
Sample Aquatic Therapy Evaluation (s/p Total Knee Replacement)
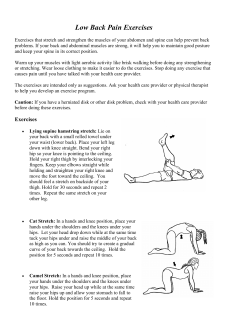
Sample Aquatic Therapy Evaluation (s/p Total Knee Replacement) Evaluation and reassessments should always be performed on land. Goals should all be land-based with the exception of “independent in aquatic exercise” or “transferred to group aquatic class” type goals. Items highlighted in RED pertain specifically to aquatic therapy care. This evaluation has been EXAGGERATED GREATLY for effect. The assessment section (especially) is much longer and much more detailed than necessary; however, this information has been fleshed-out in such detail in order to show therapists how to make the case for medical necessity for any or all of these common complaints. PATIENT INFORMATION Patient name: John Anyman Patient record number: A564917 Patient birth date: 8/12/57 Medical diagnosis/ ICD-9 code: 715.16 (Primary localized OA, lower leg). V43.65 (S/p Total Knee Arthroplasty) Therapeutic diagnosis/ ICD-9 code: 781.2 (Abnormal gait) SUBJECTIVE General medical history – Good health with few comorbidities, except obesity (patient weighs 290# at 5’10”). S/p gall bladder removal > 20 yrs ago. Slightly HOH. No other surgeries per his report. High blood pressure (controlled with meds x 10 years). Takes daily vitamin (over the counter). Works full-time in physical job (Home Depot in gardening department). Participated in tennis and swimming until 6 months ago when knee pain sidelined his efforts. Is very comfortable in water and competent swimmer. Has never performed vertical aquatic exercise or fitness, only horizontal swimming, but arthritic knees always “felt much better” during immersion. Chief complaint – S/p TKA right with swelling, pain, loss of weight-bearing capacity, loss of ROM/strength. History of current episode (including date of onset) – Mr. Anyman has a 5+ year history of bilateral knee pain with R knee pain becoming so unbearable that he agreed to surgery 6 weeks ago. Surgery date was set for 6/1/10. He had attempted conservative management, including 2 cortisone injections and 2 bouts of PT (8 visits; 6 visits) with little to no functional improvement. Neither course of therapy included aquatic intervention. Patient is currently 14 days s/p TKR. He was seen in hospital for 3 days, then received home health until PO day 10. He is ambulatory and has been discharged from home health. Classified as – Acute (s/p surgery) Diagnostic tests already performed and pending – MRI bilateral knees (5/22/10). Arthroscopic surgery right knee 6/1/10. Prior Status – Prior to surgery was working full-time at Home Depot (gardening dept) with knee swelling and pain by 11AM daily. Had to ice knees after work. Was taking ibuprofren “like candy”. Current Status – Is off work for 6 weeks for surgery and rehab. Has wife at home to help. Just graduated from home health PT. Cannot drive. Has difficulty getting into car. Can walk household distances (<100 1| © 2011, Aquatic Therapy University | All rights reserved | www.aquatic-university.com Sample Aquatic Therapy Evaluation (s/p Total Knee Replacement) feet) easily with walker. Pain – 5/10 pain with weight bearing. 8/10 pain with flexion > 45 degree. Mild (3/10) pain with terminal knee extension unless it is held for a prolonged period. When knee is non-weight bearing and held in partial flexion, pain is minimal (<2-3/10). ROM limitations – Cannot lower self into car or onto toilet without “kicking leg out”. Cannot tolerate terminal extension stretch with pillows for > 5 minutes. Weakness – Right leg “buckles” with weight bearing unless using walker. Cannot use right leg to raise or lower self on steps. Doesn’t trust leg “at all”. Aggravating factors – Weight bearing and ROM. Swelling alone stops him from pushing too hard. Relieving factors – Ice, elevation, compression (Ace wrap) and gentle movement (like arc motions on bike). Patient has not returned to swimming pool since surgery; he is looking forward to immersion in pool as he experienced considerable pain relief from immersion prior to surgery. Patient’s goals for therapy – To normalize gait, decrease pain and swelling, gain confidence in weight bearing, be able to sit down on toilet without needing external support, return to driving safely, and return to job without need to ice or medicate at end of day. Wants to return to exercise without pain and feels confident that aquatics is part of that. OBJECTIVE General observations – Patient arrives in clinic using walker with wife by his side. He is limping; does not sustain equal stance time on right leg, even with excessive weight-bearing through upper extremities on walker. His stride length is shortened bilaterally. His right knee is wrapped in an Ace wrap (circumferentially, not figure 8 method). He has obvious edema, effusion and discoloration (purple and yellow bruising) on right shin and ankle. He requires a rest break after ambulating approximately 125’ into gym. He winces with weight bearing and advances limb without normal knee flexion component. He lacks terminal knee extension bilaterally at any point in gait cycle. When he answers questions, he stops walking and shifts full weight onto left leg and upper extremities. Impairments – Only deficits listed Posture – Exaggerated kyphosis. Part of problem is that walker set too low. Slight (<10 degrees), bilateral knee flexion and hip flexion gait posture. ROM – Left knee 10-130 degrees. Right knee 12-66 degrees with overpressure and obvious discomfort. Bilateral hip abduction < 25 degrees. Bilateral hip extension -10 degrees. Strength – Left knee flexion 4-/5, extension 4-/5 (gave to pain). Right knee flexion 3+/5, extension 3+/5 (gave to pain). Bilateral hip extension 3+/5. Right hip abduction 4-/5. Neurological signs – None noted. Palpation – Right knee warm to touch. Effusion present in knee joint. 2+ pitting edema right ankle. 2| © 2011, Aquatic Therapy University | All rights reserved | www.aquatic-university.com Sample Aquatic Therapy Evaluation (s/p Total Knee Replacement) Crepitus left knee. Disabilities – Only deficits listed Functional mobility – Cannot get in and out of car without excessive effort and finessing of position of leg. Cannot stand in kitchen for long enough to prepare even light meal. Wife continues to bring meals in bed or chair. Cannot tolerate any position for >10 minutes; constantly shifting. Transfers – Cannot rise to stand from his sofa or favorite recliner without moderate assistance. Cannot rise to stand from toilet (raised seat) without pulling on wife or grab bar. Cannot lower self down without propping back of left calf on chair and controlling lowering with that leg and bilateral UEs. Balance – Single limb stance on left 8 secs, 6 seconds and 12 seconds (3 trials). Unable to attempt on right. Berg score 32 (see below). Gait – Ambulates with 2 wheeled walker (set too low) with excessive weight on UEs and markedly decreased swing length. Circumducts to clear right leg. No terminal knee extension on either knee. Rests after approx. 125’ by sitting down on bench. Functional tool score (performance tests) – Berg score 32 (out of maximum score of 56). Did not attempt single limb stance, tapping, tandem stance, picking up items, or forward reach. BERG SCORING: 0–20=wheelchair bound 21–40=walking with assistance 41–56=independent Patient comfort in water (check one) Strong swimmer (×××) Prior swimming experience Non-swimmer/feels safe alone Non-swimmer/doesn’t feel safe alone Hydrophobic Medical reason to not leave side (e.g. seizures) Treatment performed today – Eval x 35 minutes (1 unit 97001); Aquatic therapy – 29 minutes (2 units 97113) (35 minutes). Initial evaluation (5 minutes) Patient encouraged to arrive for future appts 15 minutes early to give him time to shower and not have to rush onto pool deck. Oriented to pool including the equipment/ depth/ slope/ temperature/ entry methods. Patient shown how to enter via sloped ramp, leaving walker at top of ramp. (7 minutes) Shown water walking x forward, backward, sidewise, high stepping, cross-over with skilled intervention element (cuing heel strike, terminal knee extension, selecting and adjusting pace). Shown how to maximize hydrostatic pressure’s effect on edematous leg (by maximizing vertical immersion and how to couple this effect with muscle pump to increase circulation. (12 minutes) Therapist instructed patient in water squats, lunges, toe/heel rocks, marching and other gentle, introductory exercises. These exercises will remain skilled care only until pt is able to successfully 3| © 2011, Aquatic Therapy University | All rights reserved | www.aquatic-university.com Sample Aquatic Therapy Evaluation (s/p Total Knee Replacement) execute them; patient will then transition to performing these exercises independently as warm-up or cool-down for PT session and will not be billed for them. (5 mins) Grade I-II joint mobilizations of immersed right knee to decrease pain. Patient tolerance of treatment – Excellent. Patient felt no greater than 2/10 pain during pool session and only experienced small spike (up to 3/10) when got out of water. At ease in water and reports that it “feels like coming home”. Obvious candidate for aquatic therapy. ASSESSEMENT Need for skilled intervention (check one) Patient’s medical condition is unstable (gleaned from general medical history) Patient’s treatment plan requires the skill of a licensed PT to implement plan of care (×××) Rehab potential (check one) Poor (shouldn’t be treated for long — education only) Fair (shouldn’t be treated for long — treat and then assess again to see if still needs skilled care) Good/ Very Good (×××) Excellent (treat for short period then transition) Treatment precautions – New total knee replacement. Cover surgical site with tegaderm and check for signs of infection. General assessment – Patient presents with post-operative lower extremity edema and joint effusion, limb pain, restricted ROM and loss of functional strength. He is unable to weight-bear on the surgical side without limping. He is reliant on an assistive device which alters his postural relationship with the environment. He is in pain, unwilling to move freely or try novel challenges, and is expressing frustration with rehab. I choose to perform 's physician-authorized physical therapy using an aquatic medium in order to capitalize on water's physical properties for the following reasons. Rationale for use of aquatic versus land-based therapy - Immersion in water facilitates treatment of multiple sites simultaneously/ in rapid succession. Immersion also facilitates ease of handling of patient by the therapist and allows positioning and access to patient’s body in a way that is unachievable on land. The thermal properties of water decrease pain and muscle guarding and may improve joint and soft tissue elasticity. Additionally, aquatic-based intervention brings the following to the table, therapeutically: Edema and effusion: Post-surgical effusion and edema creates pain and reduces ROM and strength. Vertical immersion in water produces a pressure gradient which drives pooled venous blood and lymphatic fluid from the lower extremities to the chest. In water, can be directed to exaggerate this effect by performing specific lower extremity exercises to create a venous muscle pump. 4| © 2011, Aquatic Therapy University | All rights reserved | www.aquatic-university.com Sample Aquatic Therapy Evaluation (s/p Total Knee Replacement) Restrictions in ROM: Proper positioning in water provides a low friction surface for movement, encouraging spontaneous active ROM with less effort than when restricted by gravity. Additionally, the water can provide the “ultimate treatment plinth” – allowing a skilled therapist ease of positioning and access for stretching and joint mobilization. Weakness: Water immersion provides a resistive medium that can be manipulated by a skilled therapist to either assist or resist movement. During early rehab, the immersed limb is automatically supported by buoyancy, which will assist in PATIENT moving his body against gravity. As rehab progresses, movements can be accelerated to create more drag. Such activities can be structured to create more effort than the identical movements on land. Pain: Post-surgical pain decreases PATIENT's willingness to move and weight bear, both necessary for healing. During immersion, the properties of buoyancy, viscosity, hydrostatic pressure and thermal shifts couple to create an environment where activities are less painful than their land-based counterparts. This new movement freedom helps interrupt the pain cycle. Weight-bearing restrictons: In water, can be directed to weight-bear in a controlled, graded and progressive manner, merely by choosing an appropriate level of immersion. The buoyant forces present during chest-deep immersion will limit PATIENT's weight-bearing forces to <50% -- even when coupled with moderate exercise. Dependence in ambulation: PATIENT depends heavily on an assistive device (a front wheeled walker) which is creating abnormal movement patterns and teaching him to rely on an artificially expanded support base. Buoyancy can reduce PATIENT's weight by over 90% allowing him the opportunity to relearn normal movement engrams, without use of his upper extremities. Additionally, the water's refraction makes it difficult to trust vision for proper foot placement, requiring to develop kinesthetic awareness of where his surgical limb is in space. Compromised balance: PATIENT's compromised balance places him at risk for post-surgical falls and learned immobility. In the pool, buoyancy provides a safe environment in which to attempt new movements (a necessary component of learning) and to fail without catastrophic consequences (which increases the willingness to try). Additionally, the viscosity of the water allows for increased processing time and ability to right the body, which aids in PATIENT’s ability to generalize and produce the needed corrections on land. Poor endurance: PATIENT was home-bound for the month prior to surgery which means he fatigues quickly and is unable to complete repetitions of motor sequences. The properties of the water can be manipulated to allow for lowered resistance. The therapeutic value of aquatic therapy is essential for PATIENT to not only to gain endurance, but be able to practice gross motor skills without fatiguing in order to facilitate higher motor learning such as bilateral coordination and motor planning. Comorbidities (patient’s obesity): Gait and balance training in the weeks immediately after surgery can result in damage to the new joint. This is compounded when a patient is morbidly obese and can not be trained in natural gait and stair climbing safely. By placing PATIENT in the pool, it is possible to increase 5| © 2011, Aquatic Therapy University | All rights reserved | www.aquatic-university.com Sample Aquatic Therapy Evaluation (s/p Total Knee Replacement) nutrient delivery to the tissue, maximize the osteogenic effects of exercise and provide early return to movement – all without encouraging potentially catastrophic stressors on the new joint. Short term goals Within 2 visits, patient will: 1. Be able to alter his position and movements without cues to maximize the therapeutic properties of water during his sessions 2. Be able to place Tegaderm on surgical knee without assistance 3. Decide whether he will be pursuing aquatic exercise (in group or indeptly) after discharge from aquatic therapy. This will permit therapist to focus on exercise education only as necessary for independence. Long term goals Within 10 visits: patient will: 1. Score 5 points higher on Berg 2. Ambulate without walker (with cane or no assistive device) for 100’ without circumduction to clear limb. Ambulate >500’ with cane without need to rest. 3. Demonstrate 5-115 degrees right knee ROM 4. Be able to single limb stand on right leg for >10 seconds without UE support 5. Report he is able to lower self onto toilet and get into driver’s seat of car without difficulty 6. Report pain <3/10 with all activities except during ROM exercises 7. Report taking no pain pills during daytime hours; continues to ice at-will 8. Perform water walking and simple aquatic exercises with written cues PLAN Skilled physical therapy provided in an aquatic medium by PT for 8-10 visits. Although this care will be billed under the aquatic therapy code (97113), the content of the care will include: Instruction Balance and coordination training Gait, locomotion and balance training Manual therapy (including connective tissue massage, joint mobilization, passive ROM, soft tissue mobilization, therapeutic massage) Motor function training or retraining Neuromuscular education or reeducation Perceptual training Sensory training or retraining ADL training (as appropriate in water) Frequency 2x/week Duration 8-10 visits THERAPIST INFORMATION Therapist’s signature/ Therapist’s title Therapist’s license number Facility name Facility phone/fax 6| © 2011, Aquatic Therapy University | All rights reserved | www.aquatic-university.com Sample Aquatic Therapy Evaluation (s/p Total Knee Replacement) PROGRESS NOTE During the re-evaluation, the following information should be gathered. Patient Information Patient name Patient record number Patient birth date Attendance # 1:1 visits since (insert initial eval date) # monitored visits since (insert initial eval date) # cancellations. Reason for cx. # no shows. Reason for n/s. Subjective Subjective change Impairments Functional limitations Disabilities Functional tool score (if self-report test used) Objective Objective change Impairments Functional limitations Disabilities Functional tool score (if performance test used) Assessment Overall progress Good Fair Poor Mixed Therapy goals status? Patient goals status? New goals/ Revision of existing goals? Rationale for continued need of skilled intervention Patient’s medical condition is unstable Patient’s treatment plan requires the skill of a licensed (insert discipline) to implement Rationale for continued need of aquatic-based treatment Immersion in water facilitates treatment of multiple sites simultaneously/ in rapid succession Immersion in water facilitates ease of handling of patient by therapist Immersion in water allows positioning and access to patient’s body Thermal properties of water decrease pain and muscle guarding Resistance is performed in functional patterns and is velocity-specific, 3-dimensional, graded, and 7| © 2011, Aquatic Therapy University | All rights reserved | www.aquatic-university.com Sample Aquatic Therapy Evaluation (s/p Total Knee Replacement) safe to perform Buoyancy of water allows progressive implementation of weight-bearing Hydrostatic pressure reduces edema in lower extremities Other Plan Continue with existing treatment plan as outlined in initial evaluation Alter treatment as follows (insert treatment changes) Instruction Aerobic endurance exercises Balance and coordination training Body mechanics and ergonomics training Breathing exercises and ventilatory muscle training Breathing strategies Conditioning and reconditioning Developmental activities training Gait, locomotion and balance training Manual therapy (including connective tissue massage, joint mobilization, manual lymphatic drainage, manual traction, passive ROM, soft tissue mobilization and manipulation, therapeutic massage) Motor function training or retraining Neuromuscular education or reeducation Neuromuscular relaxation, inhibition and facilitation Perceptual training Posture awareness training Sensory training or retraining ADL training (as appropriate in water) IADL training (as appropriate in water) Injury prevention or reduction training (as appropriate in water) Organized functional training programs (as appropriate in water) Leisure task adaptation (as appropriate in water) Leisure and play activity training (as appropriate in water) Require new orders for continued care Frequency Duration Awaiting work from referral source re: continuation of care Transfer to group class/ Continue on independent basis at pool (circle which) Therapist Information Therapist’s signature Therapist’s title Therapist’s license number Facility name Facility phone/fax 8| © 2011, Aquatic Therapy University | All rights reserved | www.aquatic-university.com Sample Aquatic Therapy Evaluation (s/p Total Knee Replacement) DISCHARGE NOTE During the final evaluation, the following information should be gathered. Patient Information Patient name Patient record number Patient birth date Medical diagnosis/ ICD-9 code Therapeutic diagnosis/ ICD-9 code Attendance # 1:1 visits since (insert initial eval date) # monitored visits since (insert initial eval date) # cancellations. Reason for cx. # no shows. Reason for n/s. Subjective Subjective change Impairments Functional limitations Disabilities Functional tool score (if self-report test used) Objective Objective change Impairments Functional limitations Disabilities Functional tool score (if performance test used) Summary of Aquatic Treatment Treatment Patient tolerance of treatment Assessment Overall progress Good Fair Poor Mixed Therapy goals achieved? Patient goals achieved? Rationale for discharge? Plan Plan is to: Transfer to land-based therapy 9| © 2011, Aquatic Therapy University | All rights reserved | www.aquatic-university.com Sample Aquatic Therapy Evaluation (s/p Total Knee Replacement) Transfer to aquatic group class Transfer to independent aquatic exercise Discharge from all intervention Therapist Information Therapist’s signature Therapist’s title Therapist’s license number Facility name Facility phone/fax 10 | © 2011, Aquatic Therapy University | All rights reserved | www.aquatic-university.com









© Copyright 2026