ABC
docz
Explore
Log in
Create new account
Download
Report
No category
Joint Health and Social Care Integration Programme Information Sharing Protocol
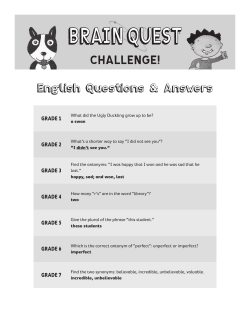
Brain Quest English Questions & Answers Grades 1-7
Document 25539
Tariffs and Profitability for Gynaecological Oncology Services Rob Gornall Gynaecological Oncologist
Endocrine Advisory Group Meeting 2 September 2003
Lv Jian-wei Department of Urology, Renji Hospital Affiliated to Shanghai
HTA in the UK: 10 years experience of NICE Francoise Cluzeau NICE International
20s Plenty for Us Abbey Community Association Ltd
The Royal Marsden Thyroid Cancer Conference The Royal Marsden Conference Team
Step-by-Step Guide: Calculating 2013-14 National Tariff
Trainees’ session AUTOPSY HISTOPATHOLOGY Sebastian Lucas Dept of Histopathology
Ann B. Rodriguez Cancer Center Helping cancer patients along their
Document 10802
© Copyright 2026
About abcdocz
DMCA / GDPR
Report