
Sample Abstract – Research Track Title: Summary:
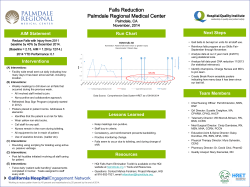
Sample Abstract – Research Track Title: Child Life in the ED: A Driving Force for Quality Care Summary: This presentation will demonstrate the impact of child life in the emergency department, on quality care, patient satisfaction and interdisciplinary collaboration. Results of a pilot study on child life interventions on laceration repair will be shared, which include lower patient/parent anxiety and increased parent satisfaction. A panel of child life, administration and physician will discuss the value of addressing psychosocial needs and how partnering with child life ensures quality, improves satisfaction and impacts the organizations’ bottom line. Objectives: Attendees will understand how child life interventions impact quality care and interdisciplinary collaboration in the peds ED Attendees will understand how child life interventions can impact the bottom line. Attendees will understand current research and future initiatives for child life interventions in the ED. Domain and task: Domain III (intervention), task 4 Abstract Introduction: Today’s competitive healthcare arena demands that healthcare facilities not just meet customer’s expectations, but exceed them. Establishing a culture of quality is on the forefront of all children’s healthcare initiatives as we aggressively compete for a finite number of resources. Hospitals must look beyond traditional methods to enhance quality of care, improve patient satisfaction and enhance collaboration with the interdisciplinary team. Child life specialists play a vital role in this process. Through research, this presentation will demonstrate the impact of child life in this process by examining their role in the pediatric emergency department. Research has demonstrated that emergency department visits for injured children are highly stressful experiences, especially when they include a painful procedure (Grantz, 1984; Resnick, 1975; Edwinson, Arnbjornsson & Elkman, 1988; Alcock, Feldman,Goodman, McGrath & Park, 1985; Tiedeman & Cladworthy, 1990; Elliott & Woody, 1987) . This pilot study explored the impact of preparation and distraction on procedure-related distress in children treated for laceration repair in the emergency department (Gursky, Kestler & Lewis, 2010). Description: A quasi-experimental study was conducted using a convenience sample procedure. Distress and parent ratings of satisfaction were compared between children who received individualized interventions for laceration repair provided by a child life specialist and children who received no intervention. Twenty-four subjects, aged 3 – 13 years were recruited from a pediatric emergency department within a university medical center. Patients receiving the intervention were provided with pre-procedure age appropriate information relating to the laceration repair and distraction during the procedure. All interventions were provided by a child life specialist, based on a standardized protocol. The preparation was standardized at 15 minutes and included child life specialist introduction to patient/family, explanation of the suturing procedure using a doll to demonstrate, and role playing each step of the laceration repair including age appropriate definitions. The specialist also asked the child and parents what normally helps them cope when they are stressed, and then provided age appropriate distraction. Children were also encouraged to ask questions and share any concerns. The comparison group received standard nursing care before and during suturing without any individualized preparation or distraction. Outcomes: Results of the pilot study showed that children who received child life interventions had lower observed distress behaviors during suturing compared with patients who did not receive the intervention. Results also showed that parents of patients who received the intervention perceived less distress in their children and rated their overall care significantly higher. These results, along with Press Ganey reports and anecdotal information will be shared to demonstrate child life as a driving force in improving patient satisfaction, increasing return likelihood to your facility, thus contributing to the bottom line. Physicians and administration will also share observations that include child life interventions resulting in decreased procedural times, decreased anxiety, and increased compliance and better comprehension by caregivers of procedures. Relevance to child life practice: The findings of this study have significant implications for child life practice and children’s health care as a whole, as to better supporting patient and family needs when a child enters the emergency department. This will ensure that healthcare facilities recognize the contribution of child life specialists to quality care and the bottom line. Continued research in this arena will demonstrate that child life interventions and their involvement as a key member of any interdisciplinary team will result in “return use” of hospital services, thus participating in the overall revenue of the organization. Organization of presentation: I. II. Description of hospital’s child life role in the ED Overview of research study III. IV. V. VI. VII. VIII. IX. a. Measurement tools b. Study flow chart c. Preparation protocol d. Results Value added Emergency department statistics Patient satisfaction implications a. Specific results and future directions b. Impact to the bottom line Anecdotal information and results Revenue information related to child life/patient satisfaction Building a case for senior leadership Future implications References Grantz RR. Children’s responses to emergency department care. Ann Emerg Med. 1984;13:322–333. Resnick R. Children and the emergency room. Child Today. 1975;4:5–8. Edwinson M, Arnbjornsson E, Elkman R. Psychologic preparation program for children undergoing acute appendectomy. Pediatrics. 1988;82:30–36. Alcock DS, Feldman W, Goodman JT, McGrath PH, Park JM. Evaluation of child life intervention in emergency department suturing. Pediatr Emerg Care. 1985;1:111–115. Tiedeman ME, Clatworthy S. Anxiety responses of 5–11 year old children during and after hospitalization. J Pediatr Nursing. 1990;5:334–343. Elliott CH, Jay SM,Woody P. An observation scale for measuring children’s distress during medical procedures.J Pediatr Psychol. 1987;12:543–551. Gursky B, Keslter L, Lewis M. The impact of psychological interventionon procedure related distress in children being treated for laceration repair in the pediatric emergency department. J Dev and Be Pediatr. 2012; 31: 217-222.




© Copyright 2026