
WHAT IS THE EVIDENCE THAT WORKLOAD IS AFFECTING
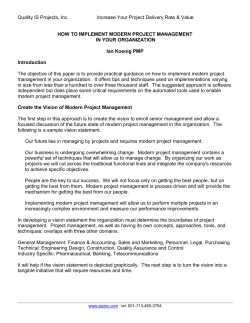
WHAT IS THE EVIDENCE THAT WORKLOAD IS AFFECTING HOSPITAL PHARMACISTS’ PERFORMANCE AND PATIENT SAFETY? Dr Sarah Willis; Dr Rebecca Elvey; Professor Karen Hassell University of Manchester May 2011 What is the evidence that workload is affecting hospital pharmacists’ performance and patient safety? TABLE OF CONTENTS Table of contents ................................................................................................................ 1 Executive summary .......................................................................................................... 2 Context .................................................................................................................................. 3 1 Introduction .............................................................................................................. 4 2 Aims and objectives ............................................................................................... 6 3 Methodology ............................................................................................................. 8 3.1 Search strategy ............................................................................................................... 8 3.2 Key words and search terms used ........................................................................... 8 4 Findings .................................................................................................................... 11 4.1 Overview ......................................................................................................................... 12 4.2 Pharmacy workload and what is measured....................................................... 12 4.3 The impact of pharmacy workload on pharmacists’ performance .......... 13 4.4 The impact of pharmacy workload on pharmacists’ well-being................ 13 4.5 The impact of pharmacy workload on patient outcomes ........................... 14 5 Discussion ................................................................................................................ 15 6 Appendix 1 ............................................................................................................... 16 7 References ............................................................................................................... 22 © CfWI | May 2011 1 EXECUTIVE SUMMARY This paper reviews and then synthesises the published evidence on workload in the hospital pharmacy setting in the UK. Evidence is reviewed in relation to three questions: 1. 2. 3. Has hospital pharmacy workload changed (increased)? Does workload influence workforce behaviours and attitudes to work? Does workload affect pharmacists’ performance? Findings suggest the following: 1. 2. 3. 2 There is limited evidence to show that workload has increased. Pharmacists’ physical and mental well-being are being affected by their workload. In particular, workload is perceived as causing job stress and job dissatisfaction. High workload is associated with an increase in medication errors. What is the evidence that workload is affecting hospital pharmacists’ performance and patient safety? CONTEXT The Centre for Workforce Intelligence (CfWI) workforce risks and opportunities project sets out the major risks and opportunities facing the health and social care workforce in 2011 and beyond. The University of Manchester is providing specialist knowledge to CfWI through an integrated approach across a range of disciplines. This is one of a series of briefing papers to provide managers and workforce planners with evidence to inform their choices when addressing short, medium, and long-term workforce challenges. The 2011 series focuses on: Labour substitution and efficiency in health care delivery: general principles and key messages Recession, recovery and the changing labour market context of the NHS Workforce risks and opportunities: working time practices in nursing and midwifery The policy context for dentistry skill mix in the NHS in the UK Identifying the risks and opportunities associated with skill mix changes and labour substitution in pharmacy What is the evidence that workload is affecting hospital pharmacists’ performance and patient safety? Managing people in networked organisations: identifying the challenges for health and social care © CfWI | May 2011 3 1 INTRODUCTION As the pharmacy profession shifts towards providing a wider range of healthcare and clinically focused services, pharmacists’ work increasingly involves activities based on their specialist medicines knowledge in addition to more traditional, technical tasks related to the supply of medicines. Evidence suggests that this shift in focus – or the reprofessionalisation2 of pharmacy – while offering pharmacists opportunities to take on more patient-oriented roles,1 may result in work intensification,3 conflicting task priorities and increased workload.4-10 Moreover, in terms of the impact of adopting new professional roles on occupational well-being,11;12 it appears that rising work pressure is associated with pharmacists feeling unvalued13 and stressed.14 One consequence of this is that pharmacists may reduce their work hours to cope with stress, or it may result in pharmacists leaving the profession altogether, with obvious consequences for labour market supply. Increasing workload or intensification of work has also been associated with poor performance, perceived or actual, (dispensing errors for example), thus compromising patient safety. The expansion in services provided by pharmacists taking place within the reprofessionalisation2 movement also coincides with a growth in the technical medicines supply aspects of pharmacy work. This growth can be seen in analysis of government data on community pharmacists’ dispensing activities demonstrating a 54 per cent rise in dispensing volume in England and Wales between 1998/9 and 2007.15;16 While no equivalent national data are available for hospital pharmacy work, the complexity of hospital patients’ medication needs (arising from high levels of co-morbidity and from the toxicity of some drug regimens) means it is likely that activities directly or indirectly involving the supply of medicines will constitute a major feature of hospital pharmacists’ work.17 Certainly, growth in the number of medicines used per hospital patient has been cited as contributing to rising workload among hospital pharmacists,18 and this situation is undoubtedly exacerbated by high vacancy rates in the sector, with inadequate staffing reported as creating pressure among hospital pharmacists to work intensively.14 It appears, then, that both the nature of pharmacy work and pharmacists’ workload have changed. It also appears that changes in workload have had a negative impact on pharmacists’ occupational well-being,11;12 and may explain why many pharmacists describe the daily demands of their work as ‘constantly 4 What is the evidence that workload is affecting hospital pharmacists’ performance and patient safety? stressful’.19;20 There are also concerns that pharmacists’ workload may be having a negative impact on the quality of care being delivered to patients. Given these concerns, and in light of growing opinion within the pharmacy profession that workload and workload pressures are rising, it is important to determine whether there is any research evidence that workload is in fact increasing, and what evidence there is that workload is affecting the performance or labour market activity of hospital pharmacists, or is affecting patient safety. In this review, we therefore set about systematically evaluating research on pharmacy workload in the secondary healthcare context and its impact on both patient and employee outcomes. In doing so, we review evidence of workload where it is operationalised at job level, which refers to the general demands of a job, the amount of work done in a day, and the level of concentration needed to get the work done at task level, which is more about the specific resources and demands required to complete a specific task.21 © CfWI | May 2011 5 2 AIMS AND OBJECTIVES The aim of this review is to synthesise the published evidence on workload in the hospital pharmacy setting in the UK. The effects of UK community pharmacists’ workload have been comprehensively documented in a recent review by one of the authors (KH) in a paper demonstrating how much community pharmacists’ workload has grown since the introduction of new contractual frameworks that reimburse pharmacists for performing both new reprofessionalised roles as well as more traditional technical supply activities.16 As well as providing quantitative data related to pharmacists’ work activities, Hassell et al’s paper also considers the extent to which research has established links between changes in community pharmacists’ workload and a number of outcomes, including prescribing errors, workforce behaviours, and effects on pharmacists’ wellbeing.16 It appears that while there is an emerging evidence base related to growth in community pharmacists’ workload, and limited, small-scale material on workload and its impact on pharmacists themselves, there is a lack of robust studies establishing links between workload and patient safety outcomes that take into account confounding factors such as skill mix or the organisational context in which pharmacists work. While it has, therefore, been recognised that much of the evidence in community pharmacy is derived from studies that have limited representativeness, the next step in determining the extent to which pharmacists’ workload is affecting pharmacists’ performance and patient safety is to review workload in the hospital pharmacy setting in the UK. In conducting this review we set the following objectives: 1. 2. 3. to investigate evidence that hospital pharmacy workload has changed (increased) to explore evidence that workload is linked to hospital pharmacists’ workforce behaviours and attitudes to work (including their labour market decisions and/or occupational well-being) to explore evidence related to links between hospital pharmacists’ workload and pharmacists’ performance (including the impact of workload on patient outcomes and the implications for patient safety). A number of outcome measures or effects of workload have been considered in conducting this review, including job satisfaction, job stress, labour market withdrawal and reduction in activity. We have also considered pharmacist performance outcomes, and here we concentrate on performance related to safe and effective medicines use that 6 What is the evidence that workload is affecting hospital pharmacists’ performance and patient safety? may be studied in terms of medication errors (and operationalised in studies of errors in prescribing, dispensing, administering and/or monitoring medicines). © CfWI | May 2011 7 3 METHODOLOGY In conducting this review we have not followed the methodology for undertaking a systematic review in the conventional sense; rather, our approach has been to provide a synthesis of findings from relevant research literatures. We have attempted to minimise bias by using robust methods in our search strategies, and by providing detail of inclusion and exclusion criteria so that the review could easily be replicated and updated in future if necessary. 3.1 Search strategy A librarian experienced in conducting reviews of health services research conducted the literature search, with the following electronic databases searched from 2000 onwards: The Cumulative Index to Nursing and Allied Health Literature (CINAHL) International Pharmaceutical Abstracts (IPA) Medline Embase British Nursing Index (BNI) Scopus. 3.2 Key words and search terms used Given the difficulty in defining workload search terms reported by Hassell et al16 we used diverse terms to identify relevant material. Moreover, in order to complement the work undertaken on community pharmacists’ workload we used many of the same search terms, but adapted them (where relevant) to the hospital setting. Search terms used in conducting this review relate to four categories: contextual or hospital-setting terms terms referring to workload terms describing the pharmacy workforce terms designed to capture literature reporting outcomes of workload See Table 1 for further details. A UK filter was applied to remove studies conducted outside the UK. 8 What is the evidence that workload is affecting hospital pharmacists’ performance and patient safety? Table 1: Search terms used in electronic databases Category of search term Terms used Contextual terms Hospital pharmacy*.tw (hospital adj 6 (pharmacy or pharmacies or pharmacist or pharmacists)) Exp Pharmacy Service, Hospital/ Exp Pharmacies/st,ut Workload terms Exp Workload/ *Task Performance and Analysis/ Workflow*/tw Workload*.tw “workload measure*”.tw “work measure*”.tw “work intensification”.tw “work condition*”.tw “work pattern*”.tw “work outcome*”.tw “work activit*”.tw “work assignment*”.tw “dispensing load*”.tw “dispensing volume*”.tw “Staff* level*”.tw Productiv*.tw Workforce terms Exp Pharmacists/ut Pharmacy staff Outcomes of workload terms Error Mistakes Adverse events Patient safety (job) satisfaction well-being pressure Following the approach used in Hassell et al’s review of community pharmacy,16 this review was not restricted to any particular study design. We wanted to include a range of study types, using appropriateness as a condition for inclusion. Instead of using a hierarchy of evidence where randomised controlled trials are considered the ‘gold standard’ against which other research study types are compared, in this review the relative value of research evidence was assessed during the process of evidence synthesis. Quality criteria were applied to restrict evidence included in the review to peer-reviewed, empirical primary research. © CfWI | May 2011 9 Where a conference abstract had also been published as a full, peer-reviewed paper, we only included the full paper, as this was deemed to be of higher quality. Inclusion criteria were applied to the results of the search strategies so that studies of workload in the hospital setting per se were included, but studies that considered one of the outcome measures without explicitly investigating how it related to workload were excluded. Table 2 provides further detail of criteria applied in conducting the review. Table 2: Inclusion and exclusion criteria Category Include in review if ALL met by Exclude from review if ANY a study met by a study Setting Hospital pharmacy Community pharmacy; health centre Location UK Outside UK Design/study type Any empirical study Non-empirical study; methodological paper Publication type Peer-reviewed journal papers; peer-reviewed conference abstracts Letters; non-peer-reviewed articles/reports Publication date 2000–2011 Pre 2000 Focus of study Workload and/or its impact Studies addressing outcomes without exploring how related to workload The inclusion/exclusion criteria were applied during two stages of the review process. Firstly, they were applied to the title and abstract of a paper, with those papers not meeting ALL the criteria excluded. Where inclusion criteria were met, or where it could not be determined from reading the title and abstract whether a study met ALL the criteria, full papers were then retrieved. On reading these, criteria were applied again. For rigour, two of the authors (SW and RE) reviewed titles and abstracts and independently applied inclusion and exclusion criteria. Results of this process were compared. At this stage, both authors included and excluded the same studies. Using a data extraction tool, key features of all the studies meeting the inclusion criteria for this review were recorded (see Table 3 in the Appendix). 10 What is the evidence that workload is affecting hospital pharmacists’ performance and patient safety? 4 FINDINGS The initial search strategy identified 290 papers once duplicates had been removed. After the inclusion/exclusion criteria had been applied to titles and abstracts, 231 citations were excluded, mostly because they were either not reporting empirical work, or related to studies conducted in settings other than hospitals, or outside the UK. Copies of 59 full papers were obtained for full consideration, after which a further 48 were excluded.1 A hand search of the bibliography from a review paper on the incidence, type and causes of dispensing errors was also undertaken, together with a search of key authors. This resulted in a further five papers being included in the review.22-26 Figure 1 summarises the results of this review process. Figure 1; Flow chart of review process 1 Key features of the papers included in this review can be found in Table 3 in the Appendix © CfWI | May 2011 11 4.1 Overview Of the 16 papers we reviewed, it is notable that few papers had workload and its impact as their primary focus. Moreover, although nine of the papers used objective, quantifiable measures of workload – comparing, for example, rates of items dispensed with dispensary error rates – two of these papers relied on subjective, qualitative perceptions of workload derived from a small number of interviews27, or contained limited detail about the study and its findings.28 However, some studies were larger in scale. Of particular note is a study of measuring dispensing workload (as items/person/hour) at 17 non-specialist hospital pharmacy dispensaries in Wales.29 4.2 Pharmacy workload and what is measured Workload was defined and measured differently across the studies reviewed here. That makes it difficult to compare results across studies and/or to determine the extent to which hospital pharmacists’ workload may have increased. Several studies included in our review quantified workload in relation to dispensing activity – a postal survey of oncology dispensing workload across Britain measured the number of cytotoxic IV chemotherapy doses prepared each month, and found that oncology dispensing workloads had increased over the five years to 2003 by an average of 178 per cent (although this measure of increased workload was self-reported by pharmacists taking part in the study, and so should be treated with some caution).30 A larger-scale study collating data from hospital dispensaries across Wales found that on average 9.9 items were dispensed per person per hour, but this study aimed only to provide a benchmark of workload and did not measure change in workload over time. 29 Two studies considered workload in relation to service reconfigurations, and report less than positive findings. In an evaluation of whether introducing a wardbased technician reduces pharmacists’ workload, the number of non-stock item requests made to pharmacists was used to measure workload.31 Since requests were found to increase after introducing the new service by 14 per cent – and hence pharmacists’ workload was viewed as having increased by the same amount – findings suggest that skill-mix initiatives aimed at redesigning ward supply services in order to make better use of pharmacists’ clinical knowledge may result in work intensification for pharmacists. Another study, this time of a pharmaceutical care intervention promoting self-medication on a paediatric ward, found that there was no net gain in workload after redesigning pharmacy 12 What is the evidence that workload is affecting hospital pharmacists’ performance and patient safety? services, as workload shifted from the dispensary to the ward but was not reduced overall.32 4.3 The impact of pharmacy workload on pharmacists’ performance Six studies evaluated in this review investigated the impact of workload on performance, in relation to medication errors. Studies tended to use qualitative methods (interviews) to provide insight into the causes of error in order to throw light on quantitative data on medication errors. In terms of pharmacists making dispensing errors, there is some evidence to suggest that interruptions, distractions, lack of staff, inadequate skill mix, being busy, and time restraints contribute to errors.23;24;33-35 In this context, it is important to note that causes of errors in the literature tend to be recognised as multi-factorial, with high workload mentioned most frequently, although low workload was also linked to error by one study.35 High workload has also been linked to the likelihood of a pharmacist identifying an error when checking patient drug charts: where workload was high, fewer errors were identified.36 4.4 The impact of pharmacy workload on pharmacists’ well-being Studies of workload that described workers’ subjective experiences of work demands (n=5) in the main employed qualitative methods to explore the nature and impact of pharmacy work and workload on pharmacists.24;27;28 We found that unmanageable work demands (caused by interruptions and being pressurised to hurry, as well as understaffing in the dispensary) were associated with a number of pharmacists’ well-being outcomes, most typically physical and mental stress, that on one occasion was also linked to job dissatisfaction.28 Similar findings of the impact of workload on pharmacists – that interruptions, staff shortages and workload make an important contribution to pharmacists’ job stress – was also reported by a quantitative study of work stressors.37 We also found quantitative evidence that, as a consequence of high workload, pharmacists were increasingly likely to experience repetitive strain injury problems.30 © CfWI | May 2011 13 4.5 The impact of pharmacy workload on patient outcomes A considerable amount of research on dispensing errors in hospital pharmacy has been conducted, and this tends to focus on quantifying dispensing errors38 or on the type of error made (in terms of wrong drug, wrong strength of drug, etc.) or on who identified the error39. There is, in addition, a growing body of evidence addressing the causes of errors, and as we reported above (in relation to pharmacist performance outcomes) workload is often a key variable in explaining dispensing errors. Alongside affecting pharmacists’ performance, in this review we identified nine papers linking errors to patient outcomes, although in many instances (5/9) this impact on patients was implied by findings in terms of errors being harmful to patients in general rather than in terms of how serious an error was for patients. There were, however, a number of papers that did classify errors in terms of the severity of risk they presented to patients.25;26;40 14 What is the evidence that workload is affecting hospital pharmacists’ performance and patient safety? 5 DISCUSSION From this review, it is clear that measuring workload in hospital pharmacy and its outcomes is often undertaken in the context of researching quality and safety in medicines use. This should be no surprise, given the medicines focus of the pharmacy profession. However, investigating workload in relation to error rates may not reflect the complexity or difficulty of pharmacists’ work or what is involved in completing a task (interruptions, enquiries, etc.) at a job-level rather than at a task-level of analysis. Studies that focus on relationships between multiple variables are an obvious omission from the literature. Such studies would make it possible to determine whether errors attributed to workload are more or less likely to cause harm to patients (that is, are more serious) than incidents caused by other factors. There is also a lack of research providing robust evidence (that does not derive from qualitative studies of perceptions) in investigating the impact of workload on pharmacists’ well-being. Questions of whether pharmacy workload in the secondary healthcare context is rising the impact of pharmacy workload on both patient and employee outcomes cannot, therefore, be addressed by the existing research literature. Further research is needed to explore these important topics in more depth. © CfWI | May 2011 15 6 APPENDIX 1 Table 3: Key features of papers included in this review Study Method and subjects Study aim Outcome measure(s) Main findings 22 Anto et al: Int J Pharm Pract 2010;18:122-4 Qualitative: 10 interviews with staff involved in labelling errors. To evaluate causes of dispensing-label errors. Causes of error. Under-staffing during lunch identified as a source of workload pressure leading to label-generation errors. A busy environment and distractions also contributed to errors. 35 Armitage et al: J Eval Clin Pract 2010;16:11891197 Quantitative and qualitative: Retrospective analysis of a sample of error reports submitted 1999-2003 at one hospital. Follow-up interviews with doctors, nurses and pharmacists (n=40). To improve reporting of and learning from drug errors; to investigate factors contributing to errors. Error type, location, contributory factors. Interruptions and stress had the lowest frequencies of contributory factors identified in quantitative analysis (1.31% and 1.72%) – workload not reported as a factor. Qualitative data demonstrated that error causes were viewed as multi-factorial, with high workload mentioned most frequently, although low workload was also seen as precipitating error. Error prevention believed to rest on reforming working practices rather than about increasing resources or adjusting volume of work. 41 Quantitative analysis of national aseptic error reporting scheme (NAERS) error data. Self-reported errors & (potential) severity of errors Jan-Dec 2007 from 43 UK hospitals. To identify factors Details of errors contributing to (type, severity etc); pharmacy compounding contributory factors. errors. Bateman & Donyai: Qual Saf Health Care 2010;19(5):1-6 16 The highest rated factor was 'individual staff error'; (78%) - second highest was 'distraction/interruption’ 4.3%);'workload above planned capacity' and 'staffing level below establishment' 4th and 5th (3.2 and 3.1%). Reduced staffing & workload above capacity especially contributed to errors with parenteral nutrition products. What is the evidence that workload is affecting hospital pharmacists’ performance and patient safety? Study Method and subjects Study aim Outcome measure(s) Main findings 23 Beso et al: Pharm World Sci 2005;27:182-190 Quantitative and qualitative: Analysis of recorded dispensing errors identified at the final check stage over two weeks (weekdays only) in June and a further 7 weeks during July-September 2002; dispensing errors reported outside the pharmacy department examined for June fortnight & all of 2002. Interviews with staff on perceived causes of errors (n=27). To determine the frequency and types of dispensing errors; to explore perceived causes of errors. % dispensed items for which one or more errors occurred at the final check stage; % errors reported outside pharmacy department; perceived errorcausing conditions. One or more dispensing errors identified at final check stage in 2.1% of 4849 dispensed items, outside the pharmacy error reporting accounted for 0.02% of dispensed items. Error producing conditions most frequently identified as related to workload (being busy, time restraints, being shortstaffed). Distractions, interruptions, working conditions, dispensary design (environmental factors) also commonly cited, as were stressors (impacting on morale / physical health / performance). Difficulty in managing the workload resulting from enquiries was considered a contributory factor. 31 Quantitative: Data on errors and workload collected for two weeks before and two weeks after introduction of new technician service to five wards (two acute admissions and three elderly) with perceived high workload at Bristol Royal Infirmary in 2001. To determine if having a ward-based technician service reduces medication administration errors and/or pharmacist workload. Incidence of unavailable medication administration errors (U-MAEs); frequency of calls to pharmacy; volume of weekend medicine supply; workload of pharmacist measured via number of nonstock item requests. U-MAEs and calls to pharmacy reduced, & overall item requests during weekend reduced by introduction of ward-based technician service; pharmacist workload (requests for non-stock supply) increased for acute admissions-related work but declined in relation to care-of-the-elderly-related work. Conroy et al: Int J Pharm Pract 2002;10:171-5 © CfWI | Month Year DRAFT # CONFIDENTIAL – footer 17 Study Method and subjects Study aim Outcome measure(s) Main findings 27 Eden et al: Int J Pharm Pract 2009;17:181-7 Qualitative: Interviews with recently qualified pharmacists (n=12; only n=3 working in hospital pharmacy). To explore why pharmacists leave or intend to leave profession. Perceptions of work and workload, job satisfaction, stress. Dissatisfaction with workload pressures influences workforce behaviours (decisions to leave the workforce). 28 Ferguson et al: Int J Pharm Pract 2009;19:B2 Qualitative: Interviews with hospital pharmacists (n=15) exploring aspects of workload associated with job dissatisfaction (n=26 pharmacists interviewed for study). To explore aspects of pharmacists' job dissatisfaction. Perceptions of workload and work pressure; job dissatisfaction. All pharmacists expressed dissatisfaction with workload; understaffing, work intensification, working conditions and stress / pressure contribute to job dissatisfaction. 29 Hiom et al: J Clin Pharm & Therapeutics 2006;31:357-62 Quantitative: Measure of dispensing workload (items/person/hour) collected for 3 days from 17 non-specialist hospital pharmacy dispensaries in Wales in2002. To develop / benchmark Dispensing activity dispensing rates. items/person/hour. Influence of hospital size, skill mix, telephone interruptions on dispensary activity. Average dispensary rate was 9.9 items/person/hour. Dispensary activity was not significantly correlated to hospital size; dispensing rates were higher with increased % pharmacists & technicians, lower with increased % ATOs. 25 James et al: Int J Pharm Pract 2008(a);16:17588 Quantitative: Retrospective analysis of unprevented dispensing incident data reported to UKDEAS (UK Dispensing Error Analysis Scheme) Jan 2003-Dec 2004 for all hospitals in Wales (n=20) . To monitor unprevented dispensing incidents by type & drugs involved; to identify contributory factors. Frequency and type of dispensing incidents; drugs and dosage forms associated with incidents; patient outcomes; causes. Overall unprevented dispensing incident rate was 16 per 10,000 items dispensed; contributory factors were reported for 484 (48%) of these, with high workload cited in 141 incidents, low staffing in 74 and being a lone worker in 10. Patient outcomes of errors are reported (although not linked to workload). 24 Qualitative and quantitative: interviews, a focus group, observations To evaluate the causes of prevented dispensing incidents for drugs at Frequencies of prevented dispensing incidents 24 incidents were reported at 10 hospitals. High workload reported in 14 incidents, and inadequate staffing in 5 incidents. Physical and mental stress James et al: Int J Pharm Pract 2008(b);16:239- 18 What is the evidence that workload is affecting hospital pharmacists’ performance and patient safety? Study Method and subjects Study aim Outcome measure(s) Main findings 49 and literature review used to design tool for collecting data on prevented dispensing incidents from hospitals in Wales (n=16) for four months in 2006. Dispensary workflow data also collected. high risk of dispensing incidents. and their causes. associated with high workload, interruptions and inadequate staffing were also reported as errorcontributing factors or conditions. 40 James et al: Int J Pharm Pract 2011;19:36-50 Quantitative: Comparison between unprevented and prevented dispensing errors at 5 Welsh hospitals over 3 months in 2005. To compare between the rate, type and causes of prevented / unprevented dispensing incidents. Frequencies of and differences between prevented / unprevented dispensing incidents; causes of errors compared. 35 unprevented (0.016% of items dispensed) and 291 prevented dispensing incidents (0.13%) were reported. Contributory factors were reported for 171 of the prevented and 25 of the unprevented incidents (59% and 71% respectively). High workload was cited in 21% of prevented and 29% of unprevented incidents, low staffing, interruptions, urgent deadlines and being a lone worker were also reported. There was no significant different in the proportion of unprevented and prevented dispensing incidents attributed to each contributory factor. Low workload was cited as a factor for one prevented incident. No patient experienced harm after taking drug associated with unprevented dispensing incidents. 37 Quantitative: Postal survey To determine levels of of pharmacists in job satisfaction and Northern Ireland work stressors. (766/1965, 39% responses). Level of job satisfaction; levels of work stress associated with 5 domains (managing workload was 1 Interruptions, workload, staff shortages perceived as main sources of work stress. McCann et al: Pharm World Sci 2009;31:188-94 © CfWI | Month Year DRAFT # CONFIDENTIAL – footer 19 Study Method and subjects Study aim Outcome measure(s) Main findings domain). 26 Roberts et al: Int J Pharm Pract 2002;10:R6 Quantitative: Analysis of dispensing error reports submitted by chief pharmacists from 89 hospitals in England, Wales and Scotland 19912001. To determine type of prescription & type of error, drugs / staff involved; causes and outcomes of errors. Types of dispensing errors; causes and outcomes of errors. 10 drugs are most commonly involved in dispensing errors. Of 7158 error reports received, contributory factors were reported for 5026, high workload/low staffing was reported for 1,156 (26%). Moderately detrimental effects were recorded for 291, serious detrimental effects for 26 and fatality for 1. 30 Summerhayes: J Oncol Pharm Practice;2003;9:1 23-8 Quantitative: Postal survey of pharmacist members of the British Oncology Pharmacy Association and nursing colleagues (54/104, 51.9% responses). To determine extent of change in IV chemotherapy workload; availability of pharmacy and nursing staff to carry out this work. Number of cytotoxic doses prepared per month; number of patients for whom chemotherapy is prepared per week; workload trends; staff stress; treatment waiting times. Mean number of cytotoxic doses prepared per month=896, mean patients having prepared chemotherapy drugs for each week=92.7; 43/46 pharmacists reported an increase in workload over five years of an average of 178%. Consequences of rising chemotherapy demand included inability to carry out other aseptic dispensing work; increased staff repetitive strain injury problems; strained working relationships between pharmacy and the rest of the oncology team. 32 Tomlin & Saunders: Paed Nurs;2001; 13(4):25-9 Quantitative: Evaluation of pre- and postpharmaceutical care intervention promoting self-medication on a paediatric ward. To determine whether intervention reduced workload and errors. Dispensary workload; dispensing time; errors; cost; turnaround time; patient /carer satisfaction. Workload shifted from dispensary to ward but was not reduced; turnaround time drug errors, medication costs were reduced. High levels of satisfaction with the new service reported by carers/patient /nurses. 36 Quantitative: Analysis of prescribing errors recorded by 39 pharmacists on ward visits on 38 randomly selected To investigate the prevalence of prescribing errors and factors influencing identification by Proportion of new medication orders with a prescribing error; predictors for error detection Drug chart checking workload was the strongest predictor of prescribing error identification. Errors were 16% less likely to be identified on Fridays than any other day of the week. Tully & Buchan: Pharm World Sci 2009;31:682-8 20 What is the evidence that workload is affecting hospital pharmacists’ performance and patient safety? Study 37 McCann et al: Pharm World Sci 2009;31:188-94 © CfWI | Month Year DRAFT # CONFIDENTIAL – footer Method and subjects Study aim Outcome measure(s) days between Mar 2003 and Aug 2005 at a teaching hospital in England. pharmacists. included checking workload (measured as the number of patients' drug charts examined per day) Quantitative: Postal survey To determine levels of of pharmacists in job satisfaction and Northern Ireland work stressors. (766/1965, 39% responses). Level of job satisfaction; levels of work stress associated with 5 domains (managing workload was 1 domain). Main findings Interruptions, workload, staff shortages perceived as main sources of work stress. 21 7 REFERENCES 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. 22 Edmunds J, Calnan MW. The reprofessionalisation of community pharmacy? An exploration of attitudes to extended roles for community pharmacists amongst pharmacists and General Practitioners in the United Kingdom. Soc Sci Med 2001 Oct;53(7):943-55. Birenbaum A. Reprofessionalisation in pharmacy. Soc Sci Med 1982;16(8):871-8. Konzelmann SJ, Wilkinson F, Mankelow R. Work Intensification and Employment Insecurity in Professional Work. Centre for Business Research, University of Cambridge; 2007. Report No.: Working Paper No. 345. Bond C, Blenkinsopp A, Inch J, Celino G, Gray N. The effect of the new pharmacy contract on the community pharmacy workforce. London: Pharmacy Practice Research Trust; 2008. Jukes AJ. Heavy workload is taking its toll (letter). Pharm J 2008;280(7493):305. Koziol M. Excessive workload (letter). Pharm J 2008;280(7497):436. Watson CM. What is an acceptable workload? [letter]. Pharm J 2008;280(7491):244. Gilpin LK. Improve pharmacists' working conditions (letter). Pharm J 2008;280(7497):439. Bradley F, Wagner AC, Elvey R, Noyce PR, Ashcroft DM. Determinants of the uptake of medicines use reviews (MURs) by community pharmacies in England: A multi-method study. Health Policy 2008;88(2-3):258-68. Gidman WK, Hassell K, Day J, Payne K. The impact of increasing workloads and role expansion on female community pharmacists in the United Kingdom. Research in Social and Administrative Pharmacy 2007 Sep;3:285302. Van Horn JE, Taris TW, Schaufeli WB, Schreurs PJG. The structure of occupational well-being: A study among Dutch teachers. Journal of Occupational and Organizational Psychology 2004;77(3):365. Warr PB. The measurement of well-being and other aspects of mental health. Journal of Occupational Psychology 1990;63:193-210. Heathcare Comission. National Survey of NHS staff 2007. 2008. Willis S, Seston EM, Hassell K. How do experiences at work influence pharmacy career and workforce behaviours? A qualitative study of occupational well-being and career development. London: Pharmacy Practice Research Trust; 2011. Information Centre. General Pharmaceutical Services in England and Wales 1998-99 to 2007-08. London: The Information Centre (Health Care); 2008. Hassell K, Seston EM, Schafheutle EI, Wagner A, Eden M. Workload in community pharmacies in the UK and its impact on patient safety and pharmacists' well-being: a review of the evidence. Health and Social Care in the Community 2011. What is the evidence that workload is affecting hospital pharmacists’ performance and patient safety? 17. 18. 19. 20. 21. 22. 23. 24. 25. 26. 27. 28. 29. 30. 31. 32. Pedersen CA, Schneider PJ, Scheckelhoff DJ. ASHP national survey of pharmacy practice in hospital settings: Dispensing and administration2005. Am J Health-Syst Pharm 2006;63(4):327-45. Fitzpatrick RW. Comparison of staffing establishments in hospital pharmacies in England. Pharm J 2010;284:504-6. Bond CM, Blenkinsopp A, Inch J, Celino G, Gray N. The effect of the new community pharmacy contract on the community pharmacy workforce. London: Pharmacy Practice Research Trust; 2008. Anon. Half of all pharmacists are "constantly stressed". Pharm J 2009;282:706. Scanlon MC, Karsh B-T. Value of human factors to medication and patient safety in the intensive care unit. Critical Care Medicine 2010;38(6):S90-S96. Anto B, Barlow D, Oborne A, Cape A, Vlassoff A, Whittlesea C. Dispensinglabel errors in hospital: types and potential causes. Int J Pharm Pract 2010;18(2):122-4. Beso A, Franklin BD, Barber N. The Frequency and Potential Causes of Dispensing Errors in a Hospital Pharmacy. Pharmacy World & Science 2005 Jun 20;27(3):182-90. James KL, Barlow D, Hiom S, Roberts D, Whittlesea C. Development and use of the critical incident technique in evaluating causes of dispensing incidents. Int J Pharm Pract 2008;16(4):239-49. James KL, Barlow D, Burfield R, Hiom S, Roberts D, Whittlesea C. A study of unprevented dispensing incidents in Welsh NHS hospitals. Int J Pharm Pract 2008;16(3):175-88. Roberts DE, Spencer MG, Burfield R, Bowden S. An analysis of dispensing errors in NHS hospitals. Int J Pharm Pract 2002;10(S1):R6. Eden M, Schafheutle EI, Hassell K. Workload pressure among recently qualified pharmacists: an exploratory study of intentions to leave the profession. Int J Pharm Pract 2009;17(3):181-7. Ferguson J, Hassell K, Ashcroft D. Qualitative insights into aspects of job dissatisfaction with workload among community and hospital pharmacists. Int J Pharm Pract 2009 ;17(s2):B2. Hiom S, Roberts D, Hawksbee M, Burfield R, Francis M, Walker K, et al. Benchmarking the current dispensing rate of Welsh hospital pharmacies. J Clin Pharm Ther 2006;31:357-62. Summerhayes M. The impact of workload changes and staff availability on IV chemotherapy services. Journal of Oncology Pharmacy Practice 2003;9(4):123. Conroy C, Cattell R, Nicholls M. Contribution of a ward-based technician service to delivering effective patient health care and reducing dispensary workload. Int J Pharm Pract 2002;10(3):171-5. Tomlin S, Saunders D. Pharmaceutical care: improving practice for children in hospital. Paediatric Nursing 2001;13(4):25-9. © CfWI | Month Year DRAFT # CONFIDENTIAL – footer 23 33. 34. 35. 36. 37. 38. 39. 40. 41. 24 James KL, Barlow D, Hiom S, Whittlesea C. The use of the critical incident technique to investigate prevented dispensing incidents developed by key informant interviews, focus group and observation. Int J Pharm Pract 2007;15(S1):A31. Anto B, Barlow D, Oborne A, Cape A, Vlassoff A, Whittlesea C. Dispensinglabel errors in hospital: types and potential causes. Int J Pharm Pract 2010;18(2):122-4. Armitage G, Newell R, Wright J. Improving the quality of drug error reporting. Journal of Evaluation in Clinical Practice 2010;16(6):1189-97. Tully MP, Buchan IE. Prescribing errors during hospital inpatient care: factors influencing identification by pharmacists. Pharmacy World & Science 2009;31(6):682. McCann L, Hughes CM, Adair CG. Assessing job satisfaction and stress among pharmacists in Northern Ireland. Pharmacy World & Science 2009;32(2):188-94. Noott A, Phipps GC. Monitoring and preliminary analysis of internal dispensing errors within a hospital trust. Pharmacy World & Science 2003;25:A42-A43. Barker S. Dispensing errors: recording, analysis and human error. Pharmacy management 2003;19(1):11-6. James KL, Barlow D, Burfield R, Hiom S, Roberts D, Whittlesea C. Unprevented or prevented dispensing incidents: which outcome to use in dispensing error research? Int J Pharm Pract 2011;19(1):36-50. Bateman R, Donyai P. Errors associated with the preparation of aseptic products in UK hospital pharmacies: lessons from the national aseptic error reporting scheme. Quality and Safety in Health Care 2010 Oct 1;19(5):1-6. What is the evidence that workload is affecting hospital pharmacists’ performance and patient safety? DISCLAIMER The Centre for Workforce Intelligence (CFWI) is an independent agency working on specific projects for the Department of Health and is an operating unit within Mouchel Management Consulting Limited (MMC). This report is prepared solely for the Department of Health by MMC, in its role as operator of the CFWI, for the purpose identified in the report. It may not be used or relied on by any other person, or by the Department of Health in relation to any other matters not covered specifically by the scope of this report. MMC has exercised reasonable skill, care and diligence in the compilation of the report and MMC's only liability shall be to the Department of Health and only to the extent that it has failed to exercise reasonable skill, care and diligence. Any publication or public dissemination of this report, including the publication of the report on the CFWI website or otherwise, is for information purposes only and cannot be relied upon by any other person. In producing the report, MMC obtains and uses information and data from third party sources and cannot guarantee the accuracy of such data. The report also contains projections, which are subjective in nature and constitute MMC's opinion as to likely future trends or events based on i) the information known to MMC at the time the report was prepared; and ii) the data that it has collected from third parties. Other than exercising reasonable skill, care and diligence in the preparation of this report, MMC does not provide any other warranty whatsoever in relation to the report, whether express or implied, including in relation to the accuracy of any third party data used by MMC in the report and in relation to the accuracy, completeness or fitness for any particular purposes of any projections contained within the report. MMC shall not be liable to any person in contract, tort (including negligence), or otherwise for any damage or loss whatsoever which may arise either directly or indirectly, including in relation to any errors in forecasts, speculations or analyses, or in relation to the use of third party information or data in this report. For the avoidance of doubt, nothing in this disclaimer shall be construed so as to exclude MMC's liability for fraud or fraudulent misrepresentation. © CfWI | Month Year DRAFT # CONFIDENTIAL – footer 25 www.cfwi.org.uk 26 The Centre for Workforce Intelligence produces quality intelligence to inform better workforce planning that improves people’s lives









© Copyright 2026