
The abdomen The urinary bladder; the male urethra Retention of urine
The abdomen The urinary bladder; the male urethra (Chapter 9.1) Retention of urine Presentation: Acute retention: failure to pass urine, with pain. Chronic retention of urine: pseudo-incontinence, overflow incontinence, often with kidneys dilatation and renal failure. Causes: Prostate enlargement: benign prostate hypertrophy (adenoma), cancer, prostatitis. Urethral stricture. Severe pelvic trauma with urethral rupture. Neurological cause. Methods for draining urine: Urethral catherization Suprapubic catheterization Cystostomy. Urethral catheterization The most commonly used, but to be avoided in case of prostatitis, rupture of urethra, recurrent urethral stenosis. Always use a Foley catheter of reasonable calibre (not less than CH 16), smaller catheters are more difficult to insert into the bladder. In case of difficulties, and only if you are experienced, you can use an introducer (risk of trauma and bleeding). Wash hands. Don sterile gloves. Clean the urethral meatus with povidone-iodine or chlorhexidine. Place a fenestrated towel over the penis. Technique Clean again with gloves. Connect catheter to bag straight away. Lubricate the catheter with sterile K-Y jelly or Lidocain jelly. The left hand holds up the penis under slight traction, the right hand inserts the catheter slowly and continuously. Issue of urine confirms introduction into the bladder but it is wise to insert the catheter fully (so as not to risk inflating the balloon in the posterior urethra). Inflate the balloon with sterile water and withdraw the catheter to pull the balloon against the bladder neck. Monitoring Maintain a sufficient urine output to avoid blockage of the catheter. Avoid opening the closed system and any lavage that may cause infection. The high urine output will ensure the system is clean. The same catheter can stay for several weeks if necessary. No routine antibiotics unless there is fever caused by UTI, even if the urine analysis shows evidence of UTI. 127 Suprapubic catheterization (see procedure) To be preferred because it is cleaner and less traumatic. It allows easy reestablioshment of normal urination when re-established. Compulsory in case of: prostatitis, traumatic rupture of urethra, recurrent urethral stenosis, failure of urethral catheterization. To be avoided in case of: known bladder tumour. Monitoring The only disadvantage is the small size of the drain, maintain a high urine output. No routine antibiotics. Cystostomy Surgical drainage of the bladder when urethral and suprapubic catheterization have failed (rare) Anaesthesia General or spinal. Local is possible, with 1% Lidocain. Position Supine. Drapes allowing a midline infra-umbilical incision. Povidone iodine painting. Technique Short suprapubic midline incision. Incise the fascia at the top of the incision, where it is easier to find. Avoid dissection. Insert a self-retaining retractor or two small retractors. Push up the peritoneum. Insert two traction stitches with big bites on either side of the anterior aspect of the bladder. In case of doubt, aspirate to make sure this is the bladder Stab with the knife between the two stitches and grasp the bladder edges with two Allis forceps. Palpate inside the bladder for tumour or stone. Insert a large Pezzer catheter (CH 16 or bigger) and close the bladder with 2/0 Vicryl around the catheter. Close the fascia. Interrupted sutures on the skin on either side of the Pezzer catheter. Fix the catheter to the skin with a strong stitch (braided 0 for example). Dressing and sterile bag attached to the catheter. 128 Suprapubic catheterization procedure Equipment - Povidone iodine Sterile gauze swabs 1 table towel 1 sterile fenestrated towel 1 sterile gallipot 1 suturing set 1 pair of sterile surgical gloves 1 IM needle (green) and / or 1 spinal needle 1 suprapubic catheter placement kit 1% lidocaine without adrenalin 20 cc syringe (one) n° 0 non-absorbable suture material (one) bottle for urine analysis 129 1- Mark the aspiration spot 2 finger-breadths above the symphisis pubis. 2- Don surgical gloves 3- Paint with Povidone iodine 130 4- 5- Drape with sterile towel Inject the LA (1% Lidocaine without adrenalin) with the IM needles or the spinal needle ( according to the patient’s size) Insert the needle at a right angle until urine is aspirated. Do not insert catheter if there is no urine. 131 6- Wait for LA to act 7- Place the catheter into the trocard (don’t go beyond the tip) 8- Make a short incision with n°11 knife (insert the blade fully) 9- Insert trocard at a right angle until urine comes out 132 10- Insert catheter into bladder as far as possible 11- Withdraw the introducer (trocard) 12- Fix catheter to the skin 133 13- Save urine for routine urinalysis 14- Connect to urine bag. 15- Apply a sterile dressing, avoiding kinking of the catheter. 134 The abdomen Phimosis – Paraphimosis (Chapter 11.4) Phimosis (failure to retract the foreskin or prepuce) has two possible complications: Paraphimosis which is the result of failure to pull the foreskin cover the glans (in case of loose phimosis). Oedema develops at the level of obstruction (under the glans penis) and it becomes impossible to cover the glans again. Oedema makes obstruction even worse and may lead to glans necrosis. It is an emergency. Infection, with pus formation under the foreskin. Infection often subsides with simple bath but may require emergency intervention. Antibiotics are not required except in rare cases of extensive penile infection associated with fever. Two possible procedures: Circumcision (removal of the foreskin); may also be performed for religious or ritual reasons. Dorsal slit, very easy, makes it easier to pull back the foreskin without removing it. Both can be done under local anaesthesia but circumcision is more comfortable under general or spinal anaesthesia; local anaesthesia changes the contours of the foreskin and may increase bleeding. Equipment - Fenestrated sterile towel. One pair of gloves for surgeon and assistant. Instrument set with: knife needle-holder non-toothed dissecting forceps scissors 2 small forceps - Suture material: ideally 3/0 Vicryl (or Chromic). 1 – Dorsal slit: slide the scissors under the dorsal part of the prepuce (to avoid the artery of the frenulum), between glans and foreskin. Cut. Most often there is no bleeding and suturing of the mucocutaneous layer with quick resorption material is enough (2/0 Chromic). 135 2 – Circumcision must be done carefully - Paint penis and glans after retraction with disinfectant.(B) - Bring the foreskin back over the glans and pull slightly on it. - Cut the skin over the glans with scissors, while the assistant pulls back the penile skin ©. - Make a circumferential incision of the mucosa about ½ cm from the corona (going back slightly at the ventral part).(E) - Ligate and cut the artery of the frenulum with 3/0 Vicryl on the ventral aspect of the corona (G); control bleeding carefully, the only complication being haematoma. - Cut redundant skin and mucosa, until the previous incision of the mucosa is met. - Check bleeding. - Approximate the cut edges with interrupted suture (Vicryl 3/0), without twisting. Use loose interrupted suture, it must not be water-tight. - Tied-over dressing or no dressing at all (F). No postoperative care is necessary, the only risk is haematoma within next few hours. Infection is very rare. Paraphimosis: always try manual reduction by compression, then return the foreskin over the glans. If successful, oedema will subside within a few hours. Otherwise, release the obstructing ring with diathermy with or without dorsal split. Interval circumcision is recommended. Infection: if there is no fever and infection is limited to the foreskin, try bath with a disinfectant solution. Otherwise, make an urgent dorsal slit. Interval circumcision is recommended 136 The abdomen The perineum; perianal area (Chapter 9.2) Clinical examination Anal fissure Diagnosed on history (acute pain during defecation and for half an hour following it) and on examination (little crack on the posterior side of the anal margin, sometimes hidden behind a sentinel skin tag). But examination may be painful and must be repeated under anaesthesia. If a medical diet for soft stools does not succeed, a simple anal stretching under general anaesthesia, gradually with two or three fingers, may be enough. In case of recurrence, or residual chronic fissure, refer him for more radical surgery (excision and sphincterotomy or sphincteroplasty). 137 Prolapsed haemorrhoids Try to reduce, give PO metronidazole, and surgery later. Acute thombosed piles Signs: Acute pain with bluish, tender, fixed anal swelling, making sitting or defecation painful. Treatment: If there is one or two localized thrombosed haemorrhoids, make an incision under general or large local anaesthesia on top of the pile and dislodge the clot without leaving anything behind (use a curette). If there is numerous thrombosed haemorrhoids, with circular oedematous prolapse, don’t try multiple thrombectomy or radical haemorrhoidectomy. Sooth the patient with warm bathes and pain killers. Refer him in case of failure. Notes • Due to acute local pain, it may be difficult to distinguish between anal fissure, internal pile thrombosis and early anorectal abscess. In these cases, an examination under general anaesthesia is necessary. • The elective radical operation for uncomplicated piles is not that easy. There is no emergency, so refer the patient for it. Prolapsed haemorrhoids (top), thrombosed heamorrhoids (bottom) 138 Anorectal abscess; fistula-in-ano Surgery has two goals: 1. Relieve the patient’s symptoms and stop the infection process. 2. Look for a fistula between the abscess and the anorectal canal. The cause of the abscess is a primary infection inside the anal canal, on the “pectinate” line or ”dentate” line, spreading secondarily through the anal (or rectal) wall up to the subcutaneous space; there it may burst spontaneously unless it is treated surgically. 3. Treat the fistula only if a track is present and if you are sure it is a superficial (infrasphincteric) fistula. Clinical signs and indication for surgery Acute, throbbing pain severe enough to keep the patient awake, fever, local tense swelling with or without fluctuation are sufficient. Rectal examination is usually impossible without anaesthesia because of the pain. Always operate under general (or spinal) anaesthesia, in lithotomy position. Start by examining the anorectal canal Insert one then two fingers without dilating the anus. Look for pus discharge revealing the internal orifice of the fistula. Put one or two retractors in the anus (or better: an anal bivalve retractor) and have a look around all over the pectinate line. If the internal orifice can’t be located with these manoeuvres, puncture the top of the abscess up to its centre and aspirate pus to confirm the collection and its site, and to order a culture. Keeping the needle steady, inject 10 cc of air or blue colouring while looking for bubbles or blue drops at the internal orifice of the fistula. Whatever you find go to the next step: Incise and explore the abscess Use the routine technique (see above). Keep especially in mind two possible extensions of the abscess: 1. Up through the levator ani muscle, up to the infraperitoneal space (collar-stud abscess) 2. Back, up to the midline and even through it up to the opposite side (horseshoe abscess) 3. Inwards: going back the blue coloured track of the fistula, and exploring that track with your finger then, quite gently, with a smooth curve instrument, searching for an opening into the anal canal. Caution! Do not insist with that instrument, you risk perforating the anal mucosa and creating a second fistula (while ignoring the first one!). If you don’t find easily the track, give up! Drainage and postoperative care • If there is no fistula, treat as in general case. Tell the patient he may suffer again from a new abscess or a chronic fistula (refer). • If there is a fistula, assess it by passing a probe through it and palpating the tissue over that instrument. If that tissue is thin (less than 5 mm) and does not contract when applying electro-diathermy, you can divide it, laying open the fistula. If the tissue is thicker, assume it contains the anal sphincter, just incise the skin and the anal mucosa between the internal orifice of the fistula and the incision, and replace the director by one thick non-absorbable ligature, loosely tied around the sphincter. Later (but not before two weeks) you or a proctologist will have to replace that thread by an elastic band slightly tightened every week, cutting through the sphincter gradually. 139 140 The abdomen The scrotum (Chapter 9.3) Hydrocele; epididymo-orchitis; testicular torsion Hydrocele (fluid around the testis) Common, the only treatment is surgical; it is not painful or dangerous, so surgery should be offered only when the patient is troubled by the volume of the scrotum. The surgical treatment is easy but most be done carefully to avoid the one postoperative complication: scrotal haematoma, which may be bigger than the initial hydrocele. The diagnosis is clinical and easy in the face of: Large, regular scrotum, irreducible, testis cannot be palpated. In children the cause is patency of the processus vaginalis, which can be associated with a congenital hernia. In case of doubt: US scanning will easily show the hydrocele as a fluid-filled mass with the testis on one side. Needle aspiration will draw a straw-colour fluid (like urine) but should be avoided because of the risk of infection. Differential diagnosis: Scrotal hernia, which is softer, reducible (at least partially), the testis is palpable. Elephantiasis, where the skin is thick, infiltrated, sometimes even card-board-like (cannot be pinched between two fingers). Two surgical techniques (adults): Eversion of the tunica vaginalis (Jaboulay’s procedure), the safest. To be preferred to: Resection and placation of the tunic vaginalis (Lord’s procedure), preferred in case of thick wall. Two complications : Intra-operative: injury to the cord. Post-operative: scrotal haematoma. Anaesthesia Spinal anaesthesia is best. Or general anaesthesia. Installation Patient supine. Skin preparation must include the penis (not alway easy when the hydrocele is very big) and the lower aspect of the scrotum (which must be lifted by the assistant with a sponge-holding forceps during skin preparation until the towel has been placed underneath). Prepare a narrow field (the penis can be covered) with 2-4 towels. When the hydrocele is large, prepare for suction. 141 Transverse incision over the anterior aspect of the scrotum, with the assistant stretching the skin with his hands. Dissect layer by layer until the bluish layer of tunica vaginalis has been reached, trying not to enter it. Remove the fluid with a small stab incision of the tunica vaginalis, then grasp the edges with two tissue forceps (the assistant must release its tension then!). The fluid is typically straw colour but may be turbid, sometimes even brown when the wall is thick. Once the hydrocele fluid has been removed, bring out the testis after enlarging the tunica opening. Check the testis. Jaboulay’s operation = eversion of tunica vaginalis First choice but possible only when the tunica is soft. The idea is to evert the tunica vaginalis and resuture it behind the testis, with interrupted 3/0 absorbable (chromic) stitches. Two precautions: - identify and protect the cord, - do not strangulate the cord or leave a gap leading to recurrence. Always check for bleeding and add if necessary small figure-of-eight 3/0 Vicryl stitches. Drainage Not compulsory if there is no bleeding at all. More often when tunica has been resected the risk of bleeding is higher. Insert a corrugated drain through a stab incision at the lowest spot; fix it with a large non absorbable stitch Closure Do not remove skin, even for a large hydrocele. The subcutaneous layer is closed with a continuous 2/0 absorbable suture taking big bites of all the layers. The skin is closed. In any case (even if there is a drain), apply a criss-cross dressing i.e.: - several gauze swabs over the operated scrotum, - compressive dressing with Elastoplaster: two strips going from the iliac crest up to below the opposite thigh after crossing under tension over the scrotum. - remove the dressing the same evening or the following day (if tight it may prevent micturation). Postoperative period Usually uneventful, mobilization as soon as the effect of spinal anaesthesia is over. If there is a drain, mobilize it the following day, and remove it by the 3rd or 4th day. Sutures removal on day 8 or 10. In case of haematoma, wait for spontaneous absorption if not too large. Otherwise it must be evacuated surgically. The patient can be discharged on the 2nd day if there is no problem. Avoid this operation in children: identification and closure of the sac may be difficult. Refer. 142 Epididymo-orchitis Bacterial infection of the epididymis of prostate origin. The infection goes along the vas deferens from the prostate to the epididymis. The prostate infection may go un-noticed but there may be a history of: recent unexplained fever, burning micturation recent frequency. The clinical diagnosis is easy most of the time: unilateral scrotal swelling, inflammation, often with high fever > 39°C (except when antibiotics were taken blindly) physical examination is not very reliable, as tenderness and oedema prevent palpation of the epididymis. The only possible mistake is to miss a testicular torsion, therefore, in the absence of signs of infection, any scrotal pain requires surgical exploration because it is better to explore a scrotum unnecessarily than risk loosing the testicle. Urine analysis when available. Antibiotics target the most common agent, Escherichia Coli. The treatment must last 3 weeks to treat both epididymitis and prostatitis. Teat according to national protocols for STDs. Avoid penicillin / ampicillin – Augmentin and β lactamines poorly active on Gram (-) germs. Aminoside injections may be used. Progress is slow and even though the fever ususally subside within 2-3 days, it may take 3-4 weeks for the clinical findings to go back to normal. There may be residual nodules, without significance. Cause: recent instrumental manoeuvre: bougies or catheter, to be investigated in case of recurrence: mostly urethral stricture seen on cystoscopy or retrograde urethro-cystogramme or IVP, often unidentified. Special cases: TB epididymitis: mild pain, no fever, but significant changes to the epididymis without signs of infection. The diagnosis is based on identification of AAFBs in urine; when possible, an IVP should be done looking for infection of the upper urinary tract because ‘TB goes down the urine stream, and goes up the sperm stream’ the kidney infection always precedes the epididymal infection. Subacute epididymitis, difficult to diagnose and treat, either because the cause is intra-cellular germs (Chlamydiae), or because antibiotics have already been given. 143 Testicular torsion A misnomer: the cord gets twisted, not the testicle! It is an emergency that cannot suffer any delay, as the testis can get gangrenous within a few hours. The history is usually typical: At any age, but more common in children and young men (10- 30 years). Severe, acute, sudden scrotal pain, without causing factor and no infection (no fever, no burning micturation, no urethral discharge). Clinical examination is often un-necessary (the diagnosis is obvious) and impossible (severe tenderness). Just check that inguinal lymph nodes are not enlarged. Sometimes there can be doubt after testicular trauma, epididymo-orchitis complicating a missed prostatitis, or a scrotal abscess. Therefore, any acute testicular pain without infection must lead to surgical exploration. It is better to operate un-necessarily for an atypical epididymitis than to miss an atypical torsion. 144 Surgical technique Surgery is quick and easy. Short general anaesthesia to be preferred to spinal anaesthesia. Installation: - Supine, paint penis and scrotum with disinfectant. - Drape scrotum only with 2-4 towels. Incision: - Scrotal, horizontal. - On opening the tunica vaginalis, you may encounter clear (in case of torsion or infection) or bloody fluid (in case of trauma). Procedure: - Bring out the testis. - If the epididymis is swollen and inflammed with a normal looking testicle, this is epididymitis put the testis back and close. Give antibiotics (2nd generation Quinolones for 3 weeks or Bactrim). - If the testicle is bluish, ischaemic and the cord is twisted one or more times, it is indeed torsion. Then: Detwist the cord. Allow the testis to go back to its normal colour (with warm saline). Fix the testis to the septum with 3 non-absorbable stitches (e.g. 4/0 Prolene) taking testis and septum (in normal position!). Subcutaneous layer with 2/0 Chromic or 3/0 Vicryl. Skin closure with interrupted 3/0 Vicryl (or non absorbable or skin clips). - If the testis is black, obviously gangrenous or doesn’t go back to normal after detorsion, it must be removed (the patient should have been informed of the possibility before-hand): Separate the structures of the cord carefully. Put a double ligature on each of the two cord structures with a ‘large’ ligature (n° 0 Vicryl or Chromic without needle). Cut the cord and remove the testis. Subcutaneous layer with 3/0 Vicryl or Chromic without drain. Skin closure with interrupted 3/0 Vicryl or Chromic (or non absorbable or skin clips). Postoperative period Haematoma is rare. Remove skin sutures after 8 – 10 days. If there was torsion, plan orchidopexy of the opposite testis next month. Key points Careful haemostasis for hydrocele operations. Symptoms of testicular torsion are typical. Explore the scrotum urgently in any suspicion of testicular torsion. 145 146 TRAUMATOLOGY AND ORTHOPAEDICS 147 148 Traumatology and Orthopaedics Principles of Primary Trauma Care A, B, C, D, E Procedures Chest injuries Head injuries 149 150 Traumatology and Orthopaedics Principles of Primary Trauma Care (16.2) Primary Survey: A, B, C, D, E A: Airway B: Breathing C: Circulation D: Disability E: Exposure Secondary Survey: head to toe examination. Head: Scalp, eyes, ears, mouth Neck: Tenderness, tracheal deviation, JVD Chest: Breath sounds, tenderness, crepitus, dullness, hyper-resonance Abdomen: Tenderness, masses, distention Pelvis: Instability, blood at meatus Extremities: Pulses, neurologic exam, fractures 151 Airway Is the airway free? If the patient is talking, the airway is free. If breathing is noisy or absent, use the following measures in that order: -Extend the neck and lift the jaw forwards. -Suck out the mouth. -Remove pieces of vomit or foreign bodies with your finger. -Insert an oropharyngeal airway. -Intubate the trachea (if you know the technique), especially if the patient is unconscious. -Create a surgical airway through the cricothyroid membrane (see procedure) Breathing (ventilation) The airway being clear or cleared, is the patient breathing? Look at the chest movements. Auscultate the chest for air entry. If it is normal, give oxygen. Otherwise, ventilate the patient with Ambu-bag and oxygen. 152 Circulation Positioning the patient Tilt the patient head down if possible or raise the legs so that most of the blood will go to the most important organ, the brain, which is very sensitive to ischaemia. Controlling external bleeding If there is obvious severe external bleeding, start by applying firm pressure on the bleeding part with your gloved fist and a pack and keep pressing as long as it is bleeding. Raise a bleeding limb; this will lower the venous pressure and reduce the bleeding. Applying a tourniquet to a limb is permitted as long as the patient can go to theatre immediately. This is not recommended for first aid at the scene of an accident, pressure is prefered because of the ischaemic complications of tourniquet. Is the heart beating? If there is no heart sounds on auscultation and no carotid pulse, start cardiopulmonary resuscitation: Continue to support ventilation and give oxygen. Start external cardiac massage (see technique in skills practice). Give 1 mg of adrenalin IV, repeat if necessary. Emergency IV access In case of hypovolaemic shock, the most common type of shock in surgical practice, it is essential to get urgent IV access because the body response to hypovolaemia is by vasoconstriction; the veins will rapidly get collapsed and become very difficult to cannulate. Peripheral vein cannulation You need a secure, reliable IV access. If available, use the biggest cannula you think you will be able to insert. Draw blood immediately for blood grouping if it is a case of haemorrhagic shock: you will save time and will not have to find another vein to draw the blood. Send it to the laboratory for urgent blood grouping and request blood at the same time (at least 2 units for an adult). Secure your cannula well. Splint the arm of children or restless patients, they may have no other usable vein and you don't want to lose it. If possible put up 2 IV lines which offer more security in case one of them is pulled out or get tissued. 153 External jugular vein cannulation This is an easily accessible vein, which can be used in shocked patients whose peripheral veins are collapsed or in children with difficult veins. Tilt the patient head down and ask someone to press on the root of the neck just above the clavicle to make the vein more visible. Connect a syringe to the cannula to aspirate the blood because it can be under negative pressure. The disadvantage of this site is that the rate of infusion varies with the position of the head. You may have to keep the head turned to the other side to allow good flow. Central vein cannulation In desperate cases, even if you don't have central catheters, you can try to cannulate the femoral vein or the subclavian vein with a large IV cannula. Cutdown Cutdown to the long saphenous vein or one of the superficial veins of the cubital fossa can also be very useful in difficult situations. Note on laboratory tests: haematocrit is not a useful emergency test in case of acute haemorrhage as red cells are lost in equal proportion to plasma and the haematocrit is initially normal. Only after compensation by fluid shift from the intracellular compartment will it be lowered. Infusion fluids Give IV crystalloids (eg normal saline) as fast as it will go. In case of haemorrhagic shock, give blood as soon as it is available if indicated. Keep the patient warm. Monitor the patient's response You are looking for a reversal of the signs of shock: extremities must warm up, consciousness must improve, ventilation rate must decrease, BP must pick up, pulse must slow down, and urine must be passed: the urine output should be at least 0.5 ml/kg/hour. If he is not responding to fluid replacement, suspect a missed injury. Re-examine him. 154 155 Chest trauma Look: - rate and depth of the breathing - paradoxical movement (flail chest) - distension of intercostal spaces (tension pneumothorax) - cyanosis - bruises or wounds (don’t forget to look at the back). Feel: - tenderness - crepitus (rib fracture) Surgical emphysema (air in the soft tissues) - surgical emphysema . Percuss: Dullness (haemothorax) or tympanism (pneumothorax). Listen: Reduced or absent air entry, suggesting pneumothorax, haemothorax, or lung collapse. 156 Also examine the abdomen because of the frequent association of rib fractures with splenic (left side) or hepatic (right side) injuries. X-rays, when available are useful may must not delay emergency measures (needle insertion for a tension pneumothorax, insertion of a chest tube). The majority of patients with thoracic trauma can be managed by simple manoeuvres and do not require surgical treatment. Simple pneumothorax: air in the pleural cavity The affected side is hyper-resonnant on percussion and air entry is reduced. On X-Ray: the lung markings do not reach the edge of the thoracic cage. Chest drainage is indicated when: - there is dyspnoea; - the apex of the lung is about 3 cm below the top of the pleural cavity; - the patient is going to need general anaesthesia for another injury: ventilation can convert a simple pneumothorax into a tension pneumothorax. Open pneumothorax or ‘sucking’ chest wounds Air is sucked into the pleural cavity every time the patient breathes. As a first aid, occlude the wound immediately with any available dressing or a plastic sheet. Then insert an intercostal chest drain and proceed to close the wound, if possible under local anaesthesia: wound toilet, debridement if necessary; then close pleura, muscle and skin; check that there is no air leak. 157 Tension pneumothorax: air under tension in the pleural cavity. Develops when air enters the pleural space but cannot leave. The consequence is progressively increasing intrathoracic pressure in the affected side resulting in mediastinal shift. The patient becomes short of breath and hypoxic. There is severe chest pain, increasing dyspnoea and sometimes cyanosis; the chest is hyper-resonant with poor respiratory movements and absent breathing sounds. The trachea and the apex beat are deviated to the other side. Don’t wait for X-Rays! This is a real life-threatening emergency and immediate treatment is required. Urgent needle decompression is required prior to the insertion of a chest tube. The trachea may be displaced (late sign) and is pushed away from the midline by the air under tension. Emergency treatment: insert a large needle in the 2nd intercostal space in the midclavicular line to let the air out of the pleura. This will considerably improve his breathing and you can then insert a chest drain as usual. Haemothorax: blood in the pleural cavity. Hypovolaemic shock and respiratory distress may be present. There is chest pain, dullness to percussion and reduced breath sounds on the affected side. X-Ray, when available, shows a diffuse opacity but may be difficult to interpret. If you are in doubt, do a needle aspiration of the chest before draining the chest. In fresh, closed haemothorax, you can use the blood for autotransfusion by collecting it into a bloodcollecting bag. The complication of undrained haemothorax is clotting of the blood, preventing the lung from re-expanding, and very difficult to treat. Rib fractures The ribs spontaneously become stable within 10-15 days. Pain control is important to allow easier ventilation. Nothing else is necessary. Flail chest: two or more ribs fractured at two different sites The unstable segment moves separately and in the opposite direction from the rest of thoracic cage during the respiratory cycle (‘paradoxical breathing’). Severe respiratory distress may ensue. 158 Pulmonary contusion A potentially life threatening condition. The onset of symptoms may be slow and progress over 24 hours post-injury. It is likely to occur in cases of high speed accidents, falls from great heights and injuries by high-velocity bullets or missiles. Symptoms and signs include: dyspnoea (shortness of breath), hypoxia, tachycardia, rare or absent breath sounds, rib fractures, cyanosis. Oxygen therapy is essential. Key points Check all trauma patients for chest injury. Take emergency measures if X-Ray is not available or is delayed. Deflate a tension pneumothorax urgently by needle insertion. Have a chest drainage set always ready to drain any significant pneumothorax or haemothorax. 159 160 Traumatology and orthopaedics Procedures (Chapter 16.3) Chest drainage; cricothyroidotomy; diagnostic peritoneal lavage Chest drainage Indications Pneumothorax (see above). Haemothorax. Haemopneumothorax. Acute empyema. Technique Always have a chest drain set ready in your hospital. The method commonly used is the underwater-seal chest drainage. If you have no special chest drain, use any large sterile tube such as a gastric tube or a large rubber tube on the sides of which you will have cut holes, and lead the tubing under the surface of the water. Make an incision under local anaesthesia in the 4th intercostal space (nipple level in a male patient), at the upper border of a rib, anteriorly to the midaxillary line (fig 1 and 2). Fig 1 Fig 2 161 Enlarge the opening with forceps (fig 3-4), insert the tube (fig 5) and fix it to the chest wall (fig 6); insert a purse-string suture for easier removal later (not shown) Fig 3 Fig 5 Fig 4 Fig 6 Connect to under-water system bottle (fig 7) Fig 7 Important points - do not puncture the lung by forceful use of the trocard - secure the drain well, as accidental removal may have serious consequences - get a control X-Ray after insertion - monitor the drain frequently: presence of the tube tip in the chest cavity is indicated by the swinging of the fluid level. The water in the bottle prevents air from coming up into the pleura. 162 Cricothyroidotomy A cricothyroidotomy is a surgical airway, which can be necessary in case of obstruction. Severe hypoxia from obstruction of the airways can occur in case of: • Head injury in unconscious patients • Severe neck injury with laryngeal trauma • Face injury. • Burn injury to the face or the respiratory tract • During the postoperative care of patients after neck surgery. It is usually easy to detect the obstruction of the upper airway. The patient cannot have free breathing or no breathing at all. He becomes cyanosed. It is an extreme emergency, therefore: • Have the various steps clear in your mind; • all the equipment: o tracheostomy set o cannula o oxygene o suction apparatus must be always kept in the same place, at hand, ready for use; everybody in the Operating Theatre must know about the equipment, which ahs to be checked and sterilized at least once a month. Surgical setup Except in cases of trauma or compression, when you have the possibility of inserting a tracheal tube without wasting time, you may try it. You may also immediately insert a large-bore needle or cannula into the trachea below the cricoïd cartilage; this can improve temporarily the patient and give him some air while you get ready for crocothyroidotomy The procedure is quick and simple. Local anaesthesia, when necessary, may be given. A pillow is placed under the shoulders, head and neck are extended (fig 1). Give oxygen through mask until the last seconds. Have suction ready. 163 Surgical technique Stand on the patient’s right side. Feel for the thyroïd cartilage with your right index, then maintain it between left thumb and middle finger placed on either side of the cartilage. Remove the index and incise the skin and the subcutaneous layer until the space between the thyroïd and cricoïd cartilages. The incision can be transverse or vertical midline and should not be too long (fig 2). Place the tip of your index in the incision to prevent bleeding (fig 3). Fig 2 ig3 Incise transversely the membrane until air comes out: take the tracheal dilator (if you do not have, any short, curved forceps will do). Open it and extend the opening (fig 4). Do not dissect. Fig 4 164 Insert the cannula in horizontal position, at a right angle to the trachea. Push it and rotate it downward (Fig 5). Push again along the curvature of the cannula and insert it fully. Fig 5 When inserting the cannula, breathing sounds must be heard. If not, it means that it is not in the proper place, may be in the subcutaneous layer in front of the trachea; take it out and try again. Suck out secretions and blood clots with a soft tube. Fix a tape around the neck (Fig 6). Suck out again. As soon as possible give O2 to the patient through the new airway. Fig 6 Follow- up: intensive care is mandatory to prevent complications Oxygen as needed. Humidify the air if possible. A wet gauze may be placed over the tube. Avoid obstruction of the cannula. Suck out secretions on a regular basis but not too often, using sterile material. According to the cause, the patient may have to be referred if safe to do so. Difficulties: In a life-threatening emergency, even when you have no cannula, any tube can do. The size of the cannula is the same as his little finger. The incision must be short, not much longer than the size of the tube. 165 Diagnostic peritoneal lavage (DPL) This is a safe and valuable technique in abdominal trauma when positive; but a negative result doesn’t rule out a visceral injury. Contraindications: • Pregnancy • Previous abdominal surgery (because of possible adhesions) • When the result will not influence your management. Technique Make sure bladder and stomach is empty. If in doubt, insert a catheter. Infiltrate the abdominal wall and the peritoneum below the umbilicus with a local anaesthetic (with adrenaline if available, to reduce abdominal wall bleeding) (Fig. 1). Make a 2.5 cm midline incision below the umbilicus (Figure 2). Fig 1 Fig 2 166 Lift up the fascia with two stay sutures and make a 3–5 mm incision through the fascia (Figure 3). Gently introduce a large catheter on an introducer into the peritoneum and push the catheter into the pelvis (Figure 4). You also can use a cannula, a soft probe, or a gastric tube. Spontaneous reflux or gross aspiration of blood or intestinal liquid is sufficient to make a decision. Fig 3 Fig 4 Fig 5 Fig 6 If there is no fluid reflux, infuse 1 litre of saline rapidly through the catheter (Fig 5). Attach the catheter to a closed container and place it on the floor (Fig 6). About 100 ml of fluid should flow back into the container. Interpretation When laboratory examination is available, ask for a red and white cells count and microscopic examination for bacterias. More than 100,000 red cells per ml indicate abdominal bleeding; if white cells are greater than 500 / ml, consider there is a damaged organ. Presence of bacterias is a sign of intestinal perforation and of the need for a laparotomy. When laboratory examination is not available, check the clarity of the fluid. If you cannot read “newsprint” through the red-stained fluid, there is a haemoperitoneum; if the fluid is cloudy due to presence of material, it is likely that there is a bowel injury and therefore laparotomy is indicated. 167 168 Traumatology and orthopaedics Head injuries (Chapter 16.2) On admission apply the ABC primary trauma survey. Get history of the trauma. Admit when criteria for 24-hour admission and observation are present. Specific examination and management Initial and repeated assessment of the level of consciousness by the Glasgow Coma Scale (GCS) is essential Glasgow Coma Scale Eyes opening 4 3 2 1 Spontaneously To speech To pain None Best verbal response 5 4 3 2 1 Orientated Confused Inappropriate words Incomprehensible sounds None Best motor response 6 5 4 3 2 1 Obeys command Localises pain Withdraws to pain Flexes to pain Extends to pain None Minimum score: 3 / 15 Maximum score: 15 / 15 Patients with GCS below 8 are generally considered to have severe head injuries. Many patients will recover with attentive supportive care. 169 For all severe head injuries, also assess: Size and reactivity of pupils Motricity of limbs Presence of blood or clear fluid (CSF) coming from ears or nose (suggest basal skull fracture). X- Rays (when available): - X-Ray the cervical spine for all significant head injuries. - AP, lateral right, left and special views of the skull are useful in some cases (see criteria for skull radiology in annex). Neurological assessment Secondary brain injury means that symptoms not present when the patient arrived appear after a few hours or days. The “free interval” after head injury I initial loss of consciousness II conscious state III deterioration or coma - Deterioration of level of consciousness. - Pupil dilation on the side of injury; controlateral motor weakness. The association of deterioration of level of consciousness and new neurological signs means haematoma (fig1-2 and photo) and is characteristic of a space-occupying lesion such as extradural haematoma, and is an indication for emergency surgery: burr-holes, craniectomy, release of haematoma. 170 When neurological symptoms are present from presentation, it is difficult to say whether the cause is primary brain injury or secondary brain injury such as haematoma (which may be associated with brain injury). In your circumstances, we advise transfer whenever possible. The wound When the wound is significant, with bone fragments and hair inside, do a thorough wound toilet, remove obviously damaged or prolapsed brain matter and close the wound (if possible the dura, otherwise only the skin). Give chloramphenicol + penicillin. General management Prevent hypoxia and hypovolaemia but do not overload. No 5% dextrose. No steroids! Nurse in lateral position because of the risk of aspiration. Seizure prophylaxis in all severe head injuries (phenobarbitone). Treat seizures with IV diazepam. In case of CSF leak through ear or nose, nasal bleeding, ear bleeding, open skull fracture: antibiotics are mandatory to avoid meningeal infection: chloramphenicol + penicillin. Key points ABC of acute rauma care Assess GCS, pupils and motricity on arrival. Prevent gastric fluid aspiration, hypoxia, hypovolaemia, seizures. No steroids. No 5% dextrose Re-assess frequently. 171 Fig 1: left extradural haematoma; right: subdural haematoma Above: ‘jelly’ of an extradural haematoma 172 Fig 2: intracerebral haematoma Criteria for skull radiology in head injury History of loss of consciousness Scalp laceration or contusion Palpable depression Suspicion of compound fracture Criteria for 24-hour admission and observation after head injury History of loss of consciousness Alteration of level of consciousness (GCS 14 or lower) Fracture on skull X-Ray Any abnormal neurological sign Seizures CSF leakage for ear or nose Bleeding from ear or nose No responsible adult to take charge of the patient 173 174 Traumatology and Orthopaedics Fractures and dislocations 175 Traumatology and orthopaedics General principles of fractures and dislocations Definitions; principles of treatment; open fractures; conservative management; complications Fractures general principles. 2006 1 Definitions • Fracture: broken bone; may be complete or incomplete. • Sprain: ligament injury without loss of contact of the joint surfaces. • Dislocation: complete rupture of all the ligaments with loss of contact between the joint surfaces. • Union: incomplete repair. • Consolidation: complete repair. 2 Approach to orthopaedic trauma patient ABCDE of acute trauma management Timing and mechanism of injury. Look (deformity, swelling, wound) Feel getly for tenderness, deformity Move very gently for tenderness, restriction of movements. Look for complications. Immobilize and get X-Rays (when available 3 X-Rays in orthopaedic trauma (when available) Anteroposterior and lateral views. • Centered on the suspected area. • Must show the whole bone and the joints proximal and distal to it. • Type of fracture, quality of bone, displacement. • When in doubt, X-Ray opposite (normal) side in children. 4 176 Fracture mechanisms • Direct trauma Usually transverse fractures with soft tissues injury. • Indirect trauma, twisting injury Spiroid or oblique fractures (short or long) • Pathological fractures Minimal trauma, occuring on infected or tumoural bone 5 How to describe a fracture • Bone, and part of bone involved (shaft, distal, epiphysis) • Open or closed. • Complete or incomplete. • Displaced or not displaced. • Type of fracture: transverse, oblique, spiral, comminuted. • Articular, partial articular or extraarticular. 6 Transverse fracture (left); wedge fracture (right) • 7 Spiral fracture Rotational displacement (left); segmental fracture (right) 8 177 Comminuted fracture Direct trauma. A wound is common. Soft tissues injury to muscles, vessels, nerves 9 Articular fractures Metaphysis and epiphysis fractures Complications: restriction of mobility, early or delayed osteo-arthritis, algodystrophy, non union 10 Fracture displacements Sideways shift Shift with overlap Rotation 11 Impacted fractures Stable fractures. Conservative treatment with no need for manipulation. Examples: Colles’ fracture, femoral or humeral neck fracture (below), spine (right) 12 178 Principles of treatment of fractures and dislocations Reduce (when necessary) Hold until it unites (using one of different methods). Exercise (muscle activity and early weightbearing). 13 Conservative treatment • The most common management. • When manipulation is necessary, it must be done early, under anaesthesia and correct alignment must be obtained with contact of the 2/3 bone surface. Rotation must be corrected. • Stabilisation by POP cast or traction. • If reduction is not obtained, refer. 14 Surgical treatment Compulsory for open fractures. But not to be used in your circumstances for closed fractures. 15 179 Open fractures • Fractures with a wound communicating with the fracture. • The major risk is infection. • The risk is greater in contaminated wounds and with delay since injury. • After 6 hours, consider the fracture as infected. 16 Open fractures: classification Grade 1: small wound with clear cut edges, no contusion of soft tissues. Grade 2: wound is more than 1 cm with no skin flap, not much soft tissue damage. Grade 3: extensive damage to skin and soft tissues with contamination of the wound. Grade 1 Grade 2 Grade 3 17 Principles of open fractures management • Urgent wound toilet under anaesthesia. • Bone stabilization by traction, cast, or external fixation. • Tetanus prophylaxis. • Start antibiotics early and continue for a minimum one week. 18 Wound toilet for open fractures • Irrigate with at least 3 litres of boiled water. • Excise skin edges minimally. • Check muscle 4 C’s: colour, consistency, contractility, capacity to bleed and excise dead mucle. • Leave cut nerve undisturbed. • Leave cut tendon ends alone: suture only if totally clean. • Only remove small and completely detached bone fragments. • Look for and remove any foreign bodies. • Reduce the fracture. 19 180 Wound closure for open fractures • Only grade 1 open fractures with very small, very clean wouinds and seen early may be closed primarily. Immobilize with a cast with a window or a plaster back-slab. • Delayed primary closure must be used for all other injuries, apply a large American dressing on the opened wound, plan DPC after 3-4 days under anaesthesia. Apply a cast with windom, a back-slab or traction as appropriate. 20 Options for immobilization of open fractures • Circular Plaster of Paris cast with window. • POP backslab. • Or skeletal traction. 21 Grade 2 open fracture of the distal leg suitable for calcaneal traction (here treated by external fixation) 22 Grade 3 open fractures may require amputation Immediately: major injuries, irreversible ischaemia, limb beyond repair (right) Later: infected bone, gangrene, painful limb that will never be useful. 23 181 Sprains Clinically: Pain Swelling Inability to use the limb. Principles of management: Elastic bandage for 10 days. Analgesics and NSAIDs. 24 Ligamental ruptures Clinically: Haemarthrosis (knee, ankle) Deformity. Principles of management: Immobilize in a cast, or a backslab in case of major swelling. Partial weightbearing with crutches. Analgesics and NSAIDs. Physiotherapy later. 25 Dislocations Clinical diagnosis is often possible when seen early. Reduce early under anaesthesia and immobilize. Analgesics and NSAIDs. 26 182 Conservative management of fractures (17.1) When necessary, manipulate the fracture early or after oedema has subsided, under anaesthesia, and apply cast Fractures general principles. 2006 27 Protect the skin with cotton; include joints proximal and distal to the fracture; immobilize in position of function. Here a back-slab 28 Here a circular cast 29 Always split a circular cast to prevent limb compression and compartment syndrome 30 183 Special plaster casts Walking cast 31 Complications of POP casts • Compartment syndrom • Deep vein thrombosis • Fat embolism • Skin problems • Secondary displacement 32 Skin problems No tight casts, protect the skin with enough cotton and keep the cast dry. 33 Secondary displacement under cast Control X-Rays; gypsotomy correction is possible • Get a control X-Ray after gypsotomy • Complete the cast if the control is satisfactory • New control X-Ray on Day 8 and D 15 34 184 Compartment syndrom: caution! Always elevate the limb Don’t stretch circular plasters Check movements, skin temperature after applying a 35 cast Detect compartment syndrom (leading to Volkman’s syndrom) • Severe pain is the first symptom. • Neurological signs in fingers and in the whole fore-arm. • Vascular signs (oedema) 36 Prevent this! Fixed deformity • Flexed wrist • Extended MP joints • Flexed IPP 37 Treatment of compartment syndrome: Remove the cast and all bandages immediately. Urgent fasciotomy may be necessary. 38 Photo J. Chouteau 185 Tractions: different types 10% of body weight Trans-tibial pin (adults) Skin traction (children) 39 Pin tractions • Pin insertion under LA or ketamine just posterior to the upper tibial tuberosity. •Daily checks: pin site, position of limb, isometric exercises and mobility of other joints. •Position: greater trochanter, midpatella and big toe must be aligned. 40 The 4 stages of fracture healing • Tissue destruction and haematoma formation • Inflammation and cellular proliferation • Consolidation • Remodelling 41 Clinical guide to union and consolidation of fractures • Union is incomplete repair: slight tenderness, the bone moves in one piece, attempted angulation is painful; it is not safe to subject the unprotected bone to stress. • Consolidation is complete repair: fracture site is not tender, no movement can be obtained, attempted angulation is painless; further protection is unnecessary. 42 186 Duration of immobilization of common fractures in days Bone Adults Children under 10 years Clavicle 21 21 Neck of humerus 15 15 Shaft of humerus 60 60 Supracondylar elbow 45 45 Radius and ulna 90 45 Distal radius 45 30 Scaphoid 45 45 Metacarpals 30 21 Phalanx 30 21 Neck of femur 90 60 Shaft of femur 90 60 Tibia and fibula 90 60 Ankle 60 60 Metatarsals 15 15 187 43 Complications of fractures (18.8) 44 General complications Hypovolaemic shock (femur fracture, polytrauma) Infection, gas gangrene (wide debridement, crystalline penicillin) Tetanus (prevent by wound toilet and tetanus toxoid for any wound, even minor). Deep vein thrombosis. Fat embolism 45 Deep vein thrombosis Due to bed rest, hypotension, lack of mobility, trauma. Calf pain on dorsal flexion of the foot; slightly raise temperature; limb swelling; groin pain in caseof pelvic DVT. Life-threatening complication: pulmonary embolism: tachycardia, low BP,polypnoea, chest pain. Prevent by early mobilization and physiotherapy. Treat by aspirin. Late complications: chronic limb swelling, skin problems. 46 Fat embolism Rare but serious. Shock, mental confusion, spots on the skin (petechies), fundoscopic examination. Supportive treatment with oxygen. 47 188 Local complications Vascular injury Compartment syndrom (see other lecture) Bone infection Skin necrosis: blisters, necrosis, plaster pressure sores. 48 Vascular injury Always examine distal pulses. Reduce displaced fractures and dislocations early! 49 Bone infection (open fractures) Acute osteomyelitis Prevention by wound toilet. Treat agressively ! May lead to chronic infection, even more difficult to treat 50 Skin complications: blisters, necrosis, plaster sores When the skin is necrosed, the bone becomes exposed, 51 with risk of infection. 189 Late complications Avascular necrosis (compromised blood supply, neck of femur fractures) Delayed union, non-union Malunion Nerve compression and entrapment Joint instability, stiffness, osteoarthritis 52 Delayed union; non-union Pain on walking Local signs of inflammation: tenderness. Pain and movement on mobilizing the limb. Fracture line still visible on X-rays, very little callus formation. • Delayed union: continue with conservative management. • Refer nonunion for possible surgery. • • • • 53 Nonunion: atrophic (left), hypertrophic (right) 54 Malunion Malunion of distal right tibia 190 55 Regional orthopaedics Upper extremity injuries: shoulder, arm, elbow, fore-arm, wrist (18.1) 1 Clavicular fracture Tenderness with or without abnormal mobility X-Ray confirmation not compulsory Triangular bandage or sling for 5-6 weeks; no surgery. 2 Fall on outstretched hand; the patient cannot touch his chest; typical deformity, easy diagnosis: humeral head anterior, prominent acromion, glenoid cavity feels empty, arm abducted and externally rotated. 3 Anterior shoulder dislocation The humeral head is not in front of the scapula but in the antero-lower position X-Ray may show a fracture of the greater tuberosity or head of humerus (arrow). 191 4 Early complications of shoulder dislocation Axillary nerve palsy (sensory loss at the shoulder) - Brachial plexus injury. 5 Treatment of dislocated shoulder Urgent manipulation Traction on the arm with or without anaesthesia if recent, with counterpressure in the axilla. Collar and cuff for 3 weeks; avoid external rotation. 6 When not displaced, keep in a bandage in neutral position (no rotation) 7 Fracture of the glenoid cavity of the scapula (here with humerus dislocation) 8 192 9 Extracapsular shoulder fractures Fractures of neck of humerus Greater tuberosity fracture 10 Articular shoulder fractures Non-displaced displaced very displaced fracture + dislocation 11 Conservative treatment of shoulder fractures Manipulation under anaesthesia and stabilisation !"!#$ Sling or bandage for 6-8 weeks The major complication is shoulder stiffness. 12 193 Humerus shaft fractures . 13 Humeral shaft fracture Look for radial nerve injury +++ (sensation, wrist drop) Keep the patient’s arm in a sling for 6 - 8 weeks. The weight of the fore-arm will reduce the fracture. 14 Fractures of the distal humerus Metaphysis fractures Lateral condyle fractures Articular fractures 15 Medial condyle fractures Treatment of olecranon fractures Non-displaced fractures: splint the elbow at 90 degrees flexion. Displaced fractures: splint the elbow in extension. 16 194 Elbow posterolateral dislocation Fall on outstretched hand. Inability to move the elbow. Prominent olecranon posteriorly. 17 Elbow dislocation Complications: Brachial artery compresion Ischaemia Radial or ulnar nerve compression Check sensation, motion. Associated fractures: coronoid, medial epicondyle, lateral epicondyle. 18 Elbow dislocation Manipulation under anaesthesia, elbow flexed 90°, posterior counter-traction on arm, anterior traction on forearm POP 21 days + physiotherapy. 19 195 Fore-arm fractures in adults Always complete, most of the time, radius and ulna are broken. When only one bone is broken, look for a dislocation of the extremity of the other bone - isolated fracture of ulna Æ possibility of dislocation of the radial head. - Isolated fracture of radius Æ watch for dislocation of distal radio-ulnar joint 20 Incomplete radius and ulna fracture Plaster cast for 2 months 21 Displaced fracture of radius and ulna: traction, disimpaction, angulation and recovery of initial length with good bone contact. 22 Complications of radius and ulna fractures - Open fractures - Non-reducible fracture - Compartment syndrom - Non-union - Secondary displacement. 23 196 Colles’ fracture • Elderly, fall on the extended wrist • Compression + significant extension • Fracture of distal radius 2.5 cm above the joint; typical deformity. 24 Non-displaced Colles’ fractures: cast 6 weeks. Displaced fractures: manipulation under anaesthesia 25 Position of the wrist joint after reduction of Colles’ fracture • Flexion + ulnar deviation • Control X-Ray • Plaster cast for 6 weeks. 26 Main complication of Colles’ fracture: malunion 27 197 Traumatology and orthopaedics The hand (18.2) 28 Sensory areas of the wrist and the hand Palmar aspect Dorsal aspect Radial nerve (green), median nerve (red), ulnar nerve (purple), medial cutaneus brachialis nerve (brown), musculocutaneous nerve (yellow). 29 Scaphoid fractures Often minimally displaced Plaster cast immobilizing the thumb 2 months 30 Carpal dislocation (lunate); risk of necrosis 31 198 Benett’s fracture-dislocation Proximal fracture of 1st metacarpal bone, extends into the joint, unstable; conservative treatment with the thumb in abduction for 6 weeks 32 Carpo-metacarpal dislocation: urgent reduction and plaster cast for 6 weeks. 33 Documents J. Chouteau Examples of phalangeal fractures The 1st phalanx is often displaced in extension (left): reduce it in flexion; oblique proximal phalangeal fracture (right) 34 Malunion of fractures may cause deformity and disability 35 199 Management of open hand injuries Clinical examination: - Sensation of each finger - Motion of each phalanx. - When in doubt, surgical exploration in OR under LA or GA. If a joint is open, wound toilet under anaesthesia . Tendons may be difficult to identify in large palmar wound with many tendons injured Æ thorough exploration of the wound. . Flexor tendons often retract Æ large incisions are necessary to find the proximal end of the tendon(s). . Splint wrist and fingers in correct position to relax sutures of tendons ‘position of safety of the hand’. 36 Flexor tendon sheaths 37 Tendon avulsions Direct suture Pull out procedure 38 Complications of hand trauma • Osteomyelitis • Arthritis • Tendon sheath infection (may spread to the whole hand) 39 200 Traumatology and orthopaedics Injuries of the lower extremity (18.4) 40 Dislocation of the hip Pain and limb shortening; typical position: anterior dislocation (left), posterior dislocation (right) 41 Dislocation of the hip Anterior dislocation (left) posterior dislocation (right) Possible complications of posterior dislocations: Iliac bone fracture; partial fracture of femoral head; posterior circumflex artery injury (risk of femoral head avascular necrosis); sciatic nerve injury. 42 Manipulation for dislocated hip • Under GA or spinal anaesthesia. • Place the patient on the floor. • Pull on the flexed thigh, an assistant maintaining the patient on the floor. 43 201 Femoral neck fractures • Common in elderly people after simple fall. • The blood supply to the femoral head may be disrupted, leading to avascular necrosis. • Clinically there is hip pain, inability to bear weight. • Usually, but not always, shortness and external rotation. X-Ray confirmation and fracture type: – Intracapsular – Intertrochanteric (extracapsular) – Subtrochanteric (extracapsular) Management: • Non-displaced or impacted fractures: bed-rest or early ambulation if possible. • Displaced fractures, when internal fixation is not available, traction for 2 months by femoral or tibia pin with 10% of patient’s body weight. 44 Femoral shaft fractures Major trauma, often with associated injuries. Blood loss within the limb 1-2 litres; risk of haemorrhagic shock. Treat by trans-tibial traction. Trans-tibial pin Trans-femoral pin 1/7 of body weight Skin traction (children) 45 Distal femoral fractures • • • • Condylar, supra-condylar. Reduce early when displaced. Aspirate the joint. Traction for 2 months. Patellar fractures • Often very displaced because of the quadriceps muscle traction on the proximal part of the bone. • Involves the joint and requires perfect reduction • When the quadriceps mechanism is intact, the patient can extend his knee: plaster cast with knee in full extension for 45 days, weight bearing possible. • When the quadriceps mechanism is not intact: refer for surgical repair; if not possible, cast 4-6 weeks. Weight bearing possible. 46 Patella fracture Pins and metal wiring 202 47 Knee ligament injuries: management Minor injuries - Short term immobilisation, pain killers, early rehabilitation Major injuries - Plaster cast for 45 days with knee 20° flexed and without weight bearing - The lateral, medial and sometimes PCL heal - The anterior cruciate never heals spontaneously: rehabilitation or surgery (young and active people) - Rehabilitation is essential. 48 Knee dislocation Posterior, Posterior, anterior, anterior, medial or lateral All the ligaments are ruptured. ruptured. Major vascular risk to popliteal vessels: vessels: always check pulses before and after reduction Reduction is URGENT 49 Patellar dislocation Trauma in valgus-flexion-lateral rotation Lateral dislocation; partial fractures may be associated. Reduce without anaesthesia when seen early. Aspirate the knee. Immobilisation in extension in a plaster cast for 45 days Weight bearing possible; rehabilitation Recurrence and chronic instability are possible. 50 Muscle trauma Contusions, stretches, ruptures. • Partial rupture: sudden pain, patient can walk, recovery in 4-6 weeks • Complete rupture: quadriceps is the most common. • Complete rupture requires surgical repair. 51 203 Tibiofibular fractures When tibia and fibula are fractured, they are usually displaced (here transverse fracture). . • 52 Check the skin carefully (commonly breached) and distal pulses for vascular complications. Closed reduction and long leg plaster cast for 3 months, knee 20° flexed, ankle 90° dorsiflexed. • 53 Wedge tibia fracture (left); left spiral fracture (right) Control X-Rays are normally immediately and on a regular basis. No weight bearing for 45 days. 54 Upper tibia metaphysis fracture direct trauma; common soft tissue injury to skin, muscle, vessels, nerves. Calcaneus traction is an option. Consolidation takes 3 months. Convert cast to short leg after 2 months. 55 204 Ankle sprains and dislocation Minor sprain Æ little stretch of ligament without instability Major sprain Æ rupture of ligament(s) with instability The most common ankle sprain is the lateral type. Trauma in varus with immediate severe pain and large lateral swelling. Management: Minor sprains Æ strapping for 3 weeks Major sprain Æ Plaster cast for 1 month In major injuries Æ suture of ligaments Importance of rehabilitation to prevent recurrence Usually good outcome Ankle ligaments 56 Ankle dislocations Severe trauma. Medial, posterior, anterior, lateral displacement. Skin problems, tendon, blood vessels and nerve injuries are common. Urgent reduction +/- suture of ligaments Plaster cast 6 weeks. Outcome may be poor. Here medial dislocation 57 Articular ankle fractures • Isolated fractures of distal fibula (stable): walking cast for 3 weeks. • Non displaced fractures: plaster cast with the ankle at 90° of dorsal flexion for 45 days. No weight bearing. Immediate control X-Ray, then after 15 days, 1 month and after cast removal. • Displaced fractures of medial and lateral malleolus (unstable): early closed reduction under anaesthesia and plaster cast in the same position and for the same duration. 6 weeks non weight bearing. 58 Calcaneus Calcaneus fracture fracture Major foot swelling. Wait for swelling to subside. Then plaster cast 2 months with a window under the heel. Early weightbearing on the forefoot. 59 205 Talus fracture (right) Partial or complete fracture; joint often involved. Reduction and plaster cast 45 days without weightbearing, X-Ray control every 15 days. Metatarsal fractures: Plaster cast for one month without weight bearing. 60 Rupture of Achille’s tendon Often sport trauma; partial or complete rupture. Inability to plantar flex; visible gap.Conservative treatment for high rupture. Surgery when seen after 8 days, in lower ruptures or in sportsmen. Surgical suture and plaster cast for 6 weeks, including 3 weeks in equinus. 61 206 Traumatology and orthopaedics Fractures of the pelvis (Chapter 18.3) ABC Trauma Survey. Look for signs of shock (not uncommon), scrotal haematoma, blood in urine or at the urethral meatus (below), blood in the rectum. An AP X-Ray view of the pelvis is usually sufficient. Check: • • • • Disruption of the ring Sacro-iliac joints Shenton’s line (here broken) Sacral fractures Ask for further views if indicated. 207 Fractures without disruption of the pelvic ring (Shenton’s line) Avulsions Often sports injuries, may involve the anterosuperior iliac spine, the antero-inferior iliac spine, or the ischial tuberosity. Most avulsions can be treated conservatively by rest and analgesics and heal within 3 months. Iliac bone fractures Usually resulting from a direct compressive force. Muscle attachments minimize the displacement and bleeding. Treat by bed rest until the patient is comfortable enough to be mobilised. Gradual protected weightbearing. Pubic and ischial rami fractures Fracture of a single ramus is uncommon, usually both rami are broken following a fall, often in the elderly. X-ray is important to exclude an impacted fracture of the femoral neck. Rest and progressive mobilization and weightbearing. Coccyx fractures Usually caused by direct blow. Symptomatic management. Sacrum fractures Usually direct trauma. Neurological complications may occur (with urinary retention). If the rectum is breached, there is a serious risk of contamination of the retroperitoneal space and fracture site (it is an opened fracture). Conservative treatment (bed rest). 208 Fractures with disruption of the pelvic ring Fractures of the 4 pubic rami Anteroposterior compression fractures (a) Lateral compression injuries (b) Vertical fractures (c) ‘Open book’ fractures’ (c)may be immobilized by a bed-sheet passed round the back and closed with a safety-pin Fracture of the acetabulum Usually in young people after violent trauma (not just a fall). Acetabular injuries range from simple avulsion of the periphery of the acetabulum to burst of the hip socket with fractures of the anterior and posterior columns. The femoral head is usually dislocated. After reduction, there is often poor fit between the femoral head and the acetabulum. Conservative treatment. 209 Complications of pelvic fractures Vascular The chief causes of death in pelvic fractures, especially severe ones. Tear of pelvic vein may cause haemorrhagic shock. Patients may require blood transfusions. Urinary tract complications Intraperitoneal bladder rupture: Trauma on a full bladder. Urine not passed. Lower abdominal pain, then rigidity due to peritonitis. Blood and no urine on catheterization. Open the lower abdomen and repair the bladder in 2 layers of chromic catgut; keep Foley catheter for 10 days. In extra-peritoneal bladder rupture, drainage of the bladder will allow the laceration to heal. Urethral injury: Retention of urine. Perineal pain. Blood at the urethral meatus Scrotal haematoma. A high riding or ‘floating’ prostate on PR examination. No urethral catheter! Insert a suprapubic catheter to divert the urine for 6 weeks. This may be difficult in case of large pelvic haematoma. Later, refer to a urologist for repair of the urethra. Rectal injury Some require a defunctioning colostomy. Key points Pelvic fractures may cause haemorrhagic shock. No urethral catheter if there blood at the urethral meatus, scrotal haematoma, or obvious pelvic fracture, insert a suprapubic catheter. Most pelvic fractures can be managed by bed rest and/or traction. 210 Traumatology and orthopaedics Spine injuries (Chapter 18.5) ABC of trauma ‘Primum non nocere’: first do not harm. The management of spinal injuries in your circumstances aims at: 1: Not making things worse by unskilled manipulation or movements. Immobilize the injured part until a fracture has been ruled out. 2- Prevent complications and promote recovery of patients with incomplete spinal cord injuries. 3- Prevent complications and promote rehabilitation of patients with complete spinal cord injuries. 211 Neurological assessment Sensory examination (see dermatomes diagram) Sharp-dull discrimination is examined and marked with a skin marker from the anaesthetic areas to the areas where sensation is maintained. The level of dermatome sensation still present suggests the level of possible spinal cord injury. Motor impairment Grading Grade 0: No contraction 1: slight contraction, no motion 2: Complete range of motion with gravity removed 3: “ “ “ “ against gravity with some resistance applied. 4: Normal or nearly normal Muscles involved - Above C4: Respiratory muscles paralysis. No survival in usual conditions. - Under C5: Abduction of shoulders, flexion of elbows are present C6: Extension of wrist and thumb C7: Flexion of wrist, extension of fingers C8: flexion of fingers T1: Interossei muscles L3: Adduction of thighs L4: Extension of the knee; dorsiflexion of the ankle L5: Active extension of the great toe S1: Plantar flexion of the ankle. Rectal examination: (sacral roots); an intact rectal tone suggests that spinal cord injury is only partial with a much better chance of neurological recovery. An absent voluntary rectal tone, after spinal cord shock has resolved, or priapism, indicates a complete cord injury with no chance of recovery distal to the cord lesion. Spinal shock It is the absence of all spinal reflex activity below the level of cord injury that usually persists for 24 hours after injury. 212 X-Rays Lateral view, A.P. View, oblique and special views. Denis’ 3-column concept of spinal stability When 2 out of the 3 columns are disrupted, the spine is considered unstable. 213 214 Cervical spine injuries The exact mechanism of the injury gives information about the resulting fracture. Common causes of cervical spine injury are driving without seat belts, falls from height, penetrating injuries. Radiographic examination of the cervical spine Cervical spine What to check on X-Rays : • • • • • • • C1 to T1 must be seen Alignment - trace out 4 lines Pre-vertebral soft-tissue shadow Atlanto-dens interval =3mm Open-mouth view for C1 &C2 fractures AP view for facet dislocations Swimmer view may be helpful Subluxation and ligament instability of the cervical spine If the fracture fragments or the spine segments are likely to get displaced before healing occurs, the fracture is said unstable. A fracture which is acutely unstable at the time of the injury may become stable, three months later, after bone healing. Burst fractures Odontoid fractures (3 types); immobilize by halo brace, plaster cast or traction. Locked facet dislocation: dislocation of the facets joints may be unilateral or bilateral. Reduce by cervical tong traction. A cervical collar may be sufficient for immobilization. 215 Fractures of the thoracolumbar spine In elderly people with osteoporosis, compression fractures (b) are common and stable. Fractures with compression of the anterior part of the vertebra limited to 50 % are stable. Treatment is symptomatic. If the height of the anterior vertebral body is reduced by more than 50 % (d), the fracture is unstable and may require more intensive treatment. Burst fractures (a) are also unstable. Fracture dislocations (c) are common in this region. It is a crucial area for stability and surgery may be necessary. Thoracic & lumbar spine What to look for • • • • • Loss of Vertebral body height Displacement of posterior body Angulation of spinous processes On AP films look for : Widening of interpedicular distance CT is best for upper thoracic spine Here: loss of vertebral height 216 Indications for referral - In theory, unstable fractures with incomplete spinal cord injuries (nothing can be done for complete spinal cord injuries) require surgery, but transport may make matters worse. - A neurologically normal patient with a fracture able to heal by immobilization must be treated conservatively. Nursing, bedsore prevention, urinary rehabilitation, neurological assessment are essential in all cases. Natural history of lower limbs paralysis Compression of the spinal cord will give first a flaccid paralysis and then a spastic one; spastic palsy allows walking with crutches and equipment. Roots compression results in a flaccid permanent palsy. Walking is impossible if the spinal lesion is bilateral and complete. Urinary and rectal paralysis needs special rehabilitation and care. 217 218 Peripheral nerve injuries Clinical test for peripheral nerve injuries: Axillary nerve injury Cannot abduct the shoulder (deltoid weakness), small sensory loss Testing for median nerve injury (a) Ask patient to clench the fist: index is pointing (b) Wasting of opponens of thumb (c) Sensory loss Testing for radial nerve injury 219 (b) Inability to extend the wrist: drop wrist (c) inability to extend the fingers at the knucke joints (d) wasting of extensor muscles (e) sensory loss Testing for ulnar nerve injury Motor: weakness of abductor pollicis compensated by flexor pollicis longus Sensory loss. Testing for sciatic nerve injury 220 (b): inability to dorsiflex the ankle joint: foot drop Sensory loss in: (c): complete sciatic nerve injury; (d) lateral popliteal nerve; (e) tibial nerve; (f) deep peroneal nerve Femoral nerve: Quadriceps action is lacking. Sensory loss anterior thigh. 221 222 223 Traumatology and orthopaedics Congenital and developmental problems: club-foot (19.1) 1 • The normal foot at birth is often in talus • Malformation (fixed deformity) is different from malposition (reducible deformity) • Check where is the deformity, whether it is reducible or not, what is the participation of the hind foot ? • Full examination (neurological +++) • Are there other deformities (toes +++) • Family history of malformations or diseases. 2 Movements of the ankle and foot joints Pronation (left), supination (centre), dorsal flexion (right) 3 Congenital talipes equinovarus (CTEV) ‘club-foot’ • It is a fixed deformity of the whole foot with abnormal bones (talus and calcaneus +++). • 1 / 1000 births. • There are club foot families (genetic factors? ). • Commonly associated deformities: hip and spine. 4 224 Deformity 5 Clinical diagnosis: Fore-foot is in supination and equinus; heel in varus; sole turned medially. The medial edge of the sole is hollow, its lateral edge convex. There is retraction of the joint capsules, ligaments and muscles (tibialis posterior, flexor digitorum, gastrocnemius). 6 Urgent management at birth: Physiotherapy twice a day with manipulations, stimulations and plaster splints between sessions OR corrective plaster casts changed every week to correct varus, adduction and supination. Equinus will be corrected last. If this method fails, surgery at the age of one year. Whatever the method, physiotherapy must continue until 3 years with plaster splints at night and proper shoe-ware. 7 8 225 Good result of conservative treatment (70%) 9 Results: - 30% will need surgery at the age of 1 year. - Even with good treatment recurrences do happen. - Possible complications: . Fixed bone deformity . Short foot . Walking difficulties. LONG FOLLOW UP is needed 10 Late complications 11 12 226 Infection of bones and joints (19.3) 13 Acute osteomyelitis Epidemiology It may be blood-borne, spread from a nearby infection (tooth,urinary tract,skin,chest), or may start in an open fracture. It is more common in children and in long bone metaphysis (femur, tibia, humerus). The knee is the most common site. Staphylococcus aureus is the most common germ (60%) 14 Acute bloodblood-borne osteomyelitis CHILD ADULT Knee, Hip, Shoulder Femur, Spine, Foot 15 Symptoms History of a recent infection in another site High grade fever: 39° - 40°, chills Severe, localized pain (knee ++) Soft tissue swelling The area feels warm to touch. 16 227 X - Ray Early signs are minimal: swelling of soft tissues. After a few days: lysis in the metaphyseal region: periosteal elevation with new bone formation. After a couple of weeks: sequestrum formation. 17 X - Ray after a few days Don’t wait for this! 18 Treatment The only hope of cure is an emergency treatment +++ Debridement of contaminated bone Two IV antibiotics for 6 weeks Then one antibiotic PO for 6 months If possible, regular X-Ray controls (every month) High risk of recurrence 19 Case N°1 15-year old male Acute osteomyelitis following an open finger fracture Bone sclerosis and periosteal elevation 20 228 Case N°2 Acute osteomyelitis of distal femur Good progress with surgical treatment and appropriate antibiotics. But recurrence is common. 21 Case N°3 Acute osteomyelitis of radius Good progress after agressive surgical treatment 22 Complications of acute osteomyelitis General complications Septicaemia Spread to other sites: heart, lung, brain, liver. 23 Complications of acute osteomyelitis Local complications Diffusion to the bone shaft Acute arthritis: partial, then complete joint destruction Chronic osteomyelitis. 24 229 Case N°1 Chronic osteomyelitis Symptoms After a long history of osteomyelitis. 22-year old male Infection from bone to skin: Partial, a sinus forms through the skin with then total joint spontaneous pus discharge destruction or after pressure around the area. 29 25 Case N°2 17-year old male Pain, fever, hot arm, swelling after sport Day 15 Case N°3 Spine osteomyelitis 27 Complete destruction of the disc, partial bone destruction 230 Day 20: Shaft diffusion Day 45: Sequestrum and recurvatum 26 Chronic osteomyelitis : Clinical aspect Chronic sinus Pus Skin inflammation 30 Chronic osteomyelitis: radiological aspect Periosteal destruction Sequestrum 31 Chronic osteomyelitis: treatment Antibiotics cannot reach the bone in a sufficient concentration. Repeated debridement : removal of necrotic bone, foreign bodies, necrotic soft tissue. The best indication is presence of a sequestrum for sequestrectomy. Time consuming and expensive: therefore transfer If transfer is not possible, amputation is sometimes necessary after a long hsitory. 231 32 232 Acute pyogenic arthritis 33 Acute pyogenic arthritis Epidemiology Often blood-borne infection. More common in children < 3 yrs old. More common in hip and knee. The risk is major joint cartigage Damage. 34 Acute pyogenic arthritis Symptoms Fever, chills Search for a portal of entry Pain +++: walking is difficult or impossible Every movement of the joint is difficult. Swelling of the joint and warm skin on palpation. 35 Acute pyogenic arthritis X-Ray Initially normal Sometimes shows enlarged joint space because of joint abscess 36 233 Acute pyogenic arthritis Treatment Urgent +++. Start immediately IV antibiotics. In the OR, within 12 hours, under full aseptic conditions : Joint aspiration for pus. Irrigation of the large joints (hip, knee) Immobilize the joint by cast or traction. 37 Acute pyogenic arthritis Complications Destruction of the joint arthritis early osteo- Joint fusion Shortening walking difficulties 38 Acute pyogenic arthritis Complications : Case N°1 • Female, 2 Yrs • Early treatment Sinuses Osteomyelitis 39 Acute pyogenic arthritis Complications: late cases Case N°2: femoral head necrosis 234 Case N°3: dislocation of the hip 40 RESUSCITATION AND ANAESTHESIA 235 Resuscitation and anaesthesia Shock and resuscitation of critically ill patients (Chapter 13.1) 1- Definition Shock is a failure of the cardiovascular system to meet the demands of the body, causing hypoperfusion of the tissues. 2- Symptoms and signs of shock In established shock, the patient is pale, cold, thirsty, cyanosed, sweating, anxious, hyperventilating with a low blood pressure, a rapid and feeble pulse and low urine output. For treatment to be effective, shock must be recognized early when not all those signs and symptoms are present. In particular, the fall in blood pressure occurs late, after at least one litre of blood or plasma has been lost. A rising pulse rate is an earlier and more reliable sign. 3- Shock management The treatment will be more efficient if done by several people: call for help. Refer to the ‘ABCDE’ assessment of acute trauma (‘Trauma module’). Monitor the patient's response If he is not responding to fluid replacement, suspect a missed injury. Re-examine him. When to abandon unsuccessful resuscitation? After 15 minutes of unsuccessful CPR or after 15 minutes of fixed dilated pupils, you can stop the resuscitation. 236 Identify the cause of shock The patient having been resuscitated, you can now look for the cause of the shock if this was not obvious from the start. This requires clinical examination, especially in cases of trauma where the obvious injury (head injury or peripheral injury) may not be the cause of the shock. Head injuries in particular do not cause shock. Hypovolaemia It is the most common cause of shock in surgical patients. It includes: - Haemorrhagic shock in which the bleeding can be: - external and obvious (femoral artery injury, heavy PV bleeding); - or internal and hidden (ruptured ectopic pregnancy, ruptured spleen, etc...). Estimating blood loss (see diagram). - Dehydration (loss of extracellular fluid) e.g. vomiting and accumulation of intestinal fluid in cases of intestinal obstruction. - Severe burns (loss of plasma). Other causes of shock: - Neurogenic shock and vasovagal attack. One example is cases of abortions with placenta stuck in the cervix or curettage performed without anaesthesia, because of a response to cervix stimulation. - Septic shock (often hyperdynamic with warm extremities) is difficult to diagnose and manage. Give fluids, IV antibiotics and treat the cause (e.g. peritonitis, septic abortion). - Anaphylactic shock. - Cardiogenic shock: myocardial contusion or cardiac tamponade (rare). Once the cause has been identified, initiate the specific management of the cause, e.g. urgent laparotomy.However the patient must be in a reasonably stable condition before anaesthesia is given, otherwise this will decompensate the condition further because he is only maintaining his blood pressure by severe vasoconstriction. 237 Complications of shock They are due to prolonged ischaemia of vital organs. Acute renal failure due to prolonged hypovolaemia and kidney ischaemia. Adult respiratory distress syndrom (ARDS), often fatal even with the best critical care provided in sophisticated hospitals. Hepatic failure. Brain damage due to prolonged hypoxia. Disseminated intravascular coagulation (DIC). Myocardial infarction. Intestinal infarction. Key points Identify shock early and treat it energetically. Care for the airway, ventilation and circulation in that order. Monitor the patient's response and reassess frequently. Look for the cause, do a head to toe examination in case of trauma. Don't operate on a shocked patient without resuscitation. 238 Resuscitation and anaesthesia Blood Transfusion (Chapter 13.2) General principles Blood transfusion is a life-saving procedure in surgical patients when properly indicated; however, strict safety procedures must be followed to avoid fatal complications. Blood has usually been donated by a related or unrelated blood donor. Under current conditions, the absolute safety of this blood cannot be guaranteed and indications for blood transfusion must be kept to the strict minimum. Indications/contraindications Because of the multiple complications including transmission of HIV, the risk of which cannot be completely eliminated, blood transfusion is indicated only for saving the life of the patient, i.e. a patient in haemorrhagic shock who cannot be resuscitated by blood substitutes. A blood transfusion that is not absolutely indicated is absolutely contraindicated. This includes chronic anaemia which is well tolerated, even at very low rates of haemoglobin or haematocrit and acute haemorrhage within certain limits. For example a fit adult, such as a mother having a caesarean section, can tolerate a blood loss of up to 1 litre or even a litre and a half, before you need to give her blood. But when an adult needs blood, he needs at least two units. The transfusion of a single unit is useless. On the other hand children can easily bleed to death during relatively minor operations or injuries because of their smaller circulating volume. Laboratory results (haemoglobin rate, haematocrit) are never a justification for blood transfusion as it is the clinical state of the patient that must justify the indication. 239 Complications Transmission of HIV This has become a major problem because of the high prevalence of HIV in the general population and therefore in the blood donors, the fact that there is no cure and that the disease is always fatal. To keep the risk of transmission to the minimum all blood donors, however urgent the case, must be screened by one of the quick tests available. However, tests have a variable sensitivity and may also give some false negatives. There is a 'window' of about 3 months after contamination by the virus during which a person is infected and can transmit the virus but will test negative. Therefore tested blood is never absolutely safe and for more protection of recipients the indications of transfusion must be kept to the minimum. Transmission of hepatitis (B and C) and other diseases such as syphilis, malaria, cytomegalovirus, bacteria. Transfusion reactions Major transfusion reactions They cause haemolysis, are potentially fatal and are usually due to incompatibility in the ABO system; they are the result of a mistake, either in the grouping of the donor or recipient, the labelling of the blood unit, or the control of the blood before transfusion. They are therefore avoidable. They occur early in the course of the transfusion with feeling of unease, headache, lumbar pain followed by a state of shock with rigors. In a patient under anaesthesia the first symptoms will be absent and there will be an otherwise unexplained state of shock.If the patient survives, later there will be oliguria, dark urine followed by jaundice. Minor transfusion reactions They are due to incompatibility in other blood group systems which are not checked in basic laboratories, or to high agglutinins titre in the donated blood. Fortunately, they are seldom fatal. Febrile allergic reactions They are due to the presence of pyrogenic substances in the blood. Circulatory overload It is a hazard especially in children, elderly patients or patients with heart failure. Causes acute heart failure with pulmonary oedema. Clotting problems This happens with massive transfusions of stored blood which is deficient in unstable clotting factors and platelets. Other complications Hypothermia, when large amounts of cold blood are transfused, hyperkalaemia. 240 Alternatives to transfusion of donated blood -Plasma expanders (Haemacel, Gelafundin, Gelafusin, Dextran) These are solutions of macromolecules (colloids) which remain in the intravascular compartment of the body; they are expensive and no longer recommended in shock. -Emergency autotransfusion In this method, blood for the peritoneal cavity is collected and immediately transfused to the patient. Indications: ruptured ectopic pregnancy; rupture of the spleen or the liver. Contraindications: when the blood is obviously infected (offensive smell) ; chronic ectopic pregnancy ; splenic rupture by open trauma or with concomitant gut injury. Equipment (to keep ready in theatre in case of emergency): a few blood collecting bags, already containing citrate (anticoagulant); a metallic funnel that can be bought in a shop and sterilized; a medium-size sterilized gallipot. Procedure As soon as the abdomen is opened collect escaping blood in the gallipot. Pour it through a filter made of 2 or 3 thicknesses of gauze placed over the funnel, and collect it in a blood tacking set. Then pass it to the anaesthetist for immediate transfusion. You can collect a few blood units in this way and save the need for transfusion of donated blood. Advantages: The patient can be transfused immediately. You are giving the patient's own blood, so there is no problem of compatibility or transmission of diseases. Key points Absolute safety of donated blood cannot be guaranteed. Blood transfusion has numerous complications. If a blood transfusion is not absolutely indicated, it is absolutely contraindicated. Only the clinical state of the patient is an indication. To an adult give two units or none. Use alternatives to transfusion of donated blood. 241 242 Resuscitation and anaesthesia Fluids and electrolytes (Chapter 13.3) Causes of dehydration in the surgical patient: - Vomiting (acute abdomens, intestinal obstructions, peritonitis). - Accumulation of fluids in the bowel (intestinal obstruction or ileus) or in the peritoneal cavity (peritonitis). - High fever. - Uncompensated losses through drains, stomas or fistulae. Assessing the severity of dehydration If you operate on a dehydrated patient before correcting at least part of the deficit, there is a real risk of death on the table or soon after the operation. Always assess the state of hydration before taking a patient to theatre. - Mild dehydration (5% of the body weight) These are patients whose history indicates that they must be dehydrated but who do not yet show any signs of it, e.g. patients who have had no fluids for 24 hours, or have been vomiting. - Moderate dehydration (8% of the body weight). Clinically these patients have a dry mouth, sunken eyes, moderate reduction of their skin elasticity. An infant may have a depressed fontanella. - Severe dehydration (10% or more of the body weight) They have a very dry mouth, severely sunken eyes, and greatly reduced skin elasticity. An adult may be confused and a child delirious, comatose or shocked. The hands are cold and the blood pressure is low. Intravenous access Peripheral vein cannulation If the patient is in poor condition, undergoing a major operation or likely to require IV fluids or IV antibiotics for a few days, you need to have a secure reliable IV access (with an IV cannula) for both the anaesthesia and the postoperative period. Especially if the patient is shocked or requires IV fluids at a high rate, choose the biggest cannula you can find and secure it well. Critical patients may require 2 IV lines which offer more security in case one of them is pulled out or gets tissued. You can also use: - External jugular vein cannulation; - Central vein cannulation; - Cutdown. 243 Correction of dehydration Amount of fluid required This depends on the severity of the dehydration estimated as above, and the patient's body weight. Weigh the patient if you can, otherwise estimate his weight. This is particularly important in children who can easily be under or over hydrated. See chart. Example for a 60 kgs patient: -Mild dehydration (5%): 3 litres deficit. -Moderate dehydration (8%): 4.8 litres deficit. -Severe dehydration (10% or more): 6 litres deficit. Rate of correction Severely dehydrated patients are often rehydrated too slowly. Correct dehydration quickly: give half the fluid needs in the first hour and the other half in the next 4 hours. Type of fluids required A surgically dehydrated patient has lost more water than sodium and chloride. He will also have lost potassium. Give him the first half of the deficit as Ringer's lactate (or 0.9% saline) and the second half as alternate bottles of Ringer's lactate (or saline) and 5% dextrose. Add 10 mmol of KCl to each 500 mls of fluid after the first two. Monitoring the response to IV fluid treatment Monitor the pulse, blood pressure, skin turgor and urine output. Insert a urinary catheter early and discard any urine present in the bladder at the time of catheterization. Start recording the urine output from that time. The pulse should decrease, the blood pressure increase, the skin turgor go back to normal, and the urine output should be 1 ml/kg/h at least. Only if you rehydrate them energetically like this, can you operate on surgically dehydrated patients without risk within 4 hours of admission. Intraoperative fluids requirements Continue to correct any preoperative deficit not been completely corrected. Patients undergoing laparotomy lose water all the time that their abdomen is open. Give them 15 ml/kg of fluid during the first hour, 8 ml/kg/hour after that. Compensate for fluid sucked during the operation (e.g. peritonitis) as measured in the suction machine and for blood loss. 244 Fluid and electrolytes requirements in the postoperative period You have to provide the normal requirements, replace any deficit that has not been replaced before or during surgery and compensate any abnormal losses. Basal requirements Water: 35-40 mls/kg/24h ; for an adult 2500 mls/24 h ; in a hot climate 3000 mls. Sodium: 1 mmol/kg/24h Potassium: 1 mmol/kg/24h Energy: 35 Kcal/kg/24h Nitrogen, vitamins and trace elements: these are not available in isolated hospitals. Abnormal losses - NG suction and vomiting. - Sweat and perspiration especially in a hot climate or in case of high fever.Give 250 mls extra fluids for each °C of temperature above 37°C. - Diarrhoea. - Other losses (through drains, stomas, fistulae) Intravenous fluids - 5% Dextrose It is isotonic and contains 50 g of dextrose/litre. Provides water and little energy (200 calories/litre) and no electrolytes. If you want to give more energy to a patient who is unable to eat for a long time, you will have to use or prepare more concentrated solutions by adding the appropriate amount of hypertonic dextrose to 5% solutions. These hypertonic solutions thrombose the veins. - 0.9% (normal) saline It is isotonic and contains water 154 mmol/l of sodium and 154 mmol/l of chloride, which is approximately the same concentration as in the extracellular fluid. - Ringer's lactate (Hartman's solution) It is isotonic and the best solution to replace water and electrolytes losses in case of surgical dehydration. It contains: - 131 mmol of sodium - 5 mmol of potassium - 29 mmol of bicarbonate (as lactate) - 0.9% saline in 5% dextrose (dextrose normal saline or DNS) It contains 5O g of dextrose, 154 mmol of sodium and 154 mmol of chloride per litre. It is hypertonic (osmolarity 585.5 mosm/litre while plasma osmolarity is 298 mosm/l) and is not recommended in routine use. 245 Examples of fluid regimens in surgical patients - Fit patient undergoing a non abdominal operation (including hernias repairs) This patient will be able to drink a few hours after his operation. There is no need to give him IV fluids after that. The drip can be discontinued as soon as he has recovered from the anaesthetic. - Fit patient undergoing an elective laparotomy He will require IV fluids for a few days to cover his basal requirements until his bowel sounds reappear and he can drink.Then his IV intake should be reduced until he can drink enough to cover his needs. Example 1 (60 kg adult who has had an elective laparotomy) : 2.5-3 litres of IV fluids in the form of one l litre of Ringer's lactate followed by 2 litres of 5% dextrose.Avoid saline in the first 2 postoperative days because of the metabolic response to surgery with salt and water retention.You can give it if you have no Ringer's lactate. - Patient undergoing an emergency laparotomy for intestinal obstruction You must compensate his deficit before and during the operation.He may still have some deficit at the end of the surgery which will have to be compensated.He needs to have his basal requirements covered plus any abnormal losses. Example 2: a 60 kg adult who has had a laparotomy for detorsion of sigmoid volvulus.Urine output in the first 24 hours : 1200 mls, indicating that his deficit has been well corrected.Drainage through the nasogastric tube in the first 24 hours : 600 mls. Maintenance needs can be covered by 1 litre of Ringer's lactate (or saline) and 2 litres of 5% dextrose. If he is passing urine, add 10 mmol of potassium to each litre of solution. Don't give potassium if he is not passing urine. Abnormal losses: 600 mls. Replace this by an equal quantity of normal saline and for each 500 ml of aspirate add 20 mmol of potassium to the patient's intravenous fluids. Example 3: a 30 kg child who has had a laparotomy for peritonitis due to perforated typhoid perforation. Temperature: 39°C, drainage through the nasogastric tube : 400 mls. Maintenance needs can be covered by 30 x 40 mls = 1200 mls given as 400mls of Ringer's lactate (or saline) and 800 mls of 5% dextrose. Add 250 mls of 5% dextrose to compensate his abnormal losses through the skin and 400mls of saline to compensate his abnormal losses through nasogastric suction. Total: (400+400) = 800 mls of Ringer's (or saline) and (800+250)= 1 litre of 5% dextrose. 246 Starting oral fluids Intravenous infusion fluids are expensive and require good nursing supervision.They should not be given unnecessarily. If a patient has no nasogastric tube, give him sips of water the day after the operation, then increase gradually. If a patient has a nasogastric tube, start oral fluids as soon as his stomach is empty, his bowel sounds have returned, and he has passed flatus. Reduce his IV fluids as you give him fluids by mouth and discontinue them when he is taking a sufficient amount orally. Nursing care Postoperative patients and all patients on IV fluids for more than 24 hours should have a fluid balance chart stating: - intake: intravenous and oral. - output: urine, gastric fluid (suction or vomiting), drainage, output through fistulae or stomas, diarrhoea. Prescribe the infusions in the column on the left. Ask the nurses to enter the bottles on the 'intake' column only when they are finished. Every day in the morning calculate the intake and output of the previous day. The nursing staff will be more likely to fill these charts if they understand how important they are and if you take the records into consideration. Use them for serious patients. Urine and gastric fluid collecting bags must not be emptied or changed by the relatives because output must be recorded on the patient's chart. The output must be measured and recorded at a fixed time in the day, preferably early in the morning so that fluids for the following day can be accurately prescribed. Nurses should be aware of the rate of infusion to be given and not just replace one bottle by another when it is empty. Patients, especially children, can be dangerously under or over loaded if this is not applied. For children,write on the infusion bottle the time it should start and finish, and the rate of infusion. Remove the excess fluid from the bottle before the drip is started; like this they will not receive more than necessary. Key points Assess all patients for fluid deficit. Get reliable IV access and correct deficit quickly. Correct deficit preoperatively. Postoperatively provide normal requirements, deficit and abnormal losses. 247 248 Resuscitation and anaesthesia Pre-operative care (Chapter 14.1) (Especially emergency laparotomy) Pre-operative preparation Careful preoperative preparation is essential except in case of extreme emergency. A good preparation will prevent many complications during and after surgery. In any case make sure he (the relatives in case of a child) understands and accepts the operation, its risks and its possible consequences (e.g. colostomy, hysterectomy…). This is called ‘informed consent’. First check the patient’s clinical signs - Inspection: look at the patient, watch any facial expression of pain, how he is breathing, the respiratory rate and its type (deep or superficial, abdominal wall movement), the coloration of conjunctiva, mucosa and nails, sweating, shivering. - Palpation: temperature of skin and nose, abdominal wall, signs of dehydratation, tongue and skin; capillary refill. - Auscultation: heart and abdominal sounds. Vital signs - Temperature: fever or hypothermia - Pulse: tachycardia, bradycardia. - Blood pressure: hypo or hypertension - Urine output. - Pulse oxymetry. We recommend that all patients who need emergency laparotomy should be prepared in the Recovery Room. The ‘four tubes’` rule Reliable IV line: One or two reliable IV lines are essential to rehydrate the patient. If necessary treat shock with epinephrine only if there is no response to fluid challenge. Start antibiotics if necessary. Gastric tube: a nasogastric tube is routinely inserted to assure an empty stomach especially in case of intestinal obstruction, vomiting, for any operation involving the gastrointestinal tract, or when you are not sure that the stomach is empty (as may often be the case in an emergency operation). There is a risk of aspiration of stomach contents into the airway. Urinary catheter: to monitor the urine output and to protect the bladder (lower abdominal or pelvic surgery, caesarean-section). It should be inserted under strict aseptic conditions and any urine present in the bladder discarded to start monitoring urine output. Concentrated urine is also an indication of dehydration. Tracheal tube (in theatre by anaesthetists). 249 In the operating theatre, before surgery Position the patient supine, both arms resting on arm-boards for the anaesthesia team. If the diagnosis is unclear, take the chance of the relaxation caused by anaesthesia to deeply reexamine the abdomen and look for masses. Wash the patient’s back in case of a spinal anaesthesia. Once the patient is under anaesthesia, wash the abdomen with soap and water. Then prepare the skin generously with a strong antiseptic (povidone iodine preferred), starting from the site of incision and extending from the nipples to below the groins and to both flanks on the sides. Remember that you may have to extend the incision you originally planned. Draping must expose the whole of the anterior abdominal wall, from xiphoid process to pubis. Check suction and diathermy. During surgery Intravenous infusion must be continued. Urine output, pulse oxymetry, blood pressure, pulse and skin coloration will be watched by the anaesthetist. Communication between anaesthesia and surgical team is essential. Take into account all intra-operative fluid losses, including fluid sucked out from the abdomen, fluid sucked out of the stomach, long exposure of the bowels to air, urine output, bleeding. The surgeon should check the correct position of the gastric tube. Key points Assess and resuscitate carefully patients before emergency laparomy. 4 tubes: IV, gastric, urinary, tracheal. 250 Resuscitation and anaesthesia Postoperative care (Chapter 14.2) The surgeon’s or Health Officer’s responsibility does not end when the patient leaves the OT. It continues until the patient has been discharged. Transfer of the patient from OT to recovery room This must be coordinated by the anaesthetist who looks after the head and ensure the safety of all drips, drains and catheters. A minimum of 2 additional people are needed to help. Criteria for the patient to leave the OT (for the anaesthetists) • • • • • • • the patient is awake the patient can move but is not very agitated his breathing is calm and regular oxymetry is above 90% on air; if no oxymetry, the extremities are well coloured and warm, the capillary refill is good blood pressure and pulse are close to the pre-operative values the drains, drips and catheters are not blocked the book of the patient is completed and the anaesthesia card correctly filled Post-operative patient’s position As a rule, all patients who have had a general anaesthesia must be nursed in recovery position, on the stretcher and in the bed of recovery room: On the side, semi prone, with the legs and knees semi flexed. This is to prevent respiratory obstruction by the tongue falling backwards and to reduce the risk of inhalation in case of vomiting. Exceptions: patients with large plaster casts, traction for fractures, multiple drains…it’s difficult to put the patient on the side so he may to remain on his back with the head turned on the side and additional supervision; also, in case of breathing difficulties, a semi-sitting position is better to improve breathing. 251 In recovery room The patient must never be left alone, and the barriers of the bed raised. Check vital signs again: blood pressure, pulse, oxygen saturaation or extremities… Check IV drips, drains, catheters… Oral and written handover to the nurse in charge: • which kind of operation has been done • condition of the patient • how often to check vital signs • drip rates • medications: antibiotics, analgesics… • when to call in case of problem. Immediate postoperative care • monitoring vital signs : frequency and duration will depend on the operation and the patient’s condition. • correct amount of fluids IV : the best guide to adequate fluid replacement is the urine output and concentration. • medications: - pain relief: paracetamol ( 1g TID ), diclofenac ( 75mg TID) - antibiotics as necessary. • oxygen therapy if necessary after major surgery • checking for bleeding • attending to general nursing care and comfort of the patient. When can the patient start drinking? • After a minor operation: when he is fully conscious and has no nausea. • After a major operation not involving the abdominal cavity ( orthopaedic for example): usually after 12-24 h. • caesarean section : 12 hours after surgery. • After a laparotomy for GI surgery: usually only after the patient has passed gas or there evidence of peristaltism. When to start a solid diet The next day if bowel movements are confirmed. When to remove the nasogastric tube? If output is less than 100 mls, and when flatus have been passed. Sometimes the postoperative ileus may be prolonged, in which case gastric suction must continue (vomiting, no flatus, abdominal distension). When to mobilize the patient? As soon as he/she is comfortable to do so, encourage leg movements in bed and ambulation as soon as possible, as well as deep chest exercises. 252 Resuscitation and anaesthesia Principles of Anaesthesia for surgeons (Chapter 14.3) An-aesthesia means ‘without pain’. It is a reversible condition witch allows a surgical operation. A surgical operation requires: Analgesia with or without unconsciousness, with or without muscle relaxation. There are different types of anaesthesia In general anaesthesia: the patient is unconscious, breathing alone or assisted by the anaesthetist. In local anaesthesia: the patient is conscious. There are 3 types: Regional anaesthesia, spinal and epidural anaesthesia. Blocks: scalenic, lumbar, troncular, ulnar, sciatic. Local anaesthesia, skin. Local and general anaesthetics can be used to treat the postoperative pain. There is no such thing as minor anaesthesia. When a patient needs surgery, the anaesthetist shares responsibility for the patient. He must check all the parameters to ensure the patients safety from the preoperative period to the exit from the recovery room. His work is not confined to the operating room. 253 General anaesthesia Achieves absence of pain, unconsciousness, and sometimes muscle relaxation for abdominal surgery. To control pain, the anaesthetist uses opioids such as pethidine, or ketamine which is sufficient for superficial surgery. To make the patient sleep, hypnotics are given such as Ketamine, diazepam, thiopentone. He can use also gas such as halothane. For muscle relaxation two cases are possible: Intubation needs Suxamethonium. This depolarisant muscle relaxant has a short action and causes rapid spontaneous breathing. At the beginning of his action, it stimulates the nerve (fasciculations) and a deep block is realized. Abdominal surgery needs long-acting drugs such as Tracrium, with no depolarisation effect. Ventilation during general anaesthesia can be spontaneous or assisted. In case of long surgery or full stomach, intubation may be required. When you are ready to cut, he must ask the anaesthetist’s permission to start. And when the end of operation approaches, alert the anaesthetist. For children, induction can be achieved by IM injection of Ketamine+/-diazepam without IV line. For a very young patient gas induction is often necessary. When you have finished the procedure, the anaesthetist awakes the patient. When all parameters of recovery are right, he goes with the patient in the recovery room. He orders infusions, analgesics in writing. General anaesthesia risks include: Asphyxia due to: airway obstruction: aspiration, tongue drop, laryngal or bronchospasm, respiration arrest: muscle relaxant, morphinomimetic, pneumothorax… Circulation failure due to: Septic shock, hemorrhagic, anaphylactic, infarctus deshydratation, third sector in digestive occlusion, large burns. 254 Regional anaesthesia Spinal and epidural anaesthesia give a block of nervous center. 1 - Spinal anaesthesia The spinal needle is introduced between L3 and L4 vertebrae into the subarachnoid space. This space is chosen because the spinal cord finishes at L2 level. When the needle is in correct position cerebrospinal liquid appears. A small volume of hyperbaric lidocaine or Bupivacaine is injected slowly. The block is complete motility and sensitivity. If the patient is positioned on the side, the spinal anaesthesia can be lateralized. Risks: Cardiovascular Collapse, bradycardia, respiratory cardiac arrest if the block increases to the thoracic and cervical nervous centre, meningitis, headache, urinary block permanent paralysis by local nervous poisoning or compressive hematoma. 2 – Epidural An epidural causes a block of the nerves where they cross the dura mater. It is not widely practised in Ethiopia. Regional blocks 1 – Plexus block 2 – Troncular block. 255 Local Anaesthesia Advantages - practical and easy - cheap - safe - no need for admission - done by the surgeon himself. Disadvantages - may fail - not possible if tissues are infected - complications are rare but can happen - requires patient's cooperation; not for young children, anxious or restless patients. Maximum safe doses per body weight for an adult ml of 1% solution Without adrenaline 3 mg/kg 200 mg 20 ml With adrenaline * 6 mg/kg 400 mg 40 ml * Adrenaline added to a local anaesthetic causes vasoconstriction and delays absorption of the anaesthetic.The maximum safe dose of solutions with adrenaline is higher. A 1% solution contains 10 mg/ml = 1 g/100 ml Contra-indications - No cooperation from the patient - When you would need to use doses above the safe dose. - Local infection. - Hypersensitivity. Contra-indications to the use of adrenaline in local anaesthesia solutions: extremities. - Fingers and toes. - Nose. - Penis. Precautions - Give a diazepam premedication if the procedure is more than a minor one. - Tell the patient what you are going to do. - Aspirate to check that you are not in a blood vessel. - Wait for 10-15 minutes. 256 Complications Usually occurs when safe doses have been exceeded or in case of intravenous injection. - Neurological complications Anxiety,pins and needles, twitches, fits, loss of consciousness. - Cardiovascular complications Tachycardia, cardiac arythmia, cardiac arrest. Neurological symptoms occur before cardiovascular symptoms and are a warning. - Hypersensitivity (allergy) What to do in case of complications? Be ready: have equipment ready for ventilation and resuscitation. Give IV diazepam slowly. Put up an IV drip for venous access. Local anaesthetics can also be used for: - Surface anaesthesia (lignocaine jelly or spray). - Spinal anaesthesia. - Nerve blocks - Infiltration anaesthesia can also be combined with spinal or general anaesthesia. Key points There is no such thing as ‘minor anaesthesia’ Cooperation and communication between surgeon and anaesthestist is essential. Properly used,local anaesthesia is safe , easy and very useful for minor procedures. Do not exceed 20 ml of 1% plain solution of lidocaine for an adult. Complications of local anaesthesia are neurological and cardiovascular. 257 258






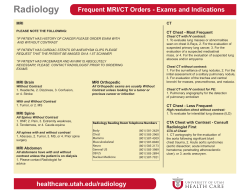




© Copyright 2026