
Volumetric Capnography: Objectives 4/30/12 Clinical Utility of VCO
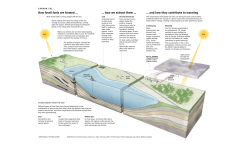
4/30/12 Volumetric Capnography: Clinical Utility of VCO2 during Mechanical Ventilation of Pediatric and Neonatal Patients Robert Campbell, RRT FAARC National Ventilation Technical Specialist Philips Healthcare Objectives • • • • • Define VCO2 Describe how VCO2 measured Describe the difference between EtCO2 & PaCO2 Explain the relationship between VCO2 & PaCO2 Understand the clinical application of VCO2 for ventilator management in the Pediatric and Neonatal environment What is VCO2??? • VCO2 is the volume of carbon dioxide eliminated or excreted through the lungs • VCO2 reflects changes in both ventilation and perfusion • In steady state, reflects CO2 production 1 4/30/12 Why Monitor VCO2??? • Validates need for ABGs • Identifies immediate changes in Ventilation and Perfusion (V/Q matching) • Allows optimization of MV parameters • Trended data may expedite weaning • VD/VT measurements can determine the severity of insult and prognosis Ventilation- Perfusion Relationships Relationship between ventilated alveoli and blood flow in the pulmonary capillaries CO2 O2 Shunt perfusion Alveoli perfused but not ventilated Normal Ventilation and perfusion is matched Deadspace Ventilation Alveoli ventilated but not perfused What Have We Traditionally Used To Monitor Our Patients? 2 4/30/12 Respiratory Parameters • ABG – Arterial Blood Gas – Gold standard – Measures ventilation and oxygenation • Pulse oximetry measures oxygenation • Capnography measures ETCO2 Non-Invasive CO2 • Detector/Indicator • Capnometry • Capnography Advanced Monitoring Capabilities • EtCO2 • Capnogram • Respiratory Rate • CO2 Elimination • Deadspace • Alveolar Ventilation • Physiologic VD/VT 3 4/30/12 Volumetric CO2 Leap Frog Technology Single Breath CO2 4 4/30/12 Volumetric Capnography Measures the Volume of Exhaled CO2 ETCO2 is a Measure of the partial pressure exerted in a gas Volumetric CO2 EtCO2 = 32 mmHg Vt = 600 ml VCO2 = 50 ml/min . EtCO2 = 32 mmHg Vt = 800 ml VCO2 = 200 ml/min EtCO2 = 32 mmHg Vt = 1000 ml VCO2 = 300 ml/min . . Important Parameters – Phys VD / VT PaCO2 - PeCO2 PaCO2 – Alveolar Ventilation – Min. Vol. CO2 (VCO2) = Y+Z X+Y+Z 5 4/30/12 ETCO2/PaCO2 Gradient • What Does This Gradient tell us? Capnography Arterial - End Tidal CO2 Gradient In healthy lungs the normal PaCO2 to ETCO2 gradient is 2-4 mmHg In diseased lungs, the gradient will increase due to ventilation/perfusion mismatch Gradient as a tool • Why? – Lets clinicians know when patient status improves PaCO2/ETCO2 gradient narrows – Aids in determining what caused a drop in ETCO2 If ventilation hasnt changed a sudden and large drop in ETCO2 usually indicates a change in perfusion – Requires an ABG to differentiate 6 4/30/12 Dead Space Ventilation ETCO2 = 33 mmHg PaCO2 = 53 mmHg 53 53 0 0 0 53 0 0 0 0 Alveoli that do not take part in gas exchange will still have no CO2 – Therefore they will dilute the CO2 from the alveoli that were perfused The result is a widened ETCO2 to PaCO2 Gradient VD/VT • Ratio of Total Deadspace (VD and VDphys) to Tidal Volume (VT) • Total Deadspace = Airway + Alveolar Deadspace • Normal = 0.25 to 0.30 • Estimates the Overall (In)efficiency of the Cardiorespiratory System Why measure Vd/Vt? • Pulmonary dead space is ventilation that is wasted as it does not participate in gas exchange. • Increase in Vd represents impaired ability to excrete CO2 • Increased dead-space fraction is a feature of the early phase of the ARDS • Elevated values of Vd/Vt are associated with an increased risk of death* *New England Journal of Medicine 2002;346: 1281-6 7 4/30/12 Outcomes • Deadspace fraction • Elevated in early ARDS: 0.58 ± 0.09 • Higher in patients who died (0.63±0.10 vs. 0.54±0.10) • For every 0.5 , odds of death by 45% MValv • Alveolar ventilation per minute • Amount of VT that reaches the alveoli and is available for gas exchange (effective ventilation) Why Measure MValv ? To provide the most effective CO2 Removal To manage alveolar ventilation and not Vte as measured by the ventilator Evaluate ventilator settings 500 ml delivered VT – 150 ml airway deadspace = 345 ml Why is this important? 8 4/30/12 Evaluate ventilator settings Knowing how much of the delivered VT is available for gas exchange is important – if the patient is fighting the vent and restless, the issue may be alveolar VT Ineffective Ventilation Monitoring CO2 elimination • CO2 elimination provides continuous feedback regarding ventilation and perfusion – Relationship between PaCO2 and CO2 elimination is either stable or inverse – Instant feedback when making ventilator setting changes: Did perfusion change? Did ventilation change? With PaCO2 from an ABG, you can answer the question, did Vd/Vt change? 9 4/30/12 VCO2/MValv Relationship VCO2/MValv Relationship VCO2/MValv Relationship 10 4/30/12 Duke university medical center • Extubation Study – Demonstrated that VD/ VT ratio measurements successfully predicted extubation outcomes – Elevated VD/VT, warning of patient risk for respiratory difficulty 100 4 90 33 80 70 80 60 50 96 40 67 30 20 20 10 0 <0.50 0.51-0.64 % Success >0.64 % Failure Independent Effect of Etiology of Failure and Time to Reintubation on Outcome for Patients Failing Extubation S. Epstein & R Ciubotaru, AJRCCM, Vol. 158, N°2, August 1998, 489-493 Successful Weaning Trial Shows in spontaneous alveolar ventilation & corresponding decrease in ventilator support. VCO2 suggests metabolic activity due to additional task of breathing by the patient. Delivered mechanical tidal volume has not changed & spontaneous tidal volume is increasing (SIMV rate ). Shows PATIENT RESPONSE to the trial allowing for better management of the weaning process. 11 4/30/12 Unsuccessful Weaning Trial SIMV and patient started to take over ventilation. But patient shows signs of fatigue at early stage ( VCO2 followed by in spontaneous tidal volume). Leads to in PaCO2 & EtCO2. Return to mechanical ventilation. Assists clinicians in determining PATIENT RESPONSE. When used effectively, these utilities may help reduce costly ventilator days. Spont Breathing Trials-SBT Successful SBT . 12 4/30/12 Unsuccessful SBT Initially, patient had a small amount of ventilatory support, but then was placed on a T-piece. The entire task of breathing was placed on the patient. Within minutes trends showed that the patient was unable to support the required level of ventilation (VCO2 decreasing since total Alveolar Ventilation is decreasing). Spontaneous Tidal Volume trend also shows inadequate ventilation. Removal of mechanical support, increased Vd/Vt, reducing ventilatory efficiency and the patients ability to remove CO2. This resulted in a pattern of rapid shallow breaths requiring the patient to be placed back on full mechanical support. Stable Ventilation with Decreasing VCO2 Showing a Change in Perfusion Monitoring trends allows for detection of sudden and rapid in VCO2, without change in Alveolar Minute Volume or Tidal Volumes. Drop in VCO2 suggests change in blood flow to the lungs. VCO2 may be due to in C.O. or blood loss. VCO2 may be due to in C.O. or malignant hyperthermia. Coupled with Alveolar Ventilation and Deadspace measurements, this allows for quick patient assessment. Optimization of PEEP • To Minimize Lung Injury: – Provide enough PEEP to recruit the recruitable alveoli, but not apply too much PEEP to over distend the healthier regions – Avoid a PEEP/Vt/P combination that doesnt unnecessarily over distend lung regions at end inspiration (overall PIP) 13 4/30/12 How Much Peep is Enough? ALuRT Observe for stable baseline • PEEP is at 10 cm H2O in this example ALuRT Step 1 • PEEP is from 10 cm H2O to 12 cm H2O for 5-15 minutes. No change in Vtalv and VCO2 (CO2 elimination) indicates no alveolar recruitment 14 4/30/12 ALuRT Step 2 • PEEP is to 14 cm H2O for 5-15 minutes and Vtalv and CO2 elimination begin to increase indicating alveolar recruitment. ALuRT Step 3 • PEEP is increased to 16 cm H2O and VTalv and CO2 elimination continue to rise. ALuRT Step 4 • At a PEEP of 18 cm H2O we see no increase in Vtalv and VCO2 drops indicating worsening V/Q from decreased pulmonary perfusion. 15 4/30/12 ALuRT Step 5 • When PEEP is to 16 cm H2O, CO2 elimination back to baseline meaning optimal recruitment pressures and pulmonary perfusion (V/Q). Store plot prior to first PEEP increase Single breath CO2 waveform 16 4/30/12 Drop in Perfusion Recruitment Maneuver Before recruitment After recruitment ALuRT provides continuous monitoring to detect derecruitment of alveoli • Alveolar ventilation and VCO2 will decrease if the lung de-recruits 17 4/30/12 Using VTalv and VCO2 to recruit alveoli • Clinical Course – PEEP increased by 2 cm H2O every 10 minutes – Observed Vtalv/VCO2/SpO2 • Red arrows show PEEP • No deterioration in VCO2 V/Q stable • VTalv starts to at 16 cm H2O, alveoli are being recruited • SpO2 responds at 20 cm H2O Pt in Bronchospasm Patient with Asthma – Improvement Following Aerosol Therapy CO2 Day 1 Day 5 Exhaled Volume 18 4/30/12 Bedside Applications Monitoring the Patients Response to Ventilator Management Ventilation Management Optimize Vt Setting • Use Vdaw and Vdalv to assure adequate VT VCO2 • Use Single Breath Curve to assess phase III Vd/Vt MValv Ventilation Management Optimize PEEP VCO2 Vd/Vt MValv • Use Vtalv, VCO2, and trend to determine lung recruitment and optimal PEEP • Use Single Breath Curve for immediate feedback 19 4/30/12 Ventilation Management Optimize Weaning VCO2 Vd/Vt • Use MValv and VCO2 to trend weaning tolerance • Early detection of fatigue and failure MValv • Enhanced titration of adequate support and confirmation of resting state Ventilation Management Surfactant Replacement VCO2 • Use MValv, VCO2, and single breath curve to manage ventilation during surfactant replacement therapy Vd/Vt MValv • Detect open and available lung units • Enhanced titration of adequate settings as lung compliance and volume change Ventilation Management Inhaled Nitric Oxide VCO2 • Use MValv, VCO2, and single breath curve to manage ventilation during Inhaled Nitric Oxide therapy Vd/Vt MValv • Especially useful during weaning of INO • Confirm maintenance of lung recruitment and adequate PEEP 20 4/30/12 Weaning Criteria Guide Weaning Process Vd/Vt is a single variable that defines total cardiorespiratory system efficiency and can predict successful extubation “A Vd/Vt ratio less than 0.50 reliably predicts successful extubation whereas a Vd/Vt ratio greater than 0.65 correlates with extubation failure. Dead Space to Tidal Volume Ratio (Vd/Vt) Predicts Successful Extubation in Infants and Children – Christopher Hubble MD, Mike Gentile RRT, Donna Tripp RRT, Damian Craig MS, Jon Meliones MD, FCCM, Ira Cheifetz MD – Critical Care Medicine, Vol. 28, N°6 – June 2000 VCO2: Useful adjunct for monitoring during Mechanical Ventilation Questions ? 21








© Copyright 2026