-24. 2. Koskiniemi M, Rantalaiho T, Piiparinen H, et al. Infections of the central nervous system of suspected viral origin: a collaborative study from Finland. J Neurovirol 2001; 7: 400-8. 3. Downs AGARBO viruses. In: Evans AS, ed: Viral infections of humans: epidemiology and control. NewYork, Planum, 1989: 105-32. 4. Annegers JF, Hauser WA, Beghi E, Nicolosi A, Kurland LT. The risk of unprovoked seizures after encephalitis and meningitis. Neurology 1988; 38: 1407-10. 5. Whitley RJ. Herpes simplex virus. In: Schield WM, Whitley RJ, Durack DT, eds: Infections of the central nervous system, 2nd ed. Philadelphia: LippincottRaven, 1997: 73–89. 6. Koskiniemi M, Piiparinen H, Mannonen L, Rantalaiho T, Vaheri A. Herpes encephalitis is a disease of middle aged and elderly people: polymerase chain reaction for detection of herpes simplex virus in the CSF of 516 patients with encephalitis. The Study Group. J Neurol Neurosurg Psychiatry 1996; 60: 174-8. 7. Aurelius E, Johansson B, Skoldenberg B, Forsgren M. Encephalitis in immunocompetent patients due to herpes simplex virus type 1 or 2 as determined by type-specific polymerase chain reaction and antibody assays of cerebrospinal fluid. J Med Virol 1993; 39: 179-86. 8. Baringer JR, Pisani P. Herpes simplex virus genomes in human nervous system tissue analyzed by polymerase chain reaction. Ann Neurol 1994; 36: 823-9. 9. Johnson RT. Viral infections of the nervous system, 2nd ed. Philadelphia, Lippincott Raven, 1998: 13368. 10. Damasio AR, Van Hoesen GW. The limbic system and the localisation of herpes simplex encephalitis. J Neurol Neurosurg Psychiatry 1985; 48: 297-301. 11. Fodor PA, Levin MJ, Weinberg A, Sandberg E, Sylman J, Tyler KL. Atypical herpes simplex virus encephalitis diagnosed by PCR amplification of viral DNA from CSF. Neurology 1998; 51:554-9. 12. McGrath N, Anderson NE, Croxson MC, Powell KF. Herpes simplex encephalitis treated with acyclovir: diagnosis and long term outcome. J Neurol Neurosurg Psychiatry 1997; 63:321-6 13. Hsieh WB, Chiu NC, Hu KC, Ho CS, Huang FY. Outcome of herpes simplex encephalitis in children. J Microbiol Immunol Infect 2007; 40:34-8. 14. Chen SF, Huang CC, Wu HM, Chen SH, Liang YC, Hsu KS. Seizure, neuron loss, and mossy fiber sprouting in herpes simplex virus type 1-infected organotypic hippocampal cultures. Epilepsia 2004; 45: 322-32. 15. Chen YJ, Fang PC, Chow JC. Clinical characteristics and prognostic factors of postencephalitic epilepsy in children. J Child Neurol 2006; 21: 1047-51. 16. Yamada S, Kameyama T, Nagaya S, Hashizume Y, Yoshida M. Relapsing herpes simplex encephalitis: pathological confirmation of viral reactivation. J Neurol Neurosurg Psychiatry 2003; 74: 262-4. 17. Hokkanen L, Launes J. Cognitive recovery instead of decline after acute encephalitis: a prospective follow up study. J Neurol Neurosurg Psychiatry 1997; 63:222–7. 18. Jay V, Hwang P, Hoffman HJ, Becker LE, Zielenska M. Intractable seizure disorder associated with chronic herpes infection. HSV1 detection in tissue by the polymerase chain reaction. Childs Nerv Syst 1998; 14:15-20. 19. Asenbauer B, McEntagart M, King MD, Gallagher P, Burke M, Farrell MA. Chronic active destructive herpes simplex encephalitis with recovery of viral DNA 12 years after disease onset. Neuropediatrics 1998; 29:120-3. 20. Cornford ME, McCormick GF. Adult-onset temporal lobe epilepsy associated with smoldering herpes simplex 2 infection. Neurology 1997; 48: 425-30. 21. Millner M. Complicated febrile convulsion vs herpesencephalitis. Pediatr Padol 1993; 28:A7-9. 22. Wu HM, Huang CC, Chen SH, Liang YC, Tsai JJ, Hsieh CL, Hsu KS. Herpes simplex virus type 1 inoculation enhances hippocampal excitability and seizure susceptibility in mice. Eur J Neurosci 2003; 18:3294-304. 23. Solomon T. Flavivirus encephalitis. N Engl J Med 2004; 351: 370-8. 24. Mostashari F, Kulldorff M, Hartman JJ, Miller JR, Kulasekera V. Dead bird clusters as an early warning system for West Nile virus activity. Emerg Infect Dis 2003; 9:641-6. 25. O’Leary DR, Marfin AA, Montgomery SP, et al. The epidemic of West Nile virus in the United States, 2002. Vector Borne Zoonotic Dis 2004; 4: 61-70. 26. Monath TP. Epidemiology. In: Monath TP, ed: St Louis encephalitis. Washington, D.C.: American Public Health. 1980:239-312. 27. Nash D, Mostashari F, Fine A, et al. The outbreak 11 Neurology Asia 28. 29. 30. 31. 32. 33. 34. 35. 36. 37. 38. 39. 40. 41. 42. 43. 44. 45. 46. 12 of West Nile virus infection in the New York City area in 1999. N Engl J Med 2001; 344: 1807-14. Brinker KR, Monath TP. The acute disease. In: Monath TP, ed: St. Louis encephalitis Washington, D.C.: American Public Health. 1980:503-34. Desai A, Shankar SK, Jayakumar PN, Chandramuki A, Gourie-Devi M, Ravikumar BV, Ravi V. Co-existence of cerebral cysticercosis with Japanese encephalitis: a prognostic modulator. Epidemiol Infect 1997; 118: 165-71. Libraty DH, Nisalak A, Endy TP, Suntayakorn S, Vaughn DW, Innis BL. Clinical and immunological risk factors for severe disease in Japanese encephalitis. Trans R Soc Trop Med Hyg 2002; 96:173-8. Kalita J, Misra UK. Comparison of CT scan and MRI findings in the diagnosis of Japanese encephalitis. J Neurol Sci 2000; 174: 3-8. Zimmerman HM. Pathology of Japanese encephalitis. Am J Pathol 1946; 22: 965-91. Shankar SK, Rao TV, Mruthyunjayanna BP, Gourie Devi M, Deshpande DH. Autopsy study of brains during an epidemic of Japanese encephalitis in Karnataka. Indian J Med Res 1983; 78:431-40. Misra UK, Kalita J. Movement disorders in Japanese encephalitis. J Neurol 1997; 244: 299-303. Solomon T, Kneen R, Dung NM, et al. Poliomyelitislike illness due to Japanese encephalitis virus. Lancet 1998; 351:1094-7. Kalita J, Misra UK. Markedly severe dystonia in Japanese encephalitis. Mov Disord 2000; 15: 116872. Misra UK, Kalita J. Prognosis of Japanese encephalitis patients with dystonia compared to those with parkinsonian features only. Postgrad Med J 2002; 78: 238-41. Hsu YK. Cerebral cysticercosis and acute poliomyeloencephalitis. Chinese Med J 1940;57: 318-9. Lin YF, Teng CL, Liu-Kai. Chinese Med J 1977, 75:101. Quoted by Gourie Devi M, Ravi V, Shankar SK. Japanese encephalitis an overview. Clifford Rose F ed: Recent advances in Tropical Neurology. Elsevier. 1995:211-35. Shankar SK, Rao TV, Mruthyunjayanna BP, Gourie Devi M, Deshpande DH. Autopsy study of brains during an epidemic of Japanese encephalitis in Karnataka. Indian J Med Res 1983;78:431-40. Gourie Devi M, Ravi V, Shankar SK. Japanese encephalitis an overview. Clifford Rose F, ed: Recent advances in Tropical Neurology. Elsevier. 1995: 211-35. Misra UK, Nag D, Shukla R, Kar AM. Parkinsonism and diencephalic epilepsy as sequelae of Japanese encephalitis. Neurol Ind 1980; 28: 252. Misra UK, Kalita J. A comparative study of Japanese and Herpes simplex encephalitis. Electromyog Clin Neurophysiol 1998; 38: 41-6. Misra UK, Kalita J. Seizures in Japanese encephalitis. J Neurol Sci 2001; 190: 57-60. Kalita J, Misra UK. EEG in Japanese encephalitis: A clinicoradiological correlation. Electroencephalogr Clin Neurophysiol 1998; 106: 238-43. Kalita J, Misra UK, Pandey S, Dhole TN. A June 2008 47. 48. 49. 50. 51. 52. 53. 54. 55. 56. 57. 58. 59. 60. 61. 62. 63. 64. 65. comparison of clinical and radiological findings in adults and children with Japanese encephalitis. Arch Neurol 2003; 60:1760-4. Soloman T, Dung MN, Kneen R , Thao LTT, Gainsborough M, Nisalak A, Day NPT Kirkham FJ, Voughn DW, Smith S, White NJ. Seizure and raised intracranial pressure in Vietnamese patients with Japanese encephalitis. Brain 2002;125:1084-93. Misra UK, Hashmi AA, Kalita J. Alpha coma in Japanese encephalitis. Neurol India 1995; 43: 113-4. Lum LC, Lam SK, Choy YS, George R, Harun F. Dengue encephalitis: a true entity? Am J Trop Med Hyg 1996; 54: 256–59. Solomon T, Dung NM, Vaughn DW, et al. Neurological manifestations of dengue infection. Lancet 2000; 355: 1053–9. Misra UK, Kalita J, Syam UK, Dhole TN. Neurological manifestations of dengue virus infection. J Neurol Sci 2006; 244:117-22. Kalita J, Misra UK. EEG in dengue virus infection with neurological manifestations: A clinical and CT/ MRI correlation. Clin Neurophysiol 2006; 117:225256. Powell RE, Blakey DL. St Louis encephalitis. JAMA 1977; 237:2294-98. Hinson VK, Tyor WR. Update on viral encephalitis. Curr Opin Neurol 2001; 14:369-74. Ahmed S, Libman R, Wesson K, Ahmed F, Einberg K. Guillain Barre syndrome: An unusual presentation of West Nile virus infection. Neurology 2000; 55: 144-6. Petersen LR, Roehrig JT, Sejvar JJ. West Nile virus in the Americas. In: Fong W, Alibek K, eds: New and evolving infections of the 21st century. Springer, 2007: 3-56. Deresiewicz RL, Thaler SJ, Hsu L, Zamani AA. Clinical and neuroradiographic manifestations of Eastern equine encephalitis. New Engl J Med 1997; 336:1867-74. Chua KB, Goh KJ, Wong KT, Kamarulzaman A, et al. Fatal encephalitis due to Nipah virus among pigfarmers in Malaysia. Lancet 1999; 354:1257-59. Chua KB, Koh CL, Hooi PS, et al. Isolation of Nipah virus from Malaysian flying-foxes. Microbs Infect 2002; 4:145-51. Chong HT, Tan CT. Relapsed and late-onset Nipah encephalitis, a report of three cases. Neurol J Southeast Asia 2003; 8:109-112. Wong KT, Shieh WJ, Kumar S, et al. Pathology and pathogenesis of an emerging paramyxoviral zoonesis. Am J Pathol 2002; 161: 2153-67. Tan CT, Goh KJ, Wong KT, et al. Relapsed and late-onset Nipah encephalitis. Ann Neurol 2002; 51:703-8. Ahmad Sarji S, Abdullah BJJ, Goh KJ, Tan CT, Wong KJ. MR imaging features of Nipah encephalitis. AJR 2000; 175:437-42. Chew NK, Goh KJ, Tan CT, Ahmad Sarji S, Wong KT. Electroencephalography in acute Nipah encephalitis. Neurol J Southeast Asia 1999; 4: 45-51. Chong HT, Kamarulzaman A, Tan CT, et al. Treatment of acute Nipah encephalitis with ribavarin. Ann Neurol 2001; 49:810-13. 66. Gilden DH, Lipton HL, Wolf JS, Akenbrandt W, Smith JE, Mahalingam R, Forghani B. Two patients with unusual forms of varicella-zoster virus vasculopathy. N Engl J Med 2002; 347:1500-3. 67. Gilden DH, LaGuardia JJ. Varicella-Zoster virus infection. Nath A, Berger JR, eds: Clinical Neuroviology. Marcel Dekker 2003; 129-53. 68. Bang Ho, Bang J. Involvement of central nervous system in mumps. Acta Med Scand 1943; 113:487-90 69. Russell RR, Donald JC. The neurological complications of mumps. Br Med J 1958; 2:27-30. 70. Levitt LP, Rich TA, Kinde SW, Lewis AL, Gates EH, Bond JO. Central nervous system mumps. A review of 64 cases. Neurology 1970; 20:829-34. 71. Yoshiokawa H, Yamazuki S, Watanabe T, Abe T. Study of influenza virus associated encephalitis /encephalopathy in children during 1997 to 2000 influenza seasons. J Child Neurol 2001; 16:885890. 72. Johnson RT. Meningitis, encephalitis and poliomyelitis In: Viral infections of the nervous system 2nd ed Newyork, Lippincort Raven 1998; 87-132 73. Nakajima H, Hosoya M, Takahashi Y, et al. A chronic progressive case of enteroviral limbic encephalitis associated with autoantibody to glutamate receptor. Eur Neurol 2007; 57:238–40. 74. Huang CC, Liu CC, Chang YC, Chen CY, Wang ST, Yeh TF. Neurologic complications in children with enterovirus 71 infection. N Engl J Med 1999; 341:936-42. 75. Chang LY, Shih SR, Huang LM, Lin TY. Enterovirus 71 encephalitis. In: Fong W, Alibek K, eds: New and evolving infections of the 21st century. Springer, 2007: 295-325. 76. Gibbs FA, Gibbs EL, Carpenter PR, Spies HW. Electroencephalographic abnormality in “uncomplicated” childhood diseases. JAMA 1959; 171:1050-55. 77. Chong HT, Ramli N, Wong KT, et al. Subacute measles encephalitis: A case of long term survival with follow-up MR brain scans. Neurol Asia 2007;12:121-5. 78. Struve O, Zambir SS. Pathogenesis, diagnosis and treatment of acute disseminated encephalomyelitis. Curr Opin Neurol 1999; 12:395-401. 79. Hynson JL, Kornberg AJ, Coleman LT, Shield L, Harvey AS, Kean MJ. Clinical and neuroradiologic features of acute disseminated enepahalomyelitis in children. Neurology 2001;56:1308-12. 80. Tenembaum S, Chamoles N, Fejerman N. Acute disseminatalomyelitis aerm folowup study of 84 pediatric patients. Neurology 2002; 59:1224-31. 13










© Copyright 2026