
Objectives: 4/4/2013 Neonatal Nutrition—Our experience with the NYS Perinatal Quality
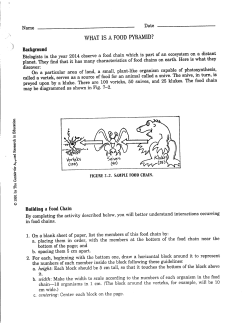
4/4/2013 Neonatal Nutrition—Our experience with the NYS Perinatal Quality Collaborative Anne Marie Reynolds, MD, MPH y , , SUNY at Buffalo School of Medicine Assistant Professor of Pediatrics Division of Neonatology Who is involved? • 18 New York State Regional Perinatal Centers • NYS Department of Health • NICHQ—National Initiative for Children’s Healthcare Quality lh Q li Objectives: • Highlight the difference between research and quality improvement • Define growth for the purposes of this project and factors that affect growth and factors that affect growth • Explain a PDSA cycle • Explore the changes made in the NICU nutrition protocol as a result of the NYS Perinatal Quality Collaborative What is the Difference? Research vs. Quality Improvement • Quality Improvement: an effort to apply current best knowledge • Research: an effort to find new knowledge by testing a potentially better practice NYSPQC Neonatology Intervention • Goal – Optimize early enteral nutrition in newborns ≤ 30 6/7 weeks gestational age • Aim – In one year, reduce statewide the percentage of newborns ≤ 30 6/7 weeks gestational age that are discharged from the NICU below the tenth percentile Why Discharge Weight Percentile? • Adamkin, Neoreviews 2006 – goal of nutrition management in VLBW infants is the achievement of postnatal growth at a rate that approximates the intrauterine growth of a normal fetus at the same postconceptional age (AAP Committee on Nutrition) – Although non‐nutritional factors (morbidities) are involved in the slow Although non nutritional factors (morbidities) are involved in the slow growth of VLBW infants, nutrient intakes are low and critical in explaining their poor growth…early growth deficits have long‐lasting effects, including short stature and poor neurodevelopmental outcomes – Nutrition management of VLBW infants is marked by a lack of uniformity from one NICU to the next as well as within individual practices • Diversity of practice thrives where there is uncertainty 1 4/4/2013 Extra Uterine Growth Failure Why Discharge Weight Percentile? • Clark, Thomas, Peabody, Pediatrics 2003 – the prevalence of growth restriction (<10th percentile) at discharge (<34 weeks to 41 weeks CGA) was 28% for weight, 34% for length and 16% f h d i for head circumference f • Lemons, et al. NICHD Neonatal Research Network, Pediatrics 2001 – 97% of all surviving VLBW and 99% ELBW infants had weights less than the 10th percentile at 36 weeks corrected GA Ehrenkranz, et al, Pediatrics 1999 PDSA= Plan, Do, Study, Act Learning Session 1 • Overview of Project – What do we know about enteral feeding? – What can we readily measure? • NYS DOH SPDS NICU Module NYS DOH SPDS NICU Module – What can we infer from our data? – Describe current process and outcome variation in NYS RPCs 2 4/4/2013 In 1 year, decrease the number of AIM Statement: < 31 week GA babies discharged at less than the 10th percentile for weight from our NICU. 3 4/4/2013 Where are we starting and how do we compare with other NYS RPCs? 4 4/4/2013 2009 Box and Whisker Plot Change in z‐score o o adjacent line <- outside values <- upper adjacent value whiskers <- 75th p percentile (upper ( pp hinge) g ) box <- median <- 25th percentile (lower hinge) whiskers adjacent line <- lower adjacent value o <- outside value 2009 2009 5 4/4/2013 • Recognize that there is a gap between care as it is and optimal care that could be provided for your patients and their families • Identify a set of goals that your NICU would like to Id if f l h NICU ld lik accomplish • Understand and implement improvement techniques that can change the nature of care delivery in your NICU setting 6 4/4/2013 7 4/4/2013 We were sent out to create change… PDSA= Plan, Do, Study, Act Action Period 1 Who is ahead of us? • Based on 2009 data, we had 19% of babies born at GA < 32 weeks discharged less than 10th percentile for weight…not too bad! • What were we doing that was working? –? – Compared our practices to other centers who were also doing well – Identified areas for improvement WCHOB • Trophic feeding • Protocol for stopping feeds related to “intolerance” Stony Brook North Shore University Hospital (LIJ) What do they have that we don’t? • North Shore – 13 page feeding protocol – Specific protocol for assessing tolerance of feeding • Stony Brook St B k – Protocol for evaluating residuals – Start at 24 kcal preterm formula Consistency? 8 4/4/2013 9 4/4/2013 Ideas for first action period • Standardize trophic feeding protocol • Standardize protocol for stopping feeds based on strict definitions of feeding intolerance • Standardize protocol for using high protein S d di lf i hi h i formula • Consider starting with 24 kcal formula Data From January 2009 to March 2011 Related to Trophic Feeding at WCHOB • Are we using Trophic Feeding? • Definition of Trophic feeds: MBM or PF 20 kcal/oz at volumes of ≤20 ml/kg BW for ≥3 days days • Does Trophic Feeding… – Impact on growth • Our goal is to decrease the number of infants discharged below the 10th percentile – Affect the Incidence of NEC Action Period 1 Data Trophic Feeding in Infants Born at < 30 weeks GA, Surviving to Discharge Trophic Feeds (n= 61) No Trophic Feeds (n = 106) Average GA (weeks) 26 3/7 27 5/7 Average LOS (days) 101.4 82.5 Average Discharge Weight Percentile 29.1 25.3 Rate of NEC 19.7% 16.9% Overall rate of Trophic feeding of 36.5% What Does the Literature Say? Evidence for trophic feeding • Recent study compared gut stimulation protocol (constant feed volume for 10 days prior to advancement) with a traditional enteral feeding protocol that used standard enteral feeding protocol that used standard rates of volume advancement. • Study closed early due to incidence of NEC in group randomized to early advancement was 10% vs. 1.4% in the gut stimulation protocol • “Gut stimulation protocols are beneficial to VLBW infants and should be routine in all NICUs.” • “There There are few contraindications to using are few contraindications to using these protocols, even in infants weighing 500 to 600 g who have indwelling umbilical catheters and are receiving assisted ventilation.” Adamkin, NeoReviews 2006 Adamkin, NeoReviews 2006 10 4/4/2013 Evidence for trophic feeding Cochrane Review • Significant increases in plasma concentrations of enteroglucagon, gastrin and gastric‐ inhibiting polypeptide are seen in preterm infants after milk feedings of as little as 12 infants after milk feedings of as little as 12 mL/kg/day. (Trophic Hormones) • Bombell and McGuire, 2009 • Babies who received trophic feeding reached full enteral feeds earlier, had less mortality and shorter hospital stays. – Most Most participants were AGA VLBW infants participants were AGA VLBW infants – Generally started within the first 3 days after birth and continued for varying duration (generally between 7‐ 10 days after birth) – 12‐24 ml/kg/d – EBM or formula – Controls not fed for at least one week after birth Lucas 1998 Cochrane Review • No difference in the rate of NEC What Was Going on in NYS RPCs? 11 4/4/2013 12 4/4/2013 Where to go from here…. PDSA= Plan, Do, Study, Act Action Period 2 Activity NEC in our Unit related to Trophic feeding Jan ‘09 to March ‘11 • Presented a modification to our Trophic Feeding Protocol to faculty, fellows and NP/PAs on 6/13/11. • Monitored adherence to the protocol over a 4 Monitored adherence to the protocol over a 4 month period. • 3 babies <31 weeks died of NEC‐‐never received trophic feeds (step wise advance right away) • 1 baby <31 weeks died of NEC—trophic feed only 3 days 3 days • In surviving infants: – Trophic feeding • NEC in 8/61 or 13.1%, surgical in only 1 case (rate of 12.5%) – No trophic feeding • NEC in 16/106 or 15%, surgical in 4 cases (rate of 25%) 13 4/4/2013 Action Period 2 Data • 59 babies admitted < 1500 gms during this 4 month period • 8 deaths (86.5% survival) (1 trisomy 13, 2 with congenital anomalies died shortly after birth) • 24 babies ≤ 1000 gms g – 45.8% in compliance with protocol • • • • • • Action Period 2 Data • 35 babies 1001 gms ‐ 1500 gms – 60% in compliance with protocol Average day trophic feeds started = 2 (0‐7) 1 death prior to assessment Average days of trophic feeding = 3.6 (0‐9) Lack of compliance was due to early advancement 2 babies with early advancement had non surgical NEC 1 baby with trophic feeding course of 9 days (formula) had NEC—colonic • There was no surgical NEC during this period Action Period 2 Lessons Learned • Adherence to Protocol is not going to be 100%, but can be better than current – There is more trophic feeding going on than prior to the protocol modification (36.5% based on last action period data) • Based on early advancement in our NICU, there seems to be an increasing comfort with “early” feeding – Maybe unwarranted based on NEC with early advancement • More education is needed Median Newborn Birth (BWT) & Discharge (DWT) Weights in Relation to Fenton Growth Percentiles for All Regional Perinatal Centers (January ‐ September 2011) 7000 6000 Growth Data from 2011… 5000 Weight in n Grams • • • • • • Average day trophic feeds started = 4.5 (0‐12) 5 deaths prior to assessment (66.7% compliance if excluded) Average days of trophic feeding = 4.3 (0‐11) Lack of compliance was due to early advancement 2 babies with early advancement had non‐surgical NEC No babies who received trophic feeds for 4 days or longer had NEC 4000 3000 2000 1000 0 N= 4 3 3 8 10 14 17 47 126 153 158 137 112 71 63 33 36 19 17 19 10 7 1 3 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 Weeks Gestational Age Fenton 10%‐90% Fenton 50% RPC Median BWT RPC Median DWT 14 4/4/2013 Median Newborn Birth (BWT) & Discharge (DWT) Weights in Relation to Fenton Growth Percentiles for Women's and Children's Hospital of Buffalo RPC (January ‐ September 2011) 7000 6000 Weight in n Grams 5000 4000 3000 2000 1000 0 N= 6 9 11 10 9 7 5 2 2 1 1 2 2 1 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 Weeks Gestational Age Fenton 10%‐90% Fenton 50% RPC Median BWT RPC Median DWT Change from BWT to DWT BWT Percentile DWT Percentile Change from BWT to DWT BWT Percentile DWT Percentile -0.71 47 22 -0.69 55 28 15 4/4/2013 To What Do We Credit our Success? • Faculty members with specific interest in nutrition • Dietician rounding as part of the NICU team Dietician rounding as part of the NICU team • Certified Lactation Specialist • Good system of communication • State of the Art Formula Lab for compounding formula and human milk Next steps • Resurvey Neonatologists at the NYS RPCs • Continue with PDSA cycles – Work on feeding intolerance protocol Questions? 16







© Copyright 2026