
Review article COMMON CAUSES OF PAIN IN THE FOREFOOT IN ADULTS
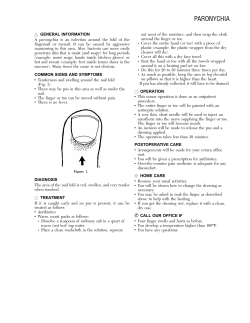
Review article COMMON CAUSES OF PAIN IN THE FOREFOOT IN ADULTS Michael J. Coughlin From Oregon Health Sciences University, Portland, USA A complaint of pain in the forefoot may be a potential source of frustration to the orthopaedic surgeon but the evaluation needed to give a definitive diagnosis is usually straightforward and the treatment uncomplicated. The forefoot includes the digits and extends as far proximal as the middle of the shafts of the metatarsals. The term metatarsalgia is often used to describe pain in the distal forefoot, but does not define a specific diagnosis or indicate a particular mode of treatment. Pain in the forefoot must be carefully analysed to establish a correct diagnosis. It is necessary to assist the patient in determining the exact location of the pain. This may not be easy since the initial complaint may be of a large area of ill-defined pain. With time, however, it is usually possible to isolate this to a small discrete site. Other pertinent information includes the presence of a deformity, inflammation of the soft tissue, pain on palpation of a specific region, and/or associated neuritic symptoms. Radiological studies are helpful in determining the presence and magnitude of deformities, although physical examination may be sufficient in the evaluation of many lesser abnormalities of the toes. Radiographs are most helpful in assessing the presence of intra-articular problems such as degenerative arthritis, Freiberg’s infraction, stress fracture of the metatarsal and inflammatory arthritis, but there is no substitute for an adequate physical examination. Radionucleide scanning, MRI and CT may be of value in establishing a diagnosis in the case of pain not associated with clinical or radiological deformity. Laboratory evaluation including a full blood count and measurement of the ESR, the level of uric acid and rheumatoid factor is occasionally helpful in the diagnosis of a patient with recalcitrant pain in the forefoot in whom inflammatory arthritis is suspected. Observation of the presence or absence of a callus associated with well-localised pain in the forefoot is the M. J. Coughlin, MD, Clinical Professor of Orthopaedic Surgery Oregon Health Sciences University, Portland, Oregon, USA. Correspondence should be sent to Professor M. J. Coughlin at Suite 503, 901 N Curtis Road, Boise, Idaho 83706, USA. ©2000 British Editorial Society of Bone and Joint Surgery 0301-620X/00/611422 $2.00 J Bone Joint Surg [Br] 2000;82-B:781-90. VOL. 82-B, NO. 6, AUGUST 2000 first step in the diagnostic evaluation (Fig. 1). A dorsal callus overlying a plantar flexed distal interphalangeal joint (DIP) occurs in a mallet-toe deformity and a similar callus overlying a plantar flexed proximal interphalangeal joint (PIP) in a hammer toe. With a claw toe, hyperextension of the metatarsophalangeal joint (MTP) and flexion of the PIP joint may be associated with a callosity beneath the involved head of the metatarsal, overlying the PIP joint, and even at the tip of the toe (Fig. 2). A callus localised to the lateral aspect of the fifth toe may indicate a hard corn while that in the webspace between the lesser toes occurs with a soft corn. A callus overlying the lateral aspect of the head of the fifth metatarsal is associated with a bunionette. With an intractable plantar keratosis (IPK) a callus develops beneath the head of a lesser metatarsal. The complaint of pain in the forefoot in the absence of a callus should alert the physician to other abnormalities of the soft tissue or joint. The presence of neuritic symptoms in the digits may indicate an interdigital neuroma. In the absence of such symptoms, capsulitis or instability of a lesser MTP joint should be considered. Palpation of the painful areas can differentiate many of these diagnoses. A positive drawer sign (Fig. 3) in a lesser MTP joint and/or malalignment of the symptomatic toe (Fig. 4) may help in the diagnosis of capsulitis, synovitis or instability of the joint. Often symptoms may be vague and ill-defined, necessitating repeated physical and radiological evaluation to establish a correct diagnosis. Problems in the first ray such as hallux valgus, hallux rigidus, and sesamoiditis are beyond the scope of this discussion, but have been thoroughly discussed in other 1-3 articles. Interdigital neuroma This frequent cause of ill-defined pain in the forefoot commonly occurs in the second or third intermetatarsal 4,5 space, but rarely in the first or fourth. It is unusual for 6 two neuromas to occur in the same foot. Symptoms often increase with activity and diminish with the removal of shoes. Numbness or neuritic symptoms may be noted in the distribution of either the second or third common digital nerve (Fig. 5). It is important to assess the state of the circulation of the foot since vascular insufficiency is an 781 782 M. J. COUGHLIN Fig. 1 Algorithm for diagnosis of pain in the forefoot. Fig. 3 With the involved toe grasped between the examiner’s thumb and index finger, a dorsalplantar stress will often elicit exquisite pain in the involved MTP joint. This finding is absent in patients with a symptomatic interdigital neuroma. Fig. 2 A hyperextended MTP joint and a flexion deformity of the PIP joint occur with a claw toe. A callus may develop beneath the involved metatarsal head, on the dorsal aspect of the DIP joint, and at the tip of the involved toe. occasional cause of pain in the forefoot. The presence or absence of instability of a lesser metatarsophalangeal joint, a plantar callosity, and deformity of a lesser toe should be noted. The intermetatarsal spaces are palpated since pain may be experienced on compression. With simultaneous compression of both the transverse arch and the involved 7 interspace, a click (Mulder’s sign) may be demonstrated as the neuroma is subluxed beneath the transverse metatarsal ligament. The clinician aims to educate and assist the patient in defining the location of pain. Over time, it is often possible to pinpoint the exact area. When this proves difficult, an 8 injection with a local anaesthetic agent may be helpful. Multiple injections may be necessary to differentiate pain originating from either the second and third intermetatarsal spaces or the adjacent MTP joints. Temporary relief after infiltration of anaesthetic around a specific nerve and increased pain when the anaesthesia subsides is diagnostic of an interdigital neuroma. Treatment. Non-surgical management of a symptomatic THE JOURNAL OF BONE AND JOINT SURGERY COMMON CAUSES OF PAIN IN THE FOREFOOT IN ADULTS Fig. 4a Fig. 4b 783 Fig. 4c Fig. 4d Figure 4a – Photograph showing the clinical appearance of mild cross-over second toe. Figure 4b – Radiological appearance demonstrating medial deviation of the second toe. Figure 4c – Photograph showing end-on view of cross-over second toe. Figure 4d – Photograph showing severe cross-over second toe. Fig. 5 Diagram showing an interdigital neuroma with entrapment of the common digital nerve beneath the transverse metatarsal ligament. Hyperaesthesia and/or radiating pain may be observed. The shaded area in the inset shows the neuritic area in a neuroma of the third intermetatarsal space. neuroma requires diminished activity, the wearing of roomy footwear or modification of the shoe with a less constricting toe box, the administration of non-steroidal anti-inflammatory drugs and the redistribution of weight-bearing with a metatarsal pad placed just proximal to the area of the symptomatic neuroma (Fig. 6a). Occasionally, an injection of corticosteroid in the involved interspace will relieve 9,10 symptoms. Conservative measures are successful in 5,11,12 over 50% of cases, but when these fail operation may be considered. 5,13 A dorsal approach is preferred since this avoids the possibility of a painful plantar scar which may be the source of intractable postoperative pain. The incision can also be extended should other pathology be identified in the webspace. Transection of the transverse metatarsal ligament exposes the common digital nerve and the neuroma in the depths of the intermetatarsal space. The nerve is sectioned distally at the level of division into the digital nerves 14 and any capsular branches to the MTP joint are severed. The nerve is transected in the interosseous region and the proximal segment allowed to retract. In general, the results of operation are satisfactory with relief of symptoms in VOL. 82-B, NO. 6, AUGUST 2000 Fig. 6a Fig. 6b Figure 6a – Photograph showing a soft wool pad placed on the insole just proximal to the symptomatic area which may relieve symptoms. Figure 6b – A Harris Mat study shows increased pressure beneath the involved metatarsal head. 4,5,12 about 80% of patients. Postoperative complications may include recurrence of or failure to relieve the pain, limitation in shoe wear, a painful scar or a painful sensory deficit. Intractable plantar keratosis When a callus develops beneath one or more of the lateral metatarsals, it is termed an intractable plantar keratosis (IPK). It may be a well-localised discrete keratosis or a 15 large diffuse callus (Fig. 7). The latter often develops as a result of repetitive abrasion associated with athletic activities, but is also associated with a long second and third metatarsal. Pain often increases with build-up of a thick 784 M. J. COUGHLIN Fig. 7a Fig. 7b Fig. 7c Fig. 7d Photographs showing various plantar keratoses: a) a small discrete keratosis; b) a large keratotic lesion; c) a diffuse abrasion-type callosity; and d) a verruca. Fig. 8 Fig. 9a Through a dorsal approach, a plantar condylectomy resects 30% of the plantar metatarsal head. A prominent fibular condyle is resected. An intramedullary Kirschner wire may be used to stabilise the toe. callus. A discrete callus develops most often beneath a single metatarsal head and is associated with an enlarged 16 lateral condyle. It is important to determine the magnitude of symptoms and the duration of pain as well as which activities influence discomfort. Minimal symptoms rarely demand treatment. Evaluation using the Harris Mat (Fig. 6b) or a similar pressure plate, together with weightbearing radiographs using a marker placed beneath the keratosis, will help to determine the location of the IPK and any osseous abnormalities. On examination, it is important to differentiate a callosity from a verruca or wart (Fig. 7). A wart is infrequently located beneath the head of a lesser metatarsal. Shaving of a callosity helps to differentiate it from an IPK since there are minute punctate arterioles in the centre of a wart while an IPK has an avascular centre. Treatment. This involves trimming the callus to relieve pressure. Initially, the physician may debulk the callus and then on a weekly basis the patient may use a rasp or pumice stone to reduce the keratosis further. A wool pad placed on the insole just proximal to the symptomatic metatarsal head (Fig. 6a) helps to redistribute pressure to the metatarsal diaphysis. A prefabricated or custom orthosis can then be Fig. 9b Diagram showing a capital oblique osteotomy. Figure 9a – A sagittal saw is used to create an oblique osteotomy as parallel as possible to the plantar aspect of the foot. The amount of proximal displacement is determined before operation. If elevation is desired, two or three saw blades may be stacked together in the saw to create a larger area of bone resection which elevates the capital fragment. Figure 9b – As the osteotomy is completed, the capital fragment is displaced proximally and is fixed by one or two mini-fragment compression screws. The remaining metaphyseal flare is excised. used to maintain this redistribution of pressure. With unremitting pain, operation may be warranted. A plantar condylectomy is indicated for a well-localised discrete IPK (Fig. 8). Through a dorsal approach the MTP joint is plantar flexed and the plantar aspect of the metatarsal head is shaved. For a large diffuse callus, a capital oblique osteotomy is performed on the second and/or third metatarsals (Fig. 9). THE JOURNAL OF BONE AND JOINT SURGERY COMMON CAUSES OF PAIN IN THE FOREFOOT IN ADULTS Fig. 10a Fig. 10b Figure 10a – The Chevron osteotomy is proximally based and orientated in a medial/lateral direction. The capital fragment is shifted medially and stabilised with a 0.045 Kirschner wire. Figure 10b – The midshaft oblique osteotomy is directed in a dorsal/proximal to plantar/distal direction and the distal fragment is rotated in a medial direction to reduce the wide intermetatarsal angle. It is stabilised by two mini-fragment compression screws. 16 Mann and DuVries described the results of MTP arthroplasty and condylectomy in 142 feet, noting that 95% of the results were satisfactory with elimination of or a substantial reduction of the callus in these patients. Transfer lesions occurred in 13% of cases. While several techniques of distal metatarsal osteotomies have been proposed for the 17-20 (Weil, personal communication), varitreatment of IPK able results have been reported, with the incidence of 17 20 postoperative pain varying from 12% to 53%, transfer 20 21 20 lesions from 32% to 41%, recurrence in 50% and 17 21 21 malunion or pseudarthrosis in 8% to 53%. Trnka et al in comparing distal metatarsal osteotomy with and without internal fixation found significantly better results with a capital oblique osteotomy noting no transfer lesions but recurrent metatarsalgia or pseudarthrosis in 15 cases. These procedures may be associated with delayed or nonunion or transfer lesions and should be undertaken only after conservative measures have been exhausted. Unsecured and simultaneous multiple osteotomies have a high rate of 20 complications including malunion and transfer lesions. Bunionettes A bunionette is characterised by a painful callus overlying the head of the fifth metatarsal and results from friction between an underlying bony prominence and constricting VOL. 82-B, NO. 6, AUGUST 2000 785 footwear. Neuritic symptoms may develop because of compression of the lateral digital nerves of the fifth toe. With a progressive deformity, ulceration or infection may occur. On physical examination a lateral keratosis is seen in approximately 70% of cases, a plantar keratosis in 10% and 22 combined plantar and lateral keratosis in 20%. Radiographs may demonstrate a large head of the fifth metatarsal or a widening of the angle between the fourth and fifth metatarsals and an abduction deformity of the fifth toe at the MTP joint. Treatment. Symptoms can often be substantially reduced with a change in footwear or by stretching the shoe overlying the head of the fifth metatarsal. Shaving of the hypertrophic callus and placing a soft wool pad just proximal to the head of the fifth metatarsal may also reduce symptoms. A prefabricated or custom orthotic device may eliminate pronation and thus reduce symptoms. Surgery may be considered when symptoms are refractory to conservative care. Lateral condylectomy has been 23 associated with minimal angular correction and is rarely 15,24 While many performed as an isolated procedure. operations have been suggested to correct a symptomatic bunionette deformity, the author currently favours two procedures. The location of the keratosis (plantar, lateral or plantar-lateral) helps to determine the appropriate choice for correction of the deformity. In the presence of a lateral callosity and a large head of the fifth metatarsal, a 25 Chevron osteotomy is performed (Fig. 10a). When there is a wide angle between the fourth and fifth metatarsals, an 22 oblique diaphyseal osteotomy is carried out (Fig. 10b). For a combined plantar and lateral keratosis, a modification of the oblique osteotomy is performed in which the saw blade is angled in a more dorsal direction allowing the 22 distal fragment to elevate as it is rotated medially. Extensive stripping of soft tissue, multiple metatarsal osteotomies, and unsecured osteotomies in general should be avoided. 22 Coughlin reported a satisfaction rate of 93% after a diaphyseal osteotomy. No cases of nonunion developed. 25 Kitaoka et al reported experience with the distal Chevron metatarsal osteotomy for correction of a bunionette in 19 feet with good results in 17. One case of transfer metatarsalgia was noted. Metatarsophalangeal joint instability The diagnosis of instability of a lesser MTP joint can be difficult to make as ill-defined pain in the forefoot can also be associated with both extra-articular abnormalities such as an interdigital neuroma and formation of a synovial cyst, and intra-articular disorders, including inflammatory arthritis, degenerative arthritis and Freiberg’s infraction. The second MTP joint is most often involved. In older women, it has been suggested that the long-term use of high-heeled shoes places the lesser MTP joints in a position of chronic hyperextension, which eventually leads to attenuation and 786 M. J. COUGHLIN Fig. 11a Fig. 11b Fig. 11c Figure 11a – Photograph showing methods of padding the lesser toes which include a pad over the hard corn on the fifth toe, a pad placed in the webspace to alleviate pain from a soft corn, and tube gauze placed over either a soft corn or hammer-toe deformity. Figures 11b and 11c – Photographs showing the taping technique. Adjacent toes may be taped to stabilise an involved toe. This technique is used both before and after operation. A sling-type method of taping may be used to pull the toe in a plantar/lateral direction. It is also secured by circumferential tape around the forefoot. Fig. 13a Fig. 12 Diagram showing MTP arthroplasty. Reefing of the lateral capsuloligamentous complex combined with a medial release may achieve soft-tissue realignment. later rupture of the plantar capsule with resultant instab26 ility. Instability has also been reported in younger athletes 27,28 associated with an overuse syndrome. The initial complaint of pain in the forefoot must be differentiated by repeated examination to pinpoint an exact area of tenderness. Palpation often isolates the pain to the joint capsule beneath the involved metatarsal head. Typically, neuritic symptoms are not noted nor is pain observed in the second or third intermetatarsal spaces. The use of a drawer test (Fig. 2) is a reliable means of differentiating capsulitis and instability of the MTP joint from an interdigital neuroma. Early on, without obvious clinical or radiological deformity, the diagnosis of instability of the MTP joint is more difficult to make. With time, obvious deformity of the lesser toe is characterised by dorsal/medial or dorsal deviation at the MTP joint (Fig. 4). This may occur acutely although it usually progresses insidiously over several months. Serial injections of an anaesthetic agent performed during sequential office visits may be helpful in determining the location of maximal symptoms. Radiological examination may demonstrate widening of the MTP joint because of synovitis or an effusion, narrowing of the space secondary to degenerative joint disease or hyperextension of the MTP joint, or medial or lateral malalignment due to Fig. 13b Fig. 13c Figures 13a and 13b – The tendon of flexor digitorum longus is released through a distal puncture wound at the level of the DIP joint and brought out through the more proximal plantar incision. The tendon is split longitudinally and a limb of the tendon is passed through the tunnels on either side of the proximal phalanx. Figure 13c – The limb may be tightened to create more medial or lateral deviation depending upon the alignment desired. The tendon limbs are then tensioned appropriately to control dorsiflexion/plantar flexion and rotation of the digit, and sutured to the extensor tendon with the toe in proper alignment. THE JOURNAL OF BONE AND JOINT SURGERY COMMON CAUSES OF PAIN IN THE FOREFOOT IN ADULTS 787 Photographs showing a) mallet-toe and b) hammer-toe deformities. Fig. 14a Fig. 14b capsular rupture consistent with instability of the MTP joint. Treatment. Conservative treatment may be successful when capsulitis or instability is diagnosed early. Before the onset of deformity, the use of a metatarsal pad placed just proximal to the involved metatarsal head helps to redistribute weight-bearing (Fig. 6a). Taping adjacent toes or taping the toes using a sling technique to minimise dorsiflexion also helps (Fig. 11). The judicious use of an intraarticular injection of steroid has been shown to be effective 29 in decreasing synovitis and pain. With continued discomfort or progression of the deformity, surgical intervention may be necessary. Operative correction of instability of the lesser MTP joints is performed in a sequential fashion depending upon the magnitude of the deformity. If hyperextension is present a capsulotomy of the MTP joint, lengthening of the extensor tendon and fixation with a Kirschner wire may stabilise and realign the involved toe. With medial deviation, lateral 26 deviation is uncommon, an additional reefing of the ruptured or attenuated lateral capsuloligamentous complex may be necessary to realign the MTP joint (Fig. 12). A flexor tendon transfer is often added to give dorsoplantar stability to the toe (Fig. 13). For severe subluxation and dislocation of the MTP joint, a more extensive soft-tissue release and reconstruction may be necessary. Bony decompression with a distal metatarsal osteotomy (Fig. 9) has been used successfully in combination with soft-tissue 21 realignment in cases of more severe deformity. Reconstruction of the unstable deviated lesser MTP joint is a technically demanding procedure which requires a meticulous surgical technique and careful postoperative followup. Decreased range of movement, recurrent deformity, and transfer metatarsalgia are complications which may be associated with attempts at surgical reconstruction. 30 Coughlin reported good or excellent long-term results in 93% of cases in which the sequential technique described above had been used. In a later report on a younger group of more athletic patients, 73% were noted to have 21 good or excellent results. Trnka et al described 15 lesser toes treated by a capital oblique osteotomy for subluxation VOL. 82-B, NO. 6, AUGUST 2000 of the lesser MTP joint and noted no symptomatic transfer lesions. All subluxated or dislocated MTP joints were successfully reduced. Hammer toes, mallet toes, claw toes IPKs may develop in association with contractures of the lesser toes because of the buckling effect on the toe (Fig. 2). Realignment of the MTP and interphalangeal joints may decrease plantar pressure and relieve symptomatic callosities. A mallet toe is characterised by a flexion contracture of the DIP joint (Fig. 14a), a hammer toe by a flexion contracture of the PIP joint (Fig. 14b) and a claw toe by hyperextension of the MTP joint and flexion of the PIP joint (Fig. 2). These deformities may be flexible and easily correctable, but eventually a rigid contracture may develop. The presence and location of callosities, the position of the involved toe and the magnitude and rigidity of the deformity determine the method of treatment. Treatment. The use of roomy shoes which avoid pressure on the deformed toe will often relieve discomfort. Padding of a toe (Fig. 11a), shaving of a prominent callus and the use of a soft wool pad placed just proximal to the plantar callosity (Fig. 6a) may reduce symptoms and allow increased activity. When these measures do not alleviate symptoms, surgery may be considered. The distal condyles of the middle phalanx and the proximal articular surface of the distal phalanx are resected to 31,32 (Fig. 15). correct a fixed mallet-toe deformity With a fixed hammer toe, the condyles of the proximal phalanx and the articular surface of the middle phalanx are resected and a 0.05 Kirschner wire is used to stabilise the 33-35 repair (Fig. 16). For correction of a flexible hammer toe or a claw toe which is correctable passively, a flexor tendon transfer is 32,36,37 undertaken (Fig. 13). This allows flexor digitorum longus to assume the function of the intrinsic muscles, namely plantar flexion of the MTP joint and extension of the interphalangeal joint, while removing a deforming 32 force. 31 Coughlin described the results of mallet toes treated by 788 M. J. COUGHLIN resection arthroplasty. Relief of pain was achieved in 97% of patients and satisfactory results were noted in 86%. 35 Coughlin et al also reported the results of the treatment of 118 hammer toes by resection arthroplasty. Relief of pain was noted in 92% and subjective patient satisfaction was 36 achieved in 84%. Barbari and Brevig noted a high level of satisfaction in patients after flexor tendon transfer for a 8 flexible hammer-toe deformity, but Thompson and Deland found that in only seven of 13 cases was complete correction of a subluxated MTP joint achieved. Hard and soft corns Fig. 15 Diagram showing correction of a mallet-toe deformity. The condyles of the middle phalanx are excised. The articular surface of the distal phalanx is resected and a flexor tenotomy is performed in the depths of the wound. The repair is stabilised with a 0.045 Kirschner wire. Fig. 16a Fig. 16b Diagram of correction of a hammer-toe deformity showing a) the proposed resection and b) after repair with excisional arthroplasty and fixation with a Kirschner wire (X, MTP release and extensor tenotomy performed for fixed claw-toe deformity). A hard corn is a hyperkeratotic lesion which develops on the lateral border of the fifth toe usually because of extrinsic pressure from constricting shoe wear (Fig. 17). A painful callus develops over a prominent lateral distal condyle of the proximal phalanx. A soft corn is a hyperkeratotic lesion which occurs either in the webspace or between two adjacent toes (Fig. 18). It is often exquisitely painful and may be misdiagnosed as a mycotic infection because of maceration of the skin. With radiological examination, a marker placed over the cutaneous lesion may help to localise the underlying osseous exostosis. Treatment. Treatment of a hard corn is directed at reducing pressure over it by the wearing of roomy shoes or by modifying existing footwear. Careful shaving of the callus, dessication of any macerated areas and placement of a pad between adjacent toes or over the border of the toe (Fig. 11a) often eliminates compression and relieves symptoms. When these measures are unsuccessful, surgical resection of the prominent exostosis may be indicated. The preoperative planning of surgical repair of a soft corn involves the decision as to whether to excise one or both lesions. If there is a large callosity and a small corresponding lesion, resection of the large exostosis will usually suffice. With two relatively similar sized lesions, a dual resection is recommended (Fig. 18c). For a hard corn, a lateral condylectomy of the distal aspect of the proximal phalanx is undertaken (Figs 17 and 17b). No results have been reported on the value of lateral exostectomy for the treatment of a hard corn. Zeringue and 38 Harkless evaluated 16 patients who had a PIP arthro- Photographs showing a) a hard corn, b) a longitudinal incision centred over the distal condyle and the exostosis resected with a rongeur, and c) repair of the capsule to prevent subluxation. Fig. 17a Fig. 17b Fig. 17c THE JOURNAL OF BONE AND JOINT SURGERY COMMON CAUSES OF PAIN IN THE FOREFOOT IN ADULTS Fig. 18a Fig. 18b 789 Fig. 18c Photographs (a,b) of a hard corn and diagram (c) showing the resection area of a hard and soft corn. plasty of the fifth toe and a lateral condylectomy of the proximal phalanx of the fourth toe for a soft corn between the fourth and fifth toes. No recurrence of the lesion was noted at a mean follow-up of 33 months. Proximal forefoot pain Although most abnormalities of the lateral forefoot occur either in the digits or at the level of the lesser MTP joints, on occasion a patient will complain of pain in the midmetatarsal region. The onset may be variable, but when pain is felt in the diaphysis of the metatarsal a stress fracture should be considered. Pain on direct palpation and moderate diffuse swelling localised to a specific metatarsal are characteristic of this condition. Although routine radiography may not show the lesion, a positive bone scan may be obtained. With pain in the proximal forefoot, consideration should also be given to entrapment neuropathy of the 39-41 which may be susdeeper superficial peroneal nerves tained after injury to the dorsum of the foot or the anterior aspect of the lower leg. A positive nerve-percussion test and associated neuritic symptoms with decreased sensation in the distribution of the involved nerve may give clues to this diagnosis. Conclusions Pain in the forefoot or metatarsalgia is frustrating for the patient and a challenging diagnostic problem. A meticulous history will elicit information regarding exacerbation of symptoms such as athletic activity and specific shoe wear. Careful observation will delineate the presence or absence of callosities and anatomical deformity, and palpation will further define the exact location of pain. Radiological examination, imaging studies and laboratory tests will assist in further differentiating the vague symptoms of metatarsalgia into a specific diagnosis for which appropriate treatment can be initiated. No benefits in any form have been received or will be received from a commercial party related dirctly or indirectly to the subject of this article. VOL. 82-B, NO. 6, AUGUST 2000 References 1. Coughlin MJ. Hallux valgus: an instructional course lecture. J Bone Joint Surg [Am] 1996;78-A:932-66. 2. Shereff MJ, Baumhauer JF. Hallux rigidus and osteoarthritis of the first metatarsophalangeal joint: an instructional course lecture. J Bone Joint Surg [Am] 1998;80-A:898-908. 3. Coughlin MJ. Sesamoid pain: causes and treatment. AAOS Instructional Course Lectures 1990;39:23-35. 4. Friscia DA, Strom DE, Parr JW, Saltzman CL, Johnson KA. Surgical treatment for primary interdigital neuroma. Orthopedics 1991;14:669-72. 5. Mann RA, Reynolds JC. Interdigital neuroma: a critical clinical analysis. Foot Ankle 1983;3:238-43. 6. Thompson FM, Deland JT. Occurrence of two interdigital neuromas in one foot. Foot Ankle 1993;14:15-7. 7. Mulder JD. The causative mechanism in Morton’s metatarsalgia. J Bone Joint Surg [Br] 1951;33-B:94-5. 8. Thompson FM, Deland JT. Flexor tendon transfer for metatarsophalangeal instability of the second toe. Foot Ankle 1993;14:385-8. 9. Greenfield J, Rea J, Ilfeld FW. Morton’s interdigital neuroma: indications for treatment by local injections versus surgery. Clin Orthop 1984;185:142-4. 10. Rasmussen MR, Kitaoka HB, Patzer GL. Nonoperative treatment of plantar interdigital neuroma with a single corticosteroid injection. Clin Orthop 1996;326:188-93. 11. Bennett GL, Graham CE, Mauldin DM. Morton’s interdigital neuroma: a comprehensive treatment protocol. Foot Ankle Int 1995;16:760-3. 12. Dereymaeker G, Schroven I, Steenwreckx A, Stuer P. Results of excision of the interdigital nerve in the treatment of Morton’s metatarsalgia. Acta Orthop Belg 1996;62:22-5. 13. Coughlin MJ. Soft tissue afflictions of the foot. In: Chapman MW, ed. Operative orthopaedics. 2nd edition. Vol. 3. Philadelphia: J. B. Lippincott, 1993:2287-98. 14. Amis JA, Siverhus SW, Liwnicz BH. An anatomic basis for recurrence after Morton’s neuroma excision. Foot Ankle 1992;13:153-6. 15. Mann RA, Coughlin MJ. Intractable plantar keratoses and bunionettes. In: Coughlin MJ and Mann RA, eds. Video textbook of foot & ankle surgery. St Louis: Medical Video Productions, 1991:85-103. 16. Mann RA, DuVries HL. Intractable plantar keratosis. Orthop Clin North Am 1973;4:67-73. 17. Helal B. Metatarsal osteotomy for metatarsalgia. J Bone Joint Surg [Br] 1975;57-B:187-92. 18. Helal B, Greiss M. Telescoping osteotomy for pressure metatarsalgia. J Bone Joint Surg [Br] 1984;66-B:213-7. 19. Pedowitz WJ. Distal oblique osteotomy for intractable plantar keratosis of the middle three metatarsals. Foot Ankle 1988;9:7-9. 20. Winson IG, Rawlinson J, Broughton NS. Treatment of metatarsalgia by sliding distal metatarsal osteotomy. Foot Ankle 1988;9:2-6. 21. Trnka HJ, Muhlbauer ¨ M, Zettl R, Myerson MS, Ritschl P. Comparison of the results of the Weil and Helal osteotomies for the treatment of metatarsalgia secondary to dislocation of the lesser metatarsophalangeal joints. Foot Ankle Int 1999;10:72-9. 790 M. J. COUGHLIN 22. Coughlin MJ. Treatment of bunionette deformity with longitudinal diaphyseal osteotomy with distal soft tissue repair. Foot Ankle 1991;11:195-203. 23. Kitaoka HB, Holiday AD. Lateral condylar resection for bunionette. Clin Orthop 1992;278:183-92. 24. Mann RA, Coughlin MJ. Keratotic disorders of the plantar skin. In: Coughlin MJ and Mann RA, eds. Surgery of the foot & ankle. 7th edition. St Louis: Mosby Yearbook, 1999:392-436. 25. Kitaoka HB, Holiday AD, Campbell DC. Distal chevron metatarsal osteotomy for bunionette. Foot Ankle 1991;12:80-5. 26. Coughlin MJ. Subluxation and dislocation of the second metatarsophalangeal joint. Orthop Clin North Am 1989;20:535-51. 27. Coughlin MJ. Forefoot disorders. In: Baxter D, ed. The foot and ankle in sport. St Louis: Mosby Yearbook, 1995:221-44. 28. Coughlin MJ. Second metatarsophalangeal joint instability in the athlete. Foot Ankle 1993;14:309-19. 29. Mizel MS, Michelson JD. Nonsurgical treatment of monarticular nontraumatic synovitis of the second metatarsophalangeal joint. Foot Ankle Int 1997;18:424-6. 30. Coughlin MJ. Crossover second toe deformity. Foot Ankle 1987; 8:29-39. 31. Coughlin MJ. Operative repair of the mallet toe deformity. Foot Ankle Int 1995;16:109-16. 32. Coughlin M, Mann R, Vol. 1. Lesser toe deformities. In: Coughlin MJ and Mann RA, eds. Surgery of the foot & ankle. 7th edition, St Louis: Mosby Yearbook, 1999:320-91. 33. Coughlin MJ. Lesser toe deformities. Orthopedics 1987;10:63-75. 34. Coughlin MJ. Mallet toes, hammer toes, claw toes and corns: causes and treatment of lesser-toe deformities. Postgrad Med 1984;75:191-8. 35. Coughlin MJ, Dorris J, Polk E. Operative repair of the fixed hammertoe deformity. Foot Ankle Int 2000;21:94-104. 36. Barbari SG, Brevig K. Correction of clawtoes by Girdlestone-Taylor flexor-extensor transfer procedure. Foot Ankle 1984;5:67-73. 37. Coughlin MJ. Lesser toe abnormalities. In: Chapman M, ed. Operative orthopaedics. 2nd edition, Vol 3. Philadelphia: J. B. Lippincott, 1993:2213-24. 38. Zeringue GN, Harkless LB. Evaluation and management of the web corn involving the fourth interdigital space. J Am Podiatr Med Assoc 1986;76:210-3. 39. Deese JM, Baxter DE. Compressive neuropathies of the lower extremity. J Musculoskeletal Med 1988;5:68-91. 40. Gessini L, Jandolo B, Peitrangel A. The anterior tarsal tunnel syndrome: report of four cases. J Bone Joint Surg [Am] 1984;66-A:786-7. 41. Kernohan J, Levack B, Wilson JN. Entrapment of the superficial peroneal nerve: three case reports. J Bone Joint Surg [Br] 1985;67-B:60-1. THE JOURNAL OF BONE AND JOINT SURGERY










© Copyright 2026