
Document 231263
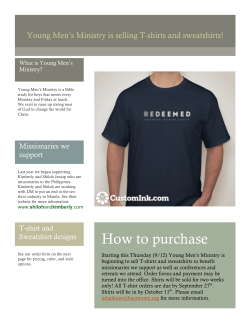
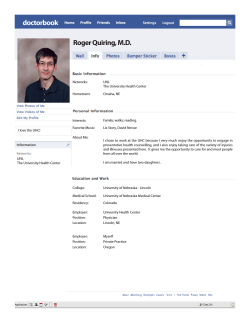
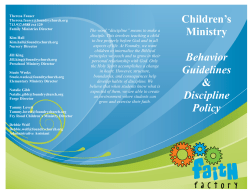
$ "% ()#(*!(&'( ! Dz ǣ dz ʹͶǦʹǡʹͲͳʹ ǡ TableofContents ExecutiveSummary.............................................................................................................................1 Introduction.........................................................................................................................................5 WorkshopObjectivesandFormat........................................................................................................6 WorkshopHost.........................................................................................................................................7 WorkshopParticipants..............................................................................................................................7 WorkshopOrganizers................................................................................................................................8 WorkshopThemesandTakeaways......................................................................................................9 WorkshopEvaluations.......................................................................................................................12 ConclusionsandNextSteps...............................................................................................................13 Annexes.............................................................................................................................................14 Annex1–TheRAMEDSiteVisits............................................................................................................14 Annex2–DetailedAgenda.....................................................................................................................17 Annex3–FinalWorkshopParticipantList.............................................................................................20 Annex4–MarrakechDeclaration..........................................................................................................28 Annex3–WorkshopEvaluationSummary.............................................................................................29 Ascountriesstrivetoachieveuniversalhealthcoverage(UHC),ensuringequalaccesstoquality health care for the poorest remains a major challenge. Many African countries are experimentingwithdifferentapproachesandmechanismstoimproveaccesstohealthcarefor thistargetpopulation,yetnonehasyetprovedtotallysuccessfulinimprovingaccesstohealth careforthepoorestonanationalscale.IncoͲoperationwiththeMoroccangovernment,the JointLearningNetworkforUniversalHealthCoverage(JLN),andUNICEF,theHarmonizationfor Health in Africa (HHA) Financial Access to Health Services Community of Practice (FAHS CoP) organized a fourͲday workshop, from September 24Ͳ27 in Marrakech, Morocco on improving access to health care for the poorest. The workshop’s focus was discussion and experience sharinginordertodiagnose,understandandidentifystrategiestoovercomethechallengesof covering the poorest, as well as site visits to learn from the recent scaleͲup of RAMED, Morocco’smedicalassistanceschemetocoverthepoor. Over90participantsfromBenin,Coted’Ivoire,Ethiopia,Ghana,Kenya,Mali,Morocco,Nigeria, Rwanda and Senegal came together with CoP members, experts from Cambodia, Vietnam, India, and international organizations. Participants included a mix of technical experts, senior level policy makers, and parliamentarians who engaged in dynamic dialogue and exchange, interactingfreelyandopenlywitheachotheroverthefourdaysoftheworkshop,andworking insmallercollaborativegroupstodevelopconcretecountryactionplans.Morocco’sMinisterof Healthpresidedovertheopeningceremony,andpresscoverageoftheeventwassignificant. TheworkshopagendaincludedframingandcomparativepresentationsonDay1,sitevisitsto RAMED facilities on Day 2, analysis of challenges faced on reaching the poor on Day 3, and political views on equity in UHC, sustainability issues, and sharing of country action plans on Day4.Highlightsoftheworkshop’smethodologicalapproachesincluded: Plenarysessionswerehighlyinteractive. Countryworkgroupsessionsprovidedanopportunityforcountriestoconveneinsmall groupstoholdindepthdiscussionsandcollaborativelydevelopcountryactionplans. The workshop agenda was flexible and allowed for adjustments that gave countries moretimeforgroupworksessions. ThesitevisitstoobserveimplementationofRAMEDencouragedworkshopparticipants toengagedirectlywithpractitioners,andprogramadministrators,aswellastoanalyze thestrengthsandweaknessesofaconcreteexampleofaprogramtoreachthepoorest, andtousethislearningtobothprovidefeedbacktoMoroccoandtoinformthedesign andimplementationoftheirowncountry’sprogramtoreachthepoorest. 1|P a g e The workshop confirmed that much remains to be learned and documented about how to effectively target and cover the poorest within a context of UHC. Some of the key learnings fromthe4daysofvibrantexchangeincludethefollowingpoints. Defining and identifying the target population remains a major problem, and social protectionprogramsbetterunderstandwhothepoorestare.Countriesneedtomove towards uniform criteria and intersectoral approaches to target the poor, and better classifypoverty(temporary/seasonalvspermanent).Participantsnotedthathealthcare needs to be integrated into the wider scope of social protection programs and other initiatives to reach the poor, and that poverty targeting mechanisms should be harmonized. Participants also called for the need to consider broader social and economicfactorsresultinginpoverty. There is broad consensus that strong political will and commitment are needed to carry programs for the poorest forward; specifically to mobilize resources, identify challenges and adapt to them, and ensure a continuous equity focus. However, political will alone is not sufficient. Elections and social movements such as the Arab Springcanpropelpoliciestocoverthepoorestforward,aswasthecasewiththerapid scaleͲupoftheRAMEDinMorocco.Theformulationoftheseprogramsmust,however, be the result of a comprehensive analysis of the context to understand all the contributingfactorsthatrestrictaccesstohealthservices,andtoidentifyareaswhere bottlenecksmayoccurinprovision,demand,andqualityofservicesandinterventions. Programbeneficiariesandcivilsocietyorganizationsmusthaveaclearrolethroughout theprocess. Financial sustainability is a serious concern. Financial sustainability of programs to coverthepoorestremainsamajorchallenge,andalthoughthereisconsensusthatuser fees must be removed, most countries have insufficient resources to finance such programs over time. Key principles thus include putting in place progressive and innovativewaysofraisingsufficientrevenues,establishinglargeriskandresourcepools and avoiding fragmentation, improving efficiencies and equity of resource allocation, andintegratingthesereformsintoacomprehensivehealthfinancingstrategy.It’slikely, however,thatlowerincomecountriesmayneedsignificantexternalassistanceforthe mediumtermtoextendcoveragetothepoorest. Active vs passive targeting of the poorest? Both are necessary. Most participants agreed that some combination of active targeting (identifying the beneficiary before he/she falls ill) and passive targeting (identifying the person once they are sick and in contact with the health system) is necessary to cover the poorest. However, ensuring thatthiscoverageofthepoorestisactuallyeffective–thatbeneficiariesactuallyusethe services they need – is not monitored in most cases, and needs to be. There are also tradeͲoffs and choices that must be made to effectively target eligible populations, 2|P a g e especiallyinruralareaswherepovertytendstobemoregeneralized.Severalparticipant countries use communityͲbased processes and local commissions to identify and determine eligibility of the poor, which may reduce potential errors of exclusion or inclusion through their geographic proximity to and familiarity with communities, inclusive processes, and accountability. In some countries, however, the familiarity of local authorities with the population has resulted in unfair privileges for some community members over others (leakage). Passive targeting relies on effective communication, and yet participants highlighted the general lack of awareness and adequate information about programs targeting the poorest especially among beneficiaries, but also with communities, healthcare workers, social workers, health serviceprovidersandlocalgovernments. Strongmonitoringandevaluationsystemsareneededtoevaluatehowwellprograms aredoing.Itisessentialtoputinplaceasystemwithclearindicatorsandreliabledata sources to monitor progress, manage problems, and evaluate performance. The frequent absence of reliable, systematically collected data at the community level makes evaluating the effectiveness of mechanisms to reach the poorest difficult, as evidencedbyMali’sstruggletomeasuretheimpactofitsRAMED.Ghanatheoretically coversthepoorestthroughtheNationalHealthInsuranceScheme(exemptions),butitis having to reͲthink its data collection strategy, which currently does not allow specific identification or tracking of this group. Participants also called for more inclusion of beneficiary voices in monitoring programs to reach the poorest. In Cambodia, managementoftheHealthEquityFund(HEF)isentrustedtoanindependentthirdparty (usuallyanNGO). One goal, multiple pathways Ͳ there is no one solution to reaching the poorest and country contexts are important. While there exists a wide range of mechanisms and institutionaldesignsusedtoincreasecoverageofthepoorest,theconsensusisthatthe time has come for action everywhere. A longͲterm vision is essential, yet countries havingmadesignificantprogressshowthatthepathtakenwilllikelybetheoutcomeof politicalcontestationandinclusivepolicydialogues.Becausetheprocessisincremental, flexibility and a strong monitoring and evaluation system are key to chart progress, makeadjustments,andensurethatpublicresourcesarebeingtargetedtowardsmore equity. The participation and empowerment of the target population can help build a constituencyandcriticalmasstoapplyconsistentpressureforcontinuedpublicsupport totheprogramovertime. Theworkshopevaluationshowedaveryhighlevelofappreciationfortheworkshopformatand content(sitevisitsuseful,exchangeswithpeersstimulating,majorityplannedtofollowͲupwith otherparticipants).Participantswerelesscertainthattheactionplansdevelopedwerelikelyto 3|P a g e beimplemented,pointingtotheimportanceofensuringcontinuityandmobilizingsupportfor countryͲlevelworkshopfollowͲup. Manycountrieshavealreadybeguntotranslatetheirplanstoaction,withthedelegationfrom Ghanareportingwithindaysoftheworkshopthattheyhadintroducedanamendmenttothe Ghana National Health Insurance Bill mandating the National Health Insurance Authority to annuallyreportonequityofaccesswithinGhana’sNationalHealthInsuranceScheme.Nigeria expressedaninterestinlearningmoreabouttheCambodiaHealthEquityFundastheyworkto set up their Vulnerable Groups Fund, Kenya is interested in learning more about Ghana’s planned study to determine whether the National Hospital Insurance Scheme’s targeting mechanisms are effective in identifying and registering the poor, and Mali plans to make a studytourtoGhana. In the coming weeks and months, the FAHS CoP, in collaboration with the JLN and other partners,willcontinuetominetheexchangesandlearningfromtheMarrakechworkshoptobe shared in editorials, blogs and onͲline discussions. The baseline information gathered from participatingcountrieswillalsobefurthersynthesizedandpublishedasacomparativearticle onthestatusofequityinUHC.Wewillworkwithparticipantcountriestofurtherdocumentthe stagestowardcoveringthepoorestontheirrespectivepathtoUHC;andtracktheirprogress against the action plans developed in Marrakech. Where possible, the CoP will work to consolidateexistingtoolsbeingusedtoimplementprogramstoreachthepoorest(notablyfor identification) and make them available through onͲline platforms. One or more inͲdepth discussions on key challenges will be held as a webinar, and inͲdepth interviews with participantsfromMarrakechwillbeconductedtodocumentprogressmade. In response to Morocco’s expressed interest in further documenting, monitoring, and evaluatingtheRAMEDexperience,theInstituteofTropicalMedicine–Antwerphasproposeda set of potential research activities to the Ministry of Health. The CoP and its partners stand readytoaccompanythegovernmentinMoroccointheseandotheractivities,andwillcontinue toshareevidenceandexperienceontheevolutionoftheRAMEDthroughCoPplatforms. Countriesrecognizethatthereisnoonesolutionforimprovingaccesstohealthservicesforthe poorest. They are eager to learn from, and benefit greatly from opportunities to share and exchange experiences with peers facing similar challenges. Plans to learn further from each otherwerehatchedinMarrakech.Ascountriesseektogathertheevidenceonhowtobetter cover the poorest and most vulnerable in their steps toward universal health coverage, the FAHS CoP will continue to provide a dynamic forum for dialogue, discussion, and practical, handsͲonlearningexperiencestohelpthemreachtheirgoals. 4|P a g e Ascountriesstrivetoachieveuniversalhealthcoverage(UHC),reduceoutofpocketpayments andprovidegreaterfinancialprotectionforallcitizens,ensuringequalaccesstoqualityhealth care for the poorest remains a major challenge. Despite noble intentions, all too often programs to reach the poorest do not realize their objectives: access to health care for the poorestremainsminimalandallocatedresourcesarefrequentlyabsorbedbyotherpopulation categories. Many African countries are experimenting with different approaches and mechanisms to improve access to health care for this target population: equity funds, subsidies for health insurance premiums, health care vouchers and even cash transfers. However, none of these mechanismshasyetprovedtotallysuccessfulinimprovingaccesstohealthcareforthepoorest onanationalscale,highlightingamajorchallengetoreachinguniversalhealthcarecoverage. Although there is no one size fits all approach to reaching the poorest, countries face similar challenges in identifying and defining the poor, sustaining political commitment, mobilizing resources, creating awareness and monitoring the progress and impact of their programs to reach the poor, among others. Shared learning approaches can play an important role in promoting dialogue and exchange among countries grappling with these complex issues, allowing them to critically reflect on progress, jointly problem solve and draw on context specificevidencefromothercountries,toarriveatsolutionsthatmeettheirneeds. IncoͲoperationwiththeMoroccangovernmentandtheJointLearningNetworkforUniversal HealthCoverage(JLN),theHealthforHarmonizationinAfrica(HHA)FinancialAccesstoHealth Services Community of Practice (FAHS CoP) organized a four day workshop, from September 24Ͳ27inMarrakech,Moroccoonthetopicofimprovingaccesstohealthcareforthepoorest. The workshop’s topic and focus on promoting discussion and experienceͲsharing in order to diagnose, understand and identify strategies to overcome the challenges of covering the poorest, were identified as priorities by members of the FAHS CoP, JLN countries and supporting partners. Embedding site visits in the workshop program to both observe the practical implementation issues of the RAMED (Régime d’Assistance Médicale), Morocco’s medicalassistanceforthepoor,andtoshareobservationsandfeedbackonscaleͲupofRAMED, wasalsoanimportantfeatureoftheworkshop.Morocco’sMinisterofHealthpresidedoverthe opening ceremony, and press coverage of the event was significant. Workshop preparations included a planning visit to Morocco (June 2012), the convening of an organizing committee that met virtually biͲmonthly, and background research and country interviews to compile “countrysheets”onparticipatingcountries’programstocoverthepoorest. Over90participantsfromBenin,Coted’Ivoire,Ethiopia,Ghana,Kenya,Mali,Morocco,Nigeria, Rwanda and Senegal came together over the four days to engage in interactive peerͲtoͲpeer exchange and learning on the topic of expanding health coverage to the poorest. Country 5|P a g e delegations and CoP members were joined by experts from Cambodia, Vietnam, India, and international organizations. The participants included a mix of technical experts, senior level policy makers, and parliamentarians who engaged in dynamic dialogue and exchange, interactingfreelyandopenlywitheachotheroverthefourdaysoftheworkshop,andworking todevelopconcretecountryactionplans.AfullparticipantlistisincludedinAnnex3. Thisdocumentsummarizestheproceedingsfromtheworkshopreportandreflectskeythemes thatemergedfromdiscussions.Additionalinformationabouttheworkshop,includingsession presentations can be found on the Health for Harmonization in Africa website: http://www.hhaͲonline.org/hso/marrakesh. ThemainobjectivesoftheSeptember24Ͳ27,2012workshopon“EquityinUniversalCoverage: HowtoReachthePoorest”wereto: Identifyanddocumentefficientstrategiestocoverthepoorest(fromAfricancountries andothercountrieswhererelevant); Diagnose how and why mechanisms intending to cover the poorest have been less successfulthandesiredandseeksolutionstoovercomeweaknesses; Identify gaps in knowledge concerning coverage of the poorest and define research priorities; Linkstrategiesforcoverageofthepoorestwithotherfinancialstrategiesforuniversal healthcarecoverage; Support countries in drawing up action plans to improve their policies on access to healthcareforthepoorest. Theworkshopwasdesignedtofacilitatepeertopeerlearningandexchangebetweencountries andamongvariousactorsfromeachcountry.Theagendafortheworkshopfollowedthehigh leveloutlinebelow:overviewandframingpresentationsonDay1,sitevisitstoRAMEDfacilities on Day 2, analysis of challenges faced in reaching the poor on Day 3, and political views on equityinUHC,sustainabilityissues,andsharingofcountryactionplansonDay4. Adetailed workshopagendawithsessiontitlesandpresenterinformationisincludedinAnnex2. Day1 Day2 Day3 Day4 Workshopframingandsharingofexperiencesamongparticipatingcountrieson differentmechanismstocoverthepoorestanddiscussionofhealthequity SitevisitstoobserveimplementationofRAMED Analysis of the challenges faced in covering the poorest (analysis at countryͲ levelandcomparativeanalysis),sharingoffeedbackonRAMED PoliticalviewsonequityinUHC,sustainabilityissues,sharingofcountryaction plans,andworkshopwrapͲup 6|P a g e Highlightsoftheworkshop’smethodologicalapproachincluded: Plenarysessionswerehighlyinteractive. Countryworkgroupsessionsprovidedanopportunityforcountriestoconveneinsmall groupstoholdindepthdiscussionsandcollaborativelydevelopcountryactionplans. The workshop agenda was flexible and allowed for adjustments that gave countries moretimeforgroupworksessions. ThesitevisitstoobserveimplementationofRAMEDencouragedworkshopparticipants toengagedirectlywithpractitioners,andprogramadministrators,aswellastoanalyse thestrengthsandweaknessesofaconcreteexampleofaprogramtoreachthepoorest, andtousethislearningtobothprovidefeedbacktoMoroccoandtoinformthedesign andimplementationoftheirowncountry’sprogramtoreachthepoorest.(SeeAnnex1) WorkshopHost:MinistryofHealth,Morocco SincethefirstFAHSCoPworkshopheldinNovember2011inBamako,Malionmaternalhealth fee exemptions, Morocco has played a dynamic leadership role in the CoP. Given that expanding access to healthcare for the poorest was a top priority for the government of Morocco,CoPmembersfromthehighestlevelsoftheMoroccanMinistryofHealthpresentat theBamakoworkshopsuggestedhostingthenextannualCoPevent.AsRAMEDwaspreparing to expand from a pilot phase to a national level program, Morocco proved to be a unique concretelearningopportunity,aswellasanenthusiastic,engagedhostcountryandworkshop coͲorganizer. Aware of the many challenges of scalingͲup such a program Ͳ from technical implementation issuesassociatedwithidentifyingandenrollingthepoor,tofinancialsustainabilityconcerns,to sustaining political will and government commitment Ͳ and recognizing that other countries facesimilarchallenges,MoroccowaskeentohostaCoPworkshopthatwouldbringtechnical expertsanddecisionmakerstogethertoreviewtheevidencebaseonmechanismstoreachthe poorestandtosharecountryexperiences,andtoprovidefeedbackandinsightsontheRAMED withinacontextofUHC.Morocco’spilotexperienceimplementingRAMEDandrecentscaleͲup of the program offered an opportunity for workshop participants to see and discuss the practical implementation issues of programs designed to cover the poorest. Marrakech was selected as the venue for the workshop because of its proximity to RAMED implementation sites. WorkshopParticipants The workshop convened country delegations and CoP members from ten African countries (Anglophone and Francophone): Benin, Côte d’Ivoire, Ghana, Kenya, Mali, Morocco, Nigeria, Rwanda, Senegal and Ethiopia. Delegations included high level decision makers, technical 7|P a g e expertsinvolvedinimplementingprogramsandpoliciestocoverthepoorest,practitionerswith direct operational experiencesand parliamentarians. Somewhat lacking from delegations was representation from civil society and from outside the health sector. Workshop participants also included experts from “resource countries1” Cambodia, India, Vietnam and several internationalorganizations.AfullparticipantlistisincludedinAnnex3. Participant countries were selected based on their engagement in universal health coverage reformsandcurrentimplementationofstrategiestoreachthepoorest,aswellasthepresence ofapartnerwillingtofundtheirparticipation. WorkshopOrganizers FAHSCoP2 The Financial Access to Health Services Community of Practice (FAHS CoP) supports the development and implementation of initiatives and policies to improve financial access to healthcareinAfricaandtopromoteconstructivesharingofexperienceandexpertiseamong countries. By mobilizing experts working on policies and mechanisms to improve financial accessacrossthecontinent–throughvirtualexchangesandduringworkshops–theFAHSCoP actsasaforumtogatherandshareknowledgeamongitsmembers.TheCoPalsoservesasa platformtocoordinateinitiativesledbydifferentactorsandsupportingagencies. JLN3 TheJointLearningNetworkforUniversalHealthCoverage(JLN)isaplatformforknowledge andsouthͲsouthexchangesforcountriesimplementinghealthcarefinancingreforms.Theaim istoimprovefinancialprotectionandaccesstohealthcareserviceswithinauniversalhealth carecoverageframework. Since its creation in 2010, the JLN has ten country members: Ghana, India, Indonesia, Kenya, Malaysia, Mali, Nigeria, the Philippines, Thailand and Vietnam. The JLN is built around four technical tracks, defined by members of the network: provider payment mechanisms, informationsystems,expandingcoverage.Itisthroughits“ExpandingCoverage(EC)”trackthat the JLN supported theCoP workshop in Morocco. The EC track facilitates knowledge transfer and exchange among member and resource countries across the benefit (essential and costͲ effectiveinterventions)andpopulation(informalsector,disadvantagedgroups)dimensions. TheGovernmentofMorocco The topic of medical coverage for the poor is a major focus for the Governmentof Morocco sinceitconcernssome8.5millioninhabitants,inotherwords,around28%ofthepopulation. InNovember2008,Moroccobeganpilotingamedicalassistancescheme(RAMED)intheTadla 1 Withlonger,yetstillfairlyrecentexperiencethanparticipantcountriesandsignificantprogressincoveringthepoorest,these countrieswereinvitedasresourcecountriestosharelessonsandadvice. 2 http://www.hhaͲonline.org/hso/financing/group/accesstoservices 3 http://www.jointlearningnetwork.org 8|P a g e Azilalregion(targetpopulationof420,000inhabitantsoutofatotal1.5million).Assessmentof the pilot phase in 2010 led to recommendations about scaling up RAMED, which, on orders from the King of Morocco, was launched on a national scale in 2012, one year prior to its plannedextension. TheMinistryofHealthhasputanationalobservatory,alongwithregionaloffices,inplaceto document and monitor the scaleͲup process (and ultimately, to measure equity in access to healthservices).Theobservatory,afeatureofthesitevisits,providesongoingsupporttothe scaleͲupofRAMEDandistaskedwithreportingonissuesthatmayarise. UNICEF/WestandCentralAfricaRegionalOffice(WCARO) In2012,UNICEFadoptedastrategicframeworkforsocialprotection4,aimingtoextendhealth carecoveragesupportedbysustainableandequitablefinancialsystems.Since2010,UNICEFis also at the forefront in terms of support to the HHA strategy to strengthen Communities of Practice. The workshop confirmed that much remains to be learned and documented about how to effectively target and cover the poorest within a context of UHC. Some of the key learnings fromthe4daysofvibrantexchangeincludethefollowingpoints. Defining and identifying the target population remains a major problem, and social protectionprogramsbetterunderstandwhothepoorestare.Countriesneedtomove towards uniform criteria and intersectoral approaches to target the poor, and better classify poverty (temporary/seasonal –vsͲ permanent). Participants noted that healthcare needs to be integrated into the wider scope of social protection programs andotherinitiativestoreachthepoor,andthatpovertytargetingmechanismsshould beharmonized.InGhanatheNationalHealthInsuranceAuthority(NHIA)haspartnered withasocialprotectionprogramtodevelopanationaltargetingmechanism.Cambodia recognizes the need to harmonize and integrate the Health Equity Fund (HEF) into a wider social health protection framework. Participants called for the need to consider broadersocialandeconomicfactorsresultinginpoverty. There is broad consensus that strong political will and commitment are needed to carry programs for the poorest forward; specifically to mobilize resources, identify challenges and adapt to them, and ensure a continuous equity focus. However, political will alone is not sufficient. Elections and social movements such as the Arab Springcanpropelpoliciestocoverthepoorestforward,aswasthecasewiththerapid 4 http://www.unicef.org/socialprotection/framework/index_61841.html 9|P a g e scaleͲupofRAMEDinMorocco.Theformulationoftheseprogramsmust,however,be theresultofacomprehensiveanalysisofthecontexttounderstandallthecontributing factors that restrict access to health services, and to identify areas where bottlenecks may occur in provision, demand, and quality of services and interventions. Program beneficiaries and civil society organizations must have a clear role throughout the process.InIndia,despitethefactthathealthcareisahighlypoliticizedissue,effortsto coordinate policy discussions with operational aspects of programs to reach the poor havenotbeensuccessful.Severalcountriesnotedhowtensionsbetweenfederaland state structures hindered progress in expanding coverage. In Senegal and in Mali, despite strong support from the Ministry of Health, the Equity Fund and RAMED are strugglingtoattractlocalgovernmentinterestandfunding.InNigeria,whereeachstate decidesitsownhealthpolicy,progressinscalingͲupprogramstoreachthepooresthas beenslowduetothelackofstateͲlevelbuyͲinandcommitment. Financial sustainability is a serious concern. Financial sustainability of programs to coverthepoorestremainsamajorchallenge,andalthoughthereisconsensusthatuser fees must be removed, most countries have insufficient resources to finance such programs over time. Key principles thus include putting in place progressive and innovativewaysofraisingsufficientrevenues,establishinglargeriskandresourcepools and avoiding fragmentation, improving efficiencies and equity of resource allocation, andintegratingthesereformsintoacomprehensivehealthfinancingstrategy.It’slikely, however,thatlowerincomecountriesmayneedsignificantexternalassistanceforthe mediumtermtoextendcoveragetothepoorest. Active vs passive targeting of the poorest? Both are necessary. Most participants agreed that some combination of active targeting (identifying the beneficiary before he/she falls ill) and passive targeting (identifying the person once they are sick and in contact with the health system) is necessary to cover the poorest. However, ensuring thatthiscoverageofthepoorestisactuallyeffective–thatbeneficiariesactuallyusethe services they need – is not monitored in most cases, and needs to be. There are also tradeͲoffs and choices that must be made to effectively target eligible populations, especiallyinruralareaswherepovertytendstobemoregeneralized.Manyparticipant countries use communityͲbased processes and local commissions to identify and determine eligibility of the poor, which may reduce potential errors of exclusion or inclusion through their geographic proximity to and familiarity with communities, inclusive processes, and accountability. In some countries, however, the familiarity of local authorities with the population has resulted in unfair privileges for some community members over others (leakage). Passive targeting relies on effective communication, and yet participants highlighted the general lack of awareness and adequate information about programs targeting the poorest especially among beneficiaries, but also with communities, healthcare workers, social workers, health serviceprovidersandlocalgovernments. 10|P a g e Dr. Tran Van Tien (Ministry of Health, Vietnam) explained that Vietnam has adopted nationalguidelinestoidentifythepoorin 50,000villages, basedonmeansandproxyͲ means testing. A community targeting process that involves multiple representatives (medical, social, head of village, civil, etc.) is used. In Ghana, the NHIS promotes community ownership and a participatory process of identification and enrolment, in order to strengthen transparency and accuracy. In Cambodia, households are preͲ identified at the community level through screening and postͲidentified at health facilities through interviews. A common constraint in these community targeting processes is their timeͲintensive nature, which may result in temporary exclusion and havedifficultykeepingpacewithpovertydynamics. WhileMoroccodidemployacommunicationcampaigntolaunchtheRAMED–including campaigns, television spots and advertisements, and pamphlets Ͳ participants noted that RAMED primarily uses a passive identification process. There was general agreementthatthisapproachcanfailtocapturethosewhoneedtoaccessservicesthe most,thepoorestinhardtoreachruralareas,andthevulnerable.AsnotedbyThiMinh Phuong Ngo (UNICEF) in her presentation, targeting that occurs when patients are ill oftenresultsinerrorsofinclusionandexclusion. Strongmonitoringandevaluationsystemsareneededtoevaluatehowwellprograms aredoing.Itisessentialtoputinplaceasystemwithclearindicatorsandreliabledata sources to monitor progress, manage problems, and evaluate performance. The frequent absence of reliable, systematically collected data at the community level makes evaluating the effectiveness of mechanisms to reach the poorest difficult, as evidencedbyMali’sstruggletomeasuretheimpactofitsRAMED.Ghanatheoretically coversthepoorestthroughtheNationalHealthInsuranceScheme(exemptions)butitis having to reͲthink its data collection strategy, which currently does not allow specific identification or tracking of this group. Participants also called for more inclusion of beneficiary voices in monitoring programs to reach the poorest. In Cambodia, managementoftheHealthEquityFund(HEF)isentrustedtoanindependentthirdparty (usuallyanNGO). ParticipantslearnedabouttheITsystemputinplaceforMorocco’sRAMEDtofiledaily and monthly activities, collect referral and counterͲreferral data, and monitor RAMED casesatthehospitallevel5. One goal, multiple pathways Ͳ there is no one solution to reaching the poorest and countrycontextsareimportant. 5 RAMEDisoperationalatthehospitallevelashealthservicesatlowerlevelsofthehealthsystemareprovidedforfree. 11|P a g e While there exists a wide range of mechanisms and institutional designs used to increase coverage of the poorest, there is broad consensus that now is the time for actioneverywhere,andthatpaststrategieshavenotbeeneffective.AlongͲtermvision isessential,yetcountrieshavingmadesignificantprogressshowthatthepathtakenwill likely be the outcome of political contestation and inclusive policy dialogues. Because theprocessisincremental,flexibilityandastrongmonitoringandevaluationsystemare key to chart progress, make adjustments, and ensure that public resources are being targeted towards more equity. The participation and empowerment of the target populationcanhelpbuildaconstituencyandcriticalmasstoapplyconsistentpressure forcontinuedpublicsupporttotheprogramovertime. During the workshop, ‘live’ evaluations were undertaken in order to understand the participants’ views of the content and format of the workshop activities. These evaluations weredonewiththe“TurningPoint”technology,whichallowspollstobecarriedoutwiththe useofMSPowerPointand“clickers”distributedtorespondents. OnͲtheͲspotevaluationswereconductedduringthreesessionsofquestions;theresponserate was 80% on average for each question. Questions focused on the usefulness of the different sessions,theworkinggroupsonactionplans,andthegeneralqualityoftheworkshop.Thefull resultsoftheevaluationscanbefoundinAnnex5,butselectedresultsarepresentedbelow. 100%oftherespondentsfoundthefieldvisitusefulorveryuseful. 90%oftherespondentsagreedorstronglyagreedfoundthesmallgroupdiscussionson thefieldvisitsdynamicandstimulating,and72%founditpertinentorverypertinentto brainstormonanactionplanfortheircountry. 50%oftheconcernedrespondentsansweredthattheactionplantheyworkedonwould verylikelyplayaroleintheircountry’sstrategiesaftertheirreturn.33%answeredthat itwassomewhatlikely,while17%thoughtthatitwasnotverylikelyornotlikelyatall. 95%foundthatasofday3,thecontentandthelevelofexchangehadbeenthoughtͲ provokingforthem. 95% agreed or strongly agreed with the statement that, overall, the process of describingtheirowncountrychallengescausedthemtoreflectandthinkconstructively abouttheircountry’ssituation. 98%agreedorstronglyagreedwiththestatementthattheworkshophadbeenvaluable forthemoverall. 91%agreedorstronglyagreedwiththestatementthattheyexpectedtofollowupwith otherparticipantsfromtheworkshopafterwards. 12|P a g e Manycountrieshavealreadybeguntotranslatetheirplanstoaction,withthedelegationfrom Ghanareportingwithindaysoftheworkshop,thattheyhadintroducedanamendmenttothe Ghana National Health Insurance Bill mandating the National Health Insurance Authority to annuallyreportonequityofaccesswithinGhana’sNationalHealthInsuranceScheme.Rather thanissuingaformaltraditionalworkshopdeclaration,participantswereinspiredbytherecent documentary “AhͲ les indigents” (by Malam Saguirou) to issue the “Marrakech Declaration,” shared on the HHA Facebook page (www.facebook.com/hhacops), which, in the spirit of the CoP, is an individual call to action to improve coverage of the poorest and most vulnerable (includedasAnnex5). In the coming weeks and months, the FAHS CoP, in collaboration with the JLN and other partners,willcontinuetominetheexchangesandlearningfromtheMarrakechworkshoptobe shared in editorials, blogs and onͲline discussions. The baseline information gathered from participatingcountrieswillalsobefurthersynthesizedandpublishedasacomparativearticle onthestatusofequityinUHC.Wewillworkwithparticipantcountriestofurtherdocumentthe stagestowardcoveringthepoorestonthepaththeUHC;andtracktheirprogressagainstthe actionplansdevelopedinMarrakech.Wherepossible,theCoPwillworktoconsolidateexisting toolsbeingusedtoimplementprogramstoreachthepoorest(notablyforidentification)and make them available through onͲline platforms. One or more inͲdepth discussions on key challengeswillbeheldasawebinar. In response to Morocco’s expressed interest in further documenting, monitoring, and evaluatingtheRAMEDexperience,theInstituteofTropicalMedicine–Antwerphasproposeda set of potential research activities to the Ministry of Health. The CoP and its partners stand readytoaccompanythegovernmentinMoroccointheseandotheractivities,andwillcontinue toshareevidenceandexperienceontheevolutionoftheRAMEDthroughCoPplatforms. Countriesrecognizethatthereisnoonesolutionforimprovingaccesstohealthservicesforthe poorest. They are eager to learn from, and benefit greatly from opportunities to share and exchange experiences with peers facing similar challenges. Plans to learn further from each other were hatched in Marrakech, with Ghana planning to bring a group back to Morocco, NigeriaexpressinganinterestinlearningmoreabouttheCambodiaHealthEquityFundasthey worktosetuptheirVulnerableGroupsFund,Kenyaidentifyinginterestinlearningmoreabout Ghana’s planned study to determine whether the National Hospital Insurance Scheme’s targetingmechanismsareeffectiveinidentifyingandregisteringthepoor,andMalihopingto makeastudytourtoGhana.Ascountriesseektogathertheevidenceonhowtobettercover thepoorestandmostvulnerableintheirstepstowarduniversalhealthcoverage,theFAHSCoP will continue to provide a dynamic forum for dialogue, discussion, and practical, handsͲ on learningexperiencestohelpthemreachtheirgoals. 13|P a g e Annex1TheRAMED–Sitevisits Fieldvisits Onthesecondday,fieldvisitswereconductedinthecommunesofMarrakesh,Essaouira(170 kmfromMarrakesh)andElKalaa(80kmfromMarrakesh).Participantsvisitedthecommunity building,whereapplicationsandregistrationsareconducted.Theprocesswaspresentedtous by members of the permanent commission: the Caïd (district commissioner) and the Khalifa (deputyheadofdistrict)–bothcivilservants,appointedbyHisMajestytheKingofMorocco. InEssaouira,450applicationshavebeenprocessed,127poorandaround100vulnerable.Five to six vulnerable beneficiaries were not able to pay for the card. These cases are being reviewed.IntheLagunehealthcentre,44patientsareRAMEDbeneficiaries. 14|P a g e Applica ationpro ocedure 1. Applicationsaresubmittedto otheadministrativeoff ice. 2. Thelo ocalcommisssionreview wsitandcheccksitsautheenticity. 3. TheC Caïdsignsan nddatesthe eapplication nanddelive rsareceipt totheappliicant.Thisserves asan ninterimdoccumententittlingtheapp plicanttofreeeemergenccyhealthcareforaperiodof three emonths(orruntiltheoffficialRAMED Dcardisdellivered). 4. Inparallel,afield denquiryis conducted tofindout thelivingco onditionsofftheapplicaant.A repre esentativeoffthecommiissionwillco overonestr eet.Allappllicantsarereviewedino order toen nsureagainstterrorsofin nclusionore exclusion. 5. Follow wing 40 pro ocessed applications, th he commissi on represen ntatives crosss check all their inform mationfore eachapplicattion,toensu uretheauth enticityand deligibilityofftheapplicaant. 6. Applicationsaresenttothep prefecturefo orelectroniccregistrationanddecisiononeligibility. 7. The decision d is then sent baack. The responsecan bbe ‘eligible’ (poor or vu ulnerable) orr ‘not eligib ble’.Ifanap pplicationis turneddow wn,theappliicantcanap ppealforassecondrevieew.A further investigaation will be b conductted, to wh ich the ap pplicant, ph hysician or local comm missionmem mbermayad ddanyrelevaantinformattionorjustiffications. 8. Ifthe eapplicantisseligible,the eyarecalled dtotheadm ministrationo officetopickuptheircaard.If their statusis‘po oor’,thecardisfreeoffcharge.Ifttheirstatus is‘vulnerab ble’,a120DH Hfee per person p (up to t 600DH maximum m pe er householdd beyond five memberrs) is requireed to receivvethebene eficiarycard.Vulnerable ebeneficiari eshavelefttwithouttheircards,dueto lacko offunds.The eycanappeaaltobeclasssifiedaspooor. Figure1.A Applicationp procedureforrRAMED Step1:R RAMED applicationform submissiion Step6:Delliveryof cardsbyLo ocal Authority 155days Step22:Reviewof appliccationby LocalCommission n 30 0days 30days Step5:ANAM registersRA AMED cards Step33:Permanen nt LocalC Commission n enquiry Rejecttion/Appeaal (Walii,Governor) Step4:Re egional Permanen nt Commission:finalist 660days 15|P a g e Feedba ackfromp participa antsando observatio onsonRA AMED Strengths Weakne esses Identificationand dRegistratio on Permanentl P ocalcommisssiontoproccessapplicattionsandmonitor cant’seligibility Doubleenqu D uiryonapplic Illiteracyhassnotlimitedhighapplica ationnumbeers Adequateto A olstomanageapplicatio ons Possibilityto P oappealifap pplicationisrefused Coverrage/Serviccesprovided d Automatic A delivery d of application n receipt, applicants can beneffit from immediatee emergencycare Nopayment N atfirstpoin ntofcare,athealthcenttres Samelevelo S ofcoveragefforRAMEDaandnonRAM MEDbeneficciaries Coverageof C transportin ncaseofeme ergency Expensive E treatments are available to RAM ED beneficiaries (e.g. corneal transplant,d t dialysis) Wellorganis W edhealthsttructures Goodreferra G alsystem Weakn nesses Identifficationand dRegistratio on SelfͲdeclaration,passiverecruitmentt,application nfollowingillness Risk of fraud d, need for photograph hs of all ho usehold beneficiaries, not only motherandf m father Waitingtime W RAMEDcardfollowingappplication toreceiveR High H adminisstrative costts to proce ess applicatiions, conduct double eenquiries (ccentralandlocal) MonittoringandEvvaluation La ackoffeedb backonimpaactofRAMEDonseconddaryhealthccare Drugshortag D es,leadingttoOOPpaym ments Frequentrenewalofstatusandcardss(2to3yea rs) La ackofrealm monitoringandevaluatio onofthesysstemintheo observatory 16|P a g e Annex2ǦDetailedAgenda Sunday23 September Arrivals,transporttoMarrakesh 5:00–8:00PM Registrationofparticipants(HotelKenziFarah) DAY1–Monday24thSeptember 8:00–9:00AM Participantregistrationandwelcome 9:00–10:00AM Opening Presentationofparticipants WelcomefromtheFAHSCoP WelcomefromtheMoroccanMoH Presentationoftheworkshopobjectives Presentationoftheprogram Informationonlogistics,notablyregardingthefieldvisit (FAHSCoPfacilitatingteam) 10:00–10:40AM Frameworkpresentation:Universalcoverageandequity x Universalhealthcarecoverage x Fragmentationofpresenthealthcoverageindevelopingcountries (andparticularlyinAfrica) x Challengesandstakesofhealthcoverageforthe“poorest” Presenter:FahdiDkhimi,ITMͲAntwerp 10:40–11:10AM Coffeebreak 11:10AM–12:30PM Groupdiscussionsbetweenpeercountries Preparatoryworkfordevelopinganactionplan x Presentation/Analysisoftheprincipalinequalityindicators(if available) x Country’spresentsituationwithrespecttouniversalcoverage objectives(cube–universalcoverage) x Principalstrategyorstrategiesimplementedinordertocoverthe poorest x Principallessons(2)concerningcoverageofthepoorest(strengths, weaknessesofthesestrategies) 12:30–1:15PM OverviewofmechanismsimplementedinAfrica:summaryof experiencesfromparticipatingcountries(resultsfromquestionnaire) Presentationandplenarydiscussion Presenter:AbebaTaddese,ResultsforDevelopment/JLN 1:15–2:30PM Lunchbreak 2:30–3:45 Theevidencebaseonmechanismstoextendhealthcovertothe 5minpercountry, poorestindevelopingcountries 20mindiscussion Presenter:ValéryRidde,MontrealUniversity Presentationofcasestudies(HEFCambodia,RSBYIndia,Vietnam, Ghana) Presentationsandpaneldiscussions Presenters:Por,Seshadri,Tien,Gingong 3:45–4:15PM Coffeebreak 4:15–5:30PM TheRAMEDinMorocco:experienceandlessonslearntfromthepilot rd 17|P a g e 5:30–6:00PM 6:00–6:15PM 6:15–6:35PM 6:35–6:55PM 6:55–7:15PM 7:15–7:30PM 7:30PM 7:00/7:30/8:30AM 4:30–5:00PM phase Presentation(RegionalHealthDirectorofTadlaAzilal),followedby panelmoderateddiscussions(multipleactorsofTadlaAzilalpilot region) Moderator:Dr.Ennaciri,MoroccanMinistryofHealth Organizationandplanningoffieldvisits(Day2) Officialopeningoftheworkshop–Welcomeofparticipants Summary/conclusionsofthefirstday: Differentpoliticaloptionstoexpanduniversalhealthcovertothe poorest x Reminderonnotionofequityinhealth,healthcoverageandhealth inequalities+Stakesofuniversalhealthcoverage x Typologyofdifferentmechanismsimplementedtoovercome inequalitiesandimproveaccessforthepoorest x Strengthsandweaknessesofeachmechanism x Principallessonsfromcasestudies Presenters:Makinen(ResultsforDevelopment) UniversalHealthCoverageStrategyinMoroccoandstakesofnational expansionforRAMEDandotherinterventions AddressoftheMinisterofHealthofMorocco AddressfromtheEUambassadortoMorocco ConclusionsandclosingwordsfromtheCoPandtheMinisterofHealth ofMorocco CocktaildinnerofferedbytheFAHSCoP DAY2–Tuesday25thSeptember DepartureforfieldvisitsintheTensiftAlhaouzregionofMarrakesh x Visitsofhealthstructures(communityhealthcenterswith maternityfacilitiesandprovincehospital)intheprovincesElKalaa andEssaouira,andtheprefectureofMarrakesh x Visittotheregionalhospital,universityhospitalcenter,and/orthe RAMEDregionalobservatory x Eachgroupwillbeaccompaniedbyaresourcepersonfrom Morocco,anexpertandaninterpreter x Lunchbreakinthefield Returntohotel,informalmeetingbycountry–observations,ideas, lessonslearnt 8:30–9:15AM 9:15–10:45AM 10:45–11:15AM Day3–Wednesday26September HighlightsDay1et2 ObjectivesDay3 Evaluation(1stphase) Discussionsaroundthemainfindings/observations/impressions/key challengesonthefieldvisit. Groupworkincountrypairs,Groupingbylanguage Coffeebreak 18|P a g e 11:15AM–12:45PM 12:45–2:00PM 2:00–2:15PM 2:15–2:30PM 3:30–4:15PM 4:15–4:45PM 4:45–5:30PM 7:30PM IdentifyingthepoorestͲapproachesandchallenges InterͲsectoralpaneldiscussion Discussioninplenary Moderator:ThiMinhPhuongNgo/UNICEFͲWCARO Lunchbreak WorldTour–Assessmentofthepassports Howtomonitorequity–methodsandcasestudyfromSenegal (practicalapplicationtoresultbasedfinancinginterventions) Presentationanddiscussioninplenarysession Presenter:AlexErgo Groupworkbydelegation x Keylessons x Mainchallenges x Actionplan CoffeeBreak Groupwork(continued) DepartureforGaladinner(offeredbytheMoroccanMinistryof Health) Day4–Thursday27September 8:30–9:15AM RecapDay3 ObjectivesDay4 Evaluation(2ndphase) 9:15–10:15AM RoundtablewithMembersofParliament:UHCandequityfroma politicalperspective Moderator:MartyMakinen,ResultsforDevelopment 10:15–10:45AM Coffeebreak 10:45–11:45AM Providingeffectivecoverageofthepoorest:linksbetweendifferent mechanismstoreachthepoorestandnationalstrategiestofinance healthcare/socialprotection/developmentandgrowth PresentationandinterͲsectorialpaneldiscussions Presenter/moderator:RikuElovainio,WHO 11:45AM–12:45PM Finalcountryactionplanning Groupworkbydelegation 12:45–2:00PM Lunchbreak 2:00–3:30PM Expectationsreached?«Feedback»fromdifferentdelegations– lessonslearnt,actionplans «Talkshow»format+Evaluation3rdphase Moderator:BrunoMeessen,IMT 3:30–4:15PM Closingceremony x SynthesisofthemainrecommendationfortheRAMED implementation,researchtracksandwayforward x ClosingspeechCoP/JLN/MOH End 19|P a g e Annex3ǦFinalWorkshopParticipantList COUNTRY TITLE/ROLE NAME Benin DeputySecretaryGeneraloftheMinistryofHealth JustinAdanmavokinSossou Benin FocalPointforRégimed'AssuranceMaladieUniverselle(RAMU) HuguesTchibozo Benin CoordinatorofPRPSS AlphonseAkpamoli Benin HospitalDirectorforBassilaZone CyrGoudalo Benin DirectorofAIMSParakou IsmailouYacoubou Ghana Director,Adm.&GeneralCounsel,NationalHealthInsurance Authority NathanielOtoo Ghana AgDirector,Operations,NationalHealthInsuranceAuthority AnthonyGingong Ghana Director,CentralRegionalHospital,CapeCoast DanielAsare Ghana MemberofParliament&DeputyRankingMember,Parliamentary CommitteeonHealth MatthewOpokuͲPrempeh Ghana NHISFocalPerson,PlanningPolicyMonitoring&EvaluationDivision, MinistryofHealth RahiluHaruna Ghana Manager,DistrictMutualHealthInsuranceScheme,WestGonja JohnKippoKara Kenya ChiefEconomist,MinistryofMedicalServices ElkanaOnguti Kenya MalindiBranchManager,NHIF OmarMwatabu 20|P a g e Kenya SeniorProgrammeOfficer,NHIF JulietMaara Mali MinisterofHumanitarianAction,Solidarity,andtheElderly MamadouSidibé Mali NationalDirector,SocialProtectionandEconomicSolidarity AnkoundioLucTogo Mali GeneralDirector,ANAM FadimataMaiga Mali MemberoftheHighCouncilofLocalGovernments MamadouTraoré Mali TechnicalAdvisortotheMinistryofHumanitarianAction,Solidarity, andtheElderly AlmouctarHaidara Mali ChiefofHospitalSocialServices,Mali SeydouTraoré Morocco DirectorofHospitalServicesandAmbulatoryCare,MinistryofHealth AbdelaliBelghitiAlaoui Morocco GeneralDirector,ANAM ChakibTazi Morocco DivisionChiefforHospitalServices,MinistryofHealth AhmedBoudak Morocco DirectorforRegionalHealthServicesforTadlaAzilaregion,Ministryof MalmouzNourredine Health Morocco DirectorforRegionalHealthServicesforMarrakechTansiftAlHaouz, MinistryofHealth AchibetMustapha Morocco Deputy,MinistryofHealth BrahimiMostafa Morocco Deputy,MinistryofHealth FatimaMazziGouaima Morocco DivisionChiefforCommunication,MinistryofHealth AbdelghaniDrhimeur 21|P a g e Morocco MinistryofHealth MalikaMazine Morocco Official,MinistryofHealth LafkiriHatim Morocco ResearchDirector,MinistryofHealth HichamMouhdi Morocco SecretaryGeneral,MinistryofHealth ElOuardZakaria Morocco MinistryofHealth KhoudariRachid Morocco Manager,MinistryofHealth ZekkaouiMohammed Morocco DivisionChief,Auditing,ANAM AbdellatifMoustatraf Morocco Doctor HamouiyiMohammed Morocco PFEquitéetsanté,WorldHealthOrganization(WHO) MmeJabalS. Morocco Programdirector,EuropeanUnion(EU) ElFarjaniHikmat Morocco Representative,UnitedNationsPopulationFund(UNFPA) LardiMohammed Morocco Expert,BAD JaaforLeila Morocco Healthspecialist,UNICEF AhmedLaabid Nigeria GeneralManager(Tech.Operations),NHIS HopeUweja Nigeria DeputyGeneralManager/NHISLagosZonalCoordinator,NHIS Victor.C.Amadi Nigeria FamilyHealthDept.,FedMinistryofHealth Dr.D.B.Okara Nigeria HouseCommitteeonHealth Mr.NasiruGarbaShehu 22|P a g e Nigeria Manager,TechnicalOperationsDepartment,NHIS Mr.AgboolaOluwasunkanmi Senegal Director,CabinetoftheMinistryofHealth MameAbdoulayeGueye Senegal Coordinator,SupportCellforUniversalHealthCoverage OusseynouDiop Senegal Doctor,DistrictchiefofBambey JacquesDiaméNdour Senegal Sociologist,CAFSP RokhayaBadianeMBAYE Senegal Deputy,PresidentoftheHealthCommissionoftheNationalAssembly AlphaBalde Senegal ChiefoftheUnitforHealthInsurance,SupportCellforUniversal HealthCoverage SérigneDIOUF Senegal TechnicalAssistant,NationalProjectPAMAS2 BabacarLô Côted'Ivoire Healthspecialist,UNICEFCôted'Ivoire AbdoulayeKonaté Côted'Ivoire DirectorofForecasting,Planning,andStrategy,MinistryofHealth MamadouSamba Ethiopia RegionalDirector,USAID/HealthSectorFinancingReformProject AntenehGenet Organizing Committee MinistryofHealth,Morocco EnnaciriM. Organizing Committee MinistryofHealth,Morocco ZerhouniMohammedWadie Organizing Committee MinistryofHealth,Morocco NadaBouarif Organizing FAHSCoP,SeniorFacilitator AllisonKelley 23|P a g e Committee Organizing Committee FAHSCoP,Facilitator IsidoreSieulenou Organizing Committee FAHSCoP,Facilitator YambaKafando Organizing Committee UNICEF/WCARO JerômePfaffmann Organizing Committee UNICEF/WCARO JeanServais Organizing Committee CAFSP FahdiDkhimi Organizing Committee ResultsforDevelopment(R4D),USA MarilynHeymann Organizing Committee ResultsforDevelopment(R4D),USA AbebaTaddese Expert Professor,UniversityofMontreal,Canada ValeryRidde Expert MCHIP/BroadBranchAssociates(BBA),USA AlexErgo Expert EconomistandManagingDirectoratResultsforDevelopment(R4D), USA MartyMakinen Expert ProgramDirector,ResultsforDevelopment(R4D),USA AmandaFolsom 24|P a g e Expert OMS,Geneva,Switzerland RikuElvainio Expert HeadofHealthSystemDevelopmentSupportUnit,NationalInstitute ofPublicHealth,Cambodia IrPor Expert DepartmentofHealthInsurance,MinistryofHealth,Vietnam TranVanTien Expert InstituteofPublicHealth,Bangalore/Coordinator,RSBYevaluation, Gujarat,India TanyaSeshadri Expert CAFSP BrunoMeessen Expert UNICEF/WCARO MariameSylla Expert UNICEF/WCARO/SocialPolicy ThiMinhPhuongNgo PTF/ONG DeputyDirectoratHealthDivision1ofJICA/HQ MTaroKikuchi PTF/ONG LSHTM/FemHealth,UK IsabelleLange PTF/ONG PharmAccess/SeniorProgramManager/Researcher ChristineFenenga PTF/ONG PharmAccess/ProjectManager MarthevanAndel Regional Organization Projectcoordinator,UEMOA JeanͲJacquesMongbo Regional Organization Healtheconomist,UEMOA BakaryͲSirikiKoné Regional Organization Professional,OOAS NamoudouKeita 25|P a g e Regional Organization Economist,OOAS AlbertDiao Memberof FAHSCoP ResearchAssistant,InstitutdeRechercheenSciencesdelaSanté (IRSS)/BurkinaFaso KadiatouKadio Memberof FAHSCoP ChiefAdministrativeManager/NationalHealthInsuranceCoordinator /Ghana PhillipAsenahAkanzinge Memberof FAHSCoP DeputyGeneralManager,UnionTechniquedelaMutualitéMalienne (UTM)/Mali CheicknaHamalaTouré Memberof FAHSCoP ProgrammeCoordinator,GreatLakesInitiativeonAIDS(GLIA)/ Rwanda RichardAlia Memberof FAHSCoP ResearchAssistant,CenterforResearchonSocialPolicy(CREPOS)/ Senegal MaymounaBa Memberof FAHSCoP ResearchInstructor,UniversityofBambey/Senegal PapaGalloSow Memberof FAHSCoP Healtheconomist,AEDES/Belgium MatthieuAntony Memberof FAHSCoP Healtheconomist,InstituteofTropicalMedicine/Belgium CatherineMarieKorachais Memberof FAHSCoP HealthPolicy&ResearchAdviser,SavetheChildren/UnitedKingdom LaraBrearley Rapporteur France AntoniaMills 26|P a g e Morocco Translation RhrissiYoussef Morocco Translation SifEddineBoukhef Morocco Translation MarwanZerrouk Morocco Interpreter FatimaLaaouina Morocco Interpreter SaadiA.Taleb Morocco Cameraman,producer ZahidAbdelaziz 27|P a g e Annex4ǦMarrakechDeclaration MarrakeshDeclarationonaccesstohealthcareforthepoorest–our commitment We, as participants of the workshop on “Equity in UHC: How to reach the poorest”, we as members of the communities of practice affiliated to “Harmonization for Health in Africa”, we as experts involved in health systemsinAfrica, Areconsciousofthedeepinequalitiesintermsofaccesstohealthcarein ourcountries, Are conscious of the impact of these inequalities on the health of the poorest, Areconsciousthataccesstohealthcareforthepoorestisdependenton ourhealthsystems, Areconsciousthatassistingtheindigents,theexcluded,thepoorestofthe poorisinscribedinoursharedhumandignity, AreenthusiasticaboutthegrowinginterestoftheAfricanStatesandtheir partnersintheireffortstoimprovehealthcarecoverage. We consider essential that this interest be translated as rapidly as possible into actions and concrete measures in order to benefit the poorest. Consequently, Wecommittotakingactionpersonally: By supporting the implementation of strategies to improve access to healthcareforthepoor. By building on and accompanying the mechanisms to extend universal healthcoverage. Finally, by continuing to focus all our energy on facilitating equitable accesstohealthcareinourcountries. 28|P a g e Annex5ǦWorkshopEvaluationsummary Methodology During the workshop, ‘live’ evaluations were undertaken in order to understand the participants’ views of the content and format of the workshop activities. These evaluations weredonewiththe“TurningPoint”technology,whichallowspollstobecarriedoutwiththe useofMSPowerPointand“clickers”distributedtorespondents. OnͲtheͲspot evaluations were conducted during three sessions of questions: on day 3 in the morning,onday4inthemorning,andonday4intheafternoon.Eachtime,all51clickerswere distributedamongtheparticipants.Therewerenotenoughclickerstocoveralltheworkshop participants, but clickers were distributed in priority to the delegation participants (coverage 100%).Theresponseratewas80%onaverageforeachquestion(onaveragewereceived41 responses out of 51 distributed clickers). The response rate improved with each session (on average,wereceived37responsesduringthefirstsession;40duringthesecondsession;and 46duringthelastsession). Questions focused on the usefulness of the different sessions, the working groups on action plans,andthegeneralqualityoftheworkshop. Duringthetwofirstevaluationsessions,participantsansweredthequestionsbyclickingtheir remotes, but results were not directly displayed. During the final evaluation on day 4 in the afternoon, the feedback feature of the Turning Point software was employed: participants’ resultswereimmediatelydisplayedonthescreenaftereachquestionhadbeenposed,sothat thosepresentreceivedfeedbackfromthislastevaluationonthespot. Results Usefulnessofselectedactivities Efforts were made to create a program in which the plenary sessions were stimulating, informativeanduseful.Belowareparticipantassessmentsofafewofthesesessions,aswellas thefieldtripondaytwooftheworkshop. Firstsessionofquestions: The presentation on the overview of mechanisms implemented in Africa during the first day wasconsideredusefulorveryusefulby83%oftherespondentswhile11%founditminimally useful or not useful at all. The field visit on Day 2 was very appreciated as 100% of the respondentsfounditusefulorveryuseful. 29|P a g e Secondssession: OnDay3 3,thepanel on‘identifyyingthepoorest–approoachesandcchallenges’w wasfoundu useful or very useful u by 77 7% of the re espondents. Comparativvely less inteerest was reegistered fo or the session on o methodss to monitor and meassure equity: the presen ntation on ‘‘how to mo onitor equity’w wasfoundussefulorveryusefulbyon nly53%ofthherespondeents. Thirdse ession: Participantsareshow wntobemo oreintereste edinthepoliticalissuesspresented duringtherround tablewitthmembersofParliamentonday4.Thissessionnwasfoundusefulorveeryusefulbyy89% oftherespondents. Figure2:Resultsreggardingtheu usefulnesso ofactivities A) Presentation:overviewo of mechanisms m implemente edin Africa:summ A maryofexpe eriences Day1 D B) Fiieldvisit Day2 D C) Panelon‘ide entifyingthe epoorest– approachesa andchallengges’ Day3 D 30|P a g e D) Presentation‘howtomo onitor equity:methodsandcassestudy frromSenegal’ Day3 D E) Roundtable R withmembersof Parliament Day4 D Usefuln nessofthe eworkinggroupson nactionpllans A core feature f of this t worksh hop was the e work withhin and between coun ntry delegattions. Participantswereaskedastowh hethertheyvaluedthis workandin nparticulartthetaskthattwas definedfforthem:th hecreationo ofanactionplanonequ ityinUHCfo ortheircoun ntry. Session1: Thediscu ussionbetweencountryypairsonDaay1wasfouundusefulo orveryusefu ulfor78%o ofthe responde ents. Session2: 90% of the t respond dents agreed d or stronglyy agreed wiith the stateement that the small ggroup discussio onsonthefie eldvisitswe eredynamicandstimulaating,and722%oftherespondentsffound itpertine entorveryp pertinenttobrainstormo onanactionnplanfortheeircountry. Session3: edresponde entsanswere edthatthe actionplan theyworkeedonwould dvery 50%oftheconcerne likely plaay a role in their country’s strateggies after thheir return. 33% answeered that itt was somewhaatlikely,while17%thou ughtthatitw wasnotveryylikelyorno otlikelyatall. 31|P a g e Figure3:Resultsreggardingtheu usefulnesso oftheworkin nggroupsonactionplaans A) Howusefulw H wasthediscu ussion betweencou untrypairs Day1 D B) Themorning’’sgroupworkonthe fe eedbackoftthefieldvisiitswere dynamicandstimulatingg Day3 D C) Howpertinen H ntisittobraainstorm onanactionplanforyou ur co ountry? D) Howlikelyis H itthatthisaaction planwillplayyaroleinyo our co ountry’sstra ategiesafteryour re eturn? 32|P a g e Genera alevaluatio on x x x x x 73% of the respondents r s agreed or strongly agreed with the statement that theyy had enough time e to exchange with oth her participaants inform mally about equity and UHC Days1and2 2). (D 95%foundth hatasofday3,thecon ntentandthhelevelofeexchangehaadbeenthoughtͲ provokingforrthem. 95% agreed or stronglyy agreed with w the staatement that, overall, the processs of describingtheirowncountrychallen ngescaused themtorefflectandthinkconstructtively ountry’ssitu uation. abouttheirco 98%agreedo orstronglyagreedwithtthestatemeentthatthew workshophadbeenvalu uable fo orthemoverall. 91%agreedo orstronglyaagreedwiththestatemeentthattheyyexpectedttofollowup pwith pantsfromtheworkshopafterwards. otherparticip When assked if they would join the ‘Financiial Access’ C CoP after th his workshop p, 24% answ wered they werre already members; m 12% respond ded «What’’s that?» att the end o of the worksshop: we’reno otsurewhethertheywe ereplayingalongwithouurjokeorsttilldidn’tkno owaboutit!!64% answered dtheywould djoin. Figure4:Generalevaluation A) Iamfindinge enoughtime eto exchangewitthotherparrticipants in nformallyab boutequityaandUHC (D Days1and2 2) B) So ofar(day3)),havetheccontent andlevelofe exchangebe een th houghtͲprovvokingforyo ou? 33|P a g e C) Overall,thep O processofdescribing ourownchalllengescaussedmeto re eflectandth hinkconstru uctively aboutmyow wncountry’ssituation D) Thisworksho ophasbeenvaluable fo ormeoverall E) Iexpecttofo ollowupwithother participantsffromthewo orkshop affterthemee eting F) Willyoujoin W the‘Financiial Access’CoPa A afterthiswo orkshop? 34|P a g e Limitsofthisanalysis x x x Questions were prepared upon consultation of others in the facilitating group, but normallypreparedatthelastminuteandthequalityofthequestionsvaried. Theturningpointtechnologywasnewtothefacilitatorsofthequestionnaires. TheturningpointtechnologydoesnotallowopenͲendedquestionstobeposed.Forthis reason, an anonymous postͲworkshop online survey with both open and closed questionswasdevelopedinordertogetabetterunderstandingofparticipants’overall perceptions of the workshop. The objectives were the same: to improve future community of practice workshops and better understand the capacities of the CoP in thisfield.ThethemesofthepostͲworkshopsurveyquestionsareorganizedasfollows: demographics, expectations, format of the workshop, participants, overall perception, followͲupafterleaving,andrecommendationsforimprovement.Thetimetocomplete the survey was estimated at approximately 10Ͳ20 minutes. The questionnaires were offered separately in English and French on the www.formsite.com (using an ITM account) platform that allows the results to be exported to Excel. So far only 20 responseshavebeenobtainedwhichwillbeanalyzedinthecomingweeks. 35|P a g e






© Copyright 2026