
AAGL Vaginal Cuff Closure: How to Minimize Dehiscence and Prolapse
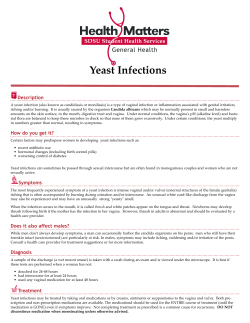
Vaginal Cuff Closure: How to Minimize Dehiscence and Prolapse MODERATOR Stuart R. Hart, MD FACULTY Kate O’Hanlan, MD & Michele Vignali, MD Sponsored by AAGL Advancing Minimally Invasive Gynecology Worldwide Professional Education Information Target Audience This educational activity is developed to meet the needs of residents, fellows and new minimally invasive specialists in the field of gynecology. Accreditation AAGL is accredited by the Accreditation Council for Continuing Medical Education to provide continuing medical education for physicians. The AAGL designates this live activity for a maximum of 1.75 AMA PRA Category 1 Credit(s)™. Physicians should claim only the credit commensurate with the extent of their participation in the activity. DISCLOSURE OF RELEVANT FINANCIAL RELATIONSHIPS As a provider accredited by the Accreditation Council for Continuing Medical Education, AAGL must ensure balance, independence, and objectivity in all CME activities to promote improvements in health care and not proprietary interests of a commercial interest. The provider controls all decisions related to identification of CME needs, determination of educational objectives, selection and presentation of content, selection of all persons and organizations that will be in a position to control the content, selection of educational methods, and evaluation of the activity. Course chairs, planning committee members, presenters, authors, moderators, panel members, and others in a position to control the content of this activity are required to disclose relevant financial relationships with commercial interests related to the subject matter of this educational activity. Learners are able to assess the potential for commercial bias in information when complete disclosure, resolution of conflicts of interest, and acknowledgment of commercial support are provided prior to the activity. Informed learners are the final safeguards in assuring that a CME activity is independent from commercial support. We believe this mechanism contributes to the transparency and accountability of CME. Table of Contents Course Description ........................................................................................................................................ 1 Disclosure ...................................................................................................................................................... 2 Vaginal Cuff Closure: How to Minimize Dehiscence and Prolapse K. O’Hanlan ................................................................................................................................................... 3 Vaginal Cuff Closure: How to Minimize Dehiscence and Prolapse M. Vignali ...................................................................................................................................................... 9 Cultural and Linguistics Competency ......................................................................................................... 20 Surgical Tutorial 4 Vaginal Cuff Closure: How to Minimize Dehiscence and Prolapse Moderator: Stuart R. Hart Kate O’Hanlan & Michele Vignali This course provides rich video and didactic learning to overcome one of the strongest deterrents to TLH: confident laparoscopic closure of the vagina. The three key elements of closure that effectively prevent prolapse, as well as hemorrhagic and dehiscence complications, will be reviewed and demonstrated in detailed videos. Even if suture closure of the vagina is already possible, this tutorial can advance your skills to make it consistently reliable and effective. Learning Objectives: At the conclusion of this course, the participant will be able to: 1) Differentiate the reasons why some patients have hemorrhagic, prolapse and dehiscence complications; 2) design a system for learning suture skills outside of the operating rooms; and 3) construct a plan for laparoscopic closure of the vaginal apex when closure cannot be accomplished any other way; 4) differentiate those cases who deserve a prophylactic vaginal vault suspension. 1 PLANNER DISCLOSURE The following members of AAGL have been involved in the educational planning of this workshop and have no conflict of interest to disclose (in alphabetical order by last name). Art Arellano, Professional Education Manager, AAGL* Viviane F. Connor Consultant: Conceptus Incorporated Kimberly A. Kho* Frank D. Loffer, Executive Vice President/Medical Director, AAGL* Linda Michels, Executive Director, AAGL* M. Jonathan Solnik* Johnny Yi* SCIENTIFIC PROGRAM COMMITTEE Ceana H. Nezhat Consultant: Ethicon Endo-Surgery, Lumenis, Karl Storz Other: Medical Advisor: Plasma Surgical Other: Scientific Advisory Board: SurgiQuest Arnold P. Advincula Consultant: Blue Endo, CooperSurgical, Covidien, Intuitive Surgical, SurgiQuest Other: Royalties: CooperSurgical Linda D. Bradley* Victor Gomel* Keith B. Isaacson* Grace M. Janik Grants/Research Support: Hologic Consultant: Karl Storz C.Y. Liu* Javier F. Magrina* Andrew I. Sokol* FACULTY DISCLOSURE The following have agreed to provide verbal disclosure of their relationships prior to their presentations. They have also agreed to support their presentations and clinical recommendations with the “best available evidence” from medical literature (in alphabetical order by last name). Stuart R. Hart Consultant: Boston Scientific, Covidien, Stryker Endoscopy Speakers Bureau: Boston Scientific, Covidien, Stryker Endoscopy Kate O’Hanlan Consultant: Cardinal Health, Medical Products and Services, CONMED Corporation, Covidien Speakers Bureau: Baxter, CONMED Corporation, Covidien Other: Medical Director: Laparoscopic Institute for Gynecologic Oncology Michele Vignali* Asterisk (*) denotes no financial relationships to disclose. Vaginal Cuff Closure: How to Minimize Dehiscence and Prolapse • Consultant: Cardinal Health Medical Products and Services, CONMED Corporation, Covidien, • Speakers Bureau: Baxter, CONMED Corporation, Covidien • Other: Medical Director: Laparoscopic Institute for Gynecologic Oncology Kate O’Hanlan, MD Laparoscopic Institute for Gynecologic Oncology Management of Dehiscence: Sx, when to suture, observe etc Objectives • Differentiate reasons risk factors for prolapse or dehiscence complications; • Design a system for learning suture skills outside of the operating rooms; • Construct a plan for laparoscopic closure of the vaginal apex when closure cannot be accomplished any other way; • Differentiate those cases who deserve a prophylactic vaginal vault suspension. • Risk factors: • Sx, when to suture, observe etc Avoiding vaginal dehiscence Vaginal cuff dehiscence • Vaginal .18% • Laparoscopic .64% • Robotic 1.64% • 1-2% in most studies, 77days post-op. • Malignancy, diabetes, cigarette smoking, pelvic adhesions, radical hyst greater risk. • Suture cuff with same standards as open: (p<0.05) (p<0.05) – Stitch every 5-8mm, 5mm deep. Same as diameter. • Two-layer closure better than single. • Transvaginal suturing can reduce risk after TLH. • Monopolar no difference. » Hur, et al. (2007). "Incidence and patient characteristics of vaginal cuff dehiscence after different modes of hysterectomies." JMIG 14(3): 311-317. » Nick, et al. (2011). "Rate of vaginal cuff separation following laparoscopic or robotic hysterectomy." Gyn Onc 120(1): 47-51. Uccella et al O&G Sept 2012 » Jeung et al. (2010). "A prospective comparison of vaginal stump suturing techniques during total laparoscopic hysterectomy." Archives of gynecology and obstetrics 282(6): 631-638. • My take: Since you cannot close every patient transvaginally, learn to suture laparoscopically. 3 Vaginal dehiscence • Related to placement of sutures during the vaginal closure. • Scope or Robot: place the same size stitches in the apex as for open. • Consider closing the bladder over the apex: – May prevent adhesions of small bowel to vaginal raw edges of apex. – May prevent though-and-through dehiscence from penetration. Managing dehiscence • See immediately if SSx: – Copious serous or sanguinous discharge. – Pain after intercourse. No support to cuff from apex • Suture vagina from below, or by scope if: – see small bowel. Prep before put back. – Opening greater than 2cm. – Double ‘cidal antibiotics. – Pelvic rest another 6 weeks, then recheck. – Advise shallow. Consider foam donut for spouse. » Nick, A. M., J. Lange, et al. (2011). "Rate of vaginal cuff separation following laparoscopic or robotic hysterectomy." Gynecologic oncology 120(1): 47-51. Good support to cuff from apex. 4 Cystocele repair can be accomplished laparoscopically “Three to five mattress sutures are inserted through the fascia which becomes duplicated and shortened, thus strengthening the anterior vaginal wal and holding the bladder.” Cysto/enterocele repair from above by Soferman et al International Surgery, 1974 “Suture is passed through the vagina and brought through both sacrouterine ligaments without tying. Another suture is passed through the cardinal ligaments...tying these approximates the ligaments to each other and to the vaginal wall.” • Cysto/enterocele repair from above by Soferman et al International Surgery, 1974 Support procedures that even a Gyn Oncologist can do…….. Digesu et al. A case of laparoscopic uterosacral ligaments plication: a new conservative approach to uterine prolapse. Eur J Obstet Gynecol Reprod Biol. 2004 5 Quadri et al, Transabdominal repair of cystocele by wedge colpectomy during combined abdominal-vaginal surgery. Int Urogynecol J Pelvic Floor Dysfunct. 1997 Laparoscopic closure of the vaginal apex: when closure cannot be accomplished any other way Resect enterocele Ethibond 0 Suture Obstacles to learning in the OR • Seniors won’t give away critical parts. Design a system for learning suture skills outside of the operating rooms; pelvic trainers, holiotomy challenge. – Newer surgeons take longer. Costs time. – Newer surgeons make more mistakes. • Newest technology and techniques hard to learn on live patient in front of all. • Surgeons who trained on simulators had greater accuracy in vivo, made fewer mistakes. • High tech “virtual reality” no better. Scott et al, JACS, 2000 Banks et al AJOG, 2007 Kundhal et al, Surg Endosc, 2009 6 JMIG, 2011 Intracorporeal suturing incorporates all basic laparoscopic skills and is a prerequisite because it is needed to manage possible complications or in case of instrument failure. Novice Expert Residents with little or no previous laparoscopic experience are able to perform the task competently after a short training course. Laparoscopic skills • Performance on trainers significantly improves competency in the OR. – Practice on trainers improves OR competency. – At least 5-7 suture repetitions needed til efficacy plateau. – At least 25 knots til efficacy plateau. • Self assessment and formal evaluation of skills possible on trainer. Goff BA, Obstet & Gynecol, 2008. Kanumuri et al, JSLS, 2008. The Holiotomy™ Challenges • Complete three holiotomies™: – Two with three “figure of N” stitches, each piercing the dots. – Close one running. • Place your holiotomy™ repairs on the board at registration. • Get certificate! www.LIGOcourses.com 29 2 9 7 31 3 1 www.LIGOcourses.com Comfort performing procedures before and after a surgical course P<.001 You get a way cool cap!!!! P<.001 NS P<.001 P<.001 1= very comfortable 2=somewhat 3‐neutral 4‐uncomfortable 5=very uncomfortable 33 3 www.LIGOcourses.com 3 8 Surgical Tutorial 4 Vaginal Cuff Closure: How to Minimize Dehiscence and Prolapse I have no financial relationships to disclose. Moderator: Stuart R. Hart Professor Michele VIGNALI, MD, PhD Associate Professor of Obstetrics and Gynecology Director of Endoscopic Gynecologic Surgery Unit Department of Biomedic Science for the Health Macedonio Melloni Hospital University of Milan, Italy At the conclusion of this activitiy, participants will be better able to: Differentiate the reasons why some patients have vaginal vault prolapse and dehiscence complications Identify those patients at risk who deserve a prophylactic vaginal vault suspension Part 1 – VAULT DEHISCENCE Incidence, Reasons and Risk Factors Construct a plan for laparoscopic closure of the vaginal apex using different sutures Summarize the current literature regarding the diagnosis and management of vaginal vault dehiscence and prolapse. [email protected] [email protected] Can Med Assoc J. 1952 January; 66(1): 68 The first abdominal hysterectomy was performed by Charles Clay in Manchester, England in 1843, but only 1853 that Ellis Burnham from Lowell, Massachusetts achieved the first successful abdominal hysterectomy Vaginal hysterectomy dates back to ancient times. The procedure was performed by Soranus of Ephesus 120 years A.C. but the first planned, successful vaginal hysterectomy was performed in 1813 by Conrad Langenbeck, although he did not report the case until 1817 9 [email protected] [email protected] [email protected] [email protected] [email protected] [email protected] Evisceration occurs in up to 70% of vaginal cuff dehiscence cases 10 [email protected] [email protected] Obstet Gynecol 2004;103:572-576 The Mayo Clinic experience from 1970 through 2001 yielded a 0.032% incidence of vaginal evisceration after a pelvic operation 7039 total and 247 supracervical The cumulative incidence of vaginal dehiscence by mode of hysterectomy was 4.93% among TLH, 0.29% among VH, and 0.12% among TAH The relative risks of a vaginal cuff dehiscence complication after TLH compared with TVH and TAH were 21.0 and 53.2, respectively. Both were statistically significant. Aust N Z J Obstet Gynaecol. 2007 Dec;47(6):516-9 Rupture of the vaginal vault with subsequent extrusion of the peritoneal contents appears to be a rare occurrence, complicating less than one in 1000 hysterectomies. However, it seems that this risk is significantly higher in TLH. JMIG 2007;14:311–317 [email protected] [email protected] JMIG 2009;16:313–317 JMIG 2009;16:313–317 The time interval between hysterectomy and occurrence of vault dehiscence in the laparoscopic group (8.4±1.2 weeks) was significantly shorter than in the abdominal hysterectomy (112.7±75.1 weeks, p<.01) and in vaginal hysterectomy (136.5±32.2 weeks, p<0.0001) groups, respectively The incidence of vault dehiscence was higher after TLH (1.14%) than after AH (0.10%, p.0001) and after VH (0.14%, p.001) 10 632 hysterectomies [email protected] [email protected] Eur J Obstet Gynecol Reprod Biol 2011;158(2):308-313 34/8635 (0.39%) experienced vaginal evisceration. The laparoscopic route was associated with a significantly higher incidence of dehiscence (0.80%) Obstet Gynecol 2012;120:516-523 TLH was associated with a higher incidence of cuff separations, compared with AH (0.64% compared with 0.21%, P.003) and VH (0.64% compared with 0.13%, P<.001). 11 [email protected] [email protected] Vaginal cuff dehiscence can occur at any time after a pelvic surgical procedure and has been reported as early as 3 days and as late as 30 years postoperatively In retrospective cohort studies and larger case series the mean time to cuff dehiscence varied between 6.1- weeks up to 1.6 years (range 2 weeks to 5.4 years) [email protected] [email protected] Obstet Gynecol Surv 2002;57(7):462-467 59 cases from 1900 to 2001 These symptoms typically occur after: sexual activity vaginal instrumentation increased intraabdominal pressure Protruding mass in the vagina Abdominal pain Vaginal bleeding or discharge Am J Obstet Gynecol 2012;206(4):284–288 Pelvic or abdominal pain (58-100%) Vaginal bleeding or watery discharge (33%90%) Patients with evisceration of bowel into the vagina often describe feeling a mass or pressure [email protected] [email protected] WHY?-Risk Factors Route of hysterectomy Increased age and hypoestrogenism Increase in intra-abdominal pressure In addition, there are Swift return to everyday activities theoretical risks of and sexual activity incomplete full thickness cuff closure Vaginal infection/hematoma Way of cuff vaginal cuff closure The type and size of the suture material used to close the vault Tissue damage in the vaginal cuff due to electrocautery JMIG 2007;14:311–317 7039 total and 247 supracervical Obstet Gynecol 2011;118:794–801 The 10- year cumulative incidence of dehiscence after all modes of hysterectomy was 0.24% and 1.35% among total laparoscopic hysterectomies (Total abdominal hysterectomy was 0.38%, and total vaginal hysterectomy was 0.11%). or shallow suture placement less than 1 cm from the vaginal cuff edges because of LPS magnification 12 [email protected] [email protected] Literature search 57 articles, 13.030 endoscopic hysterectomies + 635 TLH Am J Obstet Gynecol 2011;205:119.e1-12 JSLS 2012;16:530–536 3/654 robotic-assisted TLH 0.4% Obstet Gynecol 2009;114(2 Pt 1):369–371 TRANSVAGINAL colporraphy after TLH is associated with a 3- and 9-fold reduction in risk of vaginal cuff dehiscence compared with LPS and robotic suture, respectively “..Robotic instruments do not allow exerting enough tension on the knots when cuff closure is performed” “It has been speculated that because of electrosurgical energy at the time of colpotomy may account for the observed increased risk of vaginal cuff dehiscence..” The pooled incidence of vaginal dehiscence was LOWER for TV cuff closure (0.18%) than for both LPS (0.64%) and robotic (1.64%) colporraphy. LPS cuff closure was associated with a lower risk of dehiscence than robotic closure (OR=0.38) [email protected] [email protected] 0.032% Gynecologic Oncology 120 (2011) 47–51 362 underwent simple hysterectomy (249 laparoscopic, 113 robotic) 57 underwent radical hysterectomy (36 laparoscopic, 19 robotic). Obstet Gynecol 2004;103:572-576 Mayo Clinic medical records (1970 –2001) 7/417 (1.7%) developed a cuff complication 3/285 (1.1%) patients in the LPS group suffered a vaginal cuff evisceration (n=2) or separation (n=1) 4/132 (3.0%) had a vaginal evisceration (n=1) or separation (n=3) No difference based on surgical approach (p=0.22) Women with a history of abdominal hysterectomy tended to rupture through the vaginal cuff.. ..and those with a history of vaginal hysterectomy tended to rupture through a posterior enterocele Vaginal cuff complications were 9.46-fold higher among patients who had a radical hysterectomy. Changes in the vaginal support and/or foreshortening of the vagina may play a role in the development of vaginal cuff complications [email protected] [email protected] Obstet Gynecol 2012;120:516–23 JSLS 2013;17:414–417 Patients who underwent vaginal closure with LPS knots had a higher rate of cuff dehiscence than patients who had suture with transvaginal knots (0.86% vs. 0.24%, P.028), When vaginal suture was performed transvaginally, no statistical difference in vaginal cuff dehiscence rate was observed compared with both AH and VH 463 TLH and 147 LAVH performed entirely by use of electrosurgery There were no vaginal cuff dehiscences in the LAVH group compared with 17 vaginal cuff dehiscences (4%) in the TLH group (P=.02). Because all LAVHs were performed entirely by electrosurgery including colpotomy and there were no vaginal cuff dehiscences in the LAVH group, it does not appear that ELECTROSURGERY plays a major role in vaginal cuff dehiscence Use of at the time of colpotomy and reducing the power of monopolar energy from 60 watts to 50 watts when colpotomy was performed at the end of TLH didn’t alter the rate of cuff separations. Vaginal cuff closure suture was changed to 2-0 glycolide/lactide copolymer (delayed absorbable) and tissue suture placement was increased to at least 1.5 cm 13 [email protected] [email protected] Incidence of vaginal cuff dehiscence 4.2% Aust N Z J Obstet Gynaecol. 2007 Dec;47(6):516-9 Careful, full-thickness closure of the vaginal vault with a delayed absorbable suture is recommended at TLH It may be prudent to advise women undergoing TLH to delay first intercourse postoperatively JMIG 2011;18:218–223 387 women 149 0-barbed suture (double layer) 9 0-monofilament suture 229 braided sutures comprised of polyglycolic acid (Vicryl) or Endo Stitch NO CASES of dehiscence among those who had closure with bidirectional barbed suture (p=.008). Post OP bleeding, presence of granulation tissue, and cellulitis ALL occurred more frequently in patients without barbed suture closure. [email protected] [email protected] Eur J Obstet Gynecol Reprod Biol 2011;158(2):308-313 Gynecol Surg 2012;9:393–400 34/8635 (0.39%) experienced vaginal evisceration [8 (0.25%) AH, 4 (0.15%) VH, 22 (0.80%) TLH (p< 0.01)]. The laparoscopic route was associated with a significantly higher incidence of dehiscence (0.80%) NO superiority of one of the suturing methods over the other was found. Regardless of the suturing method, the surgical approach towards the colpotomy in TLH in comparison to the abdominal approach, with additional (extensive) application of coagulation, has inherent its specific side effects. 8635 pts 3194 (37%) AH 2696 (31.2%) VH 2745 (31.8%) TLH No differences were found between the 6027 patients (69.8%) who had closure of the vaginal cuff and the 2608 (30.2%) who had an unclosed cuff closure technique. [email protected] Vaginal Cuff Dehiscence is a rare complication of hysterectomy, but more frequently after TLH (0.4-0.8%) It is associated to vaginal evisceration in 70% of cases It can occur at any time but the mean time varied between 6.1- weeks up to 1.6 years after hysterectomy TRANSVAGINAL colporraphy after TLH is associated with a 3- and 9-fold reduction in risk of vaginal cuff dehiscence compared with LPS and robotic suture Main symptoms are: protruding mass in the vagina, abdominal pain and vaginal bleeding or discharge Discourage swift return to sexual activities Prefer delayed absorbable sutures and big bites of tissue Part 2 – VAULT PROLAPSE Incidence, Reasons and Risk Factors 14 [email protected] [email protected] Int Urogynecol J 2008;19:1623–1629 Pelvic organ prolapse is a common problem, affecting 30% to 50% of women The overall incidence of prolapse after hysterectomy was reported to be 3.6 per 1,000 women-years (Mant J et al, 1997). The incidence was 1.1 per 1,000 women-years if initial hysterectomy was performed for prolapse, compared with 0.2 per 1,000 women-years if the hysterectomy was performed for other reasons (hazard RR 5.8). The incidence of vault prolapse after hysterec-tomy varies between 0.2% to 43%, but realistically between 1.8 and 11.6% [email protected] [email protected] Int Urogynecol J 2008;19:1623–1629 Am J Obstet Gynecol. 1992 Jun;166(6 Pt 1):1717-24 6,214 hysterectomies 4,304 (69.3%) abdominal hysterectomy 1,749 (28.1%) vaginal hysterectomy 65 (1%) LAVH 96 (1.5%) TLH The upper third of the vagina (level I) is suspended from the pelvic walls by vertical fibers of the paracolpium, which is a continuation of the cardinal ligament In the middle third of the vagina (level II) the paracolpium attaches the vagina laterally to the arcus tendineus and fascia of the levator ani muscles. 32/6214 (0.5%) were reoperated for subsequent vault prolapse. The mean interval between the two operations was 6.2 yrs (range 0.2 to 21.8 yrs). The incidence of vault prolapse requiring surgical correction after hysterectomy was 0.36 per 1,000 women-years Dissection reveals that the paracolpium's vertical fibers in level I prevented prolapse of the vaginal apex and vaginal eversion [email protected] The vagina's lower third fuses with the perineal membrane, levator ani muscles, and perineal body (level III). [email protected] Curr Opin Obstet Gynecol 2010;22:420-424 15 Predisposing factors (growth and development, genetic factors, connective tissue weakness, joint mobility) Inciting factors pelvic surgery) Intervening factors (agerelated changes, obesity, constipation, co-morbidities, heavy occupationalwork,and vigorous physical activity) (childbirth, History of POP at the time of hysterectomy has consistently been shown as a strong and independent predictor of POP recurrence [email protected] [email protected] Curr Opin Obstet Gynecol 2010;22:420-424 Apical support defects The role of AGE is still controversial: Advanced age is a indipendent factor Younger patients have a higher risk of prolapse recurrence as a consequence of a major expectancy of lasting of the reconstructive procedures To ensure durable apical support regardless of the anchoring site for the vaginal vault suspension, the surgeon should establish continuity of the anterior and posterior vaginal fascia at the vaginal apex. OBESE women are considered a high-risk group for development of POP BMI is a significant and indipendent risk factor [email protected] In 1927, Miller described the attachment of the USL to the vaginal vault for support In 1957, McCall described passing a suture from one side of the vaginal cuff and USL through the peritoneum to the other side,effectively closing the cul-de-sac [email protected] Curr Opin Obstet Gynecol 2008;20:484–488 In 2000, Shull et al described a “high” uterosacral ligament suspension in which 3 nonabsorbable sutures are “placed in the ligament on either side..to secure the superior aspect of the transverse portion of pubocervical and rectovaginal fascia” to the vaginal cuff The purpose of the USL vault suspension is to attach a strong segment of the USL to the rectovaginal and anterior pubocervical fascia The USL is considered a major source of overall support for the uterus The exact attachment of the USL from the ischial spine has been the subject of controversy as some believe it connects to the sacrum, whereas others postulate there are attachments to the sacrospinous ligament and coccygeous muscle. [email protected] [email protected] Obstet Gynecol 2004;103:447–51 Curr Opin Obstet Gynecol 2008;20:484–488 At the cervix, it is composed of closely packed bundles of smooth muscle, small and medium-sized blood vessels and small nerve bundles In the intermediate third portion of the USL, it is composed of connective tissue with a few scattered small fibers, blood vessels and nerves In the sacral portion, it is made entirely of loose strands of connective tissue and sparse fat, vessels, nerves and lymphatics 16 They extended over a mean craniocaudal distance of 218 mm (range 10–50) Although uterosacral ligament morphology was similar bilaterally, its craniocaudal extent was greater on the right side [email protected] [email protected] Obstet Gynecol 2004;103:447–51 US Ligament Suspension Surgical Technique Three regions of origin: cervix alone (33%), cervix and vagina in the same section (63%), and vagina alone (4%). Of 259 uterosacral insertion points, 82% overlaid the sacrospinous ligament/coccygeus muscle complex, 7% the sacrum, and 11% the piriformis muscle, the sciatic foramen, or the ischial spine Thus, if one does not artificially reattach the vaginal cuff to the US ligaments, more than 2/3 of patients would retain some connections of the vaginal apex to the US ligaments The ureters are identified throughout their course below the pelvic brim and a relaxing incision is placed below the level of the ureter within the peritoneum. The ischial spines identified by placing tension on the cuff in the contralateral direction The USLs are attached to the posterior surface of the vaginal vault [email protected] [email protected] Int Urogynecol J (2012) 23:223–227 Curr Opin Obstet Gynecol 2008;20:484–488 During surgery, the ureters may be kinked, tied or injured Wieslander et al. found that while placing sutures vaginally within the USL in cadavers, the distal suture was approximately 14 mm from the ureter and 13 mm from the rectal lumen The rate of obstruction with high USL suspension was found to be 5.1%. USL sutures can be placed close to the sacral foramina and injury the sacral plexus (S1-S4) Permanent (polyester) and delayed absorbable (polydioxanone) sutures were compared 105 pts: permanent suture pts: delayed absorbable suture 141 The use of permanent sutures for USLS of the vaginal apex was associated with a lower failure rate than delayed absorbable sutures in the short-term [email protected] [email protected] Curr Opin Obstet Gynecol 2008;20:484–488 Success rates vary from 82 to 96% Curr Opin Obstet Gynecol 2008;20:496–500 17 Diwan et al. compared the outcomes of 25 LPS USLS to 25 vaginal USLS among age-matched controls. Estimated blood loss and duration of hospitalization were significantly less in the LPS group There were 3 recurrences in the vaginal group diagnosed at 17, 34, and 58 weeks but NONE in the laparoscopic group. [email protected] [email protected] Surg Technol Int. 2012 Nov 18;XXII Surg Technol Int. 2012 Nov 18;XXII A) to incorporate the suture through the right USL then through the anterior and posterior endopelvic fascia across the vaginal vault, and finish by incorporating the left USL. The initial stitch is placed through the mid-portion of the USLs on stretch, and a second and third suture are placed sequentially more proximal through the USLs, with each stitch incorporating both anterior and posterior endopelvic fascia. The suture is tied using extracorporeal knot tying technique B) to incorporate the USL stitch through the anterior and posterior endopelvic fascia on each respective side without crossing the midline. The initial stitch is placed through the mid-portion of the USL and then through the anterior and posterior endopelvic fascia on the lateral aspect of the vaginal cuff on each respective side. The next stitch is placed more proximal through the USL and then more medially through the anterior and posterior endopelvic fasciaon each respective side, until the midline vaginal cuff is incorporated. [email protected] Am J Obstet Gynecol. 2010 Feb;202(2):124-34 McCall Culdoplasty 1966-2007 McCall ML. Posterior culdeplasty; surgical correction of enterocele during vaginal hysterectomy; a preliminary report. Obstet Gynecol. 1957 Dec;10(6):595-602 In the anterior, apical, and posterior compartments, the pooled rates for a successful outcome were 81.2%, 98.3%, and 87.4% Traction of the cul-desac and posterior vaginal epithelium and placement of three rows of sutures across the cul-de-sac from one uterosacral ligament to the other Uterosacral ligament suspension is a highly effective procedure for the restoration of apical vaginal support. A successful outcome (stage 0 or 1) is observed in 98% of women [email protected] [email protected] Obstet Gynecol Int. 2009;275621 J Minim Inv Gynecol 2007;14:397-398 ..A permanent 3-0 suture was placed through the USL and the peritoneum of the cul-de-sac. A second suture was placed in the same way 1 cm above and parallel to the previous stitch. Sutures were kept to be tied after placement of the external suture. The external adsorbable 2-0 McCall suture was then placed through the posterior vaginal wall and peritoneum. This suture was then placed through the uterosacral ligaments and then brought back out through the vagina Am J Obstet Gynecol 1999;180(4):859-865 18 [email protected] Vaginal vault prolapse after hysterectomy varies between 1.8 and 11.6% An alteration in the level of the fibers of the paracolpium (level I) which suspend the upper third of the vagina could modify vault suspension Risk factors: Genetic or structural factors, previous deliveries or pelvic surgery, co-morbidities, age, BMI and history of prolapse at time of surgery USLs suspension is highly effective procedure for the restoration of apical vaginal support with a success rates varying from 82 to 96% The rate of ureteral obstruction with high USL suspension was found to be 5.1% McCall culdoplasty can be performed laparoscopically in order to correct enterocele and prevent vaginal prolapse DeLancey JO. Anatomic aspects of vaginal eversion after hysterectomy. Am J Obstet Gynecol. 1992 Jun;166(6 Pt 1):1717-24 Croak AJ, Gebhart JB, Klingele CJ, Schroeder G, Lee RA, Podratz KC. Characteristics of patients with vaginal rupture and evisceration. Obstet Gynecol. 2004 Mar;103(3):572-6 Siedhoff MT, Yunker AC, Steege JF. Decreased incidence of vaginal cuffdehiscence after laparoscopic closure with bidirectional barbed suture. J Minim Invasive Gynecol. 2011 Mar-Apr;18(2):218-23 Fanning J, Kesterson J, Davies M, Green J, Penezic L, Vargas R, Harkins G. Effects of electrosurgery and vaginal closure technique on postoperative vaginal cuff dehiscence. JSLS. 2013;17(3):414-7 Baskett TF. Hysterectomy: evolution and trends. Best Pract Res Clin Obstet Gynaecol. 2005 Jun;19(3):295-305 Hur HC, Guido RS, Mansuria SM, Hacker MR, Sanfilippo JS, Lee TT. Incidence and patient characteristics of vaginal cuff dehiscence after different modes of hysterectomies. J Minim Invasive Gynecol. 2007 May-Jun;14(3):311-7 Hobbs FS. Spontaneous evisceration through vagina. Can Med Assoc J. 1952 Jan;66(1):68 Uccella S, Ceccaroni M, Cromi A, Malzoni M, Berretta R, De Iaco P, Roviglione G, Bogani G, Minelli L, Ghezzi F. Vaginal cuff dehiscence in a series of 12,398 hysterectomies: effect of different types of colpotomy and vaginal closure. Obstet Gynecol. 2012 Sep;120(3):516-23 Uccella S, Ghezzi F, Mariani A, Cromi A, Bogani G, Serati M, Bolis P. Vaginal cuff closure after minimally invasive hysterectomy: our experience and systematic review of the literature. Am J Obstet Gynecol. 2011 Aug;205(2):119.e1-12 Hur HC, Donnellan N, Mansuria S, Barber RE, Guido R, Lee T. Vaginal cuff dehiscence after different modes of hysterectomy. Obstet Gynecol. 2011 Oct;118(4):794-801 Miller N. A new method of correcting complete inversion of the vagina: with or without complete prolapse; report of two cases. Surg Gynecol Obstet 1927;44:550–555 Crigler B, Zakaria M, Hart S. Total Laparoscopic Hysterectomy with Laparoscopic Uterosacral Ligament Suspension for the Treatment of Apical PelvicOrgan Prolapse. Surg Technol Int. 2012 Nov 18;XXII McCall ML. Posterior culdeplasty; surgical correction of enterocele during vaginal hysterectomy;a preliminary report.ObstetGynecol1957;10:595–602 Margulies RU, Rogers MA, Morgan DM. Outcomes of transvaginal uterosacral ligament suspension: systematic review and metaanalysis. Am J Obstet Gynecol. 2010 Feb;202(2):124-34 Shull BL, Bachofen C, Coates KW, Kuehl TJ. A transvaginal approach to repair of apical and other associated sites of pelvic organ prolapse with uterosacral ligaments. Am J Obstet Gynecol 2000;183:1365-74 Chung CP, Miskimins R, Kuehl TJ, Yandell PM, Shull BL. Permanent suture used in uterosacral ligament suspension offers better anatomical support than delayed absorbable suture. Int Urogynecol J. 2012 Feb;23(2):223-7 Wieslander CK, Roshanravan SM, Wai CY, et al. Uterosacral ligament suspension sutures: anatomic relationships in unembalmed female cadavers. Am J Obstet Gynecol 2007; 197:672e1–672e6 Diwan A, Rardin CR, Strohsnitter WC, et al. Laparoscopic uterosacral ligament uterine suspension compared with vaginal hysterectomy with vaginal vault suspension for uterovaginal prolapse. Int Urogynecol J Pelvic Floor Dysfunct 2006; 17:79–83. Ricci P, Solà V, Pardo J, Guiloff E. Laparoscopic McCall culdoplasty. J Minim Invasive Gynecol. 2007 Jul-Aug;14(4):397-8 Diwadkar GB, Chen CC, Paraiso MF. An update on the laparoscopic approach to urogynecology and pelvic reconstructive procedures. Curr Opin Obstet Gynecol. 2008 Oct;20(5):496-500 Dällenbach P, Kaelin-Gambirasio I, Jacob S, Dubuisson JB, Boulvain M. Incidence rate and risk factors for vaginal vault prolapse repair after hysterectomy. Int Urogynecol J Pelvic Floor Dysfunct. 2008 Dec;19(12):1623-9 Wattiez A, Mashiach R, Donoso M. Laparoscopic repair of vaginal vaultprolapse. Curr Opin Obstet Gynecol. 2003 Aug;15(4):315-9 Ceccaroni M, Berretta R, Malzoni M, Scioscia M, Roviglione G, Spagnolo E, Rolla M, Farina A, Malzoni C, De Iaco P, Minelli L, Bovicelli L. Vaginal cuff dehiscence after hysterectomy: a multicenter retrospective study. Eur J Obstet Gynecol Reprod Biol. 2011 Oct;158(2):308-13 Robinson BL, Liao JB, Adams SF, Randall TC. Vaginal cuff dehiscence after robotic total laparoscopic hysterectomy. Obstet Gynecol. 2009 Aug;114(2 Pt 1):369-71 Blikkendaal MD, Twijnstra AR, Pacquee SC, Rhemrev JP, Smeets MJ, de Kroon CD, Jansen FW. Vaginal cuff dehiscence in laparo-scopic hysterectomy: influence of various suturing methods of the vaginal vault. Gynecol Surg. 2012 Nov;9(4):393-400 Kashani S, Gallo T, Sargent A, Elsahwi K, Silasi DA, Azodi M. Vaginal cuffdehiscence in robotic-assisted total hysterectomy. JSLS. 2012 OctDec;16(4):530-6 Cronin B, Sung VW, Matteson KA. Vaginal cuff dehiscence: risk factors and management. Am J Obstet Gynecol. 2012 Apr;206(4):284-8 Ramirez PT, Klemer DP. Vaginal evisceration after hysterectomy: a literature review. Obstet Gynecol Surv. 2002 Jul;57(7):462-7 Agdi M, Al-Ghafri W, Antolin R, Arrington J, O'Kelley K, Thomson AJ, Tulandi T. Vaginal vault dehiscence after hysterectomy. J Minim Invasive Gynecol. 2009 May-Jun;16(3):313-7 Nezhat CH, Nezhat F, Seidman DS, Nezhat C. Vaginal vault evisceration after total laparoscopic hysterectomy. Obstet Gynecol. 1996 May;87(5 Pt 2):868-70 Nick AM, Lange J, Frumovitz M, Soliman PT, Schmeler KM, Schlumbrecht MP, dos Reis R, Ramirez PT. Rate of vaginal cuff separation following laparoscopic or robotic hysterectomy. Gynecol Oncol. 2011 Jan;120(1):4751 Crigler B, Zakaria M, Hart S. Total Laparoscopic Hysterectomy with Laparoscopic Uterosacral Ligament Suspension for the Treatment of Apical Pelvic Organ Prolapse. Surg Technol Int. 2012 Nov 18;XXII 19 Umek WH, Morgan DM, Ashton-Miller JA, DeLancey JOL. Quantitative analysis of uterosacral ligament origin and insertion points by magnetic resonance imaging. Obstet Gynecol. 2004 Mar;103(3):447-51 Cruikshank SH, Kovac SR. Randomized comparison of three surgical methods used at the time of vaginal hysterectomy to prevent posterior enterocele. Am J Obstet Gynecol. 1999 Apr;180(4):859-65 Salvatore S, Siesto G, Serati M. Risk factors for recurrence of genital prolapse. Curr Opin Obstet Gynecol. 2010 Oct;22(5):420-4 Rardin CR, Erekson EA, Sung VW, Ward RM, Myers DL. Uterosacral colpopexy at the time of vaginal hysterectomy: comparison of laparoscopic and vaginal approaches. J Reprod Med. 2009 May;54(5):273-80 Yazdany T, Bhatia N. Uterosacral ligament vaginal vault suspension: anatomy, outcome and surgical considerations. Curr Opin Obstet Gynecol. 2008 Oct;20(5):484-8 Uzoma A, Farag KA. Vaginal vault prolapse. Obstet Gynecol Int.2009;2009:275621 CULTURAL AND LINGUISTIC COMPETENCY Governor Arnold Schwarzenegger signed into law AB 1195 (eff. 7/1/06) requiring local CME providers, such as the AAGL, to assist in enhancing the cultural and linguistic competency of California’s physicians (researchers and doctors without patient contact are exempt). This mandate follows the federal Civil Rights Act of 1964, Executive Order 13166 (2000) and the Dymally-Alatorre Bilingual Services Act (1973), all of which recognize, as confirmed by the US Census Bureau, that substantial numbers of patients possess limited English proficiency (LEP). US Population Language Spoken at Home California Language Spoken at Home Spanish English Spanish Indo-Euro Asian Other Indo-Euro English Asian Other 19.7% of the US Population speaks a language other than English at home In California, this number is 42.5% California Business & Professions Code §2190.1(c)(3) requires a review and explanation of the laws identified above so as to fulfill AAGL’s obligations pursuant to California law. Additional guidance is provided by the Institute for Medical Quality at http://www.imq.org Title VI of the Civil Rights Act of 1964 prohibits recipients of federal financial assistance from discriminating against or otherwise excluding individuals on the basis of race, color, or national origin in any of their activities. In 1974, the US Supreme Court recognized LEP individuals as potential victims of national origin discrimination. In all situations, federal agencies are required to assess the number or proportion of LEP individuals in the eligible service population, the frequency with which they come into contact with the program, the importance of the services, and the resources available to the recipient, including the mix of oral and written language services. Additional details may be found in the Department of Justice Policy Guidance Document: Enforcement of Title VI of the Civil Rights Act of 1964 http://www.usdoj.gov/crt/cor/pubs.htm. Executive Order 13166,”Improving Access to Services for Persons with Limited English Proficiency”, signed by the President on August 11, 2000 http://www.usdoj.gov/crt/cor/13166.htm was the genesis of the Guidance Document mentioned above. The Executive Order requires all federal agencies, including those which provide federal financial assistance, to examine the services they provide, identify any need for services to LEP individuals, and develop and implement a system to provide those services so LEP persons can have meaningful access. Dymally-Alatorre Bilingual Services Act (California Government Code §7290 et seq.) requires every California state agency which either provides information to, or has contact with, the public to provide bilingual interpreters as well as translated materials explaining those services whenever the local agency serves LEP members of a group whose numbers exceed 5% of the general population. ~ If you add staff to assist with LEP patients, confirm their translation skills, not just their language skills. A 2007 Northern California study from Sutter Health confirmed that being bilingual does not guarantee competence as a medical interpreter. http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=2078538. 20








© Copyright 2026