
Minimum (floor) price Australian National Preventative Health Agency GPO Box 462
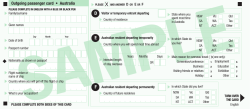
SUBMISSION COVER SHEET Please complete and submit this form with your submission to: Email: [email protected] Post: Minimum (floor) price Australian National Preventative Health Agency GPO Box 462 Canberra ACT 2601 Phone: (02) 6289 2879 Organisation or individual (this will appear on our website) Distilled Spirits Industry Council of Australia Inc (DSICA) Contact person (the name of the person wishing to receive confirmation of submission and future updates) Mr Gordon Broderick Email address: [email protected] Phone: (03) 9696 4466 Mobile (optional): Physical address 1st Floor, 117 Ferrars Street Suburb/City South Melbourne Postal address PO Box 1098 Suburb/City South Melbourne State Vic Postcode 3205 State Vic Postcode 3205 Please note: • For submissions made by individuals, all personal details other than your name and the State or Territory in which you reside will be removed from your submission before it is published on the ANPHA website. • If possible, it is preferable that all submissions are provided as public documents; however, ANPHA can accept confidential submissions if requested (for example: submissions containing sensitive information of a personal or commercially confidential nature). If you wish to make a confidential submission please contact ANPHA prior to sending any material and mark the submission as confidential. • Submissions will be placed on the ANPHA website shortly after receipt, unless ANPHA has been previously informed about material supplied in confidence. Submissions will remain on the ANPHA website indefinitely. Distilled Spirits Industry Council of Australia Inc. Submission to the Australian National Preventative Health Agency Exploring the Public Interest Case for a Minimum (Floor) Price for Alcohol Draft Report December 2012 Contact Phone Fax Email Web Mr Gordon Broderick Executive Director 03 9696 4466 03 9696 6648 [email protected] www.dsica.com.au “Free The Spirit” Who is DSICA? The Distilled Spirits Industry Council of Australia Inc (DSICA) is the peak body representing the interests of distilled spirit manufacturers and importers in Australia. DSICA was formed in 1982, and the current member companies are: • Bacardi Lion Pty Ltd; • Beam Global Australia Pty Ltd; • Brown-Forman Australia; • Bundaberg Distilling Company Pty Ltd; • Diageo Australia Limited; • Mast-Jägermeister AG; • Moët-Hennessy Australia Pty Ltd; • Rémy Cointreau International Pte Ltd; • Suntory (Australia) Pty Ltd; and • William Grant & Sons International Ltd. DSICA’s goals are: • to create an informed political and social environment that recognises the benefits of moderate alcohol intake and to provide opportunities for balanced community discussion on alcohol issues; and • to ensure public alcohol policies are soundly and objectively formed, that they include alcohol industry input, that they are based on the latest national and international scientific research and that they do not unfairly disadvantage the spirits sector. DSICA’s members are committed to: • responsible marketing and promotion of distilled spirits; • supporting social programs aimed at reducing the harm associated with the excessive or inappropriate consumption of alcohol; • supporting the current co-regulatory regime for alcohol advertising; and • making a significant contribution to Australian industry through primary production, manufacturing, distribution and sales activities. i DSICA Submission to the Australian National Preventative Health Agency “Free the Spirit” Contents Who is DSICA? i Executive summary iii 1 Structure and purpose of this submission 6 2 DSICA’s position on minimum floor pricing 8 3 Alcohol consumption in Australia 3.1 3.2 3.3 3.4 Australia’s per capita consumption of alcohol The Australian liquor industry Cost of alcohol-related harms Population approaches versus targeted approaches for addressing harmful consumption of alcohol 10 10 11 13 16 4 Minimum (floor) pricing 20 4.1 4.2 4.2.1 20 21 4.2.2 4.3 4.4 Canada Scotland Findings from the European Commission on the legality of minimum pricing Additional findings concerning the Sheffield Alcohol Policy Model England and Wales Conclusion 22 23 25 26 5 Conclusion 28 A References 30 DSICA Submission to the Australian National Preventative Health Agency ii “Free The Spirit” Executive summary As the peak body representing the interests of Australian distilled spirit manufacturers and importers, DSICA is committed to supporting strategies that can be shown to reduce the uptake of alcohol use by underage Australians, and also reduce the levels of harmful drinking amongst adult Australians. To this end, there is a need to seek evidence-based, targeted measures which reduce the levels of excessive alcohol consumption in Australia and do not unfairly burden or penalise the majority of Australian consumers who drink in moderation. Recognising this, DSICA does not believe that a minimum (floor) price for alcohol is either an appropriate or an evidence-based approach to meet the Australian National Preventative Health Agency’s (ANPHA’s) objectives to ‘discourage harmful consumption and promote safer consumption (emphasis added).1 ANPHA accurately identified this in the Draft Report Exploring the Public Interest Case for a Minimum (Floor) Price on Alcohol (the Draft Report), noting that: Because Australia’s alcohol distribution and retail systems are fully private…a regulated minimum price increase (as distinct from a tax)…significantly reduces the available public benefits which could be used to further reduce or treat alcohol harm or be redistributed by government for other purposes…a minimum (floor) price for alcohol should not be introduced nationally at this time.2 DSICA strongly supports ANPHA’s recommendation and notes that it recognises the latest international evidence relating to the (lack of) demonstrated effectiveness of minimum (floor) pricing. This is, in large part, due to: • the unique regulatory environments in which minimum (floor) pricing regimes operate internationally, limiting the appropriateness of any conclusions or findings which may be applied in the Australian context; and • the lack of support for findings drawn from the University of Sheffield’s School of Health and Related Research’s alcohol policy model, which have been critiqued by Duffy and Snowdon due to the application of false and misleading assumptions concerning alcohol consumption and drinking behaviours.3 DSICA further notes that any proposal to introduce a minimum (floor) price on the grounds of high levels of risky and high-risk drinking behaviours is unfounded. Research demonstrates that Australia does not have a high level of per capita alcohol consumption compared with comparable Organisation for Economic Co-Operation and Development (OECD) countries. Levels of risky and high-risk drinking amongst young people, and several adult age group cohorts have, in fact, generally been trending downwards over the last decade, on both a shortterm and a long-term basis. Any perception of an increasing ‘epidemic’ of high-risk drinking amongst young people, or all adult age groups, is not supported by the best available evidence. The case for the introduction of a minimum price to reverse increasing levels of alcohol-related harm amongst young people, and other age groups, cannot be made. To this end, it is noted that the overwhelming majority of consumers drink in moderation, creating no problems for themselves or society as a whole. Reports indicating that the cost of alcohol-related harms are anywhere in the vicinity of $15.3 to $36 billion are poorly researched, 1 Australian National Preventative Health Agency, Exploring the Public Interest Case for a Minimum (Floor) Price for Alcohol: Issues Paper (Australian Government, 2012) [1]. 2 Australian National Preventative Health Agency, Exploring the Public Interest case for a Minimum (Floor) Price for Alcohol: Draft Report (Australian Government, 2012) 9. 3 John Duffy and Christopher Snowdon, The Minimal Evidence for Minimum Pricing: The fatal flaws in the Sheffield Alcohol Policy Model (Adam Smith Institute 2012) 5. 3 DSICA Submission to the Australian National Preventative Health Agency “Free the Spirit” with independent economic analysis confirming that they are not reliable tools to be used in evidence-based policymaking. DSICA strongly opposes any research which relies on the cost of illness and cost of harm methodologies used by Collins and Lapsley and Laslett et. al.,4 as these research findings fail to demonstrate any evidence of best practice, internationally recognised approaches to economic cost/benefit analyses. Finally, DSICA acknowledges that in the intervening period between preparation of the Draft Report and this submission, there have been marked developments in relation to the minimum (floor) pricing debate in Scotland, England and Wales. Most notably, the European Commission (EC) has found that a proposed Minimum Unit Price (MUP) constitutes a ‘disproportionate’ response to Scotland’s aim of reducing alcohol consumption levels, and instead considers the application of excise duties to be a more appropriate and suitable option which will not result in adverse effects on competition and trade.5 The Scottish experience signals a strong warning to Australian policymakers considering the introduction of a minimum (floor) price – and reiterates both ANPHA and DSICA’s view that a minimum floor price is not an appropriate measure to reduce alcohol-related harms in Australia. DSICA remains committed to supporting evidence-based interventions aimed at reducing the harm associated with the excessive or inappropriate consumption of alcohol, however does not contend that the introduction of a single minimum (floor) price – as seen (or proposed) in Canada, Scotland, England and Wales is an appropriate or effective measure to reduce alcoholrelated harms. The Australia’s future tax system report (the Henry Review) identified the provision of a wholly volumetric alcohol taxation regime with a single rate for all alcohol beverages as a best-practice approach to alcohol taxation (as it creates a link between the amount of excise taxation paid and the product’s alcohol content), but did not recommend the introduction of a minimum (floor) price.6 DSICA’s long-term vision for alcohol taxation in Australia is in accordance with that described in the Henry Review. To achieve this vision, reform of the ad valorem Wine Equalisation Tax (WET) towards a volumetric regime is urgently required, and would effectively create a minimum (floor) price for all alcohol beverages in Australia. DSICA contends that such an approach is highly preferential to the introduction of a statutory pricing mechanism and is to be strongly supported. 4 See David Collins and Helen Lapsley, The costs of tobacco, alcohol and illicit drug abuse to Australian society in 2004/05 (Australian Government, 2008) and Anne-Marie Laslett et. al., The Range and Magnitude of Alcohol’s Harm to Others (Alcohol Education and Rehabilitation Foundation, 2010). 5 Communication from the Commission – SG(2012) D/52513; Directive 98/34/EC; Notification 2012/0394/UK. 6 Ken Henry et. al., Australia’s future tax system: Report to the Treasurer (Part Two – Detailed Analysis) (Australian Government, 2009) 442. DSICA Submission to the Australian National Preventative Health Agency 4 “Free The Spirit” 5 DSICA Submission to the Australian National Preventative Health Agency “Free the Spirit” 1 Structure and purpose of this submission DSICA lodged a substantive and detailed response to the ANPHA Issues Paper Exploring the Public Interest Case for a Minimum (Floor) Price on Alcohol (the Issues Paper) in August 2012. Each of the points made and issues discussed in that submission remain representative of DSICA’s views on minimum (floor) pricing and preferred, alternative methods to discourage harmful alcohol consumption and promote safer consumption behaviours. This submission responds to a number of key issues raised in the latter Draft Report and seeks to provide further evidence and clarification in relation to: • Australia’s comparative per capita consumption of alcohol; • contribution of the Australian liquor industry to total taxation revenue collections; • the cost of alcohol-related harms; • population wide versus targeted interventions; and • latest developments and research relating to the effectiveness of minimum (floor) pricing measures in Canada, Scotland, England and Wales. This submission is not designed to supersede DSICA’s earlier submission in respect of the Issues Paper, but rather supplement it and provide evidence-based insights to clarify a number of points made in the Draft Report. DSICA Submission to the Australian National Preventative Health Agency 6 “Free The Spirit” 7 DSICA Submission to the Australian National Preventative Health Agency “Free the Spirit” 2 DSICA’s position on minimum floor pricing DSICA congratulates ANPHA on its collaborative approach taken in preparing the Draft Report and for the thorough, evidence-based and well-researched manner in which its findings are presented. DSICA strongly supports ANPHA’s findings that: Because Australia’s alcohol distribution and retail systems are fully private…a regulated minimum price increase (as distinct from a tax)…significantly reduces the available public benefits which could be used to further reduce or treat alcohol harm or be redistributed by government for other purposes…a minimum (floor) price for alcohol should not be introduced nationally at this time;7 and …the current WET as an ad valorem tax does not target alcohol content effectively. Preferential treatment of wine, particularly at the lower value end, favours production of cheaper wines and such an arrangement may well be contributing to social and health harms…based on public health considerations…the current operation of the Wine Equalisation Tax is of concern and requires reappraisal.8 DSICA contends that these findings are sound and reflective of the complexities in Australia’s alcohol taxation regime which fails to achieve either desirable or optimal health, social policy or government revenue outcomes. A key failing of the Australian alcohol taxation system, as identified in the Draft Report, is the WET. Rather than introducing a minimum (floor) price, there is a need to reform the WET to a volumetric taxation regime which creates a correlation between the amount of tax paid and the product’s alcohol content to encourage responsible consumption decisions. Like ANPHA, DSICA does not consider the introduction of a minimum (floor) price to be an effective means of reducing harmful consumption behaviours. DSICA’s earlier submission to ANPHA detailed a number of reasons as to why a minimum (floor) price is not an appropriate population-based measure to discourage harmful alcohol consumption and promote safer consumption, including the fact that it will: • adversely affect sensible, moderate drinkers; • adversely affect low income individuals and households; • be inconsistent with Australia’s international trade obligations; • lead to windfall profits in the retail supply chain; and • produce a wide range of unintended consequences, including potential violation(s) of international trade obligations and additional costs to businesses. Further to this, there is no basis for a public interest case for introducing a minimum (floor) price in Australia due to the: • lack of a detailed analysis of the current situation with respect to drinking patterns and harms; • lack of an in-depth analysis of the relative merit of differing strategies for addressing harms; 77 8 Australian National Preventative Health Agency, above n 2, 9. Ibid. DSICA Submission to the Australian National Preventative Health Agency 8 “Free The Spirit” • absence of compelling research evidence that identifies the harms that will be best addressed through the fiscal mechanism being promoted; • lack of any compelling evidence that the preferred approach actually reduces harms in other countries of direct relevance to Australia; • absence of any evidence that the preferred approach is effective, robust, exportable and will not lead to unintended consequences; • lack of any detailed advice that such an approach is not inconsistent with Australia’s international trade obligations; • failure to commit to the development of, and provide public access to, a comprehensive econometric model of the alcohol market in Australia to forecast the likely impact of such an approach; and • lack of any credible comparative analysis of the potential merits of alternative models, such as the phased volumetric WET reform approach proposed by DSICA in its earlier response. DSICA acknowledges that a minimum price was not supported by the Henry Review, which instead recommended a single volumetric tax for all alcohol products.9 DSICA strongly supports this recommendation, and contends that the introduction of a wholly volumetric alcohol taxation regime, initially through reform of the ad valorem WET, would create an effective minimum (floor) price for all alcohol beverages, therefore removing the need to introduce a statutory minimum pricing mechanism. Such an approach is DSICA’s preferred alternative to a minimum floor price, and may be pursued using DSICA’s detailed reform proposal outlined in Appendix B to its earlier submission. Key point The existing Australian alcohol taxation regime is incoherent, riddled with anomalies and fails to achieve desirable economic, health and social policy outcomes. DSICA strongly supports ANPHA’s recommendation that a minimum (floor) price is not an appropriate measure for introduction into the Australian alcohol taxation system, and contends that it will be ineffective in reducing the incidence of harmful consumption behaviours. DSICA strongly supports the introduction of a wholly volumetric alcohol taxation regime, initially through reform of the ad valorem WET. A wholly volumetric alcohol taxation regime would create an effective minimum (floor) price for all alcohol beverages, therefore removing the need to introduce a statutory minimum pricing mechanism. 9 Henry, above n 6, 442. 9 DSICA Submission to the Australian National Preventative Health Agency “Free the Spirit” 3 Alcohol consumption in Australia DSICA contends that there is a need to understand the dynamics of the Australian alcohol market and long-term trends in alcohol consumption to develop sound, evidence-based policies. DSICA is supportive of the breadth of research ANPHA has drawn upon in preparing the Draft Report, however seeks to clarify and enhance the evidence base used in relation to matters concerning: • Australia’s per capita consumption of alcohol; • the Australian liquor industry; • the cost of alcohol-related harms; and • population approaches versus targeted approaches for addressing harmful consumption of alcohol. Each of these issues are discussed in turn. 3.1 Australia’s per capita consumption of alcohol The Draft Report states that: In 2010-11, Australia’s apparent per capita consumption of pure alcohol was 10 litres. While this represents a decrease compared to previous years, Australia’s annual per capita consumption is still considered high by world standards.10 Although there is a common perception that Australia is a nation of heavy drinkers compared with other countries, adult per capita consumption of alcohol in comparable developed countries is higher than in Australia. A comparison between the OECD countries for which per capita consumption data is available (see Figure 3-1) reveals that Australia ranked only 12th out of a total of 29 countries in 2009,11 strongly suggesting that Australia’s per capita consumption is not particularly high. 10 Australian National Preventative Health Agency, above n 2, [1]. Organisation for Economic Co-Operation and Development, Non-Medical Determinants of Health: Alcohol Consumption (Organisation for Economic Co-Operation and Development, 2009). Note that the 2009 OECD data has been revised throughout the year as new information has been made available. 11 DSICA Submission to the Australian National Preventative Health Agency 10 “Free The Spirit” Figure 3-1: Australia’s comparative alcohol consumption (2009) AUSTRALIA DOES NOT HAVE A HIGH LEVEL OF PER CAPITA ALCOHOL CONSUMPTION COMPARED WITH OTHER OECD COUNTRIES Ranking Country LPAs per capita Ranking Country 1 Luxembourg 15.3 11 Slovenia 10.5 2 France 12.3 12 Australia 10.3 3 Austria 12.2 4 Czech Republic 12.1 13 (equal ranking) United Kingdom Poland 10.2 5 Estonia 11.9 6 Germany 11.7 15 (equal ranking) Switzerland Denmark 10.1 7 Hungary 11.5 17 Finland 10.0 8 Spain 11.4 18 Netherlands 9.4 9 Ireland 11.3 19 New Zealand 9.3 10 Slovak Republic 10.7 20 Korea 8.9 LPAs per capita Statistics taken from the 2009 Non-Medical Determinants of Health: Alcohol Consumption dataseries (revised data accessed on 5 December 2012). Note that statistics relating to alcohol consumption collected by the OECD and DSICA differ, however only OECD statistics have been used in this comparison to ensure consistency across all countries. Only the top 20 alcohol consuming OECD members are shown Copyright DSICA 2012 Source: OECD DSICA also notes that the Draft Report refers to World Health Organization (WHO) data. A review of WHO’s Global Status Report on Alcohol and Health 2011 (the WHO Report) ranks Australia as 44th out of 188 countries in terms of per capita alcohol consumption.12 While DSICA appreciates the broad coverage of the WHO Report, it is acknowledged that that there are cultural and religious factors which may result in significantly lower levels of per capita alcohol consumption in other countries (when compared to Australia). As such, DSICA cautions readers about such large international comparisons due to cultural and religious factors in some other countries and believes it is appropriate to compare Australia’s consumption only against similar Western countries – as in the OECD comparisons above which demonstrate that Australia’s annual per capita consumption is not high by world standards. Key point International evidence demonstrates that Australia ranks only 12th out of a total of 29 developed countries for which per capita alcohol consumption data is available. Results from broadreaching data analysis, such as that undertaken by WHO, should be viewed with caution due to cultural and religious factors in some other countries which make reliable comparative analysis difficult. 3.2 The Australian liquor industry The Draft Report states that: Specific taxes on alcohol raised $3,853 million in tax in 2009-10, 1.3 per cent of total revenue.13 DSICA understands that this reference is taken from the recently-released report The liquor industry (the Report) by The Australia Institute.14 DSICA contends that this figure is particularly misleading, as it only accounts for the excise duty levied on domestically produced beer, spirits 12 World Health Organization, Global Status Report on Alcohol and Health 2011 (World Health Organisation, 2011) 273-7. Australian National Preventative Health Agency, above n 2, [4]. 14 David Richardson, The liquor industry (Technical Brief No. 14) (The Australia Institute, 2012). 13 11 DSICA Submission to the Australian National Preventative Health Agency “Free the Spirit” and Ready-to-Drink products (RTDs), along with the WET. The Report should not be used to inform alcohol policy development activities. In fact, the Australian alcohol industry contributes significantly more taxation revenue than the $3,853 million figure quoted which and omits a number of other alcohol beverage taxation revenue sources, including the excise-equivalent customs duty applied to imported beer, spirits and RTDs, the ad valorem customs duty applied to imported spirits, RTDs and wine, and Goods and Services Tax (GST) revenue derived through the sale of alcohol beverages. Taking these revenue sources into account, DSICA estimates that the total tax revenue (including GST) from alcohol beverages in 2009-10 was approximately $6,952 million, 80 per cent higher than the figure quoted in The liquor industry report. Indeed, DSICA’s latest estimates indicate that the Australian alcohol industry will contribute $7,718 million in taxation revenue in 2012-13, as outlined in Figure 3-2 below. Figure 3-2: DSICA estimates of Commonwealth revenue from alcohol taxation (2012-13) DSICA REVENUE ESTIMATES 2012-13 ($ MILLIONS) Customs Duty* Beer low-strength - 68 - 68 38 106 1.38% Beer mid-strength - 275 - 275 90 365 4.73% Beer full-strength 264 1,781 - 2,045 472 2,517 32.61% Total Beer 264 2,124 - 2,388 600 2,988 38.72% RTDs and Flavoured Cider -+ 920 - 920 330 1,250 16.20% Brandy 26 25 - 51 7 58 0.76% Spirits 1,597 214 - 1,811 306 2,117 27.43% Total Spirits, Brandy, RTDs and Flavoured Cider 1,623 1,159 - 2,782 644 3,426 44.39% 12 - 731 743 481 1,224 15.86% Wine Traditional Cider Total Wine and Traditional Cider TOTAL Excise Duty WET Total Non-GST Revenue Product Category GST Revenue Total % - - 44 44 36 80 1.04% 12 - 775 786 518 1,304 16.90% 1,898 3,283 775 5,956 1,762 7,718 100.00% * Customs duty includes both the five per cent ad valorem customs tariff applied to imported spirits, RTDs, wine and traditional and flavoured cider, and exciseequivalent customs duty applied to imported spirits , beer and flavoured cider. + It has been assumed that ‘imported’ RTDs are imported in the form of bulk spirits then bottled as RTDs in Australia, therefore customs duty on imported RTDs has been included in the ‘spirits’ category. No estimate has been made of the very small customs duty amount paid by the imported flavoured cider market. Copyright DSICA 2012 Source: DSICA Pre-Budget Submission 2012-13 DSICA contends that there is a need to undertake policy development activities which are based on the most comprehensive, thorough research available. Given this, attention must be paid to the fact that the Australian alcohol industry contributes significantly more in alcohol taxation revenue than the $3,853 million figure identified. Key point The liquor industry report grossly underestimates contribution the Australian alcohol industry makes to government revenue and should not be used in the development of evidence-based alcohol policies. Estimates suggest that the Australian alcohol industry contributed $6,952 million in taxation revenue in 2009-10 – some 80 per cent more than the figure suggested by the Australia Institute. DSICA Submission to the Australian National Preventative Health Agency 12 “Free The Spirit” 3.3 Cost of alcohol-related harms The Draft Report states that: The total social costs of harmful alcohol consumption to the Australian community are estimated to be $15.3 billion annually.15 In addition, the Draft Report contains further discussion in relation to the varying estimates of social costs of alcohol misuse in Australia, which range from $3.8 billion to $36 billion annually.16 DSICA understands that the reference to the $15.3 billion figure has been derived from the Collins and Laspey monograph The costs of tobacco, alcohol and illicit drug abuse to Australian society in 2004/05,17 while the reference to the $36 billion figure has been taken from the report by Laslett et. al, The range and magnitude of alcohol’s harm to others.18 DSICA strongly opposes the methodologies used by Collins and Lapsley to estimate the social costs of alcohol consumption to the Australian community and Laslett et. al. to estimate the costs of alcohol harm to others as they grossly overestimate the true costs of alcohol misuse. As outlined in Figure 3-3 and Figure 3-4, DSICA’s view is supported by independent economic analysis and review undertaken by: • Access Economics; • Dr Eric Crampton of the University of Canterbury; and • Professor Klaus Mäkelä, former Secretary of the Finnish Foundation for Alcohol Studies. In essence, the methodologies used by Collins and Lapsley and Laslett et. al. are seriously flawed, with a significant degree of double-counting of individual cost components resulting in gross over-estimation of the true social costs associated with alcohol misuse and the costs of alcohol’s harm to others. They are not reflective of internationally accepted methodologies used to calculate social cost estimates and should not be used in public policy development. Figure 3-3: Key flaws identified in the report The costs of tobacco, alcohol and illicit drug abuse to Australian Society in 2004/05 Researcher/ agency Key flaws and conclusions Access Economics Key flaws • The report uses a ‘demographic approach’ to cost estimation, an uncommon methodology that means the authors have attempted to estimate the impact of alcohol abuse retrospectively. The reason for undertaking a retrospective rather than forward-looking approach is unclear, as is the policy usefulness of such an approach, and is likely to yield a much higher cost estimate than the human capital approach.19 • ‘Alcohol abuse’ is never clearly defined in the report, and definitions implicit in different cost elements vary throughout.20 • There is no mention in the report of the very large private benefits of responsible alcohol consumption in terms of utility value (choice, enjoyment). It is a major flaw to exclude private costs from total social costs and private benefits from total social 15 Australian National Preventative Health Agency, above n 2, [12]. Ibid [15]. David Collins and Helen Lapsley, The costs of tobacco, alcohol and illicit drug abuse to Australian society in 2004/05 (Australian Government, 2008). 18 Anne-Marie Laslett et. al., The Range and Magnitude of Alcohol’s Harm to Others (Alcohol Education and Rehabilitation Foundation, 2010). 19 Access Economics, Collins and Lapsley report review: social costs (Access Economics 2008) i. 20 Ibid. 16 17 13 DSICA Submission to the Australian National Preventative Health Agency “Free the Spirit” Researcher/ agency Key flaws and conclusions benefits, and it is incorrect to claim that costs borne by individuals are irrelevant to public decision-making.21 • The revenue estimation shows that taxation raise from alcohol abuse exceeds its cost to Government, so it is budget positive and abusers pay their way by some $1.4 billion (2004-05 prices) per annum. Alcohol taxes thus more than pay for the social costs of alcohol abuse, by a considerable margin, each year.22 Conclusion ‘There is apparent upward bias in most of the cost estimates and uncertainty is not dealt with due to grossly inadequate sensitivity analysis. Using a best possible approach would exclude one cost item, making the overall cost of alcohol abuse at least 18 per cent lower. The other findings of the report should be viewed with substantial scepticism.’23 Dr Eric Crampton, University of Canterbury Key flaws • Collins and Lapsley use survey methods to assign the proportion of crime attributable to alcohol which are inadequate for addressing alcohol’s causal role in crime.24 • The public health method used in identifying and calculating the costs imposed on others diverges with methodologies used in regarded economic methods and literature. In particular, the social cost estimation method used in public health literature results in a cost-inflating bias as social costs and private costs are conflated, and many cost categories are double-counted.25 • The application of per capita Gross Domestic Product (GDP) as a measure of foregone production arising from absenteeism and premature mortality is considerably larger than the preferred method which uses foregone wages plus employer hiring costs (which constitute an upper bound on gross productivity losses consequent to premature mortality) results in a much larger aggregate wage bill and three significant issues: where the death is incurred by the drinker, costs are properly considered internal rather than external – only increased employer search costs are plausibly external costs (and therefore able to be included in the calculation);26 using per capita GDP rather than wages are a measure of forgone output requires strong assumptions about worker irreplaceability and capital-labour complementarity. Indeed, this method has been rejected by WHO;27 and the latter inclusion of intangible costs of loss of life in conjunction with per capita GDP as a measure of forgone production constitutes double-counting.28 Conclusion Only $3.8 billion of the reported $15.3 billion cost can be considered potentially external, a figure which is close to aggregate alcohol excise taxation revenue.29 Professor Klaus Mäkelä, former Secretary Key flaws • Collins and Lapsley argue that resources spent on hazardous drinking should be classified as social costs, since abusive consumers are not fully informed of the effects of alcohol on health. However, a number of studies indicate that users are more knowledgeable than non-users.30 21 Ibid ii. Ibid. Ibid iv. 24 Eric Crampton, Matt Burgess and Brad Taylor, ‘What’s in a cost? Comparing economic and public health measures of alcohol’s social costs’ (2012) 125 New Zealand Medical Journal 1, 2. 25 Ibid 1. 26 Ibid 5. 27 Ibid. 28 Ibid. 29 Ibid 1. 30 Klaus Mäkela, ‘Cost-of-alcohol studies as a research programme’ (2012) 29 Nordic Studies on Alcohol and Drugs 321, 322. 22 23 DSICA Submission to the Australian National Preventative Health Agency 14 “Free The Spirit” Researcher/ agency of the Finnish Foundation for Alcohol Studies Key flaws and conclusions The cost calculations treat the value of stolen property as a loss, however this is misleading from the societal perspective advocated by the cost-of-alcohol literature as it overlooks the revenue of the thief.31 Conclusion ‘Even the most sophisticated cost-of-alcohol calculations include entries based on misleading assumptions or logical mistakes. Traditional measures of alcohol problems offer a better picture of the effects of policy measures than cost-of-alcohol estimates’.32 • Figure 3-4: Key flaws identified in the report The range and magnitude of alcohol’s harm to others Researcher/ agency Key flaws and conclusions Access Economics Key flaws • There was an ‘overestimation of the magnitude and impact of alcohol’s harm to others within survey responses due to a number of biases’.33 • Incorrect methods were used to develop attributable fractions, meaning that all cost components are many times overstated.34 • ‘Incorrect methods (were) used to estimate the costs associated with the impact of others’ drinking, such as intangible costs of others’ drinking on health and wellbeing, of harms experienced and of harms from strangers’.35 • Flawed methods used by Collins and Lapsley in undertaking earlier studies (which were heavily relied on in the Report) to estimate the cost of alcohol abuse in Australia are out-of-line with best practice cost of illness studies, and are likely to overestimate the true cost.36 Conclusion The costs presented in the Report ‘appear to be grossly overestimated, and therefore the reported $36 billion total costs represents a poor estimate of the real cost of alcohol’s harm to others. Consequently, the total cost and individual cost components should not be used to inform policy decisions regarding the consumption of alcohol’.37 As recognised in the critiques above and by the United Kingdom research group Findings, cost studies are generally limited to quantifying the adverse consequences of drinking, and include benefits (if at all) only in terms of health. While in some instances studies may be limited to these considerations alone, if the study purports to assess total costs to a society, then there is no rationale for excluding other non-health related benefits including the pleasures/value derived through taste, food value, enjoyment of an altered state of consciousness and greater expressiveness, as well as social rewards such as the pleasure given to dinner guests, the solidarity of round-buying and broader social cohesion.38 In addition to these concerns relating to the omission of benefits derived from responsible consumption decisions, the estimates of costs imposed on society by drinking are often grossly inflated because (among other things), they assume that hazardous drinking must be irrational consumption, that crime benefits no one, that drinking has no social, psychological or indirect business benefits, and that productivity losses are not counter-balanced by benefits 31 Ibid 324. Ibid 339. Access Economics, Review of ‘The range and magnitude of alcohol’s harm to others’ (Access Economics, 2010) i. 34 Ibid ii. 35 Ibid. 36 Ibid. 37 Ibid i. 38 Findings, Cost-of-alcohol studies as a research programme (20 October 2012) <http://findings.org.uk/count/downloads/download.php?file=Makela_K_2.txt>. 32 33 15 DSICA Submission to the Australian National Preventative Health Agency “Free the Spirit” elsewhere.39 Such assumptions are based heavily on value judgments which are generally imbedded in cost studies, rather than explicitly stated – clouding any sense of objectivity which may be attributable to such studies.40 It is on this basis, and as demonstrated in Figure 3-3 and Figure 3-4 above, DSICA contends that current cost of harm studies are an inappropriate and inaccurate basis on which to develop evidence-based policy decisions. Traditional measures of alcohol problems, including longitudinal consumption and demographic data offer greater, more robust insight into the extent and nature of alcohol-related harms in society and the impact of specific interventions. Key point The cost of harm studies undertaken by Collins and Lapsley and Laslett et. al. significantly overestimate the costs of alcohol misuse to society. Inappropriate methodologies, assumptions and upward bias in estimates used in the reports negate the achievement of any robust, evidence-based findings in the reports, rendering them futile in informing public alcohol policies. 3.4 Population approaches versus targeted approaches for addressing harmful consumption of alcohol The Draft Report states that: …evidence suggests that regulatory and fiscal policies (those focusing on economic and physical availability such as restricting the days and hours of sale, restricting outlet density and taxation), drinkdriving countermeasures and policies that target the whole population are more effective than those targeting high-risk groups. Nevertheless, there was significant disagreement among the submissions regarding both the effectiveness of, and the preference for, whole of population versus targeted approaches to reducing harmful consumption.41 DSICA acknowledges that there is considerable debate regarding the most appropriate policy approach to take with respect to reducing the harms associated with alcohol misuse, however does not accept the proposition that whole of population policies are proven to be more effective than targeted policies, in reducing levels of alcohol-related harm. The International Center for Alcohol Policies in its Guide to Creating Integrative Alcohol Policies makes the following comments with respect to both approaches: Control measures are aimed at restricting access to and availability of alcohol through a range of measures applied to the population as a whole. The goal of these control measures is to reduce the overall per capita consumption in an effort to reduce the incidence of harm. 39 Ibid. Ibid. 41 Australian National Preventative Health Agency, above n 2, [22]. 40 DSICA Submission to the Australian National Preventative Health Agency 16 “Free The Spirit” The ‘control of consumption’ approach relies on the notion of a defined and linear relationship between the level of alcohol consumption across a population and the level of harm.42 Advocates for population-based measures have long argued that reducing overall consumption across all alcohol consumers will impact on the levels of alcohol-related harm. Governments have increasingly adopted control policy measures, alcohol consumption has fallen, and yet there appears to be no impact on the levels of excessive drinking amongst certain subsets of the community. In particular, population measures are broad and non-specific and as a result they: • cannot differentiate between those who drink responsibly and those who abuse alcohol; • are insensitive to variations and cultural difference in the role of alcohol in society; • require legislation and structural change for their implementation; • rely on enforcement to be effective; • are not tailored to the reality of drinking; and • are inflexible to change and shifting societal needs. Conversely, the aim of targeted interventions is to reduce misuse and the harms that flow from that, not to necessarily reduce overall consumption. Targeted interventions seek to reduce the potential for harm by specifically and selectively focusing on problematic drinking patterns amongst those individuals, settings and behaviors where risk of harm from drinking is increased. In this regard, targeted measures: • specifically address harm where it occurs; • can be tailored to individual, societal, and cultural differences; • do not require structural change or legislation for implementation; • make best use of resources that are available; • avoid most unintended outcomes by virtue of their specificity; and • are responsive to the immediacy of community needs. DSICA believes that the intention behind targeted approaches is to focus attention on those alcohol-related issues causing the greatest concern within the community. The strategy behind targeted approaches does not have as its endpoint a reduction in the overall consumption of alcohol within the community. However, what it does seek is to reduce the level of harmful drinking and its impacts on individuals and communities. DSICA’s position is supported by findings from the International Center for Alcohol Policies, which notes that: The targeted interventions approach relies on the principles of harm reduction. It is a pragmatic one, recognizing that risks are inherent in many behaviors, but that it is nevertheless possible to reduce and manage many of them. The approach also acknowledges that it is possible to preserve the ability and right of individuals to enjoy drinking, while at the same time reducing the potential for problems. 42 2. International Center for Alcohol Policies, Guide to Creating Integrative Alcohol Policies, (International Center for Alcohol Policies, 2008) 17 DSICA Submission to the Australian National Preventative Health Agency “Free the Spirit” DSICA contends that an integrated, comprehensive approach to alcohol policy development must strike a balance between targeted education, early intervention and selective enforcement strategies. Indeed, individuals must be equipped with the skills they need to make informed consumption decisions and communities must focus on addressing settings and patterns which increase the occurrence of alcohol-related harms. To this end, DSICA believes that evidence-based harm reduction and targeted interventions must include the following considerations observed in the International Center for Alcohol Polices’ Blue Book: Practical guides for alcohol policy and prevention approaches: • the provision of balanced information on both benefits and harms; • a sound evidence base founded on the best available scientific data; • an approach that is palatable and easy for the public to understand; • a focus on issues that correspond to actual, familiar and representative drinking behaviors; • the recognition that alcohol consumption is an integral part of many societies and may be associated with both positive and negative outcomes; • an approach that addresses the potential for harm in a non-judgmental way; • strengthening individual responsibility at the same time as enforcing external controls; • involvement of individuals and their communities in all aspects and levels of policy; and • development, and consistency with other approaches and measures that are being used.43 A significant benefit of targeted approaches is that they do not rely exclusively on governments for their implementation, but require a whole of community response. DSICA would argue that there is considerable scope for communities of interest to formulate a collective approach to reducing harms associated with alcohol misuse. A new research study published in the prestigious journal Alcohol and Alcoholism in July 2012 raises a broad question with respect to the efficacy of control policy measures in reducing alcohol abuse/binge drinking amongst young people. The study reaches the following conclusion that: Among all the 40 countries in the present analysis, a non-significant trend was observed, whereby higher prices, higher drinking age and stronger alcohol controls were associated with a lower weekly drinking frequency, but a potentially higher frequency of binge drinking. It is important that future research explores the causal relationships between alcohol policy measures and alcohol consumption patterns to determine whether strict policies do in fact have any beneficial effect on drinking patterns, or lead to rebellion and an increased prevalence of binge drinking.44 This research finding is particularly important in the Australian context, as we need to ensure that the policy directions we take are appropriately targeted to address binge drinking amongst young people, and address at-risk adult groups. Indeed, such an approach is in accordance with WHO’s Global strategy to reduce the harmful use of alcohol, which, as the strategy suggests, 43 International Center for Alcohol Policies, The ICAP Blue Book: Practical Guides for Alcohol Policy and Prevention Approaches (International Center for Alcohol Policies, 2011) A.1. 44 Conor Gilligan, Emmanuel Kuntsche and Gerhard Gmel, ‘Adolescent Drinking Patterns Across Countries: Associations with Alcohol Policies’ (2012) 0(0) Alcohol and Alcoholism 1, 5. DSICA Submission to the Australian National Preventative Health Agency 18 “Free The Spirit” seeks to target harmful alcohol use – particularly the behaviours and population groups known to partake in hazardous drinking practices – not alcohol use at the broader, population-wide level.45 In acknowledging the significant evidence favouring targeted harm reduction measures, DSICA contends that the introduction of a population-wide measure such as a minimum floor price is unlikely to be effective in reducing alcohol consumption of ‘at risk’ individuals and communities. While some population-based measures to restrict alcohol consumption are appropriate, specific, targeted measures are required to reduce the incidence of harmful and hazardous drinking. Key point Available evidences strongly indicates that targeted measures – in conjunction with appropriate population-based strategies – provide significant opportunities for reducing the incidence of harmful alcohol consumption in Australia. Population-based approaches such as minimum (floor) pricing are significantly less effective at changing the behaviours of at-risk groups. 45 World Health Organization, Global strategy to reduce the harmful use of alcohol (World Health Organization, 2010) 5. 19 DSICA Submission to the Australian National Preventative Health Agency “Free the Spirit” 4 Minimum (floor) pricing Since publication of the Issues Paper and Draft Report, there have been marked developments in international jurisdictions either with minimum (floor) pricing measures in operation, or contemplating the introduction of such measures. This section discusses the recent developments seen in Canada, Scotland, England and Wales and draws on the latest evidence relating to the purported effectiveness of minimum (floor) pricing and key issues associated with such measures. 4.1 Canada The Draft Report states that: In summary, the Canadian studies recommend careful consideration of minimum pricing as part of a comprehensive strategy to reduce alcohol-related harm.46 DSICA strongly cautions against the use of research findings concerning the application of Social Reference Pricing (SRP) in Canadian jurisdictions in the Australian context. In particular, the Canadian approach to alcohol regulation differs considerably from that seen in Australia, and the latest research findings available do not conclusively demonstrate the effectiveness of SRP in reducing alcohol-related harm. As stated in its earlier submission, DSICA noted that the Canadian alcohol distribution and regulatory environment is markedly different to that seen in Australia as: • in Canada, minimum prices differ between and within different types of alcohol beverages and there is not a single price per unit of alcohol; • increases in minimum prices in Canada are not simultaneous, which may potentially allow substitution behaviour and ‘trading down’; • in Canada, alcohol is sold in liquor stores and not in supermarkets, which may limit the broader impact of the alcohol industry’s response; • all alcohol distribution is state controlled in Canada; • some provinces in Canada prohibit products perceived to be especially harmful (e.g. Alberta has banned beer products over 11 per cent alcohol by volume [abv]); • in Canada, some end-of-line below-SRP selling is permitted; and • the revenue from SRP in Canada goes to the provincial government.47 In addition to these social and regulatory policy distinctions, the latest evidence concerning the application of SRP in Canada is inconclusive in relation to the effectiveness of SRP in reducing alcohol consumption by heavy drinkers and young drinkers. In particular, research undertaken by the Canadian Centre on Substance Abuse: • notes that a combination of population-wide strategies and targeted strategies are required to address all sources of alcohol-related harm;48 and 46 Australian National Preventative Health Agency, above n 2, [59]. Health and Sport Committee, Scottish Parliament, 2nd Report, 2012 (Session 4): Stage 1 Report on the Alcohol (Minimum Pricing) (Scotland) Bill (2012) [24]. 48 Gerald Thomas, Price Policies to Reduce Alcohol-Related Harm in Canada (Canadian Centre on Substance Abuse, 2012), 4l. 47 DSICA Submission to the Australian National Preventative Health Agency 20 “Free The Spirit” • views minimum pricing as one intervention available to address alcohol-related harm – not in isolation from other strategies, most notably the provision of specific taxes based on alcohol content.49 In addition to these findings, DSICA further contends that the applicability and relevance of available Canadian studies to the Australian minimum floor pricing debate must be viewed with caution. The most recent study concerning SRP in Saskatchewan is limited in both its robustness and transferability as it: • is based consumption data for only two years following the new SRP policy and prices (which were introduced in April 2010), and thus does not consider the long-term effects of SRP – a significant limitation as behavioural change is not necessarily instantaneous;50 and • acknowledges that the government maintains a monopoly over many liquor store sales – thus making the impact of SRP on retail sales prices in off-premise venues (which account for at least 63 per cent of total consumption in the province) predictable, whilst the impact on on-premise sales is difficult to quantify.51 In summary, the Canadian experience does not provide a solid evidence base on which to pursue Australian policy development activities. Indeed, the Canadian Centre on Substance Abuse acknowledges that ‘direct evidence showing conclusively that minimum pricing reduces risky drinking at the population level does not exist’ – a sound warning for Australian authorities seeking to develop evidence-based policies grounded on the best available international and national research.52 Key point There is a lack of long-term empirical evidence relating to the impact of SRP on alcohol-related harms, and risky and high-risk drinking behaviours. Given this evidence vacuum, and the significant differences between the Canadian and Australian alcohol policy contexts, the Canadian experience is not an appropriate example upon which to base Australian policy development. 4.2 Scotland The Draft Report states that: On 22 October 2012 it was reported that implementation of a minimum price was going on hold pending the outcome of legal challenges.53 Since publication of the Draft Report, there have been significant developments concerning the introduction of a MUP for alcohol beverages in Scotland. In particular, communication from the EC has confirmed that the proposed legislation concerning the introduction of a MUP in Scotland (as it currently stands) is incompatible with the Treaty on the Functioning of the European Union (TFEU). In addition to this, further evidence concerning to the modelling projections contained in the Sheffield Alcohol Policy Model casts doubt on the veracity of 49 Ibid 2. Tim Stockwell, Jinhui Zhao and Norman Giesbrecht, ‘The Raising of Minimum Alcohol Prices in Saskatchewan, Canada: Impacts on Consumption and Implications for Public Health’ American Journal of Public Health (published online ahead of print, 18 October 2012). 51 Ibid e6. 52 Thomas, Zhao and Giesbrecht, above n 48, 7. 53 Australian National Preventative Health Agency, above n 2, [62]. 50 21 DSICA Submission to the Australian National Preventative Health Agency “Free the Spirit” findings and purported benefits a MUP will have on alcohol-related harms and risky and highrisk drinking behaviours. Each of these considerations are discussed in turn below, and further highlight the difficulties and lack of international support for minimum pricing. 4.2.1 Findings from the European Commission on the legality of minimum pricing Upon passing of the Alcohol (Minimum Pricing) (Scotland) Bill 2011 (UK) (NB subsequently the Alcohol (Minimum Pricing) Scotland Act 2012 (UK)) (the draft legislation) on 24 May 2012, a number of countries raised objections to the draft legislation in light of the United Kingdom’s commitments under European trade rules.54 Following these objections, the EC issued a legal directive in November 2012 outlining the draft legislation’s incompatibility with the United Kingdom’s obligations under the TFEU Art 34. In particular, the EC found that: • although the MUP is designed to apply to both imported and domestically produced goods equally, it is capable of having an adverse effect on imported goods and is therefore considered as a measure imposing a quantitative restriction as it prevents the lower cost price (and base) of imported goods being reflected in their final selling price; • the introduction of a MUP may have negative side effects and lead to further market distortions. In particular, a MUP will create greater incentives for retailers and supermarkets to sell more alcohol beverages as a result of the fact that they will make higher margins on the products affected by the policy. This will give retailers incentives to allocate increased resources to the sale of products affected by the MUP compared with what could be expected to be the case if, for example, similar average retail price increases were cause by an across-the-board increase in excise duty; • increasing existing excise duties is a more appropriate and suitable option to achieve the goal of reducing alcohol consumption without resulting in any adverse effects on competition, and is less trade restrictive; • there are other additional measures the Scottish Government may adopt, including measures specifically targeted at particular areas where there are known to be higher levels of alcohol-related harm – such measures are likely to be more effective than measures aimed at the total population; and • on this basis, the draft legislation may create obstacles to the free movement of goods within the internal (European Union [EU]) market contrary to the TFEU Art 34, and appears to be a disproportionate response under the TFEU Art 36.55 Given these findings, the Scottish Government has been ‘invited to abstain from adopting the draft legislation at issue’, and is required to inform the EC of the action it intends to take as a result of this opinion by 27 December 2012.56 Should the Scottish Government implement the draft legislation unamended, and without following this process, a letter of formal notice may be issued by the EC under the TFEU Art 258. DSICA acknowledges that unlike Scotland (as represented by the United Kingdom Government in the European Union), Australia is not part of a similar trading bloc. However, it is noted that Australia is a World Trade Organization (WTO) member, and therefore subject to the General 54 Countries raising objections to the legislation included Bulgaria, France, Italy, Portugal and Spain. See ‘Health Secretary “firmly” believes minimum pricing meets European law’ STV News (online), <http://news.stv.tv/politics/193010-health-secretary-firmly-believesminimum-pricing-meets-european-law/>, 2 October 2012. 55 Communication from the Commission – SG(2012) D/52513; Directive 98/34/EC; Notification 2012/0394/UK. 56 Ibid. DSICA Submission to the Australian National Preventative Health Agency 22 “Free The Spirit” Agreement on Tariffs and Trade 1994 (GATT 1994) which imposes similar restrictions on the application of quantitative restrictions under Art XI:1 as follows: No prohibitions or restrictions other than duties, taxes or other charges, whether made effective through quotas, import or export licences or other measures, shall be instituted or maintained by any contracting party on the importation of any product of the territory of any other contracting party or on the exportation or sale for export of any product destined for the territory of any other contracting party.57 The GATT Art XX provides for exceptions to the application of Art XI:1, such as where a measure is: • necessary to protect public morals; or • necessary to protect human, animal or plant life or health.58 However, not only are these exceptions qualified by a necessity requirement, they must also not be applied in a manner which would constitute a means of arbitrary or unjustifiable discrimination or a disguised restriction on international trade.59 And, most importantly – in the case of a measure which may be ‘necessary to protect human, animal or plant life or health’, there must be no other reasonably available alternatives.60 As demonstrated above, and found by the EC (albeit in the context of the TFEU), the application of excise duties is a more appropriate and suitable alternative to the introduction of a minimum (floor) price. These factors strongly suggest that if a minimum (floor) price were introduced in Australia, it would be in violation of the GATT 1994 Art XI:1, and would not be subject to exemptions afforded under Art XX. Key point The EC directive of November 2012 confirms that the draft minimum pricing legislation in Scotland is incompatible with the TFEU, and the application of excise duties is a more appropriate and suitable option to achieve the goal of reducing alcohol consumption without resulting in any adverse effects on competition, and is less trade restrictive. Although not directly applicable to the Australian context, as a WTO member Australia is subject to the GATT 1994 which imposes similar prohibitions on trade restrictions – these would arguably be violated if a minimum (floor) price were introduced. 4.2.2 Additional findings concerning the Sheffield Alcohol Policy Model A considerable amount of evidence supporting the introduction of a MUP in Scotland has been taken from economic modelling undertaken by the School of Health and Related Research at the University of Sheffield (referred to as the Sheffield Alcohol Policy Model). DSICA’s earlier submission noted a number of criticisms of the Sheffield Alcohol Policy Model, particularly in relation to the (lack of) effectiveness of a MUP in targeting heavy or harmful drinkers. Since preparation of DSICA’s earlier submission, and release of the Draft Report, further criticisms of 57 General Agreement on Tariffs and Trade 1994 Art XI:1. Ibid Art XX(a)-(b). 59 Ibid Art XX. 60 See Appellate Body Report, European Communities – Measures Affecting Asbestos and Asbestos-Containing Products (WT/DS135/ABR) (12 March 2001) [169]-[170]. 58 23 DSICA Submission to the Australian National Preventative Health Agency “Free the Spirit” both the assumptions used in the Sheffield Alcohol Policy Model and the findings drawn from it have emerged, including: • the application of a false assumption that heavy drinkers are made likely to reduce their consumption of alcohol as a result of a price rise, which is based on controversial beliefs about the relationship between per capita alcohol consumption and rates of alcohol-related harm;61 • an overestimation of the putative health benefits to be derived from minimum pricing;62 • an overestimation of the reduction in overall alcohol consumption that it likely to take place following the introduction of a MUP;63 • a lack of consideration of other policy impacts arising from the introduction of a MUP, including the possibility that the introduction of a MUP will fuel the market for illegally produced alcohol and the effects of secondary poverty created by people on low incomes spending a greater share of their wage on alcohol products;64 and • application of on-trade price data and price elasticities from England, which are not inherently transferrable nor applicable to the Scottish market.65 These incorrect assumptions and oversights led Duffy and Snowdon to conclude: No degree of statistical confidence can be placed in the values produced. The models relating health consequences to consumption cannot be considered reliable as they are based almost entirely on assumptions with no direct individual level data relating consumption and consequences. They are not fit for the purpose of estimating rates of consequences, far less changes in these following policy changes (emphasis added).66 These recent research findings, along with those outlined in DSICA’s earlier submission, clearly demonstrate the lack of a robust evidence base demonstrating the effectiveness of minimum pricing. These findings, along with the international trade concerns highlighted in section 4.2.1 strongly support DSICA’s contention that the Scottish experience cannot be relied upon by policymakers as a sound case study upon which to base the introduction of a minimum (floor) price in Australia. Key point Further critiques of the Sheffield Alcohol Policy Model reinforce DSICA’s view that it does not provide a sound evidence base on which to inform public policy debate concerning the introduction of a minimum (floor) price in Australia. 61 Duffy and Snowdon, above n 3, 5. Ibid 11. 63 Ibid. 64 Ibid 12. 65 Ibid 20. 66 Ibid 23. 62 DSICA Submission to the Australian National Preventative Health Agency 24 “Free The Spirit” 4.3 England and Wales Since publication of the Draft report, there have been significant developments pertaining to the possible introduction of a MUP in England and Wales. As foreshadowed in DSICA’s earlier submission and the Draft Report, the UK Home Office has undertaken further work in relation to the Coalition Government’s earlier publication The Government’s Alcohol Strategy. Most notably, on 28 November 2012, the UK Home Office released the paper A consultation on delivering the Government’s policies to cut alcohol fuelled crime and anti-social behaviour which seeks views on a number of measures outlined in the Strategy. Of note to DSICA is the consultation process concerning the proposed introduction of a MUP of 45 pence per unit of alcohol (approximately AUD 0.69) and affiliated Impact Statement concerning minimum unit pricing,67 and the issues it raises in relation to: • the need for a holistic, integrated approach to addressing alcohol-related harms; • the fact that the introduction of a MUP in England and Wales is, to a significant degree, driven by the need to increase the price of wine and cider products, which are not subject to volumetric excise duty; and • concerns regarding the unintended consequences arising from the MUP measure. DSICA acknowledges that in the United Kingdom context, the introduction of a MUP is being considered as one of several options to ‘tackle the drink fuelled antisocial behaviour and crime blighting [its] communities’.68 Unlike the Australian debate (which is largely focused on the introduction of a minimum [floor] price alone, rather than the application of other interventions), in the United Kingdom, minimum unit pricing ‘is taken on top of, not instead of, other regulatory and non-regulatory measures to achieve the necessary impact’.69 While DSICA does not support the introduction of a MUP in England or Wales (or Australia), it does support the consideration of holistic, integrated responses to addressing risky and high risk drinking behaviours and alcohol-related harms, and contends that a similar approach should be adopted in Australia. DSICA further notes that the Impact Assessment highlights key factors driving the possible introduction of a MUP in England and Wales, which are substantially different to those in Australia, arguably rendering the United Kingdom experience inapplicable to the Australian context. To this end, the Impact Assessment notes that a MUP is a preferable approach to alcohol (excise) duty changes as ‘alcohol duties alone could not bring about a system of minimum pricing as EU rules prevent wine and cider duties being directly linked to their alcohol content’.70 Indeed, the EC Council Directive 92/83/EEC requires all EU members to impose unitary (i.e. per litre of fluid, not alcohol content) excise duty rates to wine, cider and other fermented beverage products (excluding beer).71 Such an excise duty regime severs the link between the amount of excise taxation paid and the alcohol content of the product, inhibiting responsible consumption choices. However, Australia is not subject to similar directives. As noted, replacement of the ad valorem WET with a volumetric taxation regime for wine products (which include traditional cider) would result in a wholly volumetric excise duty system for all alcohol beverages in Australia, creating an effective minimum (floor) price – hence overcoming the need to introduce a statutory minimum pricing regime. Given this, one of the key driving 67 UK Home Office, A consultation on delivering the Government’s policies to cut alcohol fuelled crime and anti-social behaviour (UK Home Office, 2012) [5.5]; UK Home Office, A Minimum Unit Price for Alcohol: Impact Assessment (UK Government, 2012). 68 UK Home Office, A consultation on delivering the Government’s policies to cut alcohol fuelled crime and anti-social behaviour (UK Home Office, 2012) 4. 69 UK Home Office, A Minimum Unit Price for Alcohol: Impact Assessment (UK Government, 2012) 1. 70 Ibid 3. 71 Council Directive 92/83/EEC of 19 October 1992 Art 9 and Art 13. 25 DSICA Submission to the Australian National Preventative Health Agency “Free the Spirit” factors behind the introduction of a MUP in the England and Wales is neither analogous nor applicable to the Australian context. Finally, the Impact Assessment also reiterates a number of DSICA’s concerns relating to the introduction of a minimum (floor) price, namely: • limitations of the Sheffield Alcohol Policy Model and subsequent conclusions relating to the purported effectiveness of a MUP which can be drawn from it;72 • the fact that a MUP has not yet been implemented in any other analogous country, rendering potential consumer responses uncertain;73 • potential ‘second round’ effects of a MUP that may result in shifts in strategy by retailers and producers, including increased incentives for producers to produce lower-strength alcohol products which retail at a lower price, and increases in price for products not affected by a MUP in order to maintain a price differential for brand identity purposes;74 and • the fact that setting a MUP at a ‘significant’ level could lead to increased levels of smuggling, illicit production and ‘bootlegging of alcohol,75 creating market distortions and further inhibiting responsible consumption decisions. DSICA contends that such concerns must be appropriate canvassed and addressed in any alcohol policy development matters concerning the introduction of a minimum (floor) price – particularly as they may lead to unintended (negative) consequences which could mitigate any purported benefits of such a measure. DSICA acknowledges that as the UK Home Office’s consultation process progresses it is highly likely that further evidence relating to the purported benefits and consequences of a MUP will emerge for review and comment. Such evidence and research findings must be viewed with considerable caution due to the different policy imperatives behind the introduction of a MUP in England and Wales and a minimum (floor) price in Australia. As noted earlier, the UK is subject to EU trade restrictions which prohibit the application of volumetric taxation to certain beverage categories – thus preventing an effective MUP being introduced through other taxation measures. Australia is not bound by such requirements – and reform of the ad valorem WET to a volumetric taxation regime would provide an effective minimum (floor) price. Key point The experience in England and Wales highlights the difficulties in identifying robust evidence bases upon which to develop arguments in support of minimum (floor) pricing and confirms that the different trade and regulatory environments observed in Australia and the United Kingdom limit the degree to which comparative analysis can be undertaken and similar approaches to addressing hazardous drinking behaviours may be adopted. 4.4 Conclusion As stated in DSICA’s earlier submission, a review of available information relating to minimum (floor) pricing and other similar interventions throughout the world does not reveal any conclusive evidence demonstrating the effectiveness of such a measure in reducing risky and 72 UK Home Office, above n 69, 8. Ibid 10. 74 Ibid 15. 75 Ibid 22. Note that what would constitute a ‘significant’ MUP has not been defined in the Impact Assessment. 73 DSICA Submission to the Australian National Preventative Health Agency 26 “Free The Spirit” high-risk drinking behaviours or alcohol-related harms. Indeed, any available evidence is to be viewed with caution due to the lack of long-term data, contested assumptions regarding price elasticities and the varying regulatory and policy environments concerning alcohol taxation, distribution and sales in operation throughout the world. In light of this, DSICA contends that available international experience relating to the effectiveness of minimum (floor) pricing is limited, and does not provide a robust evidence base on which to pursue Australian alcohol policy development activities. 27 DSICA Submission to the Australian National Preventative Health Agency “Free the Spirit” 5 Conclusion DSICA’s earlier submission and foregoing analysis strongly suggest that the introduction of a minimum (floor) price is not an appropriate policy intervention to achieve ANPHA’s stated objectives of discouraging harmful consumption and promoting safer consumption. In particular: • Australian per capita alcohol consumption is stable – and comparatively low by international standards; • while the current Australian alcohol taxation regime fails to achieve desired economic, health and social policy objectives, a minimum (floor) price will not redress these concerns effectively; • there is a lack of empirical evidence demonstrating the effectiveness of minimum pricing internationally. The application of findings from the Canadian SRP model to the Australian context is precarious due to the significant differences between the Canadian alcohol regulation model and the Australian experience; • assumptions on which much evidence regarding the effectiveness of a minimum (floor) price in Scotland, England and Wales are highly flawed, and fail to consider second-round impacts of a minimum (floor) pricing regime which may mitigate, if not entirely offset, any purported benefits; and • the EC has indicated that the introduction of a MUP in Scotland is likely to be inconsistent with the United Kingdom’s international trade obligations – arguably in a similar manner to Australia’s obligations under the GATT 1994. These factors considered, it is apparent that a minimum (floor) price would not provide an evidence-based, holistic approach to addressing risky and high-risk consumption behaviours, but would instead be a blunt, population-wide instrument which unfairly penalises the majority of Australian drinkers who consume alcohol in a responsible manner. DSICA remains committed to supporting evidence-based approaches to reducing the harm associated with the excessive or inappropriate consumption of alcohol. The introduction of a wholly volumetric alcohol taxation regime, initially through reform of the ad valorem WET, is in line with international best practice approaches to alcohol taxation. Such a regime would deliver desired health, social policy and revenue outcomes, and create an effective minimum (floor) price for all alcohol beverages therefore removing the need to introduce a statutory minimum pricing mechanism. DSICA Submission to the Australian National Preventative Health Agency 28 “Free The Spirit” 29 DSICA Submission to the Australian National Preventative Health Agency “Free the Spirit” A References Access Economics, Collins and Lapsley report review: social costs (Access Economics, 2008). Access Economics, Review of ‘The range and magnitude of alcohol’s harm to others’ (Access Economics, 2010). Appellate Body Report, European Communities – Measures Affecting Asbestos and AsbestosContaining Products (WT/DS135/ABR) (12 March 2001). Australian National Preventative Health Agency, Exploring the Public Interest case for a Minimum (Floor) Price for Alcohol: Draft Report (Australian Government, 2012). Australian National Preventative Health Agency, Exploring the Public Interest Case for a Minimum (Floor) Price for Alcohol: Issues Paper (Australian Government, 2012). Collins, David and Lapsley, Helen, The costs of tobacco, alcohol and illicit drug abuse to Australian society in 2004/05 (Australian Government, 2008). Communication from the Commission – SG(2012) D/52513; Directive 98/34/EC; Notification 2012/0394/UK. Council Directive 92/83/EEC of 19 October 1992. Crampton, Eric, Burgess, Matt and Taylor, Brad, ‘What’s in a cost? Comparing economic and public health measures of alcohol’s social costs’ (2012) 125 New Zealand Medical Journal 1. Duffy, John and Snowdon, Christopher, The Minimal Evidence for Minimum Pricing: The fatal flaws in the Sheffield Alcohol Policy Model (Adam Smith Institute, 2012). Findings, Cost-of-alcohol studies as a research programme (20 October <http://findings.org.uk/count/downloads/download.php?file=Makela_K_2.txt>. 2012) General Agreement on Tariffs and Trade 1994. Health and Sport Committee, Scottish Parliament, 2nd Report, 2012 (Session 4): Stage 1 Report on the Alcohol (Minimum Pricing) (Scotland) Bill (2012). Gilligan, Conor, Kuntsche, Emmanuel and Gmel, Gerhard, ‘Adolescent Drinking Patterns Across Countries: Associations with Alcohol Policies’ (2012) 0(0) Alcohol and Alcoholism 1. Henry, Ken et. al., Australia’s future tax system: Report to the Treasurer (Part Two – Detailed Analysis) (Australian Government, 2009). International Center for Alcohol Policies, Guide to Creating Integrative Alcohol Policies, (International Center for Alcohol Policies, 2008). International Center for Alcohol Policies, The ICAP Blue Book: Practical Guides for Alcohol Policy and Prevention Approaches (International Center for Alcohol Policies, 2011). Laslett, Anne-Marie et. al., The Range and Magnitude of Alcohol’s Harm to Others (Alcohol Education and Rehabilitation Foundation, 2010). Mäkela, Klaus, ‘Cost-of-alcohol studies as a research programme’ (2012) 29 Nordic Studies on Alcohol and Drugs 321. Organisation for Economic Co-Operation and Development, Non-Medical Determinants of Health: Alcohol Consumption (Organisation for Economic Co-Operation and Development, 2009). DSICA Submission to the Australian National Preventative Health Agency 30 “Free The Spirit” Richardson, David, The liquor industry (Technical Brief No. 14) (The Australia Institute, 2012). Stockwell, Tim, Zhao, Jinhui and Giesbrecht, Norman, ‘The Raising of Minimum Alcohol Prices in Saskatchewan, Canada: Impacts on Consumption and Implications for Public Health’ American Journal of Public Health (published online ahead of print, 18 October 2012). ‘Health Secretary “firmly” believes minimum pricing meets European law’ STV News (online), <http://news.stv.tv/politics/193010-health-secretary-firmly-believes-minimum-pricing-meetseuropean-law/>, 2 October 2012. Thomas, Gerald, Price Policies to Reduce Alcohol-Related Harm in Canada (Canadian Centre on Substance Abuse, 2012). UK Home Office, A consultation on delivering the Government’s policies to cut alcohol fuelled crime and anti-social behaviour (UK Home Office, 2012). UK Home Office, A Minimum Unit Price for Alcohol: Impact Assessment (UK Government, 2012). World Health Organization, Global Status Report on Alcohol and Health 2011 (World Health Organisation, 2011). World Health Organization, Global strategy to reduce the harmful use of alcohol (World Health Organization, 2010). 31 DSICA Submission to the Australian National Preventative Health Agency membership “Free The Spirit” Distilled Spirits Industry Council of Australia Inc. 1st Floor 117 Ferrars Street South Melbourne Victoria Australia 3205 Telephone +61 3 9696 4466 Fax +61 3 9696 6648 All Correspondence: PO Box 1098 South Melbourne Victoria Australia 3205 Website: www.dsica.com.au E-mail: [email protected] ABN: 38754934673 Reg. No. A0025393P








© Copyright 2026