
Australian Public Assessment Report (AUSPAR) for Romiplostim
SAMPLE AUSPAR Australian Public Assessment Report (AUSPAR) for Romiplostim Proprietary Product Name: Nplate Submission No: 2007-3359-4 Sponsor: Amgen Australia Pty Ltd July 2008 SAMPLE AUSPAR Contents I. Introduction to Product Submission ........................................................................3 Product Details........................................................................................................................ 3 Product Background................................................................................................................ 3 Status in Other Countries at the time of Submission .............................................................. 4 II. Quality.........................................................................................................................4 Drug Substance ....................................................................................................................... 4 Drug Product ........................................................................................................................... 5 Quality Summary and Conclusions......................................................................................... 6 III. Non-Clinical................................................................................................................6 Introduction............................................................................................................................. 6 Pharmacology.......................................................................................................................... 6 Pharmacokinetics .................................................................................................................... 7 Toxicology .............................................................................................................................. 8 Non-Clinical Summary and Conclusions.............................................................................. 13 IV. Clinical ......................................................................................................................13 Introduction........................................................................................................................... 13 Pharmacokinetics .................................................................................................................. 14 Pharmacodynamics ............................................................................................................... 15 Efficacy ................................................................................................................................. 16 Safety .................................................................................................................................... 22 Clinical Summary and Conclusions ...................................................................................... 27 V. Overall Conclusion and Risk/Benefit Assessment ................................................28 Quality................................................................................................................................... 28 Non-Clinical.......................................................................................................................... 28 Clinical .................................................................................................................................. 29 Risk-Benefit Analysis ........................................................................................................... 30 Recommendation .................................................................................................................. 31 Page 2 of 31 SAMPLE AUSPAR I. Introduction to Product Submission Product Details Type of Submission: Decision: New biological entity Approved Date of Decision Active ingredient(s): Romiplostim Product Name(s): Nplate Dose form(s): Powder for Injection Strength(s): 375 micrograms and 625 micrograms Container(s): Type I glass vial (5 mL) with an elastomeric stopper and an aluminium seal with flip-off dust cover Pack size(s): Single vial Therapeutic use: Treatment for thrombocytopenia in adult patients with chronic immune (idiopathic) thrombocytopenic purpura (ITP): who are non-splenectomised and have had an inadequate response or are intolerant to corticosteroids and immunoglobulins; who are splenectomised and have had an inadequate response to splenectomy. Route(s) of administration: Subcutaneous injection Dosage: Weekly administration. Starting dose 1 microgram/kg, with weekly adjustments in 1 microgram/kg intervals until platelet levels between 50 and 200 x 109/L. Maximum dose 10 microgram/kg. Product Background Immune (idiopathic) thrombocytopenic purpura (ITP) is an autoimmune disorder in which thrombocytopenia results when platelets are destroyed more rapidly than they can be produced. Platelet consumption is mediated by antiplatelet glycoprotein autoantibodies. The presence of antiplatelet autoantibodies results in a decrease in platelet counts due to the clearance of platelets, typically by the reticuloendothelial system of the bone marrow, spleen, and/or the liver. Thrombocytopenia, when severe (i.e., < 30 × 109/L platelet count), can result in spontaneous bruising or bleeding and occasionally can lead to death. Chronic ITP is a serious and lifethreatening condition that affects more adult women than men (approximately 2:1). The incidence of ITP in the US is estimated as 58 to 66 new cases per million population per year, or approximately 16,000 new cases per year (McMillan, 1997). Current treatments for ITP target modulation of the immune system and include corticosteroids such as prednisone, intravenous (IV) immunoglobulin infusions (IVIG), and/or anti D immunoglobulin infusion (WinRho®), splenectomy, and various salvage treatments for the refractory patient. Most current treatments for ITP have limited chronic efficacy, intolerable side effects, and/or have significant convenience issues with respect to their administration, and therefore an unmet medical need exists for patients with ITP. Page 3 of 31 SAMPLE AUSPAR Romiplostim is a novel thrombopoiesis-stimulating protein that has been developed as a treatment for adults with thrombocytopenia associated with ITP. Romiplostim is a recombinant protein that is expressed in Escherichia coli (E coli). It has an Fc domain and 4 Mpl (thrombopoietin receptor)binding domains. Romiplostim stimulates platelet production by a mechanism similar to that of endogenous thrombopoietin (eTPO). Romiplostim was known as AMG 531 during the clinical development programme. Status in Other Countries at the time of Submission A similar application has been submitted in the US (23 October 2007), European Union (EU) (2 November 2007) and Canada (16 November 2007). Orphan designation has been granted in the US and EU, and priority review has been granted in Canada and Australia. Amgen is participating in the pilot Parallel Review Project between Health Canada’s BGTD and the TGA in this submission. Romiplostim is not yet approved in any country. II. Quality Drug Substance Structure The drug substance, romiplostim or AMG 531, is a recombinant non-glycosylated 59 kDa thrombopoietic protein produced in E. coli. It is termed a peptibody comprising of two identical subunits. Each subunit consists of a human immunoglobulin IgG1 Fc domain at the N-terminus which is fused at the C-terminus to two thrombopoietin receptor binding domains (TRBD). AMG 531 is non-glycosylated and has no amino acid sequence homology to endogenous thrombopoietin. Figure 1. Manufacture The drug substance is manufactured at Amgen Inc, Boulder, CO, USA. It is expressed from an expression vector in E. coli. Cell banking processes are satisfactory. The commercial manufacturing process uses E. coli fermentation and cell processing unit operations to produce a process intermediate (slurry). The purification process begins with slurry thaw followed by solubilization. Romiplostim is purified using a series of chromatography, concentration and diafiltration steps to produce purified bulk active substance. Page 4 of 31 SAMPLE AUSPAR All viral/prion safety issues have been addressed, including use of animal-derived excipients, supplements in the fermentation process and in cell banking. Manufacturing Process Development The drug substance manufacturing process was developed to optimize the process for commercial production. Analytical comparability studies have been executed to support the manufacturing process changes during development. Physical and Chemical Properties Various techniques have been used to confirm and characterise the primary, secondary and tertiary structure of romiplostim. The molecule is comprised of two identical subunits. Each subunit consists of a human immunoglobulin IgG1 Fc domain at the N-terminus which is fused at the Cterminus to two thrombopoietin receptor binding domains (TRBD), with each binding domain consisting of a 14-amino acid sequence. Charge heterogeneity of the romiplostim molecule as a result of amino acid substitution, deamidation, oxidation and manufacturing process conditions have been characterised. Biological characterisation showed that romiplostim increases platelet production via interaction with the thrombopoietin receptor (referred to as Mpl) on megakaryocytes, which activates intracellular transcriptional pathways, and thereby, results in stimulation platelet production. Romiplostim is not glycosylated as it is synthesised in E coli. Assessment of product–related impurities was accomplished through forced degradation studies. The results of these studies identified product- and process- related impurities and showed consistency in their removal through the purification process. Specifications The proposed specifications, which control identity, content, potency, purity and other biological and physical properties of the drug substance relevant to the dose form and its intended clinical use, where provided for evaluation. Appropriate validation data was submitted in support of the test procedures. Stability The stability programme, including the testing intervals and temperature storage conditions, has been designed in accordance with the relevant guidelines. The tests chosen are a subset of tests from the release specifications selected for stability-indicating properties. Stability of the active substance was evaluated at the recommended storage temperature and under other conditions. The stability program consisted of clinical lots, commercial lots and data from the initial generation process. The stability data provided are within the specifications and the storage period at the recommended storage temperature is accepted. Drug Product Formulation(s) AMG 531 drug product is supplied as a sterile, preservative free lyophilized white powder ready for reconstitution. It is supplied for single use in 5 mL Type I glass vials containing 375 or 625 µg of AMG 531, 250 or 500 µg deliverable drug product, respectively. Manufacture The product is manufactured in Italy and sterilised by filtration. Assessment of drug product comparability includes biochemical, biophysical, biological, and structural comparisons, as well as stability under stressed (high temperature) and recommended storage conditions. Process-related impurities, formulation parameters, and other drug product Page 5 of 31 SAMPLE AUSPAR parameters were also compared. Drug product has been demonstrated to be comparable throughout development. Specifications The proposed specifications for the drug product were supplied for evaluation. Appropriate validation data have been submitted in support of the test procedures. Stability Stability data have been generated under stressed and real time conditions to characterise the stability profile of the product. Photostability data showed that the product is not photostable. The proposed shelf life of 36 month expiry period for drug product stored at the recommended storage condition of 2-8°C is supported by real time data submitted. Additionally, an in-use shelflife of up to 24 hours when reconstituted and held at 2°C to 8°C in the vial, protected from light, is also proposed. The proposed shelf-life of the drug product is acceptable. Quality Summary and Conclusions The administrative, product usage, chemical, pharmaceutical, microbiological and biopharmaceutic data (as applicable) submitted in support of this application have been evaluated in accordance with the Australian legislation, pharmacopoeial standards and relevant technical guidelines adopted by the TGA. All Module 3 issues have been resolved. There is no objection to the registration of NPLATE on quality grounds. III. Non-Clinical Introduction The general quality of the submitted studies was high. All safety-related studies were conducted under GLP conditions with the exception of a study on antigenicity, which was conducted in an established laboratory and adequately documented. Pharmacology Primary pharmacodynamics In vitro, romiplostim was shown to bind to human c-Mpl with nanomolar or subnanomolar affinity, and to also target the c-Mpl of mice, rats and monkeys. Agonism of the receptor was demonstrated by phosphorylation of c-Mpl and its downstream effector JAK2 in human platelets following exposure to romiplostim, and by the drug’s enhancement of the sensitivity of human and rabbit platelets to ADP-induced aggregation. Stimulation of megakaryopoiesis was shown in cultures of bone marrow cells (human, baboon, cynomolgus monkey and rhesus monkey) treated with romiplostim. In vivo, administration of a single dose of romiplostim by the proposed clinical route (SC) resulted in dose-dependent increases in platelet counts in mice, rats, rhesus monkeys and cynomolgus monkeys. It took several days for the increase in circulating platelets to first become apparent, reflecting the time required for megakaryocyte maturation (Hartwig and Italiano, 2003); peak increases were observed 5–11 days post-dose. Examination of bone marrow samples taken from monkeys 3 days after treatment with romiplostim revealed proliferation and maturation of megakaryocytes. Romiplostim displayed efficacy in a murine model of ITP, including in splenectomised animals. The platelets induced by romiplostim treatment were shown to be functional in repeat-dose toxicity studies conducted in rats and rhesus monkeys. The in vivo data reveal that the laboratory animal species used in the toxicity studies are vastly less sensitive to the thrombopoietic effect of romiplostim than humans. In combined Page 6 of 31 SAMPLE AUSPAR pharmacodynamic/pharmacokinetic studies, a single SC dose of romiplostim at 2 µg/kg caused a peak increase in platelets of 2.5-fold in healthy humans (AUC0–∞, 4.6 ng·h/mL; Study 20000109), compared with a 2.5-times increase observed in rats at 30 µg/kg (AUC0–∞, 793 ng·h/mL; Study 100909), a 2.3-times increase in rhesus monkeys at 500 µg/kg (AUC0–∞, 49500 ng·h/mL; Study 100998) and a 4.6-times increase in cynomolgus monkeys at 5000 µg/kg (AUC0–∞, 56000 ng·h/mL). The basis for this is unclear, and not predicted by in vitro data, nor due to drugneutralising antibodies. Secondary pharmacodynamics and safety pharmacology Romiplostim displayed no significant secondary activity against a panel of 63 other targets (comprising receptors, ion channels, transporters and enzymes). IC50 values for inhibition of ligand binging/enzyme activity were all >2 µM (i.e., >14000-times higher than the clinical Cmax 1 ). Examination of the potential cross-reactivity of romiplostim for selected human and cynomolgus monkey tissues was attempted using immunohistochemical techniques but was of limited value as no specific reactivity could be demonstrated for the drug in any of the experiments, including to c-Mpl-expressing cells. Specialised safety pharmacology studies examined potential effects on the CNS and cardiovascular system. Effects on the respiratory system were examined in a 3-/6-month repeat-dose toxicity study in monkeys. CNS function was unaffected in rats with treatment up to 100 µg/kg SC, a dose producing a peak serum concentration of romiplostim ~4-times the clinical Cmax. There were no changes in ECG, blood pressure or heart rate in cynomolgus monkeys after IV administration of romiplostim at doses up to 5000 µg/kg, where serum levels of romiplostim were >5000-times the clinical Cmax. No ECG abnormalities were observed in the repeat-dose toxicity studies conducted with cynomolgus and rhesus monkeys but the examinations were performed days after drug administration. There was no in vitro examination of the potential for inhibition of the hERG K+ channel current. Respiration was unaffected in cynomolgus monkeys at serum concentrations ~200-times higher than the clinical Cmax (4 h after dosing at 5000 µg/kg SC). Pharmacokinetics Absorption of romiplostim into the systemic circulation after SC administration was slow in all species studied, with peak serum concentrations typically reached 12 h post-dose in rats and rabbits, 4–8 h post-dose in monkeys and 24 h post-dose in humans. Terminal elimination following SC administration was also slow, with t½ values of 17–21 h observed in rats, 110–195 h in rhesus monkeys, 296 h in cynomolgus monkeys and 56 h in humans. Serum AUC after SC administration was generally seen to be greater than dose-proportional in rats and less than dose-proportional in monkeys, but this is considered to reflect the higher and wider range of doses studied in monkeys cf. rats rather than a species difference in the drug’s pharmacokinetics. The presence of antibodies to romiplostim did not affect the pharmacokinetics of romiplostim in monkeys. Whether antiromiplostim antibodies affect exposure in rats could not be ascertained as different animals were used in the antibody and pharmacokinetic analyses. Thrombocytopenia was associated with increased systemic exposure to romiplostim in mice at 3 µg/kg IV, but not at 30 µg/kg, suggesting that binding by platelets (mediated by c-Mpl and overwhelmed at high doses) is involved in drug clearance, just as it is for endogenous thrombopoietin (Fielder et al., 1996). The Clinical Overview indicates that this effect was more readily demonstrated in the clinical studies (as they involved low, therapeutic doses of romiplostim). With repeat dosing, exposure to romiplostim declined as platelet count improved. Volume of distribution exceeded the whole blood volume in all species (mice, rats, cynomolgus monkeys, rhesus monkeys and humans), indicating extravascular distribution. Accordingly, 1 Based on a value of 8 ng/mL, as predicted at the maximum recommended human dose of 10 µg/kg in patients with a baseline platelet count of 5 × 109/L Page 7 of 31 SAMPLE AUSPAR widespread tissue distribution of radioactivity was observed in female rats after IV administration of 125I-romiplostim. Besides the thyroid, the kidneys, bone marrow (the target tissue), liver, lung and ovary displayed the highest peak tissue concentrations of radioactivity relative to serum. Penetration of the blood-brain barrier was poor. Tissue levels of radioactivity declined slowly. Protein binding by romiplostim was not examined. No conventional metabolism studies were conducted, which is acceptable for a protein drug as degradation to small peptides and individual amino acids is expected. The majority of radioactivity in serum (91–95%) and selected tissues (≥ 84%) in the distribution study was observed to be TCAprecipitable, indicating that it is associated with intact romiplostim or large fragments of the molecule. Significant loss of the thrombopoietin mimetic peptide portion of the drug was indicated by the serum AUC0–∞ for romiplostim determined by the standard ELISA technique (involving a secondary antibody directed against the thrombopoietin mimetic binding portion of the molecule) being ~40% of that for total or TCA-precipitable radioactivity (the radiolabel assumed to be present on the Fc domain of the molecule) and a similar percentage of the AUC for species detected by an alternative ELISA technique in which a secondary antibody against the Fc domain was used. Excretion of 125I-romiplostim-derived radioactivity following IV dosing in rats was predominantly via the urine, principally in the form of small peptides or free iodide (88% of the dose was excreted renally and 11% of the total radioactivity recovered in urine was TCA-precipitable). The importance of renal excretion to the clearance of romiplostim was also demonstrated in a single-dose pharmacokinetic study in rats (Study 101402), where AUC0–12 h for serum romiplostim was 26– 80% higher in bilaterally nephrectomised animals cf. sham-operated controls. Routes of excretion were not examined in other laboratory animal species nor in humans. Toxicology Acute toxicity One single-dose toxicity study, conducted in rats and using the proposed clinical route, was submitted. The study established a maximum non-lethal dose for romiplostim by the SC route of ≥ 1000 µg/kg in the rat. Platelets were increased at all dose levels tested (100, 300 and 1000 µg/kg; by up to 3.2-times 9-days post-dose), as expected. Modest reductions in red blood cell counts and indices (≤ 12%) were seen from the low- or mid-dose level and are consistent with the drug’s pharmacological activity — the stimulation of megakaryopoiesis resulting in suppression of erythropoiesis due to stem-cell competition (van Zant and Goldwasser, 1979). Increased splenic extramedullary haematopoiesis and increased bodyweight-relative spleen weight, observed in highdose animals, are considered to be compensatory responses to the haematological changes. No further studies, involving IV administration or conducted in a second species, were submitted. This deficiency is largely overcome by data provided by the repeat-dose toxicity studies. Repeat-dose toxicity Studies of up to 4 weeks duration were conducted in rats, 4 weeks in rhesus monkeys and 6 months in cynomolgus monkeys. All involved SC administration (the clinical route); additional groups of animals were employed in the 4-week rat and rhesus monkey studies to receive the highest dose level IV. These species are appropriate models of romiplostim-toxicity given their pharmacodynamic responsiveness to the drug, but it must be noted that their responsiveness is substantially less than that of humans, especially so for monkeys. Numbers of animals and the use of both sexes (in the definitive studies) were appropriate. Suitable doses were used, with the selection of the high-dose levels based on their production of a maximal increase in platelet counts (rats and monkeys) and/or a substantial multiple of the anticipated clinical exposure level (monkeys). The dosing frequency in the 3- and 6-month monkey study was the same as that to be used in patients (once weekly); dosing in the other studies was 3-times weekly. Studies in rats longer than 4 weeks were not feasible due to the development of drug-neutralising antibodies. At 6 months, the duration of the pivotal monkey study was consistent with the length generally Page 8 of 31 SAMPLE AUSPAR considered appropriate under ICH guidelines for a chronically administered, biotechnology-derived drug. However, it is considered that such a study would be unlikely to yield any further insight into the drug’s toxicology given that no significant progression in toxicity was observed over the course of 1 to 6 months in the species. The use of cynomolgus rather than rhesus monkeys in this chronic study was prudent given their lesser immunological response to the drug. Relative exposure Exposure ratios have been calculated based on animal:human serum AUC0–168 h values for romiplostim (see Table 1) 2 . Animal AUC0–168 h values have been calculated based on AUC values for shorter periods (0–24 h or 0–48 h) multiplied by an appropriate factor according to the dosing frequency. This approach is a conservative one, recognised to underestimate the actual AUC0–168 h value (and, consequently, the relative exposure level), made necessary by the limited toxicokinetic sampling regimen employed in the studies. Table 1 Study 100876 Relative exposure in repeat-dose toxicity studies Species & strain Rat (SD) Treatment duration 4 weeks Dosing frequency 3/week Route SC IV 100877 Monkey (rhesus) 4 weeks 3/week SC IV 101158 Monkey (cynomolgus) 4 weeks 3/week SC Monkey (rhesus) 101814 108644 Monkey (cynomolgus) 6 months Human (platelet count, 5 × 109/L) 1/week 1/week SC SC Dose (µg/kg) AUC0–168 h (ng·h/mL) Exposure ratio† 30 651a 0.8 100 7350 9 100 13710a 16 500 142500a 168 1000 184500a 217 5000 1023000a 1204 5000 3510000a 4129 100 717b 0.8 300 5100b 6 500 8700 5000 a b 10 b 120600 142 5000 209400 b 246 500 1920c 2 1000 4190 5 5000 20100 24 10# 850 – c c † = calculated as animal:human AUC0–168 h ; a = estimated by multiplying AUC0–48 h by 3; b = estimated by multiplying AUC0–24 h by 3; c = AUC0–24 h; AUC values are for the sexes combined; # = the maximum recommended clinical dose 2 The author of the Nonclinical Overview calculated relative exposure levels using a lower human AUC0–168 h value at 10 µg/kg SC than has been used here. This was extrapolated linearly from data obtained in healthy human volunteers given romiplostim at 2 µg/kg SC (Study 20000109). Given the size of the extrapolation, the uncertainty of the dose proportionality and the demonstration of increased exposure with thrombocytopenia, a higher, more conservative value (derived from modelling performed by the Sponsor) has been used for calculating relative exposure levels in this report. Page 9 of 31 SAMPLE AUSPAR Major findings Changes attributable to the drug’s pharmacological activity, produced either directly or indirectly, were the predominant findings in the studies. Stimulation of thrombopoiesis by romiplostim, indicated by significantly increased platelet count, was apparent at every dose level in every study. With 3-times weekly administration, the highest SC doses used in the studies produced increases in platelets of 3.6-times in rats (100 µg/kg), up to 7.4times in rhesus monkeys (5000 µg/kg) and 5.7-times in cynomolgus monkeys (5000 µg/kg); platelet counts in cynomolgus monkeys treated with romiplostim once weekly at 5000 µg/kg SC were on average 2.9-times higher than controls. Stimulation of megakaryopoiesis was usually evident upon microscopic examination of the bone marrow of treated animals, and was additionally observed in the spleen of rats. Megakaryocytes were detected in the lung and liver of rats and monkeys and the submandibular lymph node of cynomolgus monkeys. Alterations in mean platelet volume, with increases observed in rats and decreases in monkeys, also indicate an effect on megakaryocyte maturation and/or platelet life-cycle. Bodyweight-relative spleen weights were higher in treated animals cf. controls, an effect consistent with the increased demand for clearance of platelets from the blood and also extramedullary haematopoiesis. Other findings considered to be related to increased platelet count were enhanced platelet aggregation and incidents of haemorrhage at the injection site in the 4-week rhesus monkey study (100877; all dose levels), haemorrhage and eosinophilic substance in blood vessels in the lungs of rhesus and/or cynomolgus monkeys treated at 5000 µg/kg SC × 3/week for 4 weeks (Study 101158), increased serum inorganic phosphorous and potassium in the 4-week rat study (100876; at all dose levels; as previously observed in the single-dose study in rats and consistent with ex vivo release), and increased serum lactate dehydrogenase in both 4-week monkey studies (100877 and 101158; at 5000 µg/kg × 3/week, SC or IV; also reflecting release from platelets ex vivo in blood samples taken for clinical chemistry [Rothwell et al., 1976]). Mortality in rats, observed at all dose levels and without prior clinical signs, might have been due to stroke or other thromboembolic events, caused by increased blood viscosity owing to the elevation in platelets (histological evidence for this was, however, lacking). There were no deaths in the monkey studies. Treatment with romiplostim produced dose-dependent hyperostosis of trabecular bone (at ≥ 30 µg/kg × 3/week) and myelofibrosis (at all dose levels 3 ) in rats. The effect on bone growth is consistent with the increase in megakaryocytes induced by the drug, with the cells recognised to influence skeletal homeostasis by stimulating the proliferation and activity of osteoblasts and inhibiting that of osteoclasts (Kacena et al., 2004, 2006; Beeton et al., 2006). Myelofibrosis has been observed in rats treated with pegylated recombinant human thrombopoietin (Yanagida et al., 1997) and mice that overexpress thrombopoietin (Yan et al., 1996) and is attributed to the increased release of cytokines such as transforming growth factor-β and platelet-derived growth factor from the elevated number of megakaryocytes. These changes were absent in monkeys, even in animals showing marked megakaryocytic hyperplasia in bone marrow. A generalised increase in leukocytes was observed in rats at ≥ 30 µg/kg × 3/week and cynomolgus and rhesus monkeys treated at 5000 µg/kg × 3/week. This is consistent with the drug’s activation of c-Mpl on pluripotent haematopoietic stem cells. Reductions in red blood cell counts and/or indices were apparent at all dose levels in the rat study and at 5000 µg/kg × 3/week (SC or IV) in rhesus monkeys, mirroring findings in the single-dose rat study. Erythroid hypoplasia, minimally severe, was observed in rhesus monkey bone marrow. The likely basis for these findings is inhibition of erythropoiesis due to the diversion of stem cells to the megakaryocytic pathway. Findings of extramedullary haematopoiesis in the spleen, liver and/or lymph nodes of treated animals are likely 3 The incidence among low-dose animals was 1/20, and this single case was of minimal severity. Page 10 of 31 SAMPLE AUSPAR to be compensatory responses to anaemia. No effects on white or red blood cell counts/indices were observed in the 6-month monkey study. Ovarian cysts were observed at an incidence and level of severity considered by the Sponsor to be above background levels at doses ≥ 1000 µg/kg × 3/week in the first monkey study, conducted in rhesus animals. This finding was not reproduced in a subsequent study, and no ovarian changes were observed in cynomolgus monkeys, nor rats. The findings of the initial study are therefore considered to be incidental and no effect of romiplostim on the ovaries is indicated. Inflammatory changes at the SC injection site were more frequent and/or more severe in treated monkeys cf. controls. They were, at most, of moderate severity, and more usually slight or very slight. The most severe findings were in rhesus monkeys, in which romiplostim was more immunogenic than in cynomolgus monkeys. Chronic inflammation was observed at the SC injection site in rats, but its relationship to treatment was unclear. All haematological, clinical chemistry and histopathological changes were shown to be reversible upon withdrawal of treatment. In most instances they were fully resolved within 4 weeks. Genotoxicity In line with ICH guidelines, no genotoxicity studies were conducted with romiplostim. Given its size and composition, the drug is not expected to interact directly with DNA or other chromosomal material. Carcinogenicity No carcinogenicity studies were conducted. While such studies are generally inappropriate for biotechnology-derived products, romiplostim’s activity as a growth factor mimetic poses cause for concern regarding its carcinogenic potential. Lifetime studies in rodents would not be feasible, though, because of the development of drug-neutralising antibodies; the absence of carcinogenicity studies is therefore acceptable. Thrombopoietin has been shown to stimulate the proliferation of a subset of acute myeloblastic leukaemia cells in vitro (Matsumura et al., 1995; Fontenay-Roupie et al., 1998; Corazza et al., 2006). Accordingly, stimulation of existing myeloid leukaemias in patients treated with romiplostim is possible. A statement to this effect appears in the draft Product Information document. No expression of c-Mpl was detected by Graf et al. (1996) in cell lines derived from 21 different solid tumour types or by Columbyova et al. (1995) in 11 primary malignant human tissues, indicating stimulation of other tumour types is unlikely. Reproductive toxicity Reproductive toxicity studies submitted by the Sponsor covered all stages (fertility, early embryonic development and pre- and post-natal development). Numbers of animals in the definitive studies and the timing and duration of treatment were appropriate. Drug administration was by the clinical route. Page 11 of 31 SAMPLE AUSPAR Table 2 Relative exposure Study Species & strain Day of sampling; (treatment period) Dose (µg/kg) AUC0–168 h† (ng·h/mL) Exposure ratio* 59.5 0.07 Rat (SD) GD19; (every second day from GD7–GD19) 10 101948 30 644 0.8 100 2566 3 10 1001 1.2 30 4515 5 100 19040 22 10# 850 – 101949 108644 Rabbit (NZW) GD19; (every second day from GD7–GD19) Human (platelet count, 5 × 109/L) * = calculated as animal:human AUC0–168 h ; † = estimated in laboratory animal species by multiplying AUC0–48 h by 3.5; # = the maximum recommended clinical dose Placental transfer of romiplostim was demonstrated in rats. No studies were conducted in lactating animals to examine the potential for excretion in milk. Such excretion is expected, though, based on the presence of the IgG1 Fc domain in romiplostim. Male and female fertility were unaffected in rats treated with romiplostim at doses ≤ 100 µg/kg, administered 3-times weekly (estimated relative exposure, ≤ 9 [based on data from Study 100876]), and no adverse effects on embryofetal development were observed in rats up to the same dose level, administered on alternate days during gestation (relative exposure, ≤ 3). Higher doses could have been used in these studies as no significant maternotoxicity was encountered. This would go some way to compensate for the development of drug-neutralising antibodies, seen to be particularly frequent in the fertility study (antibody analyses were not performed in the definitive embryofetal development study). Additional embryofetal development studies were conducted in mice and rabbits. These were limited, performed with only a small number of animals and involving only external examination of foetuses. Post-implantation loss was increased in mice treated with romiplostim at 100 µg/kg every third day, a maternotoxic dose (suppressing maternal body weight gain by 8%); no increase in fetal external abnormalities was observed. In the rabbit study, a single fetus of a dam treated at 100 µg/kg every second day displayed multiple malformations (gastroschisis, ectrodactyly and cutis aplasia). This dose was maternotoxic, suppressing maternal body weight gain by almost 50%. No follow-up study was conducted in rabbits to establish whether this single finding was treatment-related. This was due to the lack of pharmacodynamic responsiveness of the species (no increase in platelets could be demonstrated), indicating that the rabbit is not an appropriate model for romiplostim toxicity. The set of studies examining the potential embryofetal toxicity of romiplostim is not ideal, with a definitive study available for only a single species and in it only low exposure multiples achieved. Pups of rats treated at 100 µg/kg, administered every second day, were more likely to be stillborn, with a 9.5-fold increase in incidence observed overall and a 14-fold increase apparent when considering only pups of dams without drug-neutralising antibodies. Pup survival to PND4 was also decreased at this dose level (88% cf. 97% in controls). Survival over PND5–PND21 was, however, unaffected. Pup birth weight was normal and no adverse effects on development were observed at ≤ 30 µg/kg or in surviving 100 µg/kg pups. Paediatric use Romiplostim is not proposed for paediatric use and no specific studies in juvenile animals were submitted. Page 12 of 31 SAMPLE AUSPAR Non-Clinical Summary and Conclusions • The nonclinical dossier contained no major deficiencies. Certain studies that would have been desirable were not feasible. These were a chronic study in rodents (precluded by the development of drug-neutralising antibodies) and an embryofetal development study in a second, non-rodent species (the usual species used, the rabbit, is an inappropriate model for romiplostim toxicity because it is not pharmacologically responsive to the drug). • Primary pharmacology and toxicity studies, showing large increases in platelets, demonstrated to be functional, following treatment with romiplostim, support the drug’s use for the proposed indication. Efficacy in a murine model of ITP was shown. • Treatment-related findings in the toxicity studies are considered to represent desired pharmacological effects (stimulation of megakaryopoiesis and thrombopoiesis), additional pharmacological effects mediated by c-Mpl (a generalised stimulation of leukocyte production), secondary effects related to megakaryocytic stimulation (inhibition of erythropoiesis and compensatory responses to anaemia, hyperostosis of trabecular bone and myelofibrosis) and effects related to the induced thrombocytosis (haemorrhage, artefactual changes in clinical chemistry and probably mortality in rats). The most prominent toxic effects — hyperostosis and myelofibrosis — were absent in monkeys. • These exaggerated pharmacological effects, which were all demonstrated to be reversible, are considered likely to be of limited clinical relevance. This is based on their occurrence at dose levels beyond that required for significant stimulation of thrombopoiesis and/or their confinement to rodents. • The absence of studies investigating the genotoxicity and carcinogenicity of romiplostim is acceptable. There is a concern that, as a thrombopoietin mimetic, romiplostim may potentially stimulate the growth of existing myeloid leukaemias. • A marked increase in stillbirths and decreased perinatal survival in pups of rats treated with romiplostim at a relative exposure level of 3 (based on animal:human serum AUC) justify the drug’s placement in Pregnancy Category B3. • There are no nonclinical objections to registration of romiplostim for the proposed indication. IV. Clinical Introduction The marketing application includes data from 13 clinical studies: 9 clinical studies in subjects with immune (idiopathic) thrombocytopenic purpura, 2 pharmacology studies in healthy subjects, and 2 studies in other indications. In total 204 ITP subjects have received romiplostim. Page 13 of 31 SAMPLE AUSPAR Table 3 Clinical Pharmacology Studies Pharmacokinetics Absorption For Study 20000109, mean romiplostim serum concentration-time profiles after IV administration are presented in Figure 2. After SC administration, serum romiplostim concentrations were not measurable for all subjects at all timepoints in the 0.1, 0.3, and 1.0 μg/kg cohorts. At 2.0 μg/kg, serum concentrations of romiplostim were not measurable at any timepoints for 3 out of 8 subjects and were measurable at the earliest 12 hours postdose and only up to 48 hours postdose for the other 5 subjects. Half-life and absolute bioavailability could not be reliably estimated; however it was evident that serum exposure to romiplostim after SC administration was lower than that after IV administration. After SC administration, peak concentrations were observed between 24 and 36 hours after dosing. Figure 2: Study 20000109 - Mean (SD) Concentration-Time Profiles of Romiplostim after Single IV or SC Administration of Romiplostim in Healthy Subjects (M2.7.2, v3, p14) Page 14 of 31 SAMPLE AUSPAR Distribution After a single IV dose, serum exposure to romiplostim (C0 and AUC0-t) increased more than proportionally with dose and the initial volume of distribution decreased with dose. Findings suggested that romiplostim presumably binds to c-Mpl on platelets and other cells in the thrombopoiesis lineage, such as megakaryocytes, and is then internalised and degraded inside these cells. Bioavailability Most of the studies in the clinical development programme, including the two pivotal phase III studies, used material produced by a clinical manufacturing process known as P1. Later, the process was optimized for commercial manufacturing (known as P2) and this material was first administered to subjects during the open-label extension study (study 20030213). In healthy subjects, the PK parameters of romiplostim were nonlinear after a single IV dose from 0.3 to 10 μg/kg. For romiplostim, at pharmacologically active doses < 3 μg/kg, serum concentrations were not measurable in most samples collected from healthy subjects, and subjects with ITP. The absolute bioavailability of romiplostim after SC administration could not be estimated from the limited PK data available. Based on limited data from a single 2 μg/kg SC dose, peak romiplostim serum concentrations were observed between 24 and 36 hours postdose in healthy subjects. For subjects with ITP, peak serum concentrations after once-weekly SC administration over a dose range of 3 to 15 μg/kg were observed about 7 to 50 hours postdose (median, 14 hours) (study 20030213-Subset B). Romiplostim exposure after the sixth dose appeared lower than that after the first dose in subjects with ITP (study 20000137B). After up to 26 weeks of once-weekly SC administration of romiplostim in subjects with ITP, no clear relationship was observed between the serum concentration-time profiles with doses over a range of 3 to15 μg/kg (study 20030213Subset B); however, higher exposures were observed in subjects with lower platelet counts at a given dose. Pharmacodynamics Pharmacodynamic Effects Two phase 1 studies (studies 20000109 and 20040134) were conducted to evaluate the PK and PD profiles and safety of romiplostim in healthy subjects. In study 20000109, subjects receiving romiplostim at 10.0 μg/kg IV had a 4- to 7-fold increase in peak platelet counts from baseline. In light of this result, the planned dose escalation scheme was modified; subsequent IV doses were 0.3 and 1.0 μg/kg, and SC dose levels were 0.1, 0.3 μg/kg, 1.0 μg/kg, and 2.0 μg/kg. 2.0 μg/kg was identified as the optimal dose in this study. Mean platelet count-time profiles after a single IV or SC administration of romiplostim in healthy subjects and platelet parameter values were included. The reference range of platelet counts for healthy adults is approximately 150 to 450 x 109/L. After single IV and SC doses in healthy subjects, romiplostim induced a dose-dependent increase in platelet counts. Platelet counts rose above baseline 7 to 9 days postdose, reached the peak (Pmax) 11 to 15 days postdose, and returned to the baseline level after approximately 27 days. Platelet responses were similar after IV and SC administration, although exposure to romiplostim was markedly lower (or not measurable) after SC administration compared with IV administration. Platelet count profiles were essentially superimposable after IV and SC administration of romiplostim at 1 μg/kg. The 1.0 μg/kg dose was considered the minimally active dose, defined as the dose at which 2 subjects had a 1.5-fold increase over baseline for 2 consecutive platelet counts. The 2.0 μg/kg SC dose was identified as the minimally effective dose, defined as the lowest dose that increased platelet counts to ≥ 2.0-fold over baseline for 2 of 4 subjects treated with romiplostim. These Page 15 of 31 SAMPLE AUSPAR findings guided dose selection for subsequent studies in subjects with ITP, in which romiplostim was given SC starting at 1 μg/kg. Results were similar in Japanese subjects to results from study 20000109. After a single 0.3 μg/kg SC dose of romiplostim, no effect on platelet response was observed. As in study 20000109, the 1.0 μg/kg SC dose was considered the minimally active dose, and 2.0 μg/kg SC was considered the minimally effective dose in healthy Japanese subjects. Dose Response Studies 4 dose-finding studies were conducted in subjects with ITP (studies 20000137A, 2001218, 20000137B and 20050162). In the early clinical studies in subjects with ITP, a target platelet response was defined as peak platelet count achieving a doubling of baseline platelet counts and within the range of ≥ 50 x 109/L and ≤ 450 x 109/L, in the absence of rescue medication. In study 20000137A, platelet counts were below 50 x 109/L 1 week after the first dose in the majority of subjects who received doses of 1 and 3 μg/kg; and at these doses no subjects exceeded the platelet count of 450 x 109/L. Results suggested that dosing once every 2 weeks was inadequate to achieve and maintain platelet counts in a therapeutic range, and weekly dosing may be necessary. Since platelet responses were highly variable among subjects with ITP, individual dose adjustment is warranted to produce adequate platelet responses. In study 20000137B, evaluating weekly dosing of romiplostim at 1.0, 3.0 and 6.0 μg/kg, 7 of 8 subjects in the 1.0 μg/kg cohort, 5 out of 8 subjects in the 3 μg/kg cohort, and 1 out of 1 subject in the 6 μg/kg cohort achieved a platelet count ≥ 50 x 109/L after at least one dose of romiplostim. This finding supports the use of 1.0 μg/kg as the starting dose. No subject with ITP administered 1.0 μg/kg had a platelet count > 450 x 109/L, therefore, 1 μg/kg once weekly appears to be an appropriate starting dose for romiplostim, followed by individual dose adjustment based on the individual observed platelet count. Efficacy The pivotal efficacy data are from 2 multicentre, double-blind, randomized, placebo-controlled, phase III clinical trials of romiplostim in subjects with ITP; studies 20030105 and 20030212. Both studies were designed in accordance with relevant regulatory guidance and in consultation with regulatory agencies through Special Protocol Assessment (Food and Drug Administration) and Protocol Assistance (EMEA) processes to ensure an appropriate level of clinical and statistical robustness. Supportive efficacy data on long-term treatment with romiplostim were provided from an openlabel extension study (20030213) that enrolled subjects with ITP who had completed a prior romiplostim treatment study and whose platelet count subsequently fell below 50 x 109/L after cessation of treatment in the parent study (including placebo subjects). Study Overview - Studies 20030105, 20030212 and 20030213 Entry Criteria Entry criteria were the same in both of the pivotal studies except that subjects in study 20030105 were refractory to splenectomy while subjects in study 20030212 had not undergone splenectomy. Briefly the following criteria were to be met: • • Subjects were required to be at least 18 years old Subjects had to have a diagnosis of ITP according to American Society of Haematology (ASH) guidelines (George et al, 1996) Page 16 of 31 SAMPLE AUSPAR • Subjects must have completed at least 1 previous treatment for ITP and had a mean of 3 platelet counts during screening and pre-treatment that was ≤ 30 x 109/L, with no individual count > 35 x 109/L • A haemoglobin of at least 9.0 g/dL was required at baseline to ensure a single lineage deficiency • Subjects over 60 years of age were required to have a documented history of chronic ITP with a bone marrow report in order to exclude myelodysplastic syndromes • Subjects with a known history of bone marrow stem cell disorder were excluded • In study 20030105, splenectomy was required to have occurred at least 4 weeks prior to study entry. In study 20030213 subjects who completed a prior romiplostim treatment study and whose platelet count subsequently fell below 50 x 109/L could receive romiplostim. Subjects from studies 20000137 or 20010218 entered at the initial weekly dose of 1 μg/kg. Subjects entering from a blinded study entered the study on the same weekly dose as in the prior study. Placebo subjects began at the initial weekly dose of 1 μg/kg. Methodology Randomization was stratified by baseline concurrent ITP therapy (yes or no). Both studies used a romiplostim starting dose of 1 μg/kg, administered SC once weekly (based on data from studies 20000137A, 20000137B, and 20010218, which supported weight-based dosing to achieve a platelet count of > 50 x 109/L). The desired platelet range in which a constant dose was to be maintained was 50 x 109/L to 200 x 109/L. In the pivotal studies the maximum dose was15 μg/kg. In study 20030213 the maximum dose of romiplostim was initially30 μg/kg, but was reduced to10 μg/kg in protocol amendments. The amendments were made because of the lack of additional clinical benefit to incremental doses above10 μg/kg. The pivotal studies were not amended. Primary Endpoint In the pivotal studies the primary efficacy endpoint was the incidence of durable platelet response, defined as achieving at least 6 weekly platelet responses (platelet count ≥ 50 x 109/L) during the last 8 weeks of treatment with no rescue medications administered at any time during the treatment period. This endpoint is consistent with treatment guidelines and was decided in consultation with regulatory authorities. Secondary Endpoints Key secondary endpoints were as follows: i. Incidence of overall platelet response (durable and transient responders) ii. Number of weekly platelet responses iii. Proportion of subjects requiring rescue medications iv. Incidence of achieving durable platelet response with stable dose Additional Efficacy Endpoints Additional efficacy endpoints included the following: • • • • Incidence of > 25% reduction from baseline or discontinuation of concurrent ITP therapy Incidence of ≥ 20 x 109/L increase from baseline in platelet count Total number of weekly platelet counts increased by ≥ 20 x 109/L from baseline Time to first weekly platelet count increased by ≥ 20 x 109/L from baseline Page 17 of 31 SAMPLE AUSPAR • PRO Analyses - included health-related quality of life (HRQOL), and the ITP Patient Assessment Questionnaire (ITP-PAQ) scales. Statistical Methods For the primary efficacy analyses the primary statistical inferences were based on the analysis of results from the Cochran-Mantel-Haenszel test for the odds ratio of the 2 treatment groups, including p-values and 95% confidence intervals (CI) and adjusting for prior splenectomy status and baseline concurrent ITP therapy. Results from logistic regression analyses using treatment group, prior splenectomy status, baseline concurrent ITP therapy, and baseline subgroups as predictors were used for exploratory purposes. Kaplan-Meier estimates were used to analyse the median time to first weekly platelet count increased by ≥ 20 x 109/L from baseline and the time to first weekly platelet response during the treatment period. Demographic Data and Subject Disposition for Pivotal Studies Demographic characteristics were well balanced between the romiplostim and placebo groups in studies 20030105 and 20030212, and were typical of the ITP population. The median age was 52.0 years (range: 21, 88) and there were more women (64.8%) than men (35.2%). Thirteen subjects (31.0%) in the placebo group and 18 subjects (21.7%) in the romiplostim group were ≥ 65 years old. The median weight was 80.5 kg (range: 52, 169) in the placebo group and 78.2 kg (range: 44, 138) in the romiplostim group. At baseline the population was severely thrombocytopenic: median 17.7 x 109/L (range: 2, 31) in the placebo group and 15.7 x 109 /L (range: 2, 29) in the romiplostim group. Between groups and across studies the median values for RBC, WBC, haemoglobin, and endogenous thrombopoietin were balanced. All subjects had received at least 1 previous ITP therapy. Most subjects in both of the pivotal studies had received corticosteroids (94.4%), and most had received IVIG (66.1% nonsplenectomized, 93.7% splenectomized). Less tolerable therapies had been used by the splenectomized population, for example in study 20030105 vincristine or vinblastine had been used in 42.9% of subjects and azathioprine had been used in 23.8% of subjects. Rituximab (not currently approved for treatment of ITP) had been used by 71.4% of splenectomized subjects. 46.8% of subjects in study 20030212 had received 1 or 2 prior ITP therapies, and another 38.7% had received 3 or 4 prior therapies. Although they had not undergone splenectomy, these subjects had low platelet counts despite receiving several different ITP therapies, and are therefore representative of a chronic refractory population. Splenectomized subjects had been extensively treated before enrolment: 27.0% had received 8 to 10 prior treatments, 54.0% had received 5 to 7 prior treatments, and no subjects had received fewer than 3 treatments. Study 20030105 Efficacy Results A tabular summary of key efficacy endpoints in study 20030105 is provided in Table 4. Romiplostim was statistically significantly superior to placebo for both the primary efficacy endpoint and key secondary endpoints. A statistically significantly greater proportion of subjects in the romiplostim group (16 subjects, 38.1%) than in the placebo group (no subjects) achieved a durable platelet response (p = 0.0013). Page 18 of 31 SAMPLE AUSPAR Table 4 Study 20030105 - Key Efficacy Endpoints No subjects in the placebo group compared to 33 subjects in the romiplostim group (78.6%) achieved an overall platelet response (p < 0.0001). The number of weeks with platelet response was also significantly greater for the romiplostim group: mean 0.2 weeks, SD 0.5 weeks for placebo; mean 12.3 weeks, SD 7.9 weeks for romiplostim (p < 0.0001). 12 (57.1%) subjects in the placebo group and 11 (26.2%) subjects in the romiplostim group received rescue medication during the treatment period (p = 0.0175). 13 (31.0%) subjects were able to achieve a durable platelet response at a stable dose of romiplostim compared to no subject in the placebo group (p = 0.0046). By the end of study (week 25), all 12 subjects in the romiplostim group who had been receiving ITP therapies at baseline had either reduced (≥ 25%) or discontinued those therapies, compared with only 1 placebo subject. Platelet counts increased above their baseline values by ≥ 20 x 109/L for 5 (23.8%) subjects in the placebo group compared to 37 (88.1%) subjects in the romiplostim group (p < 0.0001). For the placebo group, the mean change from baseline in platelet counts showed no change, whereas for the romiplostim group a rapid increase followed by steady maintenance above 50 x 109/L was observed when rescue medications were excluded from the analysis. Results from several subscales of the ITP-PAQ indicated a positive effect of romiplostim on measures of PRO as shown by the mean change from week 1 to week 25. The subscale Physical Health - Symptoms showed a difference in means for romiplostim – placebo of 10.55 (p = 0.0205), suggesting that subjects receiving romiplostim reported an improvement in their physical symptoms. Other subscales also showed significant improvement in favour of romiplostim relative to placebo: Physical Health - Bother subscale (p = 0.0091), Social Quality of Life (p = 0.0172) and Women's Reproductive Health (p = 0.0272). Overall the results from study 20030105 support superior efficacy of romiplostim over placebo in thrombocytopenic subjects with ITP who are refractory to splenectomy. Efficacy was demonstrated in all key efficacy endpoints. Page 19 of 31 SAMPLE AUSPAR Study 20030212 Efficacy Results A tabular summary of key efficacy endpoints in study 20030212 is provided in Table 5. Romiplostim was statistically significantly superior to placebo for the primary efficacy endpoint and for key secondary endpoints. A significantly greater proportion of subjects in the romiplostim group (25 subjects, 61.0%) than in the placebo group (1 subject, 4.8%) achieved a durable platelet response (p < 0.0001). 3 subjects (14.3%) in the placebo group and 36 subjects (87.8%) in the romiplostim group achieved an overall platelet response (p < 0.0001). The mean number of weeks with platelet response was 1.3 weeks (range: 0, 15) for the placebo group and 15.2 weeks (range: 0, 24) for the romiplostim group (p < 0.0001). Table 5 Study 20030212 - Key Efficacy Endpoints 13 subjects (61.9%) in the placebo group and 7 subjects (17.7%) in the romiplostim group received rescue medication during the treatment period (p = 0.0004). 21 (51.2%) subjects were able to achieve a durable platelet response at a stable dose of romiplostim compared to no subject in the placebo group (p = 0.0001). At week 13, 4 romiplostim subjects (36.4%) had a > 25% reduction and 2 subjects (18.2%) had discontinued all concurrent ITP therapies. In the placebo group 1 subject (10.0%) had a > 25% reduction and 3 subjects (30%) discontinued all concurrent ITP treatment. At week 25, 4 romiplostim subjects (36.4%) had a > 25% reduction and 4 subjects (36.4%) had discontinued all concurrent ITP therapies. In the placebo group 2 subjects (20.0%) had a > 25% reduction and 3 subjects (30.0%) discontinued all concurrent ITP treatment. Platelet counts increased above their baseline values by ≥ 20 x 109/L for 38 subjects (92.7%) in the romiplostim group compared to only 7 subjects (33.3%) in the placebo group (p < 0.0001). In the placebo group platelet counts remained relatively steady throughout the study. In the romiplostim group median platelet count increased to a maximum of 100 x 109/L at week 11, and then remained at an increased level of between 62.5 x 109/L and 96 x 109/L over baseline for the remainder of the 25-week study period. Page 20 of 31 SAMPLE AUSPAR Results showed greater improvement from week 1 to 25 on 9 out of 10 ITP-PAQ scales, with the exception of the Work Quality of Life scale; however the Physical Health - Activity scale was the only scale that showed a statistically significant difference in mean change for romiplostim vs placebo (p = 0.0164). The SF-36 and EQ-5D scales, included as generic HRQOL measures, did not show statistically significant differences between subjects treated with romiplostim and placebo; however the scales may not have been capable of detecting small changes. The results from study 20030212 support superior efficacy of romiplostim over placebo in thrombocytopenic subjects with ITP who have not yet received splenectomy. As in study 20030105, efficacy was demonstrated in all key endpoints measured. Study 20030213 This is an ongoing long-term extension study. Data were provided from an interim analysis of subjects from 6 studies who had completed their parent study and entered the extension study. The data cut-off date was 28 November 2006. Demographic Data and Subject Disposition 137 subjects were enrolled (91 women [66.4%] and 46 men [33.6%]). The median age was 53.0 years (range, 42 to 63 years). Of the 137 subjects enrolled, 136 subjects received at least 1 dose of romiplostim. As of the data cut-off date, 120 subjects (87.6%) were continuing in the study and 17 (12.4%) had discontinued (7 due to withdrawn consent, 5 due to an adverse event, 3 due to death, 1 due to protocol-specified, and 1 due to other criterion). For the interim analysis, 136 subjects had been on treatment for a median of 39 weeks (range, 1 week to 122 weeks). Efficacy Results The interim analyses showed that a platelet response (defined as doubling of baseline platelet count and platelet count ≥ 50 x 109/L at any time on study in the absence of rescue medication within 8 weeks) was achieved in 82% of subjects (95% CI: 75%, 88%). A platelet count increase of ≥ 20 x 109/L from baseline was reached in 86% of subjects. A platelet count increase of ≥ 50 x 109/L was reached in 82% of subjects, while a platelet count ≥ 100 x 109/L was reached in 75% of subjects. 64% of subjects reached a platelet count ≥ 150 x 109/L. One week after the first dose of romiplostim the proportion of subjects with platelet responses was 31%. Kaplan-Meier analysis of time to first platelet response was 2 weeks (95% CI: 2, 3) for the 50th percentile (median) and 7 weeks (95% CI: 5, 11) for the 75th percentile. The median romiplostim dose prior to first platelet response was 3μg/kg (range, 1 to 18 μg/kg). From week 4 onwards, weekly incidence of response was in the range of 47% to 72%. At baseline, the median platelet count was 20 x 109/L, and after the first dose (week 1) was 40 x 109/L. The overall subject incidence of rescue medication use was 34.6%. Corticosteroids and IVIG were the most common rescue medications used. The subject incidence of usage of rescue medication decreased with time on study: incidences were at weeks 1 (n = 136), 13 (n = 100), 25 (n = 89), and 37 (n = 70) were 25%, 16%, 19%, and 15% respectively. 22% of subjects (30/136) entered the study on concurrent ITP therapy. In 13/30 (43%) subjects, concurrent ITP therapy was discontinued during the study; and in 6 of these subjects (20%), dosage was reduced by > 25%. Trends toward improvement were observed for many of the scale scores within the various PRO instruments used (i.e., ITP-PAQ, SF-36, EQ 5D, and Patient Global Assessment); however sample sizes for analyses were small, and meaningful conclusions from the data could not be drawn. The efficacy results from study 20030213 demonstrated that administration of romiplostim could maintain platelet counts over time in subjects with ITP. Efficacy was shown in splenectomised Page 21 of 31 SAMPLE AUSPAR subjects and in subjects who had not undergone splenectomy. Administration of romiplostim allowed the reduction of concomitant ITP medications in a large proportion of subjects. Safety The sponsor presented safety data from all 13 clinical trials submitted for evaluation. Detailed analyses of safety data were submitted from all phase III clinical studies and PK/PD studies. The most important data consisted of analyses from the phase 3 ITP safety set (n = 125), the phase 3 ITP long-term safety set (n=125), and the ITP safety set (n = 215). The romiplostim safety set consisted of data from subjects with ITP, myelodysplastic syndrome (MDS), chemotherapy-induced thrombocytopenia (CIT) and data from healthy subjects (total n=317; 284 romiplostim, 33 placebo). Extent and Duration of Exposure Exposure in the Phase 3 ITP Safety Set 41 subjects were exposed to placebo and 84 subjects were exposed to romiplostim in the phase 3 ITP safety set. The mean (SD) duration of exposure was 18.57 (6.82) and 22.83 (4.12) weeks for placebo and romiplostim, respectively. The median cumulative dose during the phase III pivotal studies was 12905 μg and 4098.0 μg for placebo and romiplostim, respectively. Exposure in the Phase 3 ITP Long-term Safety Set 117 subjects received romiplostim, and the maximum duration of exposure for these subjects in the phase 3 ITP long-term safety set was 83.9 weeks (1.6 years). The average (SD) weekly dose was 4.18 (3.21) μg/kg, the median average weekly dose was 3.15 μg/kg, and the maximum dose was 18 μg/kg. 39.3% of subjects had between 48 and 96 weeks of exposure as of the data cutoff. Exposure in the ITP Safety Set 128 subjects had at least 6 months (26 weeks) of exposure to romiplostim and 74 subjects had at least 1 year (52 weeks) of exposure. The maximum exposure in this safety set was 128 weeks, the maximum number of doses was 126, and the maximum dose received was 23.0 μg/kg. The median cumulative dose was 8542.7 μg with a minimum and maximum cumulative dose of 19 and 190866 μg, respectively. Exposure in Other Romiplostim Studies In the 20 subjects in the MDS study, the maximum dose was 1000 μg and the maximum duration of exposure was 31 weeks. The median cumulative dose was 7000 μg and the maximum cumulative dose was 12800 μg. In the 4 subjects in the CIT study at the time of the data cutoff (14 August 2006), 2 subjects had completed the first 100-μg treatment cycle and the other 2 subjects had been dosed at 100 μg, but had not completed the first treatment cycle. Page 22 of 31 SAMPLE AUSPAR Adverse Events Phase 3 ITP Safety Set The proportion of subjects that reported AEs was 100% for romiplostim subjects vs 95.1% for placebo subjects. The percentage of subjects that reported serious, severe, and fatal AEs is shown in Table 6. Table 6 Overall Summary of Adverse Events (Phase 3 ITP Safety Set) A tabular summary of the subject incidence of AEs ≥ 5% incidence in either treatment group in the phase 3 ITP safety set is provided in Table 7. The most frequently reported AEs in both treatment groups were headache (31.7% placebo, 34.5% romiplostim), fatigue (29.3% placebo, 33.3% romiplostim), and epistaxis (24.4% placebo, 32.1% romiplostim). Dizziness, myalgia, and abdominal pain had more than a 10% higher subject incidence in the romiplostim group compared with the placebo group. Subgroup analyses of AE rates were conducted by age, weight, sex, country, concurrent medications, baseline haemoglobin and years of diagnosis. There were some differences between placebo and romiplostim in several of the subgroup analyses; however because of the small numbers, the clinical significance of the differences is not certain. No clear trends were observed. In the phase 3 ITP safety set, the percentage of subjects reporting an AE that led to an intervention was similar between the placebo and romiplostim groups (82.9%; placebo vs 83.3%, romiplostim). The most common AEs leading to an intervention were headache (26.8%, placebo; 28.6%; Page 23 of 31 SAMPLE AUSPAR romiplostim), upper respiratory tract infection (9.8%, placebo; 13.1%, romiplostim), and arthralgia (7.3%, placebo; 11.9%, romiplostim). Table 7 Subject Incidence of Adverse Events ≥ 5% Incidence in Either Treatment Group by Preferred Term (Phase 3 ITP Safety Set) Page 24 of 31 SAMPLE AUSPAR ITP Safety Set The percentage of subjects that reported serious, severe, and fatal AEs in the ITP safety set is shown in Table 8. Similar proportions of subjects receiving placebo or romiplostim reported an AE: 95.7% of placebo subjects and 95.6% of romiplostim subjects. Table 8 Overall Summary of Adverse Events (ITP Safety Set) Treatment-Related Adverse Events (TRAEs) For the phase 3 ITP safety set, headache, myalgia, and fatigue were the most frequently reported TRAEs. For the ITP Safety Set, the proportion of subjects that reported TRAEs was 47.1% for romiplostim subjects vs 26.1% for placebo subjects. Headache was the most frequently reported TRAE (16.7% romiplostim, 6.5% placebo). Deaths and Other Serious Adverse Events Deaths 8 subjects died during a romiplostim ITP clinical study (ITP safety set); 3 (6.5%) placebo subjects and 5 (2.5%) romiplostim subjects. None of the deaths were considered treatment-related. In study 20030105 no romiplostim subjects died, and 3 placebo subjects died. In study 20030212, 1 romiplostim subject died, and no placebo subjects died. In study 20030213, 3 romiplostim subjects died, and no placebo subjects died. Page 25 of 31 SAMPLE AUSPAR Table 9 Table of Deaths - ITP Safety Set Serious Adverse Events (SAEs) 62 subjects reported at least 1 SAE during an ITP clinical study (ITP safety set); 10 (21.7%) placebo subjects and 52 (25.5%) romiplostim subjects The study duration-adjusted SAE rate for subjects who received placebo was 121.2/100 subject-years on study and for subjects who received romiplostim was 76.1/100 subject-years on study. Table 10 Other Serious Adverse Events Considered Related to Investigational Product (Excludes Deaths) Page 26 of 31 SAMPLE AUSPAR Table 10(cont) Other Serious Adverse Events Considered Related to Investigational Product (Excludes Deaths) Laboratory Data Clinical laboratory evaluations were provided for subjects in the phase 3 ITP safety set and ITP safety set. Overall, serum chemistry results for each analyte were similar between treatment groups. Minor fluctuations were observed; however no clinically relevant trends were observed for any of the serum chemistry analytes. Haematology laboratory results were also similar for both treatment groups, and no clinically relevant trends in any haematology parameter were noted. Effect on Vital Signs and ECG No clinically important changes in vital signs were observed. Adverse Reactions Characteristic of the Drug Several AEs were considered of special interest because of the potential association with the mechanism of action of romiplostim in subjects with ITP. These were: • • • • • • • bleeding event clinically significant bleeding event (any bleeding event that was considered grade 3 or above based on the adverse events standard grading score) thrombotic / thromboembolic event bone marrow abnormality neoplasm (any preferred term that was classified in the system organ class of neoplasms benign, malignant and unspecified [including cysts and polyps], or identified as a neoplasm by an Amgen medical reviewer) injection site event (any event occurring at the injection site). Post-market Safety Data No post-marketing data were presented for evaluation. Clinical Summary and Conclusions Pharmacokinetics In healthy subjects, the PK parameters of romiplostim were nonlinear after a single IV dose from 0.3 to 10 μg/kg. For romiplostim, at pharmacologically active doses < 3 μg/kg, serum Page 27 of 31 SAMPLE AUSPAR concentrations were not measurable in most samples collected from healthy subjects, and subjects with ITP. The absolute bioavailability of romiplostim after SC administration could not be estimated from the limited PK data available. Based on limited data from a single 2 μg/kg SC dose, peak romiplostim serum concentrations were observed between 24 and 36 hours post-dose in healthy subjects. For subjects with ITP, peak serum concentrations after once-weekly SC administration over a dose range of 3 to 15 μg/kg were observed about 7 to 50 hours post-dose (median, 14 hours) (study 20030213-Subset B). Romiplostim exposure after the sixth dose appeared lower than that after the first dose in subjects with ITP (study 20000137B). After up to 26 weeks of once-weekly SC administration of romiplostim in subjects with ITP, no clear relationship was observed between the serum concentration-time profiles with doses over a range of 3 to15 μg/kg (study 20030213-Subset B); however, higher exposures were observed in subjects with lower platelet counts at a given dose. Pharmacodynamics Romiplostim is thought to exert its therapeutic benefit by directly stimulating platelet production by binding to and activating c-Mpl on platelet precursors in the bone marrow. In healthy subjects, romiplostim induced a dose-dependent increase in platelet counts after single IV doses ranging from 0.3 to 10.0 μg/kg or single SC doses ranging from 0.1 to 2.0 μg/kg. Platelet counts rose above baseline 7 to 9 days post-dose, reached a peak 11 to 15 days post-dose, and returned to the baseline level by 27 days after IV or SC administration. Platelet responses were similar after IV and SC administration at the same dose level, although serum romiplostim concentrations were markedly lower or not measurable after SC administration compared with IV administration. Results from the dose-finding studies in subjects with ITP suggest that romiplostim increases platelet counts in a dose-dependent manner. Dosing every 2 weeks was inadequate to maintain platelet counts within the therapeutic range for many subjects. In study 20000137B in subjects with ITP, 7 of 8 subjects in the 1.0 μg/kg cohort achieved the target platelet response, supporting the use of 1.0 μg/kg once weekly as the starting dose in phase III studies. Large variability in platelet response in the dose-finding studies of subjects with ITP supported the need for individual dose adjustments based on platelet counts to achieve and maintain the desired target platelet count. Efficacy The data submitted for evaluation adequately support the efficacy of romiplostim in treatment of subjects with ITP. Efficacy has been demonstrated in splenectomized subjects who have had an inadequate response, and in non-splenectomized subjects who have had an inadequate response or are intolerant to other ITP therapies. The effective dose, and appropriate dosing adjustments have been defined from the studies submitted for evaluation. Safety The data presented for evaluation have demonstrated that romiplostim is effective in splenectomised and non-splenectomised subjects with refractory chronic ITP. The safety profile of romiplostim in this patient population appears acceptable. V. Overall Conclusion and Risk/Benefit Assessment Quality There are no objections to registration on Module 3 grounds. The initial report highlighted some issues and the application was considered by the Pharmaceutical Subcommittee (PSC). All issues were adequately resolved by the Sponsor. Non-Clinical There are no preclinical objections to registration. Administration of romiplostim to rodents and monkeys was associated with large and long-lasting increases in platelet counts. The induced platelets were shown to function normally. Page 28 of 31 SAMPLE AUSPAR Toxicity was studied in rats and monkeys. Observed toxicities were consistent with the drug’s pharmacological effect. These included: • • Increased spleen weights consistent with increased demand for platelet clearance; Enhanced platelet aggregation with incidents of haemorrhage and possibly thromboembolic events; • Hyperostosis of bone; • Myelofibrosis (in rats) due to increased release of cytokines from the elevated number of megakaryocytes; • Increases in leukocyte counts; • Decreases in red blood cell counts. There was some evidence of embryofetal toxicity, with a significant increase in the incidence of stillbirths in rats. The evaluator has therefore recommended a Pregnancy Category of B3. Clinical The clinical evaluator has recommended approval of the application. Pharmacodynamics Single doses of romiplostim administered to healthy volunteers resulted in dose-dependent increases in platelet count, with maximum effect occurring at approximately 10-14 days. In patients with chronic ITP, a dose dependant increase in platelet count was also observed, with maximum effect occurring at between 3 and 15 days. Significant inter-patient variability in platelet increase was noted. The evaluator considered that the proposed dosage regimen was adequately justified. A weekly dosage interval was chosen on the grounds that the majority of ITP patients required repeated dosing after a 2 week interval due to platelet counts falling below 50 x 109 / L (study -137A). The proposed starting dose (1.0 mcg/kg per week SC) produced platelet counts in the range 50 – 450 x 109 / L in a high proportion of subjects, whereas higher doses resulted in levels > 450 x 109 / L (study -137B). Pharmacokinetics One study in healthy volunteers (-109) examined PK after IV administration. This demonstrated non-linear PK, with greater than proportional increase in systemic exposure with increasing dose, presumably due to saturation of the TPO receptor at higher doses. At the highest dose given, the drug had a small volume of distribution (48 mL/kg) and a half-life of approximately 14 hours. PK after SC administration have not been well defined due to difficulty in measuring the low concentrations of the drug. Absolute bioavailability has not been determined. No accumulation occurred after repeated administration for 6 weeks. Efficacy Evidence for efficacy comes from two randomised, double-blind, placebo-controlled trials. • Study 2003-0105 enrolled ITP patients who had already had a splenectomy (at least 4 weeks previously). • Study 2003-0212 enrolled ITP patients who had not had a splenectomy, but who had previously received at least one prior treatment (e.g. prednisone) for ITP. Both studies included only adult patients, who had a platelet count of < 30 x 109 / L. Patients receiving treatment with steroids, azathioprine and/or danazol could be enrolled providing that dose of these agents had been constant. Patients who had received treatment with immunoglobulins in the preceding 2 weeks, or rituximab in the preceding 14 weeks, were excluded. Patients could receive rescue therapy (eg with immunoglobulins, corticosteroids, platelet transfusions) in the case Page 29 of 31 SAMPLE AUSPAR of bleeding or if the investigator felt that the patient was at immediate risk. The duration of both studies was 24 weeks. The primary endpoint was the proportion of patients who achieved a “durable platelet response” – defined as a platelet count > 50 x 109/L for at least six of the last 8 weeks of study treatment, without the need for rescue therapy. The endpoint was apparently designed in consultation with the FDA and EMEA. Romiplostim treatment was associated with a statistically and clinically significant benefit in both studies. Several secondary endpoints, also based on platelet count, were significantly improved with romiplostim treatment. Another secondary endpoint related to the frequency of rescue therapy. Romiplostim treatment was associated with a reduced requirement for such therapies. A greater proportion of patients in the romiplostim group were able to reduce or discontinue concurrent ITP therapies that were being received at baseline. Long term efficacy was examined in an open uncontrolled extension study (2003-0213). The beneficial effect on platelet count appeared to be maintained for at least a further 48 weeks. Safety In the submitted studies, a total of 284 subjects were treated with at least one dose of romiplostim. A total of 204 ITP subjects were treated, with 128 treated for periods of ≥ 26 weeks and 74 for periods of ≥ 52 weeks. The most informative safety data comes from the two double-blind, placebo controlled trials. The overall incidences of adverse events and serious adverse events were comparable between the romiplostim and placebo groups, but with a difference between the two groups in events considered treatment-related by the investigators. There was no excess of discontinuations due to adverse events, or deaths, in the romiplostim group. Specific safety findings of note were: • Compared to placebo, romiplostim treatment was associated with increased incidences of headache, myalgia, arthralgia, fatigue, dizziness, insomnia, abdominal pain and pain in an extremity; • The incidence of bleeding events was comparable in the romiplostim and placebo groups overall. Romiplostim-treated patients had a lower incidence of grade II or higher bleeding events (14.3% vs 34.1% - page 42); • There was no excess of thromboembolic events with romiplostim compared to placebo; • There was no excess of neoplasms with romiplostim compared to placebo; • In ITP studies, 8.3% of romiplostim-treated subjects developed binding antibodies against the drug. Only one patient developed neutralising antibodies and these were no longer detectable 4 months after continuing the drug. 4.9% of romiplostim-treated subjects developed binding antibodies against endogenous TPO, and none of these were neutralising antibodies. • Increased deposition of reticulin fibres in the bone marrow was documented in 6 patients receiving romiplostim in the submitted studies. This finding raises the concern that the drug could be associated with fibrosis of the marrow. • Marrow fibrosis was documented in preclinical studies in rats, but not in monkeys. Risk-Benefit Analysis The pivotal placebo-controlled studies have demonstrated that romiplostim is effective in the proposed patient populations. Safety experience with the drug is limited, with only approximately 200 ITP patients having been studied. The drug is intended for long-term administration but only 74 Page 30 of 31 SAMPLE AUSPAR ITP subjects had been treated for periods of greater than one year. With the exception of increased bone marrow reticulin, the limited available safety data do not suggest any major safety issues. It is understood from information available on the FDA website that the sponsor is proposing to conduct a number of post-marketing studies to further investigate the drug’s potential to cause bone marrow abnormalities. The sponsor’s feedback indicates that such studies include: • A prospective phase 4, open-label multi-centre study evaluating the changes in bone marrow morphology in subjects receiving romiplostim for the treatment of thrombocytopenia associated with ITP. • Determination of frequency rates of bone marrow fibrosis and thrombotic / thromboembolic events in patients with chromic ITP in Denmark. In patients with chronic ITP refractory to splenectomy, currently available treatments are associated with significant toxicity, and romiplostim would appear to be a useful agent in this setting. In addition, splenectomy itself can be associated with significant morbidity and some risk of mortality, and the drug would be of value as an alternative in patients unable to be controlled with steroids and immunoglobulins. Despite the limited safety data it is therefore considered that the overall risk-benefit ratio for the drug is favourable and it is proposed to approve the application. ADEC agreed with the delegate and noted that in the Precautions section of the product information, under Increased Bone Marrow Reticulin, it should be stated that cytogenetic analysis for the presence or absence of a clonal abnormality should also be undertaken on any bone marrow biopsy sample obtained. In addition, the TGA should seek data from the sponsor on platelet function tests performed on patients receiving romiplostim. Recommendation Based on review of quality, safety and efficacy data, TGA approves the registration of Nplate® powder for injection vial containing romiplostim rbe 375microgram and 625microgram, indicated for: The treatment of thrombocytopenia in adult patients with chronic immune (idiopathic) thrombocytopenic purpura (ITP): • who are non-splenectomised and have an inadequate response or are intolerant to corticosteroids and immunoglobulins; • who are splenectomised and have an inadequate response to splenectomy. Page 31 of 31



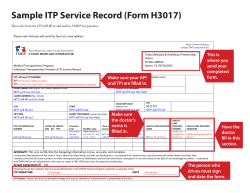





© Copyright 2026