
Document 186594
COLPOPERINEORRHAPHY
THE
AND
VAGINA
TO
PERINEUM
of
"Practical
of
its
"The
B.S.,M.D,
III.
"Landmarks
Surg-er.v,"
Intestinal
Chart
the
S.vmpathetic
and
Histolog-.v
Abdominal
in
Chicago
Surg-ery;
in
the
Post-Graduate
Professor
of
and
Mary
and
to
in
St.
Surg-eon
Hospital
and
Gynecolog-y
Abdominal
and
Colleg-e,
Thompson
"Women
of
Gynecolog-y
Consulting-
matic
Auto-
etc.
MedicalColleg-e;Gynecolog-ist
Hospital;
the
Anthony's
to
the
for
Children.
CHICAGO:
THE
CLINIC
PUBLISHING
1899.
toneum,
Peri-
Gan-
School
Medical
Harvey
Gynecolog-y,"
The
Physiolog-j."
Brain
fflia."
in
"
Nerve,"
Visceral
Professor
HOW
THEM
MEND
Chicago,
"Life-size
AND
ROBINSON,
BYRON
Author
INVOLVED
THE STRUCTURES
AND
CO.
and
inal
Abdom-
Surg-ery
Illinois
189C
ACCORDING
ENTERED,
By
IN
THE
OFFICE
THE
TO
the
THE
OF
CONGRESS,
LIBRARIAN
IN
YEAR
THE
COMPANY,
PUBLISHING
clinic
OF
ACT
OF
CONGRESS,
AT
WASHINGTON.
CD
cm
"a:
DEDICATION.
This
my
monograph,
of
fellows
(Denver,
the
June,
as
to
and
herein
them
needy
'98)
and
labors,
and
will
indirect^,
in
The
is
be
of
direct
through
and
respectfully
the
and
to
help
suffering
humanity.
The
hope
experiences
interest
them,
of
Journal
with
profession
researches,
before
Association
Association,
surgical
outlined
Medical
published
medical
the
to
my
American
Medical
American
dedicated
that
the
presentation
for
prepared
Author.
PUBLISHER'S
have
We
taken
from
book
from
work
the
to
thinks
that
of
he
life
from
during
helpful
great
the
help
to
satisfactory
be
of
process
full
those
to
and
of
X,
the
not
own,
fore
there-
who
the
ment
treat-
refers.
The
made
were
author's
numerous
and
are
such
cuts
text,
should
reached
and
to
a
must
true
as
be.
to
be
perfectly
certainly
all.
The
Station
of
complete
their
in
it
clinics,
have
We
physician
illustration
for
and
willing
are
helped
possible
who
technique
interest
is
comes
things
do.
of
extensive
it
few
which
to
cases
good
every
be
profusion
his
as
with
These,
of
the
in
operations
and
this
for
drawings
to
American
that
to
might
or
class
the
that
it
can
of
undertake
they
recommend
heartily
full
labor
of
the
of
everything
is
this
reproducing
Journal
it
pen
amount
an
The
Like
Robinson's
evidences
give
of
pages
Associatioii.
Dr.
in
pleasure
great
the
Medical
PREFACE.
Chicago.
Clinic
Publishing
Co.
of
AND
COLPOPERINEORRHAPHY
INVOLVED.
STRUCTURES
The
involved
structures
perineum
muscles
are
consists
claims
for
varied
levator
separated
and
superior
that
this
chief
the
restoration
two
classes:
of
of
and
the
have
a
the
floor,
fascial
muscles
deep
layer
The
basis
with
is
the
this
considerable
ani
of
respect
levator
The
consider
in
is
a
perinei
in
detail
rhaphy.
colpoperineor-
careful
clinical
in
ments
attach-
transversus
will
the
"
muscles
fascial
involved
labor
coccy-
sphincter
the
muscles.
the
into
layer
demands
the
We
fascise
divided
levator
extensive
of
inferior.
and
which
one
fascise,
the
superficial
and
of
that
and
be
may
the
"
of
characteristic
ends
ing.
sutur-
demonstrate
to
sutures
floor
pelvic
is
also
and
deep
to
fasciae, superior
attachment.
and
due
the
fascise
its
fasciee,
ani
and
both
or
of
of
peculiar
of
colpoperineorrhaphy
bulbo-cavernosus
experience.
is
however,
reunion
other
bulbo-cavemosus
one
investigation
means
perinei,
A
neither
aid
deep
colpoperineorrhaphy,
ani,
by
6, the
pelvic
of
the
pyriformis;
externus.
the
the
the
a,
transversus
ani
levator
the
muscles
geus
the
by
in
essay
colpoper-
generally
probable,
successful
in
of
is
chiefly
this
successful
It
some
been
of
factor
especially
with
has
object
the
The
inferior
cedure
pro-
flap-
or
the
is
muscle
ani
success
The
coaptation
basis
lies
success
defectivo
a
operative
methods
surgical
anatomical
essential
the
that
with
understood.
perfectly
nor
The
Notwithstanding
the
ineorrhaphy
of
repair
fasciae.
denudation
in
the
the
in
and
methods.
splitting
THE
and
anatomic
surgical
6
THE
VAGINA
LEVATOR
THE
The
levator
to understand
regards
origin of the
is considered
and
opinions
its
insertion,
of this
that
the
to
as
vary
muscle
muscle.
there
is
and
investigations
own
for
and
day,
function, form
foundation
a
late
this
at
even
Few
anatomists.
by
exact
My
sufficientlyplain,
is
established
exact
to
as
agree
difficult
perhaps the most
and
tion.
funcform, insertion
is
as
The
MUSCLE.
ANI
muscle
ani
PERINEUM;
AND
sertion
in-
strate
demonvaried
these
opinions.
The
1.
as^ to the
of
extent
the
raphe
and
insertion
distinct
and
rectum
also
coccyx),
lower
the
the
of
end
of
the
the
with
fascial
extreme
of
origin
this
Perhaps
by considering
and
be
to
the
and
red
of
the
as
in
the
insertion
levator
ani
as
with
disappearing
to
the
tissue,
the
muscle
endow
to
the
its
the
length
other
in
words
fibers
from
levator
ani
the
vary.
be
explained
cle
rudimentary musmay
a
the
to
sure
muscular
of
Moreover,
conditions;
insertion
variation
is
appearances
tendinous
or
distance
insertion
varying
ends
to
wall.
brace
em-
tendinous
connective
or
rectal
the
distal
vary
which
the
to
relations
exact
partial fascial origin and
extremities
loops
ani
precise relation
muscular
vaginal wall, whether
also as regards
and
of
muscular
the
regarding
levator
the
vagina, as
loops and
muscle
(between
of
origin
the
tail.
Its
double
fascial
accompaniments
complicate its origin and
insertion, as well as the interpretation of its function.
various
2. The
opinions as to the form of the levator
ani are
syncrasies
explained by difPerences
as
regards sex idioof individuals, disturbances
from
gestation
and
of the shape of the pelvis
parturition, variation
and
3.
fascial
The
levator
insertions
different
ani
ani
its size
lie in
and
views
attachments.
as
confusing
fascia, superior and
and
attributing to
to
the
function
its function
with
of
the
the
vator
le-
inferior, in exaggerating
it function
and
utilitybe-
HOW
longing
other
to
that
tensionized
of
knowledge
and
does
resemble
not
at the
vagina
relations
bottom
loop or
vagina
or
flat
sling, a
is
In
vagina.
canals
vagina
The
the
of
that
on
of
vaginal
In
thin.
a
as
the
the
does
course
an
It is
muscle
and
Origin.
from
the
point
of
to
pull
not
draws
but
the
pubic cord.
the
muscle
control
rectum.
The
bles
resem-
the
is
H- shape
compelled
of
and
vagina.
the
at
It is
H.
muscle
is
few
a
so
band
muscular
the
terior
pos-
I dissected
ani
is but
rectum
the
fold
the
which
levator
and
to
the
rectum
the
to
two
of
of
middle
the
upright columns
excellent
specimen
vagina
thickness.
The
wall
the
good- sized woman
to be really membranous,
between
or
similar
its
yet
"
the
producing
from
thin
yagina
against
vaginal wall produces the
sides
rectum
more
a
forward
excess
very
and
depends
forced
being
cle
mus-
or
encircling the rectum
controls
female
it vigorously
rectum
"
easy
collar
horse's
a
The
The
the
horseshoe, which
the rectum
directly upward,
canals forward
and
two
upward toward
The
muscular
loop of the levator ani
a
tinuous
con-
is far from
with
but
apex,
a
fragmentary
is
complicated.
funnel
or
as
viscus.
dissection
are
a
act
any
muscle
ani
Its
access.
adjacent
its
for
support
especially
ia
will
muscle
a
levator
the
of
difficult
and
It
genital supports.
inferred
erroneously
7
THEM,
MEND
TO
lines
in
really a pelvic diaphragm.
should
be
considered
as
muscle
arises:
to
its
origin,
from
bone,
insertion.
"
The
levator
ani
of the
ischial
pubis and
posterior surface
from
tendineus
pubic
vesicoand
spine; or
fascia, arcus
The
bony
origin is the posterior
ligament.
The
of
the
surface
bone
ischial
and
spine.
pubic
ani of bony
larger portion of the levator
origin arises
It begins
the
of the
from
posterior surface
pubis.
inch
the
half an
and
from
and
about
one
symphysis
This
inches
below
the
one-half
to two
pubic crest.
origin
is about
two
fingers wide
or
one
and
8
VAGINA
THE
AND
PERINEUM;
of the
its fellow
not
meet
inches, and does
to one
inch existing between
opposite side, one-half
the
them
is
on
posterior surface of the pubis, which
of musfilled in by the obturator
fascia.
The
bundle
cles
originating on the posterior surface of the pubis
downward
and
backward
the vagina
to embrace
passes
This
and rectum.
is the pubic sling or horseshoe
loop,
one-half
Fig. 1.
dissected
white
line
4, 4, the
the
author
fascia
with
pelvis
or
obturator
of
origin
the
muscle
fossa;
which
very
floor, whose
nerves
15, last
is
thin
off.
dissected
coccygeus
does
(5th) lumbar
and
ani
5, 5, the
not
12, 12, inner
;
the
levator
8, 3, the
muscle
of
loop
from
a
female
muscle;
ani
internus
;
pelvis
floor
muscular
obturator
pyriformis
flare
wall
is drawn
show
6, 6, the
the
of
2, 2. the
muscle
inner
;,
wall
the levator
ani
muscle,
the
close
to
cut
vagina,
radial wall, 10; 11, 11, the
crest ; 14, 14, iliac
13, pubic
of
9. the
the
like
pelvis
;
vertebra.
thick
quite
the
H, H, the horse-shoe
Y-shaped
urethra;
wall
;
to
1,1,
levator
:
cut
intended
and
of pelvis; 7, 7, sacrum;
darker
drawn
;"8. the
pelvic
This
(Robinson-Scholer.)
"
by
membranous
and
strong
in
in
others.
some
The
cases,
margin
and
of
is applied
loop, which
against the sides of the
thickest
rectum, is often the
part of the
vagina and
the
HOW
The
muscle.
the
to
perineal
the
vagina
and
tendon
or
others
in
while
it
smaller
The
is from
of
origin
the
one-fourth
ischial
and
raphe
it
exists,
wide
bony origin
distinct
a
the
to
anterior
Quite
inch
of
ani
immediately
strip
from
comes
plainly followed
be
can
dissections
some
levator
muscle.
coccygeus
half
to
one-
terior
pos-
ing
interven-
told.
be
spine
loop
ani
an
tendinous
the
of
portion
spine,
In
no
not
levator
the
without
raphe.
can
ischial
the
of
rectum
that
plain
absolutely
is
horseshoe
of the
side
opposite
9
THEM.
bundles
muscular
of
those
join
MEND
TO
by
the
the
eye
loop.
the
The
anterior
ligamentous
origin is from
ment
ligaof the bladder
(ligamentum
pubo-vesicale) and
the arcus
tendineus
from
(white line). The fibers of
the ligamentum
arise from
the levator ani which
pubohorseshoe
to the
vesicale
line
of little
are
in
extends
lateral
posterior
foramen
lies two
end
of
of
thickening
the
at
and
the
levator
The
it.
line
varies
The
the
the
tor
obturaanterior
ileo-
the
and
origiil of
course
levator
of
ani
may
be
the
the
In
superior.
arise
as
reddish
fine
the
tendinous
muscular
nature
from
it.
flat tendinous
layer
before
The
tendon
distance
proximal
much
below
project
it
as
well
into
the
of
being
capable
The
it
tke
of
its relations
to
as
arise
may
line
fold,
tendinous
a
line.
It
line.
fascia
ani
short
a
into
white
white
the
The
below
inches
their
or
,
from
the
over
ischium.
fibers
show
muscle
ani
white
the
levator
shade
may
reaches
the
from
a
muscular
may
white
muscle
with
the
line, the
bands,
of
spine
pubis,
white
four
inches.
length of about
line (arcus tendineus) is a part
or
tension
exan
of
the bladder, a
the anterior
true
ligament
white
white
the
three-fourths
and
line,
pectineal
The
of
surface
the
to
direction
slightly curved
a
The
practical importance.
as
pelvis
with
from
a
as
separated
muscle.
fibers
muscle
is
of
the
backward
horseshoe
and
loop
downward
of
10
in
of
surface
and
which
attached
the
'-
"
of
loops
larger
the
the
with
author.
0_n the
left
side
It
This
is
illustrates
a
the
cut
tissue
the
drawn
inferior
from
which
muscular
-"-
the
be
to
seem
fibers
muscular
the
loops
connective
-".-
by
terior
pos-
to
The
vagina
by
and
side
rectum.
interweave
rectum
Fig. 2."(Robinsoii-8ch.oler.)
dissected
the
of
the
to
and
walls
vaginal
the
while
embrace
jii^
the
of
sides
the
along
to
vagina,
wall
posterior
pass
only,
the
PERINEUM;
smaller
the
fleshy bundles,
two
side
AND
VAGINA
THE
"
a
surface
-
-^^
"-"^-"^~'
female
of
the
^'
pelvis
pelvic
the
is not
fascia
inferior
ani
fig.) the levator
the
surface
of
inferior
side,
right
showing
^ssected
levator
the
muscle.
its parallel
ani
the levator
muscle
1, 1, shows
with
am
fascia
ani
internus
2, the levator
bundles;
inferior; 3,3, the obturator
4, 4, the
muscle;
6, anogluteus
coccygeal
muscle;
5,5. the
maximus;
coccygeus
structure;
7, 7, the horse-shoe
loop of the levator
ani, showing
muscular
bundles
It is not
and
some
rectum
so
coursing between
vagina.
floor.
large
on
inferior
the
V?^I' .81urethra;
13, flaring ilium.
bundles
of
The
an
elevator.
(m
it is
oft, while
on
the
surface
9, vagina;
the
rectal
as
10,
it is
anus
of the
surface
pelvic
superior
12, sacrum;
11, pubic
arch;
flaring;
wall, forming
part interwoven
It would
the
on
in
appear
the
that
a
strong
rectal
in
some
wall
tion.
connec-
acts
oases
as
the
HOW
of
loops
the
levator
fibers
the
in
levator
is
rectum
of
of
part
the
l)elly of
relations
Its
close
muscle
if not
The
of
from
the
becoming
inserted
last
of
bone
the
in
they
acutely
the
turn
from
the
white
loop,
shaped
spine, embrace
ani arising from
chiefly in the
fourth
of
with
The
an
the
surface
of
of
phied
torn
part of
and
portion
vaginal
the
ischial
The
part of
the
levator
one
ani
spasm
muscle
and
muscle
the
rectum
of
backward
passes
and
which
which
may
one-
est
special interthe two-fingers wide, horseshoe-shaped
from
arises
the
posterior
vaginismus.
separated in lacerated
the
observe
raphe.
It is the
of
inserted
becomes
may
around
pass
rectum
muscle
horseshoethe
tendinous
gynecologist is
sling which
the pubis and
the
arising
from
spine
width
fibers
into
some
Yet
levator
inserted
from
and
vagina.
loop which
gives the
the anal
end
just before
is the sphincter
portion of
It
in
with
both
ward,
down-
and
become
as
ischial
in
backward
this
curve
is this
the
embrace
to
well
coccyx.
inch
part of
belly
the
very
which
origin
muscular
the
rectum.
intervening
no
to
the
fascial
to
of
line, as
together
tion.
situa-
levator
backward
few
A
coccyx.
and
curve,
a
large
loop and
partly
and
the
perineal raphe
of these
fibers
Many
pass
when
the median
near
raphe
coccyx.
downward
of
the
tendinous
the
in
of
part
the
over
rectovaginal
the vagina are
of
line, passes
white
external
its fibers.
muscle
the
the
of
part
the
passes
wall
with
interwoven
part
arises
the
to
to
from
arises
cular
mus-
vagina and
one-eighth
the
one-sixth
origin and
to
gain
pubic
the
band,
The
vagina.
between
which
width,
in
the
passes
small, thin
a
inch
an
which
ani
of
the
with
interweave
ani
wall
the
11
THEM.
MEND
TO
ward
down-
It
is
its
rectum
the
becomes
of
ward
for-
ward.
back-
turned
is
the
muscle.
It
hypertrothe
muscle
portion
It is the
perineum.
retards
labor, creates
prevent
coition, and
in
rare
12
Fig.
the
VAGINA
THE
3.
"
general
CAuthor.
view
clitoridis
erecto
) This
of
the
muscle
figure I drew
outlet.
pelvic
bulb
of
the
vagina
;
semi-diagramatically
1, clitoris
of
4, urethra
; 5. orifice
vaginal
(of Duverny,
glands
;
muscle
; 7, yulvoman)
commissure
vaginal
; 8, posterior
internus
10, obturator
muscle;
11,
ani
14, levator
muscle;
15,
coccyx;
osus
PEEINEUM;
AND
17, deep
layer
;
anus;
of
great
2,
vagina
;
of
9, transversus
;
sacrosCiatic
perineal
illustrate
;
3,
6, bulbo-eavern-
Barthalin,
perinei
12, sphincter
superficial
to
clitoridis
crura
ani
of
Tiede-
muscles
;
13,
externus;
16, the
ligament;
fascia.
HOW
by
In
anesthetic.
an
most
this
the
from
ischial
A
h.
tendinous
tendinous
of
on
words,
the
tip
of
of
the
fibers
with
of
median
be
side
each
also
coccyx,
of
some
downward,
of
inserted
into
The
but
the
is adherent
Deductions
be
be
in
from
drawn
the
tail
its fascial
insertion
to the
Certain
numerous.
gynecologic
of
regard
to
and
fascia
a
it is
of
the
levator
line
become
soon
is
superior
and
As
not
may
be
levator
ani
muscle.
levator
study by
becoming
connections.
fibers
The
ani
muscle
may
practical considerations
careful
practice.
the
tinuous
con-
white
to the
muscle,
intimately attached
fascia transversalis.
to the
The
compared
inferior
cular
mus-
are
the
very
fascia
pass
arriving at the
ward
turn
sharply back-
coccyx,
ani
twine
inter-
on
fibers
the
levator
from
vening
inter-
the
ani
many
tendinous.
anastomose,
with
originating
and
raphe,
to
the
ani
backward
pass
ing
interven-
no
externus
sphincter
loops of the levator ani.
the
levator
the
anus,
loop,
shaped
no
of
the
Some
loops
raphe.
of the
sphincter ani, which
those
the
to
the
an
The
c.
behind
a
of
coccyx,
horseshoe-
the
tendinous
back
of
fibers
muscular
with
forms
muscle
wide, has
the
at
or
one-third
the
inch
an
line
(not always distinct) and
sists
conthe
which
loops
originate and
In
surface.
other
posterior
pubic
the
forming
about
immediately
of
panying
accom-
originate chiefly
the
of
the
raphe
belly of
the
insert
for
front
in
immediately
portion of the muscle
three-fourths
of
tinct
dis-
to
fibers
white
the
portion
inch
about
of
raphe
The
ani
quite
is connected
muscle
the
end
posterior
spine,
median
of
portion
three
into
rectum
levator
the
cases
relaxed
until
escaping
be divided
may
parts, viz., a, the part which
of the coccyx.
fascia
and
last bone
the
behind
13
THEM.
penis from
the
prevents
cases
MEND
TO
dissection
may
and
in
originally a muscle
shown
by
vestigial in man,
it
From
ani
was
the
muscle,
origin,
it must
course
be
and
viewed
14
as
all-important
the
levator
The
ani
I think
support.
first
many
AND
muscle
fascia
it
was
happily
subjects it
who
In
VAGINA
THE
PERINEUM;
of
the
superior is
Dr. Meyers,
named
is
it the
membranous.
pelvic
the
real
floor.
visceral
German
physician,
pelvic diaphragm.
a
The
normal
and
modified
view
of
represents
a
1864,) Redrawn
modification
of Luschka's
L, L, the
figure consists
ani muscle
in magnifying
the rectal
made
by the levator
curve
; C, is
muscle
drawn
continuation
ani
of the
levator
backward,
lightly ; V,
a
The
ia
by the horse-shoe
grip on the rectum
sling of the levator
vagina.
here plain.
rolled
The
levator
ani fascia
inferior, p, is shown
up.
Fig. 4," (Luschka,
the
levator
^
ani
muscle.
TO
HOW
this boatshape of a boat, and when
the
pelvic floor is imcone-shaped,
of many
ani
is composed
levator
cular
muscoursing chiefly parallel to each other,
The
bundles
are
varying distances.
the
has
muscle
shape becomes
The
paired.
bundles
but
also
at
muscular
of
from
distance
connective
injury,
and
ani
muscle
serves
a
wide
another
in
held
are
useful
distention
at
color.
between
or
or
the
separate
and
reunite
purpose
in
pelvic
fat
Fenestra
bundles
the
less
or
of
the
of
The
greater
degrees.
varying
to
red
collections
by
observed
commonly
The
capacity of
are
loops.
levator
bright
a
fibers
one
tissue
apertures
of
and
flat, ribbon-like,
bundles
15
THEM.
MEND
cular
mus-
of
the
without
labor,
when
floor
may
rapid
occur.
muscle
distinct
as
a
figures illustrate the
between
the bundles.
plane with no parallel gaps
The
levator
ani
layer of the
(the deep muscular
the external
to
sphincter ani of
pelvis) is connected
and
the rectum
vagina (the superficial muscular
layer
of the
and
this
connection
muscular
to
by
pelvis)
the perineal body
(the punctum
fixum), the deep and
superficial muscular
layers of the pelvis are brought
of much
into intimate
relations
utility. A few fibers
lost in the
levator
ani
is in
The
perineal body.
are
closer
relation
the
than
Ihe
with
rectum
organic
the
rectum
vagina, because
requires more
frequent
and
than
the vagina.
It is chiefly
perfect evacuations
muscle.
of
weakness
its origin,
The
a
sphincter
Too
many
insertion
with
The
its
and
fading
forward
direction
out
of
of
horseshoe-shaped
loop
the
chiefly from
is
in
accordance
existence.
of
curve
its fibers
of
the
the
rectum
levator
is
due
ani, which
to
the
originates
pubis.
of the
posterior surface
of the lower, stronger fibers of the
By the contraction
lower
is forced
levator, the
portion of the rectum
to
against the perineal body, which
compels the anus
turn
backward
and
to
evacuate
its contents.
16
THE
levator
The
ani,
deficiencies
leaves
front
in
VAGINA
of
account
on
in
muscle,
coccygeus
PERINEUM;
the
its
shape
pelvic floor, which
bulbo-cavernosus
the
by
AND
and
its continuation
and
size,
filled
are
behind
by
the
backward.
lies
ani
palpable rounded
edge of the levator
above
the anus
and
threethree-quarters of an inch
the vaginal opening, making
quarters of an inch above
The
Fig. 5."
the
outlet
muscle,
in
of these
canals
internal
The
the
of
bundles
muscular
the
The
ani
levator
1889.)
(Dickinson,
as
and
the direction
pelvis is dotted
of the
levator
or
two
canals.
external
levator
averaging
marked
and
ani
about
closed.
force
or
from
as
noted
of
external
orifices
Normally the
They remain
will lift from
ten
course
the
skin;
the
chief
out.
fact, a regulator of the
always
are
ani
through
seen
open
ings
open-
of the
only by
trauma.
five to
twenty
by
Dickinson.
pounds,
Its
18
VAGINA
THE
AND
PERINEUM;
muscle.
wrote
Browning
levator ani
the subject. The
on
muscle, disappearing with the
this
process
from
arise
the
and
its fibers
the
double
of
erect
an
weakness
of
insertion,
fasciae.
as
It is
may
be
tail
and
rudimentary
a
in
the
attitude.
This
its
the
origin,
well
as
article
interesting
an
the
tionary
evolu-
view
may
direction
of
requirement
of
unphysiologio
for
a
muscle
V.
ani.
levator
after
distended
(Varnier,
The
Dickinson.)
F,
of the
vulva;
symphysis;
p,
c, clitoris; c, v, constrictor
fonrchette
neum
periperineum
A, anterior
P, posterior
; P,
; P,
; A. O, anus
with
the muscle
of sacrum
; C, R, coccyx
; P, S. point
; R, R, R, is on
In this
its separated
bundle.
the
middle
R
the
bundles,
is on
strongest
how
observe
the
itself from
by the
muscle
rupture
figure we
can
save
in one
of its various
if it were
fasciculi.
than
It yields better
separation
Fig.
bladder;
6."
s,
connected
to
can
sheath.
produce
be
not
rather
The
a
constant
considered
sphincter
levator
muscle.
ani
hence
support,
a
support
for
the
the
levator
ani
viscera;
it is
muscle.
muscle
Perhaps
from
is
an
analogous
to
the
tor
buccina-
evolutionary standpoint
HOW
we
look
may
viz.:
c, of
of
a,
a
of
tensor
a
tions,
having three funcelevator; and
sphincter; h, of an
levator
ani
fascia, superior and
levator
the
on
19
THEM.
MEND
TO
the
ani
as
inferior.
ani
is a
proof that the levator
sphincter, one
the
need
only introduce
finger into the vagina and
Cruveilmuscle.
the
request the subject to contract
tor
and
hier, Henle, Lesshaft
Budge insist that the levaand
lower
ani is a sphincter of the
rectum
anus
this
That
muscle
is an
chiefly, and not an elevator.
As
elevator
need
one
in
ending definitely
the
levator
ani
As
evacuated.
elevator,
an
rectal
the
elevated,
is
rectal
that
wall
is
completely
and
intra-abdominal
it resists
elevator,
an
elevate
only
the
as
such
illustrates
everted
mucosa
and
rectum,
defecation
in
muscle
the
action, could
in
horse
The
rectum.
find
it to
of the
walls
the
fibers, when
terminating
the
dissect
only
pressure.
The
male
levator
the
as
develop
to
those
ani
would
with
aid
to
superior and
They
originate
rectal
as
a
to
the
6, the
and
a,
outer
THE
The
of
internal
literature,and
blades
When
a
nor
ends
in
as
Roux
the
an
divide
part.
point,
lose
selves
them-
do
not
reach
muscular
fiber
neither
it will
wall,
INTERNAL
levator
the
layer, which
layer, which
is not
it
fascia
ani
active
an
and
its
which
not
act
elevator.
inner
fascia
take
in
tion
func-
chief
levator
fixed
walls.
nor
the
appear
greater
tail,from
fibers
definite
fascial
is
the
in
not
originally its
the
tensor
a
a
the
sphincter,
layers, viz.,
and
as
rectum
Lesshaft
tail,and
managing
at
vaginal
or
muscle
ani
inferior, these
between
goes
in
that
appear
a
does
labor
hence
levator
The
it.
animals
was
and
female,
developed
well
as
appears
is
a
PELVIC
of
often
the
lesser
ani
is
into
two
elevator,
an
sphincter.
FASCIA.
pelvis has
described.
As
the
a
poor
pelvic
20
VAGINA
THE
fascia
the
has
flap
somewhat
The
much
or
to
AND
do
PERINEUM;
with
perineal
any
in detail.
the
permanent
operation,
I
will
results
write
of
of
it
greater pelvis, or that fascia lying
superior to the ileopectineal line, is not here
sidered.
conThe
fasciae, the planes of strong, fibrous
tissue
under
the
here
pectineal
ileoconsideration, lie below
fascia
of the
line.
Fig.
7."
(Robinson-Scholor.)
the pelvic fascia,
to illustrate
line; 2, 2, origin of trans1, 1, white
versalis
and
iliac fascia
at the
iliac crest
ani fascia
superior;
; 3, 3, levator
4. 4, levator
ani fascia
intemus
inferior;
canal;
5,5, Alcock's
6,6, obturator
muscle
ani muscle
rectum
; 7, 7, levator
sphincter ;
or
; 8, vagina
; 9, external
10. 10, ileopectineal
line ; 11, 11, origin
of levator
ani fascia
superior
; 12, 12,
fascia
beginning of obturator
inferior
fascia
; 13, IS, transversalis
; 14, 14,
iliac muscle;
15, 15, iliac fascia;
fascia
16, 16, obturator
superior;
17, 17,
of obturator
fascia
inferior
ending
the ischial
tuberosity.
on
^
with
a
new
As
that
or
a
a
other
nomenclature
teacher
fascia
of
of
should
structure
A
diagram
same.
anatomy,
be
with
I have
named
which
always
according to
it is in
the
maintained
the
most
muscle
inti-
HOW
nomenclature
The
termed
will be
is divided
of
surface
call
that
of
fascia
The
the
pelvic aponeurosis,
the
pelvic fascia,
superior, and
levator
ani, the
named
after
sacrum
the
walls
the
of
the
pelvic
naturally
pelvic
floor,
but
be
treated
certain
continuation
an
of
the
iliac
fascia
the
name
iliac
and
lines
the
structure,
obturator
an
pelvic
fibrous
with
brane,
mem-
quality.
lesser pelvis should
transversalis
marks
median
the
and
the
extends
relations
strong, shiny,
varying quantity
independent
the
only
be
sacral
the
side to the
intimate
of
ing
cover-
will
pelvis
a
very
the fascia
levator
covering
of
of
fascia
fascia
lesser
either
into
enters
the
muscles
The
It not
floor.
a
sense
as
on
rior.
infe-
layer
ani
below
The
of the
fascia
ileopectineal line
The
takes
It is
viscera.
possessing
a
muscles.
the
by Carcassone
vesical
pyriformis
ileopectineal line
and
In
and
of
originally
levator
inferior.
fascia
ani
internal
The
fascia.
raphe
fascia
those
very
from
part of the
line
fascia
ani,
the
the
will
we
portion
levator
name
coccygeal
the
will
we
that
that
others
by
rior
poste-
white
the
rectovesicale, and
by Tyrrell the
named
the
above
the
obturator
the
fascia
spine,
above
superior, and
line
muscle
from
ischial
fascia
simple
this
As
extending
the
this
intemus
fascia.
to
the
white
the
obturator
pubis
fascia
below
fascia
the
portion
obturator
the
pelvis.
line
white
the
the
in
obturator
the
by
apply
the
covering
21
THEM.
therefore
fascia
the
to
fascia
shall
I
relation.
mate
MEND
TO
or
and
not
other
absolute
as
a
fasciae.
division
tween
be-
fascia.
The
the obturator
fascia
simplest plan is to describe
and
the
consider
obturator
to
superior and inferior
fascia as distinctly belonging
to the obturator
(interthe
fascia
of
nus) muscle, subsequently to consider
the levator
ani superior and inferior, with
a lesser
sideration
con-
of the
The
connected
coccygeus,
fasciae lining the
with
their
pyriformis
lesser
pelvis
respective associated
and
are
sacral
ciae.
fas-
intimately
muscles
and
22
THE
VAGINA
by strong
structures
of the
PERINEUM;
AND
connective
fascise with
The
tissue.
tion
connec-
is not
the
intimate,
peritoneum
tissue, richly laden
thick, loose layer of connective
a
and
the
the peritoneum
with
fat lobules, lies between
lining the lesser pelvis. This loose connection
of pelvic peritoneum
and pelvic f ascise allows the easy
between
the peland
vic
rapid spread of pelvic abscesses
in the
fasciae and the peritoneum
subperitoneal
fasciae
tissue.
Fig.
8." (Ranney.)
It illustrates
below
the
levator
Diagram
section.
the
and
ani
of the
fascia
ani
fascia
levator
of the
pelvic floor in
and
superior
T, L, triangular
muscle.
a
mesial
above
inferior
ligament;
P, F,
two
layers of
superficial
fascia.
Observe
in the anterior
gular
trianperineal
that
there
perineal
five
layers of fasciae, viz. : 1, superficial
space
are
of perineal
layer
fascia
fascia
layer of superficial
perineal
; 3,
; 2, deep
triangular
outer
inner
ligament,
layer ; 5,
layer ; 4, triangular
ligament,
levator
ani fascia
In the posterior
there
two
siiperior.
perineal space
are
the levator
layers of fascia"
ani fascia
ani fascia
the levator
superior and
inferior.
The
obturator
muscle
of
of
a
the
the
internus
at its
origin, from
innominate
obturator
considerable
fascia
the
bone, and
muscle.
internus
distance
surrounds
to
the
the
rator
obtu-
lateral
is the
It is
iliac
face
pelvic surspecial fascia
attached
portions
of
for
the
HOW
the
to
this
At
brim.
border
upper
front, the attached
ileopectineal line
the
to
nerve
obturator
the
point
of
line
of the
the
enter
In
membrane.
fascia
the
attached
becomes
obturator
the
allow
to
23
THEM.
MEXD
TO
below
the
vessels
and
passes
obturator
foramen
obturator
or
canal.
as
portion is fixed to the periosteum and appears
In front
to the
it is attached
independent
an
organ.
margin of the
body of the pubis and along the upper
foramen
obturator
by an oblique line, to a point about
Where
the
inch
below
half
the
symphysis.
onean
of the obturator
the passage
to allow
fascia dips under
to the periosvessels
and
it is firmly attached
teum
nerves
riorly,
Postefibers.
and
by strong tendinous
nerves
This
it is
attached
the
to
of
surface
anterior
the
margin of
ligament and the anterior
great sacrosciatic
notch.
the great sacrosciatic
Inferiorly, the fascia is
of
of the
foramen
obturator
attached
to the
margin
of the
the
descending
pubis, and it joins the
ramus
of the
falciform
ligament,
great sacrosciatic
process
border
of the
the
it
inner
to
which
firmly connects
and
its ascending ramus.
ischium
With
insertion
in the
ileopectineal line, the
a firm
anterior
border
anterior
and
of
the
inferior
great
margin
of
the
the
foramen,
sacrosciatic
foramen
obturator
of thjB great
edge of the falciform
process
fascia becomes
sacrosciatic
a
ligament, the obturator
in
relation
fixed, strong, thick, fibrous
membrane,
vessels
and
and
nerve
superiorly with the obturator
and
inferiorly with the internal
pudic vessels
nerves
and
"
to
the
Alcock's
obturator
canal.
internus
It has
intimate
muscle
above,
attachments
but
is
to
quite
the
loose
below.
The
obturator
fascia
we
divide
into
two
portions,
superior
fascia
obturator
The
superior and inferior.
line or arcus
tendineus.
is that portion above
the white
It looks
the lateral
into the pelvic cavity from
aspect
The
and
and
is covered
by peritoneum.
peritoneum
24
THE
VAGINA
AND
PERINEUM;
able
separated by considersuperior are
connective
tissue, composed
loose, fatless, snow-white
of many
planes, which
shiny, thin, cleavable
fascia
obturator
dissected
easily
become
the
by
of
progress
pelvic
abscesses.
The
internal
head
fixed
bony ring
The
of
its
the
surface
a
tendineus
ischiorectal
the
obturator
fossa
of the
fossa
for the
"
The
nerves.
of
of the
fascia
lesser
the
At
notch
sciatic
of the
pelvis with
postero-femoral regions of
out
passes
is inserted
fascia
pubis, where
ligament
is
each
a
into
the
fascia
the
the
the
of
ramus
plane"
size
a
and
The
and
surface
of the
gains
the
obturator
and
ischium
the
turator
ob-
fascia
obturator
thigh.
the
vessels
has
muscles
the
part
Alcock'"
"
pubic
inferior
five square
inches, one-half
fascia superior.
some
external
above
sheath
a
the
lower
inch
obturator
transmission
obturator
toward
the
At
an
below
internally
the
forms
about
the
tuberosity of the ischium
become
separated, producing
Canal
It looks
fossa.
fascia
portion
externally
It
ischiorectal
ischiorectal
the
and
or
inches.
square
line.
brim
obturator
is that
muscle.
internus
boundary
ten
the
by
and
injured by
to be
engagement
pelvis. The
white
vessels
obturator
inferior
or
low
superior just be-
liable
are
of about
fascia
obturator
arcus
into
after
the
are
the
over
pass
fascia
obturator
structures
soon
superior has
of
the
These
which
importance
ileopectineal line
nerves.
'the
of
face
the
the
of
structures
it passes
and blends
with the trianguon
lar
of the urethra, hence
the triangular ligament
continuation
of
the
or
white
from
fascia
obturator
side.
The
tendineus
arcus
aggregation
gentle
tendinous
It extends
fascia.
pubis
of
to
curve
the
spine
with
from
of
its
line
fibers
the
the
of
appears
the
concavity
It
upward.
an
obturator
posterior surface
ischium.
as
of
the
possesses
The
whit"
a
26
VAGINA
THE
If
AND
PERINEUM;
the peritoneum
and loose
carefully removes
subperitoneal tissue the levator ani fascia superior
be plainly seen
stretching from the white line to
may
the bladder, vagina and
It may
rectum.
be stripped
off the levator
ani
muscle
in
several
thin, cleavable
the
the bladder
planes. It is reflected
on
forming
anterior
true
and lateral true ligament of the bladder,
one
however
ligaments of the bladder
the
by ligaments from
vagina. The
assisted
ani
fascia
the
lower
along
lateral
the
the
superior
border
white
begins
its
of
symphysis,
line
the
anterior
laterallyto
be
may
'
levator
attachments
at
then
continues
the ischial
tinues
spine, confrom
the ischial spine on
the
superior surface
of the levator
ani muscle
The
to the median
raphe.
levator
ani fascia superior covers
of about
six
an
area
inches
square
side
each
on
of the
line
median
of
the
pelvis.
The
the
levator
anterior
fascia
ani
into
be divided
superior may
portion, the vaginal portion and
vesical
or
the
rectal portion.
The
vesical portion
is
reflected
from
bladder, forming the
bladder
and
portion
It is reflected
The
of
the
from
thick
the
levator
pubis
anterior
part of the
is very
the
lateral
and
pubis
to
fascia
ani
the
neck
ligaments
true
ligaments.
strong, even
in
an
arched
The
rior
supe-
of
the
of
the
cal
vesi-
tendinous.
manner.
vaginal portion of the levator ani fascia superior
is analogous to that which
surrounds
the prostate in
the male.
In the male, the prostate gland and
vesiculse seminales
surrounded
are
by a strong capsule
derived
from
levator
ani
fascia
superior. This
tion
porcluding
of fascia surrounds
the vagina in the female, inthe large venous
plexuses.
The
considerable
with
vaginal portion is endowed
is lost on
with
and
blended
strength and it becomes
the vaginal wall.
The
rectal
portion of the levator
ani fascia
rectal wall, becomto the
superior passes
HOW
MEND
THEM.
fibers
and
the
with
continuous
ing
TO
27
strong fillet passing between
The
part of this fascia
vaginal canal.
There
is
rectum.
This
the
muscular
wall
of
It
serves
of
layers, which
the
example,
fascia
of
to
support
space
end
to
that
of
the
region.
levator
found
parts
from
tioned
men-
the
fascia
defined
distinctly
many
that
say
in
not
many
the
over
facts
in
one
in
cleaved
be
can
the
of
consists
pelvis
the
passes
ligament
strong
I have
is that
books
the
in
rich
which
subject
A
muscle.
ani
the
a
for
attachment
an
which
and
rectum.
very
fill in
an
as
forms
the
argument
perineal body is to
the
termed
been
fascia
the
It is not
has
wall,
it.
rectal
the
a
rectal
the
to
with
blending
each
other.
coccygeal
muscle
For
may
several
be
layers, and the same
may
of the
levator
ani
degree
said, but not to such
a
Several
planes of fascia
thin, transparent
superior.
off of the obturator
fascia
be cleaved
superior.
may
is very
thin
Even
the levator ani fascia inferior, which
be cleaved
into two
and
planes.
or
more
compact, may
off in
cleaved
be
"
"
The
fibrous
side
of
plane
and
fascia
but
planes
thin
into
inferior
fascia
obturator
and
is known
of
planes
the
of
resisting
The
ischium
inserted
sacral
in
other
The
coccygeal
and
into
vertebrse.
fascia
cleavage
localties
a
and
arises
sacrosciatic
side
It
is
the
by
the
plane
planes
are
a
thick,
brane.
mem-
is
sels
pubic vesseparation
membranous
pelvis endow
tear
may
it
without
characteristic
are
capable
more
of
single plane.
muscle
lesser
the
One
of
the
is
inferior
several
in
each
on
fibrous
fascia
canal.
powerful
very
coarse,
formed
than
trauma
plane
canal
the
Several
central
transmission
utility.
more
other.
fascia
of
some
much
with
Alcock's
as
cleaved
obturator
the
The
nerve.
be
may
the
powerful
split, for
cleaved,
a
somewhat
powerful, individual,
The
is
of
a
the
flat
from
the
spine
ligament,
coccyx
and
of
the
becoming
two
musculo-tendinous
lower
tri-
28
angular plane, aiding
Its
of
backward
fascia, viz., the levator
bounds
the
posterior border
foramen.
great sacrosciatic
the
the
of
the
The
animal.
and
muscle
They
that
involved
be
in
coccygeus
that its fascia
fascia, which
of
surface
strengthened,
the
coccygeus,
of
the
levator
ani
is
fading
out
of
tailed
large
a
the
coccygeus
ligament are identical.
yield
practically they never
ever,
Howcolpoperineorrhaphy.
should
the
only
not
is
described
be
named
of
admit
not
can
degeneration
a
originally to
muscle
the
show
sacro-
sacrosciatic
strong
so
are
to
as
lesser
of
margin
of
muscle
insertion
by
superior.
lesser
by
fibers
coccygeus
belonging
origin and
existence,
fascia
The
continuation
the
The
inferior.
fascia
of
place of
the
takes
covered
anterior
formed
is
ligament, which
superficial muscular
sciatic
and
ani
same
The
so
let.
posterior pelvic outwith
the postecontact
rior
of
it is
which
muscle,
ani
continuation
practically a
the
is in
levator
the
PERINEUM;
close
to
border
anterior
border
AND
VAGINA
THE
the
The
muscle
lesser
to
coccygeal
confusion.
coccygeus
by the
order
in
is
rior
infe-
doubly
sacrosciatic
ament,
lig-
superior surface of the great sciatic
of the
represents the proximal tendon
ligament which
The
tendon
of the
long head of the bicep femoris.
attachment
at the
an
long head of the biceps formed
but
tuberosity
the
covers
3J
by
the
the
ischium.
coccygeus
muscle
of
inches
square
each
on
The
and
has
of
side
pyriformis muscle
pelvis. The
lateral portions of the second, third
the
sacrosciatic
ligament.
great
the
outlet.
the
It
foramen,
of
the
posterior muscle
It
serves
of
out
passes
border
inferior
from
and
notch
sacrosciatic
upper
most
from
sacrum,
as
a
bed
line
fsom
arises
and
great
fourth
of
the
pieces
great
sacrosciatic
pelvis through
inserted
becoming
trochanter.
in
which
closing
the
of
the
the
the
aids
on
of about
area
median
border
the
great
which
an
the
the
of
fascia
coccygeus
into
It
is
the
pelvic
sacral
nerves
the
HOW
It
rest.
may
which
is
and
is
of
the
obturator
out
into
fascia
by the internal
pelvis by the great sciatic
nal
is attached
to the
of
origin
line
the
which
It
of
the
the
to
from
the
the
ileo-
of
border
the
joint and finally
of
the
it is attached
to
the
superior
margin
great
from
the
ischial
foramen
sacrosciatic
spine to the
fascia
The
sacro-iliao
pyriformis
an
point.
covers
the
of
wing
of
area
five
The
pelvis.
to
sacrum
about
we
sacro-iliac
inches
square
is lined
sacrum
which
the
inter^
sacrum
muscle
along
passes
the
pyriformis
muscle
pyriformis
rated
perfo-
leave
The
coccygeus
is
which
foramen.
surface
the
of
border
posterior
pectineal
the
to
leaving
rapidly thins
it
vessels
above
After
membrane.
iliac
fascia
fascia
obturator
and
fascia,
pyrifonnis
anteriorly.
coccygeus
transparent thin
a
the
the
fascia
coccygeus
29
THEM.
by
covered
continuation
a
the
MEND
TO
will
by
the
name
each
on
a
thin
the
of
side
fibrous
brane
mem-
fascia; hence,
sacral
lined
fascia
by the obturator
superior, the levator ani fascia superior, the coccygeal
the
sacral
fascia.
fascia, the
fascia, and
pyriformis
This
nomenclature
recommend
we
as
as
simple, and
facilitatingthe easy acquisition of the internal fascige
of the pelvis.
the
internal
The
pelvis
of
use
the
sustain
the
is
levator
pelvic viscera,
ani
fascia
and
is
tranversalis-abdominalis; b,
each
for
side
the
analagous
to
is
superior
form
pelvic viscera, which
:
the
to
pouch
a
in
assists
a,
to
cia
fason
ing
clos-
pelvic outlet above the muscular
floor; c, to fix
the pelvic viscera; d, with
its superior pad of fat and
the
snow-white
connective
pelvic
tissue, to support
of the abdominal
peritoneum;
e, to resist the
pressure
the
muscles
and
purpose
of
diaphragm, and/, to
separating the perineal
the
serve
the
tissue
from
useful
the
peritoneum.
This
and
latter
infective
anatomic
processes
condition
from
limits
either
inflammatory
perineal
or
peri-
30
THE
AND
VAGINA
PERINEUM;
Further, the levator ani fascia superior
forms
the
pelvic floor, and by its strength prevents
The
blood-vessels
placed sijperior
are
pelvic hernia.
toneal
and
spaces.
the
Fig. 9."
of
torn
shown
with
by
thread
inferior.
nerves
An
(Author.)
pelvic floor
the
intervening
R, R,
R, R, and
illustration
the
pass
on
through
integrity
the
ani
the
right
the
levator
to
levator
muscle,
its
(X) will
The
muscle
demonstrate
side.
and
that
in
superior
and
The
ani.
The
needle
rent
fascia
levator
fascia
ani
its two
ations
lacer-
deep
inferior
is
tear
is
the
or
with
armed
layers
su-
of
fascia
in
XL, iliac fascia ; Up, the
pelvic floor.
the
at
line;
fascia
of the
obturator
ischiopectineal
beginning
superior
line ; O, the
obturator
the
white
fascia
superior
OS, the obturator
; W,
internus
white
fascia
inferior
divided
line; I. O, the obturator
by the
fascia
levator
ani
ischiorectal
fat in
the
A, the
F, the
fascia;
muscle;
fascia
S, intrapelvic
inferior;
V, the vagina;
B, the obturator
superior;
and
cervix
transverse
2, the superperineal muscle,
ficial;
; Y, the
; P, deep
space
ani
M, deep
ment;
ligalayer of triangular
B, the sphincter
externus;
S, superficial;
N, deep layer of superficial perineal fascia.
order
to
restore
the
of
the
HOW
and
perior
to
the
by
inch
levator
and
tissue
to
tissue
fascia,
the
ani
fascia
one
from
the
and
into
cocygeus
neal
subperitothe
in
occur
fat.
with
of
consists
of
margin
from
the
thin
a
esses
proc-
The
sion
exten-
an
levator
superior and
fascial
planes blend, the
Both
anterior
other
nective
con-
obturator
superior.
the
to the
filled
are
of
infective
tissue
muscles
the
sheaths
allow
of
perforated
it is
Deficiencies
versa.
and
in
disadvantage
carry
perineal
which
of
fistulse
is that
superior
pyriform
the
A
sheaths
vice
backward
anus.
these
excavations
of
all
which
;
and
nearly
vessels
from
pass
the
fascia
ani
nerves
fascia
above
31
THEM.
limits
inferior
one-half
MEND
TO
the
men
fora-
sacrosciatic
of
posterior margin
membrane
which
the
the
covers
muscle
and
the
sacral
pyriformis
plexus of nerves.
The
pyriformis fascia is perforated by the gluteal vessels
and
the
This
to
nerves
gain
plane
gluteal region.
of
fascia
dissect
is
it without
(anal
and
becomes
ani
fascia
connected
one-half
rectal
the
included
all
the
the
fascia
coccygeal
it has
sacrum;
The
to
of
localized
portions
margins
of
anterior
sacral
the
are
of
ani
anterior
thickenings
those
sacram
and
foramina.
The
located
anus,
the
may
sertions
in-
fascia
this
fibers
relations.
the
the
colpo-
extensive
its
levator
normal
lines
thickest
the
of
rectal
below
occur
fibers
deep suturing
including
By
is very
levator
the
above
the
white
It
with
inch
The
the
at
The
blend
generally
fascia.
relations
restored
and
inferior
of
surface
wall.
ferior
in-
immediate
in
muscles.
to three-fourths
perineorrhaphy.
sutures,
and
the
fascia
ani
begins
rectal
scarcely
can
lies
inferior
fascia
with
above
in
the
one
levator
fascia)
the
on
perforations
of
are
lost
superior
wallabout
and
This
that
The
it.
with
muscle.
intimately
delicate
tearing
contact
ani
and
and
ischiorectal
or
intimate
levator
line
thin
so
in
the
be
tially
par-
The
surface
sacral
of
the
and
thinnings
eral
along the lat-
especially
around
the
triangular ligament
32
(deep perineal fascia)
extending from
prolongation of
fascia
It is
a
of
union
the
sides
the
obturator
the
fascia
in
obturator
the
toward
both
floor
pelvic
the
in
closes
of
result
It is the
front.
PERINEUM;
AND
VAGINA
THE
center.
the
across
interit the
called
ligamentum
pubis, and Winslow
the
perineale;
ossei pubis; Carcassone,
ligamentum
It is
triangulare urethrse.
Colles, the ligamentum
of the fascia perinei and is an
integral
the deep blade
of
insertions
middle
fascia
It
fills up
Camper's
ligament.
between
the
levator
the
the
It is
fascia.
part of the obturator
of the
perineum, or
the
deficiency found
powerful structure
vagina. It is stronger
ani
in
in
anterior
It is
muscle.
fixing
the
lower
than
males
in
pubic
or
a
fully
wonder-
end
of the
females.
It
powerful grip,
retains, with
and
of the vagina forward
end
upward.
the anterior
The
triangular ligament whose
pierces the
vagina
around
the vaginal walls.
in and
fibers fix themselves
ferior
the lower
It joins posteriorly with
margin of the inIf one
edge of the superficialperineal fascia.
from
the
all structure
dissects
vagina except
away
the
apparent at
triangular ligament it will become
end
what
powerful support it is to the lower
a
once
The
of the vagina.
triangular ligament, as its name
ture,
implies, is triangular in shape, aponeurotic in structhe anterior
extending as a tense septum between
and
on
pelvis. It is attached
part of the perineum
rior
Its infeeither side to the rami
pubis and ischium.
margin is ill-defined, blends
posterior inferior
or
at the
ischioperiwith
the superficialperineal fascia
is
the
fascia, where
neal
surface
lower
fixes
and
vagina
useful
to
which
structure
the
fixed
the
it
the
of
purpose
pubis,
relations.
levator
urethral
at its base
or
gradually
ani
can^.
weakest
itself
loses
It
muscle.
It
is
portion.
on
sustains
pierced by
It
the
serves
the
the
and
vagina
connecting the bladder
in
of retaining
and
adjacent organs
ischiothe
with
By its connection
of
34
THE
VAGINA
AND
PERINEUM;
bands
of
aponeurotic
a
resisting character.
very
of the
lower
of
the
union
border
They result from
the
triangular ligament with the deep layer of the
The
fibers of these
superficial fascia.
ligaments play
role
in
extensive
an
important
colpoperineorrhaphy.
These
in every
ligaments form a conspicuous structure
of the female
dissection
In the advancing
perineum.
head
the
the
ischioperineal ligaments are
put on
stretch
and
Should
gradually forced backward.
they
rupture, by extensive
flap-splittingand deep suturing
the two
blend
the ligto make
layers of fascia which
ament
could
be partially restored.
the
of the pelvis in
structure
Having examined
detail
we
which
explain
may
now
combine
the
anatomic
factors
The
colpoperineorrhaphy.
first is the restoration
fascia.
A second
of damaged
A third
element
important factor is deep suturing.
in a successful
of function
operation is the restoration
of restored
muscular
relations.
A fourth
is
by means
the forcing in the
median
line of adjacent perineal
of operatissue, and a fifth factor is the flap method
tion
of
loss
there
denudation
is
tissue,
whereby
no
or
and
the flaps (skin and
and
mucosa) avoid infection
insure
enables
flap method
primary
healing. The
the operator
to reach
the seat of the
lesion, either by
handled
or
a
splitting tissue
deep suturing with
with
needle
Silk- worm
in the end.
an
gut which
eye
for
is used
in suturing, being non-septic,
remain
may
weeks
in
removing.
position, like a splint, before
the fasciae of importance
levator
ani
The
Among
are:
inferior, the
triangular ligament and
superior and
perineal
ischiothe
deep layer of the superficial fascia, and
The
rhaphy
ligament.
operation of colpoperineorof
is the
result
of evolutionary
processes
In the beginning, it was
failures
and successes.
sidered
conthe
sufficient
to unite
superficial or external
This
tissues
the
lesion.
at
site of the
experiment
successful
HOW
demonstrated
soon
its
essential
deemed
muscular
attempt
elements
external
tissue
the
it
deranged
and
pelvic
floor.
the
in
later
the
at
of
site
lesion
the
was
ated
lacer-
colpoperineorrhaphy by
successful
at
failure, and
own
restore
to
35
THEM.
MEND
TO
The
ing
reuniting
restor-
or
relations
to normal
deranged or lacerated muscles
evident
proved a failure to such a degree that it was
factor
other
that some
played a role; this factor was
the
fascia.
the
site
muscles,
factors
played
of
credit
the
given
important
an
Dr.
view
role
in
Experimental
desultory
clear
what
successful
All
anatomic
in
colpoperineorrhaphy
The
basis.
that
to
operations
various
inguinal canal,
impossible
for
the
be
restored,
the
but
so
restored
be
for
hernia.
ideas
who
are
to
its valve-like
to
only
again
the
suggest
the
that
in the
if
the
manner
a
ful
success-
process
hernia
ground
views
sutures
of
have
have
as
must
we
obliquity
of
the
makes
action
protrude.
anatomic
canals
various
restore
involved
tomic
ana-
render
to
The
In
be
base
and
as
in
hernia.
it
poperineo
col-
In
parts should
and
restored, to ensure
permanent
suturing, so essential, is only groping
also
fifty
rhaphy.
colpoperineor-
in
evolutionary
viscera
not
for
on
colpoperineorrhaphy
in
for
that
so
be
must
pelvic fascia
rhaphy.
colpoperineorperineum, in a
carried
relations, the
anatomic
the
restore
neorrhaphy
colpoperi-
experimental
must
surgical procedures
passed through the same
the
the
on
methods
operation
in
at
surgical procedures demand
deranged and lacerated parts
an
similar
the
successful
have
useful
the
are
tissue
Emmet
judiciously combined
been
data
that
been
only lately
But
years.
A.
labors
have
manner,
T.
the
lacerated
successful
which
on
To
rests.
the
deranged and ruptured
of
the
deranged fascia
the
restoration
the
three
the
are
and
with
wound,
of the
of
restoration
The
outlets
Deep
success.
after
work.
include
an
The
discerning
must
tomic
anasame
surgeons,
sufficient
of
36
THE
VAGINA
AND
PERINEUM;
the
rectovaginal septum, or if they are
forward
to make
deep enough
traction,
include
sulcus
the
vaginal wall, the
W.
R.
Wilson
side
either
on
operation
will
short
but
wrote
a
of
be
introduced
if
or
the
they
bulging
successful.
Dr.
cle
articomprehensive
excellent
principles,
the
subject, suggesting
but modestly claiming that the anatomic
basis is still
In
the
imperfectly understood.
subject of colpothe
perineorrhaphy
origin of the lesion demanding
on
should
operation
be studied.
requiring repair,
first)labor, more
pubic
from
the
hernia.
the
rarely
The
forward
levator
almost
is
ani
The
always
other
lesions
the
the
lesion,
of
result
forces"
produce
of the perineum
may
of
movement
fascia
of
cause
head
the
superior and
(the
sacrocome
jlacerating
inferior, with
age
dam-
to the
ischioperineal (ligament) fascia and tearing
of the triangular ligament, with
inevitable
consequent
lesion of the deep perineal fascia.
This
will destroy
the
of the
tone
the
posterior vaginal wall, because
fascia has
been
the vaginal wall
separated from
near
its outlet.
If the distinct
ischioperineal (ligament)
fascia be torn, which
is quite frequent
in labor, the
vulvar
end of the vagina falls backward
and
begins its
condition
of rectocele; its fascial (and doubtless
cular)
mushave
supports
levator
fascia
ani
descend,
act
as
it must
the
pelvis
by
separate
means
for it is
be
With
away.
and
for
unphysiologic
tensionized
remembered
not
are
torn
superior the pelvic viscera
continuous,
a
But
but
been
only
that
of
distinct
value
a
muscle
for
fascial
visceral
as
torn
will inevitably
support
the
a
to
viscera.
layers
of
supports
themselves,
of significant importance
they are
as
serving a
of visceral
ment
and
for a point of attachsupport
for
levator
muscles
lying
ani, which
apparatus
attachments
is
the
on
as
a
the
pelvic
visceral
connection
between
most
floor,
in
their
important
serves
support
to
The
blades.
by
the
muscular
its
fascial
rectal
and
*
HOW
walls
vaginal
well
as
MEND
TO
is
the
supported by
The
pelvic floor may
two
widely overlapping
uterus
of
relations
the
pubic hernia.
the
bladder,
The
pelvic floor, for
intact
pelvic floor.
considered
composed
as
be
valves
toward
tends
vaginal
drethra, anterior
turbs
dis-
.
pelvic valve
anterior
of
Whatever
( Hart)
valves
these
the
the
to
as
37
THEM.
is
sacro-
of
composed
and
wall
pubic
retro-
of the
posterior pelvic valve is composed
The
and rectal wall.
posterior vaginal wall, perineum
is attached
to the
pubis and
symphysis
pubic segment
The
of loose
connective
tissue.
retropubic
composed
be easily
fat is loose and
the peritoneum
may
spongy,
from
the bladder
from
the bladder, and
stripped away
elevated
becomes
the vagina.
In labor, this segment
fa
The
,
and
is
the
easily
which
one
especially
and
acquires pathologic conditions
hernia.
to prolapse
or
sacropubio
fascia superior becomes
torn
away
bladder
the
and
When
the
anterior
The
strong levator
torn
when
from
the
prolapse
planes of
from
the
wall
vaginal
and
and
ani
the
fascia
fascia
same
bladder
it
been
has
with
peritoneum
subperitoneal (fascia)
bladder.
The
sacral
downward.
hernia)
from
its
extensively
also.
its
first.
vulva
torn
been
prolapses
the
the
at
has
of
intra-abdominal
vagina
appears
ani
walls
the
(sacro-pubic
prolapses
uterus
the
walls
bladder
the
from
or
is liable
levator
The
the
vagina, allowing
force
to
pressure
deranged,
becomes
many
In
vesical
cleavable
tissue
becomes
valve
of
the
torn
pelvic
floor, consisting of the
posterior vaginal wall, the
and
is attached
by strong fascial
rectum,
perineum
and
to the coccyx
connections
interwoven
by muscles
backward
In
is forced
sacrum.
labor, this segment
and
defective
If it becomes
by
straightened out.
laceration
at the
perineal body the vagina loses its
is initiated, i. e.,
and
normal
sacro-pubic hernia
curve
retroversion
sacropubic
begins,
hernia.
which
The
is the
uterus
inevitable
itself
has
factor
in
nothing
to
38
VAGINA
THE
do
with
AND
Intra-abdominal
prolapses.
defective
sacral
the
PERINEUM:
and
pressure
for lapse;
account
pro-
and
pubic segments
is fixed; the pubic segment
segment
sacral
is movable.
functions
The
resist
intra-abdominal
vesical
and
the
to it
as
must
individual
should
organ
has
The
uterus
though
should
be
be
studied
its individual
from
separate
the
in
of
general
fascia
but
regards
as
rectal
anatomy
studied
and
to
are
allow
to
structural
only
be
floor
each
its supports.
supports, which,
and
muscles,
fascia
well
considered, for colpoperineorrhaphy
hernia
required for (prolapse) sacro-pubic
be
may
and
The
not
pelvic
valves, muscles
segments,
not
the
pressure
functions.
floor
pelvic
of
required
without
visible
lacerations.
of
supports
The
the
first elemental
uterus
the
are
vidual
indi-
uterorectal
of two
of
folds
(sacral) ligaments.
They consist
muscular
and
connective
sue
tisperitoneum
embracing
the posterior surface
of the cerextending from
vix
to the rectum
do
fibers
extend
to
(perhaps some
sacral
the
fascia). These
ligaments are an extension
of the
end
muscular
of
the
notes, the
balance
conneclive
vagina
vagina
beam
should
be
backward.
and
in
fibers
of
Dr.
Frank
As
uterorectal
which
on
borne
tissue
mind
the
that
uterus
uterorectal
muscular
and
the
ligaments
connective
are
bands
became
These
support
descend
without
the
a
Yet
it
rest
on
mesenteries.
or
all
organs
suspended
or
dissections
uterus
not
not
form
bases.
powerful, peritoneal,
which
pend
vigorously sus-
Careful
by the neck.
vaginal hysterectomy will demonstrate
eould
rests.
do
organs
upper
Foster
ligaments
bases, but .are swung
on
supports
The
uterus
brain, liver, heart and
are
and
do
other
not rest on
by supports
The
the
that
uterorectal
the
and
uterus
ligaments
elongated.
ligaments are a part
of the pelvic viscera.
of
the
The
musculo-fascial
vaginal
tube
sup-
ports the
and
tor
by the levaby being well embraced
levator
the
ani
muscle,
superior and
and
surrounded
by
being well padded
uterus
fascia
ani
39
THEM.
MEND
TO
HOW
also
by
fixed
fascial
in its walls
tissue
planes of connective
Fat
and
adjacent structures.
pads and acts as a support
by stiffening folds.
In colpoperineorrhaphy,
that
it is well to remember
and
movable
fixed
have
dispelvic segment
or
we
a
a
It will aid in repair.
The
placeable segment.
able
movthe
urethra, bladder
pelvic segment
comprises
This
and
is bound
together
vaginal walls,
segment
mobile
base
and
siderable
by a conon
a
by peritoneum
very
of
mass
This
segment
bladder, vagina
become
torn,
fascial
connections
inferior
and
to
Sacropubic
of
inside
inevitable.
is
considerable
are
the
levator
some
extent
hernia,
of
of
above
fasciae
ani
arising
vulva
from
The
the
vulva,
and
superior
levator
the
muscle.
ani
lacerated
laceration
progress
high up in
as
appear
The
gone.
and
fascia
are
which
i. e.,
with
waist
and
worst
those
outward,
a
the
ing
damag-
most
begin
the
from
fascia
the
begins
the
the
rectovaginal septum, on
of the bladder
and
These
the cases
vagina.
are
when
present distressing symptoms;
standing
tear
are
hernia
connections
is recognized
pelvic segment
by the
bladder
the vulva
at
bulging downward
cases
which
its fascial
movable
the
sides
If
rectum.
or
tissue.
displaced by labor, distended
becomes
vagina and
and
the
making
puckering string
to
connective
sacropubic
of
consisting
loose
worse
on
pronounced
of
account
"prolapse"
disturbed
circulation
and
are
the
In
by
general physician.
such
the
anterior
first at
cases
vaginal wall appears
the vulva, then
the
and
cervix
finally the posterior
The
bladder
downward
vaginal wall.
gradually sags
and
difiicult urination
is added
to the
already existing
train
of
symptoms.
of
the
pelvis
In
the
lacerations
lesions
are
of
more
the
sacral
visible.
ment
segThe
40
THE
perineal
body
the
sacral
fixed
of
the
AND
suffers
subsequent
laceration
VAGINA
perineal body
requisite
colpoperineorrhaphy.
fascia
shows
the
why
Frequently it may
is visibly torn,
because
belongs
head
fixed
levator
the
muscles.
are
two
well
or
succeeded.
also
of
the
the
descends
which
of
boat
a
floor.
bowl
or
The
muscles
from
and
the
to
All
levator
ani
i. e., the levator
deep transverse
and
ligament
of
center
the
which
perineum,
bulbo-cavemosus,
outlet.
of the
which
muscles
inclosed
muscles
Colles
are
importance
apparent,
of the
not
only
fascia
in
also
fascia, as
fascia,
the
Colles
verse
trans-
of
lie
the
vic
pel-
vaginal
inferior.
fascia.
of
the
to
the
fropa the
superior and
between
in
and
blades
double
The
triangular
bulbo-cavernosus
The
muscle
superficial transverse
The
superficial perineal fasciae.
thickening
ligament and
the
extend
related
cle
mus-
the
perineum
and
the
ani
on
surrounds
in
fascia
ani
the
fascial
pelvis
of
floor
blended
and
attachments
to its
restores
pelvic
the
superficial layer consists
of the
tuberosities
sides
the
fascia
ani
levator
the
is
rectum
fascia
of
layers
layer
follow,
prolapse,
advancing
not
"
deeper
pelvic
perineal body
superficial and deep connected
perineal body both by the muscular
The
type of
ischioperineal ligaments,
becomes
deranged
"
relations.
is but
the
levator
the
as
muscular
visible
of
the
the
restoration
The
The
consequences
intact.
The
muscle
ani
ble
inevita-
the
failed
that
tears
as
and
out
also
study
evil
and
inferior
practically the
the
the
remains
forward
but
the
But
and
It does
segment.
stretches, elongates. As
the
form
repair
no
to the
forces
the
for
observed
but
fascia
superior and
at
straightens
ered
originally consid-
was
operation
be
the
its wall
but
It
especially.
segment and retroversion
sacropubic hernia results.
the
chief
PERINEUM;
lie between
the
ischioperineal
lower
fascia.
border
The
of
two
fascia
the
angular
tri-
significant
at once
pelvis becomes
maintaining the integrity of the
of the
42
THE
lacerated, but
tooele
ble
a
bag
the
In
which
different
AND
PERINEUM
prolapsed vagina,
vesicocele
degree.
like
is
and
VAGINA
appear
fact, as
has
Dr.
lost its
at the
the
vulva
bulging
in
a
rec-
remark-
Emmet
remarks, it looks
puckering string. There
explanation for each of the above classes.
In one, the pelvic fascia
has
suffered
in the
lesion,
and
in the other, only a few
muscle
loops and
bly
possithe perineal body.
When
the lesion involves
the
pelvic fascia its consequent
tion
result is that the circulais deranged
the
vessels
seriously, because
are
held in definite
relations
by the fascial planes, hence
the
discomfort
on
standing and exercising is from
Baker
Brown
the torn
congestion.
simply united
tissue at the vaginal outlet.
does
Seldom
this simple
afford any
real relief from
ation,
measure
perineal lacerfor subjects with
such
visible slight traces
fer
sufbut little.
In general the operations for the relief
of perineal laceration
failure.
If the rectovaga
are
inal
and
be
not
septum
(fascia
muscle)
brought in
the grasp
of the deep sutures
will not
be obtained
success
The
secret
even
though the vulva be closed.
of Emmet's
success
lay in the denuding of the vaginal
i. e.. utilizing the tissue
septum,
posterior to the
In fact, if the levator
ani
fascia supevaginal wall.
rior
and
inferior
be not lacerated
the
subject suffers
but little from
the
the
lesion, though
perineal body
be torn through to the rectum.
ani fasThe
levator
cia
superior forming the gutter or sulcus on each side
of the vagina is firmly blended
with
the vaginal canal
the same
surrounds
the
as
strong fascia in the male
In labor, in perineal laceration
should
prostate.
we
not
sure
merely look for lesions in the posterior commisof the vulva, for that is done
by the escaping head
and
for
should
look
shoulders, and is visible, but we
concealed
lesions of the strong fascia, the
sulcus
on
each
side of the vagina.
of
The
serious
lesion
most
labor may
without
visible external
occur
injury. This
a
HOW
lesion
general
is in
If
vaginal wall.
posterior vaginal wall
the
and
like
the
an
canal
the
muscles
closed
condition,
of
vagina
will
be
with
oele is due
the
to
superior
from
from
this, the
drawn
the
against
filled within; it will
be
fascia
together
rectal
The
air.
little
but
fascia
the
torn
be
not
excluding
body is indicative
cavity along the
fascia
of
The
collapsed bag.
holds
the vaginal and
open
the
fascia
will
43
THEM.
separation
a
the
anterior
MEND
TO
canals
be
with
in
ballooning
a
out
the
perineal
of fascial
the pelvic
lesions
within
The
vaginal rectovaginal canal.
aside
of the
levator
ani
drawing
and
little
but
injury
to
external
the
to
tion.
lacera-
on
ercise
exbeginning of discomfort
assuming
due
to deranged
tion
pelvic circulation, to dilaof veins, to non-uniform
straightening out
The
is
and
of
support
connective
fascia
The
tissue.
forward,
forceps,
the
if
and
is, so
that
united
tissues
Perhaps
which
for
and
the
If
this
be
secured
vaginal
The
curve
posterior
situated
On
muscles.
the
case,
this
we
view
mucosa
each
on
of
curve
within
the
side
of
the
the
area
in
the
introitus.
Now,
of
the
patient
labors.
our
Emmet
vaginal
corresponds
rectovaginal
lesion.
secondarily
that
easily see
an
elliptical area
can
denuded
base
see
cally
anatomi-
the
and
we
to
lesions
fascia
by denuding
success
the
eration
lac-
denuded
in the
discomfort
the
the
unfrequent
that
and
of
either
demonstrated,
show
clinically,to
rectovaginal
involved
been
which
disable
perineum
chiefly lacerations
are
of
it is not
the
without
where
be
proper
crowds
the
and
not
never
has
in
what
may
were
sufficient
head
is terminated
chiefly
decide
to
the
by
nerves
labor
the
split unnecessarily,
tissues
and
advancing
begin
rents
It is well
septum.
or
blood-vessels
the
septum,
of
the
sulci.
to
and
the
is
by introducing
fascia
ani
deep antero-posterior satures, the levator
be
reunited,
superior and inferior
restoring the
may
of the
the
fascial
posterior vaginal wall and
curve
44
THE
layers
at the
fascia
ani
vulvar
The
levator
and
inferior
and
ani
The
its intimate
on
th"
muscle
chiefly,it
the
rectocele
that
an
its
on
the
in
would
separated
the
brings
near
line
the
muscular
fascia superior and
levator ani muscle
sheath
the
can
stretched
its muscular
the
In
that
sutures
to
be
not
muscle.
inferior
is
the
anterior
and
introduced
of
wall
bulges
antero-
of
levator
the
start
sides,
both
on
levator
the
ani
line, which
levator
The
ani
for
sheath
the
The
functions.
damage
creating
fascia
It
fibers shall
really a
its
the
so
restored.
median
it.
without
rectocele, this
support
be
with
accomplish
torn
depended
be
action
the
in
loops
restoration
raphe,
or
would
muscular
possible
as
levator
in rectonecessary
levator ani loops anterior
be so repaired that the
loop must
to act approximately
from
the
raphe
but this is accomplished
by reuniting
as
the
success
the
fascia
muscle
be
action
secure
of
through
If
levator
imperfect degree.
by its superior
its origin, insertion
closely associated
function
median
muscular
to
ani
accomplished
planes of fascia.
to reunite
is true
levator
the
from
as
depends
of
the
be
must
symmetrical
it
reuniting
embraced
planes,
restoration
of
to the
In
closely
fascial
muscle
cele
PERINEUM*,
outlet.
is
relation
fascia.
AND
superior and inferior
also reunited, but
in
becomes
ani
VAGINA
is
the
so
torn
posteriorly
and
loses
rectum
forward.
to
Whether
or
versely,
trans-
in their
little,if they include
the
levator
ani
fascia
existing in the lateral
grasp
sulci of the vagina, and
is done, to be sucwhatever
cessful,
the rectovaginal septum,
composed
chiefly of
be restored
fascia, must
to reproduce the normal
curve
it matters
of
but
of
the
posterior wall
vagina. Mr. Lawson
Taits' flap operation
the
accomplishes
on
perineum
exactly what Emmet's
operation in the lateral vaginal
sulci does, with
Both
the
exception of denudation.
operations, when
properly and successfully executed,
result in the restoration
of the continuity of the deep
the
HOW
and
superficial fascial
the
establishment
function.
MEND
TO
layers of
partial or
of
45
THEM.
the
pelvic floor, with
muscular
complete
The
the
reunite
structures
deep sutures
normal
their
(fascia and muscles) at or near
points of
attachment.
then, the
Anatomically
objects to be
in an
obtained
operation for colpoperineorrhaphy
are
the
of
levator
ani
fascia, superior
1, the restoration
of
and
the fibers of the levator
inferior; 2, the reunion
muscle
ani
and
muscle
functionate
relations
have
must
3, the
it will
that
so
at the
of
restoration
the
fascia
both
"
ment;
attach-
perineal
perinei
muscles
draw
the
which
vagina lateralward, causing
of the ischioperiit to remain
4, the restoration
:
open
neal ligaments in regard to the
perineal body; 5, the
be reproduced
of the vagina must
posterior curve
by
the
6, a new
perineal
rectovaginal septum;
restoring
should
body
of
curve
should
be
the
restored
persist;
perineal body
relations
fascia
and
hand,
"
be
areolar
and
elastic
into
distinct
fill the
of
gap
composed
of
the
lateral
walls
are
two
kind.
levator
be
are
skin
points
two
ani
The
surface
the
in
and
functional
Both
of
the
muscle.
woven
inter-
are
There
of
ligaments
dissection
he
muscle
muscles
bulbo-cavernosus
They
contract
will
Both
with
connection
possess.
each
the
comparison.
have
is
from
arise
line.
in
and
floor
pelvic
medium
two
fascise,
relations
structures
bulbo-cavernosus
sphincter
muscles,
The
carefully study
muscles.
one
the
on
vulvar
structures
pelvic outlet.
halves, whose
their
insertion
lished
estab-
other.
complicated
though
the
of
of
of
These
tissue.
fascise
true
the
"
vagina
be
body,
or
on
composed
two
with
the
should
"
fixum
join
and
as
of
curve
muscle
and
most
considered
is
will
one
impressed
sphincter
as
the
muscles,
If
and
backward
restored.
floor
pelvic
forward
punctum
"
should
The
natural
the
relations
i. e., normal
the
perineal center
between
one
and
rectum
that
so
transverse
The
three
may
be
together
46
THE
and
have
the
two
fibers
VAGINA
similar
a
muscles
of
the
tendons
and
muscles
of
ends
are
of
to the
those
as
floor
of
have
the
back
lower
structures
to afford
abdomen,
GENERAL
As
control
Fascial
rectum.
the
terminal
The
is to
which
the
to
of
sphincter ani
of the pelvic floor by
The
object of the
attachments.
muscles
feature
common
vagina.
muscles
pelvic
vagina and
to
The
attachment
and
rectum
the
common
power,
their
fascial
the
PERINEUM;
function.
is
closely united
is
AND
ing
sustain-
and
thigh.
VIEWS.
to
employ
perineorrhaphy
repair uterine
prolapse (sacropubic hernia) as well as deficiency of
the external
sphincter apparatus, the subject covers
a
vast field.
All kinds
of genital supports
peritoneal,
fascial and vaginal sphincter apparatus
be conmust
sidered.
To have
prolapse, both peritoneal and fascial
of mussupports must
yield, as well as the occurrence
cular
we
"
"
relaxation.
all others
The
No
be
can
claimed
to the
support
one
for
the
utero-rectal
tissue,
are
efficient
uterine
account
itself,on
and
pelvic viscera
the
to
very
of
which
consist
fibro- muscular
The
supports.
its
of
uterus.
(sacral) ligaments
peritoneal duplicatures, containing
of
exclusion
intimate
toneum
peri-
connection
fascia, doubtless
gives
siderable
con-
support.
The
round
ligament, with
the
broad
and
the
vesico-uterine
the
genitals.
hernia,
abdominal
the
ligaments
In
its
peritoneal duplicature
holding some
ligaments all
the
intra-abdominal
consideration
pressure,
muscular
assist
of
the
in
fibers
ing
support-
sacropubic
state
of the
well
visceral
the
walls, as
as
supports,
should
be weighed.
Whether
the patient has
enterThe
optosis is a very significant question.
peritoneal
duplicatures, with their contents, constituting mesenteries
of the genitals, elongate in enteroptosis just as*
the stomach,
and
they do with
kidneys, intestines
HOW
other
It
viscera.
excessively
viscera
ensheathed
is
in
relaxed
to
the
doubted
into
the
be
muscle
The
whole
The
levator
inferior
the
viscera
of
the
ani, closely
fascia, forms
find
of
three-fourths
of
degree
outlet.
an
inch
an
vaginal
relaxed
vagina,
the
the
ledge made
vagina can
by
be
fascia
the
and
distinctly felt.
its scabbard,
in
ensheathed
normally
and
the
rectum
directly forward
vagina and
fascia
The
inserts
toward
the
pubic arch.
muscle
upward
into
vagina and
ani. (fascial
third
their
remedied
enclosing
drives
itself
mechanism
A
medium
(Eobinson-Scholer.)
by colpoperineorrhaphy.
10."
to
the
and
diaphragm
through which
By introducing the finger
Fig.
placements
Dis-
walls.
that
complicated.
its superior
uterus
supports.
only involve
pelvic floor, but the
a
outlet,
a
not
abdominal
the
find
to
uncommon
genitals
and
be
not
not
47
THEM.
MEND
due
the
special supports
and
peritoneum
pelvic
is
mobile,
of
It need
TO
of
the
and
is
and
the
embraces
the
important
muscular)
vagina a firm
lower
support.
supports
of
third
lend
fixation, quite
levator
The
to
the
the
lower
immovable,
48
THE
forcing
VAGINA
its walls
AND
closely
in
PERINEUM;
for about
contact
inch,
an
vaginal sphincter apparatus.
third of the vagina
In marked
contrast
to the lower
and
is the upper
is lax, mobile
portion, which
ing,
yieldtissue
being surrounded
only.
by loose connective
urethral
The
portion of the vagina and the neck of
bladder
the
firmly fixed by the vesicopubic ligaments
are
producing
a
pronounced
dwindle
which
the
into
line.
white
This
during respiration with highly relaxed
displaced genitals; the urethro- vaginal portion
be
can
and
seen
still,while
remains
to
off
and
fro
the
breath
each
with
of
remainder
the
move
organs
ment.
diaphragmatic movevagina is extremely
or
the
lower
Superiorly
firmly fixed by the three layers of firm, fibrous fascia
the
posterior layer of the triangular ligament, the
the
anterior
layer of the triangular ligament, and
three
These
deep layer of the superficial fascia.
fibrous
layers originate at the
powerful and dense
and
stretch
across
margins of the isohiopubic rami
of the
arch
the
the
pubis, surrounding
vagina and
To
in
the vaginal walls.
being intimately blended
"
be
convinced
are
the
the
retain
but
prevent
only
vagina
it
the
unyielding
lower
these
that
being
away
and
them,
inlet
of
end
from
to dissect
except
on
fact
the
all-important supporting
only
needs
of
of
qualities.
(triangular ligament)
that
structures
the
away
at
position
labor, one
all supports from
the
then
by tugging and
the
Parts
vagina,
of
note
these
not
in
vagina
torn
laminae
fibrous
their
fibrous
lower
ging
dragalmost
layers
in
frequently lacerated
in
be included
the flap-splittingand
labor, and must
the lower
to restore
deep sutures
vaginal tube.
Laterally, the
vagina is firmly fixed against the
of the
pubes, not only by the sodescending rami
cia
called triangular ligament, but by the levator ani fasinferior
superior and
enclosing the levator -ani
muscle.
By introducing the finger for about an inch
are
50
THE
utero-rectal
of the
AND
neck
of the
of
stage
the
the
downward
wedge
retroversion
on
at
as
sphincter
forces
the
the
descensus.
a
body
wedge
from
pressure
to the
uterus
the
breath.
or
intra-abdominal
The
backward
conical
a
cervix
acts
the
full rectum
pushes
retroversion, the
cervix
forward, all perfecting the
beginning stage of prolapse, by elongating the
rectal
In
the
utero-
ligaments.
colpoperineorrhaphy,
deficient
descending
end
in
gradually forces
The
fillingbladder
yield.
and
surface
and
cone,
to
and
anterior
the
every
apparatus
the fundus
vix
cer-
version
Retro-
anterior
top and
uterus, driving the pointed neck, like
pressure
the
ant
import-
relax, the
intra-abdominal
posterior surface of the
After
retroversion
superior.
of
they
and
the
is exercised
If
most
forward, while
retroversion
changes
the
are
the
will pass backward.
In other
the sacrorectal
ligapaents is the
words, elongation of
initial
uterus)
and
from
(extending
peritoneal supports.
will pass
downward
fundus
of the uterus
and
PERINEUM;
(sacral) ligaments
to the
rectum
VAGINA
turned
we
must
not
only repair
cone-shaped
sphincter apparatus, but the
cervix
be amputated
must
and
its blunt
that it should
downward,
so
point and rest
the
sacro-ooccygeal region (bone and
ments)
ligainstead
of attempting to dilate the levator
ani
muscle
breath
inal
at every
by the change of intra-abdomWhen
the cervix
once
gets firmly into
pressure.
the vulva, i.e.,into
the vaginal sphincter
apparatus,
the descent
is rapid and
inevitable.
The
twoupper
thirds of the vaginal walls being loose, easily descend
against
with
the
uterus.
inverted, showing
had
pressure
of
long
descent.
retard
wall
a
In
in
descensus
all
probability
displaced the uterus
An
intact
descending
appears
ligaments
uteri, the
first in
may
that
sphincter
uterus.
prolapse;
still retain
The
is
inal
intra-abdom-
first in
the
ess
proc-
apparatus- will
anterior
nal
vagi-
however
the
vagina
the
bladder
pubic
vesicoin
posi-
tion.
Posteriorly,
cervix
and
descends
the
peritoneum
portion of the
upper
words, the upper
separated, while
closely connected
the thin
edge of
51
THEM.
MEND
TO
HOW
part of
lower
the
by
a
and
rectum
and
fascial
musculo-
In
vagina.
rectum
the
with
the
other
vagina
vagina
are
are
with
septum,
wedge upward.
the cervix
forms
where
Rare
of prolapse may
occur
and
the peritoneum
is loosened
is elongated or where
other constretched.
to many
Space forbids reference
ditions
of peritoneal supports.
and
kinds
Fig.
about
12."
(After
the
Hegar
and
Kaltentoach.)
Baker
Brown's
method,
1850.
GENERAL
IN
VIEWS
SPHINCTER
The
should
vagina
DEFICIENCY
THE
OF
THE
APPARATUS.
engage
more
of
our
attention,
apparatus that the operation of
colpoperineorrhaphy is applied. The
primary factor
which
of the
produces
deficiency in the
supports
Other
factors
sphincter apparatus is labor.
play but
role.
a secondary
because
it is
on
this
52
THE
VAGINA
AND
The
the
pelvic fascia is
ischiopubic rami;
the
The
which
contained
results
be
not
PERINEUM;
infrequently
the
where
muscular
are
fascial
fibers
cicatrices
and
also
lacerated
sheath
near
is ruptured
suffer
tion.
lacera-
loss of substance,
felt
anterior
by palpation. The
nal
vagiwall generally escapes
laceration, but the posterior
sized
vaginal wall is often damaged, showing various
is prominent
formed
lesions.
Relaxation
and
and
closure
Instead
of
the
lower
curved
incomplete.
canal with the perfect sphincter apparatus, there is a
may
Fig. 13."
Dr.
Goodell's
patulous, relaxed, open
which
lost
has
pouch
the vaginal mouth
posterior vaginal fold,
the vagina.
The
causes
method
of
colpoperineorrhaphy.
mouth, resembling a tobacco
its puckering
times
string. Someis closed
by an anterior and
for
a
considerable
distance
of
up
ual
displacements of the sexare
so
elongation of the
numerous
as
organs
uterO' rectal ligaments, elongation of the cervix, laceration
of the levator
ani
and
fasciae,muscles
triangular
that
ligament, intra-abdominal
enteroptosis
pressure,
all possible factors
be
in
considered
must
repair.
consist
in correcting vicious
Repair must
forces, as the
"
"
HOW
pointed
apparatus
distinctly
; however,
Yet, after
all, our
deficiencies
of
considered
reunited.
both
chief
attention
will
be
sphincter
combined.
often
be
may
genital
should
of the
deficiencies
from
ing
produc-
the
in
peritoneal support
of
and
back
end
factors
the
lacerations
and
Deficiencies
organs.
of
made
restored
be
be
should
fascia
be
should
rectal
the
turn
ani
analysis should
displacements
An
to
levator
lacerated
the
body
perineal
a
be
ward,
back-
turned
and
amputated
posterior vaginal curve
should
cervix
the
with
53
THEM.
MEND
TO
directed
be
to
pends
it deapparatus, for on
lacerations, chiefly arising in it.
the
sphincter
prolapse and
Deficient
give rise
peritoneal supports
primary
rectocele, vesicocele, bladder
as
vaginal inversion
of
whole
the
for
utilized
will
This
line.
floor
of
by
a
the
of
tonicity
the
will
cicatrix
which
also
reproduce
and
canals.
the
the
firm
hernia
sacro-pubic
pelvic floor should
forcing it into the median
restore
form
and
its
colpoperineorrhaphy,
In
of
tissue
support
and
loses
mouth
vaginal
the
string condition.
puckering
the
and
disturbances,
rectal
to
be
pelvic
prevent
the
normal
accomplish
this, extensive
denudations
flaps are
or
requisite.
make
the pelmust
Successful
vic
colpoperineorrhaphy
floor
formed
the newly
tense
possible and
as
as
ened
thickThe
cicatrix
will aid materially in its success.
tissue
the anterior
and
(columns) on
posterior
curves
walls
vaginal
should
Mr.
be
from
their
that
nearly
make
the
anterior
labors
Emmet
of
ducts, which
Miller's
Dr.
preserved in both
flap operations.
They furnish
Tait's
side, and
of
remnants
are
and
To
Emmet's
are
fibrous
masses.
all successful
denudations
It
in
the
may
of
methods
evident
vaginal
be
and
port
sup-
observed
perineorrhaphy
sulci
on
each
avoid
the
tissue
on
sacrificing the thickened
and posterior vaginal walls.
Reference
to the
Bischoff, Martin, Hegar, Kaltenback, Schatz,
and
others
will show
this
to
be
correct.
After
54
THE
performing
be
may
This
procedure,
method
lower
the
to
be
end
sulci
the
or
conditions, and
of
of
the
successful,
The
structures.
PERINEUM;
makes
what
posterior, Martin
of the perineum
forward.
extension
an
excellent
an
of
curve
AND
colporrhaphy
called
is
VAGINA
restoring the anterior
vagina. Any surgical
conform
must
denudation
far
have
the
of the lateral
conform
flap operations
so
to
to
tomic
ana-
nal
vagi-
anatomic
successful.
proved
The
a)
^nus
Fig. 14,
a
and
b."
denudation
reason
because
healing
method
Kearny's
Dr.
in
in
of
colpoperineorrhaphy.
perineorrhaphy
the vagina
occurs
is
so
successful
with
is
able
consider-
certainty.
THE
METHODS
OF
The
methods
of
into
vulva
three
perineorrhaphy
divisions,
(denudation)
vaginal portions
PERINEORRHAPHY.
PERFORMING
viz.
:
; those
Those
which
(denudation);
be
may
which
start
attack
those
classified
which
the
at
the
lower
depend
tried
Baker
and
which
tissue
ble
for
This
laceration.
and
the
side
each
on
value
except
to
visi-
ure
proced-
superficial vulvar
a
ficial
super-
the
prepare
way
methods.
useful
more
was
of small
was
situated
was
the
united
they simply
when
Brown,
Dieffenbach
Par6,
Ambrose
of
days
the
since
been
have
perineorrhaphy
of
methods
Numerous
colpoperine-
embraces
(which
flap procedure
orrhaphy).
the
on
55
THEM.
MEND
TO
HOW
HISTORY.
performed
If the ancients
am
unable
rhaphy
as
I
being
modern
than
more
a
the
According
reasons.
sought
of
method
first
and
attacked
Fricke
Pare.
which
episiorrhaphy
labia
and
by such
attacked
by
union
methods.
Tait
the
region
of
the
and
later
hymen.
or
of
The
surgeons
be
done
tors
OperaBrown
performed
who
of
failures
both
of
denudation
to
vulva
Baker
as
pioneer
cicatricial
The
vagina.
Fricke's
operate higher
Emmet
the
in
suggested denudation
thought
Malgaigne
deeper in the introitus.
when
it protruded,
the vagina
the raw
of the eschar, united
exfoliation
should
Girardin-
virus.
finally resulted
Mende
the
for
questionable
very
surgeons
consisted
sutures.
the
gonorrheal
the
was
episiorrhaphy induced
in the vagina, which
up
and
by
vulva
tracting
con-
a
caustics
inflammation
it with
the
produce
so
Phillips used
nedy,
Laugier, Velpeau, Kenand
Simon.
dale
Chippen-
did
vagina
infecting
have
was
the
in
contraction
up
would
wall
stone.
Colles
stir
to
vaginal
Schroeder,
to
blue
the
Laugier employed
saltpetre;" so
"smoking
Dieffenbach,
the
applied
Others
cicatrix.
same
of
prolapse by excision
resulting inflammation
prevent
that
a
Colpoperineorscarcely boast of
operation can
Surgeons sought to
century old.
records.
the
obtain
to
perineorrhaphy,
successful
Jobert
and
it
erized
caut-
after
surfaces
in
the
with
56
THE
cicatricial
produce
the
united
the
segments
to
that
since
employ
with
also
were
failed
on
He
prevailing
in
must
perineum
solid, thick, unyielding
Simon,
Dieffenthe
first
the
operation.
of anatomic
is
not
the
the
sexual
the
be
only
not
organs
not
can
many
anatomy
learned
elongated,
floor
pelvic
geons
sur-
Langenbeck
lack
It
out
and
mucosa
necessary
It was
colpoperineorrhaphy.
the
that
of
sepsis.
learned
surgeons
in
to
was
cut
sutures.
pioneers
account
zinc
Hall
Marshall
elytrorrhaphy.
of the
vaginal
surfaces
Braun
Early operators
and
knowledge
decades
employ
of
chlorid
employed
of
flaps. Velpeau was
one
successful
perineorrhaphy.
do
Karl
PERINEUM;
contraction.
denuded
formed
to
and
first to
long
or
bach
AND
Desgranges
sutures.
among
oval
VAGINA
but
be
must
escape.
a
structed
con-
haps
Per-
berg,
Czerny at Heidelthe
real founder
of colpoperineorrhaphy.
was
not
when, in 1867, he had
only performed but added
to it that of posterior colporrhaphy
Simon
freshened
the
fenestrated
vaginal wall with a scalpel, and
a
speculum
was
placed in the vagina while he freshened
the upper
tant
part of the vaginal wall by having an assisintroduce
the finger in the rectum
and
force the
vulva.
and
the
out
at
vaginal mucosa
Veit, Hegar
As
time
Speigelberg aided to develop the operation.
for support
placed
passed, instruments
gradually diswere
to
perfect operations, owing
more
by more
and
Most
of
perfect anatomic
pathologic knowledge.
the advances
due
are
chiefly to the investigations of
Freund,
(1879)
Huguier, Martin, Schroeder, Wilms
and
Staude
tioned
(1880), Breisky, Huepfel and others menin this monograph.
The
practical execution
of colpoperineorrhaphy
Heidelberg
by the celebrated
predecessor
of
.
surgeon,
labors.
Simon,
The
colporrhaphy
operation
is
success
in
that
some
prolapse
or
subsequent
addition
Simon's
attending
demonstrated
required
of
real foundation
is the
of
of
vaginal
deficiency of the
form
58
AND
VAGINA
THE
PERINEUM;
be termed
oolpopresent the operation should
New
aids have
also been
developed
perineorrhaphy.
in regard to the
operation, as A. Martin
taught for
that
should
one
begin the operation for colpoyears
of the
involution
perineorrhaphy by setting up an
I have
the cervix.
uterus
amputated
by amputating
the pointed conical
cervix
to get rid of the dangerous
dilatingwedge to the sphincter apparatus of the pelvic
for successful
floor, to prepare
colpoperineorrhaphy.
At
Fig. 15.
Colpoperineorrhaphy
of the
portion
posterior
ehaped
according
"
The
away.
and
the
A
should
new
of
introducing
appeared
era
to
in
operation
method
began
the
denudation
the
be
this
fail
of
operation
much
the
damage
sutures
in
formed.
late Berlin
wall
this
So
far
to
Bischoff.
vagina, d, is not
and bleeding
is severe
is done,
a,
a,
shape
of the
operation
when
and
as
The
the
the
records
are
and
tonguedissected
is
active,
b, b. show
denuded
area.
the
flap
accessible,
Langenbeck, in 1852, flrst
described
the flap operation
He
in perineorrhaphy.
describes
the
splitting of the rectovaginal septum
and
rectal
ward.
a
flap backmaking a vaginal flap forward
description of perineorrhaphy,
Langenbeck's
translated
as
by Dr. Marcy, is the most
important
surgeon,
von
HOW
contribution
of
to
TO
the
In
Heidelberg.
59
THEM.
MEND
subject before the
fact, it is almost
in
superior
sense
of
time
Simon
equivalent
to
of the
the use
Simon's, and in one
cultivated
also
flap. Perineorrhaphy
by Zary,
was
rhaphy
PerineorHomer,
Mureina,
Mensel, Osiander, and
silk sutures, the hot
first performed
with
was
About
chemicals.
iron, and
tury
three-quarters of a cenIn 1879,
metallic
appeared.
(wire) sutures
ago
Werth
of catgut
the use
(animal
published views
on
"
ligatures) for
the
buried
buried
spiral catgut
gut is one
Silkworm
for sutures
Schroeder
sutures.
duced
chiefly introin
sutures
of
the
at present.
general use
of
Mr.
the
Lawson
Tait
use
a
began
method, consisting of resplitting the old
in
use
of
surfaces
by
the
skin
of
means
which
sutures
membrane.
mucous
or
the
scissors, reuniting
The
rhaphy.
perineormaterials
best
About
certain
flap
by
cicatrix
wound
produced
do
1872,
not
penetrate
utilityof
this
sists
con-
application to either, or both, perineorrhaphy
The
or
flap operation was
dimly
colpoperineorrhaphy.
begun by Dieffenbach, in 1829, by his lateral incisions
The
to relieve
tension.
flap operation was
definitely
introduced
in
perineorrhaphy
by von
Langenbeck,
about
In 1861,
1850 ("Memoire,"
1852, by Verhaeghe)
of vesico- vaginal fistula,
in a case
of Dublin,
Colles
in its
.
resplit,
resultant
edges
of
instead
of
flap.
an
paring
In
1872,
artificial
anus
the
John
and
edges,
and
united
the
Duncan
resplit
reunited
them
the
with
forced
the
He
flap of
interrupted
catgut sutures.
the flap composed
of musand
drew
upward
mucosa
and
culosa
outward, thus
serosa
increasing vastly the
denuded
for coaptation,
and
surface
Barbour
Hart
applied this flap method
report that Dr. A. R. Simpson
Not
to perineorrhaphy.
far from
1872, Mr. Lawson
Tait applied the flap operation of Langenbeck,
Colles
and
Duncan
the
He
to
subject of perineorrhaphy.
added
the use
of sharp-pointed
to all previous
labors
60
THE
scissors, and
elbow
without
Silkworm
in
remain
to
Sanger, Stein,
valuable
as
in
well
views
as
are
involved
1.
the
Ambrose
the
so-called
numerous.
vulva, the
Pare
The
method
sutures
vagina
and
or
may
weeks.
According
Norwegian, used
contributed
pelvic floor,
Reamy.
ot.the
and
Byford,
method.
of
Voss, a
Hadra,
1887,
restoration
Jenks,
The
to six
the
employed
are
and
Dane,
a
on
Fig. 16." Dr. Skene's
ready for tying.
various
days
of
mucosa
or
sutures
Later,
Marcy,
situ
The
ten
methods.
similar
skin
the
gut
for
situ
PERINEUM;
introduction
the
penetrating
rectum.
AND
VAGINA
D, S, is denuded,
area
with
sutures
and
Staude.
that of Hegar
resembles
operations for (colpo) perineorrhaphy
devised
first operation
The
second
(1580)
both
used
pupil Guillenneau
practised and
(1649). LaMotte, Smellie, Noel,
rotte
practised it.
vulva
and
vagina.
His
simply sutures.
improved the method
Murenna
and
Sance-
HOW
2.
(1830)
relieved
TO
Dieffenbach, union
by lateral incisions.
it into
France,
well
as
61
THEM.
MEND
as
by
and
sutures,
Roux
Mark
See
sion
ten-
duced
(1834) intro(1885), and
Polail]on(1885).
surfaces.
denuded
(1885,
Wilms
union
and
by
of
sutures
Staude
the
cultivated
it
Germany.
in
The
4.
and
contribution
method
important
in perineorrhaphy
von
Langenbeck's flap
was
described
It
and
performed with
was
(1850).
hand.
also
Von
Langenbeck
suggests that
next
devised
method
a
Brown
Baker
3.
master
.
the
lateral
incisions
of
Dieffenbach
added,
be
may
ss
it obviates
advocated
He
dragging from movements.
after the injury, if possible. Von
operation immediately
several distinct
makes
steps in the operLangenbeck
ation
:
vivification
septum
the
formation
of
the
; the
free
undoubling
of the flap destined
border
of
of
the
to
form
the
vaginal
recto-
and
septum
in
the
new
side of the
perineum, the anterior
triangular space
the
with
formed
rectum,
canals, vagina and
by two
of the two
lips
perineum as the base; the vivification
In
the
sutures.
of the
of
laceration; the insertion
this
of perineorrhaphy
Langenbeck
von
operation
The
the flap method.
started
flap operation protects
from
the wound
secretions
(vaginal or rectal).
the
real
of
5. In
1867
Simon
began
Heidelberg
which
modern
perineorrhaphy,
was
steps in successful
of perineorrhaphy
and
posterior cola combination
BakerSimon
improved
on
porrhaphy.
simply
Brown's
method
by not only freshening the perineum,
denudation
.but also carrying the
high up into the
denuded
aid of a
Simon
the vagina by the
vagina.
fenestrated
The
speculum.
nal
angle of the vagiupper
denuded
wall was
by introducing the finger into
the rectum.
ing
Spiegelberg and Veit aided in developin
in 1871; Banga
the subject.
Englehart wrote
1875
wrote
Kolpo-perineorplastik
on
aoa thesis
"
"
62
cording
Bisohoff.
to
excellent
made
Neugebaum
Edward
of
a
1881, added
of
Jenks
of
series
really a flap
articles
of
method
x\
of
the
Pig. 17." Shapes
Hegar;
b, Simon
; c, Lossen
;
of
von
sutures
buried
by
the
away
is almost
to
flap, but
A.
Le
1877
labors.
their
Fort, and
In
Dr.
1877
"
denuded
the
In
a,
black
R. Simpson
and
lines
procedure.
similar
colpoperineorrhaphy
in
areas
d, Fitch.
afterward
precisely
Dr.
In
Kaltenbach
began the publication
was
on
perineorrhaphy which
distant
relative
a
operating
tissue,
Langenbeck's
and
Hegar
Detroit
/?"
the
1879
In
contributions.
in
W.
PERINEUM:
AND
VAGINA
THE
b, the dotted
the exposed
Dr.
preserved
to
the
by
Jenks
it. The
flap method
Hart
and
;
line
a,
sent
repre-
sutures.
first
cut
method
buted
attri-
Barbour.
HOW
MEND
TO
63
THEM.
buried
began to use
catgut to suture
buried
animal
Dr. Brose, in 1883, used
the wound.
ligatures. H. O. Marcy published a series of articles
(1883) on perineorrhaphy,
advocating the flap method
animal
he
first used
in
buried
and
ligatures, which
Werth
1879
In
hernia
labors
excellent
of
of
Berlin
of
1882.
about
Sohroeder
by the
running
Martin
A.
1881.
in
Berlin
contributed
About
obtained
1880,
excellent
fessor
Pro-
results
the
stitch, a continuous
"6tage"
in
the
of
buried
of catgut
suture
tissues
and
the denuded
As a pupil of Schroeder
surfaces.
this method.
excellent results from
Martin, I observed
of Langenin part revives
the flap operation
Bischoff
beck.
However, his operation was
quite influential
in its day.
and
Drs. Byford, father
made
able
valuson,
to the
contributions
subject.
History notes that
Duncan's
carried
Simpson
flap-splittingto the peri,
kind of four-flap perinea
performed
Simpson
orrhaphy
neum.
use
for
of
some
In
1887
suggested
Dr.
the
as
is
of
operation
Pare, Baker
Simon
to
in
Tait
the
done
1880, the laborers
imbibed
contributed
of
able
valu-
some
perineorrhaphy.
He
posterior vaginal wall for
in
in the
anterior
field
are
colporrhaphy.
legion.
ally
Gradu-
of
modified
was
perineorrhaphy
Brown,
Dieffenbach, Langenbeck
and
denuding
denuding higher
consisted
also
subject
vivification
the
and
of Texas
Hadra
on
oolporrhaphy,
from
Tait
his views.
articles
Since
Mr.
Perhaps
years.
many
not
up
The
Emmet.
only
in the
modification
the
perineal tears, but
posterior vaginal wall.
well up
especially carried the denudation
into the posterior vaginal wall.
As regards
suture
Emmet
material, Sims, Thomas,
out the application of metallic
wire
others
worked
and
the
to plastic labors
on
during the past
perineum
modem
The
tendency is to use silkworm
thirty years.
be left
This
suture.
gut as a non-absorbable
may
Hildebrandt
64
weeks
in
a
surfaces.
is due
THE
VAGINA
wound,
and
It is easy
credit of
the
PEKINEUM
AND
acts
to
as
splint in coapting
a
To
remove.
introducing
a
Dr.
T. A.
of
method
Emmet
perineorrhaphy
generally
published
the
which, until recently, was
one
In
in
1883
Dr.
Emmet
America.
practised
modification
of his
rather
method,
a new
or
a
each
denudes
the sulci on
operation. Dr. Emmet
forward.
of the vagina and
extends
the perineum
to repair perineal fascia
operation is intended
muscles.
Dr. Emmet
holds
that loss of support
on
the
2 show
each
side
of
lines
the
of
The
is due
to
Emmet's
within
loss of
denuded
of
union
column,
vaginal
lowing laceration
body.
(elytrorrhaphy
operation
Emmet's
Fig. ISA."
1 and
is not
3, which
due
support
to
after
posterior)
surfaces
still
in
the
the
old
side
His
and
fol-
for prolapse
sulci
vaginal
remains.
injury
of
the
perineal
childbirth, he claims,
and fascia.
Dr.
rupture of perineal muscles
clear
scription
by deoperation is difficult to make
in lateral denudation
but it consists
wholly
the
vagina
to
s-uch
an
extent
that
when
the
slack
or
tight,the excess
ostium
The
in the posterior vaginal wall disappears.
tion.
vaginse is not interfered with by any special denudadiscomfort
of his operation is that
The
claim
sutures
:
introduced
are
drawn
66
THE
VAGINA
AND
PEEINEUM;
disappears immediately after, and also
vaginal wall is brought in proper
relation
the
to
condition.
The
is that
wall,
anterior
maintained
view
the
it
as
is
the
posterior
position and
in
the
normal
this
in
perineal body
that
is
surgical procedure
insignificant in
of it alone
support, and that laceration
impairs
little the integrity of the genital supports.
But
tearing
fascia
and
at their
the
disturbs
stretching
excessive
or
attachments
delicate
balance
to
of
perineal muscles
the genitalsquickly
the
pelvic organs.
m
Jenks'
5." Dr.
Fig. 19 a and
flap-splitting is executed
In a the flap is marked
ready for suturing.
is
one
and
that
the
higher
of
the
the
is
Wylie added
be improved
considerable
out
The
(flap) of perineorrhaphy.
and
scalpel.
a
rectum,
fingers in the
dotted
line ; in b the flap is completed,
method
with
two
by
a
operation,
point against Dr. Emmet's
of introducing
the relatively blind method
In
sutures.
lacerated
sutures
the
of the
(a)
There
but
pelvic
other
fascia
words,
may
of
not
the
be
deep
layers
included
in
certainty. Dr. Gill.
the idea that Dr. Emmet's
operation would
by denuding the posterior vaginal wall a
with
any
distance
degree
and
then
continuing
the
denu-
TO
HOW
dation
well
method,
sacrifices
however,
67
THEM.
This
posterior vaginal sulci.
the
into
up
MEND
larger
a
of
amount
rior
poste-
vaginal wall.
1872
About
began
known
as
in
he
that
deep
Lawson
Mr.
introduce
to
the
method
a
elbow
without
sutures
introduced
penetrating
It involved
membrane.
and
scissors
all others
from
It differed
flap method.
used
land,
EngBirmingham,
of perineorrhaphy
of
Tait
the
skin
the
or
loss of tissue.
no
very
mucous
The
tion
direc-
operation is to resplit the old
of
It is modified
cicatrix.
according to the condition
the case,
anterior
and
posterior
produce
one
as
may
Tait's
is now
cuts.
quite generflap perineorrhaphy
ally
practised. I have not attempted to give all known
for
historic
chief
the
doing
of
methods
of
out
ones,
Tait
perineorrhaphy,
which
built
been
have
but
simply
the
the
modem
operation.
GENERAL
1. To
restore
rectal
2.
restore
pelvic
To
fascia
3.
To
vaginal
functions.
Normal
muscles.
and
fasciae
circulation.
normal
relation
normal
the
restore
and
for
required
is
PERINEORRHAPHY.
FOE
INDICATIONS
and
of
support
The
(colporrhaphy
posterior).
posterior wall
the
anterior
vaginal
posterior vaginal wall sustains
the
wall
4.
and
bladder.
To
provide
the
as
organs
much
as
support
of
restoration
the
for
the
pelvio
body will
perineal
afford.
5.
To
relieve
short,
6.
the
to
To
7. To
The
the
remove
Innumerable
relieve
mental
repair and
narrow
pelvio
check
relaxed
floor
conditions;
neurasthenic
physical
sacropubic
pelvic
is closed
disturbances.
hernia.
outlet.
from
behind
pyriformis with its thin, delicate
sacrorectal ligaments, the coccygeus
the
in
associations;
nervous
and
to
forward
fascia, the
with
its
by
firm
moder-
'
68
THE
AND
VAGINA
levator
ately strong fascia, the
levator
fascia
ani
double
The
tissue.
with
ligament,
practically
a
and
fascia
the
constitute
essential
Fig.
from
one
levator
the
to
20.
"
ani
of denudation
the
vagina
fascia
pelvis to the
pelvic
every
expansions
the
of
to
organ,
as
in
success
vital
its
fascia,the levator ani
the
triangular ligament
to
pelvic floor and
seem
the
the
supports;
These
perineum.
oolpoperineorrhaphy.
The
of vaginal
curved
strips, with
scissors,
other, as suggested
by Dr. Skene.
from
(both layers)*pass
viscera, firmly attaching
known
pelvic viscera
these
in
structures
Method
side
with
its
separate the pelvic cavity from
are
muscle
inferior, a strong
also
sheath, and
powerful layer of fibrous
with
coccygeus
double
its
ani
superior and
protective muscular
fibrous
triangular
the
PERINEUM;
forming
ligaments,
definite
fixed
the
the
side
of
themselves
strong, fibrous
which
serve
relations.
to
In
hold
neorrhaph
peri-
restoration
the
depends on
fact
significant anatomic
a
pelvic pathology is that the blo*od-vessels
the nerves
inferior
to the pelvic fascia and
of
in
lie superior
to it.
The
HOW
i perineal
the
in
arrive
which
blood-vessels
69
THEM.
MEND
TO
region
of
the
chiefly out
pass
pierce the pelvic fascia and
notch.
great sacrosciatic
I'^he levator ani fascia, superior and
inferior, is an
infection.
It separates
to limit
important structure
the
from
fossa
the ischiorectal
pelvio cavity proper
so
fascia
is
and
which
loose
much
where
pierced by
a
are
may
travel
and
vice
In
versa.
is
which
performed
exists
perineum
termed
I
the
best
name
is
Colpoperineorrhaphy
integrity of the supports
of
end
opinion
body in
vagina and
still prevails as
I claim
body
the
the
the
organs.
and
peritoneum
lower
the
of
Difference
the
perineal
genitals,but, from
female
work
functions
for
on
the
ject,
sub-
the
perineal
the
lower
ends
of
the
anterior
rectal
and
levator
3.
restoration,
between
posterior vaginal wall.
directs
the
2. It supports and
the vagina forward, aided
by the
and
be
sexual
the
considerable
following
may
flap method.
is colpoperineorrhaoperation to restore
utility of
to the
the
:
1. It sustains
wall
It
rectum.
of the
the
economy
and
dissections
many
the
the
tion
opera-
the
or
situated
is
perineal body
ani
of
restoration
of
of
supports include those
vaginal sphincter apparatus.
These
The
an
fossa,
levator
names.
perineauxesis,
the
think
infection
The
perineo-vaginal
perineorrhaphy,
However,
the
different
under
perineal extension,
phy,
for
sels
ves-
sheaths
ischiorectal
the
ani
these
the
which
by
inferior, is incised.
and
fascia, superior
and
nerves,
pelvis to the
perineorrhaphy
the
levator
by lymphatic
path
or
from
and
surrounded
source
The
exists.
vessels
are
nerves
tissue
ani.
supports and
rectum
backward;
It
by
the
of
discharging end
triangular ligaments
levator
ani
directs
the
the
rectum
muscle.
discharging
is
directed
end
of
ward
back-
70
THE
4. It
not
and
rectum
in
support
thus
of the
of
the
and
contents
curved
of either
the
avoids
irritation
vagina
of
are
the
an
at
their
canal.
The
wide
of
mingling
from
rectum
important
easy
escape
divergence
the
secretions
The
decomposition.
and
forward
the
factor
in
a
maintaining
the
preventing
the
termination,
for
advantages
apertures and
canals
hook
direction
mechanical
consequent
backward
of
a
of both
two
PERINEUM;
only keeps the discharging ends of
vagina widely apart, but it gives both
affording
closure
AND
VAGINA
hook
support, and
is
which
LeFort's
(1889) method,
Fig. 21." (After Pozzi.)
incision
in
is made
An
Eichert's.
(1864-1875) and
Demarquay's
rectum
line down
to the
an
; then
at the
point C, in the median
along
the line C, D, E: another
line, C, G, is carried
made
along
line
joins it by
mucosa
wall, but not into the rectal
; another
No.
in
H
3) ; the
(seen
distinct
this
makes
triangle,
G;
I,
a
E,
similar
the
to
vagina
incision
is
the rectal
means
of
cicatricial
of the vaginal
also the portion
the triangle,
H, and
from
denuded
rectal
the
from
the
dissected
and
space
is
seized
D,
;
wall,
2 and
3.
shown
in Nos.
introduced
as
is D
H
and
are
(No. 3) ; the sutures
is
The
4.
in
No.
a
operation
is
noted
the
tial
parThe
sutures
disposition of
for ordinary
practice.
but
too
complicated
flap method,
tissue
is removed
marked
HOW
The
vagina.
fat, muscles, fascia, elastic and
perineal body as a support
and
anus
has been
organs
5. It serves
as
between
is the skin
perineum
perineal body consists
The
gaping.
prevents
71
THEM.
MEND
TO
genital
the
for
itself
skin,
The
tissue.
connective
in
of
overestimated.
much
point of union
the levator
ani, the sphincter ani,
the
transversus
perinei.
and
sus,
four
of
the
muscles
:
bulbo-caverno-
the
It
also
serves
as
a
^
partial support of the pelvio
strengthens a tried point in labor.
6. It acts
a
as
7.
It
8.
Laceration
of
destroys
extent
genitals.
The
object
ruptures;
ruptures;
of
rectal
to
prevent
in
function
To
is:
prolapse
anatomic
of
female
the
restore
after
functions
partial
complete
segment
pubio
the
floor.
considerable
any
between
balance
perineorrhaphy
restore
floor.
of
methods
denudation
to
perineum
nice
the
to
pelvic
The
the
physiologic
and
structure
of the
fasciae.
various
of the
of union
point
with
fixed
The
etiologio factors
and
trauma.
perineorrhaphy
performing
-Partial
lacerations
laceration
of
flap method.
labor, coitus
perineum
may
the
coaptation, and
of
are
are
the
vaginal
patency; increased
condition
secretion; irritabilityof parts; pathologic
conditions
of nerve
structure; neuralgic or neurotic
tention)
(disinduced
by long-continued local lesions; descent
rectal wall, posterior vaginal wall,
of anterior
be
accompanied
and
uterus.
by vulvar
Complete
accompanied
increased
vaginal and
be
may
bowel
contents
irritabilityand
laceration
by vulvar
of
and
the
perineum
anal
patency;
of
secretion; incontinence
contents;
and
occasionally of bladder
parts from
of the surrounding
disease
rectal
ditions
consecretions; neuralgic and neurosal
melancholia
structure;
from
changes in nerve
of the displaceable segment
(neurasthenia) ; relaxation
the
of
abnormal
the
pelvic
floor
and
consequent
prolapse
or
hernia
72
AND
VAGINA
THE
The
pubio segment.
of
gestiou from a disturbance
of the
result
be
may
the fascia
severe
which
con--
holds
blood-vessels
If the
in relation.
blood-vessels
PEKINEUM;
the
become
circulation
results.
bed, disturbed
|
In discussing the operation for colpopefineorrhaphy
distorted
and
Emmet
by
their
in
I shall
Tait
these
consider
both
founded
|
and
successful
principles, both practical
end
ferent
by difoperations, and both arriving at the same
since
I can
methods.
However,
accomplish by
Emmet
Dr.
exactly what
accomplishes
flap method
a
I have
preferred to follow the flap proby denudation
cedure.
method
for
the
six
I have
flap
over
employed
hundred
one
operations percomprising over
formed
years,
anatomic
on
for almost
prolapse.
In
prolapsed
for
uterine
of
up
all kinds
perineal laceration
of
the
case
one
fourteen
uterus
years.
was
Another
and
pletely
comcase
thirty-fouryears' standing, with laceration extending
the length of the index
the rectum
finger,was operated
after
three
previous denuding opersuccessfully
ations.
of twenty-eight years' standing,
A third case
lacerated
was
up
the
rectum
for
four
inches
and
had
operations. One of
passed through three unsuccessful
rectal
years' standing, with three-inch
twenty-seven
of seven
difficult case
years'
laceration, and one
very
operations by wellstanding, with several unsuccessful
known
with
operated on
perfect
gynecologists,were
of long standing, atrophy was
In these
cases
success.
limited
from
far advanced
blood-supply andjnon-use
so
tissue
that it required extensive
flaps in order to secure
To show
that the perineal body
for a perineal body.
of those
is not significant in uterine
support, several
for over
with
twenty-seven
patients continued
years
laceration
a
several
of uterine
symptom
It will be
observed
up
the
the
rectum,
with
scarcely
prolapse.
from
even
patient should
If
colpoperineorrhaphy.
that
for
inches
superficial experience
be
properly prepared
the
a
patient have
a
74
the
A
uterus.
behind
has
PERINEUM;
AND
VAGINA
THE
long, pointed,
it
retroverted
a
conical
cervix
precedes
which
uterus
ally
gener-
prolapse.
Again, if there is a cystocele the patient should be
be that
prepared by an anterior colporrhaphy. It may
anterior
colporrhaphy
amputation of the cervix and
the
as
be done
at the same
sitting and anesthesia
can
We
frequently
flap-splitting colpoperineorrhaphy.
at the
perform colporrhaphy and colpoperineorrhaphy
but
rare,
cervix
much
the
if there
it should
against
as
To
time.
same
the
as
require cervical
be
retroverted
In
sacrum.
possible
to
short
secure
to the
with
uterus
and
amputated
be
it is due
same;
a
is rather
amputation
backward
turned
imitate
must
we
All
success.
destruction
pointed
nature
hernia
is
valves
of normal
Hence
straightening out of oblique canals.
normal
the
obliquity of the
in
sacropubio hernia
Colpoperineorrhaphy
vaginal canal must be restored.
porrhaphy
the
restores
posterior vaginal wall and anterior colThis
the
anterior
restores
vaginal wall.
if the
needed
often
colpoperineorraphy be
is not
neorrhaph
thoroughly performed. Prolapse is prevented by peri(or some
elytrorrhaphy, episiorrhaphy
considered
be
abdominal
Prolapse may
operation).
downward
displacement of the pubic segment of
a
as
of the pelvic floor
the pelvic floor; the sacral segment
There
of its parts.
in it by a yielding of some
shares
varied opinions as to the etiology of prolapse
so
are
many
is
not
the
fully
subject
that one
safely say
can
credit is due
to Drs.
In
settled.
opinion much
my
excellent
for their
and
Barbour
Hart
investigations
After
of the pelvic floor.
the structural
anatomy
on
and
the
considerable
many
previous
when
the
The
careful
the
views
closest
dissection
must
and
be
most
I feel
quite
changed,
continued
nearly to the same
pelvic floor come
subject of prolapse, I think, should
but
that
sure
it is
ful
hopeof
students
conclusion.
be studied
out
HOW
and
anatomically
is still
of
subject
be
to
anatomic
lesions
prolapse.
lost
be
the
pelvic
23
6."
and
a
The
of
and
be
extends
the
be
to
more.
The
whole
will
pelvic
and
processes
large
a
studied.
more
method.
the
lacerated;
septum
itself
factor
in
should
perineal support
of
sphincter apparatus
the
into
tion
investiga-
uterus
From
dissec-
The
figure is according
S, rectovaginal
septum;
b the
In
rectovaginal
rectum.
P, perineum.
to
is split.
septum
would
one
fascia
and
in
supports
at
the
the
example,
pelvic floor, and
be
must
dissection
thoroughly
conclude
once
that
triangular ligament
intelligible way
views
found
be
Fritsch-Walzberg
laceration
F, rectovaginal
tion
will
will
floor
of
labors, infectious
repeated
sight of,
of
laceration
submucous
Relaxation
Insufficiency
not
field
on
goes
the pelvic floor
and
studied.
The
the
and
attention
floor, due
Fig.
time
relaxation
more
Pozzi.
As
75
THEM.
clinically.
large.
will get less
MEND
TO
considered.
of
and
quite
in
the
main
relations
of
were
Dissection
understand
to
explained,
of anatomists
the
my
a
levator
the
the
number
mind,
gynecologists
is
the
subject.
of
the
as
bodies
ani
ports
sup-
other
only
For
has
conflicting
to
the
posi-
76
THE
of the
tion
As
uterus.
several
thousand
leans
forward
uterus
of
insisted
the
in
that
the
hollow
the
slight
of
dead
the
Now,
the
sacrum.
subject
back
version
the
that
am
normal
the
ante
normally
I
and
the
on
I
gynecologist
a
in
uterus.
that
PERINEUM;
women,
examination
will prove
AND
VAGINA
have
ined
exam-
that
sure
peated
Re-
condition.
while
and
the
standing
tion
posi-
is the
normal
anatomist
has
often
is in
position of the uterus
I have
repeatedly found
the
is in
uterus
the
of
hollow
BischofE's
method
of colpoand
Kaltenbach.)
Pig. 24." (After Hegar
side of the posterior median
denudes
He
high up on each
perineorrhaphy.
Emmet's
method
This
partially foreshadowed
B, B,A, A.
vaginal column,
the
Bischoff
saved
the
Note
butterfly
operation.
wings, 1, 2, 3, d, d.
posterior
vaginal.
precisely as the anatomist
Both
are
gynecologist and anatomist
the
normal
living woman
position
the
of
that
In
anteversion.
decubitis
the
uterus
sacrum.
In
just
of
has
described.
correct.
In
sacrum,
opinion
generally
such
relative
the
to
a
dead
of
prolapse,
arise
which
hollow
the
can
is
uterus
in
woman
lies in the
manner
the
the
dorsal
of
the
differences
only
be
HOW
TO
MEND
77
THEM.
clinical
and
by careful personal anatomic
of different
A
will
investigation.
comparison
causes
let in the light.
soon
be
of the uterus
the
peritoneal supports
Though
deficient
be put at rest and
they can
finally cured
by
carefully planned operations on the vaginal sphincter
All primary
uterus
apparatus.
supports are attached
cleared
up
neck
to the
of
the
uterus
and
before
the
uterus
shows
such
the supports
attached
to the neck
signs of hernia
be definitely elongated.
the
Doubtless
uterine
must
supports
are
frequently elongated by Infective
cesses
prohence
and
rest
a
by repairing and fortifying
the sphincter vaginal apparatus
will result in restoration.
of
forms
Especially is this true in certain
retroversion.
If
the
uterus
remains
its normal
in
and
position (i. e., perfectly movable) no retroversion
In chronic
infective
prolapse will arise.
consequent
at
times
the
swell, soften,
pelvic organs
processes
of hypertrophy
become
edematous, ending in a form
from
static
I have
frequently observed
congestion.
this slow repeated process
in the clinics.
ETIOLOGY
OF
PROLAPSE.
Insufficiency of sphincter apparatus: a, levator
ani muscle;
h, triangular ligament (anterior posterior
layers and fascia of Colles) ; c, levator ani fascia, superior
and inferior; d, perineum
(composed of levator ani,
bulbo-cavernosus, transversusperinei and sphincter ani
vaginal
ischio-perineal ligaments) ; e, vaginal walls;/, urethroA,.muscular
septum;
g, recto-vaginal septum;
lower
third of vagina.
and
elastic tissue
on
2. Insufficiency of
uteroperitoneal supports:
a,
sacral
ligaments; c, broad
ligaments; 6, round
ments;
ligad, vesico-uterine
ligaments; e, perineum;/,
elongated cervix.
1.
3.
Intra-abdominal
abnormal
directions.
pressure
increased
or
applied
in
78
of
Relaxation
4.
AND
VAGINA
THE
PERINEUM;
anterior
of
c, subinvolution
affords
floor:
facial lacerations;
and
floor
pelvio
uterus, which
of
Weight
5.
pelvio
concealed
repeated labor; 6, submucous,
a,
of
segment
organs.
for intraabdominal
surface
pressure.
OPERATIONS
PROLAPSE.
FOR
4.
(and extension)
Perineo-episiorrhaphy.
Elytro-perineorrhaphy.
Elytrorrhaphy.
5.
'Amputation
flap operation
1. Tait's
2.
3.
of cervix.
of
Shortening
Adams).
6.
of
8. Fixation
the
(hysteropexy).
9. Schucking's
10.
Herrick's
11.
Mackenroat's
uterus,
its
vagina,
their
up
simply closing
board
vulva
we
have
at the
the
operations
but
vulva
on
the
Guillenneau's
vagina
added
in the
perineum
successful
and
a
not
of
with
case
on
work
at
all their
came
variety,
Dieffen-
through
modern
the
the
to
were
Then
and
flap
rhaphy
perineor-
wall
elytrorrhaphy).
successful
that
saw
interior.
operations
(colporrhaphy
has been
quite
could
attempting
forces
and Sims, to
bach, Langenbeck, Simon
Finally to episiorrhaphy
operation.
were
plish
accom-
prolapse
soon
like
was
The
deep
in
uterus
surgeons
Vesuvius.
vulva
not
to
the
early episiorrhaphy
the
But
the
up
idea
the
that
as
attacked
have
pioneer
so
varied
as
ligaments
uterine
The
the
Mount
up
and
vulva
Kuchler.
and
Fricke
Operators
causes.
Thus
escape.
from
operation.
purpose.
to close
"wall
abdominal
the
to
operation.
of
views
was
ligaments.
uterus
operation.
operations for prolapse hav0*been
The
the
(Alexander-
ligaments
round
of broad
Shortening
7
of perineum.
addition
of
the
rhaphy
Elytrorto gyne-
MEND
TO
HOW
79
THEM.
and
hence
operation
cology, but it is a denudation
I have
that
observed
the
tissue.
destroys valuable
and
anterior
operators attempt to save
European
terior
posMen
in
the
of the vagina.
column
columns
see
of
of
valuable
tissue, and
some
piece
a
supporting
like
them,
the
done
the
line, and
its kind,
same
of
(A. Martin.)
the newly-built
25."
a,
IS
the
His
certainly
correct.
made
in
use
of denudation
sion
Dr.
his
operation
and
In
has
is
one
if mastered
it he
has
denudation
and
combined
It
method.
accordina-
posterior
denudes
and
idea
of
of
areas
to
^
could
flap-splittingmethod
it would
operation
vulvar
least
pelvic floor' is
the
supporting
If the
The
the
be
a
marked
and
vaginal operation
should
be superseded
by theflap-extenbe
which
called
might
perineo-episior-
method,
It is done
loss
with
rhaphy.
no
carried
right up to the urethra.
of
and
built
consequent
Emmet
perineum.
of in this
advance.
it.
Colpoperineorrhaphy
columns
resistance.
step
save
thoroughly is successful.
best
principles of the
saves
be
to
try
useful
most
Fig.
Hegar;
the
along
worked
of
Martin,
barrier
of
tissue
and
tissue
The
amount
up
at the
can
of
be
flap
vulva
80
THE
will
depend
the
on
of
exposed
of suturing the
amount
extension
AND*
VAGINA
method
depth of the scissors' clip and the
the mantissue, and also much
on
ner
surfaces to be coapted.
The flapwill form
for
prolapse. The
Adams
operation
PERINEUM;
one
of
the
objections against
1.
are:
best
the
supports
Alexander-
Unsatisfactory reports
and
after
A. Martin,
He
Fig. 26." Colpoperineorrhaphy
styles it elytrorthe two
lateralis.
The
first step
is to resect
denude
rhaphia
duplex
or
ened
the right side freshand
vaginal flaps; the left side is freshened
sutured;
with
the sutures,
but
not
tied,
denuded
flaps.
vaginal
a, a, the
the
bias
quite
not
no
be
a
in
selecting
number
found.
muscular
got inside
of
In
bodies
many
ligaments
the
internal
for
cases
the
cases
could
be
abdominal
2. In
operation.
round
ligaments can
I investigated
which
the
discovered
ring.
until
3. No
one
oper-
82
VAGINA
THE
Mr.
Tait
his
informed
AND
of
me
the
fact
same
in
of
many
operations.
5.
The
sutures
membrane,
or
6. The
are
and
produce
not
7.
The
therefore
in
so
liable
cous
mu-
to suppurate
pain.
flap operation
the
healing
median
calls it
He
colpoperineorrhaphy.
sutured
denudations
the vaginal
1, 2, 3, is the perineorrhaphy
space,
of
The
line
letters
of
indicate
in
secures
the
manner
coaptation and
tissues
not
are
or
certainty of healing.
convenient
most
skin
passed through
step in A. Martin's
Fig. 27." Second
b show
the lines
and
a
perineauxesis
;
The
diamond-shaped
(elytrorrhaphy).
the colporrhaphy
posterior.
following
for
PERINEUM;
sutures.
easiest
and
possible surface
fasciae and
adjacent
widest
the
the
the
for support.
HOW
The
8.
is less
pain after the
than
after
9. Tait's
where
the
10.
28."
Martin's
a
minimizes
11.
and
The
of
buried
time
experience,
operation.
be
can
with
my
practised successfully
operation
a
and
can
excess
continuous
catgrut
not
be
formed
per-
of tension.
suture
(etagr-
suture.
required
do
to
Tait's
flap
ation
oper-
shock.
resulting
linear, and will
disturbance.
in
operation,
denudation
operation
83
THEM.
loss of tissue
continuous
short
MEND
denudation
repeated
It is
The
the
flap operation
because
Fig.
enaht).
TO
cicatrix
thus
cause
is in
its
less
natural
peripheral
location
nervous
84
12.
will
The
cause
no
sulci.
to
observers
trying
builds
and
location, and
thus
to
in
most
the column
save
the
vaginal
a
perineorrhaphy;
6, the
according
to nature's
not
much
end
upper
of
flap operation is that
in a
natural
perineum
buried
;
the
thread;
by
forces
The
part
catgut,
upper
(perineauxesis)
part
end
of the catgut.
c, lower
original law,
violated
natural
subserves
with
operation
Fig. 29." Martin's
posterior colporrhaphy
(elytrorrhaphy)
are
the
observe
can
denudations
perform
all tissue
natural
One
therefore
and
cicatrices
no
irritation.
best
PERINEUM;
superiority of Tait's
The
saves
AND
leave
stitches
practical and
and
trying
it
VAGINA
THE
lower
and
anatomic
cicatrices
and
tures
struc-
cicatricial
contraction.
A
fact
not
neurasthenic
generally appreciated
condition
produced
is the
neurosis,
the
by perineal lacera-
HOW
tions.
with
an
The
visible
the
atrium,
and
MEND
wound
suflPering.
infection
muscle
TO
always
is not
There
be
may
simply
or
fascia, which
85
THEM.
an
stretches
commensurate
visible
wound,
over-stretching of
a
and
traumatizes
irritation.
peripheral nerves,
nervous
producing
hold
The
fascial planes which
the blood-vessels
in distinct
that congestion
and
derelation, are so damaged
Healthy
congestion of the pelvis frequently arise.
the
veins
Fig.
should
30."
be
Profile
spiral
view
A, B, elytrorrhaphy
;
laceration
the
of
D,
of
A.
and
uniform
Martin's
in
caliber.
colpoperineorrhaphy
The
posterior.
E, C, perineauxesis.
pelvic
fascia
allows
the
veins
to
This
straighten out and become
irregularly dilated.
and
dilatation
not
straightening out
produces
only
blood
and
lymph
congestion, but peripheral nerve
The
and
defrequent pelvic congestion
pressure.
deficient
blood-vessels'
congestion from
support, produce
conditions
which
favor
the
of
development
in the genital mucosa.
The
pathogenic microbes
gyn-
86
THE
ecologistsees
which
VAGINA
PERINEUM;
patients with
many
only
can
AND
be
attributed
neurotic
to
phenomena
lacerations
perineal
defects.
and
the
When
will
shrink
look
the
to
can
one
linear
the
sutures
tied
enormously
natural
do
are
the
cicatrix
newly
longer, but
condition.
After
flap operation
will
formed
the
resemble
the
soon
ence
experi-
some
that
so
ineum
per-
it will
on
old
healing
raphe
so
V
Fig.
dotted
of
a
method
31."
Knes
trefoil.
is
Hildebrandt's
the sutures
show
method
under
method
of
Hepner's
method
simply a peculiar
of
the
suture
of
and
denudation
tissues.
is that
The
of
suturing.
denuded
a
figure 8.
area
The
is that
Cleveland's
suturing.
that
scarcely tell after six months
can
closely that one
an
operation has been performed.
also be performed.
For cystocele the flap operation can
is alike
The
applicable to partial and
flap method
The
operation is best
complete perineal laceration.
idemonstrated
complete lacerations.
on
HOW
TO
MEND
87
THEM.
CONCLUSIONS.
GENERAL
hernia
(uterine prolapse),
saoropubio
of the
(sharp) cervix; anterior
perform
amputation
oolporrhaphy; Tait's flap perineorrhaphy.
1.
To
2.
The
cure
amputation
the
removing
cervix
backward;
of
of
sharp
the
cervical
the
purpose
directing the
point;
the
restoring
for
is
cervix
uterus
to
normal
position.
(After Pozzi.)
Pig. 32."
of
tHe
perineum.
vaginal
the
3.
wall
The
1, suture
; 3,-buried
the
backward
the
rupture
suture
The
of
wound.
and
the
fundus
forward.
is for the purpose
flap perineorrhaphy
restoring the obliquity
restoring the perineum;
floor
central
a
genital canal; restoring such
4.
the
in
incomplete
2, submucous
of
colporrhaphy is for the purpose
vagina; elevating the bladder, directing
the
of
deep
angle;
anterior
narrowing
cervix
sutures
in
method
i^autenbach's
of the superior
Tait
of
as
88
VAGINA
THE
will
AND
PERINEUM;
the
efficiently support
bladder,
rectum,
and
genitals.
5. If
does
the
6. If
the
may
be
the
and
uterus
the
bladder
cervix
be
prolapsed,
not
vagina
and
pointed
of
amputation
above
procedure.
the
and
not
exist
not
in
be
cervix
retroversion
may
be
normal
in
anterior
ted
omit-
position
colporrhaphy
omitted.
Tait's
perineal flap
of
consists
in extensive
flaps (by means
operation
front and back
cuts) and the drawing into the median
7.
The
Fig. 33.
of
the
perineal
of
"
stein's
Lauen
which
sutures
line
permanent
after
sutures
large
lateral
weeks
by deep
four
to
masses
are
to
the
granulates
of
sutures
eight
eight weeks,
suppurates,
it
of lateral
masses
These
sutures, six
in complete
laceration.
1, introduction
rectal
of
vagina and
mucosa
; 2, introduction
and
rectal
have
been
fastened.
the vaginal
suture
the
coapt
and
of
success
drawn
silkworm
number,
and
though
maintain
a
and
in
in
sutures
for
tissue
like
part of
it in
floor.
secured
for
These
gut.
act
pelvic
deep
splints for
the
wound
coaptation while
heals.
operations have
proved definitely that the
rectal sphincters may
to normal,
be practicallyrestored
after long periods of rupture.
of thirtyOne
case
even
8. Our
four
years' standing,
with
two
previous
unsuccessful
90
After
daily.
tied
by
the
its
injections
Morphin
of
quiet the pain and
to
14.
The
dissection
1/1 6 of
three
to
one
as
I
procedure
of
rectum
the
five to ten
15.
has
The
been
16.
The
was
Mr.
saw
lengthens
Mr.
thirty minutes;
to
a
rest.
inches,
never
for
induce
Figure
for
The
catheter
the
Tait
wound
the
ically
hermet-
is
limbs
should
will
bladder
The
knees.
of
use
day
oozing.
own
at the
together
require
first half
the
sealed
PERINEUM;
AND
VAGINA
THE
two
to
grain
may
generally
four days.
be given
the
from
be
vagina
34 B.
added
from
This
Tait
do
this.
the
operation
performs
his
perience,
ex-
own
my
to
tional
addififteen
operation
in
minutes.
result
of
the
foregoing
surgical procedure
gratifyingly successful.
flap operation
fits any
and
every
case,
for
HOW
it
is
old
resplits the
required.
MEND
TO
and
cicatrix
91
THEM.
adds
and
restores
what
I have
which
150
single case, in over
the flap operation not
applicable.
observed, was
makes
little scar
18. The
tissue, as the
flap method
in connective
tissue
operative procedure is performed
17.
In
no
Figure
while
cicatrices
form
oolpoperineorrhaphy
made
19.
to
sustain
to
In
give
the
their
the
in
skin
the
34
C.
and
In
mucosa.
posterior
vaginal
the
flap
wall
is
anterior.
the
flap operation
full support
to
the
vaginal
uterus
walls
"
the
are
made
posterior
92
THt
wall
the
sustains
and
also
VAGINA
to
AND
vaginal
anterior
and
support
PERINEUM;
wall
bladder
and
backward
direct
the
"
rectal
wall.
been
has
chiefly revised
flap perineorrhaphy
Lawson
Tait
introduced
to the profession by Mr.
It is true
the
flap perineal
England.
Birmingham,
ers,
performed in various
by othoperation was
ways
and
Duncan,
Colles, Jenks, Marcy
Langenas
The
and
of
Fig.
that
we
A, B, C, D."
34
as
For
example,
originally torn.
should
large as B, B, X, in A, and
in
B
the
vaginal
C, Y, D,
the
rectal
sewed
part
up;
beck.
in
But
performed
elbow
Mr.
Tait
it with
scissors
and
new
denuded
be
;
the
line
X, Y,
perineal
is
gave
wrought
it
a
phases.
introduced
which
area,
Freund's
in
sutures
with
new
He
size
that
to
of sutures,
the
to
corresponds
suturing
denuded
C, the
D, the final disposition of the
and
but
complicated,
one,
if the operation
fails.
A.
Freund
method.
the
perineum
exactly
as
the cicatrix, O, O, originally
denudation
"when
represents
Freund's
(After Pozzi.)
the
make
should
the
B, A, B, in C shows
rectum
suturing;
is still unsutured;
method.
much
;
It is
sacrifice
impetus,
performed
sutures
insists
appeared
appeared
line X, Y,
which
an
lent
excel-
of
tissue
and
also
it with
neither
skin
penetrated
for
MEND
HOW
TO
nor
mucous
93
THEM.
membrane.
As
a
pupil
I had
ample opportunity
of operation.
The
methods
his
to observe
principle
old perineal
of operation consists
in resplitting the
loss of tissue, with
fixed
without
cicatrix
coaptation
methods
I
of the flaps. After
observing Mr. Tait's
performed
by
naturally practised the
as
operation
Mr.
of
and
him
to
Tait,
his
(1
to
for
other
enabled
modification
year
to
me
variable
a
the
above
2J inches)
a
by dissecting
operation
each
from
vagina
About
assistants.
the
modify
months,
six
apply
I
later
the
tance
dis-
long
This
anus.
or
and
rectum
but
vulva
began
it to almost
all forms
tion;
perineal laceraall conditions
in short, in
requiring perineorrhaphy
and
objections
colporrhaphy
posterior. The
raised
found, after over
we
against the flap method
One
six years' trial,were
not well founded.
objection
skin
Tait's
is a
is that
flap perineorrhaphy
tion."
operaIf performed
be
it
subject
superficially
may
such
criticism
above
criticism.
to the
However,
can
The
only be applied to imperfect execution.
tor
operathe
vulva
too
must
carefully guard against closing
excessive
far.
One
by
an
perineum
easily make
can
of
This
the
flap method.
objection is, as a matter
Another
fact, worthless.
objection is that the flap
This
the vagina.
method
in no
tion
objecnarrows
way
will not hold, as the vagina can
be narrowed
so
as
of
prolapse, relaxed
vaginal
wall
or
"
to
embrace
can
tightly
dissect
for three
the
inches,
narrow
much
operator
the
the
to
up
the
of the
index
finger.
vagina from
and
rectum
desired, and
as
single
a
peritoneum,
lower
fit.
sees
third
The
of
or
the
upper
In
fact,
other
each
as
we
high
vagina
two-
unite
the
levator
the
ani.
It is
deranged
dissection
or
Another
require narrowing.
the fibers
not
approximate
the operation
excellence
par
torn
is carried
levator
beyond
ani
the
as
thirds
not
vagina does
objection is that it does
the
as
of
to
fibers, because
levator
ani
fascia
94
VAGINA
THE
AND
PERINEUM;
superior and inferior through the
In
the
fact, it enables
operator
levator
the
levator
fascia
ani
levator
muscle.
ani
fascia
ani
and
superior
to
to
muscle.
ani
both
secure
the
inferior, which
One
order
in
levator
must
the
secure
the
secure
braces
em-
levator
ani
method.
R. Simpson's
It is really
flap
a
the lines of incision
c represent
cut, a, b and
the flaps ; S, vagina
to make
flap ; 2, 2, rectal flap. The scissors
; 1,1, vaginal
at n, and
then
the point emerges
clip is made
first entered
at b, and
a
;
are
and
the vaginal
entered
between
at 1, and
the scissors
pushed
second,
are
the rectal
and
to 1, and
walls
rectal
vaginal flap. Dissect
over
a clip makes
Fig. 35."
operation.
(After
In
the
A.
Pozzi.)
left
hand
To do this,
the rectal
high as the case
requires.
as
vaginal flap from
the assistant
several
small
the vaginal
can
flap with
forceps, which
allow
several
small
and
the rectal
forceps
also seize
flaps with
gently hold;
the flap on
tension
to put
their
is sufficient
to hang,
them
weight
; with
as
the dissection
scissors
and
the two
pair of blunt-pointed
fingers in the rectum
a
introduced
sutures
made.
The
of the flaps is conveniently
as
are
and
made
Observe
that
in this operation
four
shown
in the cut.
flaps are
the
seize
that
the
and
in
and
the
sutures
rectal
and
1, 2, 3,
flap making
only
which
all cutures
one
vaginal
are
walls
entered
is absolutely
flap is made
are
in denuded
sutured
are
by
passing
different
and
from
no
tissue.
also
separately;
the
through
that
sutures
of
Mr.
enter
Tait's
the
note
The
skin.
skin
that
suturing
flap method,
or
mucosa,^
HOW
MEND
TO
95
THEM.
guarded and embraced
by a definite
The
fascial sheath.
the posreunites
flap operation
terior
fascial
without
denudation,
vaginal
septum
as
which
muscle,
Emmet's
Tdit's
and
the
on
the
the
unites
operation
Emmet's
and
is
does
other
wound.
My
of
not, but
makes
Perineorrhaphy''
"Its
field
employs
the
however,
the
to
cover
and
rectum
American
the
writer
book
Text-
"Flap-splitting
on
following
of usefulness
ally
anatomic-
flap
a
dissect
In
the
Both
denudes
one
"
sulci.
Gynecology
based
are
is to
practice
lateral
the
in
vagina
denudation.
operations
principle
same
with
it
absurd
ments:
state-
limited
is very
those
indeed.
in which
Practically it is applicable to
cases
most
exterior
fibers
of the
only the superficial and
The
torn."
above
views
are
perineum
can
certainly
be based
imperfect knowledge, execution, or
only on
of the
observation
is
of
one
the
is the
an
operator
and
inferior
*with
blind
without
makes
a
first, that,
"In
of
the
further
fascia
statement
ridiculou
as
fascia."
that
does
It is fortunate
not
represent
the
this
of
views
it will
narrow
bring together
fascia
levator
menta
superior
ani
the
the
and
fibers
muscles.
ischeo-perinei.
inferior
Also
The
with
of
the
securely
flap method
it
and
a
to
cited
s
as
the
text-book
all Americans.
vagina, abolish
separated
muscle
operation
rectocele,
a
the
pelvic
"American"
flap-splittingperineorrhaphy, in the hands
have
thoroughly practised it, has proved
that
superior
writer
same
(flap-splitting)narrow
or
bring together the
way
enables
ani
this
possible can
the vagina, abolish
separated fibers of
no
colpo-
rectocele,
a
The
uterus.
that
it
tions
opera-
of
levator
abolish
to
method
ani
enclosed
searching,
repair prolapse
above
the
that
all
of
all others
levator
the
reunite
to
flap
above
one
affirm
can
effective
The
perineum.
perineorrhaphy
We
and
certain
most
the
on
operation.
The
of those
who
absolutely
rectocele, and
levator
the
fibers
unites
of
the
is alike
ani
the
ligause-
96
VAGINA
THE
PERINEUM;
AND
partial and complete operations, and
does
all that Emmet's
rectovaginal dissections
ful in
with
and
denudations,
no
with
the infectious
healing, by avoiding
better
a
in
high
does,
Also, like
atrium.
Emmet's
operation, Tait's flap-splittingis founded
anatomic
structures
Both
functions.
Fig. 36." A perineal
hand
in the
traction
are
by the
the
between
flap
to
be
rectum
fbrceps
rectal
and
designed
operations
laceration
to
the
to
rectum.
logic
physio-
restore
have
Two
on
to
come
fingers
stay.
left
the
of
tension
lateral
is put on
recto-vaginal
septum
; the
inserted
is
the
scissors
of
each
side
the
blade
on
;
the
marks
out
line
the dotted
vaginal walls, and
produced.
The
conception
the
pathologic
a
vulva
These
old
of the
flap-splittingoperation
of the
conditions
lines
white
perineal
which
lines
lacerations
are
If
wound.
lacerations, he
with
white
narrow
of the
and
of
chance
are
the
The
will
see
linear
on
amines
ex-
one
linear
transverse
healed
rests
in
trices,
cicasection.
dis-
cicatrices
cicatrix
is
98
VAGINA
THE
The
required.
forceps and drawn
flap is seized and
from
rectum
of
(Modified
standing,
lines.
healing
rectal
old
and
The
produced.
are
made
the
to
"
Back
produce
vagina,
vaginal flap is seized
the posterior
forward, while
drawn
backward.
vagina
Pozzi.)
from
with
with
the
larger
anteriorly.
the
A
lateral
each
on
cicatricial
extend
perineal
to
introduced
side
the
body.
scissor
A
illustrate
handles;
Sims'
tissue
to
3
ation
lacer-
showing
between
the
how
the back
speculum
the
each
on
space
cicatricial
margins
(IJ
recto-vaginal
extensive
very
rectal
dissect
desired
as
radiating
large
blades
at
We
high
as
time
same
cuts"
a
PERINEUM;
anterior
scissor
walls
vaginal
are
into
the
At
inches).
Fig. 37."
the
AND
the
flaps
cuts
is inserted
the
of
side
the
make
required
to
The
fingers of
two
the
in
rectum
of
size
as
the
narrowing
be
the
sufl"cient
out
bleed
check
it.
soon
nal
check
it will
If
disinfected,
and
of
extent
of
condition
object
in
for
the
the
of
tion
dissec-
parts, the
whether
view;
extension
passage
few
a
the
the
it
perineum,
With
prolapse.
siderable
con-
need
may
cut
avoid
to
vulvo-vagi-
a
open
should
gland
order
in
arteries
scissors
whole
the
abscess
The
kept continually
clamping;
hot irrigation will nearly always be
If the
be
bulb
the
hemorrhage.
will
profusely, but
sponge-pressure
the
to
are
the
the
dissection,
however,
left hand
vagina,
closing
almost
or
as
extensively as is
(See Fig. 19)
perineal body.
and
wound,
the
dissected
guide.
by the
a
governed
is
is
vagina
99
THEM.
MEND
TO
HOW
dissected
be
abscess
an
out
in
the
wound.
of silkworm
sutures
the
from
wound
or
about
one-half
flap
needle
again
on
the
wound
along
the
from
the
median
sutures
edge
and
line.
It
the
is
the
the
made
(No.
flap
to
threaded
in
4 in
drawn
Generally
the
above
the
It
of
of
the
the
inch
on
out.
is
forced
one-half
again
emerge
and
the
angle
Fig. 21),
about
of
along
vaginal
raphe.
point
The
upper
of
the
angle
carried
median
the
of
point
penetrating
edge
out.
at
first suture.
introduced
are
of
distal
the
side
opposite
edge
constitutes
from
introduced
distal
without
the
removed
are
upper
membrane,
mucous
at
emerge
and
drawn
is
the
at
to
threaded
The
cleaned.
Fig. 21)
in
fingers
two
introduced
inch
made
and
then
is
(No. 2
vaginal
skin
The
well
and
is to introduce
operation
gut.
rectum
needle
handled
the
step of the
second
The
the
This
anterior
three
manner.
To
(three or four) the
posterior sutures
index
be placed in the rectum
a guide,
as
finger should
rectal
close
too
to the
to avoid
passing the needle
introduce
the
fistula.
endangering
quickly or slowly. If quickly
mucosa,
The
an
fistula
abscess
may
arise
will
arise;
100
AND
VAGINA
THE
PERINEUM;
slowly (two to four weeks) a fistula will arise and
In one
time.
remain
a fistula
case
longer or shorter
a
The
posterior sutures
are
persisted for three years.
anterior.
similar
to the
introduced
However,
they
should
include
be
and
the
should
deeper
thoroughly
fascia
and
inferior
with
the
ani
levator
superior
if
Fig. 38.
neorrhaphy.
the
(Author.)
"
Here
but
anus,
the
and
sutures
the
median
field, but
half
at
a
line.
one
time.
can
the
A
safest
and
make
more
as
anterior
may
perfect
be
the
method
end.
thrust
and
the
if
practical
most
needle
of
progress
appear
the
tie from
The
in
stage
sutures
All
across
deeper
colpoperi-
flap-forming
is
started
had
process
to
sutures
the
suturing
begin
are
to
at
duce
intro-
threaded
denuded
in
entire
by doing
one-
HOW
enclosed
needle
the
levator
skin,
where
into
passed
is
and
The
muscle.
ani
the
pushed
edge
of
onward
is
the
point emerges,
introduced
again
101
THEM.
MEND
TO
the
to
point of the
wound,
avoiding
median
the
line,
threaded
and
drawn
out.
and
opposite side
In all cases
threaded
sive
in the middle.
requiring extenshould
be
needle
the
dissection
passed through
In the less extensive
half of the wound
only.
part of
needle
the whole
the
wound
the
through
may
pass
five
Tait
three
Mr.
to
at
employed
;^ound
once.
sutures.
We
sutures.
employ five to seven
of silkworm
The
third
gut.
step is to tie the sutures
distal
end
the
the
left
All the "sutures
seized
at
by
are
while^he
hand
pushes the tissues of the
right hand
wound
far toward
the loop of the sutures
ble.
possias
as
and
This
it
is a partial step, as
puckers
narrows
individual
that
when
each
the wound
much,
so
very
It
is
is
suture
tied
it
should
sutures
on
assumes
be
not
tied
the
its
final
location.
too
tight, as
they
The
are
apt
After the sutures
tissue.
through considerable
width
will exist
tied, a linear gap of considerable
are
do
not
in the niedian
line, for the sutures
penetrate
draw
the skin, and
hence
will not
it in close coaptation.
will
be
of
the
Here
inexperienced
some
the
skin
to
avoid
sutures
to
tempted
place a few
Be
not
to do it, for
they
sure
gaping of the wound.
the
abscess; when
an
produce
cause
pain and
may
will
legs are placed together the edges of the wound
The
ends
of
be
left long
the sutures
should
coapt.
to cut
and
all
tied
consists
into
in
a
single
applying
no
bundle.
dressing
The
or
ment
after-treat-
chemicals
to
dermic
pain small hypofor
of
be
used
doses
thirty-six
morphin
may
Most
hours.
patients will require catheterizing, from
After
of the pubic
to the
distal ends
trauma
nerves.
quarts of a
we
forty-eight hours
begin to give two
bowels
The
and
morning.
vaginal douche, evening
the
wound.
If there
be
considerable
102
THE
should
be
of calomel
times)
and
should
Diet
before
and
YAGINA
third
on
the
Fig. 39." (Eobinson-Holland.)
flaps in the flap method
and
patient should
afterward
get
should
remain
lie in
up
as
If
If
become
for
none
three, four
or
Method
of
be watched.
removed.
fourth
day by means
given in small doses (1 grain two or three
followed
by teaspoonful doses of MgSOi.
limited
for three
be regulated and
days
to the operation.
three
days subsequent
moved
posterior
The
PERINEUM;
AND
one
of
bed
she
at
anterior
least two
able.
is
becomes
even
of
and
colpoperineorrhaphy.
for
ioosa
or
formation
executing
loose
or
The
weeks,
sutures
it should
separate they
six
weeks.
be
may
Three
HOW
MEND
TO
103
THEM.
.
weeks
is
heals
wound
weeks
The
more.
or
which
be
better
in
must
be
tight
as
not
disturb
might
THE
This
ones
labia
first
it would
perhaps
anesthetize
to
the
it.
vulva
steps in the
the
Amateurs
unnaturally
relations.
marked
The
cuts
technique.
to all
contrast
as
purposes,
the
was
sutures
OPERATION.
is in
similar
for
the
EMMET
operation
and
marital
will show
The
union.
practise
close
to
four
splints, holding
avoiding
motion,
cases
never
for
in
like
coaptation,
I
The
sutures.
sutures
act
neurotic
some
article
the
on
warned
it
the
perfect
removing,
However,
patient.
with
with
pain
give
the
remove
sutures
fixed
in
interferes
often
to
firmly
more
surfaces
the
in
enough
soon
of
union
The
procedure.
the
previous
denuded
peculiarity
of
Emmet's
of the lower
in denudation
operation consists
median
denudation
posterior vaginal wall; bilateral
of
sulci
of
lateral
the
triangular portions of the
of
vagina; in the method
introducing the sutures,
which
arranged that on tying they lift the proso
are
lapsing
the pubic
arch, restoring anaparts toward
tomic
to the vagina
the
and
structures, as the H-shape
of the vagina.
The
normal
be
curve
patient should
and
prepared for several days by cathartics
daily skin
baths.
The
bowels
be evacuated
should
by eight to
twelve
while
operating,
salt
of
In
and
tenacula
example,
one
the
bowels
will be
36
hours
not
climax
and
"
at
their
the
to
at
definite
the
median
holding
points of
crest
the
rectum
ough
Thor-
only
stimulates
the
of
secretion
but
kidneys
active
to
organs
"
skin,
activity for
patient on
maximum
anesthetized
assistant
in
after.
short, place all secretory
an
fixed
to
skin
to
the
Place
with
24
the
skin
kidney
operation.
back,
the
stimulates
secretion.
bowel
of
feces
no
for
nor
rubbing
apparatus
reflexly
that
so
passages,
each
the
of the
limb,
the
the
With
vagina, as
rectocele,
for
one
104
THE
tenaculum
point
one
the
with
junction
the
side
of
outline
well, before
large
too
undue
the
of
of
the
vagina
denudation
the
of
in
a
skin
and
the
denudation
Others
to
The
the
median
the
in
with
a
highest
sulci
wall
one
mucosa,
defined
area
line.
during
by the
the
This
denude
drawn
was
the
from
the
in
off
It
is
is
area
without
tenacula
the
handled
a
is
in
sutures
needle
photograph
long strips
curved
scissors
vaginal flap on a staff
large areas
may
requiring denudation
of slack
that
mark
scalpel.
the
the
at
can
introducing
Note
cutting
operator
with
cut
of
by
and
operation.
with
mucosa
amount
the
the
denudation, to test whether
insure
coaptation of the wound
patient
vaginal
at
posterior vaginal
Method
Fig. 40," (Robinson-Holland.)
of colpoperineorrhaphy.
flap method
denuded
the
PERINEUM;
of
the
tension.
is threaded
taken
AND
side
triangle
each
on
each
on
of
VAGINA
the
on
scalpel, rolling the
or
on
be
in
the
fingers.
rapidly denuded.
the
the
lateral
sulci
of
flat.
denuded
With
The
rience,
expearea
depends
on
posterior vaginal wall, for
106
VAGINA
THE
AND
PERINEUM;
points of the
(at the emerged
the operator,
in the denuded
suture
triangle) toward
the plan of suturing; i. e., they are
and
characterizes
in an
introduced
antero-posterior direction, and by
the pubic
tying, they lift the vaginal outlet toward
The
is introduced
next
suture
arch.
by passing the
side
needle
through the vaginal wall (on the internal
angle,
with
its
apex
of the plan of Tait's
flap colpoperineor
with
perineal body ; V, vagina,
P, intact
six
the
by
P,
urethra
it ; ", has
had
the torn
body,
repaired
above
perineal
anterior
the
marked
sutures
H-shaped
cuts, a, 6 ; c, (/,
by stars ; c, shows
the posterior
cuts
rectum
; V, vagina.
; R,
Fig. 41." (Author.)
rhaphy
: a, S, sacrum
of the
denuded
whence
Diagram
;
R, rectum
;
triangle) deep into the subvaginal
the
triangle (directly toward
it
point and
operator)
and
emerges,
carried
upward
very
deeply
under
tissue
operator),
is
re-entered
at
and
outward
(away
the
denuded
of the
the
area,
same
from
the
emerg-
HOW
TO
MEND
ing on the vaginal mucosa
sutures
triangle. The
denuded
triangle should
include
extensive
sutures
The
called
suture
passed, which
be
applied
crown
the
will
distance
the
It
the
is
the
of
of
and
point
the
should
as
the
the
in
the
to
four
as
sutures
incision,
tissue
The
in
The
be
to
The
the
mucosa
triangle.
subvaginal
cus.
sul-
soon
triangle.
passed within
introduction.
carried
tied
the
the
needle
of
center
of
of
now
close
the
in
and
side
superficial
part
wall
be
can
more
suture
the
emerge
below
to
upper
vaginal
below
external
especially deep
enable
the
to
side
Generally three
or
close the triangle of each
base
of each
triangle may
by introducing
lateral
should
be
suture.
pursing
or
vagina
at
tension
a
the
external
tissue.
sufficient
are
the
at
on
107
THEM.
on
short
a
needle
the
sulcus
needle
is
entered
re-
the
just
vaginal sulcus
the vaginal incision, emerging
below
the opposite
at
side.
One
two
added
or
auxiliary pursing sutures
are
and
the
several
sutures
tied; superficial sutures
are
then
added,
in
the
as
required, to close the
gaps
The
wound.
should
be of silkworm
deep sutures
gut
the superficials of catgut.
and
In
this
it is not
essay
after
repair
toward
chronic
floor.
It
will
will
show
demand
as
such
One
had
a
intents
show
the
views
decide
to
in
pursue.
with
but
damage,
differences
the
certain
cases
Some
cases
.few
but
pelvic
of
symptoms,
purposes
will
in
appears
of
complain
rest
on
perineal
visible
tions
lacera-
create
symptoms
probability lead to
occasionally meet
a
patient who
and
the
to
operation,
perineum
lesions
may
directed
are
examination
to
little
diate
imme-
vulva, vagina and
careful
plan
Such
the
Extensive
supports.
repair whether
they
perineal
and
of
wisest
suffering.
invisible
but
uterus
to discuss
purpose
laceration
others
severe
not,
the
extensive
while
and
be
and
the
labor,
damage
require
vulva, vagina
what
across
all
normal
;
yet
an
or
ness.
illhas
all
exami-
108
THE
nation
reveals
AND
VAGINA
the
fact of
a
PERINEUM;
reotocele
above
the restored
the results of
patient confirms
the examination
ing.
by still announcing herself as sufferIn
of the
so-called
operating, the dissection
the
extend
rectoperineal body should
as
high on
perineal body,
and
the
outlines
of the
anterior
(A, E,) and
Fig. 42." The
"cuts,"
posterior
(A, B,) in the
/i,urethra;
flap colpoperineorrhaphy.
to, Clitoris;
The
L, P, anterior
vaginal wall ; A, N, anus
; N, R, perineum
; E, C, labia.
orifice
The
laceration
is not
is wide
vaginal
complete,
i.e.,it does
open.
'*cuts"
not
reach
the
rectum,
there
vaginal septum
redundancy
as
appears
posterior vaginal wall (rectocele). Nothing
the patient.
The
perineal body, in its
cure
is a resistant
ligamentous, fibromuscular
sense,
of
the
less will
broadest
struo-
HOW
closes
which
ture
body
line
begins
located
of
side
impressed by looking into
and
as
soon
bowl-shaped,
becomes
lost, the supports
Observed
point.
to
the
from
cloaca.
are
in
the
white
curved
be
pelvis, as one
may
It is
above.
pelvis from
this
as
shape
peculiar
have
at
some
given away
a
below
between
space
orifices
from
The
the
the
and
repairing
direct
is
perineum
rectum
of
is capable
flap operation
In complete
the pelvic floor.
vulvar
cavity below.
supported
each
on
109
THEM.
abdominal
the
be
to
MEND
TO
laceration
The
vagina.
defect
any
the
anal
in
and
like
communication,
jack
boot-
show
The
rowed
nar-
a
a
rectovaginal septum
may
The
outline.
ularly-to
irregangle or an irregular arched
of the rectovaginal septum
outline
shows
a
the
sides.
At
double-walled
layer or curved
upper
the
of
rectal
the lacerated
angle
rectovaginal septum
red
or
a
pink
mucosa
as
pouts, rolls and
appears
line to split the
aids
in locating the
which
ground
flaps.
been
lacerated
the rectovaginal
has
After
septum
for a long time
it presents
irregular cicatricial bands,
of which
ent
thin, others thick, assuring differare
some
and
contraction.
Bridges or
stages of atrophy
of tissue
from
bands
stretch
one
point to another
may
condition.
a
showing
penetrated
Again, the lower
be
edges of the lacerated
rectovaginal septum
may
drawn
still
ani
by the fibers of the levator
upward
fascial
embracing the parts by the aid of its double
sheets.
Besides
be
small, irregular depressions may
felt or
the
observed
of the
where
stump of a bundle
levator
The
muscles
deep
has
been
torn
applied after
will include
these stump
ends of
of
fascia
be
that
so
they may
median
fixed
there.
raphe and
does
or
not
sutures
need
to
rectovaginal
observe
septum
and
away
splitting
the
retracted.
the
muscles
again
The
forced
by
septum
means
to
the
flap operation
whether
the sphincter, anus
be
lacerated, for it is alike
110
THE
applicable
find
VAGINA
each
to
all kinds
of
and
AND
all.
associated
PERINEUM;
On
examination
conditions
with
extensive
cervix,
colpoperineal lacerations, as lacerated
of the vagina, cystocele, rectocele, and
of the
Dissection
Fig. 43."
drawn
up
two
introduced
the
wound
the
median
X, urethra
Now
uterus.
the
of
flap and
if the
the
uterine
anterior
The
forceps.
posterior
flap, S, is drawn
already passed ; three
6, n, are
sutures,
more
the curved-handled
needle
from
by passing
with
to
the
line
;
middle
with
of
silkworm
L, P, anterior
the
denuded
gut ; D, I,
wall.
vaginal
surface
anus
;
may
we
volution
subinversion
retro-
appendages
vaginal
wall,
backward
sutures,
the
N,R,
by
one
lateral
ceps,
for-
being
edge of
it from
threading
V, perineum
; E, clitoris
and
;
HOW
freely
are
TO
movable
we
repair
by curettement,
of the
rhaphy, for much
circulation.
disturbed
from
their
The
veins
the
become
the
patient
colpoperineor-
observed
disease
bed
cure
and
cervix
vessels
The
supporting
have
generally
can
of
Ill
THEM.
MEND
been
have
Pig. 44." Sutures
tied
in the
operation
incomplete
laceration.
L, M,
A, N, anus;
median
line
E,D,
of the
raphe;
peripeal
for
torn
dilated
colpoperineorrhaphy
labia;
A, clitoris;
P, posterior
point
to
fascia.
the
deranged
straightened out,
by
du6
is
with
V, urethra:
of
perineal
space.
locally,and
in
and
blood
have
elegant spiral form,
stasis, congestion.
circulation
The
lost their
will
diagnosis
Restore
the
ing
result-
supports
resume.
consists
of
observation
and
palpa-
112
with
tion
appearance
is
a
is
like
of
widest
perineum
PERINEUM;
speculum.
large Sims
is the
notably striking feature
of the vulvar
outlet.
Normally
aid
the
diagnosis
AND
VAGINA
THE
its
at
The
changed.
of
aperture
end.
upper
vulva
the
relaxed
or
In
a
the
natural
the
vulvar
neum
peri-
lacerated
external
ance
appear-
chink
puckered
narrow
changed
With
whole
the
slit-
or
orifice
is
formed
trans-
patulous gaping.
Again, the normal
with
the
vagina presents a sigmoid curve
posterior
wall
vaginal
coapting and embracing the anterior, like
valve.
But
in
deficient
a
vaginal apparatus these
into
a
have
lost their
tions,
relacoapted
curves
It should
especially the posterior vaginal curve.
this deficiency
be remembered,
in diagnosing
at the
due
is not
vulva, that the non-closure
especially to
in the levator
loss of the perineal body,. but
to defect
two
concentric
ani
muscle
and
its double
ani
muscle
endows
fascial
levator
The
layers.
,
and
lower
the
drags
the
with
rectum
of
end
the
its anterior
curve
and
upward
vagina
This
fact can
against the pubic arch.
demonstrated
by introducing the finger into the
when
and* downward,
and
forcing backward
be
forward
finger, the
the
removing
normal
position.
sphincter like the
sphincter, the
by the pubic
and
the
mouth
or
arch
vagina is
antero-posteriorly between
There
It is H-shaped.
vagina
closed
The
muscle.
at its
external
nothing
of
the
in
it
is
a
orifice
physiology
position of
muscle
the
muscle, but
bulbo-cavernosus
to
acts
bundle
anterior
the
produces
and
rectum
a
but
has
like
a
indirect
an
ani, aided
levator
of the
indirectly closed
is
the
anus,
loop
The
arch.
by
to its
vagina quickly returns
vaginal orifice has no distinct
horseshoe
vagina
of
The
ina
vag-
fixed
by shortening,
of
the
rectum
and
practically this
On
anatomy.
in
sigmoid
relation
curve
arch.
pubic
of
to
to the
ani
its walls
of
slight puckering
means
tracting
con-
levator
by flattening
by
point
the
the
weak
amounts
account
the
tor
leva-
rectum,
114
THE
direction
the
plane of
levator
ani
of
that
to
thumb
into
with
closure
of
when
of
finger
second
a
the
well
vagina
Tait
of
elements
perineal
sphincter
studied
success
the
of
apparatus
virgin
which
the
third
acts
on
both
the
the
on
a
one
The
the
pubic
almost
as
This
intact.
is
Emmet
the relaxed
is
multipara
a
one
and
difference
vast
and
and
first
toward
The
and
apparatus.
forward
in
essarily
nec-
appreciated
vagina
nullipara, and
operations.
between
appearance
the
is best
of valve,
produces a kind
certainty against prolapse while
the
be
may
arch
of
it must
vagina upward
vaginal sphincter
the
words, the
plane of the
to the
into
It
on
other
it contracts
end
rectum.
deficient
a
is anterior
and
the
the
and
multipara
In
considerations
introducing
by
PERINEUM;
rectum.
lower
the
These
forward.
the
arch
pubic
muscle,
drag
AND
VAGINA
in
vaginal
due
to
the
of labor in nearly
by the process
This
does
all cases
not
(visceral ptosis excepted).
consider
that the
so
we
virginal
strange when
appear
inch
in
the
is
about
of
an
diameter,
vagina
passage
and
breech
demand
the passing head, shoulders
while
It is not
inches
diameter.
in
ten to twelve
strange
of
yielding
that
tissues
supports
from
to stretch
forced
one
to twelve
inches
The
levator
muscle
ani
is
forget to return.
become
arranged in fasciculi or bundles, or it would
defective
frequently. The sphincter and vaginal
more
accidental
be
injured by external
apparatus
may
should
trauma,
but
Relaxed
labor
is the
vaginal
musculo-fascial
deep
chief
factor.
outlet, concealed
tears
of
lacerations
or
not
pelvic floor, can
notice
of the physician
the
forcibly brought to the
for colpoperinean
as
important diagnostic indication
relaxation.
orrhaphy.
Kelly calls such, concealed
of loose, gaping
This
is a condition
vulva, compared
its puckering-string by
of a bag without
to the mouth
be
Dr.
of
too
Emmet.
the
If
buttocks
the
patient lie on
looks
flattened, the
the
back
anus
the
fork
appears
HOW
TO
everted, and
one
bulging out above
described
Others
that
call
it
can
perineum
stretched
rectum
ekin
line
or
mucosa.
or
as
the
below.
The
rectocele
or
vaginal
mucosa
condition
is
cystocele, or
quently
fre-
both.
it
Fig. 46." Advanced
vaginal flap held
up
by forceps ; the most
median
observe
may
115
THEM.
will
Some
write
perineal laceration.
be perineal laceration, because
not
the skin
is longer than
the
normal
The
skin
one.
is longer than
normal
it was
because, when
at labor, it never
returned
to normal
(sub-
perineum
torn
MEND
;
other
and
stage of the flap-splitting operation.
L, V, anterior
by forceps
rectal
posterior
flap is held backward
; the
suture
is placed
posterior
the
of the
along
margin
sutures
introduced
threaded
being
in the
are
by being
drawn
out.
Note
that
the
needles
do
not
penetrate
the
116
THE
VAGINA
AND
PERINEUM;
introduce
the four
can
involution). Occasionally one
and
fingers of the hand
put the long relaxed perineum
It is in these
stretch.
on
a
long, lax skin perinei .that
physicians disagree as to conditions, the one
asserting
that the perineum
is plenty large enough
and
does
not require an
operation, while the other rightly asserts
that the perineum
is but
small
a
part of the support
of the sexual
fact is, the whole
The
vagina
organs.
and
become
sphincter apparatus has
deficient, the
Fig. 47."
Another
Observe
that
the most
stage of flap forming.
terior
posis being
introduced
from
side of
by the needle
passing
one
the
denuded
wound
to
the
the
but
is short,
the
other, because
space
denuded
surface
under
the flap is generally
wide
that
it is most
so
tical
pracsuture
to
the
pass
median
threaded.
time.
the
handled
line, where
Thus
the
sutures
needle
the
from
needle
are
passed
the
is
lateral
of
margin
allowed
to
through
half
emerge
of
the
the
and
wound
to
become
wound
at
one
HOW
yulva
the
pouts,
flattens
117
THEM.
everts, and
anus
If
MEND
TO
the
floor
of
the
vis
pel-
the
patient is requested to bear
and posterior vaginal walls will roll
down, the anterior
outward, often to an
astonishing degree.
By the act
of straining, the cervix
The
felt descending.
be
can
is
patient has utero-ptosis. The
sacro-pubic hernia
out.
^*iijfe"-'
Fie
48
anterior
ani
ossus
operation
"Finished
and
end,
is
a
A,
F, posterior
in
a
end
of complete
.laceration. R, L,
newly-built
perineal raphe;
A, N,
case
of
little patent.
ing
patient in the standinspection and
palpation
position. By careful
the back, one
feel the
while the
patient lies on
may
ends of the lacerated
levator
retracted cicatricial stump
marked
more
ani
or
one
examines
by irritating
depressed stumps we
muscle,
vated
if
and
the
the
can
little cicatricial
see
the
ele-
contractions
118
THE
relaxations
and
VAGINA
in
AND
them.
PERINEUM;
Sometimes
wall
the
perineum
that it
posterior vaginal
so
to close
the vulva
like a valve.
is large enough
up
horseshoe
extends
The
loop of the levator ani, which
to the other, presents
from
pubic ramus
one
no
more
elastic
the resisting, broad,
loop felt in the virgin, but
feels
in the middle
one
an
irregular sharp edge of
or
lower
Fig. 49." (Author.)
laceration, with anterior
narrow
dimensions.
Method
and
relaxed
is
of forming
the flaps with
and
vaginal
posterior "cuts"
Also
the
loops
of
the
a
non-complete
flap.
levator
are
displaced to the side of the vagina. Though
the patient can
stool, yet the vigorous
generally control
paired.
loop is definitely imelasticityof the muscular
the
back
and
the two
With
the patient on
index
can
quickly test the
fingers in the vagina, one
degree of deficiency of the sphincter vaginal apparatus
The
and
backward.
vulva
downward
by pressing
more
TO
HOW
be
with
pout
may
said
of
side.
other
perineal
In
long-continued
very
intact, and
The
on
fascia
side
one
sensitive
irritation, the
reflex
delusive, because
119
THEM.
skin
rectum.
quite defective
be
may
the
MEND
the
levator
and
and
same
intact
made
women,
examination
irritation
may
ani
the
on
by
worse
is occasionally
puts
parts
on
a
tension.
We
Fig. 50."
_
scissors
are
scissors
only
rhaphy
classify
may
the
(Eobinson-Sclaoler,)
the
forming
is shown,
forming
shown
three
for
operations
The
anterior
the
colpoperineor-
flap formation.
"cut
posterior
;"
on
'"cut"
On
the
beside
general divisions,
oolpoperineorrhaphy, posterior
into
left
right
the
the
the
blade
of
the
the
rectum.
viz.:
posterior
colpoand
the posterior flap oolpoperineorrhaphy.
perineorrhaphy,
of the principal originators and
cates
advoSome
of posterior median
oolpoperineorrhaphy
were
Baker-Brown,
Osiander,
Dieffenbach,
Langenbeck,
Simon,
belle, Le
Jobert, DeLam
Hegar, Hildebrandt,
and
Reamy.
Fort, Sohjoeder, Werth
median
bilateral
120
The
AND
VAGINA
THE
chief
originators
are
colpoperineorrhaphy
colpoperineorrhaphy
classes
Fig.
bottom
rectal
up
into
the
and
of
the
posterior flap
Duncan,
Tait,
Langenbeck,
Marcy, Colles, Sanger.
differences
apparent
of
procedure,
that
all
the
of
the
advocates
above
praoti-
the scissors
at the
with
Flap formation
vaginal flaps. 1, 1, vaginal flaps held
cuts;" 4,
flaps; 3, 3, "back
crooks, 6, 6; 2, 2, rectal
laceration
Tnis
of cervix.
complete
a
represents
rectal
and
are
and
definite
(without
the
(flap
denudation
approximation
modifications
anatomic
Some
rectum.
sutures
lesions,
Freund,
(Robinson-Scholer.)
cally agree
)5 exact
deep
bilateral
Staude,
Emmet,
the
of gutter
between
by the shepherd's
lumen
; 5, outline
aside
high
51."
of
promoters
were
Voss, Simpson,
Whatever
three
and
and
Bischoff, Groodell
Kelly.
of the
originators and advocates
Martin,
pioneer
Jenks,
PEKINEUM;
of
wound
tension),
based
The
wise
other-
surfaces,
on
prerequisites of success.
not so important
as
are
surgical principles.
or
and
anatomic
Methods
attention
to
physiology
of
122
arly
of
labors
of A.
Martin
AND
VAGINA
THE
Schatz
As a pupil
pelvic floor.
and
the contemporaneous
of Emmet's
operations in
the
on
1884, I
in
PERINEUM;
saw
independent development
the
hands
the vaginal sulci, in
of Germany.
gynecologic surgeons
It
operations
Fig.
alike
are
as
in
seen
in
the
cut.
The
Observe
Emmet
ruptured
sutures
that
the
skilled
most
and
operations
not
case
the
for
into
the
relaxed
rectum,
threaded
are
sutures
Tait
from
penetrate
in
the
neither
mucosa.
or
vaginal outlet,
of
flap
operation
in
valuable
A
(Robinson-Scholer.)
in position.
are
"
the
that
sutures
line,
median
skin
53.
the
which
remembered
be
may
of
the
to
a
vaginal
danger
Nothing
with
of
is
loss
the
protect
is about
sulci
of
in
advantage
the
wound.
of
equal
the
Tait
The
value
is almost
certain, hence
valuable
tissue
gained by denuding
an
area
healing
but
little
healing.
vagina over
non-
of
met's
Em-
reason
is that
by
tion
opera-
HOW
retaining
its
that
original
same
size
MEND
TO
123
THEM.
intact, for it will
area
shortly
after
the
contract
which
tension
to
duced
pro-
it is removed.
The
rational
lacerations
resulting from
and
requiring colpoperineorrhaphy
are
numerous
very
In general
varied, but they follow a logical sequence.
the
chain
of
of
irritation
which
symptoms
is
symptoms
an
"
unbalances
Five
sutures
atrium;
reflex
the
viscera
(abdominal
other
Completed
employed.
were
irritation,
thoracic). The
the hypogastric plexus,
up
brain
the
chain
from
the
a
on
focal
ovarian
find
a
has
termed
call it the
each
side
collection
massive
ganglion,
been
on
the
cervico-
pelvic
brain.
of
the
of
nerve-
uterine
An
point
irritation
an
and
incomplete
point, travels
plexus and the
of
We
may
operation
ganglia to
sympathetic
aids
thoracic
and
plexus, which
facts
Anatomic
visceral
rhythm.
lateral
local
A
infection
Fig. 54.- -(Robinson-Scholer.)
laceration.
follows:
as
the
abdominal
in
disturbing
be
must
uterus
large
a
cells
which
ganglion.
enormous
spected.
in-
mass
We
of
124
nerve-cells
of
VAGINA
THE
great ganglionic
and
heart
nerve-cells
and
is in
intimate
at the
of
of
found
are
cervical
middle
nerves
these
and
close
with
connect
nerves
It is
the
important
many
care
genital organs.
each ganglion with
numerous
nerve
role,because
and
messages,
of innumerable
many
many
lines.
the
strands
Now
a
commu-
the
operation,
a
triangle
suturing.
strands, tracts, will
dispose of
ganglion
of
pelvic viscera.
which
play the
few
and
glionic
gan-
strands
ganglion cells
peripheral reports. A
cells will receive
from
Many
the
in
ganglia),
in the
large
of Dr. Emmet's
First
stage
Fig. 55." (Robinson-Scholer.)
of
"via. : Denudation
of the posterior
vaginal wall ; denudation
method
of his peculiar
with
the noted
in each
sulci of the vagina,
nication
root
Three
stomach.
the
Each
plexus.
masses
nerve
is found
"
network
vast, intricate
a
Wrisberg's
"
of
masses
(superior, inferior
neck
the
brain
axis, just behind
celiac
the
abdominal
the
"
PERINEUM;
AND
can
few
many
cells
"
carry
take
glion
gan-
messages
the tho-
HOW
over
the
Hence
the
viscus
those
to
will
three
One
of
the
rhythm.
If
this
be
defective
and
organs.
brains
disturbed
its final
Pig. 56.
(Robinson-Scholer.)
is closed
sulcus
right vaginal
Let
it be
organ
remembered
is
its mode
of
life.
stimulus
of
tract,
air
urine
in
in
the
for
the
the
at
by
The
stage,
sutures
the
the
an
as
organ,
blood
lungs,
a
is
becomes
organ
food
on
fetus
food
in
;
which
the
triangle
in
position.
sutures
from
a
in
eased
dis-
without
organ
of
occasion
urinary tract,
Fallopian tubes, and
the
viscus
a
irritation
all times,
which
of
object.
two
that
emitted
physiologic rhythm
with
of
the
Another
"
the
rhythm
functions
nected
con-
strands
nerve
many
the
over
viscera.
intimately
most
power
certain
a
respective
by
chief
fails in
assume
"
their
the
is
significant
exercise
brains
pelvic
of
rhythm
which
125
THEM.
and
racic, abdomiDal
control
MEND
TO
regard to
accomplishes
is the
rhythm
for
the
in the
material
the
ural
nat-
digestive
endocardium,
uterus,
in
the
fluids
liver,
126
carried
up
VAGINA
THE
portal
the
by
to it
AND
PERINEUM;
If
vein.
follow
we
eased
dis-
a
from
the
emitted
pathologic genitals
message
the
the lateral chain
brain
to the abdominal
over
"
hypogastric
ovarian
and
to
emitted
plexus
the
"
the
Excessive
secretion.
Fig. 57."
sutures
;
deficient
remaining
produce
of
continuation
The
to
transmitted
pathologic
reflex
the
to
such
reorganized
may
observe
secretion
in
two
induce
may
denuded
triangles
diarrhea;
closed
by
in situ.
sutures
may
is
ate
secretion; disproportion-
secretion, constipation;
secretion
genitals
The
we
Excessive
secretion
(Eobinson-Scholer.)
the
it
digestive tract,
following disturbances:
digestive traci; deficient
the
where
and
fermentation
reflex
factors
disproportionate
(bloating); the
institutes
tion.
indiges-
the diseased
irritation, passing from
abdominal
brain, is reorganized and
the
liver
irritation
over
the
produces
hepatic plexus. This
excessive, dispropor-
HOW
tionate
the
The
to
"
its
its
example,
Fig.
shows
58."
the
the
liver
rhythm
(Robinson-Scholer.)
line
of
It has
urea.
unbalances
function
the
liver.
the
pathologic
If
secretion.
disturbed
For
of
127
THEM.
in
and
transmission
irritation
MEND
secretion
bile,glycogen
heart
lungs.
or
secretes
as
deficient
or
TO
the
will
of
soon
the
Operation
rhythm
of
any
become
small
finished.
liver
rhythm,
irritation
its
rhythm
a
The
just
reflex
"
and
turbs
dis-
organ
be
defective.
intestines
The
Y-shaped
is
line
suturing.
by the superior mesenteric
ganglion, which
induces
four
to
six
times
rhythm
a
daily, according
to food
foods, disturbing the
indigestion.
Improper
scending
deinduce
regular rhythm,
soon
indigestion. The
colon, sigmoid and rectum
(the fecal reservoir)
is controlled
by the inferior mesenteric
ganglion,
which
makes
The
a
superior mesendaily rhythm.
governed
128
terio
has
ganglion
AND
VAGINA
THE
four-
a
PERINEUM;
rhythm, while
24-hour
rhythm.
causes
rhythm
six-hour
to
ganglion has a
knows
that
disturbing the
Any one
neurotic
symptoms
constipation, and eventually many
trition.
arise.
indigestion produces malnuLong-continued
at all
to viscera
Pathologic irritation passes
of season,
and
out
and
day and
times, in season
any
attempting to rest or to pass
are
night, while organs
gans
Orthrough a rhythm, always causing disturbances.
rest and
rhythms.
repair between
secure
Malnutrition
is followed
a disproportion
by anemia
continued
and plasm. Long
the blood-vessels
between
The
is followed
anemia
numerous
by neurosis.
glia
ganthe
inferior
mesenteric
"
bathed
are
Innumerable
are
local and
manifest.
Author's
Fig. 59."
toms
2, reflex
atrium;
of evil symp-
train
a
as
needle.
perineorrhaphy
following genital defects:
infection
conditions
neurasthenic
distant
have, then,
We
irritating blood.
and
waste-laden
in
1, local irritation
irritation
to the
an
"
abdominal
and
it is reorganized
sent
out
to the
brain, where
various
malnutrition; 4,
viscera; 3, indigestion and
and
5, neurosis.
anemia;
of laceration
the disturbance
In the incomplete
cases
is attributed
to
is followed
and
standing
not
only
a
exists, but
to that
When
enteroptosis.
physical
a
lacerations
or
of
the
the
consequent
those
of
mental
serious
condition
and
ritis.
met-
pains while
patients complain in a
who
lacerations
defect
of
train
and
ill-defined
These
walking.
similar
manner
from
patient suffers
The
vulva
and
uterine
by
of the
cystocele. This
prolapse, endometritis
rectocele
of
favoring
gaping
control
become
of
symptoms
lesions
afflicted with
are
and
complete,
feces
and
follow
gravely
gas
plete
com-
affect
130
VAGINA
THE
AND
PERINEUM
reflexes
sider the innumerable
which
necessarily
must
infected, frequently congested, occasionally
of the genitoinvasions
acute, inflammatory
from
arise
the
These
reflexes
arise
all
in
degrees and
the
almost
patient
conditions, and
imperceptibly
tion,
through the stages of indigestion, malnutripasses
neurosis.
and
of these
anemia
Again, many
operated on
by inexperienced surgeons,
patients are
Then
conflict
with
imperfect results.
a
consequent
to the
of opinion arises
perineal defect being the
as
whether
the
of the trouble
or
etiology is to be
cause
rectal
organs.
the
located
in
today
is the
liable
chief
to
throw
As
the
the
to
of
the
on
the
on
and
ignorance
demonstrate
It
error.
of
eases.
genital disthe genitals,
is
operator
nervous
liver
the
(and
evils
knavery)
tem.
sys-
the
are
it
is
requires wisdom,
between
to discriminate
experience
train of neurotic
and their consequent
and
knowledge
defect
system
nervous
scapegoats
difficult
whole
and
the
result, the
imperfect
consequent
a
of
one
confounding of nervous
an
imperfect operation
After
with
for
system,
nervous
genitaldiseases
definitelybelong to the
effects,and the diseases which
than the gennervous
system itself or to other causes
itals.
that
this
I must
insist,however,
requires more
time
and
is able
skill than
any
general
surgeon
or
physician
give.
it is
the practical anatomy,
Until
comprehends
one
almost
impossible to interpret the rational symptoms
of the deficiency of the supports of the sexual
organs.
that
the
The
neal
peripopular view of general physicians
illusion which
body is the chief support is one
cult
I find, after considerable
experience in teaching, diffito
to
eradicate.
It is the
indefensible
mechanical
keystone, the cork
which
plugs up
stops the bottle, or the wedge which
can
Amerithe pelvic outlet.
Unfortunately, a prominent
gjrnecologistat one time abetted this false theory.
theory
that
the
perineal body
is the
HOW
One
of
the
perineal lacerations
said
defend
to
diseases
how
for
condition,
this
explain
or
accompanying
Little
endometritis.
is
all observers
to
.
common
very
131
THEM/
MEND
TO
need
be
it is
dent
evi-
endometrium
the
be
may
by trauma, congestion and bacterial invasion,
sive
Excesdeficient
support.
unduly exposed from
insulted
when
be
then
non-infective,
with
This
its
is the
Be
is liable
into
its muscular
to
submucous
microbe
muscularis
that
their
or
Hence
produce metritis.
of
frequent accompaniments
metritis
is
rational
this
final
train
a
brunt
the
repair
view
it may
of
symptoms
generally
the
short
is
most
of the
for
lacerations
and
"
the relaxed
no
between
gain
a
barrier
its
apparatus,
which
so
the
uterine
walls
of
the
uterus
metritis
is
one
of
the
perineal laceration,
and
of
observed
pelvic
the
increase
in
to
tinue
con-
perineal injury.
the
be
apparent
Many
symptoms
by carefully noting the
has
has
uterus
barrier
injuries to
of evils which
a
disease, it is apt
chronic
very
beyond
even
From
a
the
muscular
and
as
like
muscular
its
layer
intestine
acts
no
products
the
gain
soon
has
and
apparatus
microbes
glands
It
directly
pass
submucous
The
But
invasion.
microbic
all organs
above
no
layer which
mucosae.
glandular
has
muscle.
the
protect
muscular
against
It
walls.
of
glands
call
will
we
be
to
uterus
its
It
frequently
The
general
so
But
it
infection, because
to
which
perineum.
the
lows
fol-
soon
importance.
vast
believe
we
remembered,
it
barrier
or
the
may
evils.
it subinvolution.
calls
metritis, because
origin.
of
laceration
practitioner
of
subject
a
of
train
(subinvolution)
metritis
accompanies
it
to
me
infection
pathogenic
consequent
leads
which
arises; leucorrhea,
secretion
glandular
the
can
only
many
cases
with
that
the
floor
are
time, and
nervous
tem.
sys-
accounted
be
of
invisible
pelvic floors, perineal supports
which
sphincter vagina apparatus
from
by the vessels being torn
"
disturbes
their
culation
cirproper
132
THE
fascial
VAGINA
beds, the
straight, and
veins
We
thus
and
have
disturbed
and
exists
teroptosis
been
overstretched
resumed
not
such
cleft is flattened
broad
and
drawn
up
back
much
The
more
stead
the
ani
muscle
more
floor have
labors
and
On
the
arch,
normal
furrow
anal
becomes
instead
anus,
have
examining
out, the
and
are
of
being
flat,exposed,
skin
the
The
neum
pericoccyx.
larger than normal, being overstretched.
appears
finger introduced
rigid levator ani
into
the
vagina no
the
muscle
loop, but in its
relaxed, overstretched, flabby tissues
lying
the gap
made
tor
by the separation of the leva-
feels
between
dent
pubic
toward
be
may
the
infection
pelvic
integrity.
points
and
the
of
more
En-
nerves.
of the
or
normal
shallow
fallen
one
out,
under
traumatized
avenues
Schatz
as
traumatized.
or
supports
by
their
patients,
and
of
the
The
widely exposed.
the
vascularization; congestions
blood
and lymph
also
have
from
innervation
and
spiral form,
stretch
decongestions
disturbed
elongated, dilated,
normal
the
on
PERINEUM;
becoming
losing their
being put
nerves
AND
fascia 'superior and
in
various
overlooked
practitioner
1883
Emmet
views
in
than
and
regard
inferior
with
its contained
degrees. Perhaps there
in the
pelvic floor by
is
the
the relaxed, overstretched
Schatz
to
lesion
no
general
outlet.
first"clearly announced
relaxed
pelvic
outlet.
In
their
The
very
is deficient, while
the
shallow, short
deep perineum
is the
relaxed
The
one
patient with
vigorous one.
pelvic outlet generally begins to complain of bearingdown
three
two
or
on
symptoms
rising from bed some
weeks
after
labor.
She
to work
or
weak, unable
and
the back, general lassitude
feels
herself, pain in
prostration.
The
relaxed
pelvic floor is most
impressive to the
before
after the anesand
operator, by examination
thetic,
when
he is about
Before
the anesto operate.
thetic
exert
the
pelvic
outlet
is
held
in
partial
tension
by
the
the
loops
of
levator
the
of
and
muscle
ani
133
THEM.
muscular
the
of
remnants
MEND
TO
HOW
fascial
being
supports;
irritated
by
being torn, the patient is
force
of the
by the attempts
constantly losing nerve
in keeping
When
the
reflex irritation
up the tension.
the
parts of the pelvic
patient is fully anesthetized
the
non-balance
floor
show
to
vast
relaxation
hand
the
parts
and
and
of
eye
exists, beyond
defect
it becomes
the
operator
his
at
once
parent
ap-
that
expectation,
a
in
nificant
sigthe
falls back, the anus
perineum
flattens
and
everts, the vaginal walls roll outward, and
furrow
the deep anal
plane approximating
a
assumes
Vast
of the buttocks.
that
changes in subcutaneous
have
and
submucous
occurred, capable of
supports
restores
operation which
being repaired only by an
to
vessels to a stable
bed, nerves
protected sheath,
a
will
insure
normal
to
and
position which
a
organs
and
innervation
in short, proper
circulation
ishment.
noursuch
With
patients in the erect posture the
is continually displacing the
intra-abdominal
pressure
and
into
ened
viscera
by forcing them
through the weakThe
the
pelvic outlet, beyond
pelvic outlet.
floor is full of prolapsing organs
which
often
normal
the practitioner by closing up
the gap.
deceive
the
to relapse between
The
length of time allowed
should
not
injury and the operation on the perineum
sexual
apparatus.
The
"
be
less
than
three
The
months.
shortly after labor.
parts
do
not
heal
Old
gynecologists, as Byf ord,
the
to elapse before
recommended
at least six months
be performed.
Perhaps four months
operation should
be
The
after injury it would
fairly safe to operate.
old cicatrix
not
always readily be found, but by
can
the puckdirections
ering
pulling on the vagina in various
well
tissue
about
the
also
palpating finger may
cicatrix
The
produces
of
the
torn
will
scar
fibers
find
new
of
be
discovered.
The
it.
points
the
for
levator
the
ani
ment
attachmuscles
134
THE
which
their
should
extend
of
the
ends
the
sutures.
The
In
of
regard
the
vagina
A
backward
normal
fixum
In
by
curve
the
restoring
of
of
surface
vulvar
this
from
to
suggestions
the
book
should
have
derived
W.
the
be
cia
fas-
punotum
restored.
and
and
have
regard
to
gestions
sugtempted
at-
labors.
acquired
were
persist,
and
aids
authors
the
that
between
hand
one
relations,
the
of
the
body,
accessible
credit
duly
established
be
on
so
should
vagina
perineal
I
essay
all
the
body
The
restored,
be
should
other.
writing
from
way
mid-
be
posterior
:
reproduced
curve
center
of
Some
The
body
should
relations
the
on
should
in
periods.
be
body
perineal
new
perineal
the
included
septum.
natural
i.e.,
that
so
be
may
mation
for-
flap
cicatrices
operation
perineal
must
rectovaginal
for
contract
The
the
menstrual
the
to
bundles
bundles
time
the
between
beyond
ered
puck-
irregular,
attachments.
muscular
the
peculiar,
muscular
of
points
new
PERINEUM;
a
the
when
appearance
from
outlet
the
give
may
AND
VAGINA
J.
Stewart
in
McKay.
ings
draw-



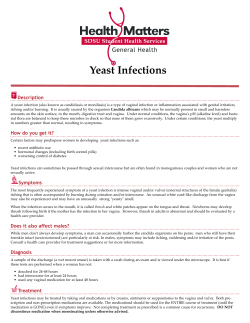






© Copyright 2026