
How to complete the enclosed documents
How to complete the enclosed documents
How to complete the enclosed Investment Account Application
If you need help completing this form, contact one of our Client Service Representatives at 1.800.387.2087
or speak with your advisor.
Section 1 (Mandatory)
Indicate the account type. If you
have an individual investment
loan, your account type will
be individual. If you have a
co-borrower, your account
type will be either Joint Rights
of Survivorship or Tenants in
Common.
You must also indicate the
intended use of the account.
For example, “investments”.
If you wish to have your
statements emailed to you,
check the “I agree…” box.
B2BBankFinancialServicesInc.("B2BBFSI")
InvestmentAccountApplication
1. AccountType(Checkoneonly)andIntendedUse
✔ Individual
a) r
r Corporation
b) r Joint Rights of Survivorship* (JTWROS; not available in Quebec)
r Unincorporated Organization (ex. Association, Charity, Condo Board, Partnership, etc.)
r Formal Trust
c) r Tenants in Common* (TIC)
•PleaseattachtheFormalTrustagreement(preparedbyclient'slegaladvisors)
d) r In Trust For* (ITF – Informal trust; includes ITF accounts with co-applicants)
•(Optional)Attachaseparatesheetwithtrustees’andbeneficiaries’addressesifdifferentfromSection2
e) r Estate: submit in Executor’s name “as executor for the estate of...”
If any of a) - d) is checked, and it is also a Group account, check here r
* Note: Attach a separate sheet for more than 2 applicants or ITF beneficiaries. Joint accounts are limited to
4 applicants. ITF accounts are limited to a combined total of 4 applicants and ITF beneficiaries.
Investing
WhatistheIntendedUseofAccount?(ie,RetirementSavings,Children’sEducation,etc.)
Electronicdeliveryofclientcommunications(includingstatements,tradeconfirmations,andtaxdocuments)isfaster,convenientandenvironmentallyconscious.Bycheckingtheboxbelow,Iwishtoreceivemyclientcommunications
✔ I agree to the foregoing.
electronically (where applicable) via the e-mail address provided below. Please send me the enrolment information for eDelivery and Investor Access. r
2. ApplicantInformation
999-999-999
BUSINESS/TRUST/OTHER ENTITY NUMBER (for tax reporting)
SOCIAL INSURANCE NUMBER
1-Mr 2-Mrs
Smith
1 3-Miss 4-Ms
LAST NAME OR COMPANY / ORGANIZATION NAME
5-Dr. 6-Prof.
123 Any Street
ADDRESS
( 555 ) 123-4567
Robert
FIRST NAME
APT.
( 555 ) 987-6543
RESIDENCE TELEPHONE NUMBER
BUSINESS TELEPHONE NUMBER
0
APT.
[email protected]
E-MAIL ADDRESS
ACME company
Canada
Canadian
CITY
POSTAL CODE
CITIZENSHIP
15
Manufacturing
Section 2 (Mandatory)
EMPLOYER ADDRESS
CITY
Complete all information in
section 2.
NATURE OF PRINCIPAL BUSINESS OR OCCUPATION
Are you: (i) an officer or director of a reporting issuer or any other issuer whose securities are
publicly traded (e.g. and entity whose securities are traded on a stock exchange or
an over-the-counter market) (an “Issuer”); or
(ii) an officer or director of a person or company which is itself an
✔ NO
r
r YES
insider or a subsidiary of such Issuer?
999 Main Street
Toronto
Human Resources Manager
If yes, please list the Issuer(s):
YEARS WITH EMPLOYER
B3B 4C4
ON
PROVINCE
POSTAL CODE
✔ NO
Are you designated as a Pro (licensed to sell securities)?
r
Doyou: (i) beneficiallyown;or
(ii) have control or direction over; or
(iii)haveacombinationofbeneficialownershipof,andcontrolordirectionover,
directly or indirectly, securities of an Issuer carrying more than 10% of the voting
✔ NO
r
rights attached to all of the Issuer’s outstanding voting securities?
r
YES
r
YES
If yes, please list the Issuer(s):
Do you or as part of a group, hold or control an Issuer?
r
YES
r
YES
✔ NO
r
If yes, please list the Issuer(s):
Pleaserefertothedefinitionof“Politicallyexposedforeignperson”(“PEFP”)andthedefinitionofprescribedfamilymember(“PrescribedFamilyMember”)includedonthisapplicationform.
✔ NO
r
Is the Applicant a PEFP or is the Applicant a PEFP because the Applicant is a Prescribed Family Member of a PEFP?
If Yes, please complete and attach the supplemental form – Politically Exposed Foreign Person Statement.
3. Co-ApplicantInformation
rCheckboxifseparatesheetattachedwithadditionalapplicants
IstheCo-Applicantthespouse/commonlawpartneroftheApplicant? r NO
r
YES
1-Mr 2-Mrs
3-Miss 4-Ms
5-Dr. 6-Prof. LAST NAME
SOCIAL INSURANCE NUMBER
(YYYY
Y Y Y Y/ M M/ /MM
DD)
DATE OF BIRTH
FIRST NAME
/ DD
INITIALS
Address: rSameasApplicant,or
ADDRESS
(
)
RESIDENCE TELEPHONE NUMBER
# OF DEPENDANTS
(
)
APT.
BUSINESS TELEPHONE NUMBER
CITY
PROVINCE
POSTAL CODE
COUNTRY*
CITIZENSHIP
* Any person who resides outside Canada is required to provide proof of citizenship
E-MAIL ADDRESS
EMPLOYER NAME
TYPE OF BUSINESS
EMPLOYER ADDRESS
CITY
PROVINCE
POSTAL CODE
Are you designated as a Pro (licensed to sell securities)?
r NO
Doyou: (i) beneficiallyown;or
(ii) have control or direction over; or
(iii)haveacombinationofbeneficialownershipof,andcontrolordirectionover,
directly or indirectly, securities of an Issuer carrying more than 10% of the voting
r NO
rights attached to all of the Issuer’s outstanding voting securities?
NATURE OF PRINCIPAL BUSINESS OR OCCUPATION
Are you: (i) an officer or director of a reporting issuer or any other issuer whose securities are
publicly traded (e.g. and entity whose securities are traded on a stock exchange or
an over-the-counter market) (an “Issuer”); or
(ii) an officer or director of a person or company which is itself an
r NO
r YES
insider or a subsidiary of such Issuer?
If yes, please list the Issuer(s):
Do not complete this section.
A1A 2B2
PROVINCE
CITY
PROVINCE
POSTAL CODE
* Any person who resides outside Canada is required to provide proof of citizenship
✔ English
Language Preference r
r French
TYPE OF BUSINESS
Section 4 (Not required)
/ 03
INITIALS
ON
EMPLOYER NAME
Complete this section only if there
is a co-applicant on this account,
including if the co-applicant is
your spouse.
( 1969
Y Y Y Y/ M M/ / D08
D)
DATE OF BIRTH
Toronto
COUNTRY*
MAILING ADDRESS IF DIFFERENT FROM ABOVE
# OF DEPENDANTS
Section 3 (Optional)
FORINTERNALUSE
YEARS WITH EMPLOYER
If yes, please list the Issuer(s):
Do you or as part of a group, hold or control an Issuer?
r
NO
If yes, please list the Issuer(s):
Pleaserefertothedefinitionof“Politicallyexposedforeignperson”(“PEFP”)andthedefinitionofprescribedfamilymember(“PrescribedFamilyMember”)includedonthisapplicationform.
Is the Co-Applicant a PEFP or is the Co-Applicant a PEFP because the Co-Applicant is a Prescribed Family Member of a PEFP?
r NO
If Yes, please complete and attach the supplemental form – Politically Exposed Foreign Person Statement.
r
YES
r
YES
r
YES
r
YES
4. InTrustForInformation-namesbelowwillbeincludedinoneaccount
•AttachaseparatesheetwithaddressesofITFindividuals(ie.beneficiaries),ifdifferentfromApplicant’saddress
LAST NAME
FIRST NAME
LAST NAME
FIRST NAME
(YYYY
Y Y Y Y/ M M/ /MM
DD)
DATE OF BIRTH
(YYYY
Y Y Y Y/ M M/ /MM
DD)
DATE OF BIRTH
/ DD
/ DD
r
Check box if separate sheet attached for
additional ITF individuals, or if ITF individual
addressisdifferentfromApplicant'saddress.
225-07-504E (01/01/2014)
How to complete the enclosed Investment Account Application — Page 2
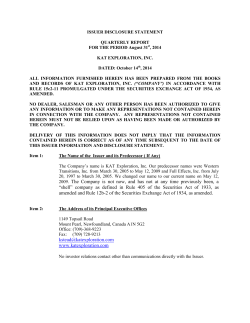
Section 5 (Optional)
The spousal information for each
of the applicants (if applicable)
should be provided in this section.
If your spouse is the co-applicant,
leave this section blank (see
section 3).
5. SpousalInformation
Applicant’sInformation(CompleteifspouseisnotaCo-Applicant)
Doyouhaveaspouse/commonlawpartner?Ifyes,completethissection
2
✔ YES
r
✔ SameasApplicant,or
Address:r
APT.
COUNTRY
CITY
1972 / 08 / 27
( Y Y Y Y/ M M / D D )
PROVINCE
Canadian
CITIZENSHIP
POSTAL CODE
ADDRESS
APT.
COUNTRY
CITY
PROVINCE
POSTAL CODE
CITIZENSHIP
YYYY / MM / DD
555-555-555
( Y Y Y Y/ M M / D D )
SOCIAL INSURANCE NUMBER
DATE OF BIRTH
EMPLOYER’S NAME
SOCIAL INSURANCE NUMBER
EMPLOYER’S NAME
1010 Centre Street
EMPLOYER’S ADDRESS
9
Financial Services
TYPE OF BUSINESS
YEARS WITH EMPLOYER
Branch Manager
Section 7 (Not required)
FIRST NAME
Address:r SameasCo-Applicant,or
ANC Financial
If you have an advisor, their
information goes here. If not,
leave it blank.
Checkboxifseparatesheetattachedwithinformationonadditionalco-applicants.
1-Mr 2-Mrs
3-Miss 4-Ms
5-Dr. 6-Prof. LAST NAME
FIRST NAME
DATE OF BIRTH
Section 6 (Optional)
Co-Applicant’sInformation(CompleteifCo-ApplicantisnotApplicant’sspouse)
Doyouhaveaspouse/commonlawpartner?Ifyes,completethissection
r NO r YES
r
Jane
Smith
1-Mr 2-Mrs
3-Miss 4-Ms
5-Dr. 6-Prof. LAST NAME
ADDRESS
r NO
NATURE OF PRINCIPAL BUSINESS OR OCCUPATION
✔ NO
r
r YES
Are you designated as a Pro (licensed to sell securities)?
Are you: (i) an officer or director of a reporting issuer or any other issuer whose securities are
publicly traded (e.g. and entity whose securities are traded on a stock exchange or
an over-the-counter market) (an “Issuer”); or
(ii) an officer or director of a person or company which is itself an
✔ NO
r
r YES
insider or a subsidiary of such Issuer?
If yes, please list the Issuer(s):
Doyou: (i) beneficiallyown;or
(ii) have control or direction over; or
(iii) haveacombinationofbeneficialownershipof,andcontrolordirectionover,
directly or indirectly, securities of an Issuer carrying more than 10% of the voting
✔ NO
r
r YES
rights attached to all of the Issuer’s outstanding voting securities?
If yes, please list the Issuer(s):
✔ NO
Do you or as part of a group, hold or control an Issuer?
r
r YES
If yes, please list the Issuer(s):
EMPLOYER’S ADDRESS
TYPE OF BUSINESS
YEARS WITH EMPLOYER
NATURE OF PRINCIPAL BUSINESS OR OCCUPATION
r NO
r YES
Are you designated as a Pro (licensed to sell securities)?
Are you: (i) an officer or director of a reporting issuer or any other issuer whose securities are
publicly traded (e.g. and entity whose securities are traded on a stock exchange or
an over-the-counter market) (an “Issuer”); or
(ii) an officer or director of a person or company which is itself an
r NO
r YES
insider or a subsidiary of such Issuer?
If yes, please list the Issuer(s):
Doyou: (i) beneficiallyown;or
(ii) have control or direction over; or
(iii) haveacombinationofbeneficialownershipof,andcontrolordirectionover,
directly or indirectly, securities of an Issuer carrying more than 10% of the voting
r NO
r YES
rights attached to all of the Issuer’s outstanding voting securities?
If yes, please list the Issuer(s):
Do you or as part of a group, hold or control an Issuer?
r NO
r YES
If yes, please list the Issuer(s):
6. DealerandFinancialAdvisorName
DEALER NAME (PLEASE PRINT)
DEALER #
FINANCIAL ADVISOR NAME (PLEASE PRINT)
FINANCIAL ADVISOR #
7. AnnualAccountFees-Themethodchosenbelow(excluding Invoice the Employer/Plan Sponsor)willapplytoallofyourannualfee
accountswithB2BBankFinancialServicesInc.("B2BBFSI")andreplacesanypreviouslychosenmethod.
I request that my annual account fees, until I direct otherwise in writing, be collected from (select one):
You do not need to complete this
section. For as long as your loan
remains active, you will not be
charged annual account fees.
A r Mychequingaccount
Section 8 (Not required)
8. BankingInformation-ForinvestmentaccountswithCo-Applicants,ifthebankaccountisnotinalltheApplicant’snames,banking
If your mutual fund(s) pay you cash
distributions, complete the Letter
of Direction for Cash Distributions
included in your package.
Section 9 (Mandatory)
Complete parts 1 and 2 of this
section
Void cheque required. This bank account will be used each year, on or about June 1, for
withdrawal of annual account fees, which will vary based on the applicable fee schedule
provided.UnpaidfeeswillbecollectedfromyourB2BBFSIaccount(s).Pleaseseetheattached
Pre-Authorized Debit (PAD) Terms & Conditions for more information on the CPA Rule H1
Requirements that apply to this fee payment option.
B
r Myindividual(notjointorITF)B2BBFSIinvestmentaccount
If an individual investment account does not exist, option C will apply.
C q MyB2BBFSIregisteredaccount(s),uptothefeeapplicableperaccount,then
frommyB2BBFSIinvestmentaccount(s),ifany.
D q InvoicetheEmployer/PlanSponsor(Available for Group accounts only.)
UnpaidfeeswillbecollectedfromyourB2BBFSIaccount(s).
informationisrequiredforeachApplicant(pleasesubmitonaseparatesheet)
0
BANK NUMBER
TRANSIT NUMBER
ACCOUNT NUMBER
ADDRESS
NAME OF CANADIAN FINANCIAL INSTITUTION
CITY
PROVINCE
POSTAL CODE
9. ShareholderCommunicationInformation
Ihavereadandunderstandthetermsunderthesection“NationalInstrument54-101ExplanationToClients”disclosedonthereverseofthisapplication.
Iagreethatthechoicesindicatedbymeapplytoallofthesecuritiesheldintheaccount.
Part1-ReceivingSecurityholderMaterials
Pleasemarkthecorrespondingboxtoshowwhatmaterialsyouwanttoreceive.Securityholdermaterialssenttobeneficialownersofsecuritiesconsistofthefollowingmaterials:(a)proxy-relatedmaterialsfor
annualandspecialmeetings;(b)annualreportsandfinancialstatementsthatarenotpartofproxy-relatedmaterials;and(c)materialssenttosecurityholdersthatarenotrequiredbycorporateorsecuritieslawto
be sent.
r IWANTto receiveALLsecurityholdermaterialssenttobeneficialownersofsecurities.
✔ IDECLINE to receive ALLsecurityholdermaterialssenttobeneficialownersofsecurities.(EvenifIdeclinetoreceivethesetypesofmaterials,Iunderstandthatreportingissuerorotherpersonorcompanyis
r
entitled to send these materials to me at its expense).
r IWANT to receive ONLY proxy-related materials that are sent in connection with a special meeting.
(Importantnote:Theseinstructionsdonotapplytoanyspecificrequestyougiveormayhavegiventoareportingissuerconcerningthesendingofinterimfinancialstatementsofthereportingissuer.Inaddition,
insomecircumstances,theinstructionsyougiveinthisclientresponseformwillnotapplytoannualreportsorfinancialstatementsofaninvestmentfundthatarenotpartofproxy-relatedmaterials.Aninvestment
fundisalsoentitledtoobtainspecificinstructionsfromyouonwhetheryouwishtoreceiveitsannualreportorfinancialstatements,andwhereyouprovidespecificinstructions,theinstructionsinthisformwith
respecttofinancialstatementswillnotapply.)
Part2-DisclosureofBeneficialOwnershipInformation
Please mark the corresponding box to show whether you DO NOT OBJECT or OBJECT to us disclosing your name, address and securities holdings to issuers of securities you hold with us and to other persons or
companies in accordance with securities law.
r IDONOTOBJECT to you disclosing the information described above.
✔ IOBJECT to you disclosing the information described above.
r
225-07-504E (01/01/2014)
Page 2 of 4
How to complete the enclosed Investment Account Application — Page 3
Section 10 (Not required)
You do not need to complete this
section.
Section 11 (Mandatory)
10. IdentityVerification(FederalLegislation*)-attachphotocopiesofID:
NAME
ID CODE
ID REFERENCE #
NAME
ID CODE
ID REFERENCE #
11. AccountInformation
Indicate “No” or “Yes” to each
question in this section and
provide an account number,
if required.
Section 12 (Mandatory)
Read the Account Agreement and
then sign and date this section.
If you have a co-applicant, they
must sign and date the
application too.
a) Is this Account to be used by or on behalf of a third party(ies)? This includes a
personwhohasafinancialinterestintheAccountorwhoexertscontrolover
the assets in the Account.
If Yes, please complete and attach the supplemental form – Third Party
Determination Statement.
b) Doesanyoneotherthanyou,theApplicant(s),haveanyfinancialinterestin
this account?
)
(If Yes, name the party
c) Do you, the Applicant(s), wish to appoint another person(s) to have full
power and authority over your account? (If yes, attach a completed Power of
Attorney, which must include the signature of and banking information – as
in Sections 8 & 10 – on the authorized individual)
✔ NO q YES
q
Doyouhaveanyaccountswithotherbrokeragefirms?
e)
Doyou,theApplicant(s),controlthetradinginanyotherB2BBFSIaccounts?
(If yes, indicate account numbers below):
Account type(s): RRSP
Account #
NO
✔ YES
r
✔ NO q YES
q
Account #
✔ NO q YES
q
12. AccountAgreement–pleaseensureallapplicantssignthissection.
PLEASEREADTHEACCOUNTAGREEMENTANDTHEDEPOSITTERMSANDCONDITIONSATTACHEDTOTHISAPPLICATIONFORIMPORTANTTERMSANDCONDITIONSTHATAPPLYTO
YOURACCOUNTANDDEPOSIT.
I/We acknowledge that I/we have read and agree to be bound by the Account Agreement terms and
conditions attached to this application. I/We undertake to advise my/our Dealer in writing of any change
to the information in this application. I/We acknowledge that I/we have read and agree to be bound by
the attached Pre-Authorized Debit (PAD) Terms and Conditions.
Privacy Protection - By signing this application form below, I/we acknowledge reading the Privacy
Protection Notice attached to this application and I/we consent to my/our personal information being
collected, held, used and disclosed (i) by each company with whom I/we have an account in the ways and
forthepurposesidentifiedinthePrivacyProtectionNoticeand(ii)bytheIntroducerDealerasnecessary
for the purpose of carrying out the functions described in clause (b) of the Account Agreement attached
tothisapplication.IfI/wehaveprovidedinformationconcerninganyotherperson,I/weconfirmthatI/we
am/are authorized to provide such information.
X
Robert Smith
SIGNATURE OF APPLICANT
X
SIGNATURE OF CO-APPLICANT
If you have an advisor, they may
complete this section. If not, leave
it blank.
r
d)
✔ NO q YES
q
I/We hereby certify that the information indicated above is complete and accurate.
Section 13 (Optional for your
advisor to complete)
YYYY / MM / DD
SelectIDCode=1=Driver’sLicense,2=Passport,3=BirthCertificate(onlyifunderage21)
PLACE OF ISSUE
EXPIRY DATE
* Notes: 1. Tocomplywithapplicablelaw,informationmustbeobtainedfromallindividualsauthorizedtogiveinstructionsontheaccountandcertainbeneficialownersoftheclientandtheiridentitiesmustbe
verified.Pleaseattachtheapplicableadditionalforms.
2. Pleasecompletetheidentityverificationforeachpersonwithauthorityoveroranyfinancialinterestintheaccount.
3. Foradditionalaccountholders,attachaseparatesheettorecordthebankinginformationandtheidentityverificationinformationforsuchpersons.
To:B2BBankFinancialServicesInc.(“B2BBFSI”)andB2BBank:IfI/wemakeaDepositwithB2BBank,or
any of its affiliates (including their successors and assigns), I/we acknowledge I/we have read and agree to
theattachedDepositTermsandConditions(capitalizedtermsareasdefinedintheattachedDepositTerms
andConditions).I/WeacknowledgethatB2BBank,oranyofitsaffiliates(includingtheirsuccessorsand
assigns) may pay my/our Dealer an upfront commission for Term Deposits and a trailing commission for
Non-Term Deposits, each based on the value of any such Term Deposit or Non-Term Deposit as described
in the attached Deposit Terms and Conditions. For a Cash Deposit held in a tax-deferred account (either
registeredornon-registered),B2BBank,oranyofitsaffiliates(includingtheirsuccessorsandassigns),
maypayB2BBFSIafeenogreaterthantheamountwhichisthedifferenceintheinterestratebetween
theprimerateofinterest(whichisvariable,subjecttofluctuation,andpostedonb2bbank.com),andthe
effectiverateofinterest(ifany)applicabletomy/ourCashDeposit,calculatedonthebalanceofmy/our
Cash Deposit on a daily basis. The maximum commissions and fees referenced herein and the Deposit
Terms and Conditions may change from time to time with Notice to me/us.
X
/ MM
/ )DD
(YYYY
Y Y Y Y/ M
M/DD
DATE
X
MM
(YYYY
Y Y Y Y/ M/ M
/ D D/ )DD
DATE
(2014
Y Y Y Y/ /M M01
/ D /D )30
DATE
SIGNATURE OF CO-APPLICANT
/ MM
(YYYY
Y Y Y Y/ M
M / D D/ )DD
DATE
SIGNATURE OF CO-APPLICANT
13. Dealer/FinancialAdvisorInformation
a) Do you have a direct or indirect interest in the Account other than an interest in
commissions charged? (If yes, give details in Financial Advisor’s Comments)
q NO q YES
Financial Advisor’s Comments:
b) Are you registered in the province in which the Applicant(s) resides?
q NO q YES
q NO q YES
SIGNATURE OF FINANCIAL ADVISOR
c)
Have you personally met the Applicant(s)?
If yes, when?
Has a credit check been done?
If Yes, what was the result (check one)
X
( YYYY
Y Y Y Y/ M/ MMM
/ D D/ )DD
DATE
X
q Personal Contact
q Walk In q Referral
q NO q YES
q Acceptable
( Y Y Y Y//MMM
M / D /DDD
)
Date YYYY
Referral by:
f)
MM
(YYYY
Y Y Y Y/ M/ M
/ D D/ )DD
DATE
BRANCH MANAGER’S APPROVAL
d) How long have you known the Applicant(s)
e) How did you come to know the Applicant(s)?
q Advertising Lead
q Phone-In
X
q Not Acceptable
MM
(YYYY
Y Y Y Y/ M/ M
/ D D/ )DD
DATE
PARTNER’S OR DIRECTOR’S ACCEPTANCE
Initialorder:
q Buy
or
Amount $
q Sell
q Solicited
or
q Unsolicited
Description
225-07-504E (01/01/2014)
Page 3 of 4
How to complete the enclosed Transfer Authorization
The information you will need to complete this form is available on statements from the mutual fund
company/companies. Speak with one of our Client Service Representatives at 1.800.387.2087 if you require
assistance or, contact your advisor.
Note: Complete one form for each mutual fund company that holds the pledged collateral for your loan.
Transfer Authorization for Non-Registered Investments
DEALER SERVICES
Section A (Mandatory)
Complete all information in this
section
A:
Client
Identification
• Thisformcanbeusedtotransfernon-registeredaccountswithexternalfinancialinstitutions.
• Dataenteredonthisformmaybescannedandstoredelectronically.
• Pleaseprintneatlytoensurecompleteness,accuracyandmachine-readability.
Account/Policy Holder Last Name
Robert
HomeTelephoneNumber
( 555 ) 123-4567
123 Any Street
Province
Toronto
Section B (Mandatory)
In this section, simply complete the
Account Type information.
999-999-999
Address
City
B:
Receiving
Institution
Information
Initial(s) Social Insurance Number
First Name
Smith
Postal Code
ON
✔ B2B Bank Financial
Receiving Institution Name
Postal Code
M5L 0A3
ON
Client Account/Policy Number
Fax Number
( 416 ) 979-0638
FOR BBS DELIVERIES ONLY USE FINS #T080
Dealer Name
Financial Advisor #
✔ Individual
Dealer Account Number
BusinessTelephoneNumber
Business Fax Number
)
(
)
✔ These assets are collateral for a B2B Bank investment loan
Estate
Corporation
UnincorporatedOrganization
Joint Rights of Survivorship
TenantsInCommon(TIC)
InTrustFor
Dealer Number
(
Account Type (Check one only)
C:
Client
Direction to
Relinquishing
Institution
CLIENT SERVICES
( 416 ) 964-0028
Province
TORONTO
Section C (Mandatory)
Contact Name
TelephoneNumber
199 BAY STREET, SUITE 610 PO BOX 35 STN COMMERCE COURT
Financial Advisor Name
Please provide:
• Relinquishing Institution Name
(the name of the mutual fund
company)
• Client Account number
B2B Bank Securities
ServicesInc.(IIROC)
Address
City
For use by
Dealers only
( 555 ) 957-6543
A1A 2B2
B2B Bank Intermediary
ServicesInc.(AMF)
ServicesInc.(MFDA)
BusinessTelephoneNumber
FormalTrust
Relinquishing Institution Name
ABC Mutual Fund Company
Address
Client Account/Policy Number
12345-67
City
Province
Postal Code
Transfer: (check one box only for asset transfer instructions)
✔ All in kind (as is)
All in cash*
All assets*, but mixed in cash and in kind; see list below or attached list
Partial*; see list below or attached list
*Please refer to statement in bold in Client Authorization section below.
Investment Amount
Section D (Mandatory)
You (and any co-applicant) must sign
and date this form. Your dealer and
financial advisor’s name is optional.
D:
Client
Authorization
In Kind
Shares/Units
In Cash
Dollars
In Kind
Shares/Units
In Cash
Dollars
In Kind
Shares/Units
In Cash
Dollars
In Kind
Shares/Units
In Cash
Dollars
Symbol and/or Certificate Number or Policy Number
Investment Description
Iherebyrequestthetransferofmyaccountanditsinvestmentsasdescribedabove.
*WHERE I HAVE REQUESTED A TRANSFER IN CASH, I AUTHORIZE THE LIQUIDATION OF ALL OR PART OF MY INVESTMENTS AND AGREE TO
PAY ANY APPLICABLE FEES, CHARGES OR ADJUSTMENTS.
Robert Smith
X
X
AUTHORIZEDCLIENTSIGNATURE(MANDATORY)
AUTHORIZEDCLIENTSIGNATURE(MANDATORY)
FINANCIALADVISORNAME
DEALERNAME
DEALER #
ADVISOR#
2 0 1 4 0 1 3 0
Y
Y
Y
Y M M D D
FORWARD TO B2B BANK DEALER SERVICES FOR PROCESSING
B2BBankDealerServicesincludesB2BBankFinancialServicesInc.(anMFDAmember),B2BBankSecuritiesServicesInc.(anIIROCmember,Member-CanadianInvestor
ProtectionFund)andB2BBankIntermediaryServicesInc.(anAMF-regulateddealeroperatinginQuebec).B2BBankisatrademarkusedunderlicense.
100-06-244E (01/22/2014)
Additional copies of the Transfer Authorization for Non-Registered Investments are available at
b2bbank.com/dealerservices
Page 4 of 4











© Copyright 2026