
Missouri Organization of Defense Lawyers
Missouri Organization of Defense Lawyers P.O. Box 1072 Jefferson City, MO 65102 Phone: (573) 636-6100 Website: www.modllaw.com Spring, 2009 MODL President’s Message by Martin J. Buckley, MODL President Buckley & Buckley, L.L.C.; St. Louis, MO The Annual Meeting is fast approaching. Block these dates on your calendar now: June 4, 5 and 6, 2009. The Annual Meeting will feature outstanding CLE programs, networking opportunities and fun for the whole family. As usual, the most competitive golf tournament in the state will take place on Saturday. A limited number of rooms will be reserved at a special rate at the Hilton Branson Convention Center, so early reservations are recommended. Be on the lookout for the brochure with reservation information, which will be mailed to all members very soon. Congratulations to the citizens of Greene County who voted to adopt the Missouri Non-Partisan Court Plan in the November general election. Despite a well-financed campaign opposing adoption of the plan, the voters made the right choice. While MODL contributed to the effort in Greene County, the real credit for this success goes to the members of the Greene County Bar who spearheaded this effort. As noted in a previous newsletter, a significant part of MODL’s mission is to work for improvement in the civil adversary system of jurisprudence and to promote improvements in the administration of justice. That is why MODL has continued to work to assure that we will have a qualified, unbiased judiciary through its defense of the Missouri Non-Partisan Court Plan. (If you spend any time speaking with defense lawyers from states where appellate judges are elected, you can appreciate the importance of maintaining the Missouri Plan.) MODL also works for improvement in the administration of justice through its assistance to the National Foundation for Judicial Excellence (NFJE). The NFJE is an independent, 501(c)(3) charitable foundation which provides judges with educational programs to enhance the rule of law and administration of justice. It was created in 2004 by the Defense Research Institute. Since 2005, NFJE has hosted an annual symposium on developments in the law. These symposia are attended by an average of 130 state judges each year. These unbiased presentations give state appellate court judges an opportunity to attend high quality seminars which they might not otherwise be able to attend because of state budgetary constraints. How unbiased are these symposia? Last year’s event featured a presentation by noted plaintiff’s lawyer Edward D. “Chip” Robertson, Jr., a former member of the Missouri Supreme Court. As a charitable organization, NFJE needs our support. It exists on contributions from the various State and Local Defense Organizations and contributions from DRI members. On your DRI dues statement, there is an option to contribute $25 to NFJE. Please support NFJE by making the $25 contribution on your DRI payment. As most of us do not make the physical arrangements to cut the check, please make sure your office manager or accounts payable employees know that you want to contribute to NFJE. The service it provides to the administration of justice is of benefit to all of us. Finally, just after Christmas, MODL lost a great friend and colleague. Chuck McPheeters, the secretary of MODL, passed away on December 28. He was a skilled lawyer, a great friend, and a delightful companion in any circumstance. He will be sorely missed and fondly remembered in many stories for years to come, especially by those of us who worked with him on the Board. Requiescat in pace. Get Ready for Summer! MODL Annual Meeting June 4 - 6, 2009 Hilton Branson Convention Center Medical Malpractice Legal Update by Michael J. Smith and Tricia J. Mueller Lashly &Baer St. Louis, MO This article provides a summary of some of the significant Missouri court decisions affecting medical malpractice litigation handed down in the past 12 months. Res Ipsa Loquitur Statute of Limitations – Tolling Sides v. St. Anthony’s Medical Center, 258 S.W.3d 811 (Mo. banc 2008) State ex rel. Bloomquist v. Schneider, 244 S.W.3d 139 (Mo. banc 2008) Plaintiff Janice Sides underwent a lumbar laminectomy with spinal fusion at St. Anthony’s Medical Center. Three days after being discharged she learned that she was infected with e-coli bacteria. She filed suit in June 2005, and her three amended petitions alleged that the infection was caused by one of various failures to take standard infection precautions before, during, and after the operation or by perforation of her bowel. In her Third Amended Petition, Plaintiff alleged a res ipsa loquitur theory against Defendants on the basis that an infection at the surgical site itself does not occur in the absence of negligence. She claimed that the healthcare providers had exclusive joint control, greater knowledge of the possible causes of the infection, and that they infected her. In reliance on Hasemeier v. Smith, 361 S.W.2d 697 (Mo. banc 1962) and Spears v. Capital Region Medical Center, Inc., 886 S.W.3d 58 (Mo. App. 2002), Defendants moved to dismiss, arguing that Plaintiffs could not proceed on the theory of res ipsa loquitur and were required to assert a specific negligence theory in a medical negligence case. The trial court agreed, and the case was dismissed and appealed. The Court of Appeals affirmed the trial court’s dismissal. Leiloni Popoalii sued 11 healthcare providers, including Dr. Raymond Bloomquist, alleging that they negligently failed to diagnose and treat her meningitis while she was in their care between March 19 and July 2, 2004. Ms. Popoalii filed her suit on July 31, 2006. The healthcare providers all moved to dismiss the Petition on the grounds that it was barred by the two-year medical malpractice statute of limitations, section 516.105, RSMo. Subsequently, Ms. Popoalii filed an Amended Petition alleging that Dr. Bloomquist changed his residence from Missouri to Kansas in approximately February 2006 and, therefore, section 516.200, which tolls the statute of limitation as to a Missouri resident who moves out of the state during the statute of limitations, prevented Dr. Bloomquist from using the statute of limitations as a defense. Dr. Bloomquist argued that the tolling statute was unconstitutional as applied to him because it violated the commerce clause. The Supreme Court held that section 516.200 applies only to a subclass of non-resident defendants – those who became non-residents of Missouri after the statute of limitations began to run and, thereby, imposes a greater burden on the out-of-state defendant than it does on resident defendants. As such, it burdens Dr. Bloomquist’s ability to move from state to state, which violates the commerce clause. Ms. Popoalii argued that tolling was a reasonable restriction on interstate commerce because it was harder to locate and serve an out-of-state resident than service on a resident of Missouri. The Court held that there was no showing by Ms. Popoalii that it was difficult to find Dr. Bloomquist and added that she could have filed suit against Dr. Bloomquist and then attempted to locate him. Additionally, Dr. Bloomquist remained fully amenable to a lawsuit under Missouri’s Long Arm Statute, section 506.500, even after his change of residence. Therefore, the Court held that the application of the tolling provision of section 516.200 to persons who move their residence out of Missouri is unconstitutional, thereby barring Ms. Popoalii’s claim against Dr. Bloomquist. The Supreme Court reversed and remanded the case. The Missouri Supreme Court adopted the approach of the Restatement (Second) of Torts, Section 238D, which allows the use of an expert witness’ testimony to show that an event usually does not occur without negligence. Further, the Court added that, where a plaintiff is unable to show that a specific act of negligence of the defendants caused his or her injury, but is able to show (1) that all of the potential causes were within the control or right to control of the Defendants ,and (2) the Defendants had greater access to knowledge of the cause of the injury than the Plaintiff, and (3) a medical expert testified that such an injury does not occur in the absence of negligence of the Defendant, the Plaintiff has made a prima facie case for medical malpractice. The Court stated that, as in other types of res ipsa loquitur cases, this doctrine simply allows a plaintiff who can show that the injury does not occur in the absence of negligence to present to the jury an inference that the defendants were negligent. The defendants then can rebut that inference with evidence that they were not negligent. Trial – Jury Selection – Challenges for Cause Joy v. Morrison, 254 S.W.3d 885 (Mo. banc 2008) Plaintiff appealed a defense verdict in this medical malpractice case on the sole ground that the trial court improperly denied Plaintiff’s challenge for cause of venireperson “Malpractice” >p3 ~2~ Malpractice claimed that Dr. Morrison failed to properly diagnose and treat his sternal instability. The jury awarded Edgerton monetary damages, and Dr. Morrison appealed. Charles Shirkey. Mr. Shirkey made statements in voir dire to the effect that, if a physician makes a mistake, one should just live with the results, that he would probably be biased for the physicians, and that he had strong negative feelings about the amounts of money people sought to recover in lawsuits. However, he also claimed he could put those feelings out of his mind, that he could be fair, and he could award damages that he thought were fair and reasonable. On appeal, Dr. Morrison raised two points of error relating to jury instructions. Dr. Morrison first claimed that the trial court erred in submitting a jury instruction because it failed to track Plaintiff’s theory of the case. The instruction discussed treating the sternum with “rigid fixation.” However, the term “rigid fixation” was not defined within the jury instruction, nor was it defined in the evidence at trial. The Southern District found that Plaintiff’s expert never used “rigid fixation” at trial, and the jury could have considered a rewiring of the sternum to be among methods capable of providing a “rigid fixation.” The court stated that the instructions allowed for a prejudicial roving commission by the jury and, therefore, the judgment was reversed and remanded. The Court of Appeals noted that the trial court had broad discretion to determine the juror’s qualifications based on its ability to observe the demeanor and credibility of prospective jurors. The Court of Appeals held that the trial court had no duty to independently voir dire Mr. Shirkey and did not abuse its discretion in declining Plaintiff’s request to strike him from the panel. On transfer to the Supreme Court, Plaintiff claimed that during voir dire, Mr. Shirkey did not recant his strong feelings and biases regarding lawsuits in general, nor was he rehabilitated by counsel on those issues. The Supreme Court found that Mr. Shirkey stated that, while he would have a problem awarding a substantial amount of money, there was no specific amount that he thought was per se excessive and, while he probably would be biased for the doctors, he could be persuaded in the other direction. However, he also conceded his opinions could affect his ability to listen to the experts and give their testimony credence. On questioning by Defendants’ counsel, Mr. Shirkey admitted that, if he did find negligence, he would be able to award damages in favor of Plaintiff and, if he did not find negligence, he would be able to find in favor of the physicians. He was also asked if he could be fair and unbiased if he were selected for the jury, and he responded that he could be fair and that neither side had a real advantage in his opinion. The Supreme Court held that, while Mr. Shirkey may have expressed a general feeling against excessive lawsuits, it was not clear that it translated into a bias against Plaintiff. Additionally, mere equivocation was not enough to disqualify a juror and, if the challenged venireperson subsequently reassured the court that he could be impartial, the bare possibility of prejudice would not deprive the trial court of its discretion to strike the venireperson. As such, the Court held that the trial court did not abuse it discretion in failing to strike Mr. Shirkey for cause. Dr. Morrison also attacked the verdict form that was submitted to the jury. The verdict form, based on MAI 36.21, stated in pertinent part, “On the claim of Plaintiff [Edgerton] for personal injuries against Defendant [Dr. Morrison], as submitted by Instruction No. 11, we, the undersigned jurors, find in favor of, [Edgerton] or [Morrison]. Dr. Morrison argued that the inclusion of the phrase “as submitted by Instruction No. 11” constituted a deviation from MAI 36.21 and, therefore, he was prejudiced. Plaintiff argued, however, that the phrase was properly submitted as an identifying phrase, as discussed under the notes section for use of MAI 36.21. The notes provide that the verdict form will contain a descriptive phrase describing and identifying the claim submitted by the particular package which would be the claim to which the verdict was applicable. The identifying phrase should be non-inflammatory and as neutral as possible and should avoid the assumption of disputed facts. The note also references MAI 2.01 for examples of appropriate identifying phrases. The court concluded that MAI 2.01 recommends that it briefly describe in words the nature of the claim and does not contain a reference to an instruction as used in this case. The Southern District held that the tendered verdict form already contained an identifying phrase consistent with the examples listed in MAI 2.0 when it stated “on the claim of Plaintiff for personal injuries against Defendant” and, therefore, the deviation was unnecessary and erroneous, but the court did not reach the question of whether the error was prejudicial. Jury Instructions Edgerton v. Morrison, et al., 2008 WL 4595367 (Mo. App. S.D. October 16, 2008) (from page 2) Standing and Relation Back This is a medical malpractice case in which the Plaintiff, Edgar Edgerton, underwent cardiac bypass surgery, requiring Dr. Morrison to cut Plaintiff’s sternum from bottom to top and then rewire it after completing the bypass. During his post-operative examination, Plaintiff complained of a rash at the surgical site and a “gritting” feeling in his chest. Dr. Morrison found that Plaintiff’s sternum was stable and referred him to a dermatologist. When Plaintiff continued to have chest pains, he saw Dr. Morrison again, who determined that his sternum was well healed. He subsequently obtained a second opinion from Dr. Hugh Lundman, who diagnosed Edgerton as having an unstable sternum that was possibly infected and required an operation. During the operation, it was found that his sternum had become necrotic and was destroyed. Plaintiff ~3~ Peyton v. Bellefontaine Gardens Nursing & Rehab, Inc., 246 S.W.3d 914 (Mo. banc 2008) Plaintiff, Sharon Peyton, sued a nursing home and several John Doe Defendants to recover damages for the wrongful death of her grandmother. Defendants moved to dismiss, arguing that Plaintiff lacked standing under Section 537.080, RSMo, because she was not within the class of persons entitled to bring the wrongful death action since her mother, Mary Jo Williams, was alive and had standing to sue. Plaintiff subsequently moved for leave to file a Second Amended Petition naming her mother in the case caption as “Mary Jo Williams, by and through Sharon Peyton, her Attorney In “Malpractice” >p4 Malpractice (from page 3) Fact.” During this time, the three-year statute of limitations expired. Therefore, the trial court overruled the motion to amend and dismissed the case, stating that the court now lacked jurisdiction over a case originally brought by one with no standing and that an amendment to add or substitute a proper party could not relate back to the original Petition so as to save the action once the statute of limitations expired. Plaintiff contended, however, that she did have standing as her mother’s attorney-in-fact so that the Second Amended Petition related back to the time of the original filing. evidence from Plaintiffs’ expert that indicated the expert was forming his opinion according to the proper definition of negligence. Upon reviewing the testimony as a whole, the Court believed the expert’s opinion was specific to what a thyroid surgeon should do when performing the thyroidectomy and the specific reasons for the surgery. The expert’s opinion was not a vague reference to the standard of care or what he perceived as his own standard of care. As such, the verdict was affirmed. Hospital Bylaws The Supreme Court agreed with Peyton’s analysis under Rule 55.33(c) and therefore reversed and remanded. Specifically, if a claim asserted in the amended petition arose from the same occurrence set forth or attempted to be set forth in the original pleading, the amendment relates back to the date of the original pleading. The Court also cited Forehand v. Hall, 355 S.W.2d 940 (Mo. 1962), which sets forth the rule that, where a wrongful death suit was timely filed by a party with a legal or beneficial interest, but who lacked authority to maintain the suit for want of a court appointment, the suit was safe from the running of the statute of limitations by substitution of a Plaintiff suing in the proper capacity because it related back to the original filing date. However, if the party filing the original petition lacked the legal or beneficial interest, then substituting the proper plaintiff does not relate back. In this case, the Supreme Court believed that Peyton had a legal or beneficial interest in the case because she was the attorney-in-fact for her mother and, therefore, it should relate back to the original filing date. Defendants attempted to argue that the original and First Amended Petition made no mention of Plaintiff’s status as an attorney-in-fact, but the Court found that paragraph 5 of the original Petition stated that notice was provided to the other surviving heirs and specifically mentioned Ms. Williams. Since she was the attorney-in-fact for Ms. Williams and notice had been provided to the Defendants of Williams’ interest in the case, Plaintiff had a legal and beneficial interest in the suit. Expert Testimony Hickman v. Branson Ear, Nose, and Throat, Inc., 256 S.W.3d 120 (Mo. banc 2008) In this medical malpractice case, Plaintiff, Roger Hickman, alleged negligence in the failure to remove his entire thyroid after finding a mass. On appeal from a jury verdict in favor of Plantiff, Defendants argued that Hickman failed to elicit expert testimony to define the phrase “standard of care” so that the jury could be properly informed of the meaning of the phrase. The Court of Appeals reversed the verdict in favor of Plaintiff, announcing that the Plaintiff failed to make a submissible case and noted that the definition of negligence requires a showing of a deviation from the accepted standard of care that other healthcare providers would use in the same or similar circumstance. The standard must be objective and could not be based upon the personal opinion of the expert. The Missouri Supreme Court disagreed with the Court of Appeals’ ruling and determined that Plaintiffs made a submissible case despite their failure to use the exact definition as set forth in the MAI Instruction 11.06. The Court held that there was sufficient ~4~ Egan v. St. Anthony’s Medical Center, 244 S.W.3d 169 (Mo. banc 2008) This is a non-medical malpractice case in which the Plaintiff surgeon, Dr. Robert Egan, had his privileges at St. Anthony’s Medical Center suspended. Dr. Egan appealed the findings to an appellate committee at the hospital which, according to St. Anthony’s bylaws, was comprised of three members of St. Anthony’s Board of Directors and three physicians selected by Dr. Egan. According to the bylaws, the decision of the appellate committee was to be based solely on the record from the evidentiary hearing. Dr. Egan alleged that the appellate committee, however, heard new testimony regarding his professional competence from at least one of its members who testified that he himself was critical of Dr. Egan based upon information he had heard at other hospitals and his own personal interactions. Another physician on the committee objected to the testimony for the reason that it was prejudicial and forbidden by the bylaws. The committee chairman overruled the objection and adopted the findings of the hearing committee. Dr. Egan subsequently filed suit seeking injunctive relief and reinstatement of his privileges pending a new hearing. In Cowan v. Gibson, 392 S.W.2d 307 (Mo. 1965), the Supreme Court previously addressed whether a physician could sue a private hospital for revoking his staff privileges. According to Cowan, under Missouri law, a private hospital’s decision regarding staff privileges was not the subject of judicial review. Since Cowan, 46 states and the District of Columbia have adopted a limited exception to this general rule. Additionally, Missouri adopted state regulation 19 CSR 30-20.021, which mandates that all Missouri hospitals adopt bylaws governing the professional activity of the medical staff: “Bylaws of the medical staff shall provide for hearings and appeal procedures for the denial of reappointment and for the denial, revocation, curtailment, suspension, revocation, or other modification of clinical privileges of a member of the medical staff.” In this case, the Court determined whether and to what extent a member of a hospital medical staff who is directly and adversely affected by a hospital’s failure to abide by its own bylaws may sue to enforce compliance with those bylaws. The Court ruled that Dr. Egan could bring an action in equity for injunctive relief to compel the hospital to substantially comply with its own bylaws before his privileges were to be revoked. It explained that injunctive relief is a less intrusive remedy. The Court further stated that it was not holding that the bylaws create or are themselves an enforceable contract between physicians and the hospital or that a breach of the bylaws gives rise to an action for damages. The Court added that it still “Malpractice” >p5 Malpractice believed that the final authority to make staffing decisions was vested in the hospital’s governing body with the advice from the medical staff, and it did not intend to create judicial oversight. As such, the Court will not impose judicial review on the merits of a hospital staffing decision, but only will act to ensure that substantial compliance with the hospital bylaws occurs. Tort Reform – Constitutional Challenge and Verdict Reduction Klotz v. St. Anthony’s Medical Center, St. Louis County Circuit Court, Cause No. 06-CC4826 This medical malpractice cause of action was tried to a jury from July 21, 2008 through July 30, 2008 in the Circuit Court of St. Louis County, Missouri. Judge Barbara Wallace presided over the trial. Named as Defendants were St. Anthony’s Medical Center, Dr. Michael Shapiro, and Metro Heart Group. This cause of action involves a complex procedural history. The Plaintiffs’ causes of action arose in March 2004 when James Klotz was hospitalized. Initially, James Klotz filed suit on December 14, 2004 against St. Anthony’s Medical Center. On April 28, 2005, James Klotz’ Petition was amended to include Mary Klotz’ claim for loss of consortium. On August 28, 2005, tort reform took effect. On December 2, 2005, the Plaintiffs voluntarily dismissed their cause of action without prejudice. Plaintiffs filed the Petition under which the case was tried on December 4, 2006 against St. Anthony’s Medical Center. This Petition subsequently was amended on March 1, 2007 to include Dr. Shapiro and Metro Heart Group. The jury returned a verdict in favor of Plaintiffs and assessed 33% of the fault to St. Anthony’s Medical Center and 67% of the fault to Dr. Shapiro and Metro Heart Group. The jury awarded Mr. Klotz’ past economic damages of $760,000, past non-economic damages of $488,000, future medical damages of $525,000, future economic damages of $22,000, and future non-economic damages of $272,000 (for a total award of non-economic damages in the amount of $760,000). Plaintiff Mary Klotz received an award of past economic damages in the amount of $184,000, past noneconomic damages in the amount of $211,000, and future non- (from page 4) economic damages of $118,000 (for a total award of noneconomic damages in the amount of $329,000). This case presented Judge Wallace with the issue of whether to apply the benefit of the tort reform statutes to some, all, or none of the Defendants. Plaintiffs claimed the non-economic damage caps were unconstitutional, but Judge Wallace rejected this assertion. Judge Wallace found that tort reform would apply to the claims against Dr. Shapiro and Metro Heart Group, but not to the claims against St. Anthony’s Medical Center. Essentially, Judge Wallace found that, because a claim originally had been filed against St. Anthony’s Medical Center before the tort reform statutes took effect, St. Anthony’s Medical Center had notice of the claim and, therefore, the filing of the Petition under which the case was tried “related back” to St. Anthony’s initial notice of suit with the filing of the December 14, 2004 Petition. Dr. Shapiro and Metro Heart Group, on the other hand, did not have notice of any cause of action Plaintiffs were asserting against them until after tort reform took effect. Therefore, tort reform applied to the claims against Dr. Shapiro and Metro Heart Group. In applying the cap on non-economic damages, Judge Wallace first applied the percentage of fault to the damages awarded. The recovery against St. Anthony’s Medical Center fell below the pretort reform cap on non-economic damages and, therefore, there was no reduction in the amount of this damages award. In applying the post-tort reform non-economic damage cap to the award of non-economic damages against Dr. Shapiro and Metro Heart Group, Judge Wallace reduced the $350,000 cap to $234,500 (Dr. Shapiro and Metro Heart Group’s percentage of fault multiplied by the amount of the damages cap). This resulted in a past non-economic damage award to James Klotz in the amount of $234,500 because the amount of past non-economic damages awarded against these defendants exceeded the cap as applied by Judge Wallace. Because the post-tort reform cap applies to the entire case, rather than to each of Plaintiffs’ claims, Mr. Klotz did not receive any future non-economic damages, and Ms. Klotz did not receive any non-economic damages. Missouri Organization of Defense Lawyers Our Mission Membership in the Missouri Organization of Defense Lawyers is open to Missouri lawyers who devote a substantial amount of their time to the representation of defendants and potential defendants in civil litigation either as trial lawyers or as lawyers otherwise directly involved with the defense of civil litigation. Our Purpose To take appropriate action where possible to insure that defendants in our civil justice system receive fair and impartial treatment by juries, the judiciary and the legislature; ~5~ To enhance the knowledge and improve the skill of its members; To cooperate with other groups in promoting seminars, lectures and other educational opportunities in matters of common legal interest to the bar and/or the public; To promote among all lawyers involved in civil litigation the highest standards of professionalism and to encourage civility and courtesy in the conduct of trials and related proceedings; To develop collegiality and camaraderie among its members. Current Issues in Preemption by Roshan D. Shah Baker Sterchi Cowden &Rice, L.L.C. St. Louis, MO Dylan Murray and Elizabeth Raines Baker Sterchi Cowden &Rice, L.L.C. Kansas City, MO Two issues involving preemption, one percolating through the Missouri appellate courts and the other recently decided by the United States Supreme Court, will impact the practices of defense counsel in Missouri. The first involves the question of whether the Health Insurance Portability and Accountability Act of 1996 (HIPAA)1 preempts Missouri law permitting ex parte communications between defense counsel and a plaintiff’s health care providers. The second involves the United States Supreme Court’s recent decision in Wyeth v. Levine,2 where the Court held that the Food and Drug Administration’s judgment regarding the appropriateness of warnings on prescription drug labels do not necessarily preempt state tort law claims. HIPAA and Ex Parte Communications In Brandt II v. Medical Defense Associates,3 the Missouri Supreme Court held that, in personal injury actions, defense counsel may engage in ex parte communications with a plaintiff’s medical providers, as long as the provider consents and the communication concerns only the medical condition at issue. The Brandt II court acknowledged that Missouri law recognizes the physician-patient privilege.4 However, the court held, once a patient puts his medical condition in issue by filing a lawsuit, the privilege is deemed waived in full.5 Thus, Brandt II placed defense counsel on equal footing with plaintiff’s counsel, who enjoy unfettered access to plaintiff’s medical providers. Now, the equilibrium struck by Brandt II is in danger of being upset, as plaintiffs have asserted and some Missouri courts have ruled that HIPAA preempts Brandt II.6 patient’s sensitive medical information.9 In response, Congress “authorized the Secretary of the United States Department of Health and Human Services (HHS) to promulgate standards governing disclosure of [protected] health information [(PHI)]10 in the event Congress did not pass privacy legislation within three years of HIPAA's enactment.”11 When Congress failed to act, the Secretary of HHS adopted the federal Privacy Rule (“Privacy Rule”), which took effect in April 2003.12 The Privacy Rule provides that a covered entity (health care providers, health plans, and health care clearinghouses) may only disclose PHI as permitted by the regulations.13 Among the methods for disclosure permitted by the regulations are: disclosures pursuant to a HIPAAcompliant medical authorization from the patient,14 The Federal Privacy Rule and HIPAA’s Disclosure Provisions disclosures during a judicial proceeding pursuant to a court order,15 and disclosures during a judicial proceeding pursuant to a subpoena, discovery request, or other lawful process, so long as the covered entity has satisfactory assurances the patient has been provided notice that such disclosures are sought, or that a qualified protective Congress enacted HIPAA in 1996 to increase access to health care by, in part, reducing costs.7 The “cornerstone” of HIPAA’s cost-reduction function was the adoption of the electronic medical record.8 While Congress recognized the benefits of the electronic medical record, it also recognized the possible threat it posed to the dissemination of a 1 2 Health Insurance Portability and Accountability Act of 1996, 42 U.S.C. §§ 1320-d, et seq. Wyeth v. Levine ,--- S.Ct. ----, 2009 WL 529172 (U.S. March 4, 2009). 3 Brandt II v. Medical Defense Associates, 856 S.W.2d 667, 674 (Mo. 1993). 4 Id. at 670. 5 Id. at 672-73 (“If a patient waives the privilege, it ceases to exist. It may not be waived in part and retained in part.” (quoting Demonbrun v. McHaffie, 156 S.W.2d 923, 924 (1941)). 6 Currently pending before the Western District Court of Appeals is the matter of State ex rel. Collins v. Hon. Marco Roldan, No. 70350 (Mo. App. W.D. filed Nov. 20, 2008) (preliminary writ issued Feb. 3, 2009), which seeks to overturn the trial court’s decision to prohibit ex parte communications between defense counsel and the plaintiff’s health care providers in the context of a medical authorization. ~6~ “Preemption” >p7 7 See Arons v. Jutkowitz, 9 N.Y.3d 393, 411 (N.Y. 2007). 8 Id. at 412. 9 See Id. 10 With certain exclusions, “[p]rotected health information means individually identifiable health information” that is transmitted by or maintained in electronic media or that is transmitted or maintained in any other form or medium. 45 C.F.R. § 160.103. 11 Arons, 9 N.Y.3d at 412. 12 45 C.F.R. § 160 through § 164. 13 45 C.F.R. § 164.502(a). 14 45 C.F.R. § 164.502(a)(1)(iv). 15 45 C.F.R. § 164.512(e)(1)(i). Preemption that a qualified protective order16 has been sought by the party seeking to communicate with the covered entity.17 (Continued from page 6) Notwithstanding the fact that HIPAA does not mention, much less prohibit, ex parte communications, plaintiffs have dogmatically asserted that HIPAA preempts the Missouri Supreme Court’s ruling in Brandt II. Plaintiffs in Missouri have principally relied on a twopronged approach to try to prevent defendants from obtaining a court order or authorization that would effectively permit the defendant to obtain PHI through ex parte communications with the plaintiff’s health care providers: 1) Plaintiffs challenge the court order or authorization sought as not complying with Missouri law; and, 2) Even if the court order or authorization sought is found to comply with Missouri law, plaintiffs argue that Missouri law permitting ex parte communications with a plaintiff’s health care providers is precluded and preempted by HIPAA. In making the preemption part of this argument, plaintiffs have often paid little or no attention to the threshold requirement that Missouri law must be “contrary” to HIPAA in order to be preempted, instead focusing almost entirely on an argument asserting that Missouri law is not “more stringent” than (and is therefore preempted by) HIPAA. As a result, defense briefing on the preemption issue should focus first on the “contrary” threshold, emphasizing that there is nothing in Missouri law concerning ex parte communications with health care providers that makes it impossible to comply with the provisions of the Privacy Rule or that stands as an obstacle to the accomplishment of the full purposes of the Privacy Rule. HIPAA’s Express, Conflict-Based Preemption Clause The Privacy Rule also contains an express, conflict-based preemption clause, 45 C.F.R § 160.203, which mirrors the preemption clause in the HIPAA statute, 42 U.S.C.A. § 1320d7(a). Section 160.203 provides for the preemption of any state law that is contrary to HIPAA, except for those laws which are: 1) designed to prevent fraud and abuse in health insurance plans, 2) concern controlled substances, or 3) more stringent in protecting patient privacy than HIPAA. Using this provision, plaintiffs are urging the courts to find that, because ex parte communications with plaintiff’s health care providers do not fall into one of the three designated exceptions in Section 160.203, they are preempted. These arguments, however, do not comport with congressional intent or the plain language of HIPAA, which establishes a two-part preemption analysis under which state law must first be found to be “contrary” to HIPAA before the three exceptions are even considered. Missouri Law Is Not “Contrary” To HIPAA An important feature of HIPAA’s express preemption clause is that it only preempts state laws which are “contrary” to HIPAA.18 A “contrary” state law is defined as one which would make it “impossible [for the treating physician or other covered entity] to comply with both the [s]tate and federal requirements,” or one which “stands as an obstacle to the accomplishment and execution of the full purposes and objectives” of HIPAA.19 Plaintiffs tend to ignore the “contrary” threshold altogether and move straight to a “stringency” analysis. In making the preemption argument, plaintiffs have typically pointed to and relied on a small number of decisions from other jurisdictions where state law concerning ex parte communications with health care providers has been found to be preempted by HIPAA. However, these decisions have tended to involve a very specific fact pattern that is not likely to be involved in a Missouri case and are therefore highly distinguishable on that basis. Such fact pattern involves the following: 1) Defense counsel who makes no attempt to comply with HIPAA by seeking a court order or authorization prior to contacting the health care provider; and 2) A particular state law (statutory or common law) that specifically authorizes or requires such ex parte communications even where no court order or authorization has been obtained pursuant to HIPAA.21 These decisions will typically be distinguishable because the preemption issue has most commonly arisen in Missouri in the context of defense counsel who have sought a HIPAA compliant authorization or court order rather than ignoring HIPAA’s requirements. Moreover, there is simply nothing in Missouri law that authorizes defense counsel to violate HIPAA by engaging in ex parte communications concerning PHI without first obtaining a court order or authorization pursuant to HIPAA.22 It Is Not Impossible for A Health Care Provider to Comply with The Privacy Rule And Engage in Ex Parte Communications with Defense Counsel The fact that Missouri law permits ex parte communications is in perfect harmony with the Privacy Rule. First, the Privacy Rule does not make any mention of ex parte communications, much less prohibit them. Thus, it is difficult to see how a health care provider acting in accordance with Missouri law could be violating a federal law that does not exist. The Secretary of HHS has made a similar observation: “What does one do when there is a State provision and no comparable or analogous federal provision, or the converse is the case? The short answer would seem to be that, since there is nothing to compare, there cannot be an issue of a ‘contrary’ requirement, and so the preemption issue is not presented.”20 “Preemption” >p8 16 A qualified protective order means an order prohibiting the requesting party from using the PHI for any purpose other than the litigation in question, and requiring the party to return to the covered entity, or destroy, any records containing PHI. See § 164.512(e)(1)(v). 17 45 C.F.R. § 164.512(e)(1)(ii). 18 45 C.F.R. § 160.203; see also 42 U.S.C.A. § 1320d-7(a)(1). 19 45 C.F.R. § 160.202(1)-(2). 20 Standards for Privacy of Individually Identifiable Health Information, 64 Fed. Reg. 59,918, 59,995 (proposed Nov. 3, 1999) (to be codified at 45 C.F.R. pts. 160 through 164). 21 See, e.g., Moreland v. Austin, 670 S.E.2d 68, 69-72, 284 Ga. 730 (2008); Law v. Zuckerman, 307 F.Supp.2d 705, 707-711 (D. Md. 2004); Croskey v. BMW of North America, Inc., No. 02CV73747DT, 2005 WL 1959452, at *3-*5 (E.D.Mich. Feb. 16, 2005) (Magistrate’s decision, which was affirmed in part and reversed in part, in Croskey v. BMW of North America, No. 02CV73747, 2005 WL 4704767 (E.D.Mich. Nov. 10, 2005)). 22 See, e.g., Brandt II, 856 S.W.2d at 662-63, 674. ~7~ Preemption (Continued from page 7) Conclusion Because all drugs carry risks, some which are unknown despite years of testing and clinical trials, the FDA’s function, in part, is to accurately emphasize the risks and benefits a drug carries. The agency must employ its scientific judgment to ensure that it does not over-warn of risks and, thus, unnecessarily deter physicians from prescribing the drug; and, simultaneously ensure it does not under-warn of risks, thus luring physicians into prescribing a drug which might not be appropriate for the patient. Whether HIPAA preempts Missouri law permitting ex parte communications will ultimately turn on the plain language of the statute, and canons of statutory construction. However, practitioners would be wise to remind courts of the stakes involved. Ex parte communications allow defense counsel the same access to plaintiff’s treating health care providers that plaintiff’s counsel enjoys. This serves as an effective system of checks and balances — ensuring that neither side is presenting biased or misleading information to plaintiff’s treaters. This delicate balance manifests itself in the form of the drug’s warning label, the “centerpiece of risk management” by which the FDA “communicates to health care practitioners the agency's formal, authoritative conclusions regarding the conditions under which the product can be used safely and effectively.”27 The FDA’s final approval of a new drug is “conditioned upon the [manufacturer] incorporating the specified labeling changes exactly as directed [by the FDA].”28 A manufacturer’s label which fails to comport exactly with the FDA’s specified label will be deemed false or misleading, subjecting the manufacturer to legal action by the government.29 Furthermore, ex parte communications allow defense counsel to greatly reduce information costs — the time, energy, and money expended to discover relevant information — by eliminating the need to depose those health care providers who possess little or no relevant information. This is especially true in complex medical cases where a plaintiff has had numerous treating physicians. Moreover, these cost-savings are realized not only by the defendant, but also by the health care providers, who would otherwise have to spend hours being deposed instead of treating patients. Thus, ex parte communications do not provide a strategic advantage for the defendants, but simply level the litigation playing field. The FDA permits two avenues by which a manufacturer may alter its label: 1) prior approval supplements, which require FDA approval before the manufacturer modifies the label, and 2) “changes being effected” (CBE) supplements, which allow a manufacturer to unilaterally strengthen its warning label, provided it notifies the FDA.30 When a label change is implemented via CBE, the FDA will review the submission and determine whether, in its judgment, the scientific evidence supports such a change.31 If it rejects the change, the manufacturer must reinstate the original label or face an enforcement action.32 The CBE supplement was one of the issues at the heart of Levine. Wyeth v. Levine: Preemption of State Law Claims Involving Prescription Medications The blockbuster case of Wyeth v. Levine23 involved a relatively straightforward question: once the FDA, pursuant to its authority under the Federal Food, Drug, and Cosmetic Act (FDCA), 21 U.S.C.A. § 301 et seq., has approved a prescription drug’s warning label, may a plaintiff bring a claim under state law asserting that a different warning was required to make the drug reasonably safe for use? In a 6-3 decision, the United States Supreme Court held that, in certain circumstances, a plaintiff may countermand the manufacturer’s warning label.24 Levine: Factual and Procedural History Levine centers around Wyeth’s FDA-approved prescription drug Phenergan, an antihistamine used to treat nausea.33 In 2000, Phenergan’s FDA-approved label provided that the drug could be injected either via intramuscular or intravenous injection, including both intravenous drip (IV drip) and intravenous push (IV push).34 However, the label warned health care providers that, when using the intravenous method of injection, there was a risk of inadvertent injection into the arteries, which could cause gangrene and, ultimately, lead to amputation.35 In 1996, the FDA rejected Wyeth’s attempt to modify Phenergan’s warnings regarding intravenous injection, instructing it to “[r]etain verbiage in current label.”36 “Preemption” >p9 The Role of the FDA in Regulating Prescription Drugs The FDCA mandates that the FDA protect the public health by ensuring that drugs are safe and effective, and that their labels adequately inform physicians of the risks and benefits of the product without providing false or misleading information.25 To fulfill this mandate, the FDA considers complex clinical studies, the “important and practical public health issues pertaining to the use of the product in day-to-day clinical practice,” and the “need for risk management measures to help assure[,] in clinical practice[,] that the product maintains its favorable benefit-risk balance.”26 23 Levine, No. 06-1249, 2009 WL 529172 (U.S. March 4, 2009). 24 Id. at *9. 25 21 U.S.C.A. § 393(b); see also Requirements on Content and Format of Labeling for Human Prescription Drug and Biological Products, 71 Fed. Reg. 3,922, 3,934 (January 24, 2006) (codified at 21 CFR pts. 201, 314, and 601). 26 71 Fed. Reg. at 3,934. 27 Id. 28 Levine v. Wyeth, 944 A.2d 179, 185 (Vt. 2006). 29 See generally U.S. v. Guardian Chemical Corp., 410 F.2d 157 (2nd Cir. 1969); see also 71 Fed. Reg. at 3,935. 30 71 Fed. Reg. at 3934. 31 Id. 32 Id. 33 Levine, No. 06-1249, 2009 WL 529172, at *2. 34 Id. 35 Id. at *2 n.1. 36 Id. at *3. ~8~ Preemption On April 7, 2000, plaintiff Diana Levine, a guitarist, visited Northeast Washington County Community Health, Inc. (the “Health Center”) and received two injections of Phenergan for the treatment of nausea caused by migraine headaches.37 The first injection was administered via intramuscular injection.38 When the first injection failed to alleviate her symptoms, plaintiff received an intravenous injection via the IV push method.39 Unfortunately, Phenergan entered an artery, causing gangrene and, eventually, required the amputation of plaintiff’s forearm and hand.40 With regard to Wyeth’s impossibility defense, the Court acknowledged that generally, “a manufacturer may only change a drug label after the FDA approves a supplemental application.”49 The Court observed, however, a manufacturer could avail itself of the CBE supplement and unilaterally strengthen its warning label, pending approval by the FDA. 50 The Court rebuffed Wyeth’s interpretation of the CBE supplement, which provided that a warning could be strengthened via CBE supplement only to reflect “newly acquired information” regarding the risk.51 According to the FDA’s notice of final rule, “newly acquired information” encompassed not only new data, but also “‘new analyses of previously submitted data.’”52 The majority found significant 20 reported events in which a Phenergan injection resulted in gangrene and, ultimately, amputation.53 The first incident came to Wyeth’s attention in 1967 and, subsequently, Wyeth worked with the FDA to modify its label to reflect the risk.54 “In later years, as amputations continued to occur, Wyeth could have analyzed the accumulating data and added a stronger warning about IV-push administration of the drug.”55 If the FDA disagreed with the stronger warning, the Court noted, it would reject it.56 Plaintiff filed suit against Wyeth, alleging failure-to-warn under theories of negligence and strict-liability.41 Plaintiff’s claims were premised on the theory that Phenergan’s label should have instructed physicians to use the IV-drip method as opposed to the IV push method or, more broadly, that Phenergan is not reasonably safe for any type of intravenous administration because the risk of gangrene outweighs any therapeutic benefits.42 The jury agreed, finding Phenergan’s warning regarding IV push administration was inadequate and entered a verdict against Wyeth for $7.4 million.43 Wyeth appealed the verdict to the Vermont Supreme Court, arguing the trial court erred in instructing the jury regarding damages and in failing to dismiss the claims on the basis that the FDA’s approval of Phenergan’s label impliedly preempted state tort law.44 The court denied Wyeth’s appeal on all counts,45 prompting Wyeth to petition the United States Supreme Court for a writ of certiorari, which was granted.46 The Court found unpersuasive Wyeth’s arguments that the FDA’s 1996 rejection of its proposed warning label, which sought to modify the warning regarding intravenous injection, was an affirmative decision by the FDA to reject a stronger warning regarding IV push administration.57 The Court’s rationale turned on an issue of fact—specifically, whether, in rejecting the label, the FDA considered the narrow question of whether a stronger warning for IV push administration needed to be added, as opposed to the broader question of whether a stronger warning was needed for all intravenous injections. The Court relied on the conclusions of the Vermont courts, which found that “the FDA had not made an affirmative decision to preserve the IV-push method [n]or intended to prohibit Wyeth from strengthening its warning about IV-push administration.”58 The majority also found significant the United States’ concession that the rejection was based on format, not The United States Supreme Court Rejects Preemption In Levine Wyeth laid before the Court two arguments for finding implied preemption: 1) it would have been impossible for Wyeth to comply with the state-law duty to strengthen Phenergan's label regarding IV push administration and also comply with the FDA’s labeling requirements (“impossibility defense”), and 2) state tort actions are an obstacle to the accomplishment and execution of the full purposes and objectives of Congress, “because [they] substitute[] a lay jury's decision about drug labeling for the expert judgment of the FDA.”47 The Court rejected both arguments.48 37 (Continued from page 8) “Preemption” >p10 Id. at *2. 49 Id. at *7. Id. at *7. Id. 50 39 Id. 51 40 Id. 41 Id. Id. Although this limit on the use of the CBE supplement was not formally adopted until 2008, Wyeth argued the formal adoption simply re-affirmed the rule in effect at the time the injury occurred. Id. 42 Id. at *2. 52 43 Levine v. Wyeth, 944 A.2d 179, 182 (Vt. 2006). The verdict was reduced to $6,774,000 to account for prejudgment interest and plaintiff’s recovery in a settlement with the Health Center. Id. at 182-83. Id. (quoting Supplemental Applications Proposing Labeling Changes for Approved Drugs, Biologics, and Medical Devices, 73 FR 49,603, 49,604 (August 22, 2008) (to be cofidied at 21 CFR Parts 314, 601, and 814)). 53 Levine, No. 06-1249, 2009 WL 529172, at *8. 44 Id. at 183. 54 Id. 45 Id. at 197. 55 Id. 46 Wyeth v. Levine, 128 S.Ct. 1118, 169 L.Ed.2d 845 (2008). 56 Id. at *9. 47 Levine, No. 06-1249, 2009 WL 529172, at *5. (internal citations and quotations omitted). 57 Id. 58 Id. at *9 (citing Levine, 944 A.2d at 188-89). 38 48 Id. at *13. ~9~ Preemption (Continued from page 9) substance.59 Thus, finding that Wyeth could have strengthened its warnings regarding the IV push administration via the CBE supplement, the majority held it was possible for Wyeth to comply with the labeling requirements imposed by the Vermont jury, as well as the labeling requirements mandated by the FDA.60 The Court rebuked the FDA’s “dramatic change in position” on the subject, finding that the agency’s prior statements contradicted its current position.71 Significant was that the FDA had previously “cast federal labeling standards as a floor upon which States could build and repeatedly disclaimed any attempt to pre-empt failure-towarn claims.”72 Thus, based on the absence of evidence that Congress intended the FDCA to preempt state law, and the zero deference given to the FDA’s position, the Court concluded that state tort actions do not stand as an obstacle to the accomplishment and execution of the full purposes and objectives of Congress.73 Finding both of Wyeth’s arguments in favor of preemption to be meritless, the Court affirmed the decision of the Vermont Supreme Court. The Court also declined to find that state-law tort suits are an obstacle to the accomplishment and execution of the full purposes and objectives of Congress.61 The Court concluded Wyeth’s argument — that in passing the FDCA, Congress intended an FDAapproved label to serve as a ceiling regarding risk warnings — was diametrically opposite to the evidence of Congress’ purpose.62 The Court found significant that Congress did not enact an express preemption provision during the 70-year history of the FDCA.63 “[Congress’] silence on the issue, coupled with its certain awareness of the prevalence of state tort litigation, is powerful evidence that Congress did not intend FDA oversight to be the exclusive means of ensuring drug safety and effectiveness.”64 Buttressing this conclusion was the fact that the first version of the bill that eventually became the FDCA included a federal cause of action for injured consumers.65 “Evidently,” the provision was removed after witnesses testified before the Subcommittee of the Senate Committee on Commerce that the provision would be duplicative, as common law claims were already available under state law.66 The Court also pointed to the fact that in 1976 and 1997, respectively, Congress preempted state tort law concerning medical devices, as well as certain state requirements regarding cosmetics and over-the-counter medications, but expressly preserved product liability actions.67 The Post-Levine World For defense counsel, the silver lining in Levine’s cloud is that the Court has not ended the battle over preemption, it has simply shifted the battlefield. Central to the majority’s rejection of Wyeth’s impossibility defense was Wyeth’s ability to avail itself of the CBE supplement to unilaterally strengthen its warnings.74 However, the majority recognized that the CBE supplement would not be available under a different factual record — one demonstrating “clear evidence” that the FDA had given the specific risk at issue “more than passing attention” and/or “made an affirmative decision” that additional or stronger warnings regarding the risk would be inappropriate.75 While the Court found the factual circumstances surrounding the FDA’s 1996 rejection of Wyeth’s modified label to be lacking in this respect, presumably in instances where such a factual record is present, the impossibility defense would bar plaintiff’s failure-to-warn claim.76 Thus, defense counsel must develop a strong factual record demonstrating that the FDA considered and rejected a stronger warning regarding the specific risk in question. Moreover, the Court found unconvincing Wyeth’s reliance on a 2006 preamble to an FDA regulation governing the content and format of prescription drug labels. The preamble declared that the FDCA establishes “both a ‘floor’ and a ‘ceiling,’” so that “FDA approval of labeling . . . preempts conflicting or contrary State law.”68 The Court reiterated the general rule that, absent delegation by Congress, an agency has no authority to conclude that state law was preempted.69 Such a determination was reserved to the courts, which must look at the substance of state and federal law.70 Eventually, as the law develops in the lower courts, the impossibility defense may evolve into an affirmative defense. Potentially, a jury could find the warning in question inadequate, and also find that the FDA rejected an additional and/or stronger warning. In such cases, the former finding would be preempted by the latter.77 “Preemption” >p11 59 Id. at *9 n.5. 70 See Id. 60 Id. at *9. 71 Id. at *12. 61 Id. at *10. 72 Id. Id. 73 Id. at *13. 63 Id. 74 64 Id. 65 Id. at *10 n.7. Id. at *9 (“Wyeth has failed to demonstrate that it was impossible for it to comply with both federal and state requirements . . . [t]he CBE regulation permitted Wyeth to unilaterally strengthen its warning . . .”). 66 Id. 75 Id. 67 Id. at *10; Id. at *10 n.8 (citing 21 U.S.C. §§ 379r(e), 379s(d) (“Nothing in this section shall be construed to modify or otherwise affect any action or the liability of any person under the product liability law of any State”)). 76 68 Id. at *10 (quoting 71 Fed.Reg. at 3,934-3,935). Id. at *9 n.5 (noting the factual finding of the Vermont trial court and the Vermont Supreme Court that the label the FDA rejected in 1996 did not materially differ from the FDA-approved label in use, and citing the United States’ concession that the rejection was based on format, not substance). 69 Levine, No. 06-1249, 2009 WL 529172, at *11. 77 See Id. at *9. 62 ~ 10 ~ Preemption Finally, in tightly circumscribing its rationale around the factual record and Congressional intent, the majority never considered the more fundamental proposition posed by Levine: Who is best-suited to regulate prescription drugs — an expert agency created by Congress and dedicated to analyzing scientific literature, weighing the risk and benefits of a particular drug, and adopting the optimal warnings or 12 lay jurors without such training? A “juror regulatory body,” which will not convene until after there is an injury, is less-equipped to weigh the risks and benefits of prescription drugs, which are “complex medicines, esoteric in formula and varied in effect.”78 As Justice Scalia stated in Riegel v. Medtronic, Inc., a case where the Court upheld preemption of state law claims against medical device manufacturers, “[a] jury . . . sees only the cost of a more dangerous design, and is not concerned with its benefits; the patients who reaped those benefits are not represented in court.”79 This debate will continue for the foreseeable future. inadequate warning; that is, plaintiff believed the warning should have been stronger.80 This is a claim that can be “manufactured” time and again — if the warning is provided in the adverse event profile, the plaintiffs argue it should have been prominently displayed in the black box; if the warning was displayed in the black box, plaintiffs argue the drug should have been contraindicated for the patient profile in question; if the word “slight” was used to describe the risk, the word “moderate” should have been substituted, etc. It is a never-ending saga, one that increases the cost, and thus the price, of drugs, but has not been shown to make them safer. Levine represented an opportunity for the Court to end the saga. For now, the defense will settle with developing a preemption defense within the confines of Levine — by presenting evidence that the FDA considered and rejected the specific risk in question.81 Conclusion The argument for FDA preemption was not borne out of a desire for deregulation of the pharmaceutical industry, as critics suggested. Rather, preemption was about centralized regulation. It is important to note that Levine did not involve a true failure to warn — the label warned against the risk of intra-aterial injection of Phenergan and resulting gangrene — but rather involved an alleged (Continued from page 10) 78 Jones v. Minnesota Min. and Mfg. Co., 100 N.M. 268, 284 (N.M. Ct. App.1983). 79 Riegel v. Medtronic, Inc., 128 S.Ct. 999, 1008, 169 L.Ed.2d 892 (2008). 80 Id. at *2 n.1. 81 Id. at *9. Medicare and Medicaid Liens – An Overview and Update for Defense Counsel by Christine A. Vaporean Brown & James, P.C. St. Louis, MO The existence of a Medicare or Medicaid lien can lead to postsettlement or post-judgment litigation if it is not properly addressed before payment on a case is made. Recent changes in the law regarding liens affect negotiations and settlements. This article provides an overview of the existing law, including the recent changes to Medicare and Medicaid liens and recommendations for addressing liens in the context of litigation and settlement. Overview of Medicare and Medicaid Liens In an effort to prevent the depletion of the Medicare Trust Fund established in 1965, Congress enacted the Medicare Secondary Payer Act as a component of the Consolidated Omnibus Reconciliation Act of 1980 (COBRA) and the Medicare Prescription Drug Act of 2003. These laws give the United States a right to recover from a third party any monies paid by Medicare for health care services of a plaintiff when the health care services were related to the third party’s liability to the plaintiff-beneficiary. In 2007, Congress enacted The Medicare, Medicaid, and SCHIP Extension Act of 2007 (MMSEA), which imposes new, affirmative obligations on primary payers to notify Medicare of an interest it may have in ~ 11 ~ a lawsuit. In combination, these laws require that any Medicare lien be satisfied before any other payment on a case is made. The Medicare Set Aside Trust, 42 USC 1395y(b)(2), also provides a set-off for future Medicare payments following a worker’s compensation settlement. The Set Aside Trust provisions will not be covered in this article, but defense counsel should be aware they exist and may impact settlements in certain cases. Additional information on the Set Aside Trust can be found on the Centers for Medicare and Medicaid Services (CMS) website, www.cms.hhs.gov. Finally, it is anticipated that the American Recovery and Reinvestment Act of 2009 (the stimulus bill) will further enhance Medicare’s right of recovery against primary payers over the next three to five years. The effect has not yet been determined by the current administration. By statute, Medicare’s right of recovery attaches automatically with the payment for health care services. Thus, the Medicare lien is often called a “super-lien.” Glenn A. Bradford, Liens, Assignments, Subrogation and other Traps for the Claimant’s Medicare and Medicaid Liens >p12 Medicare and Medicaid Liens (Continued from page 11) Lawyer, 53 J. Mo. B. 248 (1997) and Glenn A. Bradford, The Medicare Lien Revisited, 56 J. Mo. B. 44 (2000). Federal law makes clear that failure to satisfy these liens with the proceeds of a settlement or judgment can result in significant penalties for a defendant or its insurer, including having to pay for the medical expenses twice, paying double damages to Medicare in an action to recover on the lien, and the payment of interest on the lien amount. Missouri law contains similar provisions regarding the state counterpart to Medicare, Missouri Medicaid, now called MO HealthNet. MEDICARE Laws Establishing the Lien In general, Medicare provides health insurance coverage to persons over age 65, persons under age 65 who are disabled, and to persons with end-stage renal disease. To protect the government from becoming the primary health insurer for this population in all circumstances and thus depleting resources, the Medicare laws provide certain exceptions to coverage. Of interest are the provisions which establish Medicare as a Secondary Payer. In the event a covered individual obtains medical care which is also covered by a workers compensation law, an automobile or liability insurance policy or a policy of no fault insurance, Medicare will generally not make a payment. 42 U.S.C. § 1395y(b)(2)(A)(ii). The law does allow payment “if a primary plan … has not made or cannot be reasonably expected to make payment with respect to such item or service promptly.” 42 U.S.C. § 1395y(b)(2)(B)(i). If a payment is made under this section, the primary plan (i.e. the worker’s compensation, liability, automobile or no-fault insurer) “shall reimburse the appropriate [Medicare] Trust Fund for any payment made by the Secretary … if it is demonstrated that such primary plan has or had a responsibility to make payment.” 42 U.S.C. § 1395y(b)(2)(B)(ii). Payments under this section are called “conditional payments.” Responsibility of a primary plan payer (“primary payer”) to make a payment can be demonstrated by a judgment, a payment conditioned on settlement (regardless of whether liability is admitted), “or by other means.” Id. “By other means” includes contractual obligations or those imposed by a recovery demand letter. 42 C.F.R. § 411.22. The Eighth Circuit also recently held that Medicare’s right of reimbursement extends to medical expenses recovered in wrongful death actions. Mathis, et al. v. Leavitt, Opinion No. 08-1983, January 30, 2009, 2009WL211944. Enforcement Provisions The United States is authorized to bring an action to recover conditional payments “against any or all entities that are or were required or responsible (directly, as an insurer or self-insurer, as a third-party administrator, as an employer that sponsors or contributes to a group health plan, or large group health plan, or otherwise).” 42 U.S.C. § 1395y(b)(2)(B)(iii). The United States may collect double damages against any such entity and recover “from any entity that has received payment from a primary plan or from the proceeds of a primary plan’s payment to any entity.” Id. The United States also has a subrogation right to the extent of the ~ 12 ~ conditional payment amount on behalf of an individual and against a primary payer. 42 U.S.C. 1395y(b)(2)(B)(iv). Thus, not only does the United States have a lien, it may enforce the lien against an insurer (including self-insured entities) and anyone who receives payment from an insurance policy. This includes health care providers, plaintiffs, plaintiff’s counsel, insured defendants, and potentially defense counsel to the extent defense counsel are compensated pursuant to the same insurance policy which makes a payment to a plaintiff. Research by the authors revealed no cases in which Medicare sought reimbursement from defense counsel. The right of subrogation allows Medicare to assert its lien whether or not the beneficiary asserts a claim. 42 C.F.R. § 411.20 et seq. establish the procedure for recovery of conditional payments. 42 C.F.R. § 411.23 requires a beneficiary to cooperate with Medicare in any action to recover conditional payments. Medicare has a direct right of action against primary payers. 42 C.F.R. § 411.24(e). If an insurer imposes a time limit for filing a claim, the time limit does not apply to Medicare; however, in the face of such a limitations periods, the claim for reimbursement must be asserted by Medicare by the end of the year following the year in which the primary payer has notice that it is the primary payer, wherein notice received during the last three months of a year is considered received in the following year. 42 C.F.R. § 411.24(f). If no such claims-filing requirement exists, the statute of limitations for an action to recover conditional payments is six years. 28 U.S.C. § 2415(a). Medicare has a right to recover from any entity that has received a payment, including a Medicare beneficiary, provider, supplier, physician, attorney, State agency or primary insurer. 42 C.F.R. § 411.24(g). In the case of liability insurance settlements and disputed claims under workers compensation or no-fault insurance, if Medicare is not reimbursed within sixty (60) days of the beneficiary receiving a payment, the primary payer must reimburse Medicare even though it has already reimbursed the beneficiary or other party. 42 C.F.R. § 411.24(i)(1). The provisions of this section apply if payment is made to an entity other than Medicare when the primary payer is or should be aware that Medicare has made a conditional payment. If reimbursement to Medicare for a conditional payment is not made within sixty days of notice of responsibility for such payment, interest will accrue. 42 U.S.C. § 1395y(b)(2)(B)(ii). The interest allowable under this section accrues until reimbursement is made. 42 C.F.R. § 411.24(m)(2)(ii). Interest is applied for full thirty-day periods. Id. The interest rate is determined pursuant to provision set forth in 42 C.F.R. § 405.378(d). The amount of reimbursement due is determined by whether Medicare must initiate an action to recover payments. Pursuant to 42 C.F.R. § 411.24(c), if no such action is required, the amount of reimbursement due is the lesser of either a) the amount of the Medicare payment; or b) “the full primary payment amount that the primary payer is obligated to pay under this part without regard to any payment, other than a full primary payment that the primary Medicare and Medicaid Liens >p13 Medicare and Medicaid Liens payer has paid or will make, or, in the case of a primary payment recipient, the amount of the primary payment.” If an action for recovery is instituted, Medicare may recover twice the amount of its payment. 42 C.F.R. § 411.24(c)(2). 42 C.F.R. § 411.37(a) mandates that as a general rule, Medicare must reduce its recovery to account for the costs of procuring the judgment or settlement which gives rise to the right to recover conditional payments if procurement costs are incurred and those costs are borne by the party against whom recovery is sought. If Medicare must file suit against a primary payer, the recovery amount is calculated pursuant to 42 C.F.R. § 411.37(b). In general, the costs to procure a judgment or settlement are apportioned between Medicare and the claimant based on the ratio of the lien to the total award or settlement. 42 C.F.R. §§ 411.37(c) – (e). The Medicare lien which results from a conditional payment may be compromised and settled if the claim is not more than $100,000. 31 U.S.C. § 3711(a)(2). Claims in excess of $100,000 are to be handled by the Department of Justice. 31 C.F.R. § 902.1. The factors considered by Medicare when comprising a claim include: the debtor’s inability to pay; the government’s inability to collect payment promptly; the costs of collections versus the full amount of the debt; and the existence of doubt as to the government’s ability to prove its case. 31 C.F.R. § 902.2(b). If the claim does not exceed $100,000 and can be resolved by Medicare, the authority to compromise a claim lies in the CMS Regional Office. “Medicare Second Payer Manual,” available at the CMS website:www.cms.hhs.gov.manuals/downloads/msp/105c07.pdf; 31 U.S.C. § 3711; 42 C.F.R. § 405.405(d). A party wishing to compromise a claim must inform the Regional Office of their intent. Id. Notice Requirements Upon learning that Medicare made payments which were likely conditioned on reimbursement, a third party must provide notice to Medicare of its status as a primary payer. 42 C.F.R. § 411.25(a). Medicare has no duty to notify third parties of the lien; it exists as long as the third party knew or should have known of its existence. 42 C.F.R. § 411.24(i)(2). Effective July 1, 2009, the requirements that a liability, no-fault or workers compensation insurer (a non-GHP primary payer) notify Medicare of the primary payer’s responsibility to reimburse Medicare will become more comprehensive and stringent. In December 2007, The Medicare, Medicaid, and SCHIP Extension Act of 2007 (MMSEA) was enacted as Public Law 110-173. The relevant portions of this Act (Section 111) were codified 42 U.S.C. § 1395(y)(b)(8). This section requires non-GHP insurers: a) to determine whether a claimant, including a person whose claim is unresolved, is entitled to benefits under the program; and if a claimant is so entitled, b) to submit the claimant’s identity and other information necessary to allow the Secretary of Health and Human Services to make a determination regarding the coordination of benefits, “including any applicable recovery claim.” 42 U.S.C. § 1395(y)(b)(8)(A) and (B). Thus, this law now requires all categories of primary payers to identify individuals for whom ~ 13 ~ (Continued from page 12) Medicare has made a payment for which Medicare might be eligible to be reimbursed and to promptly notify Medicare of its right to reimbursement. Failure of a “Responsible Reporting Entity” (“RRE”) to comply with this section carries a penalty of $1,000 per day. 42 U.S.C. § 1395(y)(b)(8)(E). 42 C.F.R. § 411.25(b) requires insurers to describe the circumstances of their primary payment responsibility, including the particular type of insurance coverage and the time period for which coverage applies. It further provides additional reporting requirements can be imposed by the CMS Regional Office managing the particular claim. CMS has exercised that authority. CMS has issued multiple rules and notices regarding the implementation of MMSEA. The MMSEA implementing regulations generally divide MSP into “pre-payment” and “post-payment” activities. Prepayment activities are intended to stop Medicare from mistakenly making primary payments when it should be the secondary payer. Post-payment activities are designed to recover mistaken or conditional payments when a liability insurer (including self-insurer), no-fault insurer or workers compensation plan settles a case or makes a payment pursuant to a judgment or award. The MMSEA provisions mandate that Required Reporting Entities (“RRE’s”) provide data to CMS’ Coordination of Benefits Contractor (COBC). “Supporting Statement for the Medicare Secondary Payer (MSP) Mandatory Insurer Reporting Requirements of Section 111 of the Medicare, Medicaid, and SCHIP Extension Act of 2007”, available at www.cms.hhs.gov/mandatoryinsrep/. All reporting under this program will be electronic. Id. RRE’s are required to register with COBC through a secure website. Id. Once registered, the RRE will have a data reporting regimen. Data collection frequency will be no more than quarterly. Id. No-fault insurers and workers compensation plans for non-contested claims will have to report data on an ongoing basis. Id. For non-GHP RRE’s involved in contested claims, the reports will be made on a one-time basis where a single settlement, judgment, award or other payment is made. Id. The Mandatory Insurer Reporting Requirements also outline the specific information which must be provided by the non-GHP RRE’s. This information includes: the identity of the injured party including specific identifying information; the identity of the claimant, if different from the injured party; information on the primary plan, including type of insurance and other specific data; the identity of the policy holder; the identity of the injured party’s attorney; information regarding the incident giving rise to the claim; and the manner of resolution of the claim, including how a settlement or judgment is funded. Id. at Attachment D, NGHP Data Elements. Thus, the new rules implemented pursuant to MMSEA require that insurers report every payment they make to a plaintiff on a case and provide sufficient information that allows CMS to track down and recover the monies which should have gone to satisfy its lien. These new rules make it virtually impossible to “fly under the radar” and fail to satisfy a Medicare lien in the future, to the extent anyone was inclined to do so. Medicare and Medicaid Liens >p14 Medicare and Medicaid Liens (Continued from page 13) reimburse the department of social services … from the proceeds of any settlement, judgment, or other recovery …. A judgment, award, or settlement in [such] an action may not be satisfied without first giving the division notice and a reasonable opportunity to file and satisfy the claim or proceed with any action as otherwise permitted by law.” § 208.215.6, RSMo. The authors have found no Missouri cases wherein a satisfaction of judgment or settlement was held void due to failure of the plaintiff to give MO HealthNet notice of the impending payment. MEDICAID Medicaid is a state-level program supported in part by federal funds and created with the Social Security Act of 1965 to provide health care services for the needy. Missouri’s version of Medicaid is known as MO HealthNet. § 208.001.2, RSMo. MO HealthNet statutes are codified at § 208.001, RSMo et seq. The federal statutory basis for state Medicaid programs is codified at 42 U.S.C. § 1396, et seq. Laws Establishing the Lien and Notice Requirements Like their federal counterpart, MO HealthNet laws contain provisions mandating reimbursement if a beneficiary recovers from a third party tortfeasor for an injury, disease or disability for which MO HealthNet has paid benefits. Federal law requires states to determine the legal liability of third parties toward payment for services rendered under the State’s Medicaid plan and to seek reimbursement for medical assistance to the extent of such legal liability. 42 U.S.C. § 1396a(a)(25)(A) and (B). Section 1396a(a)(25)(H) gives the State the right to payment by any other party for health care items or services paid by the state. Enforcement Provisions Missouri law dictates that MO HealthNet be a payer of last resort. § 208.215.1, RSMo. Liability of “any person, corporation, institution, public agency or private agency” to a MO HealthNet participant for personal injury, disability or disease payments made by MO HealthNet is a debt due the state and is recoverable from the liable party or the MO HealthNet participant. Id. The debt due the state shall not exceed the payments made by MO HealthNet. Id. Unlike Medicare laws, workers compensation plans are excepted from the MO HealthNet recovery provisions. § 208.215.13, RSMo. Any plaintiff pursuing a claim involving injuries, disease or disability for which MO HealthNet has made a payment must promptly notify MO HealthNet of the pursuit of such a claim. § 208.215.3, RSMo. MO HealthNet applicants automatically assign their rights of recovery against a third party for funds expended by MO HealthNet to the Department of Social Services. § 208.215.4, RSMo. Participants are required to cooperate with MO HealthNet in pursuit of third parties who may be liable to pay for care and services covered by MO HealthNet. Id. A recipient who has notice of MO HealthNet’s right to third-party benefits and who directly receives a payment by the third party must pay MO HealthNet the full amount of the third-party benefits up to the amount of the lien or place the full amount of the third-party benefits in a trust account for the benefit of MO HealthNet pending judicial or administrative determination of MO HealthNet’s right to reimbursement. Id. Any person acting on behalf of a MO HealthNet beneficiary in pursuit of a claim which accrued as a result of a non-work related incident and which resulted in a payment for services by MO HealthNet must notify MO HealthNet upon agreeing to assist with the claim, and further must notify MO HealthNet of the result of the claim. § 208.215.5, RSMo. The plaintiff’s attorney must give thirty days' notice before any judgment, award, or settlement may be satisfied. Id. Participants, those suing for the wrongful death of a participant, their attorneys or representatives must promptly notify MO HealthNet of any recovery, and “shall immediately ~ 14 ~ Section 208.215.8 establishes MO HealthNet’s lien upon payments made towards a settlement or judgment. The lien applies to any moneys which come into the possession of plaintiff’s counsel and attaches to any verdict or judgment which may be recovered on a claim. Id. MO HealthNet may file an action to recover the funds due under section 208.215.1 against “the person, corporation, institution, public agency, or private agency liable to the participant, minor or estate.” § 208.215.2, RSMo. The Department of Social Services, the MO HealthNet participant or a defendant may file a petition for adjudication of the respective rights of the parties and enforcement of the lien. § 208.215.9, RSMo. The Court may determine the portion of recovery to be paid to the Department of Social Services following an evidentiary hearing on: 1) the amount of the charge sought to be enforced against the recovery, expressed as both a percentage of the gross recovery and as a percentage of the net recovery after subtraction of attorney’s fees and costs, and whether the department should bear a proportionate share of the fees and costs; 2) the amount of the attorney’s fees and costs incurred by the plan participant; 3) the total medical expenses incurred for the relevant care, the portions paid respectively by the participant, insurance, MO HealthNet and the portion unpaid; 4) whether the recovery is less than substantially full compensation for the injuries and medical expenses incurred; 5) the age of the participant and the participant’s dependents, the nature of the participant’s injuries, their impact on the participant’s employability, education and need for future treatment, and the costs of any such future treatment relative to the participant’s ability to meet those needs; and 6) the realistic ability of the participant to repay the lien. § 208.215.9(1) – (6), RSMo. The burden of proof lies with the party seeking the reduction of the amount of the lien. § 208.215.10, RSMo. The court may reduce and apportion the lien proportionate to the recovery of the claimant. The factors to be considered in such reduction include the nature and extent of the injury, the economic and non-economic loss, settlement offers, comparative negligence, and medical expenses and costs. § 208.215.11, RSMo. MO HealthNet shall pay its pro rata share of the attorney’s fees based on the amount of the lien compared to the total settlement amount. Id. The MO HealthNet lien does not affect attorneys’ liens asserted under section 484.140, RSMo but does take priority over all other liens. Id. MO HealthNet may also settle its claim for reimbursement and enforcement of the lien by considering the factors set forth above in section 208.215.9. § 208.215.12, RSMo. Medicare and Medicaid Liens >p15 Medicare and Medicaid Liens (Continued from page 14) Issues During Settlement Negotiations/Post-Judgment ISSUES FOR DEFENSE COUNSEL AND RECOMMENDATIONS A sizeable Medicare or Medicaid lien can make a settlement costprohibitive. Negotiating a lien is typically a time-consuming and arduous process. For that reason, it is in the interest of plaintiff’s counsel to begin to negotiate a reduction of the lien as early in the litigation as possible. Not all plaintiffs’ attorneys realize the importance of early contact with Medicare and MO HealthNet, so defense counsel should be prepared to prompt the interaction. Whether the case is resolved by settlement or judgment, a defendant must take steps to ensure Medicare and MO HealthNet liens are fully satisfied. Issues During Litigation/Investigation The newly-enacted Medicare reporting requirements require insurance carriers to notify Medicare of its potential right to reimbursement as soon as the carriers have cause to believe reimbursement may be due. Defense counsel should ensure their insurance clients are aware of and are complying with this law. Defense counsel should also ensure that early investigation is conducted on the existence of any potential Medicare liens. If a Medicare payment has been made, the insurance client must be notified immediately of the need to inform Medicare of its potential lien to avoid imposition of fines for a delay in reporting. Although MO HealthNet provisions do not carry the same penalties, failure to satisfy these liens could result in a satisfaction of judgment or settlement payment being rendered void. Unlike Medicare liens, the MO HealthNet lien can be adjudicated by the Court or negotiated by MO HealthNet; the final amount of the lien may therefore be determined during litigation, before settlement negotiations are conducted. Efforts to reduce Medicare or MO HealthNet lien amounts are often centered on disputing the relationship between particular health care services and the primary payer’s responsibility to reimburse Medicare or MO HealthNet. To that end, plaintiffs’ attorneys have used the testimony of defense experts to justify reduction of the lien. The process has been known to take years in some cases. Given the potential penalties to the client for failure to satisfy a lien, defense counsel must ensure that any Medicare or MO HealthNet lien is discovered as early as possible so the lien receives appropriate attention during the course of litigation. If the claimant is over age 65, under 65 but disabled or in end-stage renal disease, the existence of a Medicare lien should be presumed until proven otherwise. If the claimant is of limited means, the existence of a MO HealthNet lien must be investigated beyond simply submitting an interrogatory on the issue. Medical bills may reference a Medicare or MO HealthNet payment and should be inspected for such evidence. Also, the appropriate regional Medicare or Medicaid office will confirm both the existence and amount of a Medicare or MO HealthNet lien. Once existence of the lien is determined, the most complex issue to address is the final computation of the lien amount. The primary responsibility for this lies with plaintiff’s counsel, however defense counsel should cooperate and assist to the extent possible when necessary to ensure proper resolution of the lien. While the lien amount can be initially estimated from medical bills, defense counsel should contact the appropriate regional Medicare or Medicaid office to determine the exact amount of the lien. This should be done as soon as counsel has reason to believe the respective entity has made a payment for medical services on behalf of the plaintiff. The appropriate CMS Regional Office or the Medicare Secondary Payer Recovery Center can be reached at: 847-839-7700, 866-MSPRC-20, or through their website, www.cms.hhs.gov/MSPRecovClaimPro. The MO HealthNet Jefferson City office can be reached at 800-392-1261, 573-751-3425, or www.dss.mo.gov/mhd. Plaintiff’s counsel should be involved in, or at least apprised of, contact that defense counsel has with MO HealthNet, as he/she has an obligation to notify MO HealthNet of his/her involvement. If continuing care is expected, updated information on the lien amount must be obtained periodically throughout a case. Regardless of whether efforts to reduce a lien are successful, defense counsel must ensure that the full amount of the lien is or will be satisfied, either through reimbursement or compromise, before allowing a settlement or judgment payment to be made. Federal law specifically dictates that a primary payer may be required to pay for a lien twice if it is not satisfied with settlement or judgment proceeds. While Missouri law is not as explicit, it does prohibit satisfaction of a judgment or settlement without notice to MO HealthNet. Thus, MO HealthNet could challenge the satisfaction of a judgment or settlement. If such an action were pursued and plaintiff did not save sufficient funds to satisfy the lien, a defendant could ultimately have to pay a MO HealthNet lien amount twice. Indemnification of the defendant and the defendant’s insurer by the plaintiff for payment of the lien should be a mandatory term of any settlement so the defendant has a right of action against a plaintiff who fails to satisfy a lien. Defense counsel should not assume a lien will be satisfied, however; measures must be taken during the payment process to ensure Medicare or MO HealthNet will be reimbursed. Settlement/Judgment Payees and Ethical Issue www.MODLLaw.com Plaintiffs often demand payment of a settlement within days of an agreement being reached. If a lien exists and has not yet been negotiated, defendants can be left in a quandary about whether to include the lien-holder as a payee on a settlement check to ensure the lien is satisfied. Plaintiffs’ counsel typically do not want Medicare or MO HealthNet named as a payee on a draft for the full amount of the settlement because they will lose leverage in negotiating the lien and experience significant delays in receiving settlement proceeds. To address this, defendants have issued separate checks; one to the plaintiff and plaintiff’s counsel, and a second to plaintiff, plaintiff ’s counsel and the lien-holder in an Medicare and Medicaid Liens >p16 ~ 15 ~ Missouri Organization of Defense Lawyers (MODL) P.O. Box 1072 Jefferson City, Missouri 65102 First Class Mail U.S. Postage PAID Jefferson City, MO PERMIT NO. 118 Medicare and Medicaid Liens (Continued from page 15) amount sufficient to satisfy the lien. In that circumstance, a debate often arises regarding the amount to be held aside to ensure satisfaction of the lien. To resolve this debate and speed up the distribution of settlement proceeds, some plaintiffs’ counsel have been willing to agree to indemnify the defendant for any existing liens. The Supreme Court has recently made clear that this practice is not permitted by the Rules of Professional Conduct. On November 13, 2008, the Advisory Committee of the Supreme Court of Missouri issued Formal Opinion 125, “Agreeing to Indemnify Opposing Party as a Term of Settlement.” The Committee held that a guarantee to cover a client’s debt constitutes the provision of financial assistance to a client. Rule of Professional Conduct 4-1.8(e) prohibits a lawyer from providing financial assistance to a client in connection with a pending or contemplated litigation. Thus, the Rule precludes an attorney from agreeing to repay a client’s debt to a third party if the client fails to make the repayment out of settlement or judgment proceeds. Because the plaintiff’s counsel would violate Rule 4-1.8(e) by agreeing to indemnify the defendant for a lien, the defense attorney would commit a violation of Rule 4-8.4(a) if she requested or demanded the plaintiff’s attorney enter such an agreement. This Advisory Opinion further held that Rule 4-1.15(f) requires an attorney holding funds in which both his client and a third party have an interest to either disburse the funds to the third party, or hold the funds in trust to allow the dispute between the client and the third party to be resolved. If the dispute is not resolved in a reasonable time, the attorney must interplead the funds. The opinion goes on to state that if a valid lien exists and a plaintiff insists his attorney not satisfy it, the attorney must hold the funds in trust until the dispute can be resolved. This is consistent with the provisions of section 208.215.4, RSMo. Because this opinion prohibits incentivizing satisfaction of the lien by making plaintiffs’ counsel subject to a suit by defendants who are made to pay a lien amount twice, defense counsel must re-examine their practice for ensuring liens are satisfied. The Supreme Court Advisory Committee suggests and section 208.215.4 states the appropriate course is for plaintiff’s counsel to hold the funds in trust pending negotiation of the lien. In any settlement requiring court approval, the Order approving a settlement should reference plaintiff’s counsel’s responsibility to place a specific amount of the settlement proceeds in a trust account pursuant to Opinion 125. The release or settlement agreement should also include language referencing Opinion 125’s mandate that the plaintiff’s attorney hold funds sufficient to satisfy the lien in a trust account. Because this obligation already exists, such language in a lien-satisfaction clause would not violate Rule 4-1.15(f). See Advisory Opinion 125. Furthermore, inclusion of such language may help protect plaintiff’s counsel from the ire of a plaintiff demanding payment of the full amount of the settlement before a lien is satisfied. With inclusion of this language in the release and/or order, in most cases it would not be necessary to include Medicare or MO HealthNet as a payee on a settlement draft. Inclusion of the lienholder as a payee precludes plaintiff’s counsel from depositing the check into his or her trust account without endorsement of the check by a Medicare or MO HealthNet representative. As a practical matter, obtaining such an endorsement without the lienholder confiscating the entire settlement amount is impossible. Provided the release and/or order contains language regarding the amount of the settlement proceeds to be held in trust by plaintiff’s counsel, a second check which includes the lien-holder as a payee is also not necessary to ensure a defendant is sufficiently protected from an action for recovery on the lien. Of course, the best protection from such an action is to determine the final lien amount before settlement is reached so that satisfaction of the lien can be made directly by the defendant or its insurance carrier. In any event, the best practice would involve an agreement by plaintiff or plaintiff’s counsel to provide defense counsel with notice of satisfaction of the lien, whenever that may be achieved.
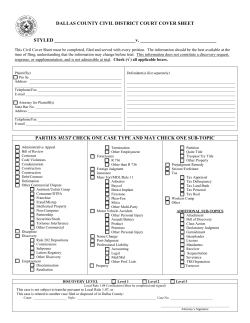









© Copyright 2026