
SAMPLE FOR CERTIFICATION OF NURSE ASSISTANTS OR HOME HEALTH AIDES A1226 Certification
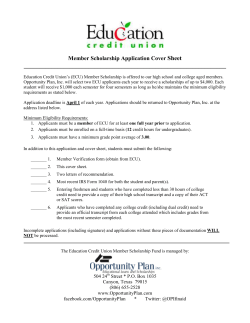
SAMPLE FOR CERTIFICATION OF NURSE ASSISTANTS OR HOME HEALTH AIDES REQUEST FOR LIVE SCAN SERVICE Applicant Submission ORI: A1226 Code assigned by DOJ Type of Application: Certification Job Title or Type of License, Certification, or Permit: Certified Nurse Assistant (CNA) or Home Health Aide (HHA) Agency Address Set Contributing Agency: 03314 California Department of Public Health (CDPH) Mail Code (five-digit code assigned by DOJ) (leave blank) Agency authorized to receive criminal history information Contact Name (Mandatory for all school submissions) MS 3301, P.O. Box 997416 ( Street or PO Box 95899-7416 Sacramento, CA City, State Name of Applicant: (Please print) Zip Code Your full name Last AKA's: Other names known as DOB: Date of birth Last SEX: Height Eye color: Color POB: Place of birth First CDL No.: First (Check one) Male Female MI California Drivers License Number Misc. No.: BIL - Weight Hair color: Color HT: WT: Misc. No.: Not applicable Agency Billing Number (if applicable) Your telephone number Home Address: (Applies only if Youth Org/HRA or Public Utility Submission) Your mailing address Street or PO Box Social Security Number: Your Number: (leave blank) ) Contact Telephone No. *Social Security Number (Required by CDPH) City, State and Zip Code *Social Security Number (Required by CDPH) OCA No. (Agency Identifying No.) Level of Service If resubmission, list Original ATI No. Employer: DOJ FBI (Additional response for Department of Social Services, DMB/CHP licensing, and Department of Corporations submissions only) (Leave blank) Employer Name (Leave blank) Street No. Mail Code (five digit code assigned by DOJ) Street or PO Box ( City State Zip Code Live Scan Transaction Completed By: Transmitting Agency Name of Operator ) Agency Telephone No. (Optional) Date ATI No. Amount Collected/Billed BCII 8016 (Rev 11/08) SAMPLE ORIGINAL-Live Scan Operator; SECOND COPY-CDPH; THIRD COPY-Applicant NOTE TO APPLICANT: *Please input your Social Security Number (SSN) where required. The submission of your SSN will allow results to be transmitted from DOJ to CDPH accurately and timely. Failure to submit your SSN could cause delay in your certification.










© Copyright 2026