
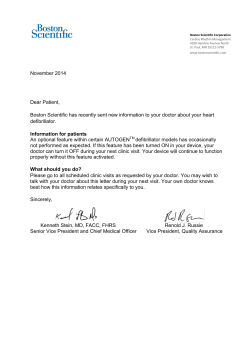
Instructions for Off Base Doctors: A B
Instructions for Off Base Doctors: How to Complete a Defence Pathology Request Form A. Patient details - Complete all fields B. P.M. Keys Number A B C PaTIENT LaST NamE GIVEN NamES Pm KEYS No. GENDER TEL (HomE & moBILE) DaTE oF BIRTH C. Unit/barracks and address D. Tests Requested - Please list required tests here TEL (BUS) aDF UNIT/SHIP NamE aND LoCaTIoN PoSTCoDE E.Fasting - The patient’s fasting status TESTS REQUESTED E D F. Clinical Notes (if required) Is patient: Fasting ■ Non Fasting ■ If drug level required: LaST DoSE TImE .................................... DaTE .......... /.......... /........... LABORATORY COPY CLINICaL NoTES Urgent Clinically High Risk/Significant YES BILL CoDE No BY TImE: ..................................... REaSoN: ...................................................................................... I CoPY REPoRTS To: REQUESTING DoCToR aND DaTE oF REQUEST H H. Duty Medical Officer Code - This code is for Path-Way. Add further ‘Copy To’ report doctors as required COPY CODE INFORMATION To ensure that the defence facility receives a copy report, please add the appropriate copy code here. Please see table below for codes. F G G.Urgency - Whether a sample is urgent or not PRINTED NamE ......................................................................................... LaV. DR CoDE .......................... SIGNaTURE ............................................................................................... DaTE .......... / ............ /............. REFERRING FaCILITY I. Requesting Doctor Details The requesting doctor’s name and Laverty doctor code are required. HoSPITaL/WaRD: PERSoN DRaWING BLooD I certify that the blood specimen(s) accompanying this request was drawn from the patient named above. established the identify of this patient by direct inquiry and/or inspection of wrist band and immediately upon the blood being drawn I labelled the specimen(s). I have also signed the sample tube. LAB USE Name: ........................................................................ Signature: ............................................................. Collect Date Coll. Time Received Date Rec. Time Collector B/C DFF aCC Specimens EDTA SST CIT Flox K2 Others Sign Collected Received Specialist Diagnostic Services Pty Ltd (ABN 84 007 190 043) t/a Laverty Pathology APA No.000042 ACT Base Medical Centre Copy Code Duntroon Duntroon Health Centre 4DUNH HMAS Harman Harman Clinic 4HMNC Russell Offices Russell Health Centre 4RUSH Weston Weston Clinic 4WESC








© Copyright 2026