
Minireview Acupuncture for Chronic Nonbacterial Prostatitis/Chronic Pelvic Pain Syndrome: A
Journal of Andrology, Vol. 33, No. 1, January/February 2012
Copyright E American Society of Andrology
Acupuncture for Chronic
Nonbacterial Prostatitis/Chronic
Pelvic Pain Syndrome: A
Systematic Review
Minireview
PAUL POSADZKI,* JUNHUA ZHANG,{ MYEONG SOO LEE,*{ AND EDZARD ERNST*
From the *Department of Complementary Medicine, Peninsula Medical School, Universities of Exeter and Plymouth,
Exeter, United Kingdom; the Evidence-based Medicine Center, Tianjin University of Traditional Chinese Medicine,
Tianjin, PR China; and the `Brain Disease Research Center, Korea Institute of Oriental Medicine, Daejeon, South Korea.
ABSTRACT: The objective of this systematic review was to
assess the effectiveness of acupuncture as a treatment option for
chronic prostatitis/chronic pelvic pain syndrome. Eight databases
were searched from their inception to October 2010. Randomized
clinical trials (RCT) were considered if they tested acupuncture
against any control intervention or no therapy in humans with
chronic prostatitis/chronic pelvic pain syndrome. The selection of
studies, data extraction, and validation were performed independently by 2 reviewers. The methodologic quality of all included
RCTs was assessed using the Jadad scale. Studies of
stimulation of acupoints other than by needles were excluded.
Nine RCTs met the inclusion criteria. They all suggested that
acupuncture is effective as a range of control interventions. Their
methodologic quality was variable; most were associated with
major flaws. Only one RCT had a Jadad score of more than 3.
The evidence that acupuncture is effective for chronic prostatitis/
chronic pelvic pain syndrome is encouraging but, because of
several caveats, not conclusive. Therefore, more rigorous studies
seem warranted.
Key words: Chronic abacterial prostatitis, effectiveness, complementary and alternative medicine.
J Androl 2012;33:15–21
C
affected with CP/CPPSs; however, the therapeutic
effects of acupuncture for this condition remain
uncertain (Capodice et al, 2005). Some studies suggested
neuropathic mechanism of action involved in CP/CPPS
(Chen and Nickel, 2003), but this is not supported by
sound evidence.
Wang and Han (2008) published a systematic review
and meta-analysis of acupuncture for CP. However, this
publication is burdened with a high risk of bias due to
ambiguous inclusion criteria and lack of appropriately
defined interventions, comprehensive search strategy, or
quality appraisal. Significant heterogeneity of the trials
included in meta-analysis was neither explained nor
accounted for. Specifically, Wang and Han (2008) only
included 3 of the 9 randomized clinical trials (RCT) we
managed to locate. Moreover, the authors failed to
critically evaluate the primary studies that they reviewed.
Also, they included such disparate interventions as
moxibustion (in 7 of 13 studies) or pricking needling
and bloodletting (in one study). Therefore, a more
rigorous systematic review is required in order to
determine the best evidence on acupuncture for CP/CPPS.
The aim of this systematic review is to summarize and
critically evaluate the RCTs testing the effectiveness of
acupuncture in treatment of CP/CPPS.
hronic prostatitis/chronic pelvic pain syndrome
(CP/CPPS) is a clinical entity defined as urologic
pain or discomfort in the pelvic region, associated with
urinary symptoms and/or sexual dysfunction and lasting
for at least 3 of the previous 6 months (Anothaisintawee
et al, 2011). The syndrome can affect 10%–15% of the
male population and results in nearly 2 million
outpatient visits each year (Murphy et al, 2009). Collins
et al (2000) concluded that CP/CPPS is difficult to
diagnose, and the routine use of antibiotics and alphablockers to treat chronic abacterial prostatitis is not
supported by sound evidence.
Acupuncture is a traditional Chinese method of
medical treatment involving the insertion of fine,
single-use, sterile needles in acupoints according to a
system of channels and meridians that was developed by
early practitioners of traditional Chinese medicine more
than 2000 years ago (Capodice et al, 2005). Acupuncture
is a ‘‘natural’’ therapy, attractive to many patients
Correspondence to: Paul Posadzki, Complementary Medicine,
Peninsula Medical School, Universities of Exeter and Plymouth,
Veysey Building, Salmon Pool Line, Exeter EX2 4SG, United
Kingdom (e-mail: [email protected]).
Received for publication February 1, 2011; accepted for publication
March 17, 2011.
DOI: 10.2164/jandrol.111.013235
15
16
Journal of Andrology
N
January February 2012
Table 1. Quality assessment of the included studies
Author (year)
Random Sequence
Generation
Appropriate
Randomization
Blinding of
Participants or
Personnel
Blinding of
Outcome
Assessors
He et al (2004)
He and Xu (2007)
Hu et al (2005)
Huang et al (2005)
Jin and Ji (2008)
Lee et al (2008)
Li and Wang (2006)
Wang (1997)
Zhang (2009)
1
1
1
1
1
1
1
1
1
1
1
0
0
0
1
0
0
1
0
0
0
0
0
1
0
0
0
0
0
0
0
0
0
0
0
0
Materials and Methods
Literature searches were performed to identify RCTs of
acupuncture for CP/CPPS. The following databases
were used: Cochrane Central Register of Controlled
Trials, MEDLINE, EMBASE, CINAHL, AMED,
PsycINFO, Chinese Journal Full-Text Database, and
Weipu Scientific Journal Database (from their respective inceptions to October 2010) using the following
search terms: acupuncture, prostatitis, chronic nonbacterial prostatitis, chronic abacterial prostatitis, chronic
pelvic pain syndrome, and prostatodynia to identify all
relevant RCTs on the subject. The reference lists of the
initially identified papers were scanned for further
relevant literature. No language barriers were imposed.
All retrieved data, including uncontrolled trials, case
studies, and preclinical and observational studies were
reviewed for safety information. However, only RCTs
testing acupuncture in adults with CP/CPPS were
included. Studies were excluded if they were uncontrolled (eg, Chen and Nickel, 2003; Honjo et al, 2004) or
used different a method of stimulation of acupoints (eg,
warm needling moxibustion; Yu and Kang, 2005;
Zhong-Xin, 2009) or electroacupuncture (Li, 2005; Lee
and Lee, 2009). Two independent reviewers validated
data using a predefined standardized form and assessed
the methodologic quality using the 5-point Jadad scale
(Jadad et al, 1996). Any differences were resolved by
discussion.
For the purpose of this review, CP/CPPS was defined
as urologic pain or discomfort in the pelvic region,
associated with urinary symptoms and/or sexual dysfunction and lasting for at least 3 of the previous
6 months (Anothaisintawee et al, 2011).
Results
The search strategy generated a total of 128 references,
of which 61 were considered to be potentially relevant.
We did not locate any unpublished trials. A total of 27
clinical trials were retrieved for further evaluation, of
which 9, involving 890 patients, were eligible for
inclusion (Wang, 1997; He et al, 2004; Hu et al, 2005;
Withdrawals and
Dropouts
Sum (Jadad Score)
0
0
0
0
0
1
0
0
0
2
2
1
1
1
4
1
1
2
Huang et al, 2005; Li and Wang, 2006; He and Xu, 2007;
Jin and Ji, 2008; Lee et al, 2008; Zhang, 2009). Eight
RCTs originated from China, (Wang, 1997; He et al,
2004; Hu et al, 2005; Huang et al, 2005; Li and Wang,
2006; He and Xu, 2007; Jin and Ji, 2008; Zhang, 2009)
and one from Malaysia (Lee et al, 2008).
The quality of studies ranged between 1 and 4 on the
Jadad scale. The study of Lee et al (2008) was well
designed in terms of randomization, partial blinding,
dropouts, and intention to treat analysis, and it used the
standardized National Institutes of Health Chronic
Prostatitis Symptom Index (NIH-CPSI) as a primary
outcome. We scored this study as 4.
All of the Chinese-language studies were described as
randomized; however, only 3 of them reported the
methods of sequence generation (ie, ‘‘table of random
number’’ [He et al, 2004; He and Xu, 2007] and softwareStatistical Analysis System [Zhang, 2009]). None of the
Chinese RCTs described allocation concealment or
blinding procedures. None of the trials described dropout
rate or intention-to-treat analyses. Overall, the methodologic quality of the Chinese trials was poor (Table 1).
Other sources of bias in these studies included lack of
standardized/validated primary outcome measures, power calculations, clearly defined inclusion and exclusion
criteria, and adequately performed statistical analyses.
Additional threats to internal validity included lack of
appropriate sampling method, wide confidence intervals,
incomplete outcome data, and selective outcome reporting. None of these trials used placebo or sham
acupuncture to control adequately for nonspecific effects.
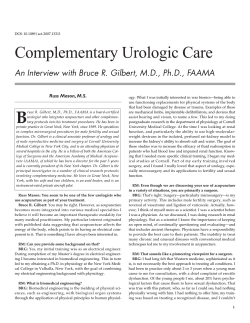
Eight Chinese-language studies used effective rate as
the primary outcome measure. According to the
different type of control treatments, the 8 articles were
classified into 4 subgroups (Figure). Needle acupuncture
treatments seem more effective than Pule’an pian (He et
al, 2004; He and Xu, 2007; Zhang, 2009), conventional
drugs for prostatic hyperplasia (Hu et al, 2005; Li and
Wang, 2006), antibiotics (Huang et al, 2005), or herbal
medicines (Wang, 1997; Jin and Ji, 2008).
Posadzki et al
N
Acupuncture for Prostatitis
17
Figure. Forest plots—effect of acupuncture for chronic nonbacterial prostatitis/chronic pelvic pain syndrome. M-H indicates Mantel-Haenszel.
Discussion
In their article, Wang and Han (2008) concluded that
‘‘acupuncture therapy exhibited a definite effect in the
treatment of chronic prostatitis.’’ Our evaluation
suggests that these conclusions are not supported by
the best available evidence. The review by Wang and
Han was wide open to bias. Therefore, our aim was to
provide a rigorous evaluation of the available RCT
data.
The 9 trials that met our eligibility criteria suggested
that acupuncture is effective for chronic CP/CPPS
(Wang, 1997; He et al, 2004; Hu et al, 2005; Huang et
al, 2005; Li and Wang, 2006; He and Xu, 2007; Jin and
Ji, 2008; Lee et al, 2008; Zhang, 2009). Thus, to some
extent we arrive at conclusions similar to those by Wang
and Han (2008). The important difference, however, is
that our results are based on higher quality and quantity
of the data.
Treatment groups received needle acupuncture
(Wang, 1997; He et al, 2004; Hu et al, 2005; Huang et
al, 2005; Li and Wang, 2006; He and Xu, 2007; Jin and
Ji, 2008; Lee et al, 2008; Zhang, 2009), whereas control
Table 2. Details of the acupuncture intervention
Author (Year)
He and Xu (2007)
He et al (2004)
Hu et al (2005)
Huang et al (2005)
Jin and Ji (2008)
Li and Wang (2006)
Lee et al (2008)
Wang (1997)
Zhang (2009)
Acupuncture Points Used (Direct Quote Where Appropriate)
1. Sanyin points; 2. Sanyin points plus Yinsan points, retaining needle for 30 min, 1 time per d, 30 treatments (36 d)
Sanyin points (points at perineum, named by the author) and other acupoints, retaining needle for 30 min, 1 time per d,
30 treatments (36 d)
CV3-to-CV2, BL32-to-BL34; BL54-to-BL35, retaining needle for 20 min, 1 time per d for 30 d
CV6, CV4, CV3, BL54, BL23, BL28, BL22, ST28, SP9, SP6, KI3, retaining needle for 20–30 min, 1 time per d. Total
treatment duration: 2–4 wk. (Not uniform for all patients)
BL54 to ST28. Other acupoints were selected individually according to the principle of traditional Chinese medicine.
Retaining needle for 30 min, 1 time per d, duration 2 mo
CV1 and CV3. Other acupoints were selected individually according to the principle of traditional Chinese medicine.
Retaining needle for 30 min, 3 times per wk, total treatment duration 8 wk
CV1 inserted with a depth of 50 mm, CV4 with 60 mm, and SP6 and SP9 with 40 mm. Two weekly sessions for 10 wk,
30 min each session
CV1. Duration: 1 time per d, without retaining needle, 4 wk (1 d stopping per wk)
BL54-to-ST28, retaining needle, 30 min per treatment, tertian treating, duration 8 wk
Study
Design
CP/CPPS
CP and
prostatodynia
CP
CP
CP
CP
Condition
90 (51/39)
89 (44/45)
60 (30/30)
84 (42/42)
90 (48/42)
115 (T1 40/T2
45/ C 30)
90 (60/30)
Sample Size
(T/C)
T: 21–52
(mean, 35)
C: 19–55
(mean, 33)
T: 40.9
C: 42.8
T: 25–50
(mean, 37.5)
C: 24–51
(mean, 37.5)
20–49 (mean
age, 32.98)
18–65
T1: 22–76
T2: 18–72
C: 20–72
T: 19–76
C: 20–72
Mean Age of
Participants or
Age Range, y
Needle
acupuncture
Acupuncture
Needle
acupuncture
Needle
acupuncture
Needle
acupuncture
Needle
acupuncture
Needle
acupuncture
Treatment Group
(Regimen)
Primary
Outcome
Measure
NIH-CPSI
Adverse Effects
No information
No information
No information
No information
No information
Adverse effects occurred
in 13 participants, 8
(18.1%) in the
acupuncture group (6
hematomas and 2 with
pain at needling sites),
and 5 (11.1%) in the
sham group (1
hematoma, 3 with pain
at needling sites, and
1 with acute urinary
retention)
Pharmacotherapy 1. Effective rate No adverse effects
(terazosin
(in %)a
occurred in the
hydrochloride) 2. WBCb
treatment group; 2
3. The amount
cases of postural
of lecithin
hypotension occurred
lipophore in
in drug group
prostatic fluid
Sham
acupuncture
Sitz bath in
Effective rate
decoction of
(in %)a
herbal medicine
Pharmacotherapy Effective rate
(ofloxacin)
(in %)a
Pharmacotherapy Effective rate
(Cernilton
(in %)a
Prostat)
Pharmacotherapy Effective rate
(Pule’an pian)
(in %)a
Pharmacotherapy Effective rate
(Pule’an pian)
(in %)a
Control
Intervention
N
Open-label RCT CP
with 2
parallel
groups
To find effective Open-label RCT
remedies for
with 2
CP
parallel
groups
To find effective Open-label RCT
remedies for
with 3
CP
parallel
groups
To evaluate the Open-label RCT
effectiveness
with 2
of pointparallel
through-point
groups
acupuncture
for CP.
To evaluate the Open-label RCT
efficacy of
with 2
acupuncture
parallel
for CP
groups
To evaluate the Open-label RCT
efficacy of
with 2
acupuncture
parallel
for CP
groups
To compare
Patient-blind
‘‘the efficacy
RCT with 2
of acupuncture groups
to sham
acupuncture
for CP/CPPS’’
Objective
(Quote)
Journal of Andrology
Li and Wang To evaluate the
(2006)
efficacy of
acupuncture
for CP.
Lee et al
(2008)
Jin and Ji
(2008)
Huang et al
(2005)
Hu et al
(2005)
He and Xu
(2007)
He et al
(2004)
Author
(Year)
Table 3. Randomized clinical trials of acupuncture chronic prostatitis/chronic pelvic pain syndrome (CP/CPPS)
18
January February 2012
b
Effective rate is the percentage of patients with improved status of disease divided by the sample size of each group and multiplied by 100.
The amount of white blood cells (WBC) in prostatic fluid after treatment.
19
a
Abbreviations: C, control group; NIH-CPSI, National Institutes of Health Chronic Prostatitis Symptom Index; RCT, randomized clinical trial; T, treatment group; T1, acupuncture at Sanyin
points; T2, acupuncture at Sanyin plus Yinsan points.
No information
Elongatedneedle
acupuncture
T: 47.1
C: 45.1
104 (54/50)
Pharmacotherapy Effective rate
(Pule’an pian)
(in %)a
Two cases of hematuria
cased by acupuncture
and recovered 1 d
later.
Decoction of
Effective rate
Chinese herbal
(in %)a
medicine
T: 17–45 (mean, Needle
29.5);
acupuncture
C: 16–40
(mean, 28.5)
Adverse Effects
Condition
Acupuncture for Prostatitis
168 (84/84)
Primary
Outcome
Measure
Control
Intervention
Treatment Group
(Regimen)
Mean Age of
Participants or
Age Range, y
Sample Size
(T/C)
Study
Design
Objective
(Quote)
Author
(Year)
Table 3. Continued
N
Wang (1997) ‘‘To evaluae the Open-label RCT CP
efficacy of
with 2
needle
parallel
acupuncture
groups
for CP’’
Zhang
‘‘To evaluate the Open-label RCT CP
(2009)
effectiveness
with 2
of pointparallel
through-point
groups
acupuncture
for chronic
prostatitis’’
Posadzki et al
groups received pharmacotherapy (He et al, 2004; Hu et
al, 2005; Li and Wang, 2006; He and Xu, 2007; Zhang,
2009; Zhong-Xin, 2009), herbal medicine (Wang, 1997;
Jin and Ji, 2008), or sham acupuncture (Lee et al, 2008).
In order to lead to any firm conclusion regarding the
effectiveness of acupuncture superiority, RCTs need to
control for placebo effects. Only one study made serious
attempts to do this (Lee et al, 2008). Equivalence trials
can only lead to interpretable results if they compare the
experimental treatment against an intervention of
proven efficacy. Unfortunately, all of the Chinese
studies failed to do so, and therefore no firm conclusions
can be drawn from such studies.
The exact psychologic or other mechanisms of action
of acupuncture remain unclear (Lewith and Kenyon,
1984; Kavoussi, 2009).Whether certain patient groups
respond to acupuncture differently than others and
whether suggestibility is an essential factor for any
response remain unclear. The possible mechanism of
action may therefore include the patients’ expectations—a part of the placebo effect (Dawn and Lee,
2004; Verbeek et al, 2004). Patients have explicit
expectations on diagnosis, instructions, interpersonal
management, or course of treatment (Verbeek et al,
2004), and they expect that these expectations will be
met (Dawn and Lee, 2004). Recently, it was shown that
the communication style of the acupuncturist is a more
important determinant of the response than the question
of whether a patient receives real or sham acupuncture
(Suarez-Almazor et al, 2010).
All of the Chinese language RCTs included effective
rate as a primary outcome measure, and one of those
trials also used white blood cell level and the amount of
lipophore in prostatic fluid (Li and Wang, 2006). Only
one RCT used standardized NIH-CPSI (Lee et al, 2008).
There was also a wide variety of acupuncture points
used in the treatment groups (Table 2). The duration of
therapeutic intervention ranged from 2 to 4 weeks
(Huang et al, 2005), 1 month, (Wang, 1997; He et al,
2004; Hu et al, 2005; He and Xu, 2007), and 2 months
(Li and Wang, 2006; Lee et al, 2008; Jin and Ji, 2008;
Zhang, 2009). Given such variability in terms of length
and diversity of the therapeutic intervention, it is
difficult to draw any definite conclusions.
The quality of the included studies was predominantly
poor. Eight (88.8%) scored less than 2 on the Jadad scale
(Wang, 1997; He et al, 2004; Hu et al, 2005; Huang et al,
2005; Li and Wang, 2006; He and Xu, 2007; Jin and Ji,
2008; Zhang, 2009). Only one RCT scored 4 on the
Jadad scale (Lee et al, 2008). Five Chinese RCTs
(55.5%) failed to describe sequence generation sufficiently (Wang, 1997; Hu et al, 2005; Huang et al, 2005;
Li and Wang, 2006; Jin and Ji, 2008). None of the
Chinese RCTs described allocation concealment or
20
blinding procedures. None of the Chinese trials described dropout rates or included an intention-to-treat
analysis or a power calculation.
Adverse events (AE) were not reported in most trials
(Table 3; He et al, 2004; Hu et al, 2005; Huang et al,
2005; He and Xu, 2007; Jin and Ji, 2008; Zhang, 2009).
Three RCTs reported the incidence of AEs (Wang, 1997;
Li and Wang, 2006; Lee et al, 2008). STRICTA
guidelines, and indeed medical ethics, require the
reporting of AEs. Underreporting distorts the overall
picture of what we know about the safety of acupuncture.
Our review has several limitations. First and foremost, the potential incompleteness of the reviewed
evidence may have limited the validity of the results.
Second, publication and location biases, which are wellknown phenomena, may also influence the results of this
systematic review. Third, the total number of trials
included in our review and analysis, and the total sample
size are too small to allow definitive judgments. Fourth,
although all of these studies were considered to have
relatively homogenous CP/CPPS populations, statistical
pooling was not possible because of lack of reporting of
sufficient raw data. Another possible source of bias is
the fact that almost all (88.8%) of the included trials
were carried out in China, where they have appeared to
produce almost no negative studies (Vickers et al, 1998).
However, this review has several strengths, including the
comprehensive search strategy, the inclusion of only the
highest-quality trial design, and use of suggested
methods for systematic reviews of interventions for
CP/CPPS.
Future studies of acupuncture in CP/CPPS should be
of adequate sample size based on power calculations;
provide sufficient details on needling, frequency, duration
of therapeutic regimen, and practitioners’ background;
use validated outcome measures; control for nonspecific
effects; and minimize other threats to internal and
external validity. Reporting of these studies should be
such that results can be independently replicated.
In conclusion, the evidence that acupuncture treats
CP/CPPS is encouraging. However, the quantity and
quality of the existing evidence prevent firm conclusions.
References
Anothaisintawee T, Attia J, Nickel JC, Thammakraisorn S, Numthavaj P, McEvoy M, Thakkinstian A. Management of chronic
prostatitis/chronic pelvic pain syndrome a systematic review and
network meta-analysis. JAMA. 2011;305:78–86.
Capodice JL, Bemis DL, Buttyan R, Kaplan SA, Katz AE.
Complementary and alternative medicine for chronic prostatitis/
chronic pelvic pain syndrome. Evid Based Complementary Altern
Med. 2005;2:495–501.
Journal of Andrology
N
January February 2012
Chen R, Nickel JC. Acupuncture ameliorates symptoms in men with
chronic prostatitis/chronic pelvic pain syndrome. Urology. 2003;
61:1156–1159.
Collins MM, MacDonald R, Wilt TJ. Diagnosis and treatment of
chronic abacterial prostatitis: a systematic review. Ann Intern Med.
2000;133:367–381.
Dawn AG, Lee PP. Patient expectations for medical and surgical care:
a review of the literature and applications to ophthalmology. Surv
Ophthalmol. 2004;49:513–524.
He TY, Xu YL. Clinical observation on acupuncture at ‘‘sanyin
points’’ plus ‘‘yinsan points’’ for treatment of chronic prostatitis.
World J Clin Acupunct Moxibust. 2007;23:12–13.
He TY, Zhao YD, Luo CL. Clinical observation on acupuncture at
‘‘sanyin points’’ for treatment of chronic prostatitis. Chin Acupunct
Moxibust. 2004;24:697–698.
Honjo H, Kamoi K, Naya Y, Ukimura O, Kojima M, Kitakoji H,
Miki T. Effects of acupuncture for chronic pelvic pain syndrome
with intrapelvic venous congestion: preliminary results. Int J Urol.
2004;11:607–612.
Hu BC, Wang S, Zhou ZK, Cai YY. Point-through-point acupuncture
for the treatment of chronic non-bacterial prostatitis. Cap Med.
2005;18:47.
Huang YJ, Fan XH, Du M. Acupuncture for the treatment of
chronic prostatitis in 42 cases. J Acupunct Moxibust. 2005;21:
8–9.
Jadad AR, Moore RA, Carrol D, Jenkinson C, Reynolds DJ,
Gavaghan DJ, McQuay HJ. Assessing the quality of reports of
randomized clinical trials: is blinding necessary? Controlled Clin
Trials. 1996;17:1–12.
Jin XH, Ji LX. Clinical study on acupuncture for the treatment of
chronic non-bacterial prostatitis and prostatodynia. Chin Naturopath. 2008;5:9.
Kavoussi B. The untold story of acupuncture. Focus Altern Complementary Therapies. 2009;14:276–285.
Lee SH, Lee BC. Electroacupuncture relieves pain in men with chronic
prostatitis/chronic pelvic pain syndrome: three-arm randomized
trial. Urology. 2009;73:1036–1041.
Lee SW, Liong ML, Yuen KH, Leong WS, Chee C, Cheah PY,
Choong WP, Wu Y, Khan N, Choong WL, Yap HW, Krieger JN.
Acupuncture versus sham acupuncture for chronic prostatitis/
chronic pelvic pain. Am J Med. 2008;121:79.e1–e7.
Lewith G, Kenyon J. Physiological and psychological explanations for
the mechanism of acupuncture as a treatment for chronic pain. Soc
Sci Med. 1984;19:1367–1378.
Li C, Wang HS. Clinical study of acupuncture for the treatment
of chronic prostatitis. Beijing J Tradit Chin Med. 2006;25:680–
681.
Li ZG. Electro-acupunture for the treatment of chronic prostatitis in
60 cases with observation on the valure of Zn, Cu, SOD. Chin J
Tradit Med Sci Technol. 2005;12:401.
Murphy AB, Macejko A, Taylor A, Nadler RB. Chronic prostatitis
management strategies. Drugs. 2009;69:71–84.
Suarez-Almazor ME, Looney C, Liu Y, Cox V, Pietz K, Marcus DM,
Street RL Jr. A randomized controlled trial of acupuncture for
osteoarthritis of the knee: effects of patient-provider communication. Arthritis Care Res. 2010;62:1229–1236.
Verbeek J, Sengers MJ, Riemens L, Haafkens J. Patient expectations
of treatment for back pain: a systematic review of qualitative and
quantitative studies. Spine. 2004;29:2309–2318.
Vickers A, Goyal N, Harland R, Rees R. Do certain countries produce
only positive results? A systematic review of controlled trials.
Controlled Clin Trials. 1998;19:159–166.
Wang C, Han R. Acupuncture for chronic prostatitis: a meta-analysis.
Natl J Androl. 2008;14:853–856.
Posadzki et al
N
Acupuncture for Prostatitis
Wang RS. Clinical observation of acupuncture in Huiyin points for the
treatment of chronic prostatitis in 84 cases. Chin Acupunct
Moxibust. 1997;7:397–398.
Yu Y, Kang J. Clinical studies on treatment of chronic prostatitis with
acupuncture and mild moxibustion. J Tradit Chin Med. 2005;25:
177–181.
21
Zhang XJ. Observations on the efficacy of point-through-point
acupuncture with elongated-needle in treating chronic prostatitis.
Shanghai J Acupunct Moxibust. 2009;28:589–590.
Zhong-Xin C. Observation of therapeutic effect on chronic nonbacterial prostatitis treated with warm needling moxibustion.
World J Acupunct Moxibust. 2009;19:19–29.











© Copyright 2026