
Document 15372
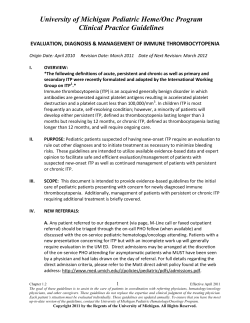
6 Platelet abnor Dr Simon McRae CBE illustrated report Analytes Result Range ✜ Analytes Haemoglobin 140 g/L (115 – 155) White Cell Count RBC 4.26 x 1012 / L (3.80 – 5.20) Neutrophils PCV 0.42 L/L (0.35 – 0.45) Lymphocytes Result 59.0 % 34.0 % Result Range 5.03 x l 09/L (4.00 – 11.00) 2.97 x l 09/L (1.80 – 7.50) 9 (1.00 – 3.50) 9 1.71 x l 0 /L MCV 90.0 fL (80.0 – 98.0) Monocytes 6.0 % 0.30 x l 0 /L (0.20 – 0.80) MCH 32.9 pg (27.0 – 33.0) Eosinophils 0.8 % 0.04 x l 09/L (0.02 – 0.50) MCHC 330 g/L (315 – 355) Basophils RDW 14.0 % (11.5 – 15.5) Platelets *52 (150 – 400) 0.2 % 9 0.01 x l0 /L (0.00 – 0.10) ✜ Female reference ranges P latelet abnormalities are common and often discovered as an incidental finding during ‘routine’ investigations; however, as consequences range from benign to fatal they create an important diagnostic challenge. Thrombocytosis No Quantitative defects of platelets, either too many (thrombocytosis) or too few (thrombocytopenia), can lead to the clinical complications of thrombosis or bleeding respectively. The purpose of this article is to provide a diagnostic approach to the underlying cause of these quantitative platelet disorders. ? Myeloproliferative Primary (Haematology referral) Reactive ? ? Myelodysplasia Thrombocytosis Defined as a platelet count greater than 400 x 109/L, there are numerous potential causes of thrombocytosis. Broadly they can be divided into primary (marrow disorders) and secondary (reactive) causes. Before considering a primary marrow disorder as the cause of an elevated platelet count, a secondary or reactive cause should be excluded. IMVS Newsletter 68 Summer 2008 Positive Negative BCR-ABL CML ET PRV Myelofibrosis Bone Marrow to confirm Yes Treat underlying cause 7 Part lV next? malities REACTIVE CAUSES Reactive causes are by far the most common cause of thrombocytosis in the general population. The clinical context in which thrombocytosis occurs may suggest that the increased platelet count is reactive in nature. Common scenarios include: • iron deficiency • inflammatory disorders – e.g. connective tissue disorders, inflammatory bowel disease, tissue injury/trauma, sepsis or infection • malignancy • previous splenectomy • rebound thrombocytosis following haemorrhage. As well as causing thrombocytosis in its own right, iron deficiency may mask an underlying diagnosis of polycythaemia rubra vera (PRV) and hence should be excluded. Similarly, the possibility of underlying malignancy needs to be considered. Investigation to exclude it should be guided by clinical symptoms and signs. you n o w ? did A normal kplatelet count is 150 – 400 x 109/L. With a life span ~ 10 days, an average 15 x 1010 platelets must be produced every day. † Myelodysplasia is a common cause of thrombocytopenia >60 years, and may be associated with dyplastic features on film. * Dependent on severity. While spontaneous bleeding is uncommon in patients with a platelet count >30 x 109/L, for those <100 x 109/L consider referral. Thrombocytopenia† Abnormal Platelet clumps Platelets abnormal Spurious? Inherited Red cells abnormal Red + white cells abnormal Pancytopenia (see text) Abnormal Normal APTT / INR D-dimer DIC? Microangiopathy? Thrombocytopenia Thrombocytosis after an acute insult such as trauma may persist for up to a month, and can reach levels as high as 1000 x 109/L and hence the magnitude of the increase alone cannot be used to distinguish primary from reactive causes. Further laboratory investigation may provide additional supportive evidence. A concurrent marked acute phase response (e.g. raised ESR, CRP) suggests reactive thrombocytosis, although it does not entirely exclude a primary process. With the advent of automated counters, the finding of thrombocytopenia, defined as a platelet count of less than 150 x 109/L, has become a common clinical problem. The implications of the underlying cause of thrombocytopenia range in severity from having no clinical relevance to being potentially fatal. Patients in whom a secondary cause for thrombocytosis cannot be identified, particularly when the platelet count is persistently above 600 x 109/L, should be referred to a haematologist to exclude a primary bone marrow disorder (see Thrombocytosis Referrals). Spurious causes of thrombocytopenia must be excluded to avoid unnecessary further investigation and management. Clot formation in the sample is a common cause of thrombocytopenia; these samples are discarded and a repeat sample recommended. IMVS Newsletter 68 Summer 2008 Immune (ITP) Normal Blood film The IMVS will perform a blood film examination as an initial investigation in all patients with thrombocytopenia. Approximately 0.2% of all individuals will have platelets that clump when their blood is exposed to the EDTA anticoagulant in blood specimen containers (purple top). The clumping causes a falsely low platelet count, an abnormality that will only be detected by examining a blood film. Where platelet clumping due to EDTA is confirmed we recommend collecting an additional sample in a Na citrate (blue top) tube for future requests. ASSOCIATED ABNORMALITIES IS IT ARTEFACTUAL? Thrombocytopenia associated with pancytopenia most commonly reflects bone marrow failure due to conditions such as acute leukaemia or myelodysplasia, marrow infiltration by secondary processes such as carcinoma, or less commonly aplastic anaemia. 8 Important treatable causes such as B12/folate deficiency or hypersplenism should not be forgotten. In patients receiving cytotoxic drugs marrow suppression is also a common cause. Findings in the peripheral blood film such as immature cells in leukaemic conditions, dysplastic changes in myelodysplasia, or a leuco-erythroblastic picture in marrow infiltration may suggest the likely diagnosis; a bone marrow examination is normally required for confirmation. Hypersplenism, often associated with liver disease, is a relatively common cause of pancytopenia due to the sequestration of blood within the spleen; it should be considered in the appropriate patient groups. Immune mediated Immune thrombocytopenic purpura is a relatively common cause of isolated thrombocytopenia in both adults and children. The underlying cause is thought to be accelerated platelet destruction due to autoantibodies. Spontaneous clinically significant bleeding is rare unless the platelet count falls to less than 30 x 109/L. The diagnosis of ITP is one of exclusion. Once spurious and other causes have been excluded, and provided the rest of the blood count and film is normal, a bone marrow examination is not required to make the diagnosis in patients under 60; older than this, due to the increased risk of myelodysplasia, bone marrow examination is advisable. less prominent and renal impairment more marked in HUS. A diagnosis of TTP/HUS should be considered in all patients with unexplained thrombocytopenia, and is suggested by prominent red cell fragmentation on the peripheral film, and features of haemolysis such as a raised LD. The coagulation screen is usually normal, as opposed to patients with DIC. Conditions associated with TTP/HUS include malignancy, pregnancy, drugs (ticlopidine, cyclosporin, gemcitabine), auto-immune disorders, and infectious diarrhoea, although it is common for no cause to be identified. The degree of thrombocytopenia is often moderate to severe. If TTP/HUS is suspected, urgent referral to a specialist centre is required. ISOLATED THROMBOCYTOPENIA Although the above causes of thrombocytopenia may predominantly manifest as thrombocytopenia, finding a low platelet count in isolation is more likely to be due to a number of other conditions: • inherited thrombocytopenia • immune mediated thrombocytopenia – idiopathic thrombocytopenic purpura (ITP) – drug mediated immune thrombocytopenia • thrombocytopenia related to microangiopathic haemolysis • disseminated intravascular coagulation (DIC) • myelodysplasia. Inherited thrombocytopenia This most commonly presents in infancy, however diagnosis may be delayed until adult years. Pointers to an inherited cause include family history, the lack of a previously documented normal platelet, and often abnormal peripheral blood film morphology including giant platelets (Mediterranean macrothrombocytopenia, Bernard Soulier-Syndrome, May Hegglin syndrome) or abnormal inclusions in other cells (May-Hegglin syndrome). This again emphasises the importance of film examination in the diagnosis. IMVS Newsletter 68 Summer 2008 HIT should be considered with recent exposure to heparin Drug induced causes of immune thrombocytopenia should be carefully considered in all patients with thrombocytopenia. Common candidates include quinine, sulphonamides, IIb/IIIa antagonists and heparin. Specific tests can be performed for quinine and heparin related antibodies. The diagnosis of heparin induced thrombocytopenia (HIT) is important, due to the high rate of often severe thrombotic complications in the absence of alternative anticoagulant therapy. Specific laboratory testing for HIT should be considered in all patients with thrombocytopenia and recent exposure to heparin (normally 5 – 14 days after first exposure). MAHA The spectrum of diseases associated with microangiopathic haemolytic anaemia (MAHA), ranging from thrombotic thrombocytopenia purpura (TTP) to the haemolytic uraemic syndrome (HUS), are important causes of thrombocytopenia to recognise early. TTP is characterised by the clinical features of thrombocytopenia, fragmentary haemolytic anaemia, neurological features and often renal impairment. Neurological features are DIC Disseminated intravascular coagulation is a syndrome characterised by initial widespread activation of the coagulation system, leading to secondary consumption of coagulation factors and platelets and a resulting coagulopathy. Thrombocytopenia in the setting of conditions known to be associated with DIC, such as sepsis, massive trauma, malignancy and obstetric disasters should lead to consideration of this as the cause. While red cell fragmentation can also be seen on the peripheral blood film in patients with DIC, it is normally less marked than in TTP/HUS, and the coagulation screen is almost always abnormal with a prolonged PT, APTT and significantly elevated D-dimer levels. Treatment of DIC is of the primary cause, along with supportive use of blood products as clinically indicated. Further assistance The IMVS on-call haematologist can help to guide the diagnostic process and determine both the need for and urgency of specialist referral. ▲










© Copyright 2026