
Provider Manual
Provider Manual For SeaView IPA Valley Care IPA Valley Care Select IPA Santa Barbara Select IPA Leisure World Managed Care Medical Group Pioneer Provider Network Management Services Administrator for Contracting Physician Organizations PART 1: PRACTITIONER ORGANIZATION INTRODUCTION Strict federal and state regulations and accreditation requirements govern the administrative operations of practitioner organizations (POs), such as medical groups and independent physician associations (IPAs), with respect to their patients who are enrolled in managed care health plans, also known as health maintenance organizations (HMOs). In order for POs contracting with MED3OOO to maintain their state licenses and the contractual arrangements with managed care organizations that help them meet market demands, practitioners employed by or under contract with them are required to meet stringent standards of performance. Practitioners granted panel privileges must share an ongoing commitment to participating in and complying with patient management, credentialing, utilization management and quality improvement program activities, which define many aspects of a practitioner’s practice. The information that follows highlights the key requirements for HMO practice management that are highly important and require your active participation as a practitioner contracting with the following MED3OOO affiliated POs: SeaView IPA Valley Care Select IPA Santa Barbara Select IPA Valley Care IPA Leisure World Managed Care Medical Group Pioneer Provider Network Section Part 1: Part 2: Pages Practitioner Organization Introduction 5 Mission Statement 6 Independent Physician Association 7 Committees and Members 8 MED3OOO Overview 11 Management Contacts 12 Primary Care Physician Responsibilities 13 PCP Functions 14 Advanced Directives 20 Eligibility Verification 21 Member Relations 22 Provider Relations 23 Finance 24 PCP Capitation EOB 27 Page 2 Management Services Administrator for Contracting Physician Organizations PART 1: PRACTITIONER ORGANIZATION INTRODUCTION Part 3: Part 4: Part 5: Part 6: Specialist Capitation EOB 29 Eligibility 30 Network Development 31 Policies and Procedures (available on the SVIPA web site) Physician Compensation 32 Billing Instructions 33 Claim Submission 34 Co-Payment/Co-Insurance Collection 35 Dual Coverage and COB 35 EOB 36 Encounter Data Submission 37 California Children Services 37 Provider Satisfaction Survey 37 Patient Access to Care and Service 38 Patient Rights and Responsibilities 38 Patient Access Standards 40 Practitioner-Patient Relationships 43 Credentialing Program 48 The Credentialing Mandates 48 Licensure and DEA/CDS Certification 49 Board Certification 49 Malpractice Liability Coverage 49 Other Credentialing Requirements 49 Availability of Credentialing Program Description 50 Credentialing Information Contact 50 Utilization Management Program 51 UM Program Responsibility 51 Decision-Making Policies 51 Availability of Utilization Management Program Description 52 UM Department Business Hours 52 Page 3 Management Services Administrator for Contracting Physician Organizations PART 1: PRACTITIONER ORGANIZATION INTRODUCTION Requirements for Specialty Care, Ancillary Service and Inpatient Referrals 52 Services Subject to Review 52 Services Not Subject to Review 53 Services Coordinated Through Patients’ Health Plans 54 Information Required for Case Reviews 55 Initiating a Case Review 56 Reporting Emergency Inpatient Admissions 57 Authorized Referral Providers 58 Authorization Problems 58 UM Decision-Making Criteria and Guidelines 59 Case Management Programs 60 Quality Improvement Program 61 Availability of Quality Improvement Program Description 61 Physician Supervision of Non-Physician Practitioners 61 Medical Records Requirements and Audits 62 Facility Operations Requirements and Audits 63 Access Audits 63 Part 8: How to Contact Us 64 Part 9: Appendix Part 7: Waiver Form 65 Sample Member Introduction Letter for PCPs 66 Referral Authorization Form 68 See Internet for current PCP & Specialist listings and EZNet User Manual Part 10: Glossary 74 Page 4 Dear Physician and Office Manager: I would like to thank you for your participation with the IPA or Medical Group. We appreciate the opportunity to work with you and your staff in a joint effort to provide high quality, effective patient care and service to our members. This Provider Manual was developed to provide you and your staff with information to assist you regarding the procedures that should be followed in the areas of authorizations, case management, quality improvement, credentialing, finance, eligibility, claims, contracting, provider relations, member relations and health education. I am confident that this manual in conjunction with communication with the appropriate departments will ensure smooth operations for your office and the members, which is our primary objective. The Provider Manual will be revised periodically and I welcome any suggestions or comments for improvement. Should you have any questions or require additional assistance, please do not hesitate to contact the Management Team. We look forward to a continued strong partnership with you and a successful future. Sincerely, Lynn Haas, Executive VP, MED3OOO Page 5 MISSION STATEMENT MED3OOO is the leader in quality cost effective health care management. We are responsive to changing markets through innovative diversified planned delivery systems. MED3OOO is committed to providing quality patient care by combining case management with medical technology. The partnership between MED3OOO and its customers realize fulfillment through a shared commitment in continuous quality improvement. Page 6 INDEPENDENT PHYSICIAN ASSOCIATIONS In the managed care industry, the Independent Physician Association (IPA) physicians, practice independently in their own offices and care for patients with HMO insurance coverage. These physician-oriented organizations were formed in order to contract with prepaid health plans (i.e., HMOs) and to function as Accountable Care Organizations. More and more third party payors, including HMOs, consider it to be cost-effective to purchase managed health care through a coordinated group of physicians. These purchasers are also looking for a long-term partnerships with physician groups to provide quality, cost-effective health care with high levels of customer satisfaction. MED3OOO provides full or partial management services to the following IPA’s prepaid physician organizations: SeaView IPA Valley Care IPA Valley Care Select IPA Santa Barbara Select IPA Leisure World Managed Care Medical Group Pioneer Provider Network MED3OOO OFFICE LOCATIONS: Oxnard Main Office: 1901 N. Solar Dr., Suite 265 Oxnard, CA 93036 Phone: (805) 988-2280 Fax: (805) 988-5164 Cerritos Satellite Office: 17777 Center Court Drive, Suite 425 Cerritos, CA 90703 Phone: (562) 865-0208 Fax: (805) 278-4275 PROVIDER & MEMBER SERVICES CONTACT NUMBERS: Member Services Provider Services SeaView IPA Valley Care IPA Valley Care Select IPA Santa Barbara Select IPA Leisure World Managed Care Pioneer Provider Network (805) 988-5188 (877) 311-5411 (805) 604-3332 (877) 299-5599 (805) 604-3332 (877) 299-5599 (805) 278-6823 (800) 705-0831 (805) 604-3317 (855) 415-4455 (805) 988-5164 (888) 720-2323 (805) 604-3325 (805) 604-3308 (805) 604-3308 (805) 278-6823 (800) 705-0831 (805) 604-3317 (855) 415-4455 (805) 988-5164 (888) 720-2323 Page 7 BOARDS OF DIRECTORS SeaView IPA Edward Banman, MD – Chairman Gary Proffett, MD – Medical Director Chris Arnold, MD Michael Bailey, MD Andrew Weymer, MD Timothy Bryant, MD Stephen Feinberg, MD Jon Schrock, MD Valley Care IPA Gary Deutsch, MD - President Santa Barbara Select IPA Jerome Kay, MD - President Michael Swartout, MD – Medical Director Michael Tushla, MD Treasurer Jeffery Tubbs, MD - Secretary Gary Wikholm, MD Geoffrey Loman, MD Logan Bundy, MD Gosta Iwasiuk, MD Ramsey Ulrich, MD Stanley Patterson, MD Kirk Gilbert, MD - Medical Director Gary Ponto, MD Leisure World Managed Care Medical Group Jesse Chang, MD Mario Curti, MD Ellen Dayon, MD L. Wayne Freeman, MD Rudolf Haider, MD - Chairman Daniel Rodiles, MD Mary Sherman, ND Victor Tacconelli, MD John Wrench, MD David Laub, MD Paul Aijian, MD - Treasurer Pioneer Provider Network Pinal Doshi, MD Jerry Floro, MD Don Garcia, MD Sanat Kumar Patel, MD - Chairman Edwardo Tellez, MD COMMITTEES UTILIZATION MANAGEMENT COMMITTEES SeaView IPA Gary Proffett, MD - Chairman/ Medical Director Michael Bailey, MD Imelda DeForest, MD Theodore Hostetler, MD Cary Savitch, MD Joseph Lopresti, MD Arthur Inoshita, MD Irene Wakam, Carl Gross, MD Alon Steinberg, MD Saumil Gandhi, MD Lorna Barte, MD Valley Care IPA Michael Swartout, MD – Medical Director Robert Dekkers, MD Chairman Kathleen Beuttler, MD Mikael Hakansson, MD Alexander Meyer, MD Gary Wikholm, MD Santa Barbara Select IPA Kirk Gilbert, MD - Chairman/ Medical Director Dennis Ashley, MD Dean Given, PhD Gary Ponto, MD Kenneth Wagner, MD John Wrench, MD Page 8 UTILIZATION MANAGEMENT COMMITTEES Leisure World Managed Care Medical Group Nancy Smith, MD - Chairman Rudolf Haider, MD Ellen Dayon, MD Prakash Narain, MD Mary Sherman, MD Gary Nemhauser, MD Abes Bagheri, MD Pioneer Provider Network Don Garcia, MD - Chairman Emerico Csepanyi, MD Pinal Doshi, MD Jerry Floro, MD – Chairman David Middleton, PHD Angelyn Moultrie-Lizana, DO Sanatkumar Patel MD Edward Tellez, MD Joseph Lombardo, MD QUALITY IMPROVEMENT COMMITTEES SeaView IPA John Ford, MD - Chairman Gary Proffett, MD - Medical Director Danielle Onstot, MD Sanjiv Verma, MD Lin Tesu, MD Scott Roberg, DPM Lisa Babashoff, MD Sahin Yanik, MD Jodi Ferro, MD Valley Care IPA Michael Swartout, MD – Medical Director Robert Dekkers, MD Chairman Santa Barbara Select IPA Kirk Gilbert, MD Chairman/ Medical Director Dennis Ashley, MD Kathleen Beuttler, MD Mikael Hakansson, MD Alexander Meyer, MD Gary Wikholm, MD Dean Given, PhD Gary Ponto, MD Kenneth Wagner, MD John Wrench, MD Leisure World Managed Care Medical Group Nancy Smith, MD - Chairman Rudolf Haider, MD Ellen Dayon, MD Prakash Narain, MD Mary Sherman, MD Gary Nemhauser, MD Abes Bagheri, MD Terri Furlow 0 LWHC Administrator Pioneer Provider Network COMPENSATION & CONTRACTING SeaView IPA Edward Banman, MD – Chairman Gary Proffett, MD – SVIPA Medical Director Timothy Bryant, MD Jon Shrock, MD Andrew Weymer, MD Valley Care IPA NA Santa Barbara Select IPA NA Page 9 COMPENSATION & CONTRACTING Leisure World Managed Care Medical Group NA Pioneer Provider Network NA CREDENTIALS COMMITTEES SeaView IPA Arthur Inoshita, MD - Chairman Valley Care IPA Gary Proffett, MD - SVIPA Medical Director Carey Chronis, MD Theodore Hostetler, MD Cheryl Geer, DO Lynn Pluche, MD Robert O’Hara, MD Michael Swartout, MD – VCIPA Medical Director Leisure World Managed Care Medical Group Mary Sherman, MD Rudolf Haider, MD - Chairman Ellen Dayon, MD Nancy Smith, MD Gary Nemhauser, MD Prakash Narain, MD Santa Barbara Select IPA Kirk Gilbert, MD Chairman/ Medical Director Dennis Ashley, MD Dean Given, PhD Gary Ponto, MD Kenneth Wagner, MD John Wrench, MD Pioneer Provider Network Jerry Floro, MD – Chairman Don Garcia, MD - Chairman Pinal Doshi, MD Emerico Csepanyi, MD Edward Tellez, MD Angelyn Moultrie-Lizana, DO Sanatkumar Patel MD Page 10 Management Services Administrator for Contracting Physician Organizations PART 2: MED3OOO OVERVIEW The following are representative of some of the Operational Tasks preformed by the administrative staff of MED3OOO: (This does not imply that all PO’s have contracted with MED3OOO for the same services) Accounting Authorizations Benefit Interpretation/Compliance Capitation Case Management Claims Encounter and/or Payment Contract Negotiations (Health Plan, Physician, Hospital and Ancillary) Detail Record-keeping EZ-CAP (MIS System) Usage and Maintenance Financial Management Health Plan Communication Legislature Compliance Member Eligibility Member Services Office Managers Education/Communication Physician Education/Communication Provider Credentialing Quality Improvement Page 11 Management Services Administrator for Contracting Physician Organizations PART 2: MED3OOO OVERVIEW MANAGEMENT CONTACTS Staff Name Title Area of Responsibility Phone Number Lynn Haas, CPA CEO Overall Operations (805) 988-2280 Debbie Tuttle, CPA CFO Finance (805) 988-2280 Janet Plait Accounting Director Leslie Young Director of Contracting Dione Webster Contracts Manager Lisa Barnes, RN Veronica Vasquez Director of Health Services Information Systems Manager Capitation, Eligibility, Accounting Contracting, Network Development Contracting, Network Development (805) 988-5187 (805) 988-5101 (805) 988-5182 Health Services (805) 604-3314 Information Systems (805) 988-5155 Kevin Taylor Director of Operations Member Services, Prov. Relations, Claims (805) 604-3324 Adrienne Gardner Claims Manager Claims (805) 988-5145 Member & Provider Relations Manager Provider Network Manager – PPN & LW Member and Provider Services Contracting & Provider Relations – Cerritos Office Christina Muro HCC & P4P Supervisor HCC & P4P (805) 278-6848 Robin Broms, LVN Case Mgmt./Quality Improvement Manager Case Management Quality Improvement (805) 988-5129 Melissa Frayre, RN Authorizations Manager Authorization Department Irene Ybarra Gabbie Nguyen Jennifer Moore Sonya Araiza Executive Director SBSIPA Executive Director VCIPA Santa Barbara Select IPA Valley Care IPA (805) 988-5116 (805) 278-6877 (805) 988-5142 (805) 988-5166 (805) 278-6818 Lynn Haas COO Leisure World Managed Care Medical Group (805) 988-2280 John M. Kirk CEO Pioneer Provider Network (562) 229-9452 Page 12 Management Services Administrator for Contracting Physician Organizations PART 2: MED3OOO OVERVIEW PRIMARY CARE PHYSICIANS RESPONSIBILITIES Generally, primary care services are provided by internal medicine providers, family providers, pediatricians, general providers, Nurse Practitioners, and Physician Assistants, under the supervision and direct monitoring of the PCP, may also be included. The scope of service for the PCP is defined as noted in the [Health and Safety Code of California (section 1367.69) and existing Knox-Keene] regulations as physicians who have the “responsibility for providing initial and primary care for patients, for maintaining the continuity of patient care, and for initiating referral for specialty care”. This includes, but is not limited to, preventive services (as outlined in the current HEDIS clinical indicators), acute and chronic conditions and psychosocial issues. The PCP is responsible for the direction and coordination of the patient’s complete medical care for covered services. The PCP will arrange for laboratory diagnostics, imaging diagnostics, referrals to specialist, hospitalization or any other covered benefit that is medically necessary. A referral is required for cases beyond the scope of expertise and practice of the PCP. The PCP must accept new members without regard to race, ethnicity, religion, gender, color, national origin, age, sexual orientation, genetic information, source of payment, any factor related to physical or mental health status including but not limited to medical condition, claims experience, receipt of healthcare, medical history, genetic information, evidence of insurability, disability, or on any other basis deemed unlawful under federal, state or local law. PCP authorizes MED3OOO, the Provider Organization (PO), health plans, the Secretary of Health and Human Services, the General Accounting Office or their designees the right to audit, evaluate or inspect any books, contracts, medical records, patient care documentation and other records of the provider that pertain to services performed, reconciliation of benefit liability, determination of amounts payable or any other relevant matters as such person auditing deems necessary for the later of six (6) years, or for periods exceeding six (6) years, for reasons specified in the federal regulation. RESPONSIBILITIES: 1. The PCP is responsible for providing the majority of and coordinating all the services required for the member, except when emergent circumstances preclude the role of the PCP. 2. The PCP is to provide periodic evaluation of all body systems, preventive services, acute and chronic care and to address psychosocial issues. 3. For Medi-Cal members, the PCP is required to conduct an Initial Health Assessment within 120 days of member’s enrollment with the PCP. 4. For Senior HCFA members, the PCP is required to conduct an Initial Health Assessment within 90 days of members’ enrollment with the PCP. 5. The PCP is required to perform all duties expected of a PCP such as on-call rotation and/or coverage for emergencies. 6. When care by a Specialist is necessary, the PCP coordinates all services required by the Specialist. Page 13 Management Services Administrator for Contracting Physician Organizations PART 2: MED3OOO OVERVIEW 7. The PCP provides those services within the skills of that specialty and obtains authorization for consultations when additional expertise or skills are required. 8. The PCP is expected to relay the PO or health plan decisions in a positive manner. When the purpose of the visit is for a non-covered service/benefit, the PCP must inform the member that the service is non-covered. This needs to be documented in the medical record. 9. In the event of the PO’s or health plan’s insolvency or other cessation of operations or termination of the health plan’s Medicare agreement, Provider will continue to provide covered services to Medicare members through the period for which premium has been paid to health plan or in the case of Medicare members who are hospitalized, benefits shall continue until discharge from facility, whichever time is greater. In the event the Provider’s contract is discontinued, the PO allows members to have continued access to that Provider if they are undergoing active treatment for a chronic or acute medical condition through the current period of active treatment or for up to 90 days, whichever is shorter. PCP FUNCTIONS Listed below, but not limited to, are services considered PCP functions. This is dependent on the level of training the physician has received, the limitations of scope of practice and consistent with State and Federal rules and regulations. These guidelines are based on routine uncomplicated cases that are ordinarily seen by a PCP. OFFICE/CLINIC Allergy: Treat seasonal allergies Treat hives Treat chronic rhinitis Allergy history Environmental counseling Minor insect bites/stings Asthma, (chronic/acute) active with or without co-existing infection Cardiology: Perform electrocardiograms Interpret electrocardiograms Evaluate chest pain, murmurs, palpitations Page 14 Management Services Administrator for Contracting Physician Organizations PART 2: MED3OOO OVERVIEW Evaluate and treat coronary risk factors, including smoking, hyperlipidemia, diabetes, Hypertension (HTN), lifestyle Evaluate and treat Congestive Heart Failure (CHF), stable angina, non life-threatening arrhythmias Evaluate syncope (cardiac and non-cardiac) Dermatology: Treat acne (acute and recurrent) Treat painful or disabling warts with topical suspensions, electrocautery, liquid nitrogen Diagnose and treat common rashes including: Contact dermatitis, dermatophytosis, herpes genitalis, herpes zoster, impetigo, pediculosis, pityriasis rosea, psoriasis, seborrheic dermatitis and tinea versicolor Identify suspicious moles Screen for basal or squamous cell carcinomas Biopsy suspicous lesions Punch Biopsy (Bx) Excisional Bx Actinic Keratosis Diagnose and treat common hair and nail problems and dermal injuries Common hair problems include: fungal infections, ingrown hairs, virilizing causes of hirsutism, or alopecia as a result of scarring or endocrine effects Common nail problems include: trauma, disturbances associated with other dermatoses or systemic illness, bacterial or fungal infections, and ingrown nails Dermal injuries include: minor burns, lacerations, and treatment of bites and stings Counsel patients regarding removal of cosmetic (non-covered) lesions Endocrinology: Diabetic management, including Type I and Type II patient Patient education Supervision of home (SBGM) testing Medication management Diagnose and treat thyroid disorders Page 15 Management Services Administrator for Contracting Physician Organizations PART 2: MED3OOO OVERVIEW Identify and treat hyperlipidemia Diet instruction and Exercise Instruction Provide patient education for osteoporosis risk factors Gastroenterology: Diagnose and treat lower abdominal pain Diagnose and treat acute diarrhea Treat protracted vomiting Occult blood testing Diagnose and treat heartburn, upper abdominal pain, hiatal hernia, acid peptic disease Diagnose and treat irritable bowel syndrome Diagnose and treat chronic jaundice under Standard Practice of Care (SPC) recommendations Diagnose and treat chronic ascites under SPC recommendations Diagnose and treat symptomatic, bleeding or prolapsed hemorrhoids Manage inflammatory bowel disease under SPC recommendations General Surgery: Evaluate and follow small breast lumps Order mammograms Aspirate cysts Foreign body removal Laceration repairs (minor) Local minor surgery for hemorrhoids Minor surgical procedures Gynecology: Perform routine pelvic exams and PAP smears Perform lab testing for sexually transmitted diseases Wet mounts Page 16 Management Services Administrator for Contracting Physician Organizations PART 2: MED3OOO OVERVIEW Diagnose and treat vaginitis and sexually transmitted diseases Evaluate lower abdominal pain to distinguish gynecological from gastrointestinal causes Diagnose vaginal bleeding Diagnose and treat endometriosis with hormone therapy Manage premenstrual syndrome with non-steroidal anti-inflammatory agents, hormones and other symptomatic treatment Hematology: Initial differential diagnosis of anemias Hemoglobinopathies Infectious Disease: Common infectious diseases Initial evaluation for Human Immunodeficiency Virus (HIV) positive Viral disorders Tuberculosis prophyaxis Neurology: Diagnose and treat all psychophysiological diseases; headaches, low back pain, myofascial pain syndromes, neuropathies Diagnose and treat tension and migraine headaches Treat syncope (cardiac and non-cardiac) Treat uncomplicated seizure disorders after SPC neurological evaluation Manage degenerative neurological disorders with respect to general medical care (i.e., Parkinson's) Treat stroke and Transient Ischemic Attack (TIA) patients Manage dementia, Alzheimer’s disease Ophthalmology: Perform thorough ophthalmologic history including symptoms and subjective visual acuity Perform common eye related services including: Distant/near testing, color vision testing, gross visual field testing by confrontation, alternate cover testing, direct funduscopy without dilation, extraocular muscle function evaluation, red reflex testing in pediatric patients Page 17 Management Services Administrator for Contracting Physician Organizations PART 2: MED3OOO OVERVIEW Diagnose and treat common eye conditions including: viral, bacterial and allergic conjunctivitis, blepharitis, hordeolum, chalazion, small subconjunctival hemorrhage, dacryocystitis and sty Orthopedics: Treat low back pain Treat sprains, strains, pulled muscles, overuse syndromes Treat inflammatory conditions Conservative treatment of chronic knee problems Manage chronic pain problems Diagnose and treat common foot problems: Ingrown nails, corns/callouses, bunions Closed emergency reduction of dislocation: Digit, elbow, patella, shoulder Treatment of minor fractures Arthrocentesis Otolaryngology: Treat tonsillitis and streptococcal infections Perform throat cultures Evaluate and treat oropharyngeal infections: Stomatitis, Herpes simplex Treat acute otitis media Treat serous effusion Evaluate tympanograms/audiograms Treat acute and chronic sinusitis Treat allergic or vasomotor rhinitis Remove ear wax Diagnose and treat acute parotitis and acute salivary gland infections Evaluate neck masses Pulmonology: Diagnose and treat asthma, acute bronchitis, pneumonia Diagnose and treat chronic bronchitis Page 18 Management Services Administrator for Contracting Physician Organizations PART 2: MED3OOO OVERVIEW Diagnose and treat chronic obstructive pulmonary disease Manage home aerosol medications and oxygen Work up possible tuberculosis or fungal infections Treat opportunistic infection Rheumatology: Diagnose and treat non-articular muscloskeletal problems: Overuse syndromes, injuries and trauma, soft tissue syndromes, bursitis or tendonitis Provide steroid injections Manage osteoarthritis Diagnose gout, pseudogout Diagnose and treat rheumatoid arthritis Diagnose and treat inflammatory arthritic diseases Diagnose and treat uncomplicated collagen diseases Urology/Nephrology: Diagnose and treat initial and recurrent urinary tract infections Provide long term chemoprophylaxis for recurrent Urinary Track Infection (UTI) Diagnose and treat urethritis Explain hematospermia Evaluate hematuria Evaluate incontinence Diagnose and treat epididymitis and prostatitis Differentiate scrotal or peritesticular masses from testicular masses Evaluate prostatism and prostatic nodules Manage urinary stones Vascular Surgery: Diagnose abdominal aortic aneurysm Diagnose and treat venous diseases, i.e., Deep Vein Thrombosis (DVT), varicose veins, stasis dermatitis Page 19 Management Services Administrator for Contracting Physician Organizations PART 2: MED3OOO OVERVIEW Treat non-surgical stasis ulcers Manage intermittent claudication Manage transient ischemic attacks Manage asymptomatic bruits Other: Basic life support Heimlich maneuver Endotracheal intubation. if Advanced Cardiac Life Support (ACLS) certified Advanced life support, if ACLS certified Tracheostomy (emergency), if ACLS certified ADVANCED DIRECTIVES It is the policy of MED3OOO that information describing the patient’s rights to formulate advance directives as well as advance directive forms and literature will be provided by providers to all adult members who may complete a Durable Power of Attorney for Health Care, or any other advance directive. Client and/or provider will not refuse to treat or otherwise discriminate against a member who has completed advance directive forms. MED3OOO and/or provider will honor advance directives and assist and guide patients with regard to these sensitive issues. The provider will document execution of an advance directive in the patient medical record and educate staff regarding issues concerning advance directives. An adult is defined as being 18 years of age or older. 1. The provider will become well informed about advance directives and take an active role in assisting patients to understand the benefits of these documents. 2. The provider will have available for the member advance directive forms and literature. 3. The provider will not refuse to treat or otherwise discriminate against a member who has completed an advance directive form. 4. The provider will honor advance directive forms completed by the member. 5. The provider will document discussion and/or execution of an advance directive in the member’s medical record. Page 20 Management Services Administrator for Contracting Physician Organizations PART 2: MED3OOO OVERVIEW ELIGIBILITY VERIFICATION Members should have a membership card, which identifies their PCP, identification number, co-pay, and enrollment information in the health plan, which is contracted for medical care and service with the PO. The identification card does not guarantee current eligibility. It is only used to identify the member information. 1. For electronic verification of eligibility you may query the MED3OOO system (see EZ-NET instructions in Chapter 4). However, the provider is advised this information is not as current as each Health Plan’s information. Therefore, to be relied upon, eligibility should be confirmed directly with the member’s health plan at the time of service. PCPs will receive computer-generated eligibility lists on a monthly basis. If these lists are not received, please notify the Eligibility Department or your Provider Relations Representative. 1. When a member presents for service, check the most current eligibility list. If the member’s name appears, they are eligible to be treated. 2. If the member’s name does NOT appear on the most current eligibility list, please ask the member for the following information: Membership card or health plan enrollment form Member’s full name Subscriber’s full name Subscriber’s date of birth Member’s date of birth Subscriber’s employer (and employer telephone if possible) Effective date of coverage (if known) 3. Call MED3OOO Eligibility Department with the above information for verification. SeaView IPA (805) 604-3325 (877) 311-5411 Valley Care IPA (805) 604-3308 (877) 299-5599 Valley Care Select IPA (805) 604-3308 (877) 299-5599 Santa Barbara Select IPA (805) 278-6823 (800) 705-0831 Leisure World MCMG (805) 604-3317 (800) 415-4455 Pioneer Provider Network (805) 988-5164 (800) 720-2323 4. If eligibility cannot be verified, and the member MUST be seen, a waiver form is to be completed. (See the Waiver Form in the appendix page 66) Page 21 Management Services Administrator for Contracting Physician Organizations PART 2: MED3OOO OVERVIEW DEPARTMENT: Member Relations CONTACT: Irene Ybarra, Member Relations Manager PHONE: (805) 988-5116 FAX: (805) 988-5163 Summary The Member Relations Department of MED3OOO is responsible to service the providers, health plans, members and MED3OOO staff including providing information and problem resolution which will assist in offering high quality services. Function The Member Relations Department is the liaison to all other departments within MED3OOO, (Authorizations, Claims, Eligibility, etc.) for members, providers and health plan representatives. Each call is fielded by a Member Relations Associate (MRA) or Lead Member Relations Associate (Lead MRA) and documented in the customer service module of EZ-Cap for tracking purposes. If a MRA is unable to answer a question or give a specific status at the time of the call, the MRA may request assistance or direction from the Lead MRA or submit an inquiry via the EZ-Cap system to the respective department for a reply. Turn-around time for inquiries routed to other departments range from twenty-four (24) hours to five (5) working days based on the level of the inquiry (stat, urgent, routine, etc.). Issues to Refer Inquiries regarding: Authorizations Claims Education Eligibility Health plans Physicians (Primary Care Physicians and Specialists) Providers (ancillary, hospitals) Page 22 Management Services Administrator for Contracting Physician Organizations PART 2: MED3OOO OVERVIEW DEPARTMENT: Provider Relations CONTACT: Irene Ybarra, Provider Relations Manager PHONE: (805) 988-5116 FAX: (805) 988-5163 Summary The Provider Relations Department of MED3OOO is responsible for providing services to the providers, health plans and staff including problem resolution which will assist the providers in offering high quality services. The Provider Relations staff acts as a liaison with other departments, participating in projects and analysis that assist in addressing and resolving concerns. Function The Provider Relations Department is the liaison to all of the other departments (Authorizations, Claims, Eligibility, etc.) for providers and health plan representatives with concerns that are out of the Member Relations Department’s function or scope. Turn-around time for replies to inquiries rerouted to other departments range from twenty-four (24) hours to five (5) working days, based on the level of the inquiry (stat, urgent, routine, etc.). Issues to Refer Problem resolution regarding: Eligibility Health Plans Physician office orientations Provider manuals Provider rosters Reimbursement Updates regarding physician practice Address changes Page 23 Management Services Administrator for Contracting Physician Organizations PART 2: MED3OOO OVERVIEW DEPARTMENT: Finance CONTACT: Janet Plait, Accounting Director PHONE: (805) 988-5187 FAX: (805) 988-5167 Capitation Procedure – Primary Care Physicians Each PO has entered into agreements with certain primary care physician providers whereby they are paid an amount of capitation per member per month in lieu of fee-for-service reimbursement for services they will render to their assigned patients. The actual amount of this capitation paid varies with the age and sex of the individual health plan member. Primary Care Physician (PCP) capitation checks are mailed on or before the 20th day of the month for the current month. Please refer to the sample PCP Capitation EOB report (Attachment 1). The following describes the calculation methodology used to compute the monthly capitation payment: Column (A) HP Code – Health plan code. Column (B) Member Months to Date – Member months by health plan for the last six (6) months. Column (C) Capitation $ Earned to Date - Member months (Column B) multiplied by applicable capitation rate table. Column (D) Capitation $ Previously Earned – Amount of capitation previously paid for the prior five (5) months. Column (E) Gross Capitation Due – Current month capitation plus/minus retroactivity for prior five (5) months. Column (F) Adjustments – Adjustments such as deduction from PCP for failure to follow applicable referral procedure, which results in a fee-for-service claim paid to a non-contracted provider. Column (G) Net Capitation Due – Payment for the current month. This equals Column E plus/minus Column D. In addition, the PCP receives a PCP Reconciliation Report. This report shows the detail of capitation paid by member for the current month and the retroactivity for the prior five months. Please refer to the sample PCP Reconciliation Report (Attachment 2). Column (A) MEMBER NAME - Member Name Column (B) MEMBID – Member I.D. as assigned by the health plan Column (C) HP CODE & OPT – Health plan code and benefit option Column (D) EFFEC DATE – Effective date with PCP Column (E) TERM DATE – Termination date from IPA Page 24 Management Services Administrator for Contracting Physician Organizations PART 2: MED3OOO OVERVIEW Column (F) AGE – Member’s age Column (G) DOB – Member’s date of birth Column (H) SEX – Member’s sex Column (I) COPAY – Office visit co-pay Column (J) CURRENT ENROLLMENT MM – Member months paid in current month Column (K) CURRENT ENROLLMENT CAP$ - Column J member months multiplied by applicable age/sex cap rate table Column (L) MANUAL ADJ MM – Adjustment to member months calculation Column (M) MANUAL ADJ CAP$ - Column L member months multiplied by applicable age/sex cap rate table Column (N) PREVIOUS CALC MM – Member months previously paid Column (O) PREVIOUS CALC CAP $ - Column N member months multiplied by applicable age/sex cap rate table Column (P) NET TO PAY MM – Net member months paid. Equals Column J plus/minus Column L minus Column N. Column (Q) NET TO PAY CAP$ - Monthly capitation paid to provider. Equals Column K plus/ minus Column M minus Column O. Subtotals by month are included for the current month plus the five (5) prior months. Capitation Procedure – Specialists Each PO has entered into agreements with certain specialty providers whereby they are paid an amount of capitation per member per month in lieu of fee-for-service reimbursement for services they will render to their assigned patients. Specialty capitation checks are mailed on or before the twentyfifth (25th) day of the month for the current month. Please refer to the sample specialty capitation summary report (Attachment 3). The following describes the calculation methodology used to compute the monthly capitation payment: Column (A) HP Code – Health plan code Column (B) Current Month Members – Member from the current month’s eligibility list. Column (C) Retroactive Members – Retroactive additions or deletions for the prior five (5) months. Column (D) Net Member Months – Current month eligibility plus/minus retroactivity for prior five (5) months. This equals Column B plus/minus Column C. Column (E) Total Due by HP – Total capitation due to provider by health plan. Page 25 Management Services Administrator for Contracting Physician Organizations PART 2: MED3OOO OVERVIEW Column (F) Current Adjustments – Adjustments such as deduction from specialist for inability to provide medical care for referred procedure which results in a fee-for-service claim pair to a non-contracted provider. Column (G) Current Net – Payment for the current month. This equals Column E plus/minus Column F. Page 26 Management Services Administrator for Contracting Physician Organizations PART 2: MED3OOO OVERVIEW ATTACHMENT 1 01/01/XX Page 1 Practitioner Organization Name CAPITATION EOB FOR JANUARY, 20XX Primary Care Physician FOR PROVIDER: XXXXXX (A) PCP NAME (B) (C) MEMBER CAPITATION $ MONTHS EARNED HP CODE HEALTH PLAN AE BSH HN PC SH AETNA HEALTH PLANS BLUE SHIELD HEALTHNET PACIFICARE SECURE HORIZONS PROVIDER TOTALS TO DATE (D) (E) CAPITATION PREVIOUSLY GROSS CAPITATION EARNED DUE TO DATE $ $ $ (F) (G) NET CAPITATION ADJUSTMENTS $ DUE __________ $ Page 27 Management Services Administrator for Contracting Physician Organizations PART 2: MED3OOO OVERVIEW ATTACHMENT 2 ____________ IPA PCP Capitation Reconciliation Report By Vendor, Provider June 20XX Through November 20XX 04/25/20XX VENDOR PROVIDER :123456 CAPITATION MONTH: Name, MD Last Name June, 20XX CURRENT ENRLMT MEMBER NAME CAPITATION MONTH: TOTALS FOR MONTH: CAPITATION MONTH: TOTALS FOR MONTH: MEMBER ID June, HP & OPT July, 20XX TERM DATE DATE AGE DOB SEX COPAY MM CAP $ MM CAP $ PREVIOUS CALC MM CAP $ NET TO PAY MM CAP $ 20XX June, 20XX July, EFF MANUAL ADJ 0 $0.00 0 $0.00 0 $0.00 0 $0.00 0 $0.00 0 $0.00 0 $0.00 0 $0.00 20XX Page 28 Management Services Administrator for Contracting Physician Organizations PART 2: MED3OOO OVERVIEW ATTACHMENT 3 Specialty Cap Payment Summary for the month of: May-20XX TO: SAMPLE SPECIALIST (A) SPECIALIST: (B) HP CODE (C) (D) (E) (F) (G) May-XX RETROACTIVE NET MEMBER TOTAL DUE CURRENT CURRENT MEMBERS MEMBERS MONTHS BY HP ADJUSTMENTS NET Commercial AE CA CC CI HN PC ________ ________ ________ _______ _________ TOTAL $ $ Specialty Cap Payment Summary for the month of: May-20XX TO: SAMPLE SPECIALIST (A) SPECIALIST: (B) May-XX HP CODE (C) RETROACTIVE (D) NET MEMBER (E) TOTAL DUE MEMBERS MEMBERS MONTHS BY HP (F) (G) CURRENT CURRENT ADJUSTMENTS NET Senior CCS SH CASH ________ ________ ________ _______ _________ TOTAL $ $ . TOTAL DUE: $ Page 29 Management Services Administrator for Contracting Physician Organizations PART 2: MED3OOO OVERVIEW DEPARTMENT: Eligibility CONTACT: Janet Plait, Accounting Director PHONE: (805) 988-5187 FAX: (805) 988-5167 Verify Eligibility 1. Call the corresponding PO at MED3OOO to speak to a Provider Relations Representative. SeaView IPA Valley Care IPA Valley Care Select IPA Santa Barbara Select IPA Leisure World MCMG Pioneer Provider Network (805) 604-3325 (805) 604-3308 (805) 604-3308 (805) 278-6823 (805) 604-3317 (805) 988-5164 (877) 311-5411 (877) 299-5599 (877) 299-5599 (800) 705-0831 (855) 415-4455 (888) 720-2323 2. Be prepared to provide the member name or the health plan ID # to the representative. 3. The representative will check the member database to determine if the member is currently eligible. 4. The representative will advise you either: a) the member is currently eligible b) the member’s name or ID # could not be located in the database 5. If the member’s name could not be located in the database, the representative will complete an eligibility request form that is forwarded to the appropriate person for research. The member’s eligibility status will be researched and reported back to the Provider Relations representative. 6. Within 1-2 working days, the member resources representative will call you back to advise you of the member’s eligibility status. Procedure for EZ-Net Users to check eligibility 1. Log on to EZ-Net. (see Chapter 4 in the EZNet user manual located in the appendix) 2. Select Eligibility from the Main Menu. 3. Type LAST NAME, FIRST (partial or complete), ID or HP to list the member. 4. Select a member from a list of names and click the blue hyperlink for detail. Click on “Inquire about this member,” at the bottom of the screen if you would like to send an e-mail to MED3OOO regarding the member’s eligibility. Page 30 Management Services Administrator for Contracting Physician Organizations PART 2: MED3OOO OVERVIEW DEPARTMENT: Contracting & Network Development CONTACT for SVIPA, VCIPA, VCSIPA: Leslie Young, Director of Contracting or Dione Webster, Contracts Manager PHONE: (805) 988-5101 or (805) 988-5182 FAX: (805) 988-5194 CONTACT for SBSIPA: Jennifer Moore, Executive Director PHONE: (805) 988-5166 FAX: (805) 988-5167 CONTACT for Leisure World or Pioneer Provider Network: Gabbie Nguyen, Provider Network Manager Phone (805) 278-6877 FAX: (805) 278-4275 Summary The Contracting & Network Development Department of MED3OOO and or the Executive Directors for each IPA is responsible for contract negotiations and providing contract information which will assist the providers. Issues to Refer Contracts (primary care, specialist, ancillary, hospitals, health plans, etc.) Letters of Agreement (specific one time case rate contracts) Prospective (interested) providers Questions regarding provider’s or IPA’s contracted responsibilities Questions regarding interpretation of contract rates Third party liability & workers comp cases Function It is the Contracting & Network Development Department’s function to ensure that there is adequate provider representation to service our membership. Recruitment of providers is based on current and anticipated needs and from information provided by other departments (Health Services, Credentials, Quality Improvement and Provider Relations). The department negotiates contracts with providers and prospective providers based upon decisions made by the Compensation and Contracting Committees, Credentials Committees and the Boards of Directors. Page 31 Management Services Administrator for Contracting Physician Organizations PART 3: POLICIES AND PROCEDURES PHYSICIAN COMPENSATION Each PO receives a fixed monthly pre-payment from their contracted health plans and the PO pays their contracted PCPs capitation. The PO pays PCP capitation from these monies. The capitation rate is based upon a fixed dollar amount multiplied by the number of members enrolled with the PCP for the month. It may also be based on a percent of the IPA’s capitation revenue for each member. The capitation amount also includes any adjustments for members who are retroactively enrolled or disenrolled with the PCP. The PCP accepts the capitation as payment in full, except for applicable copayments and/or co-insurance, for all capitated-covered services provided by the doctor to the member. Capitation is paid regardless of whether or not the member receives care. Additional compensation for services rendered that are not part of the capitation will be reimbursed according to your contract less any applicable co-payments and/or co-insurance. Please note: Payments for Medicare members are being paid for with Federal Funds, and as such, payments for such services are subject to laws applicable to individuals or entities receiving Federal Funds. The Capitation by Detail Report reads left to right and line-by-line. Below is an explanation of each column: Period Report for the Month Member # Health plan eligibility number Member Name Member’s last name and first name Birth Date Date of Birth Age Member’s age Sex Member’s sex EFFDAT Member’s effective date with the PCP EXPDAT Member’s termination date Period Report for the Month Amount Capitation dollars received for the member S/C Senior member = S / Commercial member = C HMO Parent code for health plan HMO Name Member’s health plan Group Meridian’s internal code Members: Current Current member months PCP xxxx Total member months for which PCP is receiving capitation Eligible Members Current members’ eligible Page 32 Management Services Administrator for Contracting Physician Organizations PART 3: POLICIES AND PROCEDURES Billing Instructions Standard claims forms must be submitted every time services are provided to a member, whether these are payable fee-for-service claims or capitated encounter claims. It is a contractual obligation and a regulatory requirement that the PO must receive these claims/encounters and supply full encounter records to the health plans to which the members belongs. It also assists the practitioner organization in tracking eligibility, capitation, and compensation rates to determine if the capitation is appropriate for the population. Federal and state law requires health plans to report services provided to their members. The encounter is the interaction between the member and the physician. Contractually, the provider is required to report medical services to the PO members monthly. The PO then reports these encounters to the health plans 1. Please use a separate claim form (electronic or paper) for each member visit. 2. All claims must be submitted no later than 90 days from the date of services. Provider shall certify to their best knowledge, information, or belief, as to accuracy, completeness and truthfulness of the encounter data submitted. 3. Please indicate all services provided on the forms along with your charges. 4. Please complete the form entirely and legibly, if not it may be returned. The following information is required to ensure the timely reimbursement of claims: Patients full name Subscriber employer Subscriber number Eligibility number RVS/CPT Code(s) Procedure codes Co-payment amount Date of service(s) Amount billed Referral authorization Name of PO Health plan Member name Member date of birth Member identification number (ID) Diagnosis ICD-9 Code(s) Authorization number EOB from primary insurance carrier (if applicable) Provider name Provider tax ID number Physician name and signature National Provider Identification number Do not bill the member. PO members are not to be billed for authorized covered services, except for allowable co-payments and deductibles. Page 33 Management Services Administrator for Contracting Physician Organizations PART 3: POLICIES AND PROCEDURES Provider Claim & Encounter Submission Complete and forward all claims for processing and payment to the corresponding MED3OOO PO: SeaView IPA C/O MED3OOO 1901 N. Solar Drive, Suite 265 Oxnard, CA 93036 Valley Care IPA C/O MED3OOO 1901 N. Solar Drive, Suite 215 Oxnard, CA 93036 Leisure World Managed Care Medical Group C/O MED3OOO 1901 N. Solar Drive, Suite 270 Oxnard, CA 93036 Valley Care Select IPA C/O MED3OOO 1901 N. Solar Drive, Suite 250 Oxnard, CA 93036 Santa Barbara Select IPA C/O MED3OOO 1901 N. Solar Drive, Suite 200 Oxnard, CA 93036 Pioneer Provider Network C/O MED3OOO 1901 N. Solar Drive, Suite 105 Oxnard, CA 93036 All claims received by MED3OOO are either date stamped or embedded with the date received in the document control number. All claims submitted must be on a standard current CMS 1500 form or UB04 Claim form, if applicable. Claims submitted must be clean claims (Definition: A claim which can be processed as soon as it is received, because it is complete in all aspects, including complete coding, itemization, date of services and billed amounts). The CMS standard for processing clean claims is 60 days. All clean and approved claims that are in the PO’s financial responsibility are processed and paid within sixty (60) calendar days of the stamped receipt date. Claims must be received within 90 days of the date of service. All initial billings received later than 90 days will be denied for untimely filing. If there are extenuating circumstances causing the billing to be delayed, the case will be presented to the PO for resolution. Hospital Claim Submission Claims should be submitted on the UB04 with the following information: Patient’s full name Date of birth Member identification number (ID) Authorization number Diagnosis and diagnostic code (ICD-9) Itemization of services, including procedure codes and date of each service Emergency room reports Admitting physician and name of contracted PO Date of admission and discharge Provider tax ID number Page 34 Management Services Administrator for Contracting Physician Organizations PART 3: POLICIES AND PROCEDURES All claims that are the PO’s financial responsibility are processed and paid within forty-five (45) working days of the stamped receipt date (60 calendar days, if Medicare). Health Plan Claims Responsibility Claims that are the health plan’s financial responsibility are forwarded to the health plan within 2weeks of the date received. Claims Payment Claims are paid on a weekly basis. Checks are dated and mailed out every Friday. An exception occurs when a holiday falls on a Friday – then the checks will be mailed the following business day. CO-PAYMENT/CO-INSURANCE COLLECTION Depending on the benefit plan, members are required to pay and provider is obligated to collect an out-of-pocket charge for professional services called a co-payment. The co-pay amount may vary for PCP and specialists for each service and benefit plan. Co-payments are deducted prior to payment on all fee-for-service claims. Some health plans set a limit on the total cost in co-payments that a member is required to pay during the calendar year. Once the co-payment maximum is reached, no further co-payments are required for services rendered during the remainder of the calendar year. It is the member’s responsibility to keep a record of his/her co-payments and to know when the maximum amount is reached. Some members are also responsible for co-insurance for certain services. Co-insurance refers to the percentage of the contracted fee for which the member is financially responsible. Co-insurance payments are deducted prior to payment on all fee-for-service claims. 1. Verify eligibility and determine if the member has a co-payment and/or co-insurance. The copayment amount is identified on the member’s ID card and the co-insurance, if any, can be identified by contacting the health plan. Note: Co-pay amounts may differ for PCP and specialist office visits. 2. Collect the office visit co-payment and/or co-insurance the day services are rendered. NOTE: A co-payment may not be collected from Medicare members for the influenza or pneumococcal vaccine or for any other preventive care services. 3. For electronic verification of co-payment amounts, see EZ-NET instructions in Chapter 4. DUAL COVERAGE AND COB Sometimes a member is covered by insurance other than the managed care policy. A physician may be entitled to collect additional monies from the member if he/she has other coverage. Health plans also coordinate payment for medical services if a member has dual coverage. When covered services are provided to a member who has dual coverage, the determination of the order in which benefits are payable and the order in which they are recovered is referred to as “coordination of benefits” (COB). Page 35 Management Services Administrator for Contracting Physician Organizations PART 3: POLICIES AND PROCEDURES 1. Instruct the office staff to inquire if the member has other coverage and document the information in member’s chart. 2. Determine which plan is the primary and secondary payor when coordinating benefits between two health plans. There are established rules to determine the primary payor. Please call your Provider Relations Representative if you need assistance. 3. The Birthday Rule is used to establish which health insurance plan is primary for children. The parent whose birthday (month and day only) falls closest to January is considered primary. Example: Father’s Date of Birth is 6/17/54 Mother’s Date of Birth is 2/27/56 The mother’s insurance is considered primary in this case. 4. If the parents are divorced or legally separated, the insurer of the parent who has been ordered by the court to take responsibility for the health care of the child/children is primary. 5. If the parents are divorced or legally separated and the court has awarded joint custody without designating who has responsibility for providing health care of the child/children, the birthday rule applies. When the PO is primary, the secondary plan should be billed for covered services. Do not bill the member, except for the co-payment and/or co-insurance, even if the secondary plans have denied the claim. The PCP has been paid for these services through capitation. Specialists should coordinate COB with the PO. Explanation of Benefits – “EOB” The sample EOB found in Part 2 under Finance reads from left to right and line by line. Below is an explanation of each column: Member # Patient # Claim # Member Name Provider Group # Service Code Service Dates Diag Charged Allowed Discount Deduct Copay/Coins Not Allowed Prepaid Withold Health plan eligibility number Member’s account number on bill Provider group claim reference number Member’s last name and first name Provider name Health plan employer identification number RVS Procedure code Dates of service ICD9 Code Amount billed for the procedure Amount allowed for the procedure Discount amount for procedure Member’s deductible Member’s co-pay to be collected by Provider Disallowed dollar amount N/A Withheld dollar amount based on Provider’s contract Page 36 Management Services Administrator for Contracting Physician Organizations PART 3: POLICIES AND PROCEDURES COB Paid Write Off EP Codes Dollar amount paid by other insurance Dollar amount paid Dollar amount of write off Three digit code for explanation of payment codes (See bottom of EOB for a more detailed explanation of EP Codes) ENCOUNTER DATA SUBMISSION Federal Law requires health plans to report services provided to their members. The encounter is the interaction between the member and the physician. Contractually, the Provider is required to report medical services to the PO monthly for their members. The PO then reports these encounters to the health plans. NOTE: ENCOUNTER FORMS MUST BE COMPLETED FOR ALL SERVICES INCLUDING INPATIENT VISITS. Use the same claim submission process as listed previous. Encounter claims are sent in the same method as other claims to the same locations noted. CALIFORNIA CHILDREN SERVICES The California Children Services (CCS) program provides case management and associated services for physically disabled children under age 21 with CCS-eligible conditions or diagnoses whose families are partially or wholly unable to provide for such services. Some diagnosis usually covered under CCS includes congenital anomalies, scoliosis, cardiac conditions and renal failure. Because CCS will not retroactively authorize services, it is critical that your office immediately contact your PO. The telephone numbers can be found in Part 8 How to Contact Us. If CCS approves the diagnosis, they will be responsible for only the services associated with the approved CCS diagnosis. The PO is responsible for all other care to the member. The program’s working hypothesis is that children with complex, disabling conditions receive improved care and achieve better long-term outcomes when services are provided and coordinated through special care centers and/or certified CCS Providers. For more information on the CCS program, please contact your Provider Relations Representative. Provider Satisfaction Survey MED3OOO conducts a yearly provider satisfaction surveys that measure the effectiveness of managing the IPA’s as well as learn what can be improved upon. The surveys are usually conducted in the first quarter of every year for the prior year’s performance. The data from the surveys are collected and distributed to the QI committees for review and recommendations. Page 37 Management Services Administrator for Contracting Physician Organizations PART 4: PATIENT ACCESS TO CARE AND SERVICE Equitable access to care and service is inherent in the right of every patient. To ensure that access, practitioners are expected to operate their HMO practices according to specific principles and standards. STATEMENT OF PATIENT RIGHTS AND RESPONSIBILITIES Certain rights and responsibilities are conveyed to HMO members by federal and state law, as well as by accreditation organizations. Many of those rights and responsibilities are directly related to UM program activities. The following is the statement of patient rights and responsibilities advocated by our POs, all of which directly or indirectly affect MED3OOO’s and your relationships with your patients: We honor our patients’ rights. All of our patients are entitled to be treated in a manner that respects their rights. We recognize the specific needs of our patients and maintain a mutually respectful relationship with them. This is our commitment to the rights of our patients and individuals other than the patient who have legal responsibility for making health care decisions for the patient. As our patient, you have the right to: 1. Receive health care services regardless of your race, ethnicity, national origin, religion, sex, age, mental or physical disability, sexual orientation, genetic information or source of payment. 2. Receive information about us and our services, affiliated doctors, health care professionals and providers, and patients’ rights and responsibilities, as well as information about your health plan’s coverage for services you may need or are considering. 3. Be treated with respect and recognition of your dignity and right to privacy. 4. Be represented by parents, guardians, family members or other conservators if you are unable to fully participate in treatment decisions. 5. Have information about our contracting physician and provider payments agreements, as well as explanations for any bills you receive for services not covered by us or your health plan. 6. Receive health care services without requiring you to sign an authorization, release, consent or waiver that would permit us to disclose your medical information. We will treat information about you, including information about services and treatment we provide, as confidential according to all current privacy and confidentiality laws. 7. Have round-the-clock access, seven days a week, to your primary care physician or on-call physician when your primary care physician is unavailable. 8. Know the name and qualifications of the physician who has primary responsibility for coordinating your care, and the names, qualifications, and specialties of other physicians, and non-physicians who are involved your care. 9. Have a candid discussion of medically appropriate or necessary treatment options for your condition, regardless of the cost, the extent of benefit coverage or the lack of benefit coverage. To the extent permitted by law, this includes the right to refuse any procedure or Page 38 Management Services Administrator for Contracting Physician Organizations PART 4: PATIENT ACCESS TO CARE AND SERVICE treatment. If you refuse a recommended procedure or treatment, we will explain the effect that may have your health. 10. Actively participate in decisions regarding your health care and treatment plan and receive services at your own expense if we deny coverage. The decision to receive a particular service or treatment rests with you and your treating physician or health care professional. 11. Receive complete information, before receiving care and in terms you can understand, about an illness, proposed course of treatment or procedure, and prospects for recovery, so that you may be well informed when consenting to refusing a course of treatment. This includes being able to request and receive information about how medical treatment decisions are made by physicians, health care professionals or providers and our administrators, and the criteria or guidelines applied when making such decisions an explanation of the cost of the care you will receive and what you will be expected to pay out of your own pocket Except in emergencies, this information will include a description of the procedure or treatment, the medically significant risks involved, any alternate course of treatment or nontreatment and the risks involved in each, and the name of the person who will carry out the procedure or treatment. 12. Receive information about your medications – what they are, how to take them, and possible side effects. 13. Reasonable continuity of care and to know the time, location of appointment, the name of the physician providing care and to be informed of continuing health care requirements following discharge from inpatient or outpatient facilities 14. Be advised if a physician proposes to engage in experimental or investigational procedures affecting their health care or treatment. Patients have the right to refuse to participate in such research projects. 15. Obtain upon request a copy or summary of the Utilization Management Program Description and the Quality Improvement Program Description that we publish annually. 16. Voice complaints or appeals about us or the care we provide. 17. Be informed of rules regarding patient conduct in any of the various settings where you receive health care services as our patient. 18. Complete an advance directive, living will or other instructions concerning your care in the event that in the future you become unable to make those decisions while receiving care through our physicians, health care professionals and providers. 19. Make recommendations about these patients’ rights and responsibilities policies. Our patients share responsibility for their care. In keeping with honoring our patients’ rights, we have expectations of our patients. You have a responsibility to: Page 39 Management Services Administrator for Contracting Physician Organizations PART 4: PATIENT ACCESS TO CARE AND SERVICE 1. Be familiar with the benefits, limitations and exclusions of your health plan coverage. 2. Supply your health care provider with complete and accurate information which is necessary for your care (to the extent possible). 3. Be familiar and comply with our rules for receiving routine, urgent, and emergency care. 4. Contact your primary care physician (or covering physician) for any care that you may needed after that physician’s normal office hours, including on weekends and holidays. 5. Be on time for all appointments and notify the physician’s or other provider’s office as far in advance as possible for appointment cancellation or rescheduling. 6. Obtain an authorized referral form from your primary care physician before making an appointment with a specialist and/or receive any specialty care. 7. Understand their health problems and participate in developing mutually agreed upon treatment goals to the degree possible, and inform your physicians and health care providers if you do not understand the information they give you. 8. Follow treatment plans and instructions for care you have agreed on with your physicians and health care professionals, and report changes in your. 9. Accept your share of financial responsibility for services received while under the care of a physician or while a patient at a facility. 10. Treat your physicians and health care providers and their office staff with respect. 11. Contact our Member Relations Department or your health plan’s Member Services Department if you have questions or need assistance. 12. Respect the rights, property and environment of your physicians and health care providers, their staff and other patients. PATIENT ACCESS STANDARDS Patients have a right to timely access to care and service. Access standards for HMO patients have been standardized by contracting health plans and regulatory agencies. The Department of Managed Health Care (DMHC) recently enacted new regulations concerning time-elapsed access standards for Commercial members that went into effect January 17, 2011. The DMHC is implementing these changes to ensure the health plans provider networks are sufficient to provide accessibility and continuity of covered health care services. The key components of these new DMHC time-elapsed access regulations for providers are summarized on the following page. The prior authorization process is included in the time-elapsed standards. If the appointment type requires prior authorization, obtaining authorization must be completed within the time frame for that visit or service. For example, the time elapsed standard of 15 days for nonurgent referral to a specialist will be measured from the time the PCP requests the authorization to the first appointment date offered to that patient by the specialist. For urgent Page 40 Management Services Administrator for Contracting Physician Organizations PART 4: PATIENT ACCESS TO CARE AND SERVICE appointments that require authorization, the appointment scheduling must be done in concurrence with the prior authorization process. It is expected that plans will monitor compliance with these new access standards via appointment access surveys, after-hours surveys, member and provider satisfaction surveys as well as monitoring member complaints in regards to access. Effective January 17, 2011, California health plans are required to demonstrate compliance with specific standards for scheduling appointments for non-emergency health care services, including health plan and provider standards. The key provisions of these new DMHC time-elapsed access regulations for participating providers are summarized below. APPOINTMENT ACCESS STANDARDS Contracting health plans set patient appointment access standards. Practitioners are monitored for compliance with the following standards: Commercial HMO Programs Appointment Access Standards - Medical ACCESS TYPE STANDARD Access to non-urgent appointments for primary care – regular and routine care (with a PCP) Access to urgent care services (with a PCP) that do not require prior authorization Access to urgent care (specialist and other) services that require prior authorization Within 10 business days of request Access to after-hours care (with a PCP) Ability to contact on-call physician after hours within 30 minutes for urgent issues Appropriate after-hours emergency instructions Within 15 business days of request Access to non-urgent appointments with a specialist In-office wait time for scheduled appointments (PCP and specialist) Access to preventive health services Non-urgent appointments for ancillary services for the diagnosis or treatment of injury, illness or other health condition Wait time not to exceed 48 hours of request Within 96 hours of request Not to exceed 15 minutes Within 30 business days of initial request Within 15 business days of request Appointment Access Standards – Behavioral Health ACCESS TYPE STANDARD Access to non-urgent appointment with physician for routine care Non-urgent appointments with a nonphysician behavioral health care provider Access to urgent care Within 10 business days of request Within 10 business days of request Within 48 hours of request Page 41 Management Services Administrator for Contracting Physician Organizations PART 4: PATIENT ACCESS TO CARE AND SERVICE Access to non-life-threatening emergency care Access to life-threatening emergency care Access to follow-up care after hospitalization for mental illness Within 6 hours of request Immediately Within 7 business days of request (initial visit) Within 30 business days of request (second visit) Also see Part 7 for additional information about monitoring of patient access to appointments. Telephone Response Standard. The telephone call response standard for practitioners’ offices is 30 seconds. 1 Spanish-speaking callers are expected to be directed to an office staff person within no more than an additional 30 seconds. EXCEPTIONS According to the new DMHC regulations, exceptions may be made to these standards as follows: Extending Appointment Waiting Time – The applicable waiting time for a particular appointment may be extended if the referring, treating or triage screening licensed health care provider, acting within the scope of his or her practice and consistent with professionally recognized standards of practice, has determined and noted in the relevant record that a longer waiting time will not have a detrimental impact on the health of the member. Advance Access – A PCP may demonstrate compliance with the established primary care time-elapsed access standards through implementation of standards, processes and systems providing same or next business day appointments from the time an appointment is requested. Advance Scheduling – Preventive care services and periodic follow-up care, including, but not limited to, standing referrals to specialists for chronic conditions, periodic office visits to monitor and treat pregnancy, cardiac or mental health conditions, and laboratory and radiological monitoring for recurrence of disease, may be scheduled in advance consistent with professionally recognized standards of practice as determined by the treating licensed health care provider acting within the scope of his or her practice. APPOINTMENT RESCHEDULING When it is necessary for a provider or a member to reschedule an appointment, the participating provider must promptly reschedule the appointment in a manner that is appropriate for the member’s health care needs, and ensures continuity of care consistent with good professional practice. ASSESSMENT OF COMPLIANCE 1 Behavioral health practitioners are not held to a telephone response standard, because they often are in session when calls are received. Page 42 Management Services Administrator for Contracting Physician Organizations PART 4: PATIENT ACCESS TO CARE AND SERVICE To comply with existing and new regulations, health plans may use several methods to ensure that members have adequate access to providers, including, but not limited to: Conducting provider appointment access surveys to determine the waiting time for appointments, and after-hours surveys to determine the accessibility of emergency and urgently needed services after regular office hours Administering member satisfaction surveys to determine whether members are satisfied with the accessibility of health care services Conducting provider satisfaction surveys Monitoring member grievances about access to care to identify potential trends or problems AFTER-HOURS ACCESS REQUIREMENTS Anyone calling your office after normal office hours must be given appropriate emergency instructions, regardless of whether the caller reaches a live person at your office or a recorded message. The only acceptable instructions are to call 911 or go to the nearest hospital emergency room if the caller believes it is an emergency. The information must be given at the very first opportunity after initial office identification information is given. If the caller does not know if it is an emergency or wishes to speak to the on-call physician, they may be given further instructions following the directions to call 911 or go to the nearest hospital emergency room. The time frame for the physician to contact the member must be less than 4 hours from the initial call. Recorded messages and live attendant responses must accommodate non-English speaking callers. A PCP or covering physician must be available to accept calls from or about their patients 24 hours a day, seven days a week. Recorded messages and live attendants must state the time frame when the physician will return the call. The timeframe must be less than 30 minutes from the patient’s call. PRACTITIONER-PATIENT RELATIONSHIPS We support mutually satisfactory practitioner-patient relationships through the availability of culturally and linguistically appropriate practitioners, equitable balancing of practitioners’ patient caseloads, patients’ continuing care needs, and setting expectations for their relationships with patients. Patients’ Rights to Appropriate Practitioners. As evidenced above, every effort is made to provide HMO patients with practitioners in an array of specialties appropriate for the unique and current composition of both the medical and cultural needs of patients. Page 43 Management Services Administrator for Contracting Physician Organizations PART 4: PATIENT ACCESS TO CARE AND SERVICE Interpreter Services. We encourage physicians to have the ability, either personally or through their office staff, to communicate in many different languages and serve as interpreters when needed, including American Sign Language (ASL). Anyone performing such services should be sufficiently proficient in the patient’s language to properly interpret medical terms and information. You may not charge for any interpreter services, including the use of professionals. If they wish, patients must be permitted to use their own interpreters, including professionals. MED3OOO holds a contract with Life Signs for onsite interpreter services and Language Line Services for linguistic services, but they must be authorized in advance through the UM Department. Once authorized, your office may make the arrangements with Life Signs by calling (213) 550-4210. Their fax number is (213) 550-4205. Language Assistance Program (LAP). For linguistic assistance, we offer the Language Assistance Program (LAP). The following page has the health plan telephone contact information to assist you as needed. MED3OOO also has the ability if need to access the Language Line Services if needed. To utilize this service call the provider services department for assistance. Once authorized, a customer service representative will assist with placing the call to access an interpreter. For the hearing impaired, MED3OOO also uses the California Relay Service available through all telephone companies for patients who wish to contact our offices. The toll-free number is 800-7352929 (TTY) or 888-877-5378 (TTY). Your office also should use the service when needed. Health Plan Name Aetna Anthem Blue Cross Blue Shield of California Plan LAP Threshold Languages (Other than English) English, Spanish Plan Interpreter Access Plan Translation Access (Vital Non-Standard Documents) 1-800-525-3148 1-877-287-0117 Plan Contact For Questions related to Interpreter/Transl ation Nicki Theodorou at 415-645-8264 Megan Rooney at 650-279-6091 Spanish, Chinese (traditional), Vietnamese, Tagalog, Korean 1-888 254-2721 1-888 254-2721 1-800-677-6669 Spanish, Chinese (Traditional), Vietnamese Providers: Over-thephone interpretation 800541-6652, follow IVR menu;On-site interpretation services call 800-541-6652, dial "0" and speak to a Provider Services Agent to arrange for an interpreter. Please fax Language Services Request Form & and document requiring translation to 209-371-5838 email:LanguageAs sistance@ blueshieldca.com or call your Provider Relations representative Additional Resources N/A www.anthem.com/ca Note: Cultural & Linguistic resources are available on the Provider Home Page, under Provider Services blueshieldca.com/pr oviders Page 44 Management Services Administrator for Contracting Physician Organizations PART 4: PATIENT ACCESS TO CARE AND SERVICE CIGNA Health Plan Name Spanish, Traditional Chinese Plan LAP Threshold Languages (Other than English) Oral translations in all languages, print translations Spanish and Chinese Health Net of California, Inc PacifiCare Spanish, Chinese Call 1-800-806-2059. You will need the member’s CIGNA ID number, mbr date of birth and your TAX ID number (or NCPDP for pharmacies) to confirm eligibility and access interpretation services. It is not necessary to arrange for these services in advance. Plan Interpreter Access Call the number on the member's ID card or HMO, PPO, POS, Medicare Supplemental members - (800)-5220088, After hours and weekends- (800)-5464570. The following are 24/7 access numbers: Individual and Family Plan (IFP) members(800)-839-2172. Healthy Families, Healthy Kids or AIM members please call (888)-231-9473. MediCal members- (800) 6756110 1-800-730-7270 Spanish ; 1-800-938-2300 Chinese 1-800-6248822 English (and All Other Languages) Send Word document to translate to Culturalandlingu isticsunit@cigna .com. Protect PHI by encrypting emails. Plan Translation Access (Vital Non-Standard Documents) Translation access questions contact Diana M. Carr, Manager C&L services at 626683-6307 1-800-730-7270 Spanish 1-800938-2300 Chinese 1-800624-8822 English (and All Other Languages) Culturalandlinguist icsunit3@ cigna.com Plan Contact For Questions related to Interpreter/Transl ation (800)-522-0088 Customer Contact Center, after hours and weekends 800546-4570 1-800-730-7270 Spanish 1-800938-2300 Chinese 1-800-624-8822 English (and All Other Languages) Provider Reference Manual Additional Resources www.pacificare.com www.pacificarelatino. com www.pacificareasia.c om Practice Closures. PCP practices are not limited to a set number of HMO patients. In order for a PCP to close his or her practice to new patients, the PCP must complete a special form for review by the Board of Directors of your PO. The Board evaluates whether an increase in patient census and or a significant imbalance in the type of patients customarily seen by that practitioner exists. (Does not apply to SBSIPA) Once a PCP’s practice is closed to new HMO patients, the MED3OOO Contracting Department periodically monitors the PCP’s HMO case load to determine whether the practice should again welcome new patients. Continued Care Following Practitioner Termination. Contracting specialists are required to notify the Contracting Department at least 90 days in advance when terminating their contracts. Page 45 Management Services Administrator for Contracting Physician Organizations PART 4: PATIENT ACCESS TO CARE AND SERVICE This requirement is governed by state and federal law. It is very important you provide that advance notice so that patients who have been under your care can be notified well in advance of the termination effective date of their right to continue to receive care from you. HMO patients whose specialist’s employment or contractual arrangement terminates 2 are entitled by law to continue care with that practitioner after the termination date, provided the terminating practitioner agrees to continue such care under the same contractual terms of the terminating agreement or other terms that may be negotiated for an agreed upon period. The patient must meet specific criteria to qualify for the continuation, which differ somewhat depending upon whether the patient is enrolled in a commercial HMO plan or a senior HMO plan. The duration of the continued care varies. Generally speaking, the continuation may be provided under the following circumstances: Patients who are in active treatment for a serious chronic or acute medical condition Patients who are pregnant Children between birth and 36 months whose care was initiated with the terminating practitioner Patients for whom surgery or another procedure has been authorized prior to the practitioner’s termination in connection with a documented course of treatment and recommended by the terminating practitioner Patients being treated for a terminal illness Patient Requests to Change PCPs and Voluntary Transfers from a PO. HMO patients’ requests to change their chosen PCP are honored in most instances. Exception to this policy may be made if there is evidence that the patient’s request is an attempt to subvert acceptable medical practices, such as compliance with treatment recommendations and plans or prescription-seekers. In such instances, the patient’s health plan is requested to disenroll the patient from the medical group/IPA entirely. Requests from HMO patients for voluntary departures from your PO are directed to the patient’s health plan. Reports of such transfers provided by the health plans are reviewed to identify underlying issues with practitioners or the organization as a whole. Terminating a Physician-Patient Relationship. Practitioners are entitled to set expectations for their relationships with patients, and MED3OOO has the right to maintain viable business relationships with their practitioners’ patients. Patients who do not collaborate with their practitioners or MED3OOO in maintaining a mutually satisfactory relationship are subject to transfer of their affiliation to another practitioner or, in extreme cases, another medical group/IPA. Under certain circumstances, physicians may terminate their relationship with a patient due to behaviors that affect or interfere with treatment objectives. 2 This policy does not apply to specialists whose contractual arrangements are involuntarily terminated for cause, nor to those (a) relocating out of the area and no longer available within a reasonable distance to members or (b) leaving practice. Page 46 Management Services Administrator for Contracting Physician Organizations PART 4: PATIENT ACCESS TO CARE AND SERVICE Consistent with health plan policies, three levels of severity have been established to quantify the degree of the patient’s offenses so that any action taken is appropriate for the offense. For details of the circumstances when disciplinary action may be taken against an HMO patient, please contact the MED3OOO Provider Relations Department (see Part 8). Page 47 Management Services Administrator Administrators forfor Contracting Physician Organizations Buenaventura Medical Group and Care IPA Part 5. Credentialing Program We ensure that HMO patients have access to practitioners who meet high standards and stringent qualifications requirements. CREDENTIALING MANDATES Credentialing requirements for practitioners are governed by state regulations and national accreditation standards. Through MED3OOO’s credentialing and privileging program, patients seeking care through affiliated POs are ensured that they are being treated by practitioners who are highly qualified and meet criteria established for medical professionals in their community. The Credentialing Department ensures reviews each practitioner’s qualifications when he or she first joins the panel of your PO, and every 36 months after that. The Credentialing Department initiates the credentialing and recredentialing process, subject to stringent, mandated time frames. The Credentialing Committee for your PO meets regularly to evaluate the information collected and verified by the Credentialing Department and makes the final decision whether to accept a new practitioner on the panel or continue a practitioner’s privileges for the next 36-month recredentialing period. The credentialing program is mandated and governed by federal and state regulations and accrediting organizations. It is the practitioner’s responsibility to comply with credentialing program requirements provide timely response to requests for information inform the Credentialing Department of any changes in the information previously supplied to the Credentialing Department Failure to notify the Credentialing Department may be grounds for suspension or termination of the practitioner’s privileges and employment or contract. Nondiscrimination. In making decisions about practitioners’ panel privileges, the Credentialing Committee will not consider and shall ensure nondiscrimination of practitioners based on their age, race, ethnic/national identity, gender, sexual orientation or other personal factors not relevant to the practitioner’s professional credentials, or the types of procedures (e.g., abortions) or patients (e.g., Medicaid) in which the practitioner specializes. Practitioner Considerations. Practitioners are entitled to the following considerations in the credentialing/ recredentialing process: You may review information submitted to us by primary sources in support of your application. You may correct erroneous information. Corrections will be reviewed by the Credentialing Department in a timely manner. You must request the correction prior to your records being reviewed by the Credentialing Committee if the information may affect the Committee’s decision regarding your privileges. Upon request, we will inform you of the status of your application prior to the process being finalized. Page 48 Management Services Administrator Administrators forfor Contracting Physician Organizations Buenaventura Medical Group and Care IPA Part 5. Credentialing Program LICENSURE AND DRUG ENFORCEMENT ADMINISTRATION (DEA)/CONTROLLED DANGEROUS SUBSTANCES (CDS) CERTIFICATION Practitioners are responsible for maintaining a current physician and surgeon’s license to practice in the State of California. If the practitioner is required to have a DEA or CDS certificate, it also must be continuously current. Failure to maintain a current license and DEA/CDS certificate is grounds for automatic termination of your contract. You must provide a copy of your current license and DEA certificate after each renewal. BOARD CERTIFICATION Practitioners whose specialties are subject to board certification are required to obtain their certification at the earliest possible opportunity if not certified prior to joining the practitioner panel. Board certification will be temporarily waived to permit the practitioner time to attain certification. It is your responsibility to notify the Credentialing Department when certification has been awarded. MALPRACTICE LIABILITY COVERAGE At all times, practitioners must have current malpractice insurance in amounts established for the practitioner’s specialty. Opened, pending or finalized malpractice actions must be disclosed on the application and fall within current guidelines established by the Credentialing Committee for allowing panel privileges. Any new cases, judgments or settlements occurring after initially credentialed or between any recredentialing review period must be reported to the Credentialing Department within fourteen (14) calendar days. OTHER CREDENTIALING REQUIREMENTS Other requirements for practitioners include the following: Certification by the specialty board applicable for the practitioner’s primary practice type, if such certification is available Local hospital privileges if the practitioner will see or treat hospitalized patients and is not exempt from that requirement due to the nature of his or her practice Complete and submit a signed, approved application, meet the credentialing and privileging criteria established by the Credentialing Committee and be granted panel privileges by the Credentialing Committee Sign and agree to comply with the provisions of their employment or contracting agreement, which specify » adherence to MED3OOO policies and procedures » abiding by MED3OOO’s utilization management program and quality improvement program requirements, including patient rights and access, referral authorization processes, standards for practice sites, medical record-keeping practices and as described in this document Page 49 Management Services Administrator Administrators forfor Contracting Physician Organizations Buenaventura Medical Group and Care IPA Part 5. Credentialing Program AVAILABILITY OF CREDENTIALING PROGRAM DESCRIPTION The scope of the credentialing program is described in the complete Credentialing Program Description. It is available upon request by calling the Provider Relations Department (see Part 8). The policies and procedures established to support the UM program are viewable on the network shared server. CREDENTIALING INFORMATION CONTACT Questions about the credentialing requirements and related credentialing/recredentialing policies and time frames should be directed to the Credentialing Department (see Part 8). Page 50 Management Services Administrator for Contracting Physician Organizations Part 6. Utilization Management Program In its capacity as administrator for contracting POs, MED3OOO conducts a comprehensive utilization management (UM) program for patients enrolled in HMO health plans. PO panel practitioners are contractually required to participate in and comply with UM program activities. UM PROGRAM RESPONSIBILITY Your PO delegates responsibility for meeting UM program requirements specified by contracting health plans to MED3OOO. Our UM Department is responsible for UM program activities, the scope of which currently extends to the customary array of utilization management/utilization review and health management services now accepted as integral to managed health care in the United States. The Utilization Management Committees, which report to the respective Boards of Directors of contracting PO, are the governing bodies for the UM program. DECISION-MAKING POLICIES The UM program is consistent with the administration requirements and clinical standards established by managed care organizations in the State of California to ensure compliance with state and federal regulations. It is designed to ensure that HMO patients receive the quality health care they deserve and expect while preserving the financial integrity of our contracting POs. The cornerstones of our UM program are uniformity, consistency and timeliness. The program relies on established standardized decision-making criteria and guidelines that are based on sound medical evidence. UM Department clinical staff reviews them regularly to be certain that they reflect the needs of our patients. We also make sure that our clinical decision-makers — physicians, nurses and other health professionals — consistently apply the criteria for all patients. Contracting health plans routinely monitor our UM review activities for compliance with established requirements. Failure to comply with requirements may jeopardize your PO’s contractual arrangements with HMO health plans. The UM Department makes these promises to you and your patients when it comes to making utilization management decisions about health care services: Only board certified physicians and qualified health professionals are permitted to make utilization management decisions about the health care services our patients receive. Utilization management decisions are based solely on the appropriateness of care and service and each patient’s own health plan benefits. We do not reward our decision-makers for denials of coverage, services or care. We do not offer our decision-makers any financial incentives to limit, restrict or discourage use of health care services. Case reviews are conducted to determine whether the services are covered by the member’s plan of benefits if covered, the services meet the criteria and guidelines for medical necessity and/or appropriateness of clinical or medical services and meet any applicable conditions of coverage Page 51 Management Services Administrator for Contracting Physician Organizations Part 6. Utilization Management Program Review requests are screened to verify the patient’s eligibility for HMO health plan benefits and identify the UM requirements applicable for that patient. Then, depending upon the applicable requirements for the services being reviewed, the request is either authorized, if further review is not required, or it is directed to a senior clinician for evaluation. Any case having the potential for denial is forwarded to the Medical Director for your PO or a specialty-specific practitioner designee for final determination. AVAILABILITY OF UTILIZATION MANAGEMENT PROGRAM DESCRIPTION The scope of the UM program is described in the complete Utilization Management Program Description. It is available upon request by calling the Provider Relations Department (see Part 8). The policies and procedures established to support the UM program are viewable on the network shared server. The following information summarizes the UM program. UM DEPARTMENT BUSINESS HOURS The UM Department is your primary source for UM program information and requirements. Daily UM Department business hours are 8:00 a.m. – 5:00 p.m., Monday through Friday. We observe the customary national holidays, when our offices are closed for business. The UM Department staff makes outbound calls and receives incoming calls regarding UM activities only during those hours. If you have a hospital, skilled nursing facility, rehabilitation or home health care case, a Case Manager may provide you with a number for direct contact. After normal business hours, on weekends and holidays, you may fax UM-related inquiries issues to the Provider Relations Department (see Part 8). 1 Practitioners who are connected to MED3OOO’s computer system may also submit authorization requests and view the status of a request electronically. Inquiries will be responded to at the earliest opportunity on the next business day. REQUIREMENTS FOR SPECIALTY CARE, ANCILLARY SERVICE AND INPATIENT REFERRALS HMO members must meet their health plan’s UM requirements in order for the services to be eligible for coverage. As their physician, you are responsible for initiating the UM process on your HMO patients’ behalf. Services Subject to Review. The UM Department is delegated the authority by contracting health plans to review and authorize their HMO patient referrals for elective inpatient (acute, skilled nursing and rehab facility) care, most specialty care (including behavioral health services, but only for members of senior HMO health plans), and most ancillary services. The requirements extend to services to be provided by contracting and affiliated practitioners/providers, as well as by noncontracting practitioners/providers when the needed services are not available from within MED3OOO’s contracting PO practitioner panels or affiliated practitioners/ providers. PCPs must obtain authorization prior to referring their patients to contracting specialists for elective services. Contracting specialists are required to obtain authorization for continuing care prior to services beyond those originally authorized being rendered. 1 Patients may call the Member Services Department (see Part 8). SeaView IPA practitioners may email their UM inquiries to the Member Services Department (see Part 8). Page 52 Management Services Administrator for Contracting Physician Organizations Part 6. Utilization Management Program Services Not Subject to Review. Certain services are not subject to review, depending upon the type of HMO health plan in which the patient is enrolled. As a general rule, treating physicians may order the services listed below directly from the designated provider for their HMO patients. Services received by HMO plan members under conditions other than those indicated below that have not been authorized in advance usually are not eligible for coverage, regardless of whether they are received from a practitioner, provider or vendor having a contractual arrangement with your PO. Primary Care Services. Services rendered for HMO patients within the primary care practice setting are not subject to review. The PCP determines when services are required outside the primary care setting and requests the necessary authorizations from the UM Department. Emergency Services. Emergency services generally do not require prior authorization; however, emergency facility services that do not conform to emergency services/conditions guidelines established by the State of California Health and Safety Code (for commercial and state-funded health plan members) or by the Center for Medicare-Medicaid Services (for senior health plan members), as applicable for the patient’s age group, are evaluated in the claims payment process. They must be forwarded to the UM Department for postservice review by the Medical Director. Emergency medical and behavioral health services that are necessary to screen and stabilize a member will not be denied. Any services not authorized by the patient’s PCP/treating physician that do not meet emergency criteria are subject to denial of the claim. Decisions are made after obtaining all necessary information, such as an ER summary or medical record, regarding the presenting symptoms and the discharge diagnosis. Diagnostic and Routine Preventive Screening Lab Tests. Prior authorization is not required for lab services ordered by an authorized practitioner to (1) diagnose or monitor an HMO member patient’s condition, or (2) when ordered in connection with age-appropriate routine preventive screening services, such as FDA-approved cervical cancer screening tests (i.e., Pap smears and thin prep tests). Coverage for lab services is subject to the patient’s plan of benefits, and MCO's are responsible for complying with any legislation or regulations pertaining to such services. Radiology/Imaging Services. Requests for advanced imagings are directed by the treating/ordering practitioner to the contracting imaging vendor. (SVIPA & VCIPA Only) The vendor/facility evaluates the request against agreed upon preservice review guidelines. Those falling outside the guidelines for authorization by the vendor are forwarded to the UM Department. If the request is for imaging services not subject to preservice review by the UM Department, the vendor proceeds with scheduling and providing the requested imaging. Exception: Requests for use of non-contracting imaging vendors and facilities must be submitted to the UM Department for review. OB/G Gyn and Well-Woman Services. HMO patients are not required to obtain authorization for routine office-based OB/Gyn care, including annual well-woman preventive care exams. However, they must receive the services from an OB/Gyn specialist on the practitioner panel for your PO. Surgical procedures, hospital admission, or other complex services require prior authorization. Page 53 Management Services Administrator for Contracting Physician Organizations Part 6. Utilization Management Program Behavioral Health Services. Behavioral health services for commercial HMO health plan members typically are not included in the range of services for which your PO is financially responsible, as they are provided under separate “carve-out” arrangements with behavioral health provider organizations. Direct Referral Specialists. Selected PCPs may refer their patients to some contracting specialists without prior authorization. PCPs eligible for direct referrals are selected based on their history of compliance with review requirements and protocols. The specialties to which they may refer must be approved by the UM Committee and Board of Directors and/or have capitation agreements. Direct referral utilization is monitored through post service review. Members of Blue Cross of California HMO health plan who reside in Santa Barbara County are entitled to be directly referred to specialists contracting with SBSIPA without prior authorization. Services Coordinated Through Patients’ Health Plans. A range of services are coordinated by the UM Department through the affected patient’s health plan, which is responsible for determining a member’s eligibility for the services and interfacing with the UM Department, based on the outcome of the health plan’s evaluations. When you submit an authorization request for such services, the UM Department must await the health plan’s determination, so please allow ample time for the request to be processed. The following types of services are subject to health plan review of your authorization request: Cancer clinical trials Experimental or investigational treatments Organ transplantations The patient’s health plan also may become involved in the following types of cases: Requests for second opinions from specialists who are not affiliated with your PO (the patient has the option of selecting one who has a contract with the patient’s health plan) Services of practitioners and providers outside the local service area that are medically necessary due to an emergency Healthy Families programs — The UM Department does not review some services for HMO patients from birth to age 21 who are enrolled in a contracting health plan’s Healthy Families HMO benefit plan. Requests for medical services for children enrolled in a Healthy Families HMO due to conditions falling into these general categories are referred to and managed by the State of California Children’s Services (CCS) Department: Infectious diseases Neoplasms Endocrine, nutritional and metabolic diseases and immune disorders Medical therapy program conditions Mental disorders and mental retardation Diseases of: » nervous system » blood and blood-forming organs » circulatory system » eye » ear and mastoid process » respiratory system Page 54 Management Services Administrator for Contracting Physician Organizations Part 6. Utilization Management Program » digestive system » genitourinary system » musculoskeletal system and connective tissue Congenital anomalies Accidents, poisonings and immunization reactions Specific referral criteria are issued by CCS and maintained in the UM Department. INFORMATION REQUIRED FOR CASE REVIEWS Requests for review must be submitted to the UM Department by the patient’s PCP or treating practitioner on the appropriate form. The forms can be found starting on page 68 or you may call providers services for assistance in getting the form. Request forms must be fully completed to include the following minimum data elements or be accompanied by a supplemental sheet with relevant information, as applicable for the case submitted for review: Minimum Information Required for Case Reviews Category Patient Information Minimum Data Elements Name Sex Date of birth Health plan Primary diagnosis Surgical assistant requirements Secondary diagnosis Anesthesia requirements Tertiary diagnosis Proposed admission or service date(s) Multiaxial diagnosis Proposed procedure/service date(s) Proposed procedure(s), treatment(s) or service(s) Proposed length of stay and frequency/ duration of services Clinical Information Sufficient to support the medical necessity/ appropriateness and level of service proposed Contact person for detailed clinical information Facility Information Name Type (inpatient, outpatient, special unit, SNF, rehab, office/clinic, home health agency, etc.) Diagnosis/Treatment Information Location Minimum Information Required for Case Reviews Category Concurrent (Continuing Care) Information) For Admissions to Facilities Other Than Minimum Data Elements Additional days/services/procedures proposed, with frequency and duration of services Reasons for extension, including clinical information sufficient to support medical necessity/appropriateness and level of service proposed Diagnosis (same/changed) Discharge plans History of present illness Prognosis Page 55 Management Services Administrator for Contracting Physician Organizations Part 6. Utilization Management Program Category Minimum Data Elements Acute Medical/Surgical Hospitals, Include Current special assessment reports For Special Situations: Additional information sufficient to support health insurance carrier/plan requirements, such as: Patient treatment plan and goals • Second opinion information • Information in support of the need for a procedure, drug, device or other therapy Treatment plans must be appropriate, time-specific and updated periodically. INITIATING A CASE REVIEW 1. Fax review requests directly to the MED3OOO UM Department (see Part 8. UM-related inquiries, including referral requests, are received and outbound responses provided only during normal business hours of 8:00 a.m. – 5:00 p.m., weekdays and non-holidays only. If the services are beyond the scope of those customarily screened and authorized by UM Department non-clinical staff, Review Nurse will further evaluate the request. If additional information is needed, the Review Nurse will contact you and provide a direct phone or fax number. See Part 8 for phone and fax numbers. 2. Allow the UM Department sufficient time to perform a fair review of the requested services. Federal and state regulations mandate the time frames for completing a review. Referral review requirements and response time frames are mandated by federal and state regulations and accreditation regulations. The UM Department strives to exceed those standards and makes every effort to complete reviews in advance of the required timeframe. 3. Submit complete records supporting the need for the referral and promptly respond to requests from the UM Department for additional information when needed. If requested information is not supplied, the request is at risk for being denied and may need to be resubmitted to be given further consideration. Page 56 Management Services Administrator for Contracting Physician Organizations Part 6. Utilization Management Program REPORTING EMERGENCY INPATIENT ADMISSIONS SeaView IPA patient hospital admissions following emergency room treatment must be coordinated through the inpatient physician (hospitalist) on duty at the admitting facility. Valley Care IPA patient hospital admissions may be coordinated through the hospitalist or managed directly by the PCP. The facility will notify the UM Department on the next business day. Santa Barbara Select IPA patient hospital admissions may be coordinated through the hospitalist or managed directly by the PCP. The facility will notify the UM Department on the next business day. Leisure World Managed Care patient hospital admissions should be coordinated by the hospitalist or managed directly by the PCP. Pioneer Provider Network patient hospital admissions must be coordinated by the hospitalist at the primary admitting hospital(s). The UM Department will follow up on the admission on the next business day. At the beginning of the next business day, the Case Manager checks with the facility’s admitting office to identify any patients admitted in the off-hour period and performs an evaluation of the patient’s need for continuing inpatient care. If the patient can be discharged, the Case Manager issues the appropriate denial notifications. You will be contacted if additional information is needed. When a patient is admitted to a facility following emergency treatment, continued care will be authorized until the treating practitioner believes that the member may be safely discharged, a treatment plan has been agreed upon with the treating practitioner, and both the treating practitioner and the member (or member’s representative) have been given 24 hours’ advance notice that coverage will be discontinued. For senior HMO health plan members, the authorization will be provided within one hour of receiving a request from a non-contracting facility. Out-of-Area Emergency Admissions. To accommodate post-stabilization care needs subsequent to emergency treatment by out-of-area/non-contracting hospitals, the facilities customarily attempt to contact the patient’s PCP/treating physician or behavioral health practitioner, as applicable. Post-Emergency Stabilization Services Following Discharge. PCPs and treating physicians have the authority to order post-emergency stabilization services from contracting ancillary providers/suppliers, such as skilled nursing facilities, home health agencies and medical suppliers. Such services ordered by the PCP/treating practitioner will be authorized by the Case Manager on the next business day, and the patient’s need for continuing services will be evaluated. AUTHORIZED REFERRAL PROVIDERS As a matter of policy, referrals are authorized only to practitioners and providers affiliated with your PO. Your PO’s contracting provider network also extends to tertiary facilities and major medical centers designated by contracting health plans for use by their members when needed services are not available locally. Page 57 Management Services Administrator for Contracting Physician Organizations Part 6. Utilization Management Program Use of Non-Contracting Providers. Your PO accommodates the need for services not available within their networks of affiliated practitioners and providers. For commercial members, medically necessary use of non-contracting providers is permitted when a contracting practitioner or provider capable of providing the needed services is not available through a contracting practitioner/provider. These services must be authorized and a special agreement will be executed with the practitioner/provider. For senior members, a special agreement is not required if the practitioner/provider is Medicare certified. However, authorization may be required. If the needed services are not available in-network, the Review Nurse or Case Manager will locate a non-contracting practitioner/provider appropriate for the patient. AUTHORIZATION PROBLEMS Practitioners are entitled to the following considerations in the review process: 1. If you have not received a response within the time frames indicated above, you may call the Provider Relations Department (see Part 8) to request a status. 1 If you are connected to MED3OOO’s computerized referral system, you may obtain status information online. 2. You may discuss a case submitted for review and denial decisions with your PO’s Medical Director or other physician who made the determination. If you can provide information that you believe was not considered at the time a denied request was reviewed, and an appeal has not yet been filed, the case will be given immediate reconsideration. 3. All denials are subject to appeal. Appeals must be directed to the patient’s health plan, as required by our contractual arrangements with them. You may file the appeal on behalf of your patient and encourage you to do so if your input will help with the decision. The health plan will notify us and direct a response within a time frame appropriate for the patient’s medical needs. UM DECISION-MAKING CRITERIA AND GUIDELINES The UM Department does not conduct a scripted clinical screening. When evaluating a case, UM Review Nurses, Case Managers and Physician Reviewers are required to consider information pertinent to the individual’s clinical/medical needs, including the treating/ordering practitioner/provider’s recommendation. They also must observe the terms of coverage under the patient’s specific benefit plan. They further must base their review determinations on established clinical criteria recognized within the medical community-at-large as appropriate for the medical specialty or other clinical discipline relevant to the services subject to the review. The standardized decision-making guidelines and criteria currently in use include the following resources, as applicable for the requested services: Standard reference compendia, including but not limited to » 1 InterQual Level of Care Acute Criteria® This number is dedicated to practitioner and provider inquiries. Patients may call the Member Services Department for information and assistance (see Part 8). Page 58 Management Services Administrator for Contracting Physician Organizations Part 6. Utilization Management Program » InterQual Care Planning Specialty Referral Criteria® » InterQual Care Planning Procedures Criteria® » Complete Guide to Medicare Coverage Issues Medical policy or conditions of coverage guidelines issued by the patient’s health plan Other established clinical practice guidelines and criteria that are » evidence-based » commonly applied by the medical specialty or other clinical discipline appropriate for the services subject to review Examples include » practice guidelines or criteria from the federal government » practice guidelines or criteria from nationally recognized professional associations or societies that have been developed by a peer review or consensus process » the American Hospital Formulary Service-Drug Information » American Medical Association Clinical Practice Guidelines » the American Medical Association Drug Evaluation » American Psychiatric Association Practice Guidelines » American Psychological Association Practice Guidelines » the American Dental Association Accepted Dental Therapeutics » the United States Pharmacopoeia-Drug Information » American Physical Therapy Association Guide to Physical Therapist Practice » Guidelines for Chiropractic Quality Assurance and Practice Parameters, Proceedings of the Mercy Center Consensus Conference » Clinical Practice Guideline No. 1, Vertebral Subluxation in Chiropractic Practice Criteria and guidelines developed and approved by your based on current standards of practice within our medical community for the requested services In the absence of consistent guidelines, a Reviewer’s medical judgment based on professional experience may be considered as definitive. Standardized guidelines are evaluated annually to ensure that the most current versions appropriate for PO patients are used in the UM process. Application of Criteria and Guidelines by Reviewers. Information sources for review decisionmaking are monitored and evaluated annually by your PO’s UM Committee. Reviewers are informed Page 59 Management Services Administrator for Contracting Physician Organizations Part 6. Utilization Management Program of requirements for considering appropriate information and applying relevant medical and scientific evidence in their case evaluations and are supplied with information and documents pertinent to the individual’s medical needs. Their written opinions are evaluated to ensure that that they include citation of the specific clinical criteria applied in the review. Review clinicians receive training in requirements for applying pertinent clinical criteria and providing appropriately documented written opinions. Your PO’s Medical Director also assists individuals needing access to the latest medical research findings, studies, practice, guidelines and other clinical reference materials when requested in order to complete their reviews. CASE MANAGEMENT PROGRAMS The UM Department also offers a spectrum of specialized health management services tailored to our patients’ medical needs. The case management program is geared to patients who have complex or specialized treatment needs. Whether for a long-term chronic condition or for an illness patients will recover from, these programs focus on the best possible health outcome for patients. The Case Manager coordinates multiple health care services, sees that patients have the information they need to effectively manage their illness or condition, and through telephone contact follows their progress to be sure that their treatment plan is working for them. They also work with the patient’s health plan so that their benefits are used efficiently and to the patients’ best advantage. Contact the Provider Relations Department if you wish to refer a patient who may benefit from individualized case management of their services. If you already have a patient being actively case managed, you may contact the Case Manager. Page 60 Management Services Administrator for Contracting Physician Organizations Part 7. Quality Improvement Program The quality improvement (QI) program is an ongoing, comprehensive and integrated program. It objectively and systematically monitors and continuously evaluates all aspects of the delivery of health care services. Its purpose is to identify opportunities to improve care and service, as well as resolve identified problems in the delivery of care and service in all departments. Assessment of standards, objectives and outcomes provide an ongoing basis upon which patient care related issues are evaluated, upgraded and improved for the benefit of the member, practitioners and staff. The PO I Committees, which report to their respective Board of Directors, are the governing body for the QI program. PO practitioners are contractually required to participate in and cooperate with QI program activities. Many of those activities focus on improving the operational aspects of delivering health care services. Operations activities are monitored continuously and systematically to assess corporatewide and individual performance and to identify areas for focal performance improvement. AVAILABILITY OF QUALITY IMPROVEMENT PROGRAM DESCRIPTION The scope of the QI program is described in your PO’s Quality Improvement Program Description. It is available upon request. If you are connected to MED3OOO’s computer system, the policies and procedures established to support the QI program are viewable on the network shared server. For further information, contact the Provider Relations Department (see Part 8). 1 The following summarizes the QI program. PHYSICIAN SUPERVISION OF NON-PHYSICIAN PRACTITIONERS California state law assigns physicians responsibility for direct oversight of the following nonphysician practitioners in their practice sites: Physician assistants (PAs) Nurse practitioners (NPs, RNPs, CRNPs) The Credentialing Department monitors the licenses of physician assistants and nurse practitioners practicing in contracting physicians’ offices. Contracting physicians who permit physician assistants or nurse practitioners to treat their managed care patients are responsible for ensuring that the practitioner’s license is current. Physicians must ensure that non-physician practitioners confine their treatment of your PO patients to services that fall within the scope of their license. Medical records documentation must reflect that all services falling outside the scope of a non-physician practitioner’s license were performed by a physician. For example, if the report of a physician’s services is prepared by a non-physician practitioner, it must be initialed by the physician. Accurate documentation ensures that the procedure is reimbursable and protects practitioners from claims that provided services are outside the scope of the practitioner’s license. Other supervision requirements for non-physician practitioners include the following: 1 This number is dedicated to practitioner and provider inquiries. Patients may call the Member Services Department (see Part 8). Page 61 Management Services Administrator for Contracting Physician Organizations Part 7. Quality Improvement Program The supervising physician has continuing responsibility for all medical services provided by the health professional under his or her supervision. Note: Effective 7/1/01, Californialicensed physicians can supervise a PA without MBC approval. The exception is those physicians who are expressly prohibited by the Medical Board of California (MBC) from supervising a PA. [CCR, Title 16-Division 13.8-Physician Assistant Practice Act-Section 3502; Board of Registered Nursing, Nursing Practice Act, Rules and Regulations, Article 8] PAs may perform medical services set forth by the regulations of the MBC when the services are rendered under the appropriate supervision of a licensed physician. [CCR Title 16: Division 13.8-Physician Assistant Practice Act-Section 3502] » At all times, the supervising physician must be physically or electronically available to the PA for consultation, except in emergency situations. » The supervising physician must not supervise more than two PAs at one time. Prescribing of drugs and/or devices by NPs must be in accordance with standardized procedures or protocols developed by the NP and supervising physician. [Board of Registered Nursing, Nursing Practice Act, Rules and Regulations, Article 8] » The supervising physician is not required to be physically present; availability by telephone is adequate. » The supervising one time. physician must not supervise more than four NPs at MEDICAL RECORDS REQUIREMENTS AND AUDITS Accurate medical record documentation is essential to your PO’s ongoing success, from both quality of care and financial perspectives. QI program activities in connection with medical recordkeeping that require practitioner participation or cooperation include the following: 1 Compliance with standardized recordkeeping protocols ensures the safety of patients, and data supporting such compliance are tied to financial incentives proffered by contracting health plans, as well as the stability of contractual arrangements with those health plans. The QI Department periodically audits individual practitioner’s recordkeeping practices. Any deficiencies are reported to the practitioner and the applicable PO’s QI Committee. Serious deficiencies require the practitioner to submit a corrective action plan, and compliance with the protocols will be re-evaluated at later date. For a copy of the medical record audit standards, call the Provider Relations Department (see Part 8). Timely response to health plan inquiries and patient complaints/grievances or appeals is critical. When the QI Department requests a medical record for such purposes, response time is closely monitored by the requesting health plan. If a patient’s medical record is in your office when it is needed, it must be promptly forwarded to the QI Department 1. The QI Department will return the record as soon as possible. Only a copy of the portion of the record relevant to the issue of the case will be required. The copy will not be returned. Page 62 Management Services Administrator for Contracting Physician Organizations Part 7. Quality Improvement Program Data for key statewide quality of care/quality of service measurements are collected annually by contracting health plans and reported to an external vendor for analysis and ranking of your PO’s performance in comparison to other medical groups and IPAs throughout the state. In some cases, the results may be published for public inspection as a guide for health plan purchasers. Consequently, favorable data have a direct positive impact on your PO’s financial standing. The underlying principles for these measurements are (1) timely delivery of preventive services, (2) appropriate management of high-risk conditions, and (3) appropriate documentation of services rendered. You PO’s QI Committee reviews the results of the above activities and determines ways to improve overall PO and individual practitioner performance. FACILITY OPERATIONS REQUIREMENTS AND AUDITS The QI Department assesses primary care, OB/GYN and some behavioral health practitioners’ facilities to ensure compliance with essential premises safety, staff supervision, equipment and patient access protocols. Contracts with health plans require that such assessments be performed at regular intervals. Any deficiencies at practice sites are reported to the practitioner and the PO’s QI Committee. Serious deficiencies require the site manager or practitioner to submit a corrective action plan, and compliance with the protocols will be re-evaluated at later date. For a copy of the facility audit standards, call the Provider Relations Department (see Part 8 How to Contact Us). ACCESS AUDIT Appointment access standards are set by contracting health plans (see Part 4 Patient Access to Care and Service). Timely access to needed medical services is monitored through various mechanisms, including appointment access data, facility operations audits, patient complaints and grievances, quality issue reports, patient satisfaction surveys and patient access audits. Results are used to identify individual practitioner or panel-wide access issues and develop ways to improve performance. The PO QI Committees determine any needed actions. Page 63 Management Services Administrator for Contracting Physician Organizations Part 8. How to Contact Us If you have questions about requirements or procedures, or need assistance, please contact the appropriate MED3OOO department, as indicated below: SeaView IPA (805) 604-3325 (877) 311-5411 Valley Care IPA (805) 604-3308 (877) 299-5599 Valley Care Select IPA (805) 604-3308 (877) 299-5599 Santa Barbara Select IPA (805) 278-6823 (800) 705-0831 Leisure World MCMG (805) 604-3317 (800) 415-4455 Pioneer Provider Network (805) 988-5164 (800) 720-2323 Member Services Email: [email protected] Provider Relations Email: [email protected] Page 64 Management Services Administrator for Contracting Physician Organizations Part 9. Appendix WAIVER FORM I have enrolled in ____________ health plan. (Health plan name) I understand my eligibility status does not appear on the current eligibility list provided to _____________________________. (Provider name) If eligibility is not established in the next 60 days, I assume full responsibility for all charges incurred by dependents and myself. ______________ Date Patient Full Name Patient’s signature Subscriber’s Full Name Employer Date of Birth Employer Telephone Number Subscriber’s Social Security Number Witness Verification of Eligibility was requested by: Provider Verification given on: (Date) Name of health plan representative Dependents covered: Temporary Authorization Number Effective Date $ Co-Payment Amount Page 65 Management Services Administrator for Contracting Physician Organizations Part 9. Appendix Sample Member Introduction Letter for PCPs Dear Member, We welcome you to our office and are pleased you have chosen us as your PCP. Because health plans (managed care organizations) are different from other forms of health insurance, we have found it helpful to provide some guides as to the best use of your plan. We are members of a Provider Group, which contracts with health plans to provide Provider services within the plan benefits. As such, we act as the "PCP". There are some basic rules governing the care, which will prevent any misunderstanding of how this system works for you. We operate on an appointment system, so please call if you need medical care. You should be able to be seen in a timely manner. Please call in advance for routine appointments. If you are ill, we may be able to advise you over the telephone, or we may need to see you. Please be prepared to come to the office whenever we can schedule you. It may also be that you may have to wait a day unless your illness is severe and/or quite acute. We will do our best to accommodate you promptly when you call. Be sure to make it clear to the nurse or receptionist you have an acute problem if you think your need for medical care is urgent. There are Providers on call 24 hours a day, every day of the year. It may not be your own doctor, but it will be one of` your doctor's associates. If you should require medical services when the office is closed, please call our office immediately, and the doctor on call will advise you on the best course of action. It is of utmost importance you call before going to the emergency room, whenever possible. We provide primary care services, which include all basic medical care, including well woman examinations. Specialty care, such as surgery requires a referral from your PCP when medically indicated. If a member decides to go to a specialist without an approved referral, it may be the member’s responsibility to pay the Provider for the service. If your plan has a co-payment requirement, you must pay this fee at the time service is provided. Specialty Providers must obtain authorization for additional services by contacting your PCP (this could include, but is not limited to, services such as laboratory, x-ray, surgical procedures, follow-up visits, etc.). Failure to obtain an authorization could result in a denial of reimbursement to the provider of service. We understand many of our members have seen Specialty Providers in the past as a regular source of care. However, unless it is medically indicated and authorized, routine visits to those Specialty Providers may not be covered by your plan. Page 66 Management Services Administrator for Contracting Physician Organizations Part 9. Appendix We also understand this is a change for many people who have been accustomed to choosing their own doctor for a particular problem. However, in order to provide cost effective coverage without large out of pocket costs to you, your plan requires your PCP direct your care. We encourage you to discuss these matters with us so we may address your expectations. Additionally, please remember the decision making is based only on appropriateness of care and service and the providers in our group or other individuals conducting utilization review for denials of coverage or services are not compensated to encourage barriers to care or service. Also, financial incentives for the decision makers do not encourage denials of coverage or service, nor are incentives used to reward inappropriate restriction of care as special concern must be kept in mind regarding the risk associated with under-utilization. According to your health plan agreement, if you have other insurance coverage, you are obligated to inform us so we may coordinate the benefits. We feel this is an excellent plan, which provides you with high quality, affordable medical care. Should you require such services, we have available to you the finest specialty and sub-specialty Providers in our community. We encourage your participation in making decisions regarding your medical care, and your active participation in disease prevention and wellness. It is your right and responsibility to access regular physical examinations and preventive services such as health screening tests and immunizations, and to participate in health education and health maintenance activities. With your cooperation, we are committed to provide you with quality health care. If you have any questions regarding the benefits to which you are entitled, please refer to your plan benefits booklet, or call your health plan directly. Sincerely, Practitioner Organization (SeaView IPA, Valley Care IPA, Santa Barbara Select IPA, Leisure World Managed Care Medical Group, or Pioneer Provider Network) Page 67 DATE REC’D STAMP URGENT ROUTINE REFERRAL AUTHORIZATION FORM SeaView IPA 1901 N. Solar Drive, Suite 265 Oxnard, CA 93036 Provider Services: (805) 604-3325 Member Services: (805) 988-5188 Fax: (805) 988-5162 PATIENT INFORMATION Patient Name (Last, First, MI): Sex M Address: Health Plan Name: PRIOR AUTHORIZATION REQUEST AND/OR DIRECT REFERRAL FOR SPECIALIST ICD-9 Code(s): __________ CPT Code(s): __________ Zip Code: PCP Phone Number: PCP: Member Phone Number: Plan Code: Other Insurance? Name: Yes Date Last Seen: No Diagnosis: __________ __________ __________ __________ __________ Specify Proc/Svc: __________ Frequency/Duration Requested: ________________________________________ (Chronic/exacerbated acute conditions can be >2 visits/60 days with treatment plan) Prior Treatment/Relevant Diagnostic Testing: Hospital/Facility: Expected Date of Admission: Assistant Surgeon: Inpatient/Outpatient: ____________________________________________ Physician Name (please print) Requested Service (s): DIRECT REFERRAL (FOR PCP USE ONLY) Member ID#: City / ST: Service to be provided by: ____________________________________________ _ Physician Signature ICD9 Code (s): CPT Code (s): Facility __________________________ Date ALLERGY ENDOCRINE GENERAL SURGERY ORTHOPEDICS NEUROLOGY RHEUMATOLOGY CARDIOLOGY ENT HEM/ONC PODIATRY OB/GYN UROLOGY DERMATOLOGY GE/GI NEPHROLOGY PULMONOLOGY PLEASE ATTACH CLINICAL DOCUMENTATION / LABS / IMAGING / CONSULTS ____________________________________________ Physician Name (please print) SPEC ONLY DOB: F OPHTHALMOLOGY OON (PAGES _________________) __________________________________ _Physician Signature __________________________________ Date Reason for referral adequately communicated? Yes No Adequate information received prior to the patient’s visit? Yes No Clinical guidelines followed? Yes No STANDING REFERRAL STANDING SPECIALIST REFERRAL: Yes No, IF YES, PLEASE COMPLETE BELOW Prior Standing Referral EXTENDED ______________# VISITS (>5)x _________ MONTHS MEDICAL GROUP ONLY Yes No STANDARD ______________# VISITS (<4)x _________ MONTHS [ ] APPROVED Treatment Plan agreed by Specialists/PCP Yes Accompanying this request Yes No [ ] CANCELLED No [ ] DENIED AUTHORIZATION #: ______________________________________________________________________________________________ Signature of Utilization Department ________________________ Date *NOTICE: This is not a guarantee of payment. Charges for non-covered service or services rendered to patients whose coverage is no longer in effect are the patients responsibility. This authorization is valid only for services specified for 60 days. **CONFIDENTIAL: Information protected under Federal and State law, and intended only for the use of the individual or entity named. If the reader of this form is not the intended recipient, employer, or agent responsible for delivering it to the intended recipient, you are hereby notified that any dissemination, distribution or copying of this communication is strictly prohibited. SANTA BARBARA SELECT IPA ROUTINE URGENT REFERRAL AUTHORIZATION FORM SB Select IPA 1901 N. Solar Drive, Suite 200 Oxnard, CA 93036 Provider Services: (800) 705-0831 Member Services: (800) 705-0831 Fax: (877) 216-4218 PATIENT INFORMATION Patient Name (Last, First, MI): Sex M Address: DOB: Co-Pay: F City / ST: Member ID#: Member Phone Number: Health Plan Name: Plan Code: Zip Code: PCP: Other Insurance? Name: PCP Fax Number: Yes No Service to be provided by: PRIOR AUTHORIZATION REQUEST AND/OR DIRECT REFERRAL FOR SPECIALIST ICD-9 Code(s): __________ CPT Code(s): __________ __________ __________ __________ __________ __________ __________ Description: Specify Proc/Svc: Frequency/Duration Requested: ________________________________________ (Chronic/exacerbated acute conditions can be >2 visits/60 days with treatment plan) Treatment Plan: Hospital/Facility: Expected Date of Admission: Assistant Surgeon: Inpatient/Outpatient: ____________________________________________ Physician Name (please print) ____________________________________________ Physician Signature ________________________ Date DIRECT REFERRAL (FOR PCP USE ONLY) Service to be provided by: ICD-9 Code(s): __________ CPT Code(s): __________ __________ __________ __________ __________ SPEC ONLY __________ Description: Specify Proc/Svc: Studies Completed/Comments: ____________________________________________ Physician Name (please print) MEDICAL GROUP ONLY __________ ___________________________________ Physician Signature ________________________ Date Reason for referral adequately communicated? Yes No Adequate information received by the time of the patient’s visit? Yes No Clinical guidelines followed? Yes No [ ] APPROVED [ ] CANCELLED [ ] DENIED AUTHORIZATION #: ______________________________________________________________________________________________ Signature of Utilization Department ________________________ Date *NOTICE: This is not a guarantee of payment. Charges for non-covered service or services rendered to patients whose coverage is no longer in effect are the patients responsibility. This authorization is valid only for services specified for 60 days. **CONFIDENTIAL: Information protected under Federal and State law, and intended only for the use of the individual or entity named. If the reader of this form is not the intended recipient, employer, or agent responsible for delivering it to the intended recipient, you are hereby notified that any dissemination, distribution or copying of this communication is strictly prohibited. Patient Referral Form PH: 805-604-3308 Fax: 805-278-6815 Date____________________ Patient Name__________________________________ Patient DOB ______________ HP ID#____________________ Referring Physician __________________________ Primary Care Physician ___________________________________ STAT/Urgent: Call UM for approval (once approved fax this completed form to UM for tracking) Must complete for STAT/Urgent: Specialist appointment Date: _______________ Time:________ Routine Retro (all retro referrals must be sent with claim for retro claim review) Refer to: __________________________________________________________________________________________ ICD-9/Diagnosis: ___________________________________________________________________________________ ICD-9/Diagnosis:___________________________________________________________________________________ CPT/Service: ______________________________________________________________________________________ CPT/Service: ______________________________________________________________________________________ Prior Treatment/Testing: _____________________________________________________________________________ __________________________________________________________________________________________________ Reason for Referral:_________________________________________________________________________________ __________________________________________________________________________________________________ Place of Service (name): _______________________________ Inpatient Outpatient PCP Signature: ___________________________________________________________________________________ Eligibility Checked by: ______________________________ Effective Date:____________ Aetna Aetna Senior Blue Cross Blue Shield Health Net Pacificare Secure Horizons SCAN Cigna TO BE COMPLETED BY UTILIZATION MANAGEMENT APPROVED___________________ DENIED ______________________ MODIFIED___________________________ Referral # _________________________________________________________________________________________ U.M. Physician Comment ____________________________________________________________________________ Fax Completed Referral Form to: 805/278-6815 Patient Referral Form: Request for Additional Services PH: 805-604-3308 Fax: 805-278-6815 STAT/Urgent: Call UM for approval (once approved fax this completed form to UM for tracking) Routine Retro (all retro referrals must be sent with claim for retro claim review) Date: Patient Name: Last Seen: Member ID #: DOB: Primary Care Physician: Reason for Referral: ICD-9 Code Diagnosis: ICD-9 Code Diagnosis: ICD-9 Code Diagnosis: Aetna Blue Shield Health Net Aetna SR. Cigna Scan PacifiCare Blue Cross Secure Horizons Authorization is being requested for the following Procedures/tests and/or future visits: CPT / Service: CPT / Service: CPT / Service: CPT / Service: Place of Service (name): Inpatient Outpatient List of potential consultants, (i.e., anesthesia, assistants): Consultant’s Signature Print Last Name Fax to Primary Care Physician: For routine referrals only VCIPA Primary Care Physicians Only – fax to VCIPA UM at 805/278-6815 PCP Recommendations: PCP Initials: Eligibility Checked: Effective Date: To be completed by VCIPA Utilization Management APPROVED: DENIED: MODIFIED: Referral #: _________________________________________________________________________________________ UM Comment: Management Services Administrator for Contracting Physician Organizations Part 10. Glossary Benefit Plan - refers to the specific services available to an enrollee under the HMO agreement with the employer. Capitated Services - those services listed in the Covered Services of the I.P.A./Medical Group and hospital contracts which the I.P.A./Medical Group and hospital are each responsible for providing for a fixed amount of reimbursement per member per month. Capitation - a prepaid monthly fee made to the I.P.A./ Medical Group and hospital for each enrollee in exchange for the provision of comprehensive health care services to enrolled members. Concurrent Review - review of a patient's chart, including verification of necessity of treatment and need for continued treatment, conducted during the course of treatment. Conversion Factor - the dollar amount to be applied to each relative value unit in a relative value scale to determine the payment amount for physician services. Co-Payment - a charge to a patient receiving medical care which is required by the health plan to be collected by the Provider of care. Coordination of Benefits (COB) - When a patient is covered by two or more group health plans, coordination of benefits divides the responsibility of payment between the health plans so that the coverage combined will pay up to 100% of hospital and professional services within the limits of all contracts. Dependent - includes spouse and children of the subscriber who receive coverage through the subscriber's health plan. Eligibility - a determination of whether a member is covered by the health plan for medical services. Enrollee - any person, or eligible dependent, who is enrolled in the health plan. E.O.B. - explanation of benefits. Evidence of Coverage - description of health insurance benefits as well as limitations and exclusions provided to each member by the health plan. Fee for Service – a method of payment to physicians for all services authorized based on a specific dollar amount for each service. Health Care Financing Administration (HCFA) – the federal agency responsible for administering Medicare and overseeing states’ administration of Medicaid. Health Maintenance Organization (HMO) - a prepaid health plan licensed by the appropriate state agency (for example, in California HMOs are regulated through the Department of Corporations). Individual Plan - a benefit plan available to individual members who chose their eligibility for coverage through their employer. Independent Physicians Association "IPA" - a network of private practice physicians and allied health professionals established to facilitate referrals and to contract with HMO's and other third party payors. Page 74 Management Services Administrator for Contracting Physician Organizations Part 10. Glossary Medical Assistant (MA) – an individual trained to perform a minimal amount of nursing duties and laboratory procedures, as well as front-office duties. Member - a subscriber or dependent entitled to receive medical services from Providers. National Committee for Quality Assurance (NCQA) – a Washington D.C. group that develops HMO accreditation standards. Non-Covered Services - health care services which are not benefits under the subscriber's evidence of coverage. Nurse Practitioner (NP) – a nurse with additional extensive training who is licensed to perform duties beyond the scope of the nursing profession. Open Enrollment - the annual period during which employees of a company may change their health insurance coverage. Out of Area - the area outside a 30 air-mile radius of the primary hospital. Outside this boundary the Provider Group and hospital are not directly responsible for the provision of care, according to their contractual agreement with the health plan. Participating Physician - a legally qualified physician who has entered into an agreement with the HMO or with one of the hospitals or physician groups to provide physician services to enrollees of the HMO. Per Diem Rates - cost figures negotiated with Providers to cover specific services rendered in a 24 hour period beginning at 12:00 midnight or for a one day admission. Pre-Admission Review Program - a process by which the Provider Group will arrange for the admission of enrollees to the primary hospital or referral to other hospitals. Premium - refers to the fee paid by an employer to the health plan as compensation for the provision of health care services. (PCP) Primary Care Provider - is the Provider Group physician selected by an enrollee to render first-contact medical care and may include physicians whose training is in family practice, internal medicine, pediatrics, and obstetrics/gynecology. Primary Hospital - is that hospital selected by the HMO and the Provider Group where the majority of enrollees’ inpatient care is to be provided. Provider - physicians, hospitals and other health care professionals providing health care related services to health plan enrollees. Quality Management - the process established to ensure that the quality of medical services rendered meets or exceeds objective standards developed by knowledgeable health professionals and that services provided are "medically necessary" and provided in a timely manner. Referral - the process by which the PCP directs an enrollee to seek and obtain covered services from other contracted health professionals. Retrospective Review - review conducted following the patient's treatment. Page 75 Management Services Administrator for Contracting Physician Organizations Part 10. Glossary Service Area - the geographic area that is within a 30 air mile radius of the primary hospital. Shared Risk Services - the in-patient and other patient care services which are subject to a formula for determining the amount and distribution of risk sharing incentives between the I.P.A./Medical Group, primary hospital and HMO. Stop Loss – an insurance program limiting the financial liability of a Provider Group for any given member. Subscriber - the adult who selects coverage by HMO through his/her employer. Subscriber Group - is the organization, firm or other entity contracting with HMO's to arrange health care services for employees and their dependents. Subrogation - the assumption by a third party (as a second creditor) of another's legal right to collect a debt or damages. Utilization Management - the process established to assure that services rendered are medically necessary and provided in the most cost-effective manner, consistent with the maintenance of high quality standards of practice. Page 76





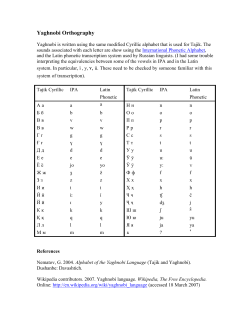




![MINISTER FOR HEALTH [[#] . CONTRACTING MEDICAL PRACTITIONER] and](http://cdn1.abcdocz.com/store/data/000041716_2-10d4161c7eb06a837afde114d879fdef-250x500.png)
© Copyright 2026