
Document 22967
CURRENT DRUG THERAPY
DOMALO S, VIDT, MD, EDITOR
TRACEY L. MERSFELDER, P H A R M D
College of Pharmacy, Ferris State University,
Grand Rapids, Michigan
Phenylpropanolamine and stroke:
The study, the FDA ruling,
the implications
ABSTRACT
HENYLPROPA.NOLAMINE
Following a recent case-control study that linked the use of
phenylpropanolamine (PPA) in diet aids to the risk of
hemorrhagic stroke, the Food and Drug Administration
requested that drug companies stop marketing products
that contain PPA. Dozens of over-the-counter and
prescription diet aids and cough and cold remedies will
need to be reformulated or discontinued. This paper reviews
the study and its implications for physicians.
KEY P O I N T S
Investigators in the Hemorrhagic Stroke Project interviewed
patients who had recently suffered a hemorrhagic stroke
and compared the prevalence of PPA use in this group with
that in a group of control subjects matched for age and sex.
In women, the odds ratio for recent use of PPA in diet aids
was 16.58 (95% C11.51-182.21, P = .02) for stroke
patients compared with control subjects. No statistically
significant relationship was found, however, between the
use of PPA-containing cough and cold remedies and stroke
in men or women, and no men in the study took PPAcontaining diet aids.
•
Possible mechanisms of PPA-induced hemorrhagic stroke
may be through hypertension, vasoconstriction, or both.
Physicians should counsel patients to avoid PPA-containing
products and to look for alternatives.
208
C L E V E L A N D C L I N I C J O U R N A L OF M E D I C I N E
VOLUME 68 • NUMBER 3
MARCH
(PPA),
a
com-
mon ingredient in dozens of cough and
cold remedies and diet aids, may cause hemorrhagic strokes in a small number of users,
according to a recent study.1'2 The risk is
small: the investigators estimated that one of
every 107,000 to3,268,000 women who take a
PPA-containing diet pill may have a PPAinduced stroke within 3 days, and no statistically significant risk could be established with
cough and cold remedies or in men.
Nevertheless, with billions of doses of PPA
products being sold in the United States,
PPA might cause up to 500 cases of hemorrhagic stroke per year.
Acting on these data, the Food and Drug
Administration (FDA) issued a warning to
consumers to immediately stop taking PPAcontaining products and asked that manufacturers voluntarily withdraw these products
immediately and replace PPA with a safer
alternative.
This paper reviews the study on which the
FDA actions were based and the implications
for physicians and patients.
WHAT IS PPA?
PPA, a sympathomimetic amine, relieves nasal
congestion via vasoconstriction, binding to
alpha-adrenergic and beta-adrenergic receptors and stimulating release of norepinephrine.
It also suppresses the appetite control center
in the hypothalamus, aiding in weight loss.
In the United States, PPA was commercially available as a combination of two
racemic structures (d- and 1-norephedrine).
2001
Downloaded from www.ccjm.org on June 15, 2014. For personal use only. All other uses require permission.
References: 1. Data on file. Pfizer Inc., New York, NY. 2. Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Summary of the second report of the National Cholesterol Education Program (NCEP) expert panel on detection,
evaluation, and treatment of high blood cholesterol in adults (Adult Treatment Panel II). Circulation. 1994;89:1329-1445.3. Jones P, Kafonek S, Laurora I, Hunninghake D, for the CURVES Investigators. Comparative dose efficacy study of atorvastatin versus
simvastatin, pravastatin, lovastatin, and fluvastatin in patients with hypercholesterolemia (the CURVES Study). Am J Cardiol. 1998;81:582-587.4. Dart A, Jerums G, Nicholson 6, et al. A multicenter, double-blind, one-year study comparing safety and efficacy
of atorvastatin versus simvastatin in patients with hypercholesterolemia. Mi J Cardiol. 1997;80:39-44.5. Bertolini S, Bon GB, Campbell LM, et al. Efficacy and safety of atorvastatin compared to pravastatin in patients withfiypercholesterolemia. Atherosclerosis.
1997;130:191-197.6. Davidson M, McKenneyJ, Stein E, etal, for the Atorvastatin Study Group I. Comparison of one-year efficacy and safety of atorvastatin versus lovastatin in primary hypercholesterolemia. Am J Cardiol. 1997;79:1475-1481.
LIPITOR® (Atorvastatin Calcium) Tablets
Brief Summary of Prescribing Information
CONTRAINDICATIONS: Active liver disease or unexplained persistent elevations of serum transaminases,
Hypersensitivity to any component of this medication. Pregnancy and Lactation—Atherosclerosis is a
chronic process and discontinuation of lipid-lowering drugs during pregnancy should have little impact on
the outcome of long-term therapy of primary hypercholesterolemia. Cholesterol and other products of
cholesterol biosynthesis are essential components for fetal development (including synthesis of steroids
and cell membranes). Since HMG-CoA reductase inhibitors decrease cholesterol synthesis and possibly
the synthesis of other biologically active substances derived from cholesterol, they may cause fetal harm
when administered to pregnant women. Therefore, HMG-CoA reductase inhibitors are contra indicated
during pregnancy and in nursing mothers. ATORVASTATIN SHOULD BE ADMINISTERED TO W O M E N OF
CHILDBEARING AGE ONLY WHEN SUCH PATIENTS ARE HIGHLY UNLIKELY TO CONCEIVE AND HAVE
BEEN INFORMED OF THE POTENTIAL HAZARDS. If the patient becomes pregnant while taking this drug,
therapy should be discontinued and the patient apprised of the potential hazard to the fetus.
WARNINGS: Liver Dysfunction — HMG-CoA reductase inhibitors, like some other lipid-lowering therapies,
have been associated with biochemical abnormalities of liver function. Persistent elevations (>3 times the
upper limit of normal [ULN] occurring on 2 or more occasions) in serum transaminases occurred in 0.7%
of patients who received atorvastatin in clinical trials. The incidence of these abnormalities w a s 0 2 % ,
0.2%, 0.6%, and 2 3 % for 10,20,40, and 80 mg, respectively. One patient in clinical trials developed jaundice. Increases in liver function tests (LFT) in other patients were not associated with jaundice or other
clinical signs or symptoms. Upon dose reduction, drug interruption, or discontinuation, transaminase levels
returned to or near pretreatment levels without sequelae. Eighteen of 30 patients with persistent LFT elevations continued treatment with a reduced dose of atorvastatin. ft is recommended that liver function tests
be performed prior to and at 12 weeks following both the initiation of therapy and any elevation of dose,
ana periodically (eg, semiannually) thereafter. Over enzyme changes generally occur in the first 3 months
of treatment with atorvastatin. Patients who develop increased transaminase levels should be monitored
until the abnormalities resolve. Should an increase in ALT or AST of >3 times ULN persist, reduction of
dose or withdrawal of atorvastatin is recommended. Atorvastatin should be used with caution in patients
who consume substantial quantities of alcohol and/or have a history of liver disease. Active liver disease
or unexplained persistent transaminase elevations are contraindications to the use of atorvastatin (see
CONTRAINDICATIONS). Skeletal Muscle — Rare cases of rhabdomyolysis with acute renal failure secondary to myoglobinuria have been reported with atonrastatin and with other drugs in this class.
Uncomplicated myalgia has been reported in atorvastatin-treated patients (see ADVERSE REACTIONS).
Myopathy, defined as muscle aches or muscle weakness in conjunction with increases in creatine phosphokinase (CPK) values >10 times ULN, should be considered in any patient with diffuse myalgias, muscle
tenderness or weakness, and/or marked elevation of CPK. Patients should be advised to report promptly
unexplained muscle pain, tenderness or weakness, particularly if accompanied by malaise or fever.
Atorvastatin therapy should be discontinued if markedly elevated CPK levels occur or myopathy is diagnosed or suspected. The risk of myopathy during treatment with other drugs in this class is increased with
concurrent administration of cyclosporine, fibric acid derivatives, erythromycin, niacin, or azole antifungals. Physicians considering combined therapy with atorvastatin and fibric acid derivatives, erythromycin,
immunosuppressive drugs, azole antifungals, or lipid-lowering doses of niacin should carefully weigh the
potential benefits and risks and should carefully monitor patients for any signs or symptoms of muscle
pain, tenderness, or weakness, particularly during the initial months of therapy and during any periods of
upward dosage titration of either drug. Periodic creatine phosphokinase (CPK) determinations may be
considered in such situations, but there is no assurance that such monitoring will prevent the occurrence
of severe myopathy. Atorvastatin therapy should be temporarily withheld or discontinued in any patient
with an acute, serious condition suggestive of a myopathy or having a risk factor predisposing to the
development of renal failure secondary to rhabdomyolysis (eg, severe acute infection, hypotension,
major surgery, trauma, severe metabolic, endocrine ana electrolyte disorders, and uncontrolled seizures).
PRECAUTIONS: General — Before instituting therapy with atorvastatin, an attempt should be made to control hypercholesterolemia with appropriate diet, exercise, and weight reduction in obese patients, and to
treat other underlying medical problems (see INDICATIONS AND USAGE in full prescribing information).
Information for Patients — Patients should be advised to report promptly unexplained muscle pain, tenderness, or weakness, particularly if accompanied by malaise or fever. Drag Interactions—The risk of
myopathy during treatment with drugs of this class is increased with concurrent administration of
cyclosporine, fibric acid derivatives, niacin (nicotinic acid), erythromycin, azole antifungals (see WARNINGS, Skeletal Muscle). Artac«/:When atorvastatin and Maalox®TC suspension were coadministered,
plasma concentrations of atorvastatin decreased approximately 35%. However, LDL-C reduction was not
altered. Antipyrine: Because atorvastatin does not affect the pharmacokinetics of antipyrine, interactions
with other drugs metabolized via the same cytochrome isozymes are not expected. Colestipol: Plasma
concentrations of atorvastatin decreased approximately 25% when colestipol and atorvastatin were coadministered. However, LDL-C reduction was greater when atorvastatin and colestipol were coadministered
than when either drug was given alone. Cimetidine: Atorvastatin plasma concentrations and LDL-C reduction were not altered by coadministration of cimetidine. Digoxin: When multiple doses of atorvastatin and
digoxin were coadministered, steady-state plasma digoxin concentrations increased by approximately
20%. Patients taking digoxin should be monitored appropriately. Erythromycin: In healthy individuals, plasma concentrations of atorvastatin increased approximately 40% with coadministration of atorvastatin and
erythromycin, a known inhibitor of cytochrome P450 3A4 (see WARNINGS, Skeletal Muscle). Oral
Contraceptives: Coadministration of atorvastatin and an oral contraceptive increased AUC values for
norethinorone and ethinyl estradiol by approximately 30% and 20%. These increases should be considered
when selecting an oral contraceptive for a woman taking atorvastatin. Warfarin: Atorvastatin had no
clinically significant effect on prothrombin time when administered to patients receiving chronic warfarin
treatment Endocrine Function — HMG-CoA reductase inhibitors interfere with cholesterol synthesis and
theoretically might blunt adrenal and/or gonadal steroid production. Clinical studies have shown that atorvastatin does not reduce basal plasma Cortisol concentration or impair adrenal reserve. The effects of
HMG-CoA reductase inhibitors on male fertility have not been studied in adequate numbers of patients. The
effects, if any, on the prtuitary-gonadal axis in premenopausal women are unknown. Caution should be
exercised if an HMG-CoA reductase inhibitor is administered concomitantly with drugs that may decrease
the levels or activity of endogenous steroid hormones, such as ketoconazole, spironolactone, and cimetidine. CNS Toxicity— Brain hemorrhage was seen in a female dog treated for 3 months at 120 mg/kg/day.
Brain hemorrhage and optic nerve vacuolation were seen in another female dog that w a s sacrificed in
moribund condition after 11 weeks of escalating doses up to 280 mg/kg/day. The 120 mg/kg dose resulted in
a systemic exposure approximately 16 times the human plasma area-under-the-curve (AUC, 0-24 hours)
based on the maximum human dose of 80 mg/day. A single tonic convulsion was seen in each of 2 male
dogs (one treated at 10 mg/kg/day and one at 120 mg/kg/day) in a 2-year study. No CNS lesions have been
observed in mice after chronic treatment for up to 2 years at doses up to 400 mg/kg/day or in rats at doses
up to 100 mg/kg/day. These doses were 6 to 11 times (mouse) and 8 to 16 times (rat) the human AUC (0-24)
based on the maximum recommended human dose of 80 mg/day. CNS vascular lesions, characterized by
perivascular hemorrhages, edema, and mononuclear cell infiltration of perivascular spaces, have been
observed in dogs treated with other members of this class, A chemically similar drug in this class produced optic nerve degeneration (Wallerian degeneration of retinogeniculate fibers) in clinically normal
dogs in a dose-dependent fashion at a dose that produced plasma drug levels about 30 times higher
than the mean drug level in humans taking the highest recommended dose. Carcinogenesis,
Mutagenesis, Impairment of Fertility — In a 2-year carcinogenicity study in rats at dose levels of 10,30,
and 100 mg/kg/day, 2 rare tumors were found in muscle in high-dose females: in one, there was a rhabdomyosarcoma and, in another, there was a fibrosarcoma. This dose represents a plasma AUC (0-24)
value of approximately 16 times the mean human plasma drug exposure after an 80 mg oral dose. A 2year carcinogenicity study in mice given 100,200, or 400 mg/kg/day resulted in a significant increase in
liver adenomas in high-dose males and liver carcinomas in high-dose females. These findings occurred
at plasma AUC (0-24) values of approximately 6 times the mean human plasma drug exposure after an
80 mg oral dose. In vitro, atorvastatin was not mutagenic or clastogenic in the following tests with and
without metabolic activation: the Ames test with Salmonella typhimurium and Escherichia coli, the
HGPRT forward mutation assay in Chinese hamster lung cells, and the chromosomal aberration
assay in Chinese hamster lung cells. Atorvastatin was negative in the in vivo mouse micronucleus test
Studies in rats performed at doses up to 175 mg/kg (15 times the human exposure) produced no changes
in fertility. There was aplasia and aspermia in tne epididymis of 2 of 10 rats treated with 100 mg/kg/day of
atorvastatin for 3 months (16 times the human AUC at the 80 mg dose); testis weights were significantly
lower at 30 and 100 mg/kg and epididymal weight was lower at 100 mg/kg. Male rats given 100 mg/kg/day for
11 weeks priorto mating had decreased sperm motility, spermatid head concentration, and increased
abnormal sperm. Atorvastatin caused no adverse effects on semen parameters, or reproductive organhistopathology in dogs given doses of 10,40, or 120 mg/kg for two years. Pregnancy—Pregnancy Category X
See CONTRAINDICATiONS. Safety in pregnant women has not been established. Atorvastatin crosses the
rat placenta and reaches a level in fetal liver equivalent to that of maternal plasma. Atorvastatin was not
teratogenic in rats at doses up to 300 mg/kg/day or in rabbits at doses up to 100 mg/kg/day. These doses
resulted in multiples of about 30 times (rat) or 20 times (rabbit) the human exposure based on surface area
(mg/m1). In a study in rats given 20,100, or 225 mg/kg/day, from gestation day 7 through to lactation day 21
(weaning), there was decreased pup survival at birth, neonate, weaning, and maturity in pups of mothers
dosed with 225 mg/kg/day. Body weight was decreased on days 4 and 21 in pups of mothers dosed at 100
mg/kg/day; pup body weight was decreased at birth and at days 4,21, and 91 at 225 mg/kg/day. Pup development was delayed (rotorod performance at 100 mg/kg/day and acoustic startle at 225 mg/kg/day; pinnae
detachment and eye opening at 225 mg/kg/day). These doses correspond to 6 times (100 mg/kg) ana 22
times (225 mg/kg) the human AUC at 80 mg/day. Rare reports of congenital anomalies have oeen received
following intrauterine exposure to HMG-CoA reductase inhibitors. There has been one report of severe congenital bony deformity, tracheo-esophageal fistula, and anal atresia (VATER association) in a baby born to a
woman who took lovastatin with dextroamphetamine sulfate during the first trimester of pregnancy. LIPITOR
should be administered to women of child-bearing potential only when such patients are highly unlikely to
conceive and have been informed of the potential hazards, If the woman becomes pregnant while taking
LIPITOR, it should be discontinued and the patient advised again as to the potential hazards to the fetus.
Nursing Mothers—Nursing rat pups had plasma and liver drug levels of 50% and 40%, respectively, of
that in their mother's milk. Because of the potential for adverse reactions in nursing infants, women taking
UPITOR should not breast-feed (see CONTRAINDICATIONS). Pediatric U s e — T r e a t m e n t experience in a
pediatric population is limited to doses of LIPITOR up to 80 mg/day for 1 year in 8 patients with homozygous
FH, No clinical or biochemical abnormalities were reported in these patients. None of these patients was
below 9 years of age. Geriatric Use — Treatment experience in adults age ¿70 years with doses of
LIPITOR up to 80 mg/day has been evaluated in 221 patients. The safety and efficacy of LIPITOR in this population were similar to tnose of patients <70 years of age.
ADVERSE REACTIONS: LIPITOR is generally well-tolerated. Adverse reactions have usually been mild and
transient In controlled clinical studies of 2502 patients, <2% of patients were discontinued due to adverse
experiences attributable to atorvastatin. The most frequent adverse events thought to be related to atorvastatin were constipation, flatulence, dyspepsia, and abdominal pain. Clinical Adverse Experiences —
Adverse experiences reported in > 2 % of patients in placebo-controlled clinical studies of atorvastatin,
regardless of causality assessment, are shown in the following table.
BODY SYSTEM
Adverse Event
Adverse Events in Placebo-Controlled Studies (% of Patients)
Placebo
Atorvastatin
Atorvastatin
Atorvastatin
10 mg
20 mg
40 mg
N = 270
N =863
N = 36
N = 79
BODY AS A WHOLE
Infection
10.0
Headache
7.0
3.7
Accidental Injury
Flu Syndrome
1.9
Abdominal Pain
0.7
Back Pain
3.0
Allergic Reaction
2.6
Asthenia
1.9
DIGESTIVE SYSTEM
Constipation
1.8
Diarrhea
1.5
Dyspepsia
4.1
Flatulence
3.3
RESPIRATORY SYSTEM
Sinusitis
2.6
Pharyngitis
1.5
SKIN AND APPENDAGES
Rash
0.7
MUSCULOSKELETAL SYSTEM
Arthralgia
1.5
Myalgia
1.1
Atorvastatin
80 mg
N =94
10.3
5.4
4.2
2.2
2.8
2.8
0.9
2.2
2.8
16.7
0.0
0.0
0.0
0.0
2.8
0.0
10.1
2.5
1.3
2.5
3.8
3.8
1.3
3.8
7.4
6.4
3.2
3.2
2.1
1.1
0.0
0.0
2.1
2.7
2.3
2.1
0.0
0.0
2.8
2.8
2.5
3.8
1.3
1.3
1.1
5.3
2.1
1.1
2.8
2.5
0.0
0.0
2.5
1.3
6.4
2.1
3.9
2.8
3.8
1.1
2.0
3.2
0.0
5.6
5.1
1.3
0.0
0.0
The following adverse events were reported, regardless of causality assessment in patients treated with
atorvastatin in clinical trials. The events in italics occurred in ¿2% of patients and the events in plain type
occurred in <2% of patients.
Body as a Whole: Chest pain, face edema, fever, neck rigidity, malaise, photosensitivity reaction, generalized edema. Digestive System: Nausea, gastroenteritis, liver function tests abnormal, colitis, vomiting,
gastritis, dry mouth, rectal hemorrhage, esophagitis, eructation, glossitis, mouth ulceration, anorexia,
increased appetite, stomatitis, biliary pain, cheilitis, duodenal ulcer, dysphagia, enteritis, melena, gum
hemorrhage, stomach ulcer, tenesmus,ulcerative stomatitis, hepatitis, pancreatitis, cholestatic jaundice.
Respiratory System: Bronchitis, rhinitis, pneumonia, dyspnea, asthma, epistaxis. Nervous System:
Insomnia, airiness, paresthesia, somnolence, amnesia, abnormal dreams, libido decreased, emotional
lability, incoordination, peripheral neuropathy, torticollis, facial paralysis, hyperkinesia, depression,
hypesthesia, hypertonia. Musculoskeletal System: Arthritis, leg cramps, bursitis, tenosynovitis, myasthenia, tendinous contracture, myositis. Skin and Appendages: Pruritus, contact dermatitis, alopecia, dry skin,
sweating, acne, urticaria, eczema, seborrhea, skin ulcer. Urogenital System: Urinary tract infection, urinary
frequency, cystitis, hematuria, impotence, dysuria, kidney calculus, nocturia, epididymitis, fibrocystic
breast vaginal hemorrhage, albuminuria, breast enlargement metrorrhagia, nephritis, urinary incontinence, urinary retention, urinary urgency, abnormal ejaculation, uterine hemorrhage. Special Senses:
Amblyopia, tinnitus, dry eyes, refraction disorder, eye hemorrhage, deafness, glaucoma, parosmia, taste
loss, taste perversion. Cardiovascular System: Palpitation, vasodilatation, syncope, moraine, postural
hypotension, phlebitis, arrhythmia, angina pectoris, hypertension. Metabolic and Nutritional Disorders:
Peripheral edema, hyperglycemia, creatine phosphokinase increased, gout, weight gain, hypoglycemia.
Hemic and Lymphatic System: Ecchymosis, anemia, lymphadenopathy, thrombocytopenia, petechia.
Postintroduction Reports—Adverse
events associated with LIPITOR therapy reported since market
introduction, that are not listed above, regardless of causality assessment include the following: anaphylaxis, angioneurotic edema, bullous rashes (including erythema multiforme, Stevens-Johnson syndrome,
and toxic epidermal necrolysis), and rhabdomyolysis.
OVERDOSAGE: There is no specific treatment for atorvastatin overdosage. In the event of an overdose,
the patient should be treated symptomatic ally, and supportive measures instituted as required. Due to
extensive drug binding to plasma proteins, hemodialysis is not expected to significantly enhance
atorvastatin clearance.
Consult package insert before prescribing LIPITOR® (Atorvastatin Calcium) Tablets,
only
January 2001
Manufactured by:
Pfizer Ireland Pharmaceuticals
Distributed by:
PARKE-DAVIS
Div of Warner-Lambert Co
A Pfizer Company
M A D E IN PUERTO RICO
BC300A0Q
© 2 0 0 1 Pfizer Inc.
All rights reserved.
Printed in USA/February 2001
U j j g j j P U.S. Pharmaceuticals
Downloaded from www.ccjm.org on June 15, 2014. For personal use only. All other uses require permission.
Other stereoisomers or combinations may also
be called phenylpropanolamine and are available in products marketed in other countries.
PPA was available a long time. First synthesized in 1910, it was initially introduced as
a parenteral medication for maintenance of
blood pressure.3 In the 1930s it began to be
widely used in oral formulations as a cold remedy, and in the 1940s its popularity grew as a
diet aid. Until the FDA ruling, PPA was available in dozens of over-the-counter diet aids
(TABLE 1 ) , cough, cold, and allergy products,
(TABLE 2), and prescription medications ( T A B L E 3 ) .
•
STROKE RISK SUSPECTED
Adverse effects reported with the use of PPA
include hypertension, dizziness, headache, agitation, psychosis, insomnia, cardiac arrhythmias, seizures, and hemorrhagic stroke.
Over the years a number of cases were
reported in which patients suffered hemorrhagic stroke after taking PPA. In a review of
the literature, Lake et al5 listed 24 such cases
reported up to 1990, and several more cases
were reported since then. 6 - 8 Other cases of
hemorrhagic stroke in PPA users have been
reported to the FDA, but this type of spontaneous reporting cannot determine an association or frequency of events.
The exact mechanism by which PPA
might cause hemorrhagic stroke is unknown.
It may be due to acute hypertension or arteritis-like vascular changes characterized by
"beading" (multiple areas of focal arterial
stenosis or constriction) or both. 9
In the early 1970s, the FDA established
the
Nonprescription
Drugs
Advisory
Committee to evaluate the safety and efficacy
of all over-the-counter medications. The committee's recommendations are published regularly in the Federal Register. Products are classified as one of the following:
• Category I (safe and effective)
• Category II (ineffective or unsafe, and
their use is prohibited)
• Category III (the data are insufficient or
conflicting, but use is allowed until publication of the final monograph).
In the late 1970s, the review board recommended that PPA be listed as a category I
drug for use in nasal decongestants, and in the
TABLE 1
Over-the-counter diet aids
that contained phenylpropanolamine*
PRODUCT
STRENGTH OF PPA
Acutrim 16-hour Steady Control
Timed-Release Tablets
75 mg
Acutrim Late Day
75 mg
Acutrim Maximum Strength Timed-Release Tablets
75 mg
AcuTrim Diet Gum
7.5 mg
Amfed T.D. Capsules
75 mg
Appedrine
25 mg
Control
75 mg
Dexatrim Caffeine Free
Extended Duration Timed-Release Tablets
75 mg
Dexatrim Caffeine Free Maximum Strength
Timed-Release Capsules
Dexatrim Caffeine Free with Vitamin C
Timed-Release Caplets
75 mg
75 mg
Dieutrim T.D. Capsules
75 mg
Permathene-16 Maximum Strength
75 mg
Permathene-16 Plus Vitamin C
75 mg
Phenoxine
25 mg
Phenyldrine
75 mg
Protrim Caplets
37.5 mg
Protrim S.R. Caplets
75 mg
Spray-U-Thin
6.58 mg
PPA = phenylpropanolamine
*Many manufacturers are reformulating their products
ADAPTED FROM OLIN BR, EDITOR. NONPRESCRIPTION DIET AIDS. DRUG FACTS AND
COMPARISONS. ST. LOUIS: FACTS & COMPARISONS, INC. 2000, AND DOERING PL. OVERWEIGHT
AND OBESITY. IN: ALLEN LV, BERARDI RR, DESIMONE EM, EDS.
HANDBOOK OF NONPRESCRIPTION DRUGS 12TH ED. 2000:476.
1980s it recommended category I listing for
PPA use in appetite suppressants, with limits
on the maximum daily dose. However, owing
to concern about adverse effects and risk of
hemorrhagic stroke, the FDA never finalized
the category I status of PPA.'O-12
In an epidemiologic study of PPA and
stroke published in 1984, 13 Jick et al concluded that if there was any risk, it was small.
These investigators looked at patients from a
group health organization, all younger than 65
years, who were identified from prescriptions
filled for PPA-containing products from 1977
29 CLEVELAND CLINIC JOURNAL OF M E D I C I N E
V O L U M E 6 8 • NUMBER 3
Downloaded from www.ccjm.org on June 15, 2014. For personal use only. All other uses require permission.
MARCH
2001
VENLAFAXINE
EFFEXORXR
HCl
EXTEND®
RBEASE
CAPSULES
Brief Summaiy
See package Insert for full prescribing information.
Indications and Usage: Effexor XR is indicated for the treatment of depression and for the treatment of Generalized
Anxiety Disorder (GAD).
Contraindications: Effexor XR is contralndlcated In patients known to be hypersensitive to veniafaxine hydrochloride.
Concomitant use in patients taking monoamine oxidase inhibitors (MAOIs) is contraindlcated (see ' Warnings")
Warnings: POTENTIAL FOR IMTEfflcnON WITH MONOAMINE OXIDASE INHIBITORS—Adverse reactions, » m e of which
were serious, have been reported in patients who have recently been discontinued from an MAOI and started on
veniafaxine, or who have recently had veniafaxine therapy discontinued prior to initiation of an MAOI. These reactions have included tremor, myoclonus, diaphoresis, nausea, vomiting, flushing, dizziness, hyperthermia with features resembling neuroleptic malignant syndrome, seizures, and death. In patients receiving antidepressants with
pharmacological properties similar to veniafaxine in combination with an MAOI, there have also been reports of
serious, sometimes ratal, reactions. For a selective serotonin reuptake inhibitor, these reactions have included
hyperthermia, rigidity, myoclonus, autonomic instability with possMe rapid fluctuations of vital signs, and mental
status changes that nciude extreme agitation progressing to delirium and coma. Some cases prraented with features resemnng neuroleptic malignant syndrome. Severe hyperthemiia and s
reported in association with the combined use of iricydic antidepressants and MAOIs. Tlnse reactions have also
been reported in patients who have recently discontinued these (hugs and have been started on an MAOI. Tin
effects of combined use of veniafaxine and MAOIs have not been evaluated In humans of animals. Therefore,
because veniafaxine is an inhibitor of both norepinephrine and serotonin reuptake, it is recommended that Effexor
XR (yenlafaxbie hydrochloride) extended release capsules not be used in combination with an MAOI, or within at
least 14 days of discontinuing treatment with an MAOI. Based on the half-life of veniafaxine, at least 7 days should
be allowed after stopping veniafaxine before starting an MAPI.
SUSTAINED HYPERTENSION—'Veniafaxine is associated with sustained increases in blood pressure in some patients.
Among patients treated with 75-375 mg per day of Effexor XR in premarketing depression studies, 3% experienced sustainedhypertension [defined as treatment-emeraent supine diastolic blood pressure ISDBP) 2 90 mm Ita and > 10 mm Hg
above baseline for 3 consecutive on-therapy visits]. Among patients treated with 75-225 mg per day of Effexor XR in premarketing GAD studies, 0.4% (2/476) experienced sustained hypertension. Experience with Immediate release veniafaxine
showed mat sustained hypertension was dose related, Increasing from 3-7% at 100-300 mg per day to 13% at doses
above 300 mg per day. An insufficient number of patients receh/ed mean doses of Effexor XR >300 mg/day to fully evaluate
the incidence of sustained increases in blood pressure at these higher doses. In premarketing depression and GAD studies,
0.7% and 0.4% of the Effexor XR-treated patients, respectively, discontinued treatment because of elevated blood pressure.
It Isrecommendedthat patientsreceivingEffexor XR have regular monitoring of blood pressure. For patients who experience a sustained increase in blood pressure, either dose reduction or discontinuation should be considered.
Precautions: GENERAL—Insomnia and Nervousness Treatment-emergent Insomnia and nervousness have been reported
for patients treated with Effexor XR. Insomnto and nervousness each led to drug discontinuation in 0.9% of the patients
treated with Effexor XR in Phase 3 depression studies. In Phase 3 GAD trials, insomnia and nervousness led to drug discontinuation In 5% and 3%, respectively, of the patients treated with Effexor XR. Changes in Appetite/Weight Treatment-emergent anorexia has been repotted in short-term depression and GAD studies. A loss of 5% or more of body weight occurred
in 7% of Effexor XR-treated and 2% of placebo-treated patients in placebo-controlled depression trials. A loss of 7% or
more of body weight occurred in 3% of the Effexor XR-treated and 0% of the placebo-treated patients in placebo-controlted
GAD trials. Activation ofMana/Hypomania Mania or hypomania has oramed during short-lemdeptKsim studies. ElfexorXR
should be used cautiously in patents with a history of mania Hyponatremia: Hyponatremia and/or the syndrome of
inappropriate antidiuretic hormone secretion (SIADH) may occur with venlalaxine. This should be taken into consideration in
patents who are, for example, volume-depleted, elderly, or taking diuretics. Mydriasis: Mydriasis has beenreportedin association with veniafaxine; therefore patients with raised intraocular pressure or at risk of acute narrow-angle glaucoma
should be monitored. Seizures No seizures occurred among Effexor XR-treated patients in short-teim trials. In all premarketing depression trials with Effexor, seizures were reported In 0.3% of venlafaxine-treated patients. Use Effexor XR cautiously in patients with a history of seizures. Discontinue in any patient who develops seizures. Skin and Mucous
Membrane Bleeding. The risk of skin and mucous membrane bleeding may be Increased in patients taking veniafaxine. As
with olfier serotonln-reuptake inhibitors, veniafaxine should be used cautiously In patients predisposed to bleeding at these
sites. Suicide. The possibility of a suicide attempt is inherent in depression and may persist until slgnfficant remission
occuis. Closely supemise high-risk patients dunng initial drug therapy. Prescriptions for Effexor XR should be written for the
smafest quantity of capsules consistent with good patient management to reduce the risk of overdose. Tfie same precautions observed when treating patients with depression should be observed when M
Use in Patients
With Concomitant Illness. Premarketing expenence with veniafaxine in patients with concomitant systemic illness is limited.
Use Effexor XR cautiously in patients with diseases or conditions that could affect hemodynamicresponsesor metabolism.
Veniafaxine has not been evaluated in patients with recent history of Ml or unstable heart disease. In short-term depression
studies electrocaidiographic changes in crarected QT interval (QTc) for Effexor XR-treated patients showed a mean increase
of 4.7 msec. In these same trials, the mean change from baseline heart rate for Effexor XR-treated patients was 4 beats
per minute. In short-term GAD studies, mean changes in OTc for Effexor XR-treated patients did not differ significantly from
placebo. The mean change from baseline heart rate for Effexor XR-treated patients in anxiety studies was 3 beats per
minute. The clinical significance of these changes is unknown. In patients with renal impairment (GFR=10-70 ml/min) or
cirrhosis of the liver, the clearances of veniafaxine and its active metabolites were decreased, thus prolonging the elimination half-lives. A lower dose may be necessary; use with caution in such patients.
INFORMATION FOR PATIENTS—Clinical studtes In healthy indmduals revealed no clinically significant impairment of psychomotor, cognitive, or complex behavior performance. However, caution patients about operating hazardous machinery,
Including automobiles, until they are reasonably sure that veniafaxine does not adverse^ affect their abilities. Tell patients to
1) notify their physician if they become pregnant or intend to become pregnant during merapy or if they are nursing; 2)
inform physician about oltier prescription or over the counter medications they are taking or plan to take; 3) avoid afconol
while taking Effexor XR: 4) notify their physician if they develop a rash, hives, or related allergic phenomena.
LABORATORY TESTS: There are no specific laboratory tests recommended.
DRUG INTERACTIONS—Cimetidine: Use with caution when administering veniafaxine with cimetidine to patients with
pre-existing hypertension or hepatic dysfunction, and the elderly.
Drugs Inhibiting Cytochrome P4502D6 Metabolism Veniafaxine is metabolized to its active metabolite, O-desmethylvenlafaxine (ODV), via cytochrome P4502D6. Drugs inhibiting this isoenzyme have the potential to increase plasma concentrations of veniafaxine and decrease concentrations of ODV. However, since the composite plasma levels of veniafaxine
and ODV are essentially unchanged in CYP2D6 poor metabolizers, no dosage adjustment is required when veniafaxine is
coadministered wNti a CYP2D6 inhibitor.
The concomitant use of veniafaxine with a drug treatments) that potential^ inhibits both CYP2D6 and CYP3A4, the primary metabolizing enzymes for veniafaxine, has not been studied. Therefore, caution is advised should a patient's thera/ include veniafaxine and any agentis) that produce simultaneous inhibition of these two enzyme systems.
nigs Metabolized by Cytochrome P450 Isoenzymes: Studies indicate that veniafaxine is a relatively weak Inhibitor of
CYP2D6. Veniafaxine did not inhibit CYP1A2 and CYP3A4 tin vitro and in vivd), CYP2C9 {in vitrdi, or CYP2C19 (it wVo).
Imipramine—Veniafaxine did not affect the pharmacokinetics of imipramine and 2-0H-imlpramlne. However,
desipramlne AUC, C™, and C mh increased by about 35% in the presence of venlalaxine. The 2-OH-desipramine AUC's
increased by 2.5-4.5 raid. Imipramine did not affect the pharmacokinetics of veniafaxine and ODV. The clinical significance
of elevated 2-OH-desipramine levels is unknown. Risperidone—Veniafaxine administered under steady-state conditions at
150 mg/day slightly inhibited the CYP2D6-mediated metabolism of risperidone (administered as a single 1 mg oral dose) to
its active metabolite, 9-hydroxyrisperidone,resultingin an approximate 32% increase in risperidone AUC. However, veniafaxine coadministration did not significantly alter the phamiacokinetic profile of the total active moiety (risperidone plus
9-hydroxyrisperidone). Indinavir—fn a study of 9 healthy volunteeis, veniafaxine administered under steady-slate conditions
at 150 mg/day resulted in a 28% decrease in the AUC of a single 800-mg oral dose of indinavir and a 36% decrease in
indinavir C ^ , . Indinavir did not affect the pharmacokinetics of venlalaxine and ODV. The clinical significance of this finding
is unknown. Monoamine Oxidase Inhibitors. See "Contraindications" and "Warnings."
CUS-Active Drugs. Use of veniafaxine with CNS-active drugs has not been systematically evaluated; use caution when
administering Effexor XR with such drugs.
Postmarketing Spontaneous Drug Interaction Reports: See "ADVERSE REACTIONS," "Postmarketing Reports."
CARCINOGENESIS, MUTAGENESIS, IMPAIRMENT OF FERTILITY—Carcinogenesis. There was no Increase in tumors in
18-month studies In mice given up to 120 mg/kg/day [1.7 times the maximum recommended human dose (MRHD) on a
mg/m 2 basis] or in 24-month studies In rats given up to 120 mg/kg/day.
Mutagenesis. Veniafaxine and ODV were not mutagenic in the Ames reverse mutation assay in Salmonella bacteria or
the Chinese hamster ovary/HGPRT mammalian cell forward gene mutation assay. Veniafaxine was not dastogenic in
several assays. ODV elicited a dastogenic response in the in vivo chromosomal aberration assay In rat bone marrow.
Impairment of Fertility. No effects on reproduction or fertility In rats were noted at oral doses of up to 2 times the MRHD
on a mg/m 2 basis.
PREGNANCY—Teratogenic Effects—Pregnancy Category C. Reproduction studies In rats given 2.5 times, and rabbfe
given 4 times the MRHD (mg/m2 basis) revealed no malformations in offspring. However, in rats given 2.5 times the
MRHD, there was a decrease in pup weight, an increase in stillborn pups, and an increase in pup deaths during the
first 5 days of lactation when dosing began during pregnancy and continued until weaning, mere are no adequate and
well-controlled studies in pregnant women; use Effexor XR during pregnancy only if clearly needed.
LABOR, DELIVERY, NURSING—The effect on labor and delivery in numans is unknown. Veniafaxine and ODV have been
reported to be excreted in human milk. Because of the potential for serious adverse reactions in nursing infants from
Effexor XR, a decision should be made whether to discontinue nursing or to discontinue the drug, taking Into account the
importance of the dnig to the mother.
PEDIATRIC USE—Safety and effectiveness In pediatric patients have not been established.
GERIATRIC USE—Approximately 4% and 3% of Effexor XR-treated patients In placebo-controlled premarketing depression
and GAD trials,respectively,were 65 years of age or over. Of 2,897 Effexor-treated patients In premarketing phase
depression studies, 12% were 65 years of age or over. No overall deferences In effectiveness or safely were observed
between geriatric patients and younger patients. However, greater sensitivity of some older individuals cannot be ruled
out As with other antidepressants, several cases of hyponatremia and syndrome of inappropriate antidiuretic hormone
secretion (SIADH) have been reported, usually In the elderiy.
Adverse Reactions: ASSOCIATED WITH DISCONTINUATION OF TREATMENT—Approximately 11 % and 23% of Effexor XR
patients In placebo-controlled clinical depression and GAD trials, respectively, discontinued treatment due to an adverse
S
event The most common events leading to discontinuation in at least 1 % of patients and at least twice that of placebo in
depression trials included: nausea, anorexia, dry mouth, dizziness, insomnia, and somnolence; in U.S. placebo-controlled
depression trials included: hypertension, diarrhea, paresthesia, tremor, abnormal (mostly blurred) vision, and abnormal
(mostly delayed) ejaculation; in GAD trials included: headache, asthenia, vasodilation, nausea, anorexia, dry mouth, dizziness, insomnia, nervousness, somnolence, thinking abnormal, tremor and abnormal vision. INCIDENCE IN CONTROLLED
TRIALS—Commonly Observed Adverse Events in Controlled Clinical faa&The most commonly observed adverse events
associated with the use of Effexor XR in placebo-controlled depression trials (incidence of 5% or greater and Incidence for
Effexor XR at least twice that for placebo): nausea (31 % vs. 12%), dizziness (20% vs. 9%), somnolence (17% vs. 8%),
abnormal ejaculation (16% vs. <1 %), sweating (14% vs. 3%), dry mouth (12% vs. 6%), nervousness (10% vs. 5%),
anorexia (8% vs. 4%), abnormal dreams (7% vs. 2%), and tremor (5% vs. 2%). In U.S. placebo-controlled depression trials,
the following were also reported wth an incidence of at least 5% and at least twice that for placebo: impotence, artorgasmia,
decreased llbkio, constipation, flatulence, Insomnia, nervousness, tremor, abnoimal vision, hypertenskxi, vasodilation, and
yawning. The most commonly observed adveise events associated wilti the use of Effexor XR in placebo-controlled GAD triate
incidence of 5% or greater and incidence for Effexor XR at least twice that for placebo): nausea (43% vs. 11 %), dry mouth
(23% vs. 5%), Insomnia (22% vs. 11%), abnormal ejaculation (17% vs. 0%), anorexia (13% vs. 2%), constipation (12% vs.
5%), nervousness (12% vs. 5%), sweating (11 % vs. <1%), abnormal vision (8% vs. 0%), yawn (6% vs. <1 %), Impotence (6%
vs. 1 %), decreased Bido (6% vs. 2%), vasodilation (6% vs. 2%), vomiting (6% vs. 2%).
Adverse Events Occumngatan Incidence of 2% or More Among Effexor XR-Treated Patients The following occurred in
short-term, placebo-controlled depression trials (up to 12 weeks) with doses of 75 to 225 mg/day, at a frequency of 2%
or more arid greater than placebo. Body as a Whole: asthenia. Cardiovascular vasodilatation, hypertension. Digestive:
nausea, constipation, anorexia, vomiting, flatulence. Metabolic/Nutritional: weight loss. Nervous System: dizziness,
somnolence, insomnia, dry mouth, nervousness, abnormal dreams, tremor, depression, paresthesia, libido decreased,
agitation. Resplratoiy System: pharyngitis, yawn. Skin: sweating. Special Senses: abnormal vision. Urogenital System:
abnormal ejaculation, impotence, anoigasmia (female). Thefollowingoccurred In short-term, placebo-controlled GAD trials (up to
8 weeks), with doses of 75 to 225 mg/day, at a frequency of 2% or more and greater than placet». Body as a Whole:
asthenia, infection, abdominal pain, fever, neck pain, chills. Cardiovascular vasodilatation, bchycardia. Digestive: nausea,
anorexia, dianhea, constipation, vomiting,flatulence.Musaioskeletal System: myalgia Nervous S y s ^ dry n w f t l n s o m a ,
dizziness, somnolence, neivousness, libido decreased, abnormal dreams, tremor, paresthesia, thinking abnormal, trismus,
twitching. Respiratory System: rtinrtis, yawn, cmgh increased. SWrc sweating. Special Senses: abnormal vision. Urogenital
System: abnoimal ejaculation, impotence, dysmenorrhea, orgasmic dysfunction (female), urinary frequency.
vital Sign Changes. In clinical depression and GAD trials, Effexor XR was associated with a mean increase in pulse rate of
about 2 beats/min. (See the "Sustained Hypertension" section of "Warnings" for effects on blood pressure.)
iaiMafary cnamss In clinical depression and GAD trials, Effexor XR was associated wiih a mean increase in serum cholesterol
concentration o f about 1.5 mg/dL and 2.5 mg/dL,respectively;clinical significance is unknown. Patients treated with Effexor
tablelsforatleast3monthsin12-monlh extension trials had a mean «rial on-lherapy Increase intotalcholesterol of 9.1 mg/dL
This Increase was duration dependent and tended to be greater with higher doses. An increase in serum cholesterol from
baseline by > 50 mg/dL and to values > 260 mg/dL, at any time after baseline, has beenrecordedIn 8.1% of patients.
ECG Charms: ISeetK "Use in stents wmCrnimitant
Illnesses" setim of "Precautions".)
OTHER EVENTS OBSERVED DURING THE PREMARKETING EVALUATION OF EFFEXOR AND EffEXOR XR—During premarketing assessment, multiple doses of Effexor XR or Effexor were administered to 4174 patients, and the following
adverse events were reported. Note: "frequent" = events occulting in at least 1/100 patients; "infrequent" = 1/100 to
1/1000 patients; "rare" = fewer than 1/1000 patients. It is Important to emphasize that although the events occuned
during treatment with veniafaxine, they were not necessarily caused by it
Body as a whole - Frequent chest pain substernal; Infrequent face edema, Intentional Injury, malaise, moniliasis, neck
rigidity, pelvic pain, photosensitivity reaction, suicide attempt; Rare: appendicitis, carcinoma, cellulitis, withdrawal
syndrome. Cardiovascular system - Frequent migraine, postural hypotension; Infrequent angina pectoris, arrhythmia,
oytrasueMo^ hypotension, peripheral vascular dismder (mainly cold feet and/or cold hands), syncope, thrombophlebitis;
is, fat-degree atrioventricular block, blgeminy, bradycarda, bundle branch block, cerebral ischemia, coronary
e heart failure, heart arrest mitral valve disorder, mucocutaneous hemonhage, myocardial Infarct
.
eructation, increased appetite; Infrequent bmxism, colitis, dysphagia, tongue
;, gastritis, gastroenteritis, gastrointestinal ulcer, gingivitis, glossitis, rectal hemorrhage, hemorrhoids,
mouth ulceration; Rare: cheilitis, cholecystitis, cholelithiasis, hematemesis, gastrointestinal hemorrhage,
hepatitis, ileitis, jaundice, intestinal obstruction, oral moniliasis, proctitis, increased salivation, soft
stools, tongue discoloration. Endocrine system - Rare: goiter, hyperthyroidism, hypothyroidism, thyroid nodule, thyroiditis.
Hemic andhrmohatic system - Frequent ecchvmosis: Infrequent: anemia, leukocytosis, leukopenia, lymphadenopathy,
thrombocythemla, thrombocytopenia; Rare: basophilia, cyanosis, eoslnophllia, lympnocytos'
Frequent edema, weight gain; Infrequent alkaline phosphatase increased, glycosuria, h
glycemia, hyperuricemia, hypoglycemia, hypokalemia, SGOT increased, thirst; Rare: al
>1 intolerance, biliroblnemia,
Jetal system - Frequent arthralgia; Infrequent arthritis, arthrosis, bone pain, bone spurs, bursitis, leg cramps,
myasthenia, tenosynovitis; Rare: pathological fracture, myopathy, osteoporosis, osteosclerosis, rheumatoid arthritis, tendon rupture. Nervous system - Frequent amnesia, confusion, depersonalization, emotional lability, hypesthesia, vertigo;
Infrequent apathy, ataxia, clrcumoral paresthesia, CNS stimulation, euphoria, hallucinations, hostility, hyperesthesia,
hyperKinesia, hypotonia, incoordination, libido increased, manic reaction, myoclonus, neuralgia, neuropathy, paranoid
reaction, psychosis, seizure, abnormal speech, stupor; Rare: akathisia, akinesia, alcohol abuse, aphasia, bradykinesia,
buccoglossal syndrome, cerebrovascular accident loss of consciousness, delusions, dementia, dystonia, facial paralysis,
abnormal gait Gulllaln-Batre Syndrome, hypokinesia, neuritis, nystagmus, psychotic depression, reflexes decreased,
reflexes Increased, suicidal Ideation, torticollis. Respiratory system - Frequent dyspnea; Infrequent asthma, chest
congestion, epistaxis, hyperventilation, laryngismus, laryngitis, pneumonia, voice alteration; Rare: atelectasis, hemoptysis, hypoventilation, hypoxia, pleurisy, pulmonary embolus, sleep apnea. Skin and appendages - Frequent rash, pruritus;
Infrequent acne, alopecia, brittle nails, contact dermatitis, dry skin, eczema, skin hypertrophy, maculopapular rash,
psoriasis, urticaria; Rare: erythremia nodosum, exfoliative dermatitis, lichenoid dermatitis, hair discoloration, skin discoloration, furunculosis, hirsutism, leukoderma, pustular rash, veslculobullous rash, seborrhea, skin atrophy, skin striae.
Special senses - Frequent abnormally of accommodation, mydriasis, taste perversion; Infrequent cataract, conjunctivitis, corneal lesion, diplopia, dry eyes, exophthalmos, eye pain, hyperacusls, otitis media, parosmia, photophobia, taste
loss, visual field defect; Rare: blepharitis, chromatopsia, conjunctival edema, deafness, glaucoma, retinal hemorrhage,
subconjunctival hemonhage, keratitis, labyrinthitis, mtosis, papilledema, decreased pupillary reflex, otitis externa, sderitis,
uveitis. Urogenital system - Frequent metrorrhagia,* prostatitis," urination impaired, vaginitis*; Infrequent albuminuria,
amenoirhea,* cystitis, dysuria, hematuria, female lactation,* leukorrhea,* menoirtiagia,* nocturia, bladder pain, breast
pain, polyuria, pyuria, unnary incontinence, urinary retention, urinary urgency, vaginal hemorrhage*; Rare: abortion,*
anuria, breast engorgement breast enlargement, fibrocystic breast calcium crystalluria, cervicitis,* ovarian cyst,* prolonged erection,* gynecomastia (male),* hypomenorrhea,* kidney calculus, kidney pain, kidney function abnormal, mastitis,
menopause,* pyelonephritis, oliguria, salpingitis,* urolithiasis, uterine hemorrhage,* uterine spasm* ('Based on the
number of men and women as appropriate.)
Posbiiaiketing Reports: Voluntary reports of other adverse events temporally associated w i h the use of Effexor (the
immediate release form of veniafaxine) that have been received since market introduction and that may have no causal
relationship with the use of Effexor include the following: agranulocytosis, anaphylaxis, aplastic anemia, catatonia,
congenital anomalies, CPK increased, deep vein thrombophlebitis, delirium, EKG abnormalities (such as atrial fibrillation,
supraventricular tachycardia, ventricular extrasystoles, ventricular tachycardia), epidermal necrosis/Stevens-Johnson
Syndrome, erythema multiforme, extrapyramidal symptoms (including tardive dyskinesia), fatigue, hemonhage (including
eye and gastrointestinal bleeding), hepatic events (including GGT elevation; abnormalities of unspecified liver function
tests; liver damage, necrosis, or failure; and fatty liver), Involuntary movements, LDH Increased, neuroleptic malignant
syndrome-like events (including a case of a 10-year-old who may nave been taking methylphenidate, was treated and
recovered), pancreatitis, panic, prolactin increased, renal failure, serotonin syndrome, shock-like electrical sensations
(in some cases, subsequent to the discontinuation of Effexor or tapering of dose), and syndrome of inappropriate antidiuretic hormone secretion (usually In the elderly).
There have been reports of elevated clozapine levels that were temporal^ associated with adverse events, Including
secures, following the addition of veniafaxine. There have been reports of Increases In prothrombin time, partial thromboplastin time, orlNR when veniafaxine was given to patients receiving warfarin therapy.
Drug Abuse and Dependence: Effexor* XR is not a controlled substance. Evaluate patients carefully for history of drug
abuse and observe such patients closely for signs of veniafaxine misuse or abuse (e.g., development of tolerance, Incrementation of dose, drug-seeking behavior).
OVERDOSAGE: In premarketing evaluation of Effexor XR for depression, there were 2 reports of acute overdosage (6 g of
Effexor XR with 2.5 mg of lorazepam, and 2.85 g of Effexor XR). Both recovered without sequelae. In premarketing evaluation of Effexor, there were 14 reports of acute overdosage (highest dose was 6.75 g). All patients recovered without
sequelae. Most patients reported no symptoms. Symptoms observed included somnolence, generalized convulsions,
prolongation of OTc to 500 msec (compared with 405 msec at baseline) in one case, and mild sinus tachycardia In
premarketing evaluation of Effexor XR for GAD, there were 2 reports of acute overdosage (0.75 g of Effexor XR and
200 mg of paroxetine and 50 mg of Zolpidem, and 1.2 g of Effexor XR). Both recovered without sequelae. In postmarketing
experience, overdose with veniafaxine has occurred predominantly In combination w'rth alcohol and/or other drugs.
Bedrocardiogram changes (e.g, prolongation of QT interval, bundle branch block, QRS prolongation), sinus and venficular
tachycardia, bradycardia, hypotension, altered level of consciousness (ranging from somnolence to coma), seizures,
vertigo, and death have been reported.
Treatment should consist of those general measures employed in the management of overdosage with any antidepressant Ensure an adequate airway, oxygenation and ventilation. Monitor cardiac rhythm and vital signs. General supportive
and symptomatic measures are also recommended. Induction of emesis is not recommended. Gastric lavage with a large
bore orogastric tube with appropriate aiiway protection, if needed, may be Indicated if performed soon after ingestion or in
symptomatic patients. Activated charcoal should be administered. Due to the large volume of distribution ofthis drug,
forced diuresis, dialysis, hemoperfuslon, and exchange transfusion are unlikely to be of benefit No specific antidotes for
veniafaxine are known. In managing overdosage, consider the possibility of multiple drug involvement The physician
should consider contacting a poison control center for additional information on the treatment of any overdose. Telephone
numbers for certified poison control centers are listed in the Physicians' Desk Reference® (PDR).
SWITCHING PATIENTS TO OR FROM A MONOAMINE OXIDASE INHIBITOR: At least 14 days should elapse between
discontinuation of an MAOI and initiation of therapy with Effexor XR. In addition, at least 7 days should be allowed after
stopping Effexor XR before starting an MAOI (see "Contraindications" and "Warnings").
Please consult full prescribing Information for detailed dosing instructions.
This brief summary is based on the circular 5044-5, revised April 14,2000.
WYETH-AYERST
W |LABORATORIES
Philadelphia, PA 19101
© 2000, Wyeth-Ayerst Laboratories
Downloaded from www.ccjm.org on June 15, 2014. For personal use only. All other
uses require permission.
l
80372-00
to 1981. They calculated that the relative risk
for having a hemorrhagic stroke when taking
PPA was 0.58 (95% CI 0 . 0 3 - 2 . 9 ) — ie, there
was a non-statistically significant trend
toward fewer strokes in PPA users than in
nonusers.
This study probably was not large enough
to detect a difference in stroke incidence
between users and nonusers of PPA in prescription products, and it did not alleviate
concerns about PPA. Both the FDA and the
manufacturers of PPA-containing products
recommended another study be conducted to
evaluate the risk of hemorrhagic stroke from
taking PPA. As a result of this recommendation, the Hemorrhagic Stroke Project was
formed.
•
THE HEMORRHAGIC STROKE PROJECT
The Hemorrhagic Stroke Project 1 ' 2 was a casecontrol study, which identified a group of
stroke patients and compared them with a similar group of healthy people to see if there were
statistically significant differences in the prevalence of PPA use between the two groups.
Inclusion criteria
Patients with symptomatic subarachnoid or
intracerebral hemorrhage were recruited at 43
hospitals in the United States between
December 1994 and July 1999. Subarachnoid
hemorrhage was diagnosed on the basis of
clinical symptoms and specific diagnostic
information, and intracerebral hemorrhage
was diagnosed by symptoms and a computed
tomographic scan.
Female and male patients were eligible if
they:
• Were between the ages of 18 and 49 years,
• Could undergo a complete interview,
• Did not have a history of a brain lesion,
and
• Did not have a previous history of stroke.
Two control subjects, matched for age and
sex, were identified for each patient within 30
days of the patient's stroke.
Why this particular mix? The main objective of the study was to evaluate the risk of
hemorrhagic stroke in women 18 to 49 years
of age. This age range was selected on the
basis of demographic data from reported cases
in the literature. In the review by Lake et al,5
all but three of the strokes were in people
within this age range, and about 6 6 % of cases
were in women. Other cases reported after
this review6.7 were in women ages 17 to 36.
One reported case was in an infant. 8
Although only a few reported cases were in
men, the investigators wanted to evaluate
potential risk in both sexes.
Methods
Stroke patients and control subjects were
asked during a structured interview whether
they had any cold symptoms during the 2
weeks before the stroke (or the same 2 weeks
for the matched control subjects), whether
they had taken any medications to treat the
cold, and whether they had taken any other
medications during this period. They were also
specifically asked about the use of particular
medications or classes of medications. To verify information about medications, they were
asked to show the package, if available, and to
pick out the medications they took from a
book containing photographs of packages.
Similarities a n d differences
b e t w e e n t h e groups
T h e stroke patients (N = 702) and the
matched control subjects (N = 1,376) did not
differ significantly in age, sex, history of diabetes, use of oral contraceptives, or cold or
influenza-like symptoms.
The stroke patients, however, had higher
rates of risk factors for stroke such as hypertension, smoking, and family history of hemorrhagic stroke. Compared with the matched
controls, more of the stroke patients were
black, more had used cocaine on the day of the
stroke or the preceding day, more used alcohol
regularly, and more had used a product that
contained nicotine or caffeine in the 3 days
preceding the stroke. The stroke patients also
had a lower average level of education, and
fewer of them had used non-steroidal antiinflammatory drugs in the 3-day window.
Only 6 women
in the stroke
group had
taken a PPA
diet aid
M o r e w o m e n stroke patients
t o o k PPA diet aids
Of the 383 stroke patients who were women, 6
(1.8%) had taken a diet pill that contained PPA
within the 3 days preceding their stroke, corn-
31 C L E V E L A N D C L I N I C J O U R N A L OF M E D I C I N E
V O L U M E 68 • NUMBER 3
Downloaded from www.ccjm.org on June 15, 2014. For personal use only. All other uses require permission.
MARCH
2001
PHENYLPROPANOLAMINE
MERSFELDER
TABLE 2
O v e r - t h e - c o u n t e r cough and cold products t h a t contained p h e n y l p r o p a n o l a m i n e *
PRODUCT
32
STRENGTH OF PPA
PRODUCT
STRENGTH OF PPA
Allerest Maximum Strength 12 Hour Caplets
75 mg
Coricidin Maximum Strength Sinus Headache
12.5 mg
Alka-Seltzer Cold Medicine
20 mg
Covangesic
12.5 mg
Alka-Seltzer Plus Cold Tablets
24.08 mg
Dapacin Cold
12.5 mg
Alka-Seltzer Plus Cold & Cough
20 mg
Demazin Syrup
12.5 mg/5 mL
Alka-Seltzer Plus Cold & Cough Medicine
Effervescent Tablets
20 mg
Demazin Tablets
25 mg
Diamaphen Elixir
12.5 mg/5 mL
Alka-Seltzer Plus Night-Time Cold
20 mg
Diamaphen Release
75 mg
Anatuss Syrup
25 mg/5 mL
Diamaphen Tablets
25 mg
Antihist-D tablets, extended release
75 mg
Dimetapp 4-Hour Liqui-Gels
25 mg
A.R.M.
25 mg
Dimetapp Cold & Allergy Chewable Tablets
BC Cold-Sinus Powder
25 mg
Dimetapp Cold & Flu
12.5 mg
BC Cold-Sinus-Allergy Powder
25 mg
12.5 mg/5 mL
Dimetapp Cold & Cough Maximum
Strength Liqui-Gels
25 mg
Bromaline Elixir
Bromanate Elixir
12.5 mg/5 mL
Dimetapp DM Elixir
12.5 mg/5 mL
Bromatapp
75 mg
Dimetapp Elixir
12.5 mg/5 mL
6.25 mg
Children's Allerest
9.4 mg
Dimetapp Extentabs
75 mg
Cheracol Plus Liquid
8.3 mg/5 mL
Dimetapp Tablets
25 mg
Chlor-Rest
18.7 mg
Duadacin
12.5 mg
Chlor-Trimeton Allergy-Sinus
12.5 mg
Entac
20 mg/5 mL
Cold & Allergy Elixir
12.5 mg/5 mL
Entex Liquid
20 mg/5 mL
Cold & Allergy DM
12.5 mg/5 mL
Gelpirin-CCF
12.5 mg
Cold-Gest Cold Capsules
75 mg
Genamin Cold Syrup
Cold Relief
12.5 mg
Genamin Expectorant Liquid
12.5 mg/5 mL
Coldloc Elixir
20 mg/5 mL
Genatap Elixir
12.5 mg/5 mL
Comtrex Liqui-Gels
12.5 mg
Gencold
75 mg
Comtrex Maximum Strength Cold & Flu
Relief Non-Drowsy Liqui-Gels
12.5 mg
GuiaCough CF Liquid
12.5 mg/5 mL
Guaifenex Liquid
20 mg/5 mL
Comtrex Maximum Strength Cold/Flu
Relief Liqui-Gels
12.5 mg
Guiatuss CF Liquid
12.5 mg/5 mL
Comtrex Max Strength Multi-Symptom
Cold & Flu Relief Liqui-Gels
12.5 mg
Histosal
20 mg
Conex Syrup
12.5 mg/5 mL
Congestant D
12.5 mg
Contac Maximum Strength 12 Hour Caplet
75 mg
Contac Severe Cold & Flu Maximum
Strength Caplets
12.5 mg
Contuss Liquid
20 mg/5 mL
Coricidin D
12.5 mg
C L E V E L A N D C L I N I C J O U R N A L OF M E D I C I N E
V O L U ME 6 8 • N U M B E R 3
Ipsatol Cough Formula Liquid for Children
and Adults
6.25 mg/5 mL
9 mg/5 mL
Kophane Cough & Cold Formula Liquid
12.5 mg/5 mL
Maximum Strength Cold & Allergy
4-Hour Liquid Gelcaps
25 mg
Maximum Strength Comtrex Liqui-Gels
12.5 mg
Myminic Expectorant Liquid
12.5 mg/5 mL
Myminicol Liquid
12.5 mg/5 mL
Naldecon DX Adult Liquid
12.5 mg/5 mL
MARCH
2001
Downloaded from www.ccjm.org on June 15, 2014. For personal use only. All other uses require permission.
S T R E N G T H OF PPA
PRODUCT
STRENGTH OF PPA
PRODUCT
Naldecon DX Children's Syrup
6.25 mg/5 mL
Tavist D
75 mg
Naldecon DX Pediatric Drops
6.25 mg/1 mL
Teldrin 12-Hour Allergy Relief Capsules
75 mg
Naldecon EX Children's Syrup
6.25 mg/5 mL
Temazin Cold Syrup
12.5mg/5mL
Naldecon EX Pediatric Drops
6.25 mg/1 mL
Threamlne DM Syrup
12.5mg/5mL
12.5 mg/5 mL
Nadelate DX Adult Liquid
12.5 mg/5 mL
Thera-Hlst Syrup
Night-Time Effervescent Cold Tablets
15 mg
Triactin
6.25 mg/5 mL
Orthoxicol Cough Syrup
8.3 mg/5 mL
Triactin Syrup
Pedicon DX Pediatric Drops
6.25 mg/1 mL
Triaminic-12
75 mg
Pediacon DX Children's Syrup
6.25mg/5 mL
Triaminic Allergy
25 mg
Pediacon EX Pediatric Drops
6.25 mg/1 mL
Triaminic Chewable Tablets
Pediatuss D.E. Drops
6.25 mg/1 mL
Triaminic Cold
12.5 mg/5 mL
Pediatuss Liquid
Phenadex Children's Cough/Cold Drops
6.25 mg/1 mL
Phenadex Pediatric Cough and Cold Drops
6.25 mg/1 mL
6.25 mg/5 mL
6.25 mg
12.5 mg
Triaminic DM Cough Relief Syrup
6.25 mg/5 mL
Triaminic Expectorant, Chest & Head
Congestion Liquid
6.25mg/5 mL
Pyrroxate Caplet
25 mg
Triaminic Expectorant Liquid
6.25 mg/5 mL
Rescon Liquid
12.5 mg/5 mL
Triaminic Syrup
6.25 mg/5 mL
Rhinocaps
20 mg
Triaminic Syrup Cold & Allergy
6.25 mg/5 mL
Robafen CF Liquid
12.5 mg/5 mL
Trlaminicin Cold, Allergy, Sinus Tablets
25 mg
Robatussin-CF Liquid
12.5 mg/5 mL
Triaminicol Multi-Symptom Cough and Cold
12.5 mg
Saleto-CF
12.5 mg
12.5 mg/5 mL
Saleto-D
18 mg
Triaminicol Multi-Symptom Cough
and Cold Liquid
6.25 mg/5 mL
Silactin Expectorant
Triaminicol Multi-Symptom Relief Colds
with Coughs Liquid
6.25 mg/5 mL
Silactln Syrup
12.5 mg/5 mL
Tricodene Forte Liquid
12.5 mg/5 mL
Silaminic Expectorant Liquid
12.5 mg/5 mL
Tricodene NN Liquid
12.5 mg/5 mL
Tricodene Pediatric Cough & Cold Liquid
12.5 mg/5 mL
Triminol Cough Syrup
12.5 mg/5 mL
Tri-Nefrin Extra Strength
25 mg
Triphenyl Expectorant Liquid
12.5 mg/5 mL
Sildicon-E Pediatric Drops
6.25 mg/1 mL
Siltapp with Dextromethorphan HBrCold
& Cough Elixir
12.5 mg/5 mL
Siltussin-CF Liquid
12.5 mg/5 mL
Sil-Tex Liquid
20 mg/5 mL
Sinapils
12.5 mg
Sinulin
25 mg
Snaplets-DM Granules
6.25 mg
Snalplets-EX Granules
6.25 mg
Snaplets-Multi Granules
6.25 mg
Spec-T Sore Throat/Decongestant Lozenges
10.5 mg
Statuss Expectorant Liquid
12.5 mg/5 mL
St. Joseph Cold Tablets for Children
3.125 mg
Triphenyl Syrup
6.25 mg/5 mL
Tussin CF Liquid
12.5 mg/5 mL
Vicks DayQuil Allergy Relief 4-Hour Tablets
25 mg
Vlcks DayQuil Allergy Relief 12 Hour Tablets
75 mg
Vicks DayQuil Sinus Pressure & Congestion
Relief Caplets
25 mg
PPA = phenylpropanolamine
' M a n y manufacturers are reformulating their products
ADAPTED FROM OLIN BR, EDITOR. RESPIRATORY COMBINATION PRODUCTS. DRUG FACTS
AND COMPARISONS. ST. LOUIS: FACTS & COMPARISONS, INC. 2000, AND TIETZE KJ. DISORDERS RELATED TO COLD AND ALLERGY. IN: ALLEN LV, BERARDI RR, DESIMONE EM, EDS.
HANDBOOK OF NONPRESCRIPTION DRUGS 12TH ED. 2000:183-184.
33 C L E V E L A N D C L I N I C J O U R N A L OF M E D I C I N E
VOLUME 68 • NUMBER 3
Downloaded from www.ccjm.org on June 15, 2014. For personal use only. All other uses require permission.
MARCH
2001
PHENYLPROPANOLAMINE
TABLE
MERSFELDER
3
Prescription products that contained
STRENGTH OF PPA
PRODUCT
Alumadrine
Ami-Tex LA
Anatuss
Aquatab C
Aquatab D
Atrohist Plus
Bromanate DC Cough Syrup
Bromphen DC w/ Codeine Cough Syrup
Bromphen/DM/PPA Syrup
Bromphen T.D.
Brompheniramine DC
Codamine Pediatric Syrup
Codamine Syrup
Codegest Expectorant Liquid
Coldloc-LA
Conex with Codeine Syrup
Cophene-X
Deconhist L.A.
Dimetane-DC Cough Syrup
Drize
Dura-Gest
Dura-Vent
Dura-Vent/A
Enomine
Endal Expectorant Syrup
Entex
Entex LA
Exgest LA
Guaifenex PPA 75
Guaipax
25 mg
75 mg
25 mg
75 mg
75 mg
50 mg
12.5 mg/5 mL
12.5 mg/5 mL
12.5 mg/5 mL
15 mg
12.5 mg/5 mL
12.5 mg/5 mL
25 mg/5 mL
12.5 mg/5 mL
75 mg
12.5 mg/5 mL
10 mg
50 mg
12.5 mg/5 mL
75 mg
45 mg
75 mg
75 mg
45 mg
12.5 mg/5 mL
45 mg
75 mg
75 mg
75 mg
75 mg
phenylpropanolamine*
Guiatex
Guiatex LA
Guiatex Liquid
Histade
Histalet Forte
Hista-Vadrin
Histex HC Syrup
Histine DM Syrup
Hycomine Pediatric Syrup
Hycomine Syrup
Hydrocodone PA Pediatric Syrup
Hydrocodone PA Syrup
lohist Elixir
lohist DM Syrup
Liqui-Histine-D Elixir
Liqui-Histine DM Syrup
Myphetane DC Cough Syrup
Naldecon
Naldecon CX Adult Liquid
Naldelate Pediatric Syrup
Naldelate Syrup
Nalgest
Nalgest Pediatric Drops
Nalgest Pediatric Syrup
Nalgest Syrup
Naldecon Pediatric Drops
Naldecon Pediatric Syrup
Naldecon Syrup
Nolamine
Norel Plus
pared with 1 (0.1%) of the 750 control subjects
who were women. After adjusting for the higher prevalence of risk factors for stroke (smoking,
hypertension, black race, and lower education)
among the stroke patients, the investigators calculated the odds ratio for having taken a PPA
diet pill among women stroke patients at 16.58
(95% CI 1.51-182.21; P = .02).
What is an odds ratio? An odds ratio is
the ratio of the odds of an event occurring in
one group to the odds of the event in another
group. This differs somewhat from the more
commonly used relative risk, which is the ratio
of the percentages of people in each group who
had the event. Without adjustment, the odds
34
C L E V E L A N D C L I N I C J O U R N A L OF M E D I C I N E
V O L U ME 68 • NUMBER 3
S T R E N G T H OF PPA
PRODUCT
MARCH
45 mg
75 mg
20 mg/5 mL
75 mg
50 mg
40 mg
6 mg/5 mL
12.5 mg/5 mL
12.5 mg/5 mL
25 mg/5 mL
12.5 mg/5 mL
25 mg/5 mL
12.5 mg/5 mL
12.5 mg/5 mL
12.5 mg/5 mL
12.5 mg/5 mL
12.5 mg/5 mL
40 mg
12.5 mg/5 mL
5 mg/5 mL
20 mg/5 mL
40 mg
5 mg/1 mL
5 mg/5 mL
20 mg/5 mL
5 mg/1 mL
5 mg/5 mL
20 mg/5 mL
50 mg
25 mg
ratio in this study would be: (6 women stroke
patients taking PPA / 377 women stroke
patients not taking PPA) / (91 women control
subjects taking PPA / 749 women control subjects not taking PPA) = approximately 12. An
odds ratio of 1, like a relative risk of 1, would
indicate no difference between the groups.
T h e association was only in women, and
only with diet aids. None of the men in the
study had taken a PPA-containing diet pill—
not one. For women who used PPA-containing cough or cold remedies, the odds ratio was
only 1.54, which was not statistically significant. For men who had taken a PPA-containing cough or cold remedy the odds ratio was
2001
Downloaded from www.ccjm.org on June 15, 2014. For personal use only. All other uses require permission.
VIOXX* (rofecoxib tablets and oral
suspension)
Brief Summary of Prescribing Information
INDICATIONS AND USAGE: VIOXX is indicated for: relief of the signs and symptoms of osteoarthritis (OA); management of acute pain in adults; treatment of primary dysmenorrhea.
CONTRAINDICATIONS: VIOXX is contraindicated in patients with known hypersensitivity to rofecoxib or any other component of VIOXX.
VIOXX should not be given to patients who have experienced asthma, urticaria,
or
. - allergic-type reactions after taking aspirin or other nonsteroidal anti-inflammatory drugs (NSAIDs). Severe, rarely fatal, anaphylactic-like reactions to NSAIDs
NSAir
have been reported in such patients (see WARNINGS, Anaphylactoid
Reactio...
and PRECAUTIONS, Preexisting Asthma).
WARNINGS: Gastrointestinal (Gl) Effects—Risk of Gl Ulceration, Bleeding, and
Perforation: Serious Gl toxicity, such as bleeding, ulceration, and perforation of the
stomach, small intestine, or large intestine, can occur at any time, with or without
warning symptoms, in patients treated with NSAIDs. Minor upper Gl problems,
such as dyspepsia, are common and may also occur at any time during NSAID
therapy. Therefore, physicians and patients should remain alert for ulceration and
bleeding, even in the absence of previous Gl tract symptoms. Patients should be
informed about the signs and/or symptoms of serious Gl toxicity and the steps to
take if they occur. Tne utility of periodic laboratory monitoring has not been
demonstrated, nor has it been adequately assessed. Only 1 in 5 patients who
develop a serious upper Gl adverse event on NSAID therapy is symptomatic. It has
been demonstrated that upper Gl ulcers, gross bleeding, or perforation caused by
NSAIDs, appear to occur in approximately 1% of patients treated for 3 - 6 months,
and in about 2 % - 4 % of patients treated for 1 year. These trends continue thus,
increasing the likelihood of developing a serious Gl event at some time during the
course of therapy. However, even short-term therapy is not without risk.
It is unclear, at the present time, how the above rates apply to VIOXX. Among
3,357 patients who received VIOXX in controlled clinical trials of 6 weeks to 1 year
in duration (most were enrolled in 6-month or longer studies) at a daily dose of
12.5 mg to 50 mg, a total of 4 patients experienced a serious upper GI event, using
protocol-derived criteria. Two patients experienced an upper Gl bleed within 3
months (at Days 62 and 87, respectively) (0.06%). One additional patient experienced an obstruction within 6 months (Day 130) and the remaining patient developed an upper Gl bleed within 12 months (Day 322) (0.12%). Approximately 23%
of these 3,357 patients were in studies that required them to be ulcer free at study
entry. It is unclear if this study population is representative of the general population. Prospective, long-term studies required to compare the incidence of serious,
clinically significant upper Gl adverse events in patients taking VIOXX vs comparator NSAID products have not been performed.
NSAIDs should be prescribed with extreme caution in patients with a prior history of ulcer disease or Gl bleeding. Most spontaneous reports of fatal Gl events are
in elderly or debilitated patients and therefore special care should be taken in treating this population. To minimize the potential risk for an adverse Gl event, the
lowest effective dose should be used for the shortest possible duration. For highrisk patients, alternate therapies that do not involve NSAIDs should be considered.
Studies have shown that patients with a prior history of peptic ulcer disease
and/or Gl bleeding and who use NSAIDs, have a greater than 10-fold higher risk
for developing a Gl bleed than patients with neither of these risk factors. In addition
to a past history of ulcer disease, pharmacoepidemiology studies have identified
several other cotherapies or comorbid conditions that may increase the risk for Gl
bleeding, such as: treatment with oral corticosteroids, treatment with anticoagulants, longer duration of NSAID therapy, smoking, alcoholism, older age, and poor
general health status.
Anaphylactoid Reactions: As with NSAIDs in general, anaphylactoid reactions have
occurred in patients without known prior exposure to VIOXX. In postmarketing
experience, rare cases of anaphylactoid reactions and angioedema have been
reported in patients receiving VIOXX. VIOXX should not be given to patients with
the aspirin triad. This symptom complex typically occurs in asthmatic patients who
experience rhinitis with or without nasal polyps, or who exhibit severe, potentially
fatal bronchospasm after taking aspirin or other NSAIDs (see
CONTRAINDICATIONS and PRECAUTIONS, Preexisting Aslhma). Emergency help
should be sought in cases where an anaphylactoid reaction occurs.
Advanced Renal Disease: No safety information is available regarding the use of
VIOXX in patients with advanced kidney disease. Therefore, treatment with VIOXX
is not recommended in these patients. If VIOXX therapy must be initiated, close
monitoring of the patient's kidney function is advisable (see PRECAUTIONS,
Renal Effects).
Pregnancy: In late pregnancy, VIOXX should be avoided because it may cause premature closure of the ductus arteriosus.
PRECAUTIONS: General: VIOXX cannot be expected to substitute for corticosteroids or to treat corticosteroid insufficiency. Abrupt discontinuation of corticosteroids may lead to exacerbation of corticosteroid-responsive illness. Patients on
prolonged corticosteroid therapy should have their therapy tapered slowly if a
decision is made to discontinue corticosteroids.
The pharmacologic activity of VIOXX in reducing inflammation, and possibly
fever, may diminish the utility of these diagnostic signs in detecting infectious
complications of presumed noninfectious, painful conditions.
Hepatic Effects: Borderline elevations of 1 or more liver tests may occur in up to
15% of patients taking NSAIDs, and notable elevations of ALT or AST ( - 3 or more
times the upper limit of normal) have been reported in approximately 1% of
patients in clinical trials with NSAIDs. These laboratory abnormalities may
progress, may remain unchanged, or may be transient with continuing therapy.
Rare cases of severe hepatic reactions, including jaundice and fatal fulminant
hepatitis, liver necrosis, and hepatic failure (some with fatal outcome) have been
reported with NSAIDs. In controlled clinical trials of VIOXX, the incidence of borderline elevations of liver tests at doses of 12.5 mg and 25 mg daily was comparable to the incidence observed with ibuprofen ana lower than that observed with
diclofenac. In placebo-controlled trials, approximately 0.5% of patients taking
rofecoxib (12.5 mg or 25 mg q.d.) and 0.1% of patients taking placebo had notable
elevations of ALT or AST.
A patient with symptoms and/or signs suggesting liver dysfunction, or in
whom an abnormal liver test has occurred, should be monitored carefully for evidence of the development of a more severe hepatic reaction while on therapy with
VIOXX. Use of VIOXX is not recommended in patients with moderate or severe
hepatic insufficiency. If clinical signs and symptoms consistent with liver disease
develop, or if systemic manifestations occur (e.g., eosinophilia, rash, etc.), VIOXX
should be discontinued.
Renal Effects: Long-term administration of NSAIDs has resulted in renal papillary
necrosis and other renal injury. Renal toxicity has also been seen in patients in
whom renal prostaglandins have a compensatory role in the maintenance of renal
perfusion. In these patients, administration of an NSAID may cause a dose-dependent reduction in prostaglandin formation and, secondarily, in renal blood flow,
which may precipitate overt renal decompensation. Patients at greatest risk of this
reaction are those with impaired renal function, heart failure, liver dysfunction,
those taking diuretics and angiotensin-converting enzyme (ACE) inhibitors, and
the elderly. Discontinuation of NSAID therapy is usually followed by recovery to the
pretreatment state. Clinical trials with VIOXX at daily aoses of 12.5 mg and 25 mg
have shown renal effects (e.g., hypertension, edema) similar to those observed
with comparator NSAIOs; these occur with an increased frequency with chronic
use of VIOXX at doses above the 12.5-mg to 25-mg range (see ADVERSE REACTIONS). Caution should be used when initiating treatment with VIOXX in patients
with considerable dehydration. It is advisable to rehydrate patients first and then start
therapy with VIOXX. Caution is also recommended in patients with preexisting kidney disease (see WARNINGS, Advanced Renal Disease).
Hematologic Effects: Anemia is sometimes seen in patients receiving VIOXX. In
placebo-controlled trials, there were no significant differences observed between
VIOXX and placebo in clinical reports of anemia. Patients on long-term treatment
with VIOXX should have their hemoglobin or hematocrit checked if they exhibit any
signs or symptoms of anemia or blood loss. VIOXX does not generally affect
platelet counts, prothrombin time, or partial thromboplastin time, and does not
inhibit platelet aggregation at indicated dosages.
Fluid Retention and Edema: Fluid retention and edema have been observed in
some patients taking VIOXX®(rofecoxib tablets and oral suspension) (see ADVERSE
REACTIONS). VIOXX should be used with caution and should be introduced at the
lowest recommended dose in patients with fluid retention, hypertension, or heart
failure.
Preexisting Asthma: Patients with asthma may have aspirin-sensitive asthma. The
use of aspirin in patients with aspirin-sensitive asthma has been associated with
severe bronchospasm, which can be fatal. Since cross-reactivity, including bronchospasm, between aspirin and other NSAIDs has been reported in such aspirinsensitive patients, VIOXX should not be administered to patients with this form of
aspirin sensitivity and should be used with caution in patients with preexisting
asthma.
Information for Patients: VIOXX can cause discomfort and, rarely, more serious
side effects, such as Gl bleeding, which may result in hospitalization and even fatal
outcomes. Although serious Gl tract ulcerations and bleeding can occur without
warning symptoms, patients should be alert for the signs and symptoms of ulcerations and bleeding, and should ask for medical advice when observing any indicative signs or symptoms. Patients should be apprised of the importance of this
Mow-up (see WARNINGS, Gastrointestinal (Gl) Effects—Risk of Gl Ulceration,
Bleeding, and Perforation).
Patients should promptly report signs or symptoms of Gl ulceration or bleeding, skin rash, unexplained weight gain, or edema to their physicians.
Patients should be informed of the warning signs and symptoms of hepatotoxicity (e.g., nausea, fatigue, lethargy, pruritus, jaundice, right upper quadrant
tenderness, and "flu-like" symptoms). If these occur, patients should be instructed to stop therapy and seek immediate medical therapy.
Patients should also be instructed to seek immediate emergency help in the
case of an anaphylactoid reaction (see WARNINGS).
In late pregnancy, VIOXX should be avoided because it may cause premature
closure of the ductus arteriosus.
Laboratory Tests: Because serious Gl tract ulcerations and bleeding can occur
without warning symptoms, physicians should monitor for signs or symptoms of
Gl bleeding.
Drug Interactions: ACE Inhibitors: Reports suggest that NSAIDs may diminish the
antihypertensive effect of ACE inhibitors. In patients with mild to moderate hypertension, administration of 25 mg daily of VIOXX with the ACE inhibitor benazepril,
10 to 40 mg for 4 weeks, was associated with an average increase in mean arterial pressure of about 3 mmHg compared to ACE inhibitor alone. This interaction
should be given consideration in patients taking VIOXX concomitantly with ACE
inhibitors. Aspirin: Concomitant administration of low-dose aspirin with VIOXX
may result in an increased rate of Gl ulceration or other complications, compared
to use of VIOXX alone. At steady state, VIOXX 50 mg once daily had no effect on
the antiplatelet activity of low-dose (81 mg once daily) aspirin, as assessed by ex
vivo platelet aggregation and serum TXB? generation in clotting blood. VIOXX is
not a substitute for aspirin for cardiovascular prophylaxis.
Cimetidine:
Coadministration with high doses of cimetidine (800 mg twice daily) increased the
Cmax of rofecoxib by 21 %, the AUCQ-i20hr by 23%, and the t i / 2 by 15%. These
small changes are not clinically significant and no dose adjustment is necessary.
Digoxin: Rofecoxib 75 mg once daily for 11 days does not alter the plasma concentration profile or renal elimination of digoxin after a single 0.5-mg oral dose.
Furosemide: Clinical studies, as well as postmarketing observations, have shown
that NSAIDs can reduce the natriuretic effect of furosemide and thiazides in some
patients. This response has been attributed to inhibition of renal prostaglandin
synthesis. Keloconazole: Ketoconazole 400 mg daily did not have any clinically
important effect on the pharmacokinetics of rofecoxib. Lithium: NSAIDs have produced an elevation of piasma lithium levels and a reduction in renal lithium clearance. In postmarketing experience, there have been reports of increases in plasma
lithium levels. Thus, when VIOXX and lithium are administered concurrently, subjects should be observed carefully for signs of lithium toxicity. Methotrexate:
VIOXX 75 mg administered once daily tor 10 days increased plasma concentrations by 23%, as measured by AUCo-24hr in patients receiving methotrexate 7.5
mg to 15 mg/week for rheumatoid arthritis. An equivalent magnitude of reduction
in methotrexate renal clearance was observed. At 24 hours postdose, a similar proportion of patients treated with methotrexate alone (94%) and subsequently treated
with methotrexate coadministered with 75 mg of rofecoxib (88%) had
methotrexate plasma concentrations below the measurable limit (5 ng/mL). The
effects of the recommended doses for OA (12.5 mg and 25 mg) of VIOXX on plasma methotrexate levels are unknown. Standard monitoring of methotrexate-related toxicity should be continued if VIOXX and methotrexate are administered concomitantly. Oral Contraceptives: Rofecoxib did not have any clinically important
effect on the pharmacokinetics of ethinyl estradiol and norethindrone.
Prednisone/Prednisolone:
Rofecoxib did not have any clinically important effect on
the pharmacokinetics of prednisone or prednisolone. Rifampin: Coadministration
of VIOXX with rifampin 600 mg daily, a potent inducer of hepatic metabolism, produced an approximate 50% decrease in rofecoxib plasma concentrations.
Therefore, a starting daily dose of 25 mg of VIOXX should be considered for the
treatment of OA when VIOXX is coadministered with potent inducers of hepatic
metabolism. Warfarin: Anticoagulant activity should be monitored, particularly in
the first few days after initiating or changing VIOXX therapy in patients receiving
warfarin or similar agents, since these patients are at an increased risk of bleeding
complications. In single- and multiple-dose studies in healthy subjects receiving
both warfarin and rofecoxib, prothrombin time (measured as INR) was increased
by approximately 8% to 11%. In postmarketing experience, bleeding events have
been reported, predominantly in the elderly, in association with increases in prothrombin time in patients receiving VIOXX concurrently with warfarin.
Carcinogenesis, Mutagenesis, Impairment of Fertility: Rofecoxib was not carcinogenic in mice given oral doses up to 30 mg/kg [male) and 60 mg/kg (female) (-5and 2-fold the human exposure at 25 mg and 56 mg daily based on AllCo-24) and
in male and female rats given oral doses up to 8 mg/kg ( - 6 - and 2-fold the human
exposure at 25 mg and 50 mg daily based on AUCo-24) tor 2 years. Rofecoxib was
not mutagenic in an Ames test or in a V-79 mammalian cell mutagenesis assay,
nor clastogenic in a chromosome aberration assay in Chinese hamster ovary
(CHO) cells, in an in vitro and an in vivo alkaline elution assay, or in an in vivo
chromosomal aberration test in mouse bone marrow. Rofecoxib did not impair
male fertility in rats at oral doses up to 100 mg/kg (-20- and 7-fold human exposure at 25 mg and 50 mg daily based on AUCo-24) and rofecoxib had no effect on
fertility in female rats at doses up to 30 mg/kg (-19- and 7-fold human exposure at
25 mg and 50 mg daily based on AUCo-24).
Pregnancy: Teratogenic Effects: Pregnancy Category C. Rofecoxib was not teratogenic
in rats at dosages up to 50 mg/kg/day (-28- and 10-fold human exposure at 25 mg
and 50 mg daily based on AUCo-24). There was a slight, nonstatistically significant
increase in the overall incidence of vertebral malformations only in the rabbit at doses
of 50 mg/kg/day (-1 - or <1 -fold human exposure at 25 mg and 50 mg daily based on
AUCo-24). There are no studies in pregnant women. VIOXX should be used during
pregnancy only if the potential benefit justifies the potential risk to the fetus.
Nonteratogenic Effects: Rofecoxib produced periimplantation and postimplantation losses and reduced embryo/fetal survival in rats and rabbits at oral doses >10
and >75 mg/kg/day, respectively ( - 9 - and 3-toid [rats] and 2- and <1 -fold [rabbits]
human exposure based on AUCo-24 at 25 mg and bO mg daily). These changes
are expected with inhibition of prostaglandin synthesis and are not the result of
permanent alteration of female reproductive function. There was an increase in the
incidence of postnatal pup mortality in rats at >5 mg/kg/day (-5- and 2-fold human
exposure at 25 mg and 50 mg daily based on AUCo-24). In studies in pregnant
rats administered single doses of rofecoxib, there was a treatment-related
decrease in the diameter of the ductus arteriosus at all doses used ( 3 - 3 0 0 mg/kg:
3 mg/kg is ~2- and <1 -fold human exposure at 25 mg or 50 mg daily based on
AUCo-24)- As with other drugs known to inhibit prostaglandin synthesis, use of
VIOXX during the third trimester of pregnancy should be avoided.
Labor and Delivery: Rofecoxib produced no evidence of significantly delayed labor
or parturition in females at doses 15 mg/kg in rats (-10- and 3-fold human exposure as measured by the AUCo-24 at 25 mg and 50 mg). The effects of VIOXX on
labor and delivery in pregnant women are unknown. Merck & Co., Inc., maintains
a registry to monitor the pregnancy outcomes of women exposed to VIOXX while
pregnant. Healthcare providers are encouraged to report any prenatal exposure tc
VIOXX by calling the Pregnancy Registry at 1-800-986-8999.
Nursing Mothers: Rofecoxib is excreted in the milk of lactating rats at concentrations similar to those in plasma. There was an increase in pup mortality and a
decrease in pup body weight following exposure of pups to milk from dams
administered VIOXX® (rofecoxib tablets and oral suspension) during lactation. The
dose tested represents an approximate 18- and 6-fold human exposure at 25 mg
and 50 mg daily based on AUCo-24- It is not known whether this drug is excreted
in human milk. Because many drugs are excreted in human milk and because of
the potential for serious adverse reactions in nursing infants from VIOXX, a decision should be made whether to discontinue nursing or to discontinue the drug,
taking into account the importance of the drug to the mother.
Pediatric Use: Safety and effectiveness in pediatric patients below the age of 18
years have not been evaluated.
Geriatric Use: Of the patients who received VIOXX in OA clinical trials, 1,455 were
65 years of age or older (this included 460 who were 75 years or older). No substantial differences in safety and effectiveness were observed between these subjects and younger subjects. Greater sensitivity of some older individuals cannot be
ruled out. Dosage adjustment in the elderly is not necessary; however, therapy with
VIOXX should be initiated at the lowest recommended dose. In 1 of these studies
(a 6-week, double-blind, randomized clinical trial), VIOXX 12.5 mg or 25 mg once
daily was administered to 174 OA patients >80 years of age. The safety profile in
this elderly population was similar to that of younger patients treated with VIOXX.
ADVERSE REACTIONS: OA: Approximately 3,600 patients with OA were treated
with VIOXX; approximately 1,400 patients received VIOXX for 6 months or longer,
and approximately 800 patients for 1 year or longer. The following paragraph lists
all adverse events, regardless of causality, occurring in at least 2% of patients
receiving VIOXX in 9 controlled studies of 6 weeks' to 6 months' duration conducted in patients with OA at the therapeutically recommended doses (12.5 mg
and 25 mg), which included a placebo and/or positive control group.
Clinical adverse experiences occurring in >2.0% of patients treated with VIOXX vs
placebo, ibuprofen 2400 mg, or diclofenac 150 mg: Body as a Whole/Site
Unspecified: abdominal pain, 3.4% (vs 4.1%, placebo; 4.6%, ibuprofen; 5.8%,
diclofenac); asthenia/fatigue, 2.2% (vs 1.0%; 2.0%; 2.6%); dizziness, 3.0% (vs
2.2%; 2.7%; 3.4%); influenza-like disease, 2.9% (vs 3.1%; 1.5%; 3.2%); lower
extremity edema, 3.7% (vs 1.1%; 3.8%; 3.4%); upper respiratory infection, 8.5% (vs
7.8%; 5.8%; 8.2%). Cardiovascular System: hypertension, 3.5% (vs 1.3%; 3.0%;
1.6%). Digestive System: diarrhea, 6.5% (vs6.8%; 7.1%: 10.6%); dyspepsia, 3.5%
(vs 2.7%; 4.7%; 4.0%); epigastric discomfort, 3.8% (vs 2.8%; 9.2%; 5.4%); heartburn, 4.2% (vs 3.6%; 5.2%; 4.6%); nausea, 5.2% (vs 2.9%; 7.1%; 7.4%). Eyes,
Ears, Nose, and Throat: sinusitis, 2.7% (vs 2.0%; 1.8%; 2.4%). Musculoskeletal
System: back pain, 2.5% (vs 1.9%; 1.4%; 2.8%). Nervous System: headache, 4.7%
(vs 7.5%; 6.1%; 8.0%). Respiratory System: bronchitis, 2.0% (vs 0.8%; 1.4%;
3.2%). Urogenital System: urinary tract infection, 2.8% (vs 2.7%; 2.5%; 3.6%).
The general safety profile of VIOXX 50 mg q.d. in OA clinical trials of up to 6
months (476 patients) was similar to that of VIOXX at the recommended OA doses
of 12.5 mg and 25 mg q.d., except for a higher incidence of Gl symptoms (abdominal pain, epigastric pain, heartburn, nausea, and vomiting), lower extremity edema
(6.3%), and hypertension (8.2%).
In the OA studies, the following spontaneous adverse events occurred in
>0.1% to 1.9% of patients treated with VIOXX, regardless of causality:
Body as a Whole: abdominal distension, abdominal tenderness, abscess, chest
pain, chills, contusion, cyst, diaphragmatic hernia, fever, fluid retention, flushing,
fungal infection, infection, laceration, pain, pelvic pain, peripheral edema, postoperative pain, syncope, trauma, upper extremity edema, viral syndrome.
Cardiovascular System: angina pectoris, atrial fibrillation, bradycardia, hematoma,
irregular heartbeat, palpitation, premature ventricular contraction, tachycardia,
venous insufficiency. Digestive System: acid reflux, aphthous stomatitis, constipation, dental caries, dental pain, digestive gas symptoms, dry mouth, duodenal disorder, dysgeusia, esophagitis, flatulence, gastric disorder, gastritis, gastroenteritis,
hematochezia, hemorrhoids, infectious gastroenteritis, oral infection, oral lesion,
oral ulcer, vomiting. Eyes, Ears, Alose, and Throat: allergic rhinitis, blurred vision,
cerumen impaction, conjunctivitis, dry throat, epistaxis, laryngitis, nasal congestion, nasal secretion, ophthalmic injection, otic pain, otitis, otitis media, pharyngitis,
tinnitus, tonsillitis. Immune System: allergy, hypersensitivity, insect bite reaction.
Metabolism and Nutrition: appetite change, hypercholesterolemia, weight gain.
Musculoskeletal System: ankle sprain, arm pain, arthralgia, back strain, bursitis,
cartilage trauma, Joint swelling, muscular cramp, muscular disorder, muscular
weakness, musculoskeletal pain, musculoskeletal stiffness, myalgia, osteoarthritis,
tendinitis, traumatic arthropathy, wrist fracture. Nervous System: hypesthesia,
insomnia, median nerve neuropathy, migraine, muscular spasm, paresthesia, sciatica, somnolence, vertigo. Psychiatric:anxiety, depression, mental acuity decreased.
Respiratory System: asthma, cough, dyspnea, pneumonia, pulmonary congestion,
respiratory infection. Skin and Skin Appendages: abrasion, alopecia, atopic dermatitis, basal cell carcinoma, blister, cellulitis, contact dermatitis, heipes simplex,
herpes zoster, nail unit disorder, perspiration, pruritus, rash, skin erythema,
urticaria, xerosis. Urogenital System: breast mass, cystitis, dysuria, menopausal
symptoms, menstrual disorder, nocturia, urinary retention, vaginitis.
The following serious adverse events have been reported rarely (estimated
<0.1%) in patients taking VIOXX, regardless of causality. Cases reported only in
the postmarketing experience are indicated in italics.
Cardiovascular: cerebrovascular accident, congestive heart failure, deep venous
thrombosis, myocardial infarction, pulmonary embolism, transient ischemic
attack, unstable angina. Gl: cholecystitis, colitis, colonic malignant neoplasm, duodenal perforation, duodenal ulcer, esophageal ulcer, gastric perforation,
gastric
ulcer, Gl bleeding, hepatitis, intestinal obstruction, jaundice, pancreatitis. Hemic
and Lymphatic: agranulocytosis,
leukopenia, lymphoma,
thrombocytopenia.
Immune System: anaphylactoid reaction, angioedema. Nervous System: aseptic
meningitis. Psychiatric: confusion, hallucinations. Skin and Skin Appendages:
severe skin reactions, including Stevens-Johnson syndrome. Urogenital System:
acute renal failure, breast malignant neoplasm, interstitial nepphritis, prostatic
malignant neoplasm, urolithiasis, worsening chronic renal failure.
In 1-year controlled clinical trials and in extension studies for up to 86 weeks
( - 8 0 0 patients treated with VIOXX for 1 year or longer), the adverse-experience
profile was qualitatively similar to that observed in studies of shorter duration.
Analgesia, Including Primary Dysmenorrhea: Approximately 1,000 patients were
treated with VIOXX in analgesia studies. All patients in postdental surgery pain
studies received only a single dose of study medication. Patients in primary dysmenorrhea studies may have taken up to 3 daily doses of VIOXX, and those in the
postorthopedic surgery pain study were prescribed 5 daily doses of VIOXX.
The adverse-experience profile in the analgesia studies was generally similar to
those reported in the OA studies. The following additional adverse experience,
which occurred at an incidence of >2% of patients treated with VIOXX, was
observed in the postdental pain surgery studies: postdental extraction alveolitis
(dry socket).
in 110 patients treated with VIOXX (average age - 6 5 years) in the postorthopedic surgery pain study, the most commonly reported adverse experiences were
constipation, fever, and nausea.
DOSAGE AND ADMINISTRATION: VIOXX is administered orally. The lowest dose
of VIOXX should be sought for each patient.
OA: The recommended starting dose of VIOXX is 12.5 mg once daily. Some
patients may receive additional benefit by increasing the dose to 25 mg once daily.
The maximum recommended daily dose is 25 mg.
Management of Acute Pain and Treatment of Primary Dysmenorrhea: The recommended initial dose of VIOXX is 50 mg once daily. Subsequent doses should be 50
mg once daily as needed. Use of VIOXX for more than 5 days in management of
pain has not been studied.
VIOXX Tablets may be taken with or without food.
Oral Suspension: WXX Oral Suspension 12.5 mg/5 mL or 25 mg/5 mL may be
substituted for VIOXX Tablets 12.5 mg or 25 mg, respectively, in any of the above
indications. Shake before using.
For more detailed information, consult your Merck representative and read the full
Prescribing
Information.
^ ^
^
MERCK
VIOXX is a registered trademark of Merck & Co., Inc.
©2000 Merck & Co., Inc
All rights reserved.
Whitehouse Station, NJ 08889.
007710(1)(806)-vt0
Downloaded from www.ccjm.org on June 15, 2014. For personal use only. All other uses require permission.
PRODUCT
STRENGTH OF PPA
PRODUCT
OrdrineAT Extended-Release
Ornade Spansules
Pannaz
Partuss LA
Phanadex Cough Syrup
Phenahist-TRTablets
Phenate
Phenchlor S.H.A.
Phenylfenesin LA
Poly-Histine CS Syrup
Poly-Histine-D Capsules
Poly-Histine-D Eixir
Poly-Histine-D Ped Caps
Poly-Histine DM Syrup
Profen II
Profen II DM
Profen LA
Resaid
Rescap-D S.R.
Rhinolar-EX
Rolatuss with Hydrocodone Liquid
Ru-Tuss with Hydrocodone Liquid
Rymed-TR
SINUvent
S-T Forte Syrup
Stahist
Stamoist LA
Statuss Espectorant Liquid
75 mg
75 mg
75 mg
75 mg
25 mg/5 mL
50 mg
40 mg
50 mg
75 mg
12.5 mg/5 mL
50 mg
12.5 mg/5 mL
25 mg
12.5 mg/5 mL
37.5 mg
37.5 mg
75 mg
75 mg
75 mg
75 mg
3.3 mg/5 mL
3.3 mg/5 mL
75 mg
75 mg
5 mg
50 mg
75 mg
12.5 mg/5 mL
Tannine S.R.
T-Koff Liquid
Triaminic Expectorant with Codeine Liquid
Triaminic Expectorant DH Liquid
Trihist-CS Syrup
Trihist-DM
TRINKOF-D
Tri-Phen-Chlor
Tri-Phen-Chlor Pediatric Drops
Tri-Phen-Chlor Pediatric Syrup
Tri-Phen-Chlor Syrup
Tri-Phen-Mine Pediatric Drops
Tri-Phen-Mine Pediatric Syrup
Tri-Phen-Mine S.R.
Tusquelin Syrup
Tussanil DH
Tuss-Allergine Modified T.D.
Tussogest Extended Release
Tuss-Ornade Liquid
Tuss-Ornade Spansules
ULR-LA
Unl-Decon
Vanex Forte
Vanex Forte-R
Vetuss HC Syrup
Statuss Green Liquid
3.3 mg/5 mL
0.62, which was not statistically significant.
shows other analyses for PPA use in the
two groups.
Extrapolating from these data, the investigators estimated that PPA might cause one
hemorrhagic stroke in every 107,000 to
3,268,000 women within 3 days of taking a
PPA-containing diet pill, which translates to
about 200 to 500 hemorrhagic strokes each
year in the United States.
TABLE 4
Limitations of the study
Case-control studies in general cannot establish causation, they can only suggest an association. In particular, the Hemorrhagic Stroke
STRENGTH OF PPA
15mg
20 mg/5 mL
12.5 mg/5 mL
12.5 mg/5 mL
12.5 mg/5 mL
12.5 mg/5 mL
37.5 mg
40 mg
5 mg/1 mL
5 mg/5 mL
20 mg/5 mL
5 mg/1 mL
5 mg/5 mL
40 mg
5 mg/5 mL
25 mg
75 mg
75 mg
12.5 mg/5 mL
75 mg
75 mg
40 mg
50 mg
75 mg
3.3 mg/5 mL
PPA = phenylpropanolamine
' M a n y manufacturers are reformulating their products
ADAPTED FROM OLIN BR, EDITOR. RESPIRATORY COMBINATION PRODUCTS. DRUG FACTS
AND COMPARISONS. ST. LOUIS: FACTS & COMPARISONS, INC. 2000, AND TIETZE KJ. DISORDERS RELATED TO COLD AND ALLERGY. IN: ALLEN LV, BERARDI RR, DESIMONE EM, EDS.
HANDBOOK OF NONPRESCRIPTION DRUGS 12TH ED. 2000:183-184.
Project had several limitations.
Potential bias. One limitation of the
Hemorrhagic Stroke Project is the possible
introduction of biases such as temporal-precedence bias, recall bias, and selection bias. The
investigators attempted to minimize these
biases in their study design, for example, by
carefully structuring the interviews and by
asking about all medication use within the
preceding 2 weeks, not just 3 days.
Types of stroke included. The study
included patients with stroke due to either
intracerebral hemorrhage or subarachnoid
hemorrhage. In a recent review, Leppala et
al'4 evaluated risk factors for different stroke
217 C L E V E L A N D C L I N I C J O U R N A L OF M E D I C I N E
VOLUME 68 • NUMBER 3
Downloaded from www.ccjm.org on June 15, 2014. For personal use only. All other uses require permission.
MARCH
2001
PHENYLPROPANOLAMINE
MERSFELDER
The Hemorrhagic Stroke Study: Association b e t w e e n
p h e n y l p r o p a n o l a m i n e use a n d h e m o r r h a g i c s t r o k e
VARIABLE
STROKE PATIENTS
Women
Number in analysis
P VALUE
6(1.6%)
1(0.1%)
16.58 (1.51-182.21)
.01
Used a PPA cough or cold remedy
16 (4.2%)
19(2.5%)
1.54 (0.76-3.14)
.23
Used any PPA product
21 (5.5%)
20(2.7%)
1.98 (1.00-3.90)
.05
4(0.4%)
3.13 (0.86-11.46)
.08
Used a PPA product
for the first time*
7 (1.8%)
Men
626
Number in analysis
218
ADJUSTED MATCHED
ODDS RATIO* AND 9 5 % CI
750
383
Used a PPA diet pillt
Many
manufacturers
are
reformulating
PPA-containing
products
CONTROL SUBJECTS
319
0
Used a PPA-containing diet pill
0
13(2.1%)
0.62 (0.20-1.92)
.41
Used a PPA cough or cold remedy
6 (1.9%)
13(2.1%)
0.62 (0.20-1.92)
.41
Used any PPA product
6 (1.9%)
Used a PPA product
for the first time
10.2%)
2.95 (0.15-59.59)
.48
1 (0.3%)
' A d j u s t e d for smoking, hypertension, race, and level of education
t W i t h i n 3 days preceding t h e onset of symptoms
• W i t h i n 24 hours before the onset of symptoms, and had not used any other such products t h e preceding 2 weeks
ADAPTED FROM KERNAN WN. VISCOLI CM, BRASS LM, ET AL. PHENYLPROPANOLAMINE AND THE RISK OF HEMORRHAGIC STROKE.
N ENGL J MED 2000; 343:1826-1832.
subtypes and demonstrated that the risk factor
profiles for subarachnoid hemorrhage and
intracerebral hemorrhage had little in common. These investigators suggest that studies
not ignore stroke subtyping, in view of the risk
of forming misleading associations. However,
they did not specifically look at medication
use as a risk factor in their evaluation, which
was the focus of the Hemorrhagic Stroke
Project.
Combination effect with caffeine.
Combining medications can sometimes lead
to an increase in adverse effects. A diet aid
that contained the combination of PPA and
caffeine was removed from the market in the
1980s because of unacceptable adverse drug
reactions and abuse potential.2-5
In the Hemorrhagic Stroke Project, 7 % of
stroke patients reported ingesting caffeine,
CLEVELAND CLINIC J O U R N A L OF MEDICINE
VOLU ME 6 8 • NUMBER 3
MARCH
compared with 2.9% of the matched control
subjects (P < .01). However, the amount or
type of caffeine consumed was not reported.
Although the odds ratio did not change after
the investigators performed a basic conditional logistic model to account for reported caffeine use by study patients,2 given the high
coffee consumption in the United States, the
combination effect of these two medications
should not be ignored.
Combination effect with herbal products. Another potentially harmful combination not addressed in the study was herbal or
natural products taken with PPA. Some of
these products contain ephedrine-like substances that could possibly enhance the
adverse effects of PPA when ingested concurrently. Examples of these include Ma huang,
Ephedra herba, and Ephedra sinensis.
2001
Downloaded from www.ccjm.org on June 15, 2014. For personal use only. All other uses require permission.
Does t h e PPA dose m a t t e r ?
The Hemorrhagic Stroke Project showed a
trend toward a dose-effect relationship: ie,
there was a higher odds ratio in the people
taking more than 75 mg per day than in those
who took less than 75 mg per day. In contrast,
Lake et al5 reported that of the 24 reported
cases of intracranial hemorrhage, 9 were in
patients who took the recommended amount
of PPA. The other 15 cases were in people
who either overused or overdosed on PPA.
The authors concluded from the case reports
that a dose-response pattern was not evident
from the data available.
Notably, most of the cases reported were
not associated with use of cough and cold
remedies in recommended doses. Cough and
cold remedies generally contain less PPA
than the diet aids; also unlike the diet aids,
they are not typically formulated as sustained-release products. It is difficult, however, to make a strong conclusion from a
series of case reports. A larger study powered
to detect a difference in dosages of PPA and
the risk of hemorrhagic stroke would be
required.
•
Cough and cold products
with pseudoephedrine
Alka-Seltzer Plus Cold & Cough Medicine Liqul-Gels
Alka-Seltzer Plus Flu & Body Aches Liqui-Gels
Comtrex Day and Night Maximum Strength Cold and Flu Relief
Contac Non-Drowsy
Novahistine DH Liquid
PediaCare Cough-Cold Liquid
Pediacare Infants' Decongestant Plus Cough Drops
Robitussin Night-Time Cold Softgels
Robitussin PE Syrup
Robitussin Pediatric Night Relief Liquid
Robitussin Severe Congestion Liqui-Gels
Sudafed Severe Cold
TheraFlu Cold & Cough Medicine NightTime
TheraFlu Maximum Strenght Non-Drowsy Caplets
Triaminic AM Non-Drowsy Cough & Decongestant
Triaminic Sore Throat, Throat Pain & cough Liquid
Tylenol Cold Multi-Symptom
Tylenol Cold No Drowsiness
Tylenol Children's Cold Plus Cough Chewable
Vicks 44M Soothing Cough, Cold & Flu Relief
IMPLICATIONS
Vicks DayQuil Multi-Symptom Cold & Flu Relief LiquiCaps
Although the overall risk of PPA-induced
hemorrhagic stroke is low (and not statistically significant for cough and cold products),
the inability to predict who is at risk, along
with the debilitating effects of stroke, produces serious concerns.
The FDA does not consider PPA to be
safe for use in over-the-counter or prescription medications. T h e results of the
Hemorrhagic Stroke Project prompted the
FDA to:
• Recommend that manufacturers voluntarily discontinue marketing all over-thecounter and prescription medications containing PPA.
• Issue a public health advisory about the
safety of PPA on October 6, 2000, indicating
that over-the-counter medications containing PPA should not be recommended to
patients for weight control or for symptomatic cold relief, and that prescription medications containing PPA should also be
avoided.
Vicks DayQuil Multi-Symptom Cold & Flu Relief
Vicks NyQuil Children's Cold & Cough Relief
Vicks NyQuil Multi-Symptom Cold & Flu Relief Liquid
ADAPTED FROM OLIN BR, EDITOR. RESPIRATORY COMBINATION PRODUCTS. DRUG FACTS AND
COMPARISONS. ST. LOUIS: FACTS & COMPARISONS, INC. 2000,
AND TIETZE KJ. DISORDERS RELATED TO COLD AND ALLERGY. IN: ALLEN LV, BERARDI RR,
DESIMONE EM, EDS. HANDBOOK OF NONPRESCRIPTION DRUGS 12TH ED. 2000:183-184,
A l t e r n a t i v e s to PPA
Oral cough, cold, and allergy products containing pseudoephedrine (TABLE 5) or nasal decongestants such as oxymetazoline or phenylephrine are alternatives for patients seeking
relief from symptoms. Caution still should be
taken when recommending pseudoephedrine
to patients with hypertension, hyperthyroidism, diabetes mellitus, coronary heart disease, ischemic heart disease, elevated intraocular pressure, or prostatic hypertrophy, because
decongestants may exacerbate these diseases.15
Although no studies have evaluated the occurrence of hemonhagic stroke with the use of
219 C L E V E L A N D CLINIC J O U R N A L OF M E D I C I N E
VOLUME 68 • NUMBER 3
Downloaded from www.ccjm.org on June 15, 2014. For personal use only. All other uses require permission.
MARCH
2001
ONCE-A-DAY
PR0ÏONIX
See package insert for full prescribing information.
M o s t F r e q u e n t A d v e r s e E v e n t s R e p o r t e d as D r u g R e l a t e d i n S h o r t - t e r m D o m e s t i c Trials
I N D I C A T I O N S A N D USAGE
Short-term treatment (up to 8 weeks) of erosive esophagitis associated with gastroesophageal reflux disease (GERD). For those patients who have
not healed after 8 weeks of treatment, an additional 8-week course of PROTONIX may be considered.
The safety and efficacy of PROTONIX for maintenance therapy (e.g., beyond 16 weeks) have not been established (see PRECAUTIONS).
CONTRAINDICATIONS
Known hypersensitivity to any component of the formulation.
PRECAUTIONS
General
Symptomatic response to therapy with pantoprazole does not preclude the presence of gastric malignancy.
In rodents, pantoprazole is carcinogenic and caused rare types of gastrointestinal tumors. The relevance of these animal findings to humans
is unknown. The safety and efficacy of PROTONIX for maintenance therapy (e.g., beyond 16 weeks) have not been established. PROTONIX is not
indicated for maintenance therapy (see I N D I C A T I O N S A N D USAGE).
No dosage adjustment is necessary in patients with mild or moderate hepatic impairment. The pharmacokinetics of pantoprazole has not been well
characterized in patients with severe hepatic impairment. Therefore, the potential for modest drug accumulation (<21 %) when dosed once daily
needs to be weighed against the potential for reduced acid control when dosed every other day in these patients.
Information for Patients
PROTONIX tablets should be swallowed whole, with or without food in the stomach and should not be split, crushed, or chewed. Concomitant
administration of antacids does not affect the absorption of pantoprazole.
Drug Interactions
Pantoprazole is metabolized through the cytochrome P450 system, primarily the CYP2C19 and CYP3A4 isozymes, and subsequently undergoes
Phase II conjugation. Based on studies evaluating possible interactions of pantoprazole with other drugs metabolized by the cytochrome
P450 system, no dosage adjustment is needed with concomitant use of the following drugs: theophylline, cisapride, antipyrine, caffeine,
carbamazepine, diazepam, diclofenac, digoxin, ethanol, glyburide, an oral contraceptive (levonorgestrel/ethinyl estradiol), metoprolol, nifedipine,
phenytoin, or warfarin. Clinically relevant interactions of pantoprazole with other drugs with the same metabolic pathways are not expected.
Therefore, when co-administered with pantoprazole, adjustment of the dosage of pantoprazole or of such drugs may not be necessary. There was
also no interaction with concomitantly administered antacids.
Because of profound and long lasting inhibition of gastric acid secretion, it is theoretically possible that pantoprazole may interfere with absorption
of drugs where gastric pH is an important determinant of their bioavailability (e.g., ketoconazole, ampicillin esters, and iron salts).
Carcinogenesis, M u t a g e n e s i s , I m p a i r m e n t of Fertility
In a 24-month carcinogenicity study, Sprague-Dawley rats were treated orally with doses of 0.5 to 200 mg/kg/day, about 0.1 to 40 times the
exposure on a body surface area basis, of a 50-kg person dosed at 40 mg/day. In the gastric fundus, treatment at 0.5 to 200 mg/kg/day produced
enterochromaffin-like (ECL) cell hyperplasia and benign and malignant neuroendocrine cell tumors in a dose-related manner. In the forestomach,
treatment at 50 and 200 mg/kg/day (about 10 and 40 times the recommended human dose on a body surface area basis) produced benign
squamous cell papillomas and malignant squamous cell carcinomas. Rare gastrointestinal tumors associated with pantoprazole treatment
included an adenocarcinoma of the duodenum at 50 mg/kg/day, and benign polyps and adenocarcinomas of the gastric fundus at 200 mg/kg/day. In
the liver, treatment at 0.5 to 200 mgAg/day produced dose-related increases in the incidences of hepatocellular adenomas and carcinomas. In the
thyroid gland, treatment at 200 mg/kg/day produced increased incidences of follicular cell adenomas and carcinomas for both male and female rats.
Sporadic occurrences of hepatocellular adenomas and a hepatocellular carcinoma were observed in Sprague-Dawley rats exposed to pantoprazole
in 6-month and 12-month toxicity studies.
In a 24-month carcinogenicity study, Fischer 344 rats were treated orally with doses of 5 to 50 mg/kg/day, approximately 1 to 10 times the
recommended human dose based on body surface area. In the gastric fundus, treatment at 5 to 50 mg/kg/day produced enterochromaffin-like
(ECL) cell hyperplasia and benign and malignant neuroendocrine cell tumors. Dose selection for this study may not have been adequate to
comprehensively evaluate the carcinogenic potential of pantoprazole.
In a 24-month carcinogenicity study, B6C3F1 mice were treated orally with doses of 5 to 150 mg/kg/day, 0.5 to 15 times the recommended human
dose based on body surface area. In the liver, treatment at 150 mg/kg/day produced increased incidences of combined hepatocellular adenomas
and carcinomas in female mice. Treatment at 5 to 150 mg/kg/day also produced gastric fundic ECL cell hyperplasia.
Pantoprazole was positive in the in vitro human lymphocyte chromosomal aberration assays, and in one of two mouse micronucleus tests for
clastogenic effects, and in the in vitro Chinese hamster ovarian cell/HGPRT forward mutation assay for mutagenic effects. Equivocal results were
observed in the in vivo rat liver DNA covalent binding assay. Pantoprazole was negative in the in vitro Ames mutation assay, the in vitro
unscheduled DNA synthesis (UDS) assay with rat hepatocytes, the in vitro AS52/GPT mammalian cell-forward gene mutation assay, the in vitro
thymidine kinase mutation test with mouse lymphoma L5178Y cells, and the in vivo rat bone marrow cell chromosomal aberration assay.
Pantoprazole at oral doses up to 500 mg/kg/day in male rats (98 times the recommended human dose based on body surface area) and
450 mg/kg/day in female rats (88 times the recommended human dose based on body surface area) was found to have no effect on fertility
and reproductive performance.
Pregnancy
Teratogenic Effects
Pregnancy Category B
Teratology studies have been performed in rats at oral doses up to 450 mg/kg/day (88 times the recommended human dose based on body surface
area) and rabbits at oral doses up to 40 mg/kg/day (16 times the recommended human dose based on body surface area) and have revealed no
evidence of impaired fertility or harm to the fetus due to pantoprazole. There are, however, no adequate and well-controlled studies in pregnant
women. Because animal reproduction studies are not always predictive of human response, this drug should be used during pregnancy only if
Nursing M o t h e r s
Pantoprazole and its metabolites are excreted in the milk of rats. It is not known whether pantoprazole is excreted in human milk. Many drugs which
are excreted in human milk have a potential for serious adverse reactions in nursing infants. Based on the potential for tumorigenicity shown for
pantoprazole in rodent carcinogenicity studies, a decision should be made whether to discontinue nursing or to discontinue the drug, taking into
account the benefit of the drug to the mother.
Pediatric U s e
Safety and effectiveness in pediatric patients have not been established.
Use in W o m e n
Erosive esophagitis healing rates in the 221 women treated with pantoprazole in US clinical trials were similar to those found in men. The incidence
rates of adverse events were also similar between men and women,
Use in Elderly
Erosive esophagitis healing rates in the 107 elderly patients (>65 years old) treated with pantoprazole in US clinical trials were similar to those
found in patients under the age of 65. The healing rates of the 25 patients at least 75 years old were 80% for those treated with 10 mg of
pantoprazole and 100% for those patients treated with either 20 or 40 mg. In addition, the safety profile, including the incidence rates of adverse
events and laboratory abnormalities, in patients 65 years and older was similar to that of patients younger than 65 years of age.
ADVERSE R E A C T I O N S
Worldwide, more than 11,100 patients have been treated with pantoprazole in clinical trials involving various dosages and duration of treatment.
In general, pantoprazole has been well tolerated in both short-term and long-term trials.
In two US controlled clinical trials involving PROTONIX 10-, 20-, or 40-mg doses for up to 8 weeks, there were no dose-related effects on the
incidence of adverse events. The following adverse events considered by investigators to be possibly, probably, or definitely related to drug occurred
in 1% or more in the individual studies of GER0 patients on therapy with PROTONIX.
References: 1. D a t a o n file, Wyeth-Ayerst Laboratories, G M R - 3 2 0 2 3 (Protocol
No. 3001 A l -301 -US). 2. D a t a on file, Wyeth-Ayerst Laboratories, GMR-32022 (Protocol
No. 3001 A l -300-US). 3. D a t a o n file, Wyeth-Ayerst Laboratories, Pantoprazole 10th
Periodic Safety U p d a t e : 24-FEB-1999 t o 23-AUG-1999. 4. 2000 Drug Topics9 Red
BookApril
2000 Update. M o n t v a l e , NJ: M e d i c a l Economics C o ; 2000:19(4).
% Incidence
Study 300-US
S t u d y Event
Headache
Diarrhea
Elatulence
Abdominal pain
Rash
Eructation
Insomnia
Hyperglycemia
PROTONIX
I n = 5211
6
4
2
1
<1
1
<1
1
Study 301-US
Placebo
In = 8 2 )
6
1
2
2
0
1
2
0
PROTONIX
(n = 1 6 1 )
9
6
4
4
2
0
1
<1
Nizatidine
In = 82)
13
6
a
4
0
0
1
0
Note: Only adverse events w i t h an incidence greater than or equal to the comparators are s h o w n .
In addition, in these short-term domestic trials, the following treatment-emergent events, regardless of causality, occurred at a rate of £1%
in PROTONIX-treated patients: asthenia, back pain, chest pain, neck pain, flu syndrome, infection, pain, migraine, constipation, dyspepsia,
gastroenteritis, gastrointestinal disorder, nausea, rectal disorder, vomiting, hyperlipemia, liver function tests abnormal, SGPT increased, arthralgia,
anxiety, dizziness, hypertonia, bronchitis, cough increased, dyspnea, pharyngitis, rhinitis, sinusitis, upper respiratory tract infection, urinary frequency,
and urinary tract infection.
In international short-term double-blind or open-label, clinical trials involving 20 to 80 mg per day, the following adverse events were reported to
occur in 1% or more of 2805 GERD patients receiving pantoprazole for up to 8 weeks.
S t u d y Event
Headache
Diarrhea
A b d o m i n a l Pain
A d v e r s e E v e n t s i n GERD P a t i e n t s i n S h o r t - t e r m I n t e r n a t i o n a l T r i a l s
% Incidence
Ranitidine
Omeprazole
Pantoprazole
300 m g
20 m g
Total
(N=594)
(N=474)
(N=2805)
3
2
Famotidine
40 mg
(N=239)
1
1
Additional adverse experiences occurring in <1% of GERD patients based on pooled results from either short-term domestic or international trials
are shown below within each body system. In most instances the relationship to pantoprazole was unclear.
BODY AS A WHOLE: abscess, allergic reaction, chills, cyst, face edema, fever, generalized edema, heat stroke, hernia, laboratory test abnormal,
malaise, moniliasis, neoplasm, non-specified drug reaction.
CARDIOVASCULAR SYSTEM: angina pectoris, arrhythmia, cardiovascular disorder, chest pain substernal, congestive heart failure,
electrocardiogram abnormal, hemorrhage, hypertension, hypotension, myocardial ischemia, palpitation, retinal vascular disorder, syncope,
tachycardia, thrombophlebitis, thrombosis, vasodilatation.
DIGESTIVE SYSTEM: anorexia, aphthous stomatitis, cardiospasm, colitis, dry mouth, duodenitis, dysphagia, enteritis, esophageal hemorrhage,
esophagitis, gastrointestinal carcinoma, gastrointestinal hemorrhage, gastrointestinal moniliasis, gingivitis, glossitis, halitosis, hematemesis,
increased appetite, melena, mouth ulceration, oral moniliasis, periodontal abscess, periodontitis, rectal hemorrhage, stomach ulcer, stomatitis,
stools abnormal, tongue discoloration, ulcerative colitis.
ENDOCRINE SYSTEM: diabetes mellitus, glycosuria, goiter.
HEPATOBILIARY SYSTEM: biliary pain, bilirubinemia. cholecystitis, cholelithiasis, cholestatic jaundice, hepatitis, alkaline phosphatase increased,
gamma glutamyl transpeptidase increased, SGOT increased.
HEMIC AND LYMPHATIC SYSTEM: anemia, ecchymosis, eosinophilia, hypochromic anemia, iron deficiency anemia, leukocytosis, leukopenia,
thrombocytopenia.
METABOLIC AND NUTRITIONAL: dehydration, edema, gout, peripheral edema, thirst, weight gain, weight loss.
MUSCULOSKELETAL SYSTEM: arthritis, arthrosis, bone disorder, bone pain, bursitis, joint disorder, leg cramps, neck rigidity, myalgia,
tenosynovitis.
NERVOUS SYSTEM: abnormal dreams, confusion, convulsion, depression, dry mouth, dysarthria, emotional lability, hallucinations, hyperkinesia,
hypesthesia, libido decreased, nervousness, neuralgia, neuritis, paresthesia, reflexes decreased, sleep disorder, somnolence, thinking abnormal, tremor,
vertigo.
RESPIRATORY SYSTEM: asthma, epistaxis, hiccup, laryngitis, lung disorder, pneumonia, voice alteration.
SKIN AND APPENDAGES: acne, alopecia, contact dermatitis, dry skin, eczema, fungal dermatitis, hemorrhage, herpes simplex, herpes zoster,
lichenoid dermatitis, maculopapular rash, pain, pruritus, skin disorder, skin ulcer, sweating, urticaria.
SPECIAL SENSES: abnormal vision, amblyopia, cataract specified, deafness, diplopia, ear pain, extraocular palsy, glaucoma, otitis externa, taste
perversion, tinnitus.
UROGENITAL SYSTEM: albuminuria, balanitis, breast pain, cystitis, dysmenorrhea, dysuria, epididymitis, hematuria, impotence, kidney calculus,
kidney pain, nocturia, prostatic disorder, pyelonephritis, scrotal edema, urethral pain, urethritis, urinary tract disorder, urination impaired, vaginitis.
Postmarketing Reports
There have been spontaneous reports of adverse events with the postmarketing use of pantoprazole, including anaphylaxis; angioedema (Quincke's
edema); anterior ischemic optic neuropathy; severe dermatologic reactions, including erythema multiforme, Stevens-Johnson syndrome, and toxic
epidermal necrolysis (TEN, some fatal); pancreatitis; jaundice; confusion; hypokinesia; speech disorder; increased salivation; vertigo; nausea; and
tinnitus.
Laboratory Values
In two US controlled trials, 0.4% of the patients on 40 mg pantoprazole experienced SGPT elevations of greater than three times the upper limit of
normal at the final treatment visit. Except in those patients where there was a clear alternative explanation for a laboratory value change, such as
intercurrent illness, the elevations tended to be mild and sporadic. The following changes in laboratory parameters were reported as adverse events:
creatinine increased, hypercholesterolemia, and hyperuricemia.
OVERDOSAGE
Some reports of overdosage with pantoprazole have been received. A spontaneous report of a suicide involving an overdosage of pantoprazole
(560 mg) has been received; however, the death was more reasonably attributed to the unknown doses of chloroquine and zopiclone which
were also taken since two other reported cases of pantoprazole overdosage involved similar amounts of pantoprazole (400 and 600 mg) with no
adverse effects observed. One patient in a flexible dosing study of refractory peptic ulcer disease received a dose of 320 mg per day for 3 months;
treatment was well tolerated. Doses of up to 240 mg per day, given intravenously for seven days, have been administered to healthy subjects and
have been well tolerated.
Pantoprazole is not removed by hemodialysis.
Single oral doses of pantoprazole at 709 mg/kg, 798 mg/kg and 887 mg/kg were lethal to mice, rats, and dogs, respectively. The symptoms of acute
toxicity were hypoactivity, ataxia, hunched sitting, limb-splay, lateral position, segregation, absence of ear reflex, and tremor,
w
M a n u f a c t u r e d for W y e t h Laboratories
A W y e t h - A y e r s t Company
Philadelphia. PA 19101
under license f r o m
Byk Gulden Pharmaceuticals
D78467 Konstanz, Germany
This Brief Summary is based on the approved PROTONIX tablets direction circular ( M a r c h 1 , 2 0 0 0 , CI 6004-1
2000, Wyeth-Ayerst Laboratories
Downloaded from www.ccjm.org on June 15, 2014. For personal use only. All other uses require permission.
52420-00
PHENYLPROPANOLAMINE
MERSFELDER
pseudoephedrine, some suggest that PPA may
not be the only alpha-adrenergic agonist that
can cause serious adverse effects.16 Sodium
chloride nasal spray may benefit some patients
without carrying the risk of serious side effects.
In view of the overwhelming number of
over-the-counter products available, patients
should ask their pharmacist for assistance in
selecting a medication best suited for their
REFERENCES
1. K e r n a n W N , Viscoli C M , Brass L M , e t al.
P h e n y l p r o p a n o l a m i n e a n d t h e risk o f h e m o r r h a g i c s t r o k e .
N Engl J M e d 2 0 0 0 ; 3 4 3 : 1 8 2 6 - 1 8 3 2 .
2. H o r w i t z Rl, Brass L M , K e r n a n W N , Viscoli C M .
P h e n y l p r o p a n o l a m i n e a n d risk o f h e m o r r h a g i c stroke:
f i n a l r e p o r t of t h e H e m o r r h a g i c S t r o k e Project.
http://www.fda.gov/ohrms/dockets/ac/00/backgrd/3647bl_t
a b 1 9 . d o c . Accessed 1 / 2 3 / 0 1 .
3. S i l v e r m a n HI. A history o f t h e r a p e u t i c uses o f p h e n y l p r o p a n o l a m i n e in N o r t h A m e r i c a . In M o r g a n JP, K a g a n
DV, B r o d y JS, e d i t o r s . P h e n y l p r o p a n o l a m i n e : risks, b e n e fits, a n d controversies. N e w York: P r a e g e r Publishers,
1985:11-24.
4. M o r g a n JP. O v e r - t h e - c o u n t e r m e d i c a t i o n : a v a i l a b i l i t y a n d
issues. In M o r g a n JP, K a g a n DV, B r o d y JS, editors.
P h e n y l p r o p a n o l a m i n e : risks, benefits, a n d controversies.
N e w Y o r k : P r a e g e r Publishers, 1 9 8 5 : 3 - 1 0 .
5. Lake CR, G a l l a n t S, M a s s o n E, M i l l e r P. A d v e r s e d r u g
effects a t t r i b u t e d t o p h e n y l p r o p a n o l a m i n e : a r e v i e w o f
142 case reports. A m J M e d 1990; 8 9 : 1 9 5 - 2 0 8 .
6. F o r m a n HP, Levin S, S t e w a r t B, Patel M , Felnstein S.
C e r e b r a l vasculitis a n d h e m o r r h a g e in a n a d o l e s c e n t t a k ing d i e t pills c o n t a i n i n g p h e n y l p r o p a n o l a m i n e : case
r e p o r t a n d r e v i e w o f l i t e r a t u r e . Pediatrics 1989;
83:737-741.
7. S l o a n M A , K i t t n e r SJ, R i g a m o n t i D, Price TR. O c c u r r e n c e o f
s t r o k e associated w i t h use/abuse o f d r u g s . N e u r o l o g y
1991; 4 1 : 1 3 5 8 - 1 3 6 4 .
8. H a m i l t o n RS, S h a r i e f f G. P h e n y l p r o p a n o l a m i n e - a s s o c i a t e d
i n t r a c r a n i a l h e m o r r h a g e in a n i n f a n t . A m J E m e r g M e d
2000; 18:343-345.
9. Kase CS, M o h r JP, C a p l a n LR. I n t r a c e r e b r a l h e m o r r h a g e . In
r
c* JJ
Li_r
J J J JZJ
— I
symptoms. If your patients have questions
about over-the-counter medications they have
at home, suggest they bring them in the original packaging to one of their health care
providers or pharmacist, since many manufacturers have or are in the process of reformulating PPA-containing products.
•
Acknowledgments.
I wish to thank Dr. Teresa Seo and Dr.
manuscript.
Steven Durst for their helpful
comments
on this
B a r n e t t H J M , M o h r JP, Stein BM, Y a t s u F M , editors. S t r o k e
p a t h o p h y s i o l o g y , diagnosis, a n d m a n a g e m e n t . N e w York:
Churchill Livingstone, 1 9 9 8 : 6 5 9 - 6 6 0 .
10. W e r t h e i m e r A l . P h e n y l p r o p a n o l a m i n e p r e p a r a t i o n s , m a r k e t i n g , a n d economics: U.S. a n d a b r o a d . In M o r g a n JP,
K a g a n DV, Brody JS, editors. P h e n y l p r o p a n o l a m i n e : risks,
benefits, a n d controversies. N e w Y o r k : P r a e g e r Publishers,
1985:37-52.
11. F o o d a n d D r u g A d m i n i s t r a t i o n C e n t e r f o r D r u g E v a l u a t i o n
a n d Research. Public h e a l t h advisory. Subject: safety o f
phenylpropanolamine.
http://www.fda.gov/cder/drug/infopage/ppa/advisory.htm.
Accessed 1 / 2 3 / 0 1 .
12. F o o d a n d D r u g A d m i n i s t r a t i o n N o n p r e s c r i p t i o n D r u g s
A d v i s o r y C o m m i t t e e . T h e safety o f p h e n y l p r o p a n o l a m i n e
h y d r o c h l o r i d e (PPA) used in O T C w e i g h t c o n t r o l a n d nasal
d e c o n g e s t a n t d r u g products.
http://www.fda.gov/ohrms/dockets/ac/00/backgrd/3647b1.
h t m . Accessed 1/23/01.
13. Jick H, A s e l t o n P, H u n t e r JR. P h e n y l p r o p a n o l a m i n e a n d
c e r e b r a l h a e m o r r h a g e [ l e t t e r ] . Lancet 1984; 1:1017.
14. L e p p a l á J M , V i r t a m o J, F o g e l h o l m R, A l b a n e s D, H e i n o n e n
OP. D i f f e r e n t risk factors f o r d i f f e r e n t s t r o k e subtypes
association o f b l o o d pressure, cholesterol, a n d a n t i o x i d a n t s . S t r o k e 1999; 3 0 : 2 5 3 5 - 2 5 4 0 .
15. T i e t z e KJ. Disorders r e l a t e d t o cold a n d allergy. In: A l l e n
LV, B e r a r d l RR, D e S i m o n e E M , eds. H a n d b o o k o f n o n p r e scription d r u g s 1 2 t h e d . 2 0 0 0 : 1 8 3 - 1 8 4 .
16. A b r a m o w i c z M , Z u c c o t t i G, Rizack M A , e t al, e d i t o r s .
Phenylpropanolamine and other OTC alpha-adrenergic
agonists. M e d Lett Drugs T h e r 2 0 0 0 ; 4 2 : 1 1 3 .
ADDRESS: Tracey L. Mersfelder,
Cherry Street SE, Grand Rapids,
PharmD,
7 7 5 Xavier
Ml
49503.
Hall,
220
Category 1 CME Credit.
Test your knowledge
of clinical topics.
IN THIS ISSUE
PAGE 263
223 C L E V E L A N D CLINIC JOURNAL OF MEDICINE
V O L U ME 6 8 • NUMBER 3
Downloaded from www.ccjm.org on June 15, 2014. For personal use only. All other uses require permission.
MARCH
2001










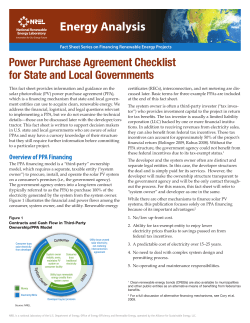
© Copyright 2026