
Change package for Quality Improvement in Orphans and Vulnerable Children Programmes in Kenya
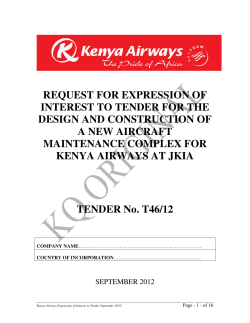
Change package for Quality Improvement in Orphans and Vulnerable Children Programmes in Kenya SEPTEMBER 2013 This change package was prepared by University Research Co., LLC (URC) for review by the United States Agency for International Development (USAID) and was authored by Roselyn Were, Stanley Masamo, and Jemimah Owande of USAID ASSIST and Emma Akinyi, Muhamed Akulima, Emily Murungi, Millicent Oluoko, and Stella Wachira of APHIA Plus. The work described was conducted under the USAID Health Care Improvement (HCI) and USAID Applying Science to Strengthen and Improve Systems (ASSIST) projects, which are made possible by the generous support of the American people through USAID, with funding from the U.S. President’s Emergency Plan for AIDS Relief (PEPFAR). Cover photo: Children under the Maua Methodist Hospital - Meru, Kenya Photo credit: Allan Gichigi and Elijah Kanyi (Afroshok media) Change package for Quality Improvement in Orphans and Vulnerable Children Programmes in Kenya By: Roselyn Were (USAID ASSIST), Stanley Masamo (USAID ASSIST), Jemimah Owande (USAID ASSIST), Emma Akinyi (APHIA Plus Nuru ya Bonde), Muhamed Akulima (APHIA Plus Kamili), Emily Murungi (APHIA Plus Nairobi Coast), Millicent Oluoko (APHIA Plus Western Kenya), Stella Wachira (APHIA Plus Nairobi Coast) September 2013 DISCLAIMER The contents of this change package are the sole responsibility of University Research Co., LLC (URC) and do not necessarily reflect the views of the United States Agency for International Development or the United States Government. © September 2013 University Research Company., LLC (URC) / USAID ASSIST (Kenya) Design and layout by Esther Kahinga Acknowledgement We would like to acknowledge all the people who contributed to the development of this change package especially the Quality Improvement Teams and coaches who worked tirelessly to ensure improvement in service delivery for orphaned and vulnerable children (OVC) across the country. This work would not have been complete without the support of the Department of Children Services, APHIA and AMPATH PLUS and the Community Based Organizations whose work is disseminated through this document. The development and production of the OVC Change Package was supported by the USAID Applying Science to Strengthen and Improve Systems (ASSIST) Project. The work of the USAID (ASSIST) Project is supported by the American people through the United States Agency for International Development (USAID) and its Bureau for Global Health, Office of Health Systems. The project is managed by University Research Co., LLC (URC) under the terms of Cooperative Agreement Number AID-OAA-A-12-00101. The ASSIST Project team includes URC, Broad Branch Associates; EnCompass LLC; FHI 360; Harvard University School of Public Health; Health Research, Inc.; Institute for Healthcare Improvement; Initiatives Inc.; Johns Hopkins University Center for Communication Programs; Women Influencing Health Education and Rule of Law, LLC. For more information on the work of the USAID ASSIST Project, please visit www.usaidassist.org. i ii Table of Content Background for Quality Improvement of Orphaned and Vulnerable Children Programs .........1 Quality Improvement Process ................................................................................................3 Change Ideas .......................................................................................................................15 Annexes ...............................................................................................................................27 List of teams testing change in each service area ..........................................................28 List of participants .......................................................................................................31 iii List of acronyms AACs ASSIST AMPATH APHIA CBO CHW CHV CSI CU DCS GOK HCI HIV / AIDS KCPE KCSE LIP NSC OVC PDSA PSS QI QIT URC VSL USAID Area Advisory Councils Applying Science to Strengthen and Improve Systems Academic Model Provinding Access to Healthcare AIDS Population and Health Integrated Assistance Community Based Organization Community Health Worker Community Health Volunteer Child Status Index Community Unit Department of Children Services Government of Kenya Healthcare Improvement Project Human Immunodeficeincy Virus / Aquired Immune Deficinecy Syndrome. Kenya Certificate of Primary Education Kenya Certificate of Secondary Education Local Implementing Partner National Steering Committee Orphans and Vulnerable Children Plan Do Study Act Psychosocial Support Quality Improvement Quality Improvement Teams University Research Company Voluntary Saving and Loaning United States Agency for International Development iv Foreword The term “orphans and vulnerable children” (OVC) includes not only children orphaned by their parents’ death, but also children considered vulnerable to psychological traumas endangering their health and well-being, including living with a chronically ill parent. In 2003, the launch of the U.S. President’s Emergency Plan for AIDS Relief (PEPFAR) called for interventions that met the needs of OVC affected by HIV and AIDS. The response to the PEPFAR call was the development of emergency humanitarian efforts to address the plight of the large numbers of OVCs resulting from the HIV and AIDS epidemic. This means programs did not address integration or sustainability due to the emergency nature of the response. In recent years however the emergency response has not been appropriate and PEPFAR through the United States Agency for International Development (USAID) has emphasized on programs that address quality improvement as an integrated aspect of OVC programming. Moreover, lessons learned from OVC programs have revealed the need to improve service quality and to strengthen harmonization across partners. But how do we define quality? While there are many definitions of quality, one that is often used is the definition from the United States Institute of Medicine (IoM), that says quality is the “ degree to which health services for individuals and populations increase the likelihood of desired health outcomes and are consistent with current professional knowledge or evidence” . Quality has six dimensions, • safety • effectiveness • patient centeredness • timeliness • efficiency With regard to quality improvement, this has been described as the systematic approach that uses specific v techniques to improve quality and the most important ingredient in successful and sustained improvement being that way in which the change is introduced and implemented . The University Research Company (URC), LLC notes that quality improvement (QI) uses quantitative and qualitative methods to improve the effectiveness, efficiency, and safety of service delivery processes and systems, as well as the performance of human resources in delivering products and services. Using this definition and various quality improvement approaches and models such as the ‘Plan-Do-Study-Act’ (PDSA) model, a key focus for URC is addressing quality programming for OVC . This change packages draws on experiences from Kenya following a 2 year program that implemented change ideas in collaboration with 6 USAID implementing partners across the country. This change package was developed following a harvest meeting where quality improvement teams shared the results of what they had successfully implemented over a period of two years since the first improvement team was formed, though majority of the teams were formed much later. The package begins with some background information on the journey towards quality improvement for orphans and vulnerable children programming followed by a guide for changes that have proven to work. Case studies of some of the teams that implemented the change ideas presented here are shared in a seperate booklet Improving the lives of vulnerable children in Kenya: Experiences from implementing quality service standards We invite you to study and utilize this package for all OVC programming. Dr. Faith Mwangi-Powell COP- URC Kenya. vi 1 BACKGROUND FOR QUALITY IMPROVEMENT OF OVC PROGRAMS The plight of Orphans and Vulnerable Children (OVC) is an issue of national concern in Kenya. It is estimated that there are over 2.6 million orphans in the country, 47% of whom are orphaned as a result of Human Immunodeficiency Virus and Acquired Immune Deficiency Syndrome (HIV and AIDS). policy on OVC to underpin intervention. In its commitment to improve the lives of OVCs in Kenya, the Government introduced the National Policy on Orphans and Vulnerable Children, which intendeds to ensure that every Kenyan child who is orphaned or vulnerable is protected and supported in order to achieve their full potential. In response to an increasing number of OVC in Kenya, a National Steering Committee (NSC) on OVC was constituted in May 2004, to deliberate upon interventions tha would address the plight of OVC. A rapid assessment on the state of OVC was carried out in June 2004, with the support of various development partners. The assessment informed on the regrettable vulnerability of children that demanded immediate action. Consequently the NSC realized the need to come up with a national Efforts to provide care and support to OVC have expanded rapidly both in terms of partners delivering services and resources allocated to meet the needs of these children. This has resulted in an increase in the number of children reached without equivalent focus on the quality and impact of services delivered. A situational analysis conducted in 2009 to assess the quality of services provided to OVC identified 1 various gaps including; 1. Quality of services offered by some organizations has been inappropriate leading to stigmatization and discrimination of OVC by the rest of the community and wastage of resources 2. Existing interventions only support small proportion of OVC 3. Inadequate and inaccurate data on the needs of the children before intervention is launched 4. Lack of regulation on the duration a service provider should support a beneficiary 5. Lack of social mapping of OVC service providers making it difficult for the Department of Children Services (DCS) to monitor and coordinate their operations. To support and streamline the standards and quality of OVC care, the Department of Children Services and stakeholders initiated the process of developing service standards for quality improvement of service delivery. The minimum service standards have eight service areas with specified desired outcomes that guide improvement work as shown in table 1. 2 Table 1: The eight service areas Service area Desired outcome Food & Nutrition OVC and other household members should have enough nutritiousfood to eat throughout the year and should not be anxious of where they will find food for the next meal. Education All orphans and vulnerable children have the right to education in a well-structured school with a proper teaching and learning system. Health OVC and their households must have access to good health care services so as to promote and maintain a healthy lifestyle.It is important to ensure children aged 0-5 years go to the clinic, get immunization and are treated when sick. Psychosocial support This is the emotional, social, spiritual, mental and physical support given to OVC and their households to promote all-round growth and development. Shelter & Care OVC and their households must live in a structure that is safe, secure, habitable and with enough space for comfortable living with at least one responsible adult caregiver. Child preotection Orphans and vulnerable children should be free from any and all forms of abuse, neglect, discrimination and exploitation. Household Economic Strengthening Households should be able to regularly and safely meet the basic needs of the OVC on their own. Coordination of care There should be a structured and well monitored system bringing together service providers who provide quality and essential services to OVC and their households. 3 2 QUALITY IMPROVEMENT PROCESS 2.1 Dissemination of Standards to key players in OVC programmes from across the country. The launch programme ensured participants were guided through the key The dissemination of the standards over the year was an elaborate process that began even before the finalization and eventual launch of the Minimum Service Standards for Quality Improvement of Orphans and Vulnerable Children Programmes, Kenya (hereafter reffrered to as the Standards). Through partnership with the AIDS Population and Health Integrated Assistance (APHIA) implementers across the country, over 100 Quality Improvement Teams (QITs) were taken through the standards and have been using them to guide their work. During the national launch, copies of the Standards in soft and hard copy were distributed Officials from the Ministry, UNICEF, HCI and Child Geusts during the Minimum Standards launch 4 components of the standards and discussions were held on the application of these standards at the point of service delivery. 2.2 Capacity building of Department of Children Services on OVC QI From March - July 2012, HCI conducted trainings for 283 government personnel from the Department of Children Services and Nairobi City Council. The outcome of the trainings was the development of region-specific work plans that are being implemented jointly with HCI, the Department of Children Services and APHIA Plus the national USAID mechanism for service delivery for HIV/ AIDS. The following activities have been ongoing since the training; After the national launch, HCI together with the OVC Technical Working Group conducted dissemination workshops in 8 regions of Kenya. In total over 800 OVC service providers attended the meetings. District and county level dissemination work plans were developed for implementation under the coordination of the Ministry of Gender Children and Social Development through the Department of Children Services. • Besides the USAID funded Academic Model Providing Access to Healthcare (AMPATH) and APHIA plus implementers other service delivery teams that are linked to the government’s Area Advisory Councils (AAC) at grassroots level have also been supporting the dissemination exercise. A total of nine thousand copies of the standards were printed for distribution. • • • • 5 Disseminating service standards to implementers at county, district, division and location levels Stakeholder mapping and development of directories of OVC service providers Harmonizing reporting and data management from the location level up to the province Building the capacity of point of service delivery providers in the standards and Quality Improvement Conducting county and district level learning sessions, documentation, reporting and consolidation of results Province 5. APHIA Plus Nairobi /Coast – Nairobi and Coast Province 6. APHIA Plus North Arid Lands (closed in 2012 and relaunched as Imarisha)- North Eastern region , Upper Eastern, Samburu and Turkana. The Department then conducted periodic stakeholder meetings and supportive supervision for the implementers. The government’s capacity to provide leadership for Quality Improvement (QI) has been enhanced through training. APHIA addresses various population and health issues including OVC. Under the OVC component, APHIA works with Local Implementing Patners (LIPs) usually Community Based Organizations (CBOs)and local Non-Governmental Organizations (NGOs) at grassroot / community level. The NGOs / CBOs then form QITs that work with the community to identify and assist OVC within that community. AMPATH directly implements their OVC component. 2.3 Institutionalizing QI at the Point of Service Delivery HCI which was later replaced by the Applying Science to Strenthen and Improve Systems (ASSIST) in October 2012, continued to support the APHIA/AMPATH plus implementers in QI through coaching and mentorship and learning sessions at both national and project levels. HCI works with 6 projects one of which faced a close out in 2012. They include: 1. 2. 3. 4. For QI to be implemented at the point of service delivery, representatives from CBOs that work with the above projects were trained as QI coaches. They then shared on the standards to their respective communities and later formed QITs. APHIA Plus Kamili - Central and Eastern provinces APHIA Plus Nuru Ya Bonde - Rift Valley province AMPATH plus - Uasin Gishu and Western Kenya APHIA Plus Western Kenya – Western and Nyanza 6 The QIT brings together about 15 members of the community who possess valuable skills in addressing the common challenges children face. The team generally consists of teachers, community health workers or volunteers, nurses, agricultural extension officers, district / volunteer children officers, a representative of the provincial administration like chief, spiritual leaders like pastors or imams, representatives of the area advisory council, guardians and OVC. A total of 150 QITs have been formed across the country. systems and child levels. The changes at systems level will inform an improvement in the service delivery process as designed by the organization whereas the changes at child level will focus on addressing the felt needs of each individual child and their households. 2.4 Learning Sessions National Learning Sessions were organised to provide an opportunity for QITs from across the country to share to learn from one another, and for HCI consolidate the results of the work done To assess improvement on child outcomes, the by QITs. Project specific learning sessions also Child Status Index tool is administered on children took place at the APHIA level. Representatives as baseline data collection with a repeat CSI of QI teams were brought together to share the administration six months later. This linked with the successes and failures they had encountered service tracking data that is collected monthly helps in testing change ideas using the QI model for determine whether the changes instituted by the QI improvement (see figure 1). teams made a difference in the lives of the children. In problem identification , the QI team compares 2.6 Process of harvesting key changes the overall CSI data with the results of the self For over 2 years more than 100 QITs across the assessment based on the standards. This helped the country with support from AMPATH and APHIA teams agree on change ideas that have the highest plus have innovated and tested many change ideas probability of leading to improvement at both geared towards improving the quality of service 7 same challenges. For a change to have worked, the teams had to share evidence (data) and experiences (qualitative data) with the others and demonstrate whether these change ideas lead to improvement or not. Langley et al – The Improvement Guide, JB, 2009 A harvest meeting was held on 20 - 21 May 2013 with representatives (Champions) of the QITs, APHIA plus, AMPATH and HCI. The harvest involved the classification of change ideas into service areas and then ranking them. The ranking was based on four parameters: • evidence - how many teams tested it • simplicity • scalability • relative importance - its contribution to the results achieved. The teams members described in detail how each change idea was tested or implemented and the results of the implementation. Teams that tested the various changes are indicated in bold in the column ‘Notes on evidence.’ USAID HEALTH CARE IMPROVEMENT PROJECT Figure 1: The Quality Improvement Model, adapted from Langely, P. et. al. (2009) The Quality Improvement Guide delivery to OVC in Kenya. With support from HCI the QITs documented and shared these change ideas during project and national learning sessions. The sessions gave the teams an opportunity to share the change ideas that had had a clear demonstration to work in improving the well being of the OVC with QITs that were struggling with the 8 3. CHANGE IDEAS 9 3.1 Service Area: Food and Nutrition 1 Change Idea Steps to implement Notes on evidence Improving food production through provision of certified seeds • Through support from the Ministry of Agriculture carry out assessment to identify the seeds required for each area, then conduct a community awareness meeting targeting caregivers with information on the new seeds. Ensure timely distribution of the seeds for increased yield. In collaboration with the Ministry of Agriculture carry out continuous follow up to ensure the caregivers are tending to the crops appropriately. • • With support from Ministry of health, carry out targeted awareness creation to caregivers on proper nutrition especially for children under the age of five. Continuous growth monitoring by community health workers (CHWs) to assess nutrition status of children. • Through collaboration with partners identify the source of water appropriate for the region. Seek resources from the community and partners and dig wells or dams to ensure continuous supply of water Formation of water management committee to ensure water is used appropriately e.g. household use and irrigation. Have systems to ensure the levies collected from sale of water are properly managed. • • • 2 Nutrition education to caregivers • • 3 Ensure access to consistent supply of water • • • • 10 • • Tested in 26 sites with moderate results Good idea however the biggest challenge is getting GOK staff to assist communities when no financial support is available. Identification of the correct seed and time for planting also requires agricultural professionals to support the caregivers. Adoption of irrigation technologies in case of insufficient rain fall increases yields. Matunda Jua Kazi, ACK Embu Tested in 12 sites with high results showing it can easily be adopted and scaled up in other sites. • The trainers need to adopt local language and use of pictorials for effective delivery, and understanding. Shangia CU, Bukonoi Tested in 2 sites with high results. However for scale up there is need to adapt to specific environment. e.g. areas with a low water table need to adopt other methods. • The water management committees need to have basic management and financial skills for proper resource management. Shangia 3.2 Service Area: Education 1 Change Idea Steps to implement Notes on evidence Enhance parents/ caregivers involvement in the education of their children • • • • • • 2 Ensure timely payment of school levies and other educational materials including sanitary pads for girls • • • • Awareness creation through school management committee, chief meetings (barazas), CHW household visits and other forums on the importance of education. Initiate monthly meetings between the class teachers and caregivers where vital information regarding the child’s performance, challenges and strengths are shared and discussed Through the caregivers monthly meetings ensure importance of education is part of education sets received by the caregivers Continuous monitoring by the caregivers and the CHWs through the school register to ensure all children attend school as required. CHWs tracking parental involvement through the class teacher register. Identify children whose caregivers cannot afford payment of school levies. Link to other partners including cooperates and government systems that support education. Link caregivers to alternative economic activities to improve household income In cases of delays in school fees payment discuss with the head teachers/principles early enough to ensure the children are not sent away from school 11 • • Tested in 17 sites with very high results Very viable and can be adopted in any environment. There is need for flexibility to accommodate the busy schedule of the caregivers. Shangia CU, Dago Dala Hera, YARD • Tested in 17 sites with moderate results. Very challenging because of the procedures within various organizations which the QIT may have no control over. However, with planning and submitting requests at the beginning of the school term most organizations are able to make payments in time APHIA Plus Western Kenya , Nuru ya bonde 3 Change Idea Steps to implement Encourage students to initiate individual and joint study plans to improve their performance • • • • • Notes on evidence Create awareness targeting school going children on • Tested in 2 sites and showed high why it is important to have their parents involved in results. Can be adopted in any their education and performance environment Through the CHWs and the teachers ensure each child • Academic clinics were adopted by has developed a personal plan for improvement. Cheer up from other CBOs. Institute student-led tuition and coaching i.e. have those in higher classes coach those in lower classes Cheer up, Dago Dala Hera Through the children clubs ensure education and performance are an integral part of their discussions Establish mentorship program in schools (academic clinics) 12 3.3 Service Area: Health 1 Change idea Steps to implement Notes on evidence Promote hand washing • Carry out advocacy and outreach campaigns in schools and households. With support from partners distribute leaky tins to schools with permanent sources of water. Encourage peer monitoring in schools where children monitor each other to ensure they wash their hands appropriately. Initiate health clubs in schools with a patron to ensure continuity De-worming primary school children and administering Vitamin A. • Carry out advocacy and outreach campaigns in schools and households on importance of ensuring water safety Encourage caregivers to treat water before use within the household • • • • • 2 Advocate for safe drinking • water • • Tested in 6 sites with high results. Can be scaled up but needs adaptation for specific sites i.e. areas with scarce water supply. The children are trained to make leaky tins using local resource like tins, buckets, jerry cans e.t.c. LOCODEI, NOFI, Shangia, Kinani CU • Tested in 6 sites with moderate results, requires more advocacy and awareness creation. Challenges faced in areas with perennial water shortage Shangia CU, NOFI, LOCODEI 13 3.4 Service Area: Shelter and Care 1 Change idea Steps to implement Renovation of dilapidated houses • • • Notes on evidence Identification of most dilapidated houses. • Mobilized resource from local business men and women Worked with the caregiver to provide labor. • • Tested in 12 sites with moderate results. However, the renovation cost is expensive and may not be sustainable in the long run. A CBO in Eastern mentioned it is cheap because of local labour. WOFAK in Nuru Ya Bonde also used very minimal resources. Linking caregivers to household economic activities ensures they repair their houses with minimal external support e.g Hakishep in Kibera and Hope Worldwide Kenya in Eastern Hakishep, WOFAK, Hope Worldwide Kenya 14 3.5 Service Area: Child Protection 1 Change idea Steps to implement Notes on evidence Enhance awareness to the community and children on importance of child protection • Awareness creation targeting the community through churches, chief meeting (barazas) and school meetings on importance of child protection and referral processes Training CHWs on child rights and protection Training children on child rights Ensuring child protection during home visits by CHW Formation of child rights clubs in school and ensuring they learn to be each other’s keepers Involve the community animators such as paralegals, parent educators and CHVs in child protection through counseling, reporting and sharing information with the community members. Organize feedback sessions with the children in schools and churches to get information on what affects them through songs, exercises, skits, drama, talks and poems. • Map areas where children are likely to get exploited e.g. local brew dens, video shows and areas where truck drivers park Sensitize local brew sellers and identify hotspots where children are not allowed to access Monitor areas truck drivers park and ensure no children go there by involving the police children’s desk and children’s office. Link with partners to provide OVC with basic needs to avoid them engaging in sexual exploitation. • • • • • • • 2 Identify areas with high prevalence of child abuse • • • • 15 Tested in 20 sites with good results. Can be easy adopted and scaled up. AMPATH Port Victoria, AMPATH Kapsoya, Kagwa, Dabaso, Bukonoi Tested in 12 sites with high results. Requires collaboration of the provincial administration and the AAC AMPATH Budalangi,AMPATH Kapsoya, Dabaso 3 Change idea Steps to implement Notes on evidence Identify and withdraw OVC from child labour • • • • Map out and identify the details of children involved in child labor i.e. their names, where they came from, local elders and caregivers during household visits. In partnership with provincial administration and the police child desk carry out a mop up of children involved in child labor. Hold awareness meetings with members of the community especially business community on the implication of child labor • Tested in 6 sites with high results. There is however need for massive awareness creation and education to the caregivers if this is to be sustained. Households linked to house hold economic strengthening have minimal cases of child labour Shangia, AMPATH Budalangi, 4 Establishment of children help desks within the police station • • • Incorporating a representative of the police in the QIT Discussions with the police officer in charge to set aside a desk where children can report abuse cases Collaboration with other partners including provincial administration and AAC to speed up investigation and processing of the cases 16 • Tested in 5 sites with high results. AMPATH Kapsoya, AMPATH Port Victoria, REEP 5 Change idea Steps to implement Notes on evidence Ensure legal registration of OVC and caregivers • • • • • • • 6 Establishing legal clinics • • • • Awareness creation during meetings with area chief on importance of legal registration. Share with the provincial administration and the registrar Mobilization of caregivers who don’t have national identity cards or birth and death certificates. Awareness creation involving the registrar office and provincial administration on importance of these documents is important. There is need to ensure the police clearly understand child rights and their role in ensuring children enjoy their rights if the desk is to be effective. There is also need for close monitoring by various partners to ensure no violation of child rights. There is need to empower children to be able to report in case they don’t receive the required service at the desk • Tested in 20 sites. With very good results. Can be easily adopted and scaled up Kagwa, Dago Dala Hera, Dabasu, Hakishep Mapping local community members with expertise in legal • matters Inviting them for a presentation on legal issues affecting OVC and their households and the impact on the entire community Identifying those willing to volunteer their time to support. • In collaboration with the legal volunteers, DCO and the area chief convene legal clinics quarterly. One CBO implemented this change idea and had remarkable progress in child protection cases. Its adoption and scale up was a challenge because most legal practitioners are based in major cities and very few are willing to volunteer their time and resources to participate in legal clinics. Cheer up 17 3.6 Service Area: Household Economic Empowerment 1 Change idea Steps to implement Notes on evidence Promote access to financial services to the caregivers through Village Saving and Loaning (VSL) activities. • Awareness creation through trained CHWs on the importance of VSL and how it operates to the caregivers. This will demystify the myths around loans. Carry out training on VSL to the caregivers. Mobilize members to join and register. Encourage saving and loaning by the caregivers • Awareness creation on diversified sources of household income e.g. farming, energy saving jikos, solar driers etc Allow the caregivers to identify and select which source is most appropriate for them Link with relevant institutions and organizations for capacity building and monitoring Through caregiver support group track progress of each caregivers Through CHW monthly meetings track progress and identify challenges. Close monitoring by the caregiver or OVC support group is important for growth and development. • • • • 2 Diversification of household income • • • • • • 18 Tested in 10 sites with good results, However at the start up stage awareness creation is important to clear the myths and beliefs around loans among the caregivers KENWA, Msambweni CORPS, Shangia, Hakishep, AMPATH Budalangi Tested in 10 sites with fair results. Important lesson is to allow the OVC or caregiver to identify which income generating activity they want to pursue. Kagwa, Dago Dala Hela, KENWA, Shangia, Msambweni CORPS 3.7 Psychosocial Support 1 2 Change idea Steps to implement Notes on evidence Strengthening community and household capacity for provision of psychosocial support to OVC and caregivers • • • Conducting sensitization activities to create awareness on psychosocial support needs to caregivers and their households. • • Training caregivers of psychosocial support with support from trained counselors There is need for clear guidance to the CHWs on what is defined as psychosocial support and how to measure results. Use practical and interesting methodologies e.g. drama and songs to pass the message 19 Tested in 4 sites. Difficult to measure results. MOCASO, Redeemed Gospel Church 3.8 Service Area: Coordination of Care 1 Change idea Steps to implement Notes on evidence Harmonize OVC service delivery • • • • • • • • Map out organizations providing OVC care and support in the region through the department of social services Hold meetings with representatives of the organization and map out their activities detailing activities, number of children, region covered and duration of project. Develop a database with the relevant details. In cases of duplication of work, hold meeting with the partners through the department of social services and department of children services for redistribution or adoption of different service areas. Quarterly meeting through the department of children service to review progress of each organization. Develop a database of OVC to reduce cases of double support. 20 Tested in 3 sites with improved results. However, this is the core business of the department of children services and they should take the lead or drive the process to ensure every actor adheres to the set standards. Njukini CU 4. ANNEXES 21 AMAPATH AMPATH Port Victoria x AMPATH Kapsoya x APHIA Hope Worldwide Kenya - Makueni x Plus Kamili Twana Twitu x Save the Children Meru x Ruiru Baptist Church x Ngoliba x Makindu Children Centre x Shephards of Life x x x x x x x x x x Society of Women Aganist AIDS in x Kenya (SWAK) x x Cheers Up x St. Joseph HIV Self Help Group x x x Food for the Hungry x x Terry Child Support x x 22 x Coordination of care Shelter Child Protection Psychosocial Support Health Economic empowermennt Education Community based org/ QI team Nutrtion Partner Food security ANNEX 1: LIST OF TEAMS TESTING CHANGE IN EACH SERVICE AREA Little Servants of the Sacred Heart Coordination of care x YARD APHIA Plus Nairobi Coast Shelter Child Protection Psychosocial Support Health Economic empowermennt Education Nutrtion Community based org/ QI team Food security Partner x Cheda x Catholic Diocese of Kitui x Anglican Church of Embu x CARITAS Nyeri x HAKISHEP x KICOSHEP x MOCASO x Shangia Community Unit (CU) x x x x x x x x x x x x x x Mkunumbi CU x Children Hope Foundation x x x Redeemed Gospel Church x KENWA Korogocho x x x x Progressive Care Coalition x MOHAB x Msambweni CORPS x 23 x x x LOCODEI Coordination of care Shelter Child Protection Psychosocial Support x Njiru Organic Farming Integrated x x St. Francis APHIA Plus Nuru ya Bonde Health Economic empowermennt Education Nutrtion Community based org/ QI team Food security Partner x x Njukini CU x Dabasu CU x Evangelising Sisters of Mary x Catholic Diocese of Eldoret x Mother Francesca x LIFA x Catholic Diocese of Ngong x Kenya National Organization of Peer Education and Training (KNOTE) x x x x x x x x Beacon of Hope x Narok District Network Forum x Deliverance Church Nakuru x WOFAK x x 24 Kagwa x x x x Bukonoi x x x x x Osiep Kiye x 25 x x Coordination of care Shelter x x REEP Matunda Jua Kazi Child Protection Psychosocial Support Health Economic empowermennt Dago Dala Hera Community Unit Education APHIA Plus Western Nutrtion Community based org/ QI team Food security Partner ANNEX 2: LIST OF PARTICIPANTS NAME 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. 17. 18. James Kamau Herbert Kahindi Mesaidi Mwarandu Lydia Simiyu Douglas Kariuki Javanson Njue Christine Kalume Millicent Akinyi Irene Masudi Susan Odero Joseph Makokha Jackson Muge Subira Kingi Abdalla Mwatari Omar Suya Metrine Mudibo Emily Murungi Peter Odongo LOCAL IMPLEMENTING PARTNER PROJECT Hope Valley Shangia Community Unit Shangia Community Unit Shangia Community Unit Cheer up ACK Embu Kinani Hakishep Dago Dala Hera Dago Dala Hera Bukonoi Sama Bungoma Bukonoi Sama Bungoma Dabaso CU Msambweni Corps Locodei Redeemed Gospel Church Aphia plus Coast AMPATH Plus APHIA Plus Kamili APHIA Plus Nairobi Coast APHIA Plus Nairobi Coast APHIA Plus Nairobi Coast APHIA Plus Kamili APHIA Plus Kamili APHIA Plus Nairobi Coast APHIA Plus Nairobi Coast APHIA Plus Western Kenya APHIA Plus Western Kenya APHIA Plus Western Kenya APHIA Plus Western Kenya APHIA Plus Nairobi Coast APHIA Plus Nairobi Coast APHIA Plus Nairobi Coast APHIA Plus Nairobi Coast APHIA Plus Nairobi Coast AMPATH Plus 26 NAME LOCAL IMPLEMENTING PARTNER PROJECT AMPATH Plus APHIA Plus Nuru ya Bonde APHIA Plus Kamili APHIA Plus Nairobi Coast APHIA Plus Western Kenya APHIA Plus Kamili 19. 20. 21. 22. 23. Lilian Astiavula Emma Akinyi Muhamed Akulima Stella Wachira Millicent Oluoko AMPATH Plus Aphia plus Rift Valley Aphia plus Kamili Aphia plus Nairobi/Coast Aphia plus Nyanza/Western 24. 25. 26. 27. 28. 29. 30. 31. 32. 33. 34. Lukas Ndung’u Joash Apollo Scevar Swaro Felix Miti Patrick Kinyae Charles Mukabi Lydiah Atieno Stanley Masamo Roselyn Were Jemimah Owande Irene Mutea YARD REEP REEP NOFI Njukini Community Unit MOCASO MOCASO HCI HCI HCI HCI 27 APHIA Plus Western Kenya APHIA Plus Western Kenya APHIA Plus Nairobi Coast APHIA Plus Nairobi Coast APHIA Plus Nairobi Coast APHIA Plus Nairobi Coast USAID HCI USAID HCI USAID HCI USAID HCI 28







© Copyright 2026