
Saturday, 27 April 2013 Autism Behavioural Intervention Association
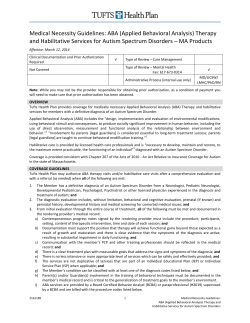
Saturday, 27 April 2013 ABA Today is presented by: Autism Behavioural Intervention Association p: 03 98300677 | w: www.abia.net.au Why is ABA Evidence-Based? 4/27/13 Why is ABA an evidence-based treatment for autism? Eric V. Larsson, PhD, LP BCBA-D The Lovaas Institute Midwest (c) Eric Larsson, PhD, BCBA-D, The Lovaas Institute Midwest 1 Why is ABA Evidence-Based? 4/27/13 ABA is not Medically Necessary? Uses rote techniques to create robotic responding 40 hours is unnecessary – robs a child of their childhood It is all drills at a table – no natural social skills It is punishment based It doesn’t work for high functioning children It doesn’t work for low functioning children It doesn’t work for older children It doesn’t work for younger children It is based upon bribery Children don’t really recover It doesn’t take into account the whole child It denies the child their own self direction It plays upon the fears of the parents It is too expensive It is not used in classrooms Its curriculum does not take into account pragmatics The staff are poorly trained It doesn’t help the parents with the real challenges of daily life It creates prompt dependency It creates anxious, and depressed children It relies upon edible reinforcers It doesn’t develop advanced abstract language Low Quality ABA comes from Low Quality Implementation (c) Eric Larsson, PhD, BCBA-D, The Lovaas Institute Midwest 2 Why is ABA Evidence-Based? 4/27/13 Nationwide Hearings on ABA 1997-2012 Primarily due to the intense resistance of school districts to funding in-home and private services, many independent state, federal, and professional task forces were convened to study intensive early intervention using behavioral models. These task forces universally found that the services were appropriate and effective, and hence medically necessary. American Academy of Pediatrics British Columbia Supreme Court California Legislative Commission Maine Administrators of Services for Children New York State Department of Health U.S. Surgeon General Mental Health Report National Research Council Autism Research Institute Centers for Disease Control American Academy of Child and Adolescent Psychiatry American Academy of Neurology American Psychological Association Division of Clinical Psychology What is the evidence for ABA? (c) Eric Larsson, PhD, BCBA-D, The Lovaas Institute Midwest 3 Why is ABA Evidence-Based? 4/27/13 B.F. Skinner The Experimental Analysis of Behavior Analysis of the continuous change in behavior: Development of the fixed interval scallop Skinner, 1950 (c) Eric Larsson, PhD, BCBA-D, The Lovaas Institute Midwest 4 Why is ABA Evidence-Based? 4/27/13 Analysis of the dynamic change in behavior vs. the static average Skinner, 1950 Don Baer, Mont Wolf, Todd Risley Applied Behavior Analysis (c) Eric Larsson, PhD, BCBA-D, The Lovaas Institute Midwest 5 Why is ABA Evidence-Based? 4/27/13 Risley & Wolf (1968) Contingent Reinforcement of Accurate Vocal Imitation (c) Eric Larsson, PhD, BCBA-D, The Lovaas Institute Midwest 6 Why is ABA Evidence-Based? 4/27/13 O. Ivar Lovaas UCLA: Early Intensive Treatment for Autism Lovaas & Simmons (1969) Gregg's self-injury (head hitting) over successive sessions (1 through 7). The upward moving hatchmarks in Sessions 3 and 5 mark delivery of sympathetIc comments, play, etc., contingent on self-injury. (c) Eric Larsson, PhD, BCBA-D, The Lovaas Institute Midwest 7 Why is ABA Evidence-Based? 4/27/13 Lovaas (1966) Development of Social Conditioned Reinforcers Koegel, Egel, & Williams (1980) (c) Eric Larsson, PhD, BCBA-D, The Lovaas Institute Midwest 8 Why is ABA Evidence-Based? 4/27/13 Parrish, Cataldo, (1986) Covariation of Compliance and Behavior in Group and Individual Sessions Why is this data important? (c) Eric Larsson, PhD, BCBA-D, The Lovaas Institute Midwest 9 Why is ABA Evidence-Based? 4/27/13 The Development of the Young Child How many successful learning trials per day does the child receive? (c) Eric Larsson, PhD, BCBA-D, The Lovaas Institute Midwest 10 Why is ABA Evidence-Based? 4/27/13 How many inadvertent autistic trials per day does the child receive? To make progress, Preventing practice of autistic responding the child must practice target responding more often than he is allowed to practice autistic responding Throughout the child’s day, he is getting many SDs in natural situations We must train the parents and staff to ensure that these teachable moments result in learning new target behavior At the end of the day, were 80% of his teachable moments successful? The Implications of Research in Applied Behavior Analysis Behavior constantly responds to its environment Resulting in all of the learned behavior patterns of life Inconsistent or maladaptive treatment does not easily result in progress toward normalcy Therefore to alter the course of autism We must transform the child’s home and community into a 24-hour therapeutic environment (c) Eric Larsson, PhD, BCBA-D, The Lovaas Institute Midwest 11 Why is ABA Evidence-Based? 4/27/13 Does ABA Research Prove This? Effect of Parent Involvement (c) Eric Larsson, PhD, BCBA-D, The Lovaas Institute Midwest 12 Why is ABA Evidence-Based? 4/27/13 Effect of Intensity Group Data backed up by Individual ABA Outcome Data Lovaas 1987 Child by Child Behavior Data 20 18 Number of Children 16 14 12 10 8 6 4 2 0 Dramatic Complex Play Play Peer Play Normal Best IQ Outcomes Pre (c) Eric Larsson, PhD, BCBA-D, The Lovaas Institute Midwest Severe MR Stereotpd Tantrum Behavior Mute Post 13 Why is ABA Evidence-Based? 4/27/13 But is this data replicated? The Scope of Individualized ABA Research before 2000 (c) Eric Larsson, PhD, BCBA-D, The Lovaas Institute Midwest 14 Why is ABA Evidence-Based? 4/27/13 Research on the Treatment of the Restricted Range of Interests Positive Reinforcement to Remediate Stereotyped, Perseverative Tendencies Significant Researchers: Ferster, Indiana U.; Wolf, Risley, U. of Washington; Koegel, Dunlap, Rincover, Newsome, Carr, Lovaas, UCLA; Hall, U. of Washington; Sajwaj, U. of Tennessee; Baer, U. of Kansas; Repp, Dietz, U. of Georgia; Iwata, Florida State U.; Dyer, The May Institute; Salient Research Studies: 39 Time Span: 1961 – 1990 Sample Study: Charlop, M.H., Kurtz, P.F., & Casey, F.G. (1990). Using aberrant behaviors as reinforcers for autistic children. Journal of Applied Behavior Analysis. 23, 163-182. Effects of Structure on Stereotyped, Perseverative Tendencies Significant Researchers: Lovaas, Schreibman, Koegel, Dunlap, Newsome, UCLA; Foxx, Azrin, U. of Southern Illinois; Iwata, Bailey, Florida State U.; Repp, Northern Illinois U.; Dyer, The May Institute; Salient Research Studies: 31 Time Span: 1965 – 1991 Sample Study: Koegel, R.L, Dunlap, G., & Dyer, K. (1980). Intertrial interval duration and learning in autistic children. Journal of Applied Behavior Analysis, 13, 91-99. Research on the Treatment of the Restricted Range of Interests Development of Effective Skill Development Strategies Significant Researchers: Risley, LeBlanc, Spradlin, U. of Kansas; Touchette, Columbia; Schreibman, Russo, Lovaas, Dunlap, Rincover, Koegel, UCLA; Dyer, Christian, Luce, The May Institute; Repp, Northern Illinois U.; Charlop, Claremont College; Heward, Heron, Ohio State U.; Salient Research Studies: 42 Time Span: 1965 – 1996 Sample Study: Schreibman, L. (1975). Effects of within-stimulus and extra-stimulus prompting on discrimination learning in autistic children. Journal of Applied Behavior Analysis, 8, 91-112. Generalization of Treatment Gains Significant Researchers: Wolf, Sulzbacher, U. of Washington; Sulzer, U. of Massachusetts; Sailor, Walker, Baer, Hart, Risley, U. of Kansas; Wahler, U. of Tennessee; Rincover, Koegel, UCLA; Handleman, Rutgers; McGee, Krantz, McClannahan, Princeton Child Development Center; Salient Research Studies: 29 Time Span: 1966 – 1996 Sample Study: McGee, G.G., Krantz, P.J., & McClannahan, L.E. (1985). The facilitative effects of incidental teaching on preposition use by autistic children. Journal of Applied Behavior Analysis. 18, 17-32. Gena, A., Krantz, P., McClannahan, L.E., & Poulson, C.L. (1996). Training and generalization of affective behavior displayed by youth with autism. Journal of Applied Behavior Analysis, 29, 291-304. (c) Eric Larsson, PhD, BCBA-D, The Lovaas Institute Midwest 15 Why is ABA Evidence-Based? 4/27/13 Research on the Treatment of Language Deficits Development of Imitation Skills Significant Researchers: Baer, Sherman, Garcia, U. of Kansas; Lovaas, UCLA; Salient Research Studies: 19 Time Span: 1964 – 1994 Sample Study: Baer, D.M., Peterson, R.F., & Sherman, J.A. (1967). The development of imitation by reinforcing behavioral similarity to a model. Journal of the Experimental Analysis of Behavior, 10, 405-416. Development of Basic Language Skills Significant Researchers: Michael, U. of Arizona; Salzinger, Columbia U.; Risley, Wolf, U. of Washington; Sloane, Mithaug, Charlop, Claremont College; Foxx, Southern Illinois U.; Salient Research Studies: 28 Time Span: 1965 – 1987 Sample Study: Schumaker, J., & Sherman, J.A. (1970). Training generative verb usage by imitation and reinforcement procedures. Journal of Applied Behavior Analysis. 3, 273-287. Research on the Treatment of Language Deficits Development of Complex Language Skills Significant Researchers: Guess, Baer, Sailor, Garcia, U. of Kansas; Krantz, McClannahan, Princeton Child Development Center; Smith, Lovaas, UCLA; Salient Research Studies: 32 Time Span: 1968 – 1992 Sample Study: Stevens-Long, J, & Rasmussen, M. (1974). The acquisition of simple and compound sentence structure in an autistic child. Journal of Applied Behavior Analysis. 7, 473-479. Development of Social Compliance Significant Researchers: Baer, Rowbury, Allen, U. of Kansas; Forehand, U. of Georgia; Neef, Russo, Cataldo, Johns Hopkins U.; Mace, U. of Utah; Salient Research Studies: 18 Time Span: 1964 – 1988 Sample Study: Larsson, D. G., & Larsson, E. V. (1983). Manipulating peer presence to program the generalization of verbal compliance from one-to-one to group instruction. Education and Treatment of Children, 6, 109-122. (c) Eric Larsson, PhD, BCBA-D, The Lovaas Institute Midwest 16 Why is ABA Evidence-Based? 4/27/13 Research on the Treatment of Significant Social Deficits Development of Social Play Skills Significant Researchers: Baer, Allen, Hart, Rogers, Rowbury, Fowler, Kohler, Greenwood, U. of Kansas; Koegel, Dunlap, Dyer, UCLA; Strain, U. of Pittsburgh; Carr, SUNY Stony Brooke; McEvoy, Vanderbilt; Salient Research Studies: 31 Time Span: 1968 – 1994 Sample Studies: Haring, T.G. (1985). Teaching between-class generalization of toy play behavior to handicapped children. Journal of Applied Behavior Analysis. 18, 127-140. Pierce, K., & Schreibman, L., (1995). Increasing complex social behaviors in children with autism: Effects of peer-implemented pivotal response training. Journal of Applied Behavior Analysis, 28. 285-296. Development of Creativity and Spontaneity Significant Researchers: Baer, U. of Kansas; Charlop, Schreibman, Claremont College; Dunlap, Marshall U; Haring, U. of Washington; Van Houten, Halifax U.; Harris, Rutgers; Salient Research Studies: 18 Time Span: 1972 – 1995 Sample Studies: Goetz, E.M., & Baer, D.M. (1973). Social control of form diversity and the emergence of new forms in children’s block building. Journal of Applied Behavior Analysis. 6, 209-217. Ingenmey, R., & Van Houten, R. (1991). Using time delay to promote spontaneous speech in an autistic child. Journal of Applied Behavior Analysis, 24, 591-596. Research on the Treatment of Significant Social Deficits Development of Social Conversation Skills Significant Researchers: Garcia, Kamps, U. of Kansas; Strain, U. of Pittsburgh; Neef, Western Michigan State; Charlop, Claremont College; Koegel, U.C. Santa Barbara; Krantz, McClannahan, Princeton Child Development Institute; Salient Research Studies: 32 Time Span: 1974 – 1995 Sample Studies: Camarata, S. (1993). The application of naturalistic conversation training to speech production in children with speech disabilities. Journal of Applied Behavior Analysis, 26. 173-182. Development of Group and Classroom Skills Significant Researchers: Koegel, Rincover, Russo, UCLA; Favell, U. of North Carolina; Fowler, Baer, Guess, Kamps, U. of Kansas; Strain, U. of Pittsburgh; Sasso, U. of Iowa; Salient Research Studies: 26 Time Span: 1967 – 1994 Sample Studies: Werts, M.G., Caldwell, N.K., & Wolery, M. (1996). Peer modeling of response chains: Observational learning by students with disabilities. Journal of Applied Behavior Analysis, 29, 53-66. (c) Eric Larsson, PhD, BCBA-D, The Lovaas Institute Midwest 17 Why is ABA Evidence-Based? 4/27/13 Service System Research Staff and Parent Training Procedures Significant Researchers: Guess, Baer, Spradlin, U. of Kansas; Koegel, Schreibman, Russo, Rincover, Glahn, UCLA; O’Dell, U. of Mississippi; McClannahan, Krantz, McGee, Princeton Child Development Center; Strain, U. of Pittsburgh; Dyer, Luce, The May Institute; Salient Research Studies: 41 Time Span: 1968 – 1993 Sample Studies: Koegel, R.L, Russo, D.C., & Rincover, A., (1977). Assessing and training teachers in the generalized use of behavior modification with autistic children. Journal of Applied Behavior Analysis, 10, 197-205. Koegel, R.L., Glahn, T.J. & Nieminen, G.S. (1978). Generalization of parent-training results. Journal of Applied Behavior Analysis, 11, 95-109. 39 Group Replications of Intensive Treatment Research Eldevik, S., Hastings, R., Jahr, E., & Hughes, J.C. (2012). Outcomes of behavioral intervention for children with autism in mainstream pre-school settings. Journal of Autism and Developmental Disorders. 42, 210-220. Leaf, R.B., Taubman, M.T., McEachin, J.J., Leaf, J.B., & Tsuji, K.H. (2011). A program description of a community-based intensive behavioral intervention program for individuals with Autism Spectrum Disorders. Education and Treatment of Children. 34, 259-285. Dawson, G., Rogers, S.J., Munson, J., Smith, M., Winter, J., Greenson, J., et al. (2010). Randomized, controlled trial of an intervention for toddlers with autism: The early start Denver model. Pediatrics, 125, 17–23. Smith, I.M., Koegel, R.L., Koegel, L.K., et al. (2010). Effectiveness of a novel community-based early intervention model for children with autistic spectrum disorder. American Journal on Intellectual and Developmental Disabilities. 115, 504–523. Kelley, E., Naigles, L., & Fein, D. (2010). An in-depth examination of optimal outcome children with a history of autism spectrum disorders. Research in Autism Spectrum Disorders. 4, 526-538. Kasari, C., Gulsrud, A., Wong, C., et al. (2010). Randomized controlled caregiver-mediated joint engagement intervention for toddlers with autism. Journal of Autism and Developmental Disorders, 40, 1045–1056. McGarrell, M., Healy, O., Leader, G., O'Connor, J., & Kenny, N. (2009). Six reports of children with autism spectrum disorder following intensive behavioral intervention using the Preschool Inventory of Repertoires for Kindergarten (PIRK). Research in Autism Spectrum Disorders, 3, 767-782, Wood, J. J., Drahota, A., Sze, K., Har, K., Chiu, A., & Langer, D. A. (2009). Cognitive behavioral therapy for anxiety in children with autism spectrum disorders: A randomized, controlled trial. Journal of Children Psychology and Psychiatry and Allied Disciplines, 50, 224-234. Perry, A., Cummings, A., Geier, J. D., Freeman, N. L., Hughes, S., LaRose, L., Managhan, T., Reitzel, J.-A., & Williams, J. (2008). Effectiveness of intensive behavioral intervention in a large, communitybased program. Research in Autism Spectrum Disorders, 2, 621–642. Osborne, L.A., McHugh, L., Saunders, J. & Reed, P. (2008). Parenting Stress Reduces the Effectiveness of Early Teaching Interventions for Autistic Spectrum Disorders. Journal of Autism and Developmental Disorders. 38, 1092–1103 Eikeseth, S., Smith, T., Jahr, E., & Eldevik, S. (2007) Outcome for Children with Autism who began Intensive Behavioral Treatment Between Ages 4 and 7: A Comparison Controlled Study. Behavior Modification, 31, 264-278. Remington, B., Hastings, R.P., Kovshoff, H., degli Espinosa, F., Jahr, E., Brown, T., Alsford, P., Lemaic, M., & Ward, N. (2007). Early intensive behavioral intervention: Outcomes for children with autism and their parents after two years. American Journal on Mental Retardation. 112, 418-438. Ben-Itzchak, E., & Zachor, D.A. (2007). The effects of intellectual functioning and autism severity on outcome of early behavioral intervention for children with autism. Research in Developmental Disabilities, 28, 287–303. Eldevik, S., Eikeseth, S., Jahr, E., & Smith, T. (2006). Effects of Low-Intensity Behavioral Treatment for Children with Autism and Mental Retardation. Journal of Autism & Developmental Disorders. 36, 211-224. Cohen, H., Amerine-Dickens, M., & Smith, T., (2006). Early Intensive Behavioral Treatment: Replication of the UCLA Model in a Community Setting. Developmental and Behavioral Pediatrics, 27, S145-S155. Butter, E. M., Mulick, J. A., & Metz, B. (2006). Eight case reports of learning recovery in children with pervasive developmental disorders after early intervention. Behavioral Interventions, 21, 227-243. Kelley, E., Paul, J.J., Fein, D., & Naigles, L.R. (2006). Residual language deficits in optimal outcome children with a history of autism. Journal of Autism and Developmental Disorders. 36, 807-828. Howard, J.S., Sparkman, C.R., Cohen, H.G., Green G., & Stanislaw H. (2005). A comparison of intensive behavior analytic and eclectic treatments for young children with autism. Research in Developmental Disabilities. 26, 359-383. Sallows, G.O., & Graupner, T.D. (2005). Intensive Behavioral Treatment for Children With Autism: Four-Year Outcome and Predictors. American Journal on Mental Retardation, 110, 417-438. (c) Eric Larsson, PhD, BCBA-D, The Lovaas Institute Midwest Eikeseth, S., Smith, T., Jahr, E., & Eldevik, S. (2002). Intensive behavioral treatment at school for 4to 7-year-old children with autism – A 1-year comparison controlled study. Behavior Modification, 26, 46-68. Green, G., Brennan, L.C., & Fein, D. (2002). Intensive behavioral treatment for a toddler at high risk for autism. Behavior Modification. 26. 69-102. Bibby P, Eikeseth S, Martin, N. T., Mudford, O. C., & Reeves, D., (2002). Progress and outcomes for children with autism receiving parent-managed intensive interventions. Research in Developmental Disabilities. 23, 81-104. Mudford, O.C., Martin, N.T., Eikeseth, S., & Bibby, P. (2001). Parent-managed behavioral treatment for preschool children with autism: Some characteristics of UK programs. Research in Developmental Disabilities, 22, 173-182. Smith, T., Buch, G.A., & Gamby, T.E. (2000). Parent-directed, intensive early intervention for children with pervasive developmental disorder. Research in Developmental Disabilities, 21, 297-309. Smith, T., Groen, A.D., & Wynn, J.W. (2000). Randomized trial of intensive early intervention for children with pervasive developmental disorder. American Journal on Mental Retardation.105, 269-285. Harris, S.L., & Handleman, J.S. (2000). Age and IQ at intake as predictors of placement for young children with autism: a four- to six-year follow-up. Journal of Autism and Developmental Disorders, 30, 137-142. Weiss, M. J. (1999). Differential rates of skill acquisition and outcomes of early intensive behavioral intervention for autism. Behavioral Interventions, 14, 3-22. Sheinkopf, S., & Siegel, B. (1998). Home-based behavioral treatment for young autistic children. Journal of Autism and Developmental Disorders. 23, 15-23. Smith T., Eikeseth, S., Klevstrand, M., & Lovaas, O.I. (1997). Intensive behavioral treatment for preschoolers with severe mental retardation and pervasive developmental disorder. American Journal on Mental Retardation. 102, 238-249. Perry, R., Cohen, I., & DeCarlo, R. (1995). Case study: Deterioration, autism, and recovery in two siblings. Journal of the American Academy of Child and Adolescent Psychiatry. 34, 232-237. Smith, T., Klevstrand, M., & Lovaas, O.I. (1995). Behavioral treatment of Rett's Disorder: Ineffectiveness in three cases. American Journal on Mental Retardation, 100, 317-322. Birnbrauer, J.S., & Leach, D.J. (1993). The Murdoch early intervention program after 2 years. Behaviour Change, 10, 63-74. Harris, S., Handleman, J., Gordon, R., Kristoff, B., & Fuentes, F. (1991). Changes in cognitive and language functioning of preschool children with autism. Journal of Autism and Developmental Disorders, 21, 281-290. Dunlap, G., Robbins, F.R., Dollman, C., & Plienis, A.J. (1988). Early intervention for young children with autism: A regional training approach. Huntington, WV: Marshall University. Sherman, J., Barker, P., Lorimer, P., Swinson, R., & Factor, D. (1988). Treatment of autistic children: Relative effectiveness of residential, out-patient and home-based interventions. Child Psychiatry and Human Development, 19, 109-125. Anderson, S. R., Avery, D. L., DiPietro, E. K., Edwards, G. L., & Christian, W. P. (1987). Intensive home-based early intervention with autistic children. Education and Treatment of Children, 10, 352-366. Harris, S.L. (1986). Parents as teachers: A four to seven year follow up of parents of children with autism. Child & Family Behavior Therapy, 8, 39-47. Fenske, E.C., Zalenski, S., Krantz, P.J., & McClannahan, L.E. (1985). Age at intervention and treatment outcome for autistic children in a comprehensive intervention program. Analysis and Intervention in Developmental Disabilities, 5, 49-58. Strain, P.S., Hoyson, M.H., & Jamieson, B.J. (1985). Normally developing preschoolers as intervention agents for autistic‑like children: Effects on class deportment and social interactions. Journal of the Division for Early Childhood. 9, 105‑115. 18 Why is ABA Evidence-Based? 4/27/13 9 Meta Analyses of Intensive Treatment Research Reichow, B. (2012). Overview of Meta-Analyses on Early Intensive Behavioral Intervention for Young Children with Autism Spectrum Disorders. Journal of Autism and Developmental Disorders. 42, 512-520. Peters-Scheffer, N., Didden, R., Korzilius, H., & Sturmey, P. (2011). A meta-analytic study on the effectiveness of comprehensive ABA-based early intervention programs for children with Autism Spectrum Disorders. Research in Autism Spectrum Disorders, 5, 60-69. doi:10.1016/j.rasd.2010.03.011 Eldevik, S., Hastings, R.P., Hughes, J.C., Jahr, E., Eikeseth, S., & Cross, S., (2010). Using Participant Data to Extend the Evidence Base for Intensive Behavioral Intervention for Children With Autism. American Journal on Intellectual and Developmental Disabilities. 115, 381-405. DOI: 10.1352/1944-7558-115.5.381 Virués-Ortega, J. (2010). Applied behavior analytic intervention for autism in early childhood: Meta-analysis, metaregression and dose–response meta-analysis of multiple outcomes. Clinical Psychology Review. 30, 387-399. doi: 10.1016/j.cpr.2010.01.008 Makrygianni, M.K., & Reed, P. (2010). A meta-analytic review of the effectiveness of behavioural early intervention programs for children with Autistic Spectrum Disorders. Research in Autism Spectrum Disorders. 4:577-593. doi: 10.1016/j.rasd.2010.01.014 Eldevik, S., Hastings, R.P., Hughes, J.C., Jahr, E., Eikeseth, S., & Cross, S., (2009). Meta-analysis of early intensive behavioral intervention for children with autism. Journal of Clinical Child and Adolescent Psychology. 38, 439–450. doi:10.1080/15374410902851739. PMID 19437303. Reichow, B., & Wolery, M. (2008). Comprehensive synthesis of early intensive behavioral interventions for young children with autism based on the UCLA Young Autism Project model. Journal of Autism and Developmental Disorders. 31:23–41. doi:10.1007/s10803-008-0596-0. PMID 18535894. Bellini, S., Peters, J.K., Benner, L., & Hopf, A. (2007). A meta-analysis of school-based social skills interventions for children with autism spectrum disorders. Remedial and Special Education. 28, 153-162. Bellini, S., & Akullian, J. (2007). A Meta-Analysis of Video Modeling and Video Self-Modeling Interventions for Children and Adolescents with Autism spectrum disorders. Exceptional Children, 73, 261-284. What are the essential features of these studies? (c) Eric Larsson, PhD, BCBA-D, The Lovaas Institute Midwest 19 Why is ABA Evidence-Based? 4/27/13 Evidence-Based Levels of Behavior Therapy, Behavior Analysis, and Clinical Supervision What is the effective age for ABA? (c) Eric Larsson, PhD, BCBA-D, The Lovaas Institute Midwest 20 Why is ABA Evidence-Based? 4/27/13 Cost Effective Age Range of EIBI The range of age cut-offs in evidence-based EIBI studies were established for the purpose of controlled research, and were based upon a number of factors, such as available funding. They weren’t meant to imply that autism was untreatable after those ages. Throughout the EIBI literature, the published range of such age cut-offs, for the purpose of research, was 48 to 84 months for the maximum age to begin receiving treatment, and then the subsequent duration of treatment was one to five years. Therefore the age of completion of these children’s intensive treatment was up to 12 years of age. Social Skills Meta Analysis Bellini and colleagues, in 2007, reported the following age ranges of 155 children who benefited from ABA social skills training: “21 studies involved preschool-age children, 23 involved elementary age children, and 5 studies involved secondary-age students.” (page 158). (c) Eric Larsson, PhD, BCBA-D, The Lovaas Institute Midwest 21 Why is ABA Evidence-Based? 4/27/13 Social Skills Meta Analysis Reichow and Volkmar, in 2010, reported on 31 studies of children, aged four to fifteen, who benefited from ABA social skills training: “The school-age category had the highest participant total of the three age categories (N = 291).” (page 156). “Within the last 8 years, 66 studies with strong or acceptable methodological rigor have been conducted and published. These studies have been conducted using over 500 participants, and have evaluated interventions with different delivery agents, methods, target skills, and settings. Collectively, the results of this synthesis show there is much supporting evidence for the treatment of social deficits in autism.” (page 161). Aggression – Peer Review Brosnan and Healy, in 2011, reported on 18 studies of children aged three to 18, who received effective ABA treatment to reduce or eliminate severe aggressive behavior: “All of the studies reported decreases in challenging behavior attributed to the intervention. Of the studies included, seven reported total or near elimination of aggression of at least one individual during intervention in at least one condition.” (page 443). “only four of the studies conducted follow-up assessments. However, each of these studies reported that treatment gains were maintained.” (page 443). (c) Eric Larsson, PhD, BCBA-D, The Lovaas Institute Midwest 22 Why is ABA Evidence-Based? 4/27/13 Anxiety Lang, et al. in 2010, reported on nine studies which involved 110 children aged nine to 23, who received a variety of forms of behavior therapy for anxiety. “Within each reviewed study, at least one dependent variable suggested a reduction in anxiety following implementation of CBT.” (page 60). “CBT has been modified for individuals with ASD by adding intervention components typically associated with applied behaviour analysis (e.g. systematic prompting and differential reinforcement). Future research involving a component analysis could potentially elucidate the mechanisms by which CBT reduces anxiety in individuals with ASD, ultimately leading to more efficient or effective interventions.” (page 53). Problem Behavior Hanley, Iwata, and McCord in 2003, reported on 277 studies which involved 536 children and adults (70% of the studies included persons between the ages of 1 and 18, and 37% also included persons older than 18), who received functional analyses of problem behaviors. Of these, 96 percent were able to yield an analysis of the controlling variables of the problem behavior. The specific functional analysis of individual problem behaviors is crucial to the successful intervention with those behaviors. “Large proportions of differentiated functional analyses showed behavioral maintenance through social-negative (34.2%) and social-positive reinforcement (35.4%). More specifically, 25.3% showed maintenance via attention and 10.1% via access to tangible items. Automatic reinforcement was implicated in 15.8% of cases.” (pages 166-167). (c) Eric Larsson, PhD, BCBA-D, The Lovaas Institute Midwest 23 Why is ABA Evidence-Based? 4/27/13 Self Injury Iwata and colleagues, in 1994, reported on the effective treatment of self-injurious behavior with 152 children, adolescents, and adults. In their sample, 39 were between the ages of 11 and 20, and 74 were 21 and older. The function of the self-injurious behavior could be identified in 95% of the persons, and in 100% of those cases an effective treatment could then be prescribed. “Results of the present study, in which single-subject designs were used to examine the functional properties of SIB in 152 individuals, indicated that social reinforcement was a determinant of SIB in over two thirds of the sample, whereas nonsocial (automatic) consequences seemed to account for about one fourth of the cases.” (page 234). The Evidence Base for Treatment Independent Panels Peer Review Long-Term and Group Outcome Studies RCTs Randomized Controlled Trials Non-Randomized Matched Trials Registries Comparison Data Meta-Analysis Cost-Effectiveness Analyses ABA Applied Behavior Analysis Within-Subject Experimental Studies (c) Eric Larsson, PhD, BCBA-D, The Lovaas Institute Midwest 24 Why is ABA Evidence-Based? 4/27/13 Independent Panels Independent National Reviews The APA Society for Clinical Child and Adolescent Psychology American Academy of Pediatrics The U.S. Agency for Health Care Research and Quality The National Institute of Mental Health National Research Council The State of California The State of New York The U.S. Surgeon General The Center for Disease Control (c) Eric Larsson, PhD, BCBA-D, The Lovaas Institute Midwest 25 Why is ABA Evidence-Based? 4/27/13 Division 53 of the American Psychological Association (the Society for Clinical Child and Adolescent Psychology) “Randomized controlled trials have demonstrated positive effects in both short-term and longer term studies. The evidence suggests that early intervention programs are indeed beneficial for children with autism, often improving developmental functioning and decreasing maladaptive behaviors and symptom severity at the level of group analysis.” “Lovaas’s treatment meet Chambless and colleague’s (Chambless et al., 1998; Chambless et al., 1996) criteria for ‘well-established”’ “Across all the studies we cited, improvements in language, communication, and IQ, and reduction in severity of autism symptoms indicate that the core symptoms of autism appear malleable in early childhood” Rogers & Vismara (2008) American Academy of Pediatrics “The effectiveness of ABA-based intervention in ASDs has been well documented through 5 decades of research by using singlesubject methodology and in controlled studies of comprehensive early intensive behavioral intervention programs in university and community settings.” “Children who receive early intensive behavioral treatment have been shown to make substantial, sustained gains in IQ, language, academic performance, and adaptive behavior as well as some measures of social behavior, and their outcomes have been significantly better than those of children in control groups.” Myers, Johnson, & the American Academy of Pediatrics Council on Children With Disabilities, (2007). (c) Eric Larsson, PhD, BCBA-D, The Lovaas Institute Midwest 26 Why is ABA Evidence-Based? 4/27/13 Hawaii Department of Health “Best Support: Intensive Behavioral Treatment was successful in three (3) studies, beating alternative treatments in two (2) of those, and beating a no-treatment control in one (1). Likewise, Intensive Communication Training was also successful in three (3) studies, beating alternative treatments in two (2) of those, and beating a no-treatment control in one (1) study.” “These results are quite promising in terms of effect size, although it should be noted that the outcome variables for these studies mainly involved reductions in the frequency of autistic behaviors or increases in social communication or other forms of social exchange (e.g., turn taking). None of these studies claimed that children were autism free following the intervention programs. Nevertheless, these findings represent an extraordinary improvement over the evidence base for interventions for autistic spectrum disorders in the previous Biennial Report. Is there a consensus? Forty-five such independent, meta-analysis, and peer reviews are available. Every review cites the obvious positive results of ABA and EIBI and accepts them as proven. The reviews are critical evaluations in many cases, other non-ABA treatments are assigned to categories such as “insufficient evidence,” “unproven,” or “potentially harmful.” (c) Eric Larsson, PhD, BCBA-D, The Lovaas Institute Midwest 27 Why is ABA Evidence-Based? 4/27/13 Cost Effectiveness Analyses - CDC “The mean medical expenditures for children with ASD were 6 times higher than those of the comparison group.” “Children with ASD and ID incurred expenditures 2.7 times higher than did children with ASD and no co-occurring condition.” Peacock, G, Amendah, D., Ouyand, L., & Grosse, S.D. (2012) Autism Spectrum Disorders and Health Care Expenditures: The Effects of CoOccurring Conditions. Journal of Developmental & Behavioral Pediatrics. 33, 2-8. Comparison Data (c) Eric Larsson, PhD, BCBA-D, The Lovaas Institute Midwest 28 Why is ABA Evidence-Based? 4/27/13 Comparison Data Lord & Schopler, 1989 What is the evidence for the outcomes without ABA “Health care utilization and costs are substantially higher for children and adolescents with ASDs” “mortality is increased as well.” “Cases of suicide in higher-functioning individuals have been reported.” American Academy of Pediatrics (2007) Howlin (2005) Liptak, Stuart, Auinger. (2006) Croen, Najjar, Ray, Lotspeich, Bernal (2006) Mandell, Cao, Ittenbach, Pinto-Martin. (2006) Shavelle, Strauss, Pickett (2001) Pickett, Paculdo, Shavell, Strauss (2006) (c) Eric Larsson, PhD, BCBA-D, The Lovaas Institute Midwest 29 Why is ABA Evidence-Based? 4/27/13 Other Medical Reviews “Recovery in children with ASD through behavioral and educational interventions seems possible in a significant minority of cases.” Helt, Kelley, Kinsbourne, Pandey, Boorstein, Herbert, & Fein (2008). (The authors are psychologists and pediatricians at the University of Connecticut, Queen’s University, the New School, Children’s Hospital of Philadelphia, and Massachusetts General Hospital). “The weight of currently available scientific evidence, however, indicates that ABA should be viewed as the optimal, comprehensive treatment approach in young children with ASD.” Barbaresi, Katusic, & Voigt (2006). (The authors are pediatricians at the Mayo Clinic and at Harvard University). Meta Analyses (c) Eric Larsson, PhD, BCBA-D, The Lovaas Institute Midwest 30 Why is ABA Evidence-Based? 4/27/13 Meta Analyses of Magnitude of Effect and Dosage Effects “Results suggested that long-term, comprehensive ABA intervention leads to (positive) medium to large effects in terms of intellectual functioning, language development, acquisition of daily living skills and social functioning in children with autism.” “Although favorable effects were apparent across all outcomes, language-related outcomes (IQ, receptive and expressive language, communication) were superior to non-verbal IQ, social functioning and daily living skills, with effect sizes approaching 1.5 for receptive and expressive language and communication skills.” “Dose-dependant effect sizes were apparent by levels of total treatment hours for language and adaptation composite scores.” Virues-Ortega, (2010) So what is the controversy? In none of the reviews do the authors systematically refute the published evidence for ABA treatments of autism. The most “negative” conclusions that are offered are: 1) ABA does not cure all children of autism 2) ABA is not the only established treatment, nor is it clearly the best treatment 3) There are not well-established means to identify the best candidates for treatment These conclusions can be drawn about any medical treatment that already enjoys full coverage, they should not be cause for denying coverage for ABA. (c) Eric Larsson, PhD, BCBA-D, The Lovaas Institute Midwest 31 Why is ABA Evidence-Based? 4/27/13 Reports cited as Negative “There is little question now that early intensive behavioral intervention is highly effective for some children. However, gains are not universal, and some children make only modest progress while others show little or no change, sometimes after extremely lengthy periods in treatment.” Howlin, Magiati, & Charman, (2009). (The authors are professors at the Institute of Psychiatry, King’s College (London, UK) and University College, London, Institute of Child Health). Agency for Healthcare Research and Quality (AHRQ) Comparative Effectiveness Review “Evidence supports early intensive behavioral and developmental intervention, including the University of California, Los Angeles (UCLA)/Lovaas model and Early Start Denver Model (ESDM) for improving cognitive performance, language skills, and adaptive behavior in some groups of children.” “Evidence suggests that interventions focusing on providing parent training and cognitive behavioral therapy (CBT) for bolstering social skills and managing challenging behaviors may be useful for children with ASDs to improve social communication, language use, and potentially, symptom severity.” Warren, et al. (2011) (c) Eric Larsson, PhD, BCBA-D, The Lovaas Institute Midwest 32 Why is ABA Evidence-Based? 4/27/13 AHRQ “Negative” Qualifiers “All of these studies need to be replicated, and specific focus is needed to characterize which children are most likely to benefit.” “Information is lacking on modifiers of effectiveness, generalization of effects outside the treatment context, components of multicomponent therapies that drive effectiveness, and predictors of treatment success.” AHRQ Review of Alternatives “No current medical interventions demonstrate clear benefit for social or communication symptoms in ASDs.” “Little evidence is available to assess other behavioral interventions, allied health therapies, or complementary and alternative medicine.” (c) Eric Larsson, PhD, BCBA-D, The Lovaas Institute Midwest 33 Why is ABA Evidence-Based? 4/27/13 What about the AHRQ? The AHRQ report reached these positive conclusions about ABA and EIBI despite: excluding a large number of studies Sample size less than 10 excluding all studies published prior to 2000 Already covered elsewhere ADOS Bias toward RCTs – Randomized Controlled Trials Not experts in ABA for autism, so analysis is lacking Yet the AHRQ report still found 78 studies of behavioral interventions, which included 34 studies of EIBI, that met their criteria for inclusion. The report of “strength of evidence” is not the same as “strength of effect.” Applied Behavior Analysis Answers the Questions Raised by the AHRQ Addresses the heterogeneous diagnosis of autism The outcomes of ABA research are the objective improvements in the behavior of individual children Analyzes the individual components of treatment, and the individual responses to treatment Addresses the needs for generalization and maintenance The research is not composed of uncontrolled case studies They are powerful within-subject controlled experiments Provides a model for clinical practice (c) Eric Larsson, PhD, BCBA-D, The Lovaas Institute Midwest 34 Why is ABA Evidence-Based? 4/27/13 Other Standards for Evidence Smith, 2012: Single-Case Experimental Designs: A Systematic Review of Published Research and Current Standards Chambless: 1998: Defining empirically supported therapies. Kazdin & Weisz, 2010: Evidence based psychotherapies for children and adolescents. Evidence Based Practices in Within Subject Controlled Experiments Reichow, Volkmar, Cicchetti, (2008) (c) Eric Larsson, PhD, BCBA-D, The Lovaas Institute Midwest 35 Why is ABA Evidence-Based? 4/27/13 Evidence Based Practices in Within Subject Controlled Experiments Reichow, Volkmar, Cicchetti, (2008) Peer Reviews (c) Eric Larsson, PhD, BCBA-D, The Lovaas Institute Midwest 36 Why is ABA Evidence-Based? 4/27/13 ABA Effects on Social Skills “Within the last 8 years, 66 studies with strong or acceptable methodological rigor have been conducted and published.” “These studies have been conducted using over 500 participants, and have evaluated interventions with different delivery agents, methods, target skills, and settings.” “Collectively, the results of this synthesis show there is much supporting evidence for the treatment of social deficits in autism.” Reichow, & Volkmar, (2010). ABA Effects on Challenging Behavior “The available intervention technology is reasonably effective at reducing problem behaviors performed by people with developmental disabilities, including autism.” “Reductions of 80% or greater were reported in half to two thirds of the comparisons.” “Reductions of 90% or greater were reported for all classes of problem behavior, and with individuals with all diagnostic labels.” Horner, Carr, Strain, Todd, & Reed, (2002) (c) Eric Larsson, PhD, BCBA-D, The Lovaas Institute Midwest 37 Why is ABA Evidence-Based? 4/27/13 National Autism Center (2009) Standards on ABA-researched procedures Established Antecedent Package Behavioral Package Comprehensive Behavioral Treatment for Young Children Joint Attention Intervention Modeling Naturalistic Teaching Strategies Peer Training Package Pivotal Response Treatment Schedules Self-management Story-based Intervention Package Emerging Unestablished Ineffective/Harmful What about Other Treatments? The RCT, Randomized Controlled Trial is not well suited to uncover many of the specific treatments that help the individual children who are under the Heterogeneous umbrella of autism. Instead it is single subject laboratory research that can detect promising therapies. (c) Eric Larsson, PhD, BCBA-D, The Lovaas Institute Midwest 38 Why is ABA Evidence-Based? 4/27/13 What evidence are the Policy Makers and Funders looking for? They want a system of cost-effective management of autism services In addition to the money that they pay out for coverage, How does the health plan control their own bureaucratic costs? Effective cost control through accountability for results Instead of managing the process, let’s manage the outcomes. (c) Eric Larsson, PhD, BCBA-D, The Lovaas Institute Midwest 39 Why is ABA Evidence-Based? 4/27/13 Cost effectiveness through Assessment of Value Conform with Medical Necessity Guidelines for Rehabilitative Treatment Identify evidence-based treatment models. Identify evidence-based service-delivery models. Certify the provider organizations who maximize value. Prescribe the optimal form of treatment, intensity, and service delivery for each child’s prognosis at intake Individual behavioral measures Complicating conditions Parent involvement Service capacity Prescribe the continuation of care based upon each individual child’s responsiveness to treatment Socially Significant Independence Discharge Objectives Receptive Language, the child will understand and comply with instructions. ____ Generalized compliance. ____ Distal compliance. Expressive Language, the child will use functional language with care-providers and natural peers. ____ Intelligible speech. ____ Functional requests. Pro-social skills, the child will interact appropriately with natural peers. ____ Generalized imitation. ____ Cooperative play with adult. ____ Cooperative play with a typical age-peer. ____ Small-group attending. ____ Maintain two mutual friendships. Community Living, the child will safely use the community. ____ Walk with adult. ____ Parent Mastery. ____ Participate in community. Self-Care, the child will attend to personal needs independently. ____ Appropriate nutrition. ____ Appropriate sleep. ____ Independent toileting. Self-control, the child will control severely health-threatening behavior at all times. ____ Waiting. ____ Self-control of health-threatening behavior ____ Self-control of stereotyped offensive behavior ____ Self-control of physical aggression. ____ Self-control of property destruction. ____ Self-control of bolting behavior (c) Eric Larsson, PhD, BCBA-D, The Lovaas Institute Midwest 40 Why is ABA Evidence-Based? 4/27/13 Socially Significant Long-Term Service Objectives Accepted standard practice process measures in supported employment Competitive work Averages at least 20 hr per week for each pay period Integrated work setting has a work group of not more than 8 individuals with handicaps, and has regular contact with typical co-workers Ongoing support services provide continuous or periodic job skill training provided at least twice monthly at the job site Implicit outcome measures in supported employment Movement from the more restrictive (sheltered workshop) to a setting with more independence (work enclave), due to case management. More accurate placement into services (accurately matching recipients to services) Cost-benefit of job retention and increased earnings, as they offset the cost of the service. Social Validity of quality of life and reduction of family anxiety. Quality of implementation of the specialized skills of the practitioner. Accessibility of services – adequate network, and adequate professional training system. Payment Reform Payment systems should reinforce best practices and reduce incentives for abuse. ABA offers objective criteria for decision making in human services. (c) Eric Larsson, PhD, BCBA-D, The Lovaas Institute Midwest 41 Why is ABA Evidence-Based? 4/27/13 Ivar Lovaas (2003) “Providers of ABA services who do not report treatment outcome should take notice of this problem of falling into the same trap of those service providers who preceded us, of misleading parents and short-changing their children. “Today the contingencies are different for the majority of providers who are reinforced by charging fees for services with minimal or no outcome data and peer review. We may be drifting off the criterion of data-based treatment procedures and, if we do, the future may look as bleak for us as for the Freudians. “I shudder at the thought of someone receiving a grant to assess long-term outcome from ABA providers. Will the parents of these children feel that they have been deceived? “Now that we are being accepted as fellow citizens and providing what is considered the ‘treatment of choice,’ we need to be concerned about the truthfulness of what treatment we offer.” Opening the road to an enlightened future. In K.S. Budd & T. Stokes (Eds.), A small matter of proof: The legacy of Donald M. Baer (pp. 225-332). Reno NV: Context Press. (c) Eric Larsson, PhD, BCBA-D, The Lovaas Institute Midwest 42








© Copyright 2026