
Hematuria Urology Didactics 5 -
Urology Didactics 5-25-04 Chris Vincent – Hematuria Rebecca Sellers – Kidney Stones SFM – Online – Prostate CA (Microscopic Asymptomatic) Hematuria Chris Vincent Tuesday, May 25, 2004 Illustrative Case (NEJM) An otherwise healthy 48-year-old woman is found to have microscopic hematuria (5 red cells per high-power field) on a urinalysis performed by a life insurance company. No other laboratory abnormalities are identified; the serum creatinine concentration is 0.8 mg/dL. The woman reports no symptoms and is a nonsmoker. Her blood pressure is 118/74, and findings on physical exam are normal. How should she be evaluated? Cohen RA, Brown RS. Microscopic hematuria. N Engl J Med June 5, 2003;348:2330-8 Hematuria Outline Definition Prevalence Causes Workup Follow up Hematuria Outline Definition Prevalence Causes Workup Follow up Hematuria Definition Urine dipstick detects 1-2/HPF so very sensitive but not specific (myoglobinuria & hemoglobinuria cause + results) Microscopy essential if dipstick + “Normal” varies by author: 1-10/HPF Most accept 0-3/HPF as nml, >3 abnml Hematuria Definition “Red” urine not always due to blood Drugs, Prophyria, foods cause red urine Substances Affecting Urine Color Artificial food coloring Beets Berries Chloroquine (Aralen) Furazolidone (Furoxone) Hydroxychloroquine (Plaquenil) Nitrofurantoin (Furadantin) Phenazopyridine (Pyridium) Phenolphthalein Rifampin (Rifadin) Hematuria Definition Hematuria Outline Definition Prevalence Causes Workup Follow up Hematuria Prevalence Varies by study/population group/age 0.2% to 20% cited Usually accepted: 2% Hematuria Outline Definition Prevalence Causes Workup Follow up Hematuria Causes By Age – <40-50 vs. >40-50 By Origin – Glomerular vs. Non-glomerular By Duration – Transient vs. Persistent (Some) Hematuria Causes by Age All <40-50 > 40-50 Stones Thin Basement Membrane Transitional cell CA Infection Trauma Renal Cell CA IgA Nephropathy Medullary sponge Mild Focal GN Polycystic kidney Bladder CA Exercise Hematuria Causes by Origin Hematuria Causes by Age & Origin Hematuria Causes by Age & Origin Hematuria Causes by Age & Origin Hematuria Causes by Age & Duration Hematuria Outline Definition Prevalence Causes Workup Follow up Hematuria Workup Recommendations & guidelines vary Depends on age, gender & “risk factors” Availability of tests Availability/opinion of referral specialists Hematuria Workup Basic workup before referral – H&P! – Lab – Imaging Referral – Nephrology – Urology Hematuria Workup Basic workup before referral – H&P! – Lab – Imaging Referral – Nephrology – Urology Hematuria Workup – H&P Dysuria, fever? – UTI, pylo, urethritis Recent URI? – PSGN, IgA nephropathy Unilateral pain – Stones, clot BPH Sx (men) Menstrual Hx (women) Medications (see next slide) – Warfarin: not a cause per se, but indicates possible underlying condition Hematuria Workup – H&P Mechanism Drugs Interstitial nephritis Captopril (Capoten), Capoten), Cephalosporins, Cephalosporins, Chlorothiazide ), Ciprofloxacin (Cipro ), Furosemide (Lasix), (Diuril), Lasix), Diuril (Cipro), NSAIDs, NSAIDs, Olsalazine (Dipentum), Dipentum), Omeprazole (Prilosec), Prilosec), Penicillins, Penicillins, Rifampin (Rifadin), Rifadin), Silver sulfadiazine (Silvadene ), Trimethoprim(Silvadene), Trimethoprimsulfamethoxazole (Bactrim, Bactrim, Septra) Septra) Papillary necrosis Acetylsalicylic acid (aspirin), NSAIDs Hemorrhagic cystitis Cyclophosphamide (Cytoxan), Cytoxan), Ifosfamide (Ifex), Ifex), Mitotane (Lysodren) ) Lysodren Urolithiasis Carbonic anhydrase inhibitors, Dichlorphenamide (Daranide), Daranide), Indinavir (Crixivan), Crixivan), Mirtazapine (Remeron), Remeron), Ritonavir (Norvir), Norvir), Triamterene (Dyrenium) Dyrenium) Hematuria Workup – H&P Fam Hx – Sickle cell, hereditary nephritis, polycystic kidney “Risk Factors” for CA – Age > 40-50, cigarette smoking, occupational exposure to certain chemicals (leather, dye, and rubber or tire manufacturing), heavy phenacetin use, past Rx w/ high doses of cyclophosphamide, ingestion of aristolochic acid (found in some herbal weight-loss preparations), and schistosomiasis Hematuria Workup – H&P PE – V.S. – BP!!! Temp Pallor? (anemia) Back (CVAT) Abd Mass? Pelvic/rectal (examine urethra, prostate/uterus) Hematuria Workup Basic workup before referral – H&P! – Lab – Imaging Referral – Nephrology – Urology Hematuria Workup - Lab UA! CBC Chemistries Other Urine tests – 24 hour – cytology UA Hematuria Workup - Lab – Gross visual inspection – Dipstick for amount of blood, protein, nitrites, leukocytes – Micro - look for casts & abnormal cells RBC Casts – glomerular origin Crenated RBC’s – concentrated urine – no significance Acanthocytes – 98% - 100% specific for glomerular origin but only 52% to 73% sensitive – RBC’s may have hemolyzed if urine dilute Hematuria Workup - Lab Hematuria Workup - Lab Hematuria Workup - Lab RBC Casts Hematuria Workup - Lab Crenated RBC’s Hematuria Workup - Lab Acanthocytes Hematuria Workup - Lab CBC – Look for anemia, abnormal red cell morphology, leukocytosis Chemistries – BUN, Creatinine Other Urine tests – 24 hour for protein – Cytology – 3 serial AM voids – Sens = 72 + 6%, Spec = 98 + 2 % Hematuria Workup Basic workup before referral – H&P! – Lab – Imaging Referral – Nephrology – Urology Hematuria Workup - Imaging IVP – Old “Gold Standard” – Good visualization of collecting system & ureters – May miss bladder lesions, expensive, dye Rxn US – Safer than IVP, good visualization of kidneys – May miss small (<3 cm) lesions CT – Most sensitive and specific, new “Gold Standard” – Expensive, dye Rxn Hematuria Workup – Imaging Risk Factors for Contrast Urography Dehydration, renal insufficiency, cardiac decompensation Diabetes with azotemia History of dye allergy or previous reaction to contrast media Asthma, hay fever Seafood allergy? Other allergies, including allergic reactions to antibiotics Hematuria Workup Hematuria Workup Basic workup before referral – H&P! – Lab – Imaging Referral – Nephrology – Urology Hematuria Workup – Referral Nephrology suspected referral if glomerular source – Hx, UA, imaging studies support – + FHx, Sx, HTN – Proteinuria > 300 (some say 1000) mg/24hr – RBC casts, acanthocytes – High or rising creatinine – ?Need for renal Bx? – may not matter if isolated glomerular hematuria as management may be the same regardless of cause Hematuria Workup Basic workup before referral – H&P! – Lab – Imaging Referral – Nephrology – Urology Hematuria Workup – Referral Urology referral if lower GU source suspected – Hx, UA, imaging studies support – No Sx, proteinuria, abnormal cells on UA, nml creatinine – Tumor on imaging – ?Need for cystoscopy? – usually indicated if nml basic workup AND risk factors for bladder CA Hematuria Workup “Risk Factors” for CA age > 40-50 cigarette smoking occupational exposure to certain chemicals (leather, dye, and rubber or tire manufacturing) heavy phenacetin use past Rx w/ high doses of cyclophosphamide ingestion of aristolochic acid (found in some herbal weight-loss preparations) schistosomiasis Hematuria Workup – Referral Hematuria Workup – Summary Hematuria Workup – Summary Hematuria Workup – Summary Hematuria Outline Definition Prevalence Causes Workup Follow up Hematuria Follow up Referral for definitive Rx if cause found If negative workup, follow up depends on risk factors, presence of other Sx, age In pts w/ a neg initial evaluation of asymptomatic microscopic hematuria, consider repeating urinalysis, voided urine cytology and BP at 6, 12, 24 and 36 months Hematuria Follow up Although cytology may not be a sensitive marker for detecting low-grade transitional cell carcinoma, it detects most high-grade tumors and carcinomas in situ, particularly if the test is repeated Such high-grade lesions are the most likely to benefit from early detection Hematuria Follow up Immediate urologic reevaluation, with consideration of cystoscopy, cytology or repeat imaging, should be performed if any of the following occur: – gross hematuria – abnormal urinary cytology – irritative voiding symptoms in the absence of infection If none of these occurs within three years, the patient does not require further urologic monitoring Hematuria Follow up - Summary Hematuria Outline Definition Prevalence Causes Workup Follow up References (following this slide) Cohen RA, Brown RS. Microscopic hematuria. N Engl J Med June 5, 2003;348:2330-8 2. Grossfeld et al Asymptomatic Microscopic Hematuria in Adults: Summary of the AUA Best Practice Policy Recommendations. Am Fam Physician 2001;63:1145-54 3. UpToDate® 'Evaluation of hematuria in adults' 1. The new england journal of medicine clinical practice Microscopic Hematuria Robert A. Cohen, M.D., and Robert S. Brown, M.D. This Journal feature begins with a case vignette highlighting a common clinical problem. Evidence supporting various strategies is then presented, followed by a review of formal guidelines, when they exist. The article ends with the authors’ clinical recommendations. An otherwise healthy 48-year-old woman is found to have microscopic hematuria (5 red cells per high-power field) on a urinalysis performed by a life insurance company. No other laboratory abnormalities are identified; the serum creatinine concentration is 0.8 mg per deciliter (70.7 µmol per liter). The woman reports no symptoms and is a nonsmoker. Her blood pressure is 118/74 mm Hg, and the findings on physical examination are normal. How should she be evaluated? the clinical problem From the Division of Nephrology, Department of Medicine, Beth Israel Deaconess Medical Center and Harvard Medical School, Boston. Address reprint requests to Dr. Cohen at the Division of Nephrology, Beth Israel Deaconess Medical Center, 330 Brookline Ave., DA517, Boston, MA 02115, or at [email protected]. Microscopic hematuria without proteinuria is often an incidental finding. Since bleeding may arise from any site along the urinary tract, it has a broad differential diagnosis, possibly reflecting an entirely benign cause, such as vigorous exercise just before urine collection, or a malignant, potentially lethal disease, such as bladder or renal cancer. Even with a thorough investigation, the source of the microscopic hematuria frequently is not found. We focus here on the evaluation of microscopic hematuria in persons older than 18 years of age. N Engl J Med 2003;348:2330-8. Copyright © 2003 Massachusetts Medical Society. definitions We define microscopic hematuria as 2 or more red cells per high-power field on microscopical examination.1,2 Definitions vary, however, from 1 to more than 10 red cells per high-power field.2 Dipstick testing for heme may be too sensitive, detecting hemoglobin from 1 or 2 red cells per high-power field. Such testing also lacks specificity, since the presence of myoglobin or hemoglobin may result in a positive test when the urine contains no red cells. Therefore, if the dipstick test is positive, the presence of red cells should be confirmed by microscopical examination. There have been only a few population-based studies addressing the prevalence of microscopic hematuria, and their results vary according to the age and sex distribution of the populations studied, whether the diagnosis was based on the dipstick test alone or that test coupled with microscopical evaluation, and the number of screening tests performed per patient. In six studies, the prevalence ranged from 0.18 percent to 16.1 percent.3,4 Only two studies report a higher prevalence among women than among men.2 Although some studies suggest that there may be an increased prevalence among older persons,2 others show no difference according to age.5 Microscopic hematuria also may be transient. In a study of male soldiers who underwent yearly examinations of urinary sediment over a 12-year period, the cumulative incidence was 39 percent with microscopic hematuria on one examination and 16 percent with microscopic hematuria on two or more examinations.6 In another study, transient microscopic hematuria was noted in about 13 percent of postmenopausal women.5 Transient microscopic hematuria may be caused by vigorous exercise before urine collection, by sexual intercourse, by mild trauma, or by menstrual contamination. There are 2330 n engl j med 348;23 www.nejm.org june 5, 2003 Downloaded from www.nejm.org at UNIVERSITY OF WASHINGTON on May 24, 2004. Copyright © 2003 Massachusetts Medical Society. All rights reserved. clinical practice no data on differences between patients with transient microscopic hematuria and those with persistent microscopic hematuria with regard to the likelihood of underlying urinary tract disease. clinical relevance dye, and rubber or tire manufacturing), heavy phenacetin use, past treatment with high doses of cyclophosphamide, and ingestion of aristolochic acid found in some herbal weight-loss preparations.11-13 strategies and evidence Causes of isolated microscopic hematuria (without proteinuria) are listed in Table 1 and can be classified as either glomerular or nonglomerular in origin. Because renal biopsies are not typically part of the evaluation of microscopic hematuria, it is difficult to estimate the percentage of cases that are clearly attributable to glomerular bleeding. In a study involving 157 men in whom renal biopsy was performed when no cause of microscopic hematuria had been identified by other tests, a glomerular source was identified in 16 percent of the patients. IgA nephropathy, a form of glomerulonephritis defined histologically by glomerular IgA deposits, accounted for the majority of cases with a glomerular source.7 In a series of 165 patients, renal biopsies were performed after renal imaging and cystoscopy. No abnormalities were noted on renal biopsy in 87 patients. Of the remaining 78 patients, 49 had IgA nephropathy.8 Although IgA nephropathy is probably the most common glomerular cause of hematuria,9 some data suggest that thin basement membrane disease, an inherited glomerular disorder defined histologically by diffuse thinning of the glomerular basement membranes, may be as frequent a cause of isolated glomerular microscopic hematuria.10 Hereditary nephritis is a less common glomerular cause. Nonglomerular sources of microhematuria involving the kidney and the upper urinary tract include neoplasm, nephrolithiasis, cystic disease (including polycystic kidney disease and medullary sponge kidney), papillary necrosis, and metabolic defects such as hypercalciuria or hyperuricosuria. The causes involving the lower urinary tract include disorders of the bladder, urethra, and prostate. Urologic cancers (mainly of the bladder and prostate) are estimated to account for about 5 percent of cases of microscopic hematuria, although estimates vary widely according to whether the study is referral-based (higher percentages) or population-based (lower percentages).2 The risk of bladder cancer increases significantly with age, particularly after 65 years of age.11 Risk factors for transitional-cell cancer of the bladder or urinary tract include cigarette smoking, occupational exposure to chemicals used in certain industries (leather, n engl j med 348;23 The first steps in evaluating microscopic hematuria should be to obtain a pertinent history and perform a physical examination. It should be noted that anticoagulant therapy alone does not cause hematuria, except in the case of a marked overdose of warfarin.14 The urine should be evaluated for bacteriuria and pyuria. If either is present, a urine culture should be ordered. Serum creatinine should be measured to evaluate the patient for renal insufficiency. If proteinuria is detected on dipstick testing, the ratio of the urinary protein concentration to the urinary creatinine concentration, in milligrams per deciliter, should be determined, or a 24-hour urine collection should be obtained for measurement of total protein excretion. Clinically significant proteinuria (a ratio of urinary protein to urinary creatinine of more than 0.3 or 24-hour urinary protein excretion of more than 300 mg) points to the kidney as a source of microscopic hematuria. urinalysis The single most important test in the evaluation of hematuria is the microscopical analysis of urine, because it often distinguishes glomerular from nonglomerular bleeding (Fig. 1). If the findings indicate a glomerular site of bleeding, no urologic evaluation is necessary. Documentation of renal insufficiency or proteinuria warrants referral to a nephrologist for evaluation and possible renal biopsy; referral should be prompt if a second measurement of serum creatinine is abnormal or higher than the first. However, renal biopsy in a patient with microscopic hematuria unaccompanied by clinically significant proteinuria or renal insufficiency is not supported by the limited data that are available. In a study involving 75 patients with isolated microscopic hematuria who underwent renal biopsy, 36 percent had thin basement membrane disease, and 23 percent had IgA nephropathy — findings that made little difference in their care.20 imaging of the upper urinary tract If a glomerular source is ruled out or considered unlikely on the basis of the clinical presentation, the upper urinary tract should be imaged. The goal is to www.nejm.org june 5, 2003 Downloaded from www.nejm.org at UNIVERSITY OF WASHINGTON on May 24, 2004. Copyright © 2003 Massachusetts Medical Society. All rights reserved. 2331 The new england journal of medicine Table 1. Causes of Isolated Microscopic Hematuria.* Origin <50 Yr of Age Glomerular ≥50 Yr of Age IgA nephropathy (increased incidence in Asians) IgA nephropathy Thin basement membrane disease (benign familial hematuria) Hereditary nephritis (Alport’s syndrome) Hereditary nephritis (Alport’s syndrome) Mild focal glomerulonephritis of other causes Mild focal glomerulonephritis of other causes Nonglomerular Upper urinary tract causes Nephrolithiasis Nephrolithiasis Pyelonephritis Renal-cell cancer Polycystic kidney disease Polycystic kidney disease Medullary sponge kidney Pyelonephritis Hypercalciuria, hyperuricosuria, or both, without documented stones Renal-pelvis or ureteral transitional-cell cancer Renal trauma Papillary necrosis Papillary necrosis Renal infarction Ureteral stricture and hydronephrosis Ureteral stricture and hydronephrosis Sickle cell trait or disease in blacks Renal tuberculosis Renal infarction or arteriovenous malformation Renal tuberculosis in endemic areas or in patients with HIV infection Lower urinary tract causes Cystitis, prostatitis, and urethritis Cystitis, prostatitis, and urethritis Benign bladder and ureteral polyps and tumors Bladder cancer Bladder cancer Prostate cancer Prostate cancer Benign bladder and ureteral polyps and tumors Urethral and meatal strictures Schistosoma haematobium in North Africans Uncertain Exercise hematuria Exercise hematuria “Benign hematuria” (unexplained microscopic hematuria) Over-anticoagulation (usually with warfarin) Over-anticoagulation (usually with warfarin) Factitious hematuria (usually presents with gross hematuria) * Disorders causing microhematuria are presented roughly in order of descending frequency of presentation, according to available data. HIV denotes human immunodeficiency virus. detect any neoplasms, including renal-cell carcinoma and the less prevalent transitional-cell carcinomas of the renal pelvis and ureters, urolithiasis, cystic disease, and obstructive lesions. Excretory urography has been used routinely to examine the upper urinary tract in most studies of microscopic 2332 n engl j med 348;23 hematuria.2 Ultrasonography is safer, does not involve exposure to intravenous radiographic contrast medium, is appropriate for use during pregnancy, and is less expensive.21 Ultrasonography, however, may be limited in its detection of solid tumors that are less than 3 cm in diameter.22 In a study in which www.nejm.org june 5 , 2003 Downloaded from www.nejm.org at UNIVERSITY OF WASHINGTON on May 24, 2004. Copyright © 2003 Massachusetts Medical Society. All rights reserved. clinical practice enhanced computed tomography (CT) was used as the standard, the sensitivity and specificity of ultrasonography for the detection of renal parenchymal masses between 2 and 3 cm in diameter were 82 percent and 91 percent, respectively. In the same study, the sensitivity and specificity of excretory urography were 52 percent and 82 percent, respectively.23 Since excretory urography may miss small renal masses and sometimes cannot differentiate solid from cystic masses, a follow-up study with the use of ultrasonography, CT, or magnetic resonance imaging is often ordered. To our knowledge, no studies have specifically compared the effectiveness of these various imaging techniques in the evaluation of microscopic hematuria. A CT scan without the use of a contrast agent is Figure 1. Findings in Urinary Sediment. In Panel A (¬ 440), urinary sediment shows a red-cell cast and red cells. Red-cell casts indicate the presence of glomerular bleeding, a finding that is very specific but rather insensitive. If no red-cell casts are found, urinary red-cell morphology should be examined. The small, dysmorphic red cell (arrow) suggests a glomerular source,15 and the uniform, biconcave disk shape of normal red cells (arrowhead) suggests nonglomerular bleeding. Some have noted that dysmorphic or abnormally shaped red cells are not reliable enough as a means for distinguishing a glomerular source of bleeding from a nonglomerular source, particularly if mixtures of dysmorphic and normal-appearing red cells are seen.16,17 (Photomicrograph courtesy of the late Dr. Richard Nesson.) In Panel B (¬ 440), urinary sediment shows normal red cells (arrow) and crenated red-cell forms with spicules (arrowhead). Crenated red cells form in concentrated urine and are not diagnostically relevant. A more specific finding with bleeding of glomerular origin may be the presence of a particular form of abnormal red cells in the urine — acanthocytes,18,19 doughnut-like cells with membrane blebs attached (Panel C, ¬ 440, arrowhead). With meaningful acanthocyturia defined as the presence of acanthocytes accounting for more than 5 percent of urinary red cells, the sensitivity of phase microscopy for detecting glomerular hematuria was 52 percent in one large series in which glomerulonephritis was documented with renal biopsy and 73 percent in another series, and the specificity for detecting a glomerular source was 98 percent and 100 percent, respectively, in the two series.18,19 The sensitivity and specificity of light microscopy for identifying acanthocytes have not been reported; since most laboratories do not routinely identify acanthocytes, this test should ideally be performed by an experienced laboratory technologist alerted to look for acanthocytes or by a nephrologist. n engl j med 348;23 appropriate as the first test for patients with suspected stone disease. In one series of patients with renal colic who underwent unenhanced helical CT followed immediately by excretory urography, the sensitivity for the detection of ureteral stones was 100 percent with the former, as compared with 67 percent with the latter.24 When there is no clinical suspicion of stone disease, CT urography should be performed first without contrast medium and then with it, particularly in patients who might be at increased risk for kidney cancer. Although CT is more expensive than excretory urography or ultrasonography, studies involving the latter techniques are often followed by additional imaging (to confirm that cysts are benign or to reevaluate questionable or negative studies) and thus cannot be considered A B C www.nejm.org june 5, 2003 Downloaded from www.nejm.org at UNIVERSITY OF WASHINGTON on May 24, 2004. Copyright © 2003 Massachusetts Medical Society. All rights reserved. 2333 The new england journal cost-saving in general. If CT is unavailable or prohibitively expensive, excretory urography, ultrasonography, or the combination of the two is a reasonable alternative. If a mass suspected to be malignant is identified, the patient should be referred to a urologist. If polycystic kidney disease is found, the patient should be referred to a nephrologist. evaluation of the lower urinary tract The source of microscopic hematuria remains obscure in about 70 percent of cases after imaging of the upper urinary tract and examination of urine for evidence of glomerular hematuria. In these cases, it may be necessary to evaluate the lower urinary tract, with particular attention to possible bladder cancer. Cystoscopy is appropriate if risk factors for bladder cancer are present. This procedure is also warranted in older men with asymptomatic microscopic hematuria, but the data are inconclusive regarding the age at which to recommend cystoscopy. In one community-based study,25 1340 men 50 years of age or older (mean age, 65 years) were tested for hematuria with urinary dipsticks daily for two weeks. Twenty-one percent had at least one episode of hematuria. Of these men, 192 underwent complete urologic evaluation. A total of 16 malignant lesions were identified: 9 bladder cancers, 1 renalcell carcinoma, and 6 prostate cancers. In another community-based study, 3152 men older than 60 years of age were screened for microscopic hematuria by urinary dipstick testing daily or weekly for 10 weeks. Twenty percent had hematuria on at least one dipstick test, and of the 319 men who underwent full urologic evaluation, 22 had cancer (bladder cancer in 17 and prostate cancer in 5).26 Thirteen of the 17 men with bladder cancer had a history of cigarette smoking. In these two studies, the positive predictive value of dipstick testing for the detection of bladder cancer was 4.7 percent and 5.3 percent, respectively. In a referral-based study involving 100 men younger than 40 years of age with microscopic hematuria, no bladder cancers were identified by cystoscopy.27 CT studies with the use of radiographic contrast medium may reduce the need for cystoscopy. In a recent series, the sensitivity of this technique was 100 percent and the specificity was 98 percent for the detection of neoplasms of the bladder.28 Available data provide less support for cystoscopy in women with asymptomatic microscopic hematuria than in men. No cases of bladder cancer were found in one prospective, referral-based study 2334 n engl j med 348;23 of medicine involving 177 women (mean age, 57.2 years) with asymptomatic microscopic hematuria who underwent cystoscopy.29 In another referral-based study, involving 1034 adults (75 percent of whom were female), only two cases of bladder cancer were identified in women with microscopic hematuria (one 54 years old and the other 70 years old).30 In contrast, in a referral-based study involving 484 women with microscopic hematuria, 12 cases of urologic cancer were identified in women between 60 and 89 years of age, and 5 cases were found in women between 40 and 59 years of age. The specific types of cancer and the number of diagnoses made with cystoscopy were unclear.31 cytologic studies of urine Cytologic analysis of voided urine is less sensitive (66 percent and 79 percent in two large series) than cystoscopy in the detection of bladder cancer32,33 but has high specificity (95 percent and 100 percent in the two series). The sensitivity is improved if specimens of urine from the first voiding in the morning on three consecutive days are obtained.34 The sensitivity is higher for the detection of highgrade bladder cancer and carcinoma in situ33 but lower for the detection of cancers of low histologic grade, and cytologic analysis is insensitive for the detection of renal-cell cancer. Cystoscopy itself had 87 percent sensitivity for the detection of bladder cancer in one large series and is especially limited for the diagnosis of carcinoma in situ.32 Urinary molecular markers for the noninvasive detection of bladder cancer are currently being evaluated but have not yet been validated.35 follow-up after negative evaluation A thorough evaluation of the urinary system may fail to identify a source of microscopic hematuria. In studies in which both imaging of the upper urinary tract and cystoscopy were performed in patients with microscopic hematuria, a source was not identified in 19 to 68 percent of the patients evaluated.29,31,36-39 Microscopy was not routinely part of the evaluation in these studies, suggesting that more glomerular causes of microscopic hematuria might be identified with this addition. Follow-up of patients with unexplained microscopic hematuria has been evaluated in two studies, both without a control group. In one, 191 patients with asymptomatic hematuria that remained unexplained after urologic evaluation with urinalysis, cytologic analysis of voided urine, excretory urog- www.nejm.org june 5 , 2003 Downloaded from www.nejm.org at UNIVERSITY OF WASHINGTON on May 24, 2004. Copyright © 2003 Massachusetts Medical Society. All rights reserved. clinical practice raphy, and cystoscopy subsequently underwent excretory urography and cystoscopy. No cancers were detected during follow-up, prompting the authors to suggest that no further studies are necessary unless symptoms develop.40 This suggestion was corroborated by similar recommendations in another prospective study.31 areas of uncertainty Currently, the data are inadequate to support clearcut recommendations regarding the evaluation and management of microscopic hematuria. Shortcomings of available studies include inconsistencies in definition, study design, selection criteria, and diagnostic-test techniques and procedures used.41 Data are lacking on outcomes in patients with microscopic hematuria who did not undergo formal evaluation and those in whom the finding remained unexplained despite evaluation. In addition, there have been no randomized trials comparing the outcomes associated with different strategies. guidelines The U.S. Preventive Services Task Force and the Canadian Task Force on the Periodic Health Examination do not recommend routine screening of urine for microscopic hematuria.11 Regarding bladder cancer, they cite the low predictive value of a positive screening test even in a high-risk population of older adults. They also cite the absence of proof that early detection improves the prognosis in the small number of patients found to have urinary tract cancer.11 The American Urological Association has issued guidelines for the evaluation of microscopic hematuria in adults (http://www.aafp.org/afp/20010315/ 1145.html). According to these guidelines, after microscopical examination of the urine, testing for proteinuria, and measurement of serum creatinine, a full urologic workup should be performed, including radiologic imaging of the upper urinary tract, cytologic analysis of urine, and cystoscopy (recommended for all persons with asymptomatic microscopic hematuria who are older than 40 years).42 conclusions and recommendations When asymptomatic microscopic hematuria is detected, as in the patient described in the vignette, the n engl j med 348;23 urinalysis should be repeated a few days later before any workup is initiated, especially if the patient has had vigorous exercise, menstruation, trauma to the urinary tract, or sexual activity just before the collection. Our recommended approach after a second urinalysis is summarized in Figure 2. If microscopic hematuria is absent on repeated testing, we do not recommend further evaluation, unless the patient has risk factors for bladder cancer or transitional-cell cancer of the urinary tract, such as cigarette smoking or exposure to toxins. If repeated urinalysis confirms the presence of microscopic hematuria, we recommend microscopical analysis for evidence of a glomerular source, such as acanthocyturia or red-cell casts. Whether or not such a source is found, if microscopic hematuria is accompanied by proteinuria or renal insufficiency, the patient should be referred to a nephrologist for evaluation. If isolated glomerular microscopic hematuria is identified, we recommend follow-up by a primary care physician, initially at six months and then annually, to check for the development of proteinuria or renal insufficiency (although there are no data supporting a specific interval between follow-up visits). We would not perform a renal biopsy in a patient with isolated glomerular microscopic hematuria, since the limited data available do not suggest that identification of the specific disease makes any difference in management or outcome. If examination of urine does not suggest a glomerular source and the patient is not pregnant, helical CT urography should be performed, first without and then with radiographic contrast medium, primarily for the detection of occult stone disease or a mass (in the upper urinary tract or possibly in the bladder). An examination without contrast medium would be appropriate if stone disease was suspected clinically. CT is highly sensitive for the detection of disease in the upper urinary tract; we do not recommend excretory urography unless CT is unavailable or deemed too expensive. Ultrasonography can be performed in place of CT (and is advised for patients with renal failure, pregnancy, or hypersensitivity to contrast medium), with the understanding that further imaging may be necessary. If imaging is unrevealing, we recommend obtaining specimens of urine from the first voiding in the morning on three consecutive days for cytologic analysis in persons older than 40 years of age, but the insensitivity of cytologic analysis for the detection of low-grade bladder cancer should www.nejm.org june 5, 2003 Downloaded from www.nejm.org at UNIVERSITY OF WASHINGTON on May 24, 2004. Copyright © 2003 Massachusetts Medical Society. All rights reserved. 2335 The new england journal of medicine Urine dipstick test positive for microscopic heme Repeated urine dipstick testing (several days later) ¡ Workup ends (unless there are risk factors for bladder cancer) ¡ Evaluation for hemoglobinuria or myoglobinuria + Microscopical examination of urine Acanthocytes or red-cell casts Isomorphic red cells Glomerular hematuria Nonglomerular hematuria Isolated microscopic hematuria Proteinuria or renal insufficiency Helical CT + Referral based on lesion + Cystoscopy ¡ Periodic medical follow-up (for onset of proteinuria or renal insufficiency) Nephrology referral Cytologic analysis of urine (3 serial first morning specimens) ¡ ≥50 Yr of age or risk factors for bladder cancer <50 Yr of age without risk factors for bladder cancer Cystoscopy Workup ends Figure 2. Evaluation of Microscopic Hematuria. If hematuria is determined to be nonglomerular in origin, computed tomography (CT) should be performed without contrast medium if a stone is suspected to be present or first without and then with contrast medium if no stone is suspected. Ultrasonography should be performed instead of CT in pregnant patients and those with hypersensitivity to contrast medium. Risk factors for bladder cancer include cigarette smoking, occupational exposure to chemicals used in certain industries (leather, dye, and rubber or tire manufacturing), heavy phenacetin use, past treatment with high doses of cyclophosphamide, and ingestion of aristolochic acid found in some herbal weight-loss preparations. Plus signs indicate positive findings, and minus signs negative findings. 2336 n engl j med 348;23 www.nejm.org june 5 , 2003 Downloaded from www.nejm.org at UNIVERSITY OF WASHINGTON on May 24, 2004. Copyright © 2003 Massachusetts Medical Society. All rights reserved. clinical practice be recognized. Cystoscopy should be performed if cytologic analysis of voided urine has identified neoplastic cells or if the patient has risk factors for bladder cancer. In the absence of these factors, the question of the age at which cystoscopy should routinely be performed to evaluate patients of either sex who have microscopic hematuria remains controversial. At variance with the American Urological Association, we would not routinely recommend cystoscopy for all persons older than 40 years of age, since we believe that such a recommendation would lead to unnecessary testing, with the attendant expense and potential risks associated with this invasive procedure; we would, however, recommend yearly follow-up with urinalysis. Recognizing the trend toward a higher incidence of bladder cancer with advancing age, we would advise men and women older than 50 years of age who have persistent microscopic hematuria to undergo cystoscopy. Cystoscopy is also recommended if gross hematuria develops, because this finding is associated with a higher risk of urologic cancer than is microscopic hematuria.2,31 We are indebted to Isaac Stillman, M.D., for his help in producing the photomicrographs; to Susan Cohen and Sven Paulen, M.D., for assistance in the translation of a Swedish manuscript; and to Thomasina Shavers for assistance in the preparation of the manuscript. references 1. Mariani AJ, Mariani MC, Macchioni C, Stams UK, Hariharan A, Moriera A. The significance of adult hematuria: 1,000 hematuria evaluations including a risk-benefit and cost-effectiveness analysis. J Urol 1989; 141:350-5. 2. Sutton JM. Evaluation of hematuria in adults. JAMA 1990;263:2475-80. 3. Woolhandler S, Pels RJ, Bor DH, Himmelstein DU, Lawrence RS. Dipstick urinalysis screening of asymptomatic adults for urinary tract disorders. JAMA 1989;262: 1214-9. 4. Hiatt RA, Ordonez JD. Dipstick urinalysis screening, asymptomatic microhematuria, and subsequent urological cancers in a population-based sample. Cancer Epidemiol Biomarkers Prev 1994;3:439-43. [Erratum, Cancer Epidemiol Biomarkers Prev 1994;3:523.] 5. Mohr DN, Offord KP, Owen RA, Melton LJ III. Asymptomatic microhematuria and urologic disease: a population-based study. JAMA 1986;256:224-9. 6. Froom P, Ribak J, Benbassat J. Significance of microhaematuria in young adults. Br Med J (Clin Res Ed) 1984;288:20-2. 7. Sparwasser C, Cimniak HU, Treiber U, Pust RA. Significance of the evaluation of asymptomatic microscopic haematuria in young men. Br J Urol 1994;74:723-9. 8. Topham PS, Harper SJ, Furness PN, Harris KPG, Walls J, Feehally J. Glomerular disease as a cause of isolated microscopic haematuria. Q J Med 1994;87:329-35. 9. D’Amico G, Imbasciati E, Barbiano Di Belgioioso G, et al. Idiopathic IgA mesangial nephropathy: clinical and histological study of 374 patients. Medicine (Baltimore) 1985; 64:49-60. 10. Tiebosch ATMG, Frederik PM, van Breda Vriesman PJC, et al. Thin-basementmembrane nephropathy in adults with persistent hematuria. N Engl J Med 1989;320: 14-8. 11. Preventive Services Task Force. Guide to clinical preventive services: report of the U.S. Preventive Services Task Force. 2nd ed. Baltimore: Williams & Wilkins, 1996. 12. Piper JM, Tonascia J, Matanoski GM. Heavy phenacetin use and bladder cancer in women aged 20 to 49 years. N Engl J Med 1985;313:292-5. 13. Talar-Williams C, Hijazi YM, Walther MM, et al. Cyclophosphamide-induced cystitis and bladder cancer in patients with Wegener granulomatosis. Ann Intern Med 1996; 124:477-84. 14. Van Savage JG, Fried FA. Anticoagulant associated hematuria: a prospective study. J Urol 1995;153:1594-6. 15. Birch DF, Fairley KF. Haematuria: glomerular or non-glomerular? Lancet 1979;2: 845-6. 16. Pollock C, Lui P-L, Gyory AZ, et al. Dysmorphism of urinary red blood cells — value in diagnosis. Kidney Int 1989;36:1045-9. 17. Offringa M, Benbassat J. The value of urinary red cell shape in the diagnosis of glomerular and post-glomerular haematuria: a meta-analysis. Postgrad Med J 1992;68: 648-54. 18. Kohler H, Wandel E, Brunck B. Acanthocyturia — a characteristic marker for glomerular bleeding. Kidney Int 1991;40: 115-20. 19. Kitamoto Y, Tomita M, Akamine M, et al. Differentiation of hematuria using a uniquely shaped red cell. Nephron 1993;64:32-6. 20. McGregor DO, Lynn KL, Bailey RR, Robson RA, Gardner J. Clinical audit of the use of renal biopsy in the management of isolated microscopic hematuria. Clin Nephrol 1998;49:345-8. 21. Corwin HL, Silverstein MD. The diagnosis of neoplasia in patients with asymptomatic microscopic hematuria: a decision analysis. J Urol 1988;139:1002-6. [Erratum, J Urol 1988;140:1558.] 22. Jamis-Dow CA, Choyke PL, Jennings SB, Linehan WM, Thakore KN, Walther MM. Small (≤3-cm) renal masses: detection with CT versus US and pathologic correlation. Radiology 1996;198:785-8. 23. Warshauer DM, McCarthy SM, Street L, et al. Detection of renal masses: sensitivities and specificities of excretory urography/linear tomography, US, and CT. Radiology 1988;169:363-5. 24. Sourtzis S, Thibeau JF, Damry N, Raslan n engl j med 348;23 www.nejm.org A, Vandendris M, Bellemans M. Radiologic investigation of renal colic: unenhanced helical CT compared with excretory urography. AJR Am J Roentgenol 1999;172:1491-4. 25. Messing EM, Young TB, Hunt VB, et al. Home screening for hematuria: results of a multiclinic study. J Urol 1992;148:289-92. 26. Britton PJ, Dowell AC, Whelan P, Harris CM. A community study of bladder cancer screening by the detection of occult urinary bleeding. J Urol 1992;148:788-90. 27. Jones DJ, Langstaff RJ, Holt SD, Morgans BT. The value of cystourethroscopy in the investigation of microscopic haematuria in adult males under 40 years: a prospective study of 100 patients. Br J Urol 1988;62:541-5. 28. Lang EK, Macchia RJ, Thomas R, et al. Computerized tomography tailored for the assessment of microscopic hematuria. J Urol 2002;167:547-54. 29. Bard RH. The significance of asymptomatic microhematuria in women and its economic implications: a ten-year study. Arch Intern Med 1988;148:2629-32. 30. Murakami S, Igarashi T, Hara S, Shimazaki J. Strategies for asymptomatic microscopic hematuria: a prospective study of 1,034 patients. J Urol 1990;144:99-101. 31. Khadra MH, Pickard RS, Charlton M, Powell PH, Neal DE. A prospective analysis of 1,930 patients with hematuria to evaluate current diagnostic practice. J Urol 2000;163: 524-7. 32. Rife CC, Farrow GM, Utz DC. Urine cytology of transitional cell neoplasms. Urol Clin North Am 1979;6:599-612. 33. Koss LG, Deitch D, Ramanathan R, Sherman AB. Diagnostic value of cytology of voided urine. Acta Cytol 1985;29:810-6. 34. Badalament RA, Hermansen DK, Kimmel M, et al. The sensitivity of bladder wash flow cytometry, bladder wash cytology, and voided cytology in the detection of bladder carcinoma. Cancer 1987;60:1423-7. 35. Stein JP, Grossfeld GD, Ginsberg DA, et al. Prognostic markers in bladder cancer: a contemporary review of the literature. J Urol 1998;160:645-59. 36. Greene LF, O’Shaughnessy EJ Jr, Hen- june 5, 2003 Downloaded from www.nejm.org at UNIVERSITY OF WASHINGTON on May 24, 2004. Copyright © 2003 Massachusetts Medical Society. All rights reserved. 2337 clinical practice dricks ED. Study of five hundred patients with asymptomatic microhematuria. JAMA 1956;161:610-3. 37. Carson CC III, Segura JW, Greene LF. Clinical importance of microhematuria. JAMA 1979;241:149-50. 38. Davides KC, King LM, Jacobs D. Management of microscopic hematuria: twentyfour-year experience with 150 cases in a community hospital. Urology 1986;28:453-5. 39. Ritchie CD, Bevan EA, Collier SJ. Impor- 2338 tance of occult haematuria found at screening. Br Med J (Clin Res Ed) 1986;292:681-3. 40. Howard RS, Golin AL. Long-term followup of asymptomatic microhematuria. J Urol 1991;145:335-6. 41. Köhler C, Varenhorst E. Mikroskopisk hematuri hos vuxna — ett diagnostiskt dilemma: vetenskapliga riktlinjer för handläggning saknas visar litteraturgenomgång. Lakartidningen 1999;96:4911-6. 42. Grossfeld GD, Litwin MS, Wolf JS Jr, et n engl j med 348;23 www.nejm.org al. Evaluation of asymptomatic microscopic hematuria in adults: the American Urological Association best practice policy. II. Patient evaluation, cytology, voided markers, imaging, cytoscopy, nephrology evaluation, and follow-up. Urology 2001;57:604-10. Copyright © 2003 Massachusetts Medical Society. june 5 , 2003 Downloaded from www.nejm.org at UNIVERSITY OF WASHINGTON on May 24, 2004. Copyright © 2003 Massachusetts Medical Society. All rights reserved. Asymptomatic Microscopic Hematuria in Adults: Summary of the AUA Best Practice Policy Recommendations GARY D. GROSSFELD, M.D., University of California, San Francisco, School of Medicine, San Francisco, California J. STUART WOLF, JR., M.D., University of Michigan Medical School, Ann Arbor, Michigan MARK S. LITWIN, M.D., M.P.H., University of California, Los Angeles, Schools of Medicine and Public Health, Los Angeles, California HEDVIG HRICAK, M.D., PH.D., Memorial Sloan-Kettering Cancer Center, New York, New York CATHRYN L. SHULER, M.D., Kaiser Permanente, Portland, Oregon DAVID C. AGERTER, M.D., Mayo Clinic, Rochester, Minnesota PETER R. CARROLL, M.D., University of California, San Francisco, School of Medicine, San Francisco, California The American Urological Association (AUA) convened the Best Practice Policy Panel on Asymptomatic Microscopic Hematuria to formulate policy statements and recommendations for the evaluation of asymptomatic microhematuria in adults. The recommended definition of microscopic hematuria is three or more red blood cells per high-power microscopic field in urinary sediment from two of three properly collected urinalysis specimens. This definition accounts for some degree of hematuria in normal patients, as well as the intermittent nature of hematuria in patients with urologic malignancies. Asymptomatic microscopic hematuria has causes ranging from minor findings that do not require treatment to highly significant, life-threatening lesions. Therefore, the AUA recommends that an appropriate renal or urologic evaluation be performed in all patients with asymptomatic microscopic hematuria who are at risk for urologic disease or primary renal disease. At this time, there is no consensus on when to test for microscopic hematuria in the primary care setting, and screening is not addressed in this report. However, the AUA report suggests that the patient’s history and physical examination should help the physician decide whether testing is appropriate. (Am Fam Physician 2001;63:1145-54.) B lood in the urine (hematuria) can originate from any site along the urinary tract and, whether gross or microscopic, may be a sign of serious underlying disease, including malignancy. The literature agrees that gross hematuria warrants a thorough diagnostic evaluation.1 By contrast, microscopic hematuria is an incidental finding, and whether physicians should test for hematuria in asymptomatic patients remains at issue. No major organization currently recommends screening for microscopic hematuria in asymptomatic adults, even though bladder cancer is the most commonly detected malignancy in such patients.2 The American Urological Association (AUA) convened a Best Practice Policy Panel to formulate recommendations for the evaluation of patients with asymptomatic microhematuria. The panel does not offer recommendations regarding routine screening for microscopic hematuria. The recommendations are based on extensive review of the literature and the panel MARCH 15, 2001 / VOLUME 63, NUMBER 6 www.aafp.org/afp members’ expert opinions. In addition to urologists, the multispecialty panel included a family physician, a nephrologist and a radiologist. Funding in support of panel activities was provided by the AUA. A summary of the recommendations is presented in this article; the full text will be published in Urology.3,4 The initial determination of microscopic hematuria should be based on microscopic examination of urinary sediment from a freshly voided, clean-catch, midstream urine specimen. Hematuria can be measured quantitatively by any of the following: (1) determination of the number of red blood cells per milliliter of urine excreted (chamber count), (2) direct examination of the centrifuged urinary sediment (sediment count) or (3) indirect examination of the urine by dipstick (the simplest way to detect microscopic hematuria). Given the limited specificity of the dipstick method (65 percent to 99 percent for two to five red blood cells per high-power microscopic field), however, the initial finding of microscopic AMERICAN FAMILY PHYSICIAN 1145 The recommended definition of microscopic hematuria is three or more red blood cells per high-power field on microscopic evaluation of urinary sediment from two of three properly collected urinalysis specimens. hematuria by the dipstick method should be confirmed by microscopic evaluation of urinary sediment.5-8 The recommended definition of microscopic hematuria is three or more red blood cells per high-power field on microscopic evaluation of urinary sediment from two of three properly collected urinalysis specimens. To account for intermittent positive tests for hematuria in patients with urologic malignancies,6,9 one group of investigators10 proposed that patients with more than three red blood cells per high-power field from two of three properly collected urine specimens should be considered to have microhematuria and, thus, should be evaluated appropriately. However, before a decision is made to defer evaluation in patients with one or two red blood cells per high-power field, risk factors for significant disease should be taken into consideration (Table 1).4 High-risk patients should be considered for full urologic evaluation after one properly performed urinalysis documenting the presence of at least three red blood cells per high-power field. The prevalence of asymptomatic microscopic hematuria varies from 0.19 percent to as high as 21 percent. In five population-based studies, the prevalence of asymptomatic microscopic hematuria varied from 0.19 percent to 16.1 percent.7 Differences in the age and sex of the populations screened, the amount of follow-up and the number of screening studies per patient account for this range. In older men, who are at a higher risk for significant urologic disease, the prevalence of asymptomatic microscopic hematuria was as high as 21 percent.6,9,11-13 1146 AMERICAN FAMILY PHYSICIAN www.aafp.org/afp TABLE 1 Risk Factors for Significant Disease in Patients with Microscopic Hematuria Smoking history Occupational exposure to chemicals or dyes (benzenes or aromatic amines) History of gross hematuria Age > 40 years History of urologic disorder or disease History of irritative voiding symptoms History of urinary tract infection Analgesic abuse History of pelvic irradiation Adapted with permission from Grossfeld GD, Wolf JS, Litwin MS, Hricak H, Shuler CL, Agerter DC, Carroll P. Evaluation of asymptomatic microscopic hematuria in adults: the American Urological Association best practice policy recommendations. Part II: patient evaluation, cytology, voided markers, imaging, cystoscopy, nephrology evaluation, and followup. Urology 2001;57(4) (In press). Patients with asymptomatic microscopic hematuria who are at risk for urologic disease or primary renal disease should undergo an appropriate evaluation. In patients at low risk for disease, some components of the evaluation may be deferred. Asymptomatic microscopic hematuria has many causes, ranging from minor incidental findings that do not require treatment to highly significant lesions that are immediately life-threatening. Therefore, hematuria has been classified into four categories: lifethreatening; significant, requiring treatment; significant, requiring observation; and insignificant1,10 (Table 2).1 Most studies in which patients with asymptomatic microscopic hematuria have undergone full urologic evaluation (often including repeat urinalysis, urine culture, upper urinary tract imaging, cystoscopy and urinary cytology) have included referral-based populations. A cause for asymptomatic microscopic VOLUME 63, NUMBER 6 / MARCH 15, 2001 Hematuria TABLE 2 Reported Causes of Asymptomatic Microscopic Hematuria The rightsholder did not grant rights to reproduce this item in electronic media. For the missing item, see the original print version of this publication. hematuria was determined in 32 percent to 100 percent of these patients.6,9-23 An algorithm for the initial evaluation of newly diagnosed asymptomatic microscopic hematuria is provided in Figure 1.4 An approach to the urologic evaluation of patients without conditions suggestive of primary renal disease is presented in Figure 2.4 The presence of significant proteinuria, red cell casts or renal insufficiency, or a predominance of dysmorphic red blood cells in the urine should prompt an evaluation for renal parenchymal disease or referral to a nephrologist. Significant proteinuria is defined as a total protein excretion of greater than 1,000 mg per 24 hours (1 g per day), or greater than 500 mg per 24 hours (0.5 g per day) if protein excretion is persistent or increasing or if other facMARCH 15, 2001 / VOLUME 63, NUMBER 6 tors suggest the presence of renal parenchymal disease. In the absence of massive bleeding, a total protein excretion in excess of 1,000 mg per 24 hours would be unlikely and should prompt a thorough evaluation or nephrology referral24 (Figure 2).4 Red cell casts are virtually pathognomonic for glomerular bleeding. Unfortunately, they are a relatively insensitive marker. Therefore, it is useful to examine the character of the red blood cells.25 Dysmorphic urinary red blood cells show variation in size and shape and usually have an irregular or distorted outline. Such red blood cells are generally glomerular in origin. In contrast, normal doughnutshaped red blood cells are generally due to lower urinary tract bleeding. Accurate determination of red blood cell morphology may require inverted phase contrast microscopy. www.aafp.org/afp AMERICAN FAMILY PHYSICIAN 1147 Initial Evaluation of Asymptomatic Microscopic Hematuria* Patient with newly diagnosed asymptomatic microscopic hematuria Exclude benign causes, including menstruation, vigorous exercise, sexual activity, viral illness, trauma and infection. If one or more of the following are present: Microscopic hematuria accompanied by significant proteinuria† Dysmorphic red blood cells or red cell casts Elevated serum creatinine level (based on normal reference ranges for men and women) Evaluation for primary renal disease If conditions suggestive of primary renal disease are not present (i.e., normal creatinine level, absence of proteinuria, absence of dysmorphic red blood cells or red cells casts), or if any of the following are present: Smoking history Occupational exposure to chemicals or dyes (benzenes or aromatic amines) History of gross hematuria Age > 40 years Previous urologic disorder or disease History of irritative voiding symptoms History of recurrent urinary tract infection despite appropriate use of antibiotics Urologic evaluation (see Figure 2) *—The recommended definition of microscopic hematuria is three or more red blood cells per high-power field on microscopic evaluation of two of three properly collected specimens. †—Proteinuria of 1+ or greater on dipstick urinalysis should prompt a 24-hour urine collection to quantitate the degree of proteinuria. A total protein excretion of > 1,000 mg per 24 hours (1 g per day) should prompt a thorough evaluation or nephrology referral. Such an evaluation should also be considered for lower levels of proteinuria (> 500 mg per 24 hours [0.5 g per day]), particularly if the protein excretion is increasing or persistent, or if there are other factors suggestive of renal parenchymal disease. FIGURE 1. Initial evaluation of newly diagnosed asymptomatic microscopic hematuria. Adapted with permission from Grossfeld GD, Wolf JS, Litwin MS, Hricak H, Shuler CL, Agerter DC, Carroll P. Evaluation of asymptomatic microscopic hematuria in adults: the American Urological Association best practice policy recommendations. Part II: patient evaluation, cytology, voided markers, imaging, cystoscopy, nephrology evaluation, and follow-up. Urology 2001;57(4) (In press). The percentage of dysmorphic red blood cells required to classify hematuria as glomerular in origin has not been adequately defined. In general, glomerular bleeding is associated with more than 80 percent dysmorphic red blood cells, and lower urinary tract bleeding is associated with more than 80 percent normal red blood cells.25,26 Percentages falling between these ranges are indeterminate and could represent bleeding from either source. 1148 AMERICAN FAMILY PHYSICIAN www.aafp.org/afp The initial evaluation of the urinary sediment generally identifies patients with parenchymal renal disease (Figure 1).4 Glomerular disease is most likely in this setting and may be associated with a variety of systemic diseases, including lupus erythematosus, vasculitis, malignancy and infections such as hepatitis and endocarditis. Glomerular diseases localized to the kidney include membranoproliferative glomerulonephritis, IgA nephropathy VOLUME 63, NUMBER 6 / MARCH 15, 2001 Hematuria Urologic Evaluation of Asymptomatic Microscopic Hematuria Patient without conditions suggestive of primary renal disease Low-risk patient: Age < 40 years No smoking history No history of chemical exposure No irritative voiding symptoms No history of gross hematuria No history of urologic disorder or disease High-risk patients Complete evaluation (upper tract imaging, cytology, cystoscopy) Upper tract imaging Cytology Cystoscopy Negative Positive, atypical or suspicious Negative Cystoscopy Negative Positive Positive Treat Treat Negative Urinalysis, blood pressure and cytology at 6, 12, 24 and 36 months Consider Negative for 3 years Persistent hematuria, hypertension, proteinuria, glomerular bleeding No further urologic monitoring Evaluate for primary renal disease. Positive Gross hematuria, abnormal cytology, irritative voiding symptoms without infection Treat Repeat complete evaluation. Glomerular bleeding or proteinuria Isolated hematuria Renal biopsy Biopsy controversial FIGURE 2. Urologic evaluation of asymptomatic microscopic hematuria. Adapted with permission from Grossfeld GD, Wolf JS, Litwin MS, Hricak H, Shuler CL, Agerter DC, Carroll P. Evaluation of asymptomatic microscopic hematuria in adults: the American Urological Association best practice policy recommendations. Part II: patient evaluation, cytology, voided markers, imaging, cystoscopy, nephrology evaluation, and follow-up. Urology 2001;57(4) (In press). MARCH 15, 2001 / VOLUME 63, NUMBER 6 www.aafp.org/afp AMERICAN FAMILY PHYSICIAN 1149 The presence of significant proteinuria, red cell casts or renal insufficiency or a predominance of dysmorphic red blood cells in the urine should prompt an evaluation for renal parenchymal disease. and crescentic glomerulonephritis. In addition, interstitial renal disease, such as druginduced interstitial disease or analgesic nephropathy, may be associated with hematuria. If systemic causes are not identified, renal biopsy is usually recommended. Patients with microscopic hematuria, a negative initial urologic evaluation and no evidence of glomerular bleeding are considered to have isolated hematuria. Although many such patients may have structural glomerular abnormalities, they appear to have low risk for progressive renal disease. Thus, the role of renal biopsy in this setting has not been defined. Nevertheless, because follow-up data are limited, these patients should be followed for the development of hypertension, renal insufficiency or proteinuria. In patients without risk factors for primary renal disease, a complete urologic evaluation should be performed. Complete urologic evaluation of microscopic hematuria includes a history and physical examination, laboratory analysis and radiologic imaging of the upper urinary tract followed by cystoscopic examination of the urinary bladder (Figure 2).4 In some instances, cytologic evaluation of exfoliated cells in the voided urine specimen may also be performed. If a careful history suggests a potential “benign” cause for microscopic hematuria (Figure 1),4 the patient should undergo repeat urinalysis 48 hours after cessation of the activity (i.e., menstruation, vigorous exercise, sexual activity or trauma).27 No additional evaluation is warranted if the hematuria has resolved. Patients with persistent hematuria require evaluation. 1150 AMERICAN FAMILY PHYSICIAN www.aafp.org/afp In women, urethral and vaginal examinations should be performed to exclude local causes of microscopic hematuria. A catheterized urinary specimen is indicated if a cleancatch specimen cannot be reliably obtained (i.e., because of vaginal contamination or obesity). In uncircumcised men, the foreskin should be retracted to expose the glans penis, if possible. If a phimosis is present, a catheterized urinary specimen may be required. The laboratory analysis begins with comprehensive examination of the urine and urinary sediment. The number of red blood cells per high-power field should be determined. In addition, the presence of dysmorphic red blood cells or red cell casts should be noted. The urine should also be tested for the presence and degree of proteinuria and for evidence of urinary tract infection. Patients with urinary tract infection should be treated appropriately, and urinalysis should be repeated six weeks after treatment.27 If the hematuria resolves with treatment, no additional evaluation is necessary. Serum creatinine should be measured. The remaining laboratory investigation should be guided by specific findings of the history, physical examination and urinalysis. Urothelial cancers, the target of a cytologic examination, are the most commonly detected malignancies in patients with microscopic hematuria. Voided urinary cytology is recommended in all patients who have risk factors for transitional cell carcinoma (Table 1).4 This test can be a useful adjunct to cystoscopic evaluation of the bladder, especially in the determination of carcinoma in situ. In patients with asymptomatic microscopic hematuria who do not have risk factors for transitional cell carcinoma, urinary cytology or cystoscopy may be used. If cytology is chosen and malignant or atypical/suspicious cells are identified, cystoscopy is required because the presence of hematuria is a significant risk factor for malignancy in such patients. VOLUME 63, NUMBER 6 / MARCH 15, 2001 Hematuria Several recently identified voided urinary markers have been examined for the early detection of bladder cancer.1 At this time, insufficient data are available to recommend their routine use in the evaluation of patients with microscopic hematuria. Further studies are warranted to determine the role of these markers in the diagnostic evaluation of such patients. Intravenous urography, ultrasonography and computed tomography are used to evaluate the urinary tract in patients with microscopic hematuria. Because of lack of impact data, evidence-based imaging guidelines cannot be formulated. In patients with microscopic hematuria, imaging can be used to detect renal cell carcinoma, transitional cell carcinoma in the pelvicaliceal system or ureter, urolithiasis and renal infection. Table 34 highlights imaging modalities used to evaluate the urinary tract.28-31 Intravenous urography (IVU) has traditionally been the modality of choice for imaging the urinary tract, and many still consider it to be the best initial study for the evaluation of microhematuria. However, IVU by itself has limited sensitivity in detecting small renal masses. When a mass is detected by IVU, further lesion characterization by ultrasonography, computed tomography (CT) or magnetic resonance imaging (MRI) is necessary because IVU cannot distinguish solid from cystic masses. CT is the best imaging modality for the evaluation of urinary stones, renal and perirenal infections, and associated complications. For the detection of transitional cell carcinoma in the kidney or ureter, IVU is superior to ultrasonography. CT urography with abdominal compression results in reliable opacification of the collecting system, comparable to that obtained with IVU. High detection rates for transitional cell carcinoma on contrast-enhanced CT images have been reported, but the studies offer no statistical analysis.31,32 There are currently no studies MARCH 15, 2001 / VOLUME 63, NUMBER 6 comparing the performance of various diagnostic-imaging modalities in the detection of transitional cell carcinomas in the upper urinary tract. Retrograde pyelography is considered the best imaging approach for the detection and characterization of ureteral abnormalities, but this general opinion is not based on evidence. No data exist showing the impact of IVU, ultrasonography, CT or MRI on the management of patients with microscopic hematuria. Therefore, evidence-based imaging guidelines cannot be formulated. IVU currently remains the initial evaluation of choice for upper tract imaging in patients with microhematuria for TABLE 3 Imaging Modalities for Evaluation of the Urinary Tract Modality Advantages and disadvantages Intravenous urography Considered by many to be best initial study for evaluation of urinary tract Widely available and most cost-efficient in most centers Limited sensitivity in detecting small renal masses Cannot distinguish solid from cystic masses; therefore, further lesion characterization by ultrasonography, computed tomography or magnetic resonance imaging is necessary Better than ultrasonography for detection of transitional cell carcinoma in kidney or ureter Ultrasonography Excellent for detection and characterization of renal cysts Limitations in detection of small solid lesions (< 3 cm) Computed tomography Preferred modality for detection and characterization of solid renal masses Detection rate for renal masses comparable to that of magnetic resonance imaging, but more widely available and less expensive Best modality for evaluation of urinary stones, renal and perirenal infections, and associated complications Sensitivity of 94 % to 98 % for detection of renal stones, compared with 52% to 59% for intravenous urography and 19% for ultrasonography Adapted with permission from Grossfeld GD, Wolf JS, Litwin MS, Hricak H, Shuler CL, Agerter DC, Carroll P. Evaluation of asymptomatic microscopic hematuria in adults: the American Urological Association best practice policy recommendations. Part II: patient evaluation, cytology, voided markers, imaging, cystoscopy, nephrology evaluation, and follow-up. Urology 2001;57(4) (In press). www.aafp.org/afp AMERICAN FAMILY PHYSICIAN 1151 several reasons: (1) the technology is standardized, (2) previous series examining patients with microhematuria have been based on this modality, (3) the rate of missed diagnoses is low when IVU is followed by appropriate studies and (4) IVU is less expensive than CT in most centers. However, the advantage of CT over IVU is that CT has the highest efficacy for the range of possible underlying pathologies, and it shortens the duration of the diagnostic work-up. If CT is chosen as the initial upper tract study, the imaging protocol should be adapted to the diagnostic goals, such as the exclusion of urolithiasis and renal neoplasm. CT urography spiral (helical) is preferred if the technology is available. Neither oral nor rectal contrast medium is required. The CT protocol should start with a noncontrast scan. If this scan demonstrates urolithiasis in a patient who is at low risk for underlying malignancy (Table 1),4 no further scanning is needed. In all other patients, including those in whom a urinary calculus is not detected, intravenous contrast medium should be injected. CT scout (topogram) or plain-film abdominal radiography (depending on the equipment avail- The Authors GARY D. GROSSFELD, M.D., is assistant professor of urology at the University of California, San Francisco, School of Medicine. J. STUART WOLF, JR., M.D., is associate professor of surgery (urology) at the University of Michigan Medical School, Ann Arbor. MARK S. LITWIN, M.D., M.P.H., is associate professor of urology and health services at the University of California, Los Angeles, Schools of Medicine and Public Health. HEDVIG HRICAK, M.D., PH.D., is chair of the radiology department at Memorial SloanKettering Cancer Center, New York City. CATHRYN L. SHULER, M.D., is a physician with Kaiser Permanente, Portland, Ore. DAVID C. AGERTER, M.D., is chair of the family medicine department at Mayo Clinic, Rochester, Minn. PETER R. CARROLL, M.D., is professor and chair of the urology department at the University of California, San Francisco, School of Medicine. Address correspondence to Carol Schwartz, M.P.H., R.D., Guidelines Manager, American Urological Association, 1120 N. Charles St., Baltimore, MD 21201-5559 (e-mail: [email protected]). Reprints are not available from the authors . 1152 AMERICAN FAMILY PHYSICIAN www.aafp.org/afp able) can be performed at the end of the CT examination to assess the ureters and bladder in an IVU–like fashion. Cystoscopic evaluation of the bladder (complete visualization of the bladder mucosa, urethra and ureteral orifices) is necessary to exclude the presence of bladder cancer. Cystoscopy as a component of the initial office evaluation of microscopic hematuria is recommended in all adult patients more than 40 years of age and in patients less than 40 years of age with risk factors for bladder cancer. This includes patients in whom upper tract imaging reveals a potentially benign source for bleeding. Cystoscopy appears to have a low yield in select patients at low risk for bladder cancer, including men and women younger than 40 years with no risk factors for this malignancy.10,14,20,21,33 In these patients, initial cystoscopy may be deferred, but urinary cytology should be performed. Initial diagnostic cystoscopy can be performed under local anesthesia using a rigid or flexible cystoscope. Compared with rigid cystoscopy, flexible cystoscopy causes less pain and is associated with fewer post-procedure symptoms.34-36 In addition, positioning and preparation of the patient are simplified, and procedure time is reduced.34 Flexible cystoscopy appears to be at least equivalent in diagnostic accuracy to rigid cystoscopy; for some lesions (i.e., those at the anterior bladder neck), it may be superior.34,37 Because some patients with a negative initial evaluation for asymptomatic microhematuria eventually develop significant urologic disease, some form of follow-up is indicated. Although most patients with a negative initial evaluation for asymptomatic microhematuria do not develop significant urologic disease, some patients do. Consequently, some form of follow-up is indicated. Because the appearance of hematuria can precede the diagnosis of bladder cancer by many years,38 such follow-up seems especially important in highVOLUME 63, NUMBER 6 / MARCH 15, 2001 Hematuria risk groups, including patients older than 40 years and those who use tobacco or whose occupational exposures put them at risk.15 Because the risk of life-threatening lesions in patients with a negative initial evaluation is low and the data regarding follow-up in such patients are sparse, recommendations regarding appropriate follow-up must be based on consensus opinion, in addition to review of the available literature-based evidence. In patients with a negative initial evaluation of asymptomatic microscopic hematuria, consideration should be given to repeating urinalysis, voided urine cytology and blood pressure determination at six, 12, 24 and 36 months. Although cytology may not be a sensitive marker for detecting lowgrade transitional cell carcinoma, it detects most high-grade tumors and carcinomas in situ, particularly if the test is repeated. Such high-grade lesions are the most likely to benefit from early detection. Additional evaluation, including repeat imaging and cystoscopy, may be warranted in patients with persistent hematuria in whom there is a high index of suspicion for significant underlying disease. In this setting, the clinical judgment of the treating physician should guide further evaluation. Immediate urologic reevaluation, with consideration of cystoscopy, cytology or repeat imaging, should be performed if any of the following occur: (1) gross hematuria, (2) abnormal urinary cytology or (3) irritative voiding symptoms in the absence of infection. If none of these occurs within three years, the patient does not require further urologic monitoring. Further evaluation for renal parenchymal disease or referral to a nephrologist should be considered if hematuria persists and hypertension, proteinuria or evidence of glomerular bleeding (red cell casts, dysmorphic red blood cells) develops. The AUA panel members thank Lisa Cowen, Ph.D., and Carol Schwartz, M.P.H., R.D., for assistance with the manuscript. MARCH 15, 2001 / VOLUME 63, NUMBER 6 Computed tomography is the best imaging modality for the evaluation of urinary stones, renal and perirenal infections, and associated complications. REFERENCES 1. Grossfeld GD, Carroll PR. Evaluation of asymptomatic microscopic hematuria. Urol Clin North Am 1998;25:661-76. 2. U.S. Preventive Services Task Force. Guide to clinical preventive services. 2d ed. Alexandria, Va.: International Medical Publishing, 1996. 3. Grossfeld GD, Wolf JS, Litwin MS, Hricak H, Shuler CL, Agerter DC, Carroll P. Evaluation of asymptomatic microscopic hematuria in adults: the American Urological Association best practice policy recommendations. Part I: definition, detection, prevalence, and etiology. Urology 2001;57(4) (In press). 4. Grossfeld GD, Wolf JS, Litwin MS, Hricak H, Shuler CL, Agerter DC, Carroll P. Evaluation of asymptomatic microscopic hematuria in adults: the American Urological Association best practice policy recommendations. Part II: patient evaluation, cytology, voided markers, imaging, cystoscopy, nephrology evaluation, and follow-up. Urology 2001;57(4) (In press). 5. Sutton JM. Evaluation of hematuria in adults. JAMA 1990;263:2475-80. 6. Messing EM, Young TB, Hunt VB, Emoto SE, Wehbie JM. The significance of asymptomatic microhematuria in men 50 or more years old: findings of a home screening study using urinary dipsticks. J Urol 1987;137:919-22. 7. Woolhandler S, Pels RJ, Bor DH, Himmelstein DU, Lawrence RS. Dipstick urinalysis screening of asymptomatic adults for urinary tract disorders. I. Hematuria and proteinuria. JAMA 1989;262:1214-9. 8. Mariani AJ, Luangphinith S, Loo S, Scottolini A, Hodges CV. Dipstick chemical urinalysis: an accurate cost-effective screening test. J Urol 1984;132: 64-6. 9. Messing EM, Young TB, Hunt VB, Wehbie JM, Rust P. Urinary tract cancers found by homescreening with hematuria dipsticks in healthy men over 50 years of age. Cancer 1989;64:2361-7. 10. Mariani AJ, Mariani MC, Macchioni C, Stams UK, Hariharan A, Moriera A. The significance of adult hematuria: 1,000 hematuria evaluations including a risk-benefit and cost-effectiveness analysis. J Urol 1989;141:350-5. 11. Britton JP, Dowell AC, Whelan P. Dipstick haematuria and bladder cancer in men over 60: results of a community study. BMJ 1989;299:1010-2. 12. Britton JP, Dowell AC, Whelan P, Harris CM. A community study of bladder cancer screening by the detection of occult urinary bleeding. J Urol 1992; 148:788-90. www.aafp.org/afp AMERICAN FAMILY PHYSICIAN 1153 Hematuria 13. Messing EM, Young TB, Hunt VB, Roecker EB, Vaillancourt AM, Hisgen WJ, et al. Home screening for hematuria: results of a multiclinic study. J Urol 1992;148(2 pt 1):289-92. 14. Bard RH. The significance of asymptomatic microhematuria in women and its economic implications. A ten-year study. Arch Intern Med 1988; 148:2629-32. 15. Carson CC 3d, Segura JW, Greene LF. Clinical importance of microhematuria. JAMA 1979;241: 149-50. 16. Davides KC, King LM, Jacobs D. Management of microscopic hematuria: twenty-year experience with 150 cases in a community hospital. Urology 1986;28:453-5. 17. Fracchia JA, Motta J, Miller LS, Armenakas NA, Schumann GB, Greenberg RA. Evaluation of asymptomatic microhematuria. Urology 1995;46:484-9. 18. Greene LF, O’Shaughnessey EJ, Hendricks ED. Study of five hundred patients with asymptomatic microhematuria. JAMA 1956;161:610-3. 19. Golin AL, Howard RS. Asymptomatic microscopic hematuria. J Urol 1980;124:389-91. 20. Jones DJ, Langstaff RJ, Holt SD, Morgans BT. The value of cystourethroscopy in the investigation of microscopic haematuria in adult males under 40 years. A prospective study of 100 patients. Br J Urol 1988;62:541-5. 21. Murakami S, Igarashi T, Hara S, Shimazaki J. Strategies for asymptomatic microscopic hematuria: a prospective study of 1,034 patients. J Urol 1990; 144:99-101. 22. Ritchie CD, Bevan EA, Collier SJ. Importance of occult haematuria found at screening. Br Med J [Clin Res] 1986;292:681-3. 23. Thompson IM. The evaluation of microscopic hematuria: a population-based study. J Urol 1987;138:1189-90. 24. Tapp DC, Copley JB. Effect of red blood cell lysis on protein quantitation in hematuric states. Am J Nephrol 1988;8:190-3. 25. Pollock C, Liu PL, Gyory AZ, Grigg R, Gallery ED, Caterson R, et al. Dysmorphism of urinary red blood cells—value in diagnosis. Kidney Int 1989; 36:1045-9. 26. De Santo NG, Nuzzi F, Capodicasa G, Lama G, Caputo G, Rosati P, et al. Phase contrast microscopy of the urine sediment for the diagnosis of glomerular and nonglomerular bleeding—data in children and adults with normal creatinine clearance. Nephron 1987;45:35-9. 1154 AMERICAN FAMILY PHYSICIAN www.aafp.org/afp 27. Mariani AJ. The evaluation of adult hematuria: a clinical update. In: AUA update series 1998; volume XVII, lesson 24. Houston: AUA Office of Education, 1998:185-92. 28. Jamis-Dow CA, Choyke PL, Jennings SB, Linehan WM, Thakore KN, Walther MM. Small (< or = 3cm) renal masses: detection with CT versus US and pathologic correlation. Radiology 1996;198: 785-8. 29. Sourtzis S, Thibeau JF, Damry N, Raslan A, Vandendris M, Bellemans M. Radiologic investigation of renal colic: unenhanced helical CT compared with excretory urography. AJR Am J Roentgenol 1999; 172:1491-4. 30. Fielding JR, Silverman SG, Samuel S, Zou KH, Loughlin KR. Unenhanced helical CT of ureteral stones: a replacement for excretory urography in planning treatment. AJR Am J Roentgenol 1998; 171:1051-3. 31. Igarashi T, Muakami S, Shichijo Y, Matsuzaki O, Isaka S, Shimazaki J. Clinical and radiological aspects of infiltrating transitional cell carcinoma of the kidney. Urol Int 1994;52:181-4. 32. Buckley JA, Urban BA, Soyer P, Scherrer A, Fishman EK. Transitional cell carcinoma of the renal pelvis: a retrospective look at CT staging with pathologic correlation. Radiology 1996;201:194-8. 33. Sparwasser C, Cimniak HU, Treiber U, Pust RA. Significance of the evaluation of asymptomatic microscopic haematuria in young men. Br J Urol 1994; 74:723-9. 34. Clayman RV, Reddy P, Lange PH. Flexible fiberoptic and rigid-rod lens endoscopy of the lower urinary tract: a prospective controlled comparison. J Urol 1984;131:715-6. 35. Denholm SW, Conn IG, Newsam JE, Chisholm GD. Morbidity following cystoscopy: comparison of flexible and rigid techniques. Br J Urol 1990;66: 152-4. 36. Flannigan GM, Gelister JS, Noble JG, Milroy EJ. Rigid versus flexible cystoscopy. A controlled trial of patient tolerance. Br J Urol 1988;62:537-40. 37. Pavone-Macaluso M, Lamartina M, Pavone C, Vella M. The flexible cystoscope. Int Urol Nephrol 1992;24:239-42. 38. Hiatt RA, Ordonez JD. Dipstick urinalysis screening, asymptomatic microhematuria, and subsequent urological cancers in a population-based sample. Cancer Epidemiol Biomarkers Prev 1994;3:439-43 [Published erratum appears in Cancer Epidemiol Biomarkers Prev 1994;3:523]. VOLUME 63, NUMBER 6 / MARCH 15, 2001 UpToDate®: 'Evaluation of hematuria in adults' ONLINE 11.3 New Search Page 1 of 18 ©2004 UpToDate Table of Contents ® Help Official reprint from UpToDate® http://www.uptodate.com/ Evaluation of hematuria in adults Burton D Rose, MD Robert H Fletcher, MD UpToDate performs a continuous review of over 300 journals and other resources. Updates are added as important new information is published. The literature review for version 11.3 is current through September 2003; this topic was last changed on March 19, 2002. The next version of UpToDate (12.1) will be released in February 2004. Hematuria that is not explained by an obvious condition (eg, cystitis) is relatively common. As an example, one study of 231 men over the age of 50, who were tested weekly for three months, found that hematuria was present in 10 percent [1]. Hematuria itself is not dangerous unless extraglomerular bleeding is so brisk that it causes clots that obstruct the ureter(s). However, the finding of hematuria is important, since it may be a symptom of an underlying serious condition. In the example noted above, of the 23 patients with hematuria, five were found to have cancers involving the urinary tract, and another five had underlying medical disorders requiring immediate treatment [1]. DEFINITION OF HEMATURIA — Hematuria may be grossly visible or microscopic. Gross hematuria — Gross hematuria is suspected because of the presence of red or brown urine. The color change does not necessarily reflect the degree of blood loss, since as little as 1 mL of blood per liter of urine can induce a visible color change. In addition, the intermittent excretion of red to brown urine can be seen in a variety of clinical settings other than blood loss. (See "Red urine: Hematuria, hemoglobinuria; myoglobinuria"). Thus, the initial step in the evaluation of patients with red urine is centrifugation of the specimen to see if the red color is in the urine sediment or the supernatant (show figure 1). As contamination with blood is a possibility in menstruating and post-partum women, urine for analysis is best obtained when the bleeding has ceased. If this is not possible, a tampon can be inserted, and urinalysis obtained after the perineum is thoroughly cleansed. Hematuria is responsible if the red color is seen only in the urine sediment, with the supernatant being clear. If, on the other hand, it is the supernatant that is red, then the supernatant should be tested for heme with a urine dipstick. A red supernatant that is negative for heme is a rare finding that can be seen in several conditions, including porphyria (show figure 2). (See "Understanding the porphyrias", section on Urine porphyrin analysis). Other causes include the use of the bladder analgesic phenazopyridine, and the ingestion of beets in susceptible subjects. (See "Red urine: Hematuria, hemoglobinuria; myoglobinuria", section on Beeturia). A red supernatant that is positive for heme is due to myoglobinuria or hemoglobinuria. mhtml:file://C:\Documents%20and%20Settings\All%20Users\Documents\F... 5/26/2004 UpToDate®: 'Evaluation of hematuria in adults' Page 2 of 18 Microscopic hematuria — Microscopic hematuria may be discovered by accident when blood (either red blood cells or hemoglobin) is found on a urinalysis or dipstick done for other purposes. Although hematuria is commonly defined as the presence of more than 2 RBCs per high power field in a spun urine sediment, there is no "safe" lower limit below which significant disease can be excluded (show sediment 1) [2]. Lowering the cut-off value of RBCs chosen to define hematuria results in a greater number of false positive test results (eg, no underlying abnormality is found). On the other hand, if higher cut-off values are chosen, it is more likely that the test will miss the presence of significant abnormalities. The urine sediment is the gold standard for the detection of microscopic hematuria. Dipsticks for hemoglobin detect 1 to 2 RBCs per high powered field and are therefore at least as sensitive as urine sediment examination, but result in more false positive tests. In comparison, false negative tests are unusual; as a result, a negative dipstick reliably excludes abnormal hematuria [3]. Although red cells may be lysed in dilute urine, their hemoglobin content will still be detected by the dipstick method. ETIOLOGY — Hematuria may be a symptom of an underlying disease, some of which are life threatening or treatable. The causes vary with age with the most common being inflammation or infection of the prostate or bladder, stones, and, in older patients, malignancy or benign prostatic hyperplasia (show figure 3) [2,4,5]. INITIAL EVALUATION — The initial evaluation of hematuria usually does not require the participation of a subspecialist (nephrologist or urologist). This evaluation should address the following three questions: Are there any clues from the history or physical examination that suggest a particular diagnosis? Does the hematuria represent glomerular or extraglomerular bleeding? Is the hematuria transient or persistent? Historical clues — There are often clues from the history that point toward a specific diagnosis. These include: Concurrent pyuria and dysuria, which are usually indicative of a urinary tract infection. A recent upper respiratory infection, suggesting either postinfectious glomerulonephritis or IgA nephropathy (see "Hematuria following an upper respiratory infection"). A positive family history of renal disease, as in hereditary nephritis or polycystic kidney disease. Unilateral flank pain, which may radiate to the groin, suggesting ureteral obstruction due to a calculus or blood clot. Flank pain that is persistent or recurrent can also occur in the rare loin pain hematuria syndrome (see below). Symptoms of prostatic obstruction in older men such as hesitancy and dribbling. The cellular proliferation in benign prostatic hyperplasia (BPH) is associated with increased vascularity, and the new vessels can be fragile. There is some controversy about whether hematuria is more common in these patients than in age-matched controls [6,7]. However, there is general agreement that the presence of BPH should not dissuade the clinician from pursuing further evaluation of hematuria, particularly since older men are more likely to have more serious disorders such as cancer of the prostate or bladder. Among those with gross hematuria in whom no other cause can be identified, finasteride usually suppresses the hematuria [8,9]. (See "Treatment of benign prostatic hyperplasia"). mhtml:file://C:\Documents%20and%20Settings\All%20Users\Documents\F... 5/26/2004 UpToDate®: 'Evaluation of hematuria in adults' Page 3 of 18 Recent vigorous exercise or trauma (see "Exercise-induced hematuria"). History of a bleeding disorder or bleeding from multiple sites due to uncontrolled anticoagulant therapy. In contrast, it should not be assumed that hematuria alone can be explained by chronic warfarin therapy. In one report of 243 patients prospectively followed for two years, the incidence of hematuria was similar to that in a control group not receiving warfarin [10]. Furthermore, evaluation of patients who developed hematuria revealed a genitourinary cause in 81 percent of cases. Infection was most common, but papillary necrosis, renal cysts, and several malignancies of the bladder were also found. A smaller study found significant urinary tract disease in nine of 30 patients, two of whom had bladder cancer [11]. These observations indicate that hematuria in an anticoagulated patient should generally be evaluated in the same fashion as in other patients unless there is evidence of bleeding from multiple sites with markedly abnormal coagulation studies. Cyclic hematuria in women that is most prominent during and shortly after menstruation, suggesting endometriosis of the urinary tract [12]. Contamination with menstrual blood is always a possibility, and should be ruled out by repeating the urinalysis when menstruation has ceased. Medications that might cause nephritis (usually with other findings, typically with renal insufficiency). In addition, black patients should be screened for sickle cell trait or disease, which can lead to papillary necrosis and hematuria, (See "Renal manifestations of sickle cell disease"). Glomerular versus extraglomerular bleeding — The identification of the glomeruli as the source of bleeding is important both prognostically and to optimize the subsequent evaluation. In particular, patients with clear evidence of glomerular hematuria do not need to be evaluated for potentially serious urologic disease [13]. Signs of glomerular bleeding include red cell casts (essentially pathognomonic for glomerular disease), protein excretion exceeding 500 mg/day at a time when there is no gross bleeding, most red cells having a dysmorphic appearance, and brown, cola-colored urine (show table 1 and show sediment 2A-2C). (See "Hematuria: Glomerular versus extraglomerular bleeding"). Although helpful if present, the absence of these findings does not exclude glomerular disease. An additional important abnormality that may be seen is blood clots. Clots virtually never occur in glomerular disease, perhaps due to the presence of urokinase and tissue-type plasminogen activators in the glomeruli and in the renal tubules. Three tube test — In addition to the routine urinalysis, a three-tube test may also help to locate the source of bleeding in selected cases. This test involves the collection and comparative evaluation of three different urine specimens of roughly equal volume: the first few mL; a mid-stream sample; and the last few mL. A urethral lesion is most likely if the hematuria primarily occurs in the first sample, whereas a lesion near the bladder trigone is most likely with terminal hematuria. Renal, ureteric, and diffuse bladder lesions result in equivalent degrees of hematuria in each of the three specimens. Similar information can on occasion be obtained from the history in patients with gross hematuria. Role of renal biopsy — Although any glomerular disease may be associated with hematuria, most patients also have other signs such as proteinuria, red cell casts, or renal insufficiency. When persistent hematuria is essentially the only manifestation of glomerular disease, one of three disorders is most likely: (1) IgA nephropathy, in which there is often gross hematuria but a negative family history of renal disease; (2) hereditary nephritis, in which gross hematuria can occur in association with a positive family history of renal failure; and (3) thin basement membrane disease (also called benign familial hematuria), in which gross hematuria is unusual and the family history may be positive for microscopic hematuria but not for renal failure [14]. (See "Glomerular hematuria: IgA; Alport; thin basement mhtml:file://C:\Documents%20and%20Settings\All%20Users\Documents\F... 5/26/2004 UpToDate®: 'Evaluation of hematuria in adults' Page 4 of 18 membrane disease"). One of these three conditions is present in more than one-half of adults with isolated hematuria and a negative radiologic and cystoscopic evaluation [14]. (See "Unexplained hematuria" below). Postinfectious glomerulonephritis and exercise also can induce isolated glomerular bleeding; however, the hematuria in these settings is typically transient, not persistent as in the above disorders. (See "Hematuria following an upper respiratory infection" and see "Exercise-induced hematuria"). Patients with glomerular hematuria should be referred to a nephrologist; they are likely to be more experienced at examining urine sediment and can make a decision regarding the need for renal biopsy. A biopsy is not usually performed for isolated glomerular hematuria, since there is no specific therapy for any of these conditions. The lack of utility of a renal biopsy in this setting is supported by a study of 111 patients presenting with isolated hematuria in whom 75 underwent renal biopsy [15]. Follow-up of 85 patients at 43 months revealed that three patients had developed proteinuria (two with IgA nephropathy and one without a biopsy), one had proteinuria and renal insufficiency (membranoproliferative glomerulonephritis), and 11 were hypertensive (three with thin basement membrane disease, two with IgA nephropathy, two with normal results, one with focal glomerular sclerosis, and three without biopsy). The management of these patients was rarely affected by the biopsy results. However, biopsy should be considered if there is evidence of progressive disease as manifested by an elevation in the plasma creatinine concentration, increasing protein excretion, or an otherwise unexplained rise in blood pressure, even when the values remain within the normal range [16]. Transient or persistent hematuria — No cause of low-level hematuria, in the absence of other signs and symptoms, requires immediate diagnosis. Thus, it is reasonable to repeat an abnormal urinalysis in a few days to determine if hematuria is transient or persistent. Transient microscopic hematuria is a common problem in adults. One study evaluated 1000 young men who had yearly urinalyses between the ages of 18 and 33; hematuria was seen in 39 percent on at least one occasion and 16 percent on two or more occasions [17]. Hematuria has also been found in up to 13 percent of postmenopausal women [4]. No obvious etiology can be identified in most cases. Fever, infection, trauma, and exercise are potential causes of transient hematuria. (See "Exercise-induced hematuria"). Malignancy risk in older patients with transient hematuria — An important exception occurs in older patients in whom even transient hematuria carries an appreciable risk of malignancy (assuming no evidence of glomerular bleeding) [2,5,18,19]. One report studied 1034 patients with more than 5 red cells per high power field on at least 1 of 3 screening urinalyses. All patients were evaluated by ultrasonography, intravenous pyelography (IVP), urinary cytology, and cystoscopy; the incidence of malignancy (bladder, kidney, or prostate) was 2.4 percent. Neither cytology nor IVP reliably detected all of the tumors. Ultrasonography was very accurate for renal tumors, while cystoscopy was required to reliably diagnose bladder or prostatic cancers [5]. Tumors were more common in men and all but one occurred in patients over the age of 50. Another 20 percent of patients had kidney stones or glomerular or other intrinsic renal disease, while the remaining 78 percent had either no identifiable cause or a minor lesion such as benign prostatic hypertrophy [5]. Other screening studies limited to healthy men over the age of 50 to 60 found an even greater risk: 8 to 9 percent of patients with intermittent asymptomatic hematuria, as detected by screening with a dipstick for heme, had a urinary tract malignancy [18,19]. mhtml:file://C:\Documents%20and%20Settings\All%20Users\Documents\F... 5/26/2004 UpToDate®: 'Evaluation of hematuria in adults' Page 5 of 18 An even greater concern about underlying malignancy applies to patients with persistent hematuria in whom there is no obvious cause from the history and no clear evidence of glomerular disease, such as red cell casts. In one study, the incidence of malignancy (mostly arising from the bladder) ranged from 5 percent with microscopic hematuria to as high as 20 percent with gross hematuria [13]. Another study of 1000 patients found an overall incidence of malignancy of 8 percent; this proportion was clearly age-dependent, increasing substantially in patients over age 50 [2]. RADIOLOGIC TESTS — Once glomerular bleeding has been excluded in a patient with otherwise unexplained hematuria, the diagnostic work-up should include a search for lesions in the kidney, collecting system, ureters, and bladder. The diagnostic yield in adults increases with age and is higher for gross hematuria (5 to 23 percent) than for microscopic hematuria (up to 14 percent) [20], and for higher grades of bleeding than for lesser grades. The optimal radiologic evaluation for isolated hematuria is uncertain because the great majority of patients will have negative or minor findings (show table 2) [17]. Nevertheless, if there is no specific clue to the correct diagnosis (such as kidney stones or red cell casts), most physicians will order an intravenous pyelogram (IVP) or a renal ultrasound, looking for calculi, a renal mass, or polycystic kidney disease [3,5]. An IVP is a reasonable first choice in young patients, since it can detect lesions such as medullary sponge kidney that may not be seen by ultrasonography. It is also preferred by urologists in older patients because it can detect lesions in the renal pelvis and ureters. In patients who have a contraindication to IVP (eg, dye allergy), ultrasound is the usual alternative [21]. Some studies suggest that ultrasonography has a somewhat lower diagnostic yield, while others found that it is more accurate [22]. Young patients with a normal IVP do not need ultrasonography, since the yield of significant findings is very low [23]. However, older patients with a normal IVP should undergo ultrasonography or helical CT scan, which are better at visualizing small renal tumors [3,24]. URINE CYTOLOGY — A voided urine specimen should be sent for cytology in patients at increased risk for urothelial cancers (see next section). The sensitivity of urine cytology is greatest for carcinoma in situ of the bladder (approximately 90 percent). By comparison, sensitivity for upper tract transitional cell carcinoma is limited, with the reported false negative rate overall being 65 percent (and as high as 96 percent with low grade tumors) [25,26]. Urine cytology is frequently obtained during cystoscopy, which is usually performed in patients at risk for malignancy. Among patients at low risk for genitourinary cancer (such as individuals under the age of 40 without specific risk factors), some investigators recommend that either urine cytology or cystoscopy be performed [27]. Cystoscopy is subsequently done if malignant and/or atypical/suspicious cells are identified. INDICATIONS FOR CYSTOSCOPY — The indications for cystoscopy when the IVP, ultrasonography, and/or CT scan and urine cytology are negative are incompletely defined [27]. The yield of these procedures is very low in men under the age of 40 and in low-risk women [3,14,20,28]. In general, cystoscopy is recommended in those patients at risk for bladder cancer: men over the age of 50 [3,5,18,19]; and those with specific risk factors such as prolonged heavy phenacetin use, heavy smoking, exposure to certain dyes, or longterm administration of cyclophosphamide[20,27,29]. Analgesic abusers also have an increased incidence of carcinoma of the kidney. (See "Urinary tract malignancy and atherosclerotic disease with chronic analgesic abuse"). There is a field cancerization effect for urothelial tumors. Thus, among patients with hematuria who first undergo cystoscopy and are found to have a bladder tumor, the upper mhtml:file://C:\Documents%20and%20Settings\All%20Users\Documents\F... 5/26/2004 UpToDate®: 'Evaluation of hematuria in adults' Page 6 of 18 tracts should also be evaluated for possible lesions in the renal pelvis and ureter. (See "Clinical presentation; diagnosis; and staging of bladder cancer"). Cystoscopy is also indicated in the infrequent patient with otherwise unexplained persistent or intermittent gross hematuria. It may be possible with this procedure to determine if the bleeding is originating from the bladder or from one or both ureters. Unilateral bleeding may be due to an arteriovenous malformation, fistula, or venous varices (see below) [29]. UNEXPLAINED HEMATURIA — If no diagnosis is apparent from the history, urinalysis, radiologic tests, or cystoscopy, then the most likely causes of persistent isolated hematuria are a mild glomerulopathy as described above, or a predisposition to stone disease, particularly in young and middle-aged patients [14,30]. Glomerular disease — Approximately 50 percent of patients with idiopathic hematuria have a glomerular disease, which is more likely to persist than other causes of isolated hematuria. In one study, 86 percent of patients with hematuria persisting for four years had either IgA nephropathy or thin basement membrane disease [30]. Hypercalciuria and hyperuricosuria — As many as 30 to 35 percent of children with apparently idiopathic hematuria (no proteinuria or infection, negative radiologic evaluation) have hypercalciuria, while 5 to 20 percent of children with recurrent hematuria have hyperuricosuria [31-33]; both disorders are often associated with a positive family history (as high as 40 to 75 percent) of stone disease [31,33]. These children are at increased risk for the future development of kidney stones. Lowering calcium excretion with a thiazide diuretic typically leads to resolution of the hematuria among those with hypercalciuria [31]; a restricted purine diet or the administration of allopurinol commonly eliminates uricosuria and hematuria in those with hyperuricosuria. Similar findings may be present in adults. Some patients have hypercalciuria or hyperuricosuria (as detected by a 24-hour urine collection) [34,35], while others have a history suggestive of stone disease without these biochemical abnormalities (although citrate excretion was not measured in this study) [30]. (See "Risk factors for idiopathic calcium stones"). Treatment with a thiazide diuretic for hypercalciuria or allopurinol for hyperuricosuria usually leads to disappearance of the hematuria [34]. Arteriovenous malformations and fistulas — Rare causes of hematuria include arteriovenous malformations and fistulas, and the loin pain-hematuria syndrome. An arteriovenous malformation (AVM) or fistula, either congenital or acquired, is an unusual cause of hematuria. The primary presenting sign is gross hematuria, but high-output heart failure and hypertension also may be seen [29]. The latter is presumably due to activation of the renin-angiotensin system resulting from ischemia distal to the AVM [36]. The diagnosis may be suspected if there is an irregular filling defect on intravenous pyelography due to compression of the pelvis or calyx. The presence of an AVM can be confirmed by arteriography (which demonstrates almost immediate visualization of the inferior vena cava) or CT scanning. There are several therapeutic options. It is often possible for an experienced radiologist to embolize the lesion at the time of arteriography by the injection of absolute ethanol, steel coils, gelatin sponges, or balloons [37]. Absolute ethanol may be safest; it denatures proteins in the vessel wall, leading to a coagulum that occludes the lumen. Surgery or nephroscopy can be performed if embolization is ineffective or the hematuria recurs [36,37]. Loin pain-hematuria syndrome — The loin pain-hematuria syndrome is a poorly defined disorder characterized by loin or flank pain that is often severe and unrelenting and hematuria with dysmorphic red cell features suggesting a glomerular origin [38,39]. Some have suggested that these patients have a subtle disorder affecting the renal vasculature, although this has not been a consistent finding. One report has suggested an important psychologic component [40]. Fifteen patients with the clinical diagnosis of the loin painhematuria syndrome were compared with 10 patients with flank pain due to nephrolithiasis mhtml:file://C:\Documents%20and%20Settings\All%20Users\Documents\F... 5/26/2004 UpToDate®: 'Evaluation of hematuria in adults' Page 7 of 18 [40]. Patients in the former group were much more likely to have medically unexplained somatic symptoms, an adverse psychologic event preceding the onset of pain, and a history of greater analgesic ingestion. It was concluded that psychologic factors were of primary importance in the loin pain; the origin of the hematuria was uncertain. One possible explanation for the hematuria in some patients with the loin-pain hematuria syndrome is thin basement membrane disease. (See "Thin basement membrane disease (benign familial hematuria)"). One report found thin basement membrane disease in 7 of 15 patients in whom renal biopsy was performed for evaluation of possible loin pain-hematuria syndrome [41]. It was proposed that bleeding into and obstruction of the renal tubules was responsible for the loin pain. Four of these seven patients had a beneficial response to the administration of an angiotensin converting enzyme inhibitor, possibly due to a reduction in intraglomerular pressure. Whether this approach might be beneficial in other patients is not known. At present, optimal treatment of the loin pain-hematuria syndrome is unclear. The primary goal is frequently pain relief. Various treatment modalities may be utilized, ranging from nonsteroidal antiinflammatory drugs to nerve blocks to surgery. Dependence upon narcotics can occur in patients with unrelenting and debilitating discomfort. Some investigators advocate renal autotransplantation as definitive and effective therapy [42], while others report only temporary relief from this procedure [43]. Follow-up studies — The most serious disorder in the patient with unexplained hematuria is the presence of an undiagnosed carcinoma of the urinary tract. The combination of negative radiologic examination(s) (which may include IVP, ultrasonography, and/or helical CT scan alone or in combination), negative cytology, and negative cystoscopy is usually sufficient to exclude malignancy in the urinary tract [5]. However, a malignancy will subsequently become evident in some cases; as an example, approximately 1 percent of older patients with an initially negative evaluation will, at three to four years, have a detectable urinary tract malignancy [5]. As a result, initial and then periodic urine cytology and urinalyses should be performed in patients at high risk for malignancy (at 6, 12, 24 and 36 months) [27]. Some physicians also recommend repeat ultrasonography and cystoscopy at one year in high-risk patients with persistent hematuria [3,5,13]. On the other hand, low-risk patients with persistent idiopathic microscopic hematuria are usually followed with periodic urinalyses and urine cytology. SCREENING FOR HEMATURIA — Screening for hematuria in patients who have no symptoms suggestive of urinary tract disease is not recommended. The most plausible argument for screening would be for the early detection and treatment of cancers of the kidney, collecting system, or bladder in older adults. However, these and other diseases causing hematuria do not meet basic criteria for screening [44]: the prevalence of undetected, asymptomatic, early disease is relatively low; and there is little evidence that hematuria is a sensitive test for localized disease, or that (in the case of renal cancer) early treatment of local disease results in a better prognosis. Thus, expert groups such as the United States Preventive Services Task Force on the Periodic Health Examination do not recommend screening for disease by tests for hematuria. Use of UpToDate is subject to the Subscription and License Agreement. REFERENCES 1. Messing, EM, Young, TB, Hunt, VB, et al. The significance of asymptomatic microhematuria in men 50 or more years old: Findings of a home screening study using urinary dipsticks. J Urol 1987; 137:919. 2. Mariani, AJ, Mariani, MC, Macchioni, C, et al. The significance of adult hematuria: 1000 mhtml:file://C:\Documents%20and%20Settings\All%20Users\Documents\F... 5/26/2004 UpToDate®: 'Evaluation of hematuria in adults' Page 8 of 18 hematuria evaluations including risk-benefit and cost-effective analysis. J Urol 1989; 141:350. 3. Schroder, FH. Microscopic hematuria. Requires investigation. BMJ 1994; 309:70. 4. Mohr, DN, Offord, KP, Owen, RA, Melton, J, III. Asymptomatic microhematuria and urologic disease. A population-based study. JAMA 1986; 256:224. 5. Murakami, S, Igarashi, T, Hara, S, Shimazaki, J. Strategies for asymptomatic microscopic hematuria: A prospective study of 1,034 patients. J Urol 1990; 144:99. 6. Mohr, DN, Offord, KP, Melton, LJ 3rd. Isolated asymptomatic microhematuria: a crosssectional analysis of test-positive and test-negative patients. J Gen Intern Med 1987; 2:318. 7. Ezz el Din, K, Koch, WF, de Wildt, MJ, et al. The predictive value of microscopic haematuria in patients with lower urinary tract symptoms and benign prostatic hyperplasia. Eur Urol 1996; 30:409. 8. Foley, SJ, Soloman, LZ, Wedderburn, AW, et al. A prospective study of the natural history of hematuria associated with benign prostatic hyperplasia and the effect of finasteride. J Urol 2000; 163:496. 9. Miller, MI, Puchner, PJ. Effects of finasteride on hematuria associated with benign prostatic hyperplasia: long-term follow-up. Urology 1998; 51:237. 10. Culclasure, TF, Bray, VJ, Hasbargen, JA. The significance of hematuria in the anticoagulated patient. Arch Intern Med 1994; 154:649. 11. Van Savage, JG, Fried, FA. Anticoagulant associated hematuria: a prospective study. J Urol 1995; 153:1594. 12. Case records of the Massachusetts General Hospital. Weekly clinicopathological exercises. Case 33-1992. A 34-year-old woman with endometriosis and bilateral hydronephrosis. N Engl J Med 1992; 327:481. 13. Schramek, P, Schuster, FX, Georgopoulos, M, et al. Value of urinary erythrocyte morphology in assessment of symptomless microhaematuria. Lancet 1989; 2:1316. 14. Topham, PS, Harper, SJ, Furness, PN, et al. Glomerular disease as a cause of isolated microscopic microscopic haematuria. Q J Med 1994; 87:329. 15. McGregor, DO, Lynn, KO, Bailey, RR, et al. Clinical audit of the use of renal biopsy in the management of isolated microscopic hematuria. Clin Nephrol 1998; 49:345. 16. Szeto, C, Lai, FM, To, K, et al. The natural history of immunoglobulin a nephropathy among patients with hematuria and minimal proteinuria. Am J Med 2001; 110:434. 17. Froom, P, Ribak, J, Benbassat, J. Significance of microhaematuria in young adults. Br Med J 1984; 288:20. 18. Britton, JP, Dowell, AC, Whelan, P. Dipstick haematuria and bladder cancer in men over 60: Results of a community study. BMJ 1989; 299:1010. 19. Messing, EM, Young, TB, Hunt, VB, et al. Home screening for hematuria: Results of a multi-clinic study. J Urol 1992; 148:289. 20. Sutton, JM. Evaluation of hematuria in adults. JAMA 1990; 263:2475. 21. Corwin HL, Silverstein MD. The diagnosis of neoplasia in patients with asymptomatic microscopic hematuria: A decision analysis. J Urol 1988; 139:1002. 22. Spencer, J, Lindsell, D, Mastorakou, I. Ultrasonography compared with intravenous urography in the investigation of adults with haematuria. BMJ 1990; 301:1074. 23. Mokulis, JA, Arndt, WF, Downey, JR, et al. Should renal ultrasound be performed in the patient with microhematuria and a normal excretory urogram. J Urol 1995; 154:1300. 24. Lang, EK, Macchia, RJ, Thomas, R, et al. Computerized tomography tailored for the assessment of microscopic hematuria. J Urol 2002; 167:547. 25. Donat, MD, Herr, HW. Transitional cell carcinoma of the renal pelvis and ureter: diagnosis, staging, management, and prognosis. In: Urologic Oncology, Osterling, JE, Richie, JP, (Eds), WB Saunders Harcourt Brace Co, Philadelphia 1997, p.215. 26. Sarnacki, CT, McCormack, LJ, Kiser, WS, et al. Urinary cytology and the clinical mhtml:file://C:\Documents%20and%20Settings\All%20Users\Documents\F... 5/26/2004 UpToDate®: 'Evaluation of hematuria in adults' Page 9 of 18 diagnosis of urinary tract malignancy: a clinicopathologic study of 1400 patients. J Urol 1971; 106:761. 27. Grossfeld, GD, Wolf, JS Jr, Litwan, MS, et al. Asymptomatic microscopic hematuria in adults: Summary of the AUA best practice policy recommendations. Am Fam Physician 2001; 63:1145. 28. Bard, RH. The significance of asymptomatic hematuria in women and its economic implications. A ten-year study. Arch Intern Med 1988; 148:2629. 29. Piper, JM, Tonascia, J, Matanoski, GM. Heavy phenacetin use and bladder cancer in women aged 20 to 49 years. N Engl J Med 1985; 313:292. 30. Nieuwhof, C, Doorenbos, C, Grave, W, et al. A prospective study of the natural history of idiopathic non-proteinuric hematuria. Kidney Int 1996; 49:222. 31. Stapleton, FB, Roy S, 3d, Noe, HN, Jerkins, G. Hypercalciuria in children with hematuria. N Engl J Med 1984; 310:1345. 32. Stapleton, FB. Idiopathic hypercalciuria: association with isolated hematuria and risk for urolithiasis in children. The Southwest Pediatric Nephrology Study Group. Kidney Int 1990; 37:807. 33. Cattini Perrone, H, Bruder Stapleton, F, Toporovski, J, Schor, N. Hematuria due to hyperuricosuria in children: 36-month follow-up. Clin Nephrol 1997; 48:288. 34. Andres, A, Praga, M, Bello, I, et al. Hematuria due to hypercalciuria and hyperuricosuria in adult patients. Kidney Int 1989; 36:96. 35. Praga, M, Alegre, R, Hernandez, E, et al. Familial microscopic hematuria caused by hypercalciuria and hyperuricosuria. Am J Kidney Dis 2000; 35:141. 36. Crotty, KL, Orihuela, E, Warren, MM. Recent advances in the diagnosis and treatment of renal arteriovenous malformations and fistulas. J Urol 1993; 150:1355. 37. Kavoussi, L, Clayman, RV, Basler, J. Flexible, actively deflectable fiberoptic ureteronephroscopy. J Urol 1989; 142:949. 38. Loin pain/haematuria syndrome. Lancet 1992; 340:701. 39. Weisberg, LS, Bloom, PB, Simmons, RL, Vinr, ED. Loin pain hematuria syndrome. Am J Nephrol 1993; 13:229. 40. Lucas, PA, Leaker, BR, Murphy, M, Neild, GH. Loin pain and haematuria syndrome: A somatoform disorder. QJM 1995; 88:703. 41. Hebert, LA, Betts, JA, Sedmak, DD, et al. Loin pain-hematuria syndrome associated with thin glomerular basement membrane disease and hemorrhage into renal tubules. Kidney Int 1996; 49:168. 42. Spitz, A, Huffman, JL, Mendez, R. Autotransplantation as an effective therapy for the loin pain-hematuria syndrome: Case reports and a review of the literature. J Urol 1997; 157:1554. 43. Harney, J, Rodgers, E, Campbell, E, Hickey, DP. Loin pain-hematuria syndrome: How effective is renal autotransplantation in its treatment? Urology 1994; 44:493. 44. Woolhandler, S, Pels, RJ, Bor, DH, et al. Dipstick urinalysis screening of asymptomatic adults for urinary tract disorders. I. Hematuria and proteinuria. JAMA 1989; 262:1214. GRAPHICS mhtml:file://C:\Documents%20and%20Settings\All%20Users\Documents\F... 5/26/2004 UpToDate®: 'Evaluation of hematuria in adults' Page 10 of 18 mhtml:file://C:\Documents%20and%20Settings\All%20Users\Documents\F... 5/26/2004 UpToDate®: 'Evaluation of hematuria in adults' Page 11 of 18 mhtml:file://C:\Documents%20and%20Settings\All%20Users\Documents\F... 5/26/2004 UpToDate®: 'Evaluation of hematuria in adults' Page 12 of 18 mhtml:file://C:\Documents%20and%20Settings\All%20Users\Documents\F... 5/26/2004 UpToDate®: 'Evaluation of hematuria in adults' Page 13 of 18 mhtml:file://C:\Documents%20and%20Settings\All%20Users\Documents\F... 5/26/2004 UpToDate®: 'Evaluation of hematuria in adults' Page 14 of 18 mhtml:file://C:\Documents%20and%20Settings\All%20Users\Documents\F... 5/26/2004 UpToDate®: 'Evaluation of hematuria in adults' Page 15 of 18 mhtml:file://C:\Documents%20and%20Settings\All%20Users\Documents\F... 5/26/2004 UpToDate®: 'Evaluation of hematuria in adults' Page 16 of 18 mhtml:file://C:\Documents%20and%20Settings\All%20Users\Documents\F... 5/26/2004 UpToDate®: 'Evaluation of hematuria in adults' Page 17 of 18 mhtml:file://C:\Documents%20and%20Settings\All%20Users\Documents\F... 5/26/2004 UpToDate®: 'Evaluation of hematuria in adults' New Search ©2004 UpToDate ® Table of Contents Page 18 of 18 Help • http://www.uptodate.com/ • [email protected] mhtml:file://C:\Documents%20and%20Settings\All%20Users\Documents\F... 5/26/2004



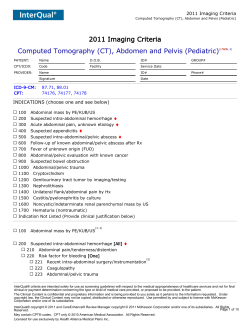







© Copyright 2026