
Ex vivo high-definition optical coherence tomography of
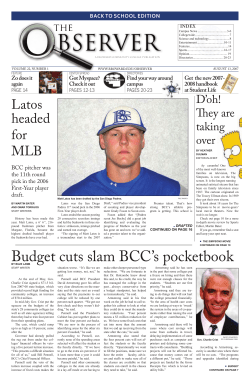
JEADV DOI: 10.1111/jdv.12063 ORIGINAL ARTICLE Ex vivo high-definition optical coherence tomography of basal cell carcinoma compared to frozen-section histology in micrographic surgery: a pilot study T. Maier,* D. Kulichová, T. Ruzicka, C. Kunte,† C. Berking† Department of Dermatology and Allergology, Ludwig-Maximilian University of Munich, Munich, Germany *Correspondence: T. Maier. E-mail: [email protected] Abstract Background Micrographic surgery is an established, but time-consuming operating procedure for facial basal cell carcinoma (BCC). A new high-definition (HD) optical coherence tomography (OCT) with high lateral and axial resolution in a horizontal (en-face) and vertical (slice) imaging mode allows a fast and non-invasive in vivo examination of BCC. Objectives To compare the diagnosis of BCC in excised tissue ex vivo by high-definition optical coherence tomography (HD-OCT) with the findings of frozen-section histology in micrographic surgery. Methods Twenty freshly excised BCC were examined by HD-OCT in the en-face and slice imaging mode divided into four sections each in concordance with the four excision margins of histography, and subsequently processed for conventional micrographic evaluation. Results A total of 80 HD-OCT images of 20 BCCs were evaluated and in 45% (9 ⁄ 20) HD-OCT correlated perfectly with the histography results. The sensitivity and specificity for the 80 evaluated HD-OCT images were 74% and 64% respectively. Conclusions High-definition optical coherence tomography allows the postoperative identification of BCC in excised tissue ex vivo, but has still limitations in the recognition of tumour margins in comparison with the micrographic evaluation of frozen sections. Received: 6 August 2012; Accepted: 9 November 2012 Conflict of Interest The high-definition optical coherence tomography device used in this study was provided by AGFA Healthcare GmbH. Dr. Maier has served as lecturer ⁄ consultant for AGFA Healthcare GmbH. Funding Sources This work was supported by the Curd-Bohnewand-Fonds of the University of Munich (to T.M.), by the Matthias Lackas Foundation and the Dr. Helmut Legerlotz Foundation (to C.B.). Introduction Basal cell carcinoma (BCC) is the most prevalent tumour in the USA, Australia and Europe1 with rising incidence.2,3 The mean age for developing BCC is 60 years, although studies show a rising incidence also in younger people of around 40 years. Tanning bed use and smoking have been shown to be independent risk factors for BCC.4 † Authors share senior coauthorship. This work is dedicated to Prof. Hans-Christian Korting who was always a source of indispensable knowledge and has recently passed away. JEADV 2012 Although it is a usually slowly growing and extremely rarely metastasizing tumour of the skin, the exact and complete excision of BCC is critical because of the locally destructive behaviour and the high propensity to recur. For this reason, micrographic surgery has been developed to reduce the recurrence rate of BCC, mainly in high-risk areas such as the face.5,6 Different approaches of micrographic surgery have been described such as the widely used Mohs surgery, the margin strip method (‘Tübinger Torte’) and the ‘Munich method’. These methods differ with regard to the technique of excision and preparation of the tumour tissue, but they have all in common the complete tumour removal with tumour-free margins at all sites to ª 2012 The Authors Journal of the European Academy of Dermatology and Venereology ª 2012 European Academy of Dermatology and Venereology Maier et al. 2 prevent local recurrence and the optimal conservation of tumourfree surrounding tissue to achieve the optimal cosmetic outcome.7–10 However, regardless of the method micrographic surgery is time-consuming, laborious and expensive. In this context, the application of new imaging techniques such as reflectance confocal microscopy and optical coherence tomography (OCT) may potentially facilitate the process of evaluating the tumour tissue immediately after excision. In a recent study, OCT was applied ex vivo for the detection of BCC before the tissue was processed for frozen sections for Mohs micrographic surgery and demonstrated a low specificity (56%) and sensitivity (19%).11 Recently, a new high-definition (HD)-OCT device has been developed, which in addition to the vertical OCT imaging mode offers a real-time horizontal ‘en-face’ imaging mode, which allows the immediate visualization of OCT pictures with high resolution in both dimensions. It could be shown recently that high-definition optical coherence tomography (HD-OCT) is useful in the detection of non-melanoma skin cancer such as BCC and actinic keratosis.12,13 In the ‘Munich method’ of micrographic surgery, the frozen tissue is also cut in horizontal sections and thus facilitating a correlation with the horizontal en-face imaging mode of HD-OCT. The purpose of this study was to evaluate the feasibility of the innovative HD-OCT in the ex vivo analysis of BCC tumour margins in comparison with the histographic analysis of the tumours as the gold standard. (speckling). According to the producer’s instruction, the penetration depth in skin in optimal conditions can be about 450– 750 lm. The resolution is 3 lm in all three dimensions according to the producer’s instruction. Skintell can work in two different modes: real-time b-scan (slice) and c-scan (en-face) and additionally allows fast capture of a 3D tomogram. The OCT probe is applied directly onto the skin with an optical gel (Skintell optical gel, AgfaHealthCare, Belgium) as coupling medium. The field of view in the en-face mode is 1.8 · 1.5 mm. The clinically suspicious lesions were systematically evaluated by HD-OCT in the slice and en-face mode and images were recorded. The lesions were examined by an experienced investigator (T.M.) prior to histographic evaluation and blinded to the histopathological result. The HD-OCT was scored positive for BCC whenever typical morphological features of BCC islands (dark ⁄ grey lobulated nodules with a dark rim) were found in the evaluated HD-OCT image as described previously by our group.12 Micrographic surgery and histopathology After the HD-OCT imaging was performed, the tissue was routinely processed for micrographic surgery according to the ‘Munich method’ as described previously.8 This method includes serial sections of the lesion in a horizontal way of sectional cutting. The histological evaluation of the frozen-cut and haematoxylineosin-stained tissue was performed by a dermatologist, experienced in the evaluation of histographic tissue, blinded to the HD-OCT result (C.K.). Patients and methods We evaluated 20 randomly selected biopsy-proven BCCs immediately after the first excision of micrographic surgery by HD-OCT. The margins of the excised fresh tissue were divided into four regions and labelled (I–IV) by the surgeons, and this was documented on a corresponding sketch. HD-OCT was then performed ex vivo placing the tissue flat on a petridish with the epidermis upside focusing on the four documented margins of the excised tissue. Multiple en-face scans were obtained at steps of 3 lm in depth. The margin was evaluated as positive if characteristic signs of BCC as described previously were recognized within the imaging field. In addition, an HD-OCT image of the centre of the excised lesion was taken. Subsequently, the tissue was processed as usual for the micrographic evaluation. High-definition optical coherence tomography (HD-OCT) The commercially available full-field HD- OCT system (Skintell, AgfaHealthCare, Belgium) was used for OCT images. The system is based on a time-domain OCT system with dynamic focus tracking, which is a synchronized motion of the imaging lens system and the reference optical system. An ultra-high-speed infrared camera is used, which allows a high scanning speed especially, in the 3D mode. The light source is a halogen lamp with a Gaussian filter and an ultra-high bandwidth centred at 1300 nm (infrared light) with high depth resolution and reduced lateral crosstalk JEADV 2012 Statistical analysis Descriptive statistics was performed to evaluate sensitivity and specificity for ex vivo HD-OCT images in reference to the histological results and P-values were determined using Chi-squared test. Statistical analysis was performed using the statistical package SPSS (Superior Performance Software System, Munich, Germany). A P-value of < 0.05 was regarded as significant. Results The 20 excised BCCs were of the following subtypes: 13 nodular, four infiltrative, one ulcerated, one nodular-infiltrative and one unclassified. The tumours were located on the nose (n = 8), on or close to the ear (n = 5), periocular (n = 4), on the forehead or temple (n = 2) and in the perioral area (n = 1) (Table 1). Four HD-OCT images per tumour were analysed according to the surgical margins (I, II, III, IV), thus 80 images were evaluated altogether. The ex vivo HD-OCT analysis of freshly excised BCCs showed typical tumour formation with grey ⁄ dark nodules often surrounded by a darker rim and bright peritumoural stroma as previously described.12 The en-face (horizontal) HD-OCT (Table 2) images of tumourous areas were matched with the horizontal sections of histography as exemplarily shown in Figs 1 and 2. The quality of ex vivo imaging did not significantly differ from HD- ª 2012 The Authors Journal of the European Academy of Dermatology and Venereology ª 2012 European Academy of Dermatology and Venereology Basal cell carcinoma in ex vivo high definition OCT 3 Table 1 Clinical and histopathological characteristics Gender Male 11 Female 9 Age range (years) 53–90 Tumour site Nose 8 Ear 5 Periocular 4 Forehead ⁄ temple 2 Perioral 1 Histopathological type Nodular 13 Infiltrative 4 Ulcerated 1 Nodular-infiltrative 1 Unclassified 1 OCT images of in vivo tissue except for tumour shrinkage and collapsed vessels; tumour islands were still recognizable as shown in Figs 1 and 2, but with slightly reduced contrast compared to in vivo tissue (data not shown). The HD-OCT imaging procedure required about 2 min per slice and en-face images, which resulted in a processing time of 8 min for four images per tumour. In nine of 20 (45%) examined tumours, the HD-OCT examination correlated exactly with the histography in all four marginal regions (Table 2). Four BCCs showed corresponding results between HD-OCT and histography in three of the four investigated margins, two BCCs in two of four margins, and three BCCs in only one of four margins. In two tumours, none of the four tumour margins was evaluated correctly by HD-OCT (Table 2). The results gained by HD-OCT were not influenced by the BCC subtype. Evaluating the 80 HD-OCT results of the marginal pictures, the sensitivity of HD-OCT in the diagnosis of BCC was 74% and the specificity was 64%. The investigated series showed a positive predictive value of 61%. Discussion Previously it has been shown that OCT is a possible tool for the imaging of BCC. The possibility to measure the tumour thickness of BCC by OCT was investigated in different studies.14–19 Recently, we could show that HD-OCT with the new en-face mode and a high lateral and axial resolution of 3 lm is a valuable tool in the diagnostics of BCC.12 (a) (b) (c) Figure 1 HD-OCT image in slice (a) and en-face mode (b, micrometre bar 200 lm) of BCC no. 17 showing the tumour margin no. II. In the slice mode (a, arrow) a darker roundish nodule is depicted at the right lateral part of the image consistent with a BCC tumour nodule as shown in the histography margin no. II (c, arrows). In the en-face mode (b, arrows), several darker oval structures are present close to the right lateral margin of the image in consistency with the histographic image (c, arrows) where blue tumour nodules and strands are found (haematoxylin–eosin staining, x2, micrometre bar 100 lm). JEADV 2012 ª 2012 The Authors Journal of the European Academy of Dermatology and Venereology ª 2012 European Academy of Dermatology and Venereology Maier et al. 4 (a) (b) (c) Figure 2 In the high-definition optical coherence tomography (HD-OCT) slice (a) and en-face mode (b, micrometre bar 200 lm) of BCC no. 19, greyish tumour strands are displayed destroying the regular architecture of the skin. The histographic image (c, arrows) shows the same tumour formations as depicted in the HD-OCT image with antlers-like blue tumour formations (arrows, haematoxylin–eosin staining, x2, micrometre bar 100 lm). This HD-OCT image was evaluated as a margin still including tumour parts in congruence with the tumour-positive histography. Table 2 Correlation of ex vivo HD-OCT and micrographic histology (MGH) in excised basal cell carcinoma (BCC, n = 20). The table shows the number of BCCs and the respective number of tumour margins (0–4) correctly identified by HD-OCT Number of MGH margins Number of correctly identified BCC by HD-OCT 4 3 2 1 0 9 4 2 3 2 In this study, the feasibility of ex vivo HD-OCT analysis of BCC was evaluated in comparison with the histographic procedure as the gold standard. As HD-OCT offers the possibility of the horizontal (en-face) imaging mode, there was a good correlation with the horizontally prepared sections for the histological evaluation. We recognized similar features of the tumour such as buds and nodules in both HD-OCT and histology. High-definition optical coherence tomography is a fast method in contrast to the time-consuming histography, but it lacks sufficient sensitivity and specificity. One main limitation of our study is that only four images of each tissue sample (one per marginal area) had been analysed and thus tumour-containing areas might have been missed. In the HD-OCT device, the imaging field is JEADV 2012 restricted to 1.8 · 0.5 mm and the penetration depth is limited to 450–750 lm in optimal conditions, whereas other OCT devices possess a scan area of 5 · 5 · 2 mm and a detection depth of about 1–2 mm. The limited penetration depth of HD-OCT does not allow a reliable evaluation of the tumour thickness in vivo. Although the advantage of HD-OCT compared to the conventional OCT is a higher resolution of about 3 lm and the possibility of a real-time en-face scanning mode, there are conventional OCT devices available with the option of 3D images but not, to our knowledge, in a real-time manner. The advantage of the ex vivo imaging is the possibility to image the tissue upside down and thus detecting the deeper layers of the excised tumour. This technique has not been performed in this pilot study, but might be an interesting goal for further studies. In consistence with Cunha et al.11 we noticed in the ex vivo scanning a shrinkage of the tissue and collapse of the vessels, but tumour islands were still visible as shown in Figs 1 and 2. To diminish the loss of image quality, a preoperative tumour scanning in vivo could be an option in further studies, although to date the size of the HDOCT probe does not allow an exact labelling of tumour margins. Here, a mapping guided by the dermoscopic image as it is possible in reflectance confocal microscopy would be helpful. Alternatively, the screening of remnants of tumour nests in the operating field after surgery could be a promising approach in the future. ª 2012 The Authors Journal of the European Academy of Dermatology and Venereology ª 2012 European Academy of Dermatology and Venereology Basal cell carcinoma in ex vivo high definition OCT In a recent study, OCT was applied ex vivo in the detection of BCC on frozen sections prepared for Mohs micrographic surgery and resulted in a low specificity (56%) and low sensitivity (19%).11 The authors speculated that further technical development might enhance the predictiveness of ex vivo OCT in the evaluation of BCC. In this study, we could show for the first time that HD-OCT with the possibility of the en-face scanning mode was able to reach a higher sensitivity (74%) and specificity (64%). But nevertheless, in the majority of cases, HD-OCT was not sufficient for a precise diagnosis of all BCC tumour margins as seen in micrographic surgery. Here, further technical developments would be necessary to reach the precision of histography, but without the time-consuming cutting and staining of the tissue. Although there are multiple studies on OCT analysis of nonmelanoma skin cancer, there is only one other study on eight periocular BCCs, which were examined ex vivo with an en-face OCT. In that study, three OCT devices were compared, but none of them reached the high resolution of HD-OCT. Nevertheless, similar to our findings, the dark tumour nodules of BCC separated clearly from the surrounding tissue by highly reflective structures and could thus easily be identified.20 Due to the low sample number, no calculation of sensitivity or specificity had been performed. Another promising imaging technique is the ex vivo reflectance confocal microscopy (RCM), which is currently studied for the evaluation of tumour margins of different skin tumours. It has already been shown that RCM is a valuable tool in the recognition of BCC21–23 and some studies have demonstrated the ex vivo RCM analysis of BCC.24–26 Schüle et al. examined 66 BCCs after preparation for histography by ex-vivo RCM, and found a sensitivity of 42% and a specificity of 77% in lateral tumour margins.27 Despite of the high resolution of RCM of about 1.5 lm, it has not been established routinely in the ex vivo diagnostics so far, although it is already very commonly used in the in vivo diagnosis of melanoma and non-melanoma skin cancer.28–30 For the in vivo examination, there is a limited penetration depth of about 250 lm, which does not allow a complete evaluation of the tumours in depth whereas in ex vivo imaging, the scanning process is not limited to a certain depth and is comparable with routine histology. One limitation is the quite time-consuming scanning and evaluation process of the RCM images and – as in OCT imaging – at present there is the lack of specific staining possibilities for the recognition of certain cell types comparable to immunohistochemistry. In this context the use of fluorescence dye might enhance tissue recognition in the future. Although innovative HD-OCT shows a certain potential for ex vivo evaluation of skin tumours, further technical developments are still necessary here. Acknowledgements This work was supported by the Curd-Bohnewand-Fonds of the University of Munich (to T.M.), by the Matthias Lackas JEADV 2012 5 Foundation and the Dr. Helmut Legerlotz Foundation (to C.B.). We thank Silke Krug for excellent technical assistance. References 1 Gilbody JS, Aitken J, Green A. What causes basal cell carcinoma to be the commonest cancer? Aust J Public Health 1994; 18: 218–221. 2 Flohil SC, de Vries E, Neumann HA, Coebergh JW, Nijsten T. Incidence, prevalence and future trends of primary basal cell carcinoma in the Netherlands. Acta Derm Venereol 2011; 91: 24–30. 3 Bath-Hextall F, Leonardi-Bee J, Smith C, Meal A, Hubbard R. Trends in incidence of skin basal cell carcinoma. Additional evidence from a UK primary care database study. Int J Cancer 2007; 121: 2105–2108. 4 Bakos RM, Kriz M, Muhlstadt M, Kunte C, Ruzicka T, Berking C. Risk factors for early-onset basal cell carcinoma in a German institution. Eur J Dermatol 2011; 21: 705–709. 5 Sterry WGC, Korting HC. EDF Guidelines for Dermatology in Europe. ABW Wissenschaftsverlag Berlin, Germany, 2009. 6 Loser C, Rompel R, Breuninger H et al. Microscopically controlled surgery (MCS). J Dtsch Dermatol Ges 2010; 8: 920–925. 7 Woerle B, Heckmann M, Konz B. Micrographic surgery of basal cell carcinomas of the head. Recent Results Cancer Res 2002; 160: 219–224. 8 Breuninger H, Schaumburg-Lever G. Control of excisional margins by conventional histopathological techniques in the treatment of skin tumours. An alternative to Mohs’ technique. J Pathol 1988; 154: 167–171. 9 Boztepe G, Hohenleutner S, Landthaler M, Hohenleutner U. Munich method of micrographic surgery for basal cell carcinomas: 5-year recurrence rates with life-table analysis. Acta Derm Venereol 2004; 84: 218–222. 10 Kunte C, Konz B. Current recommendations in the treatment of basal cell carcinoma and squamous cell carcinoma of the skin. Hautarzt 2007; 58: 419–426. 11 Cunha D, Richardson T, Sheth N, Orchard G, Coleman A, Mallipeddi R. Comparison of ex vivo optical coherence tomography with conventional frozen-section histology for visualizing basal cell carcinoma during Mohs micrographic surgery. Br J Dermatol 2011; 165: 576–580. 12 Maier T, Braun-Falco M, Hinz T, Schmid-Wendtner MH, Ruzicka T, Berking C. Morphology of basal cell carcinoma in high definition optical coherence tomography: en-face and slice imaging mode, and comparison with histology. J Eur Acad Dermatol Venereol 2012 Apr 28. doi: 10.1111 ⁄ j.1468-3083.2012.04551.x. [Epub ahead of print] 13 Maier T, Braun-Falco M, Laubender RP, Ruzicka T, Berking C. Actinic keratosis in the en-face and slice imaging mode of high definition optical coherence tomography and comparison with histology. Br J Dermatol 2012 Aug 4. doi: 10.1111 ⁄ j.1365-2133.2012.11202.x. [Epub ahead of print] 14 Mogensen M, Thrane L, Jorgensen TM, Andersen PE, Jemec GB. OCT imaging of skin cancer and other dermatological diseases. J Biophotonics 2009; 2: 442–451. 15 Mogensen M, Joergensen TM, Nurnberg BM et al. Assessment of optical coherence tomography imaging in the diagnosis of non-melanoma skin cancer and benign lesions versus normal skin: observer-blinded evaluation by dermatologists and pathologists. Dermatol Surg 2009; 35: 965–972. 16 Hinz T, Ehler LK, Hornung T, Voth H, Fortmeier I, Maier T et al. Preoperative characterization of basal cell carcinoma comparing tumour thickness measurement by optical coherence tomography, 20-mhz ultrasound and histopathology. Acta Derm Venereol 2012; 92: 132–137. 17 Gambichler T, Moussa G, Sand M, Sand D, Altmeyer P, Hoffmann K. Applications of optical coherence tomography in dermatology. J Dermatol Sci 2005; 40: 85–94. 18 Gambichler T, Jaedicke V, Terras S. Optical coherence tomography in dermatology: technical and clinical aspects. Arch Dermatol Res 2011; 303: 457–473. ª 2012 The Authors Journal of the European Academy of Dermatology and Venereology ª 2012 European Academy of Dermatology and Venereology Maier et al. 6 19 Gambichler T, Orlikov A, Vasa R et al. In vivo optical coherence tomography of basal cell carcinoma. J Dermatol Sci 2007; 45: 167–173. 20 Khandwala M, Penmetsa BR, Dey S, Schofield JB, Jones CA, Podoleanu A. Imaging of periocular basal cell carcinoma using en face optical coherence tomography: a pilot study. Br J Ophthalmol 2010; 94: 1332–1336. 21 Sauermann K, Gambichler T, Wilmert M et al. Investigation of basal cell carcinoma [correction of carcionoma] by confocal laser scanning microscopy in vivo. Skin Res Technol 2002; 8: 141–147. 22 Nori S, Rius-Diaz F, Cuevas J et al. Sensitivity and specificity of reflectance-mode confocal microscopy for in vivo diagnosis of basal cell carcinoma: a multicenter study. J Am Acad Dermatol 2004; 51: 923–930. 23 Gonzalez S, Tannous Z. Real-time, in vivo confocal reflectance microscopy of basal cell carcinoma. J Am Acad Dermatol 2002; 47: 869–874. 24 Chung VQ, Dwyer PJ, Nehal KS et al. Use of ex vivo confocal scanning laser microscopy during Mohs surgery for nonmelanoma skin cancers. Dermatol Surg 2004; 30: 1470–1478. JEADV 2012 25 Patel YG, Nehal KS, Aranda I, Li Y, Halpern AC, Rajadhyaksha M. Confocal reflectance mosaicing of basal cell carcinomas in Mohs surgical skin excisions. J Biomed Opt 2007; 12: 034027. 26 Gareau DS, Li Y, Huang B, Eastman Z, Nehal KS, Rajadhyaksha M. Confocal mosaicing microscopy in Mohs skin excisions: feasibility of rapid surgical pathology. J Biomed Opt 2008; 13: 054001. 27 Schule D, Breuninger H, Schippert W, Dietz K, Moehrle M. Confocal laser scanning microscopy in micrographic surgery (three-dimensional histology) of basal cell carcinomas. Br J Dermatol 2009; 161: 698–700. 28 González SGM, Halpern AC. Reflectance Confocal Microscopy of Cutaneous Tumors: An Atlas with Clinical, Dermoscopic and Histological Correlations. Informa Healthcare, London, 2008. 29 Hofman-Wellenhof RPG, Malvehy J, Soyer HP. Reflectance Confocal Microscopy for Skin Diseases. Springer-Verlag, Berlin, Germany, 2012. 30 Maier T, Sattler EC, Braun-Falco M, Korting HC, Ruzicka T, Berking C. Reflectance confocal microscopy in the diagnosis of partially and completely amelanotic melanoma: report on seven cases. J Eur Acad Dermatol Venereol 2012 Feb 10. doi: 10.1111 ⁄ j.1468-3083.2012.04465.x. [Epub ahead of print] ª 2012 The Authors Journal of the European Academy of Dermatology and Venereology ª 2012 European Academy of Dermatology and Venereology











© Copyright 2026