
20A Del Carmine Street Wakefield, MA 01880 Office: 781.224.3344
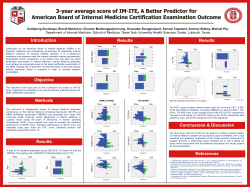
20A Del Carmine Street Wakefield, MA 01880 Office: 781.224.3344 Fax: 781.213.9417 E-Mail: [email protected] www.neems.org ALS Credentialing Study Guide Sample Test Please use this sample test as a guide in preparation for the Region III Credentialing Examination. Included are sample questions in the same format as the actual exam. The sample questions reflect the Massachusetts Statewide Treatment Protocols Version 5.1. If you need a copy of the most current protocols and protocol advisories, please refer to the NorthEast Emergency Medical Services, Inc. web site at www.neems.org for a direct link to the OEMS protocol web page. The actual examination is separated into two main sections consisting of 25 questions each. Each question is valued equally at 2 points and the passing score is 84% as decided by the Region III Medical Services Committee. The first section is Rhythm Interpretation and Treatment. In this section questions are based upon a patient care scenario and a rhythm strip followed by 2 or 3 questions about the scenario including the identification of the presented rhythm. The second section consists of questions which address a variety of protocol specific issues as well as several items from the introduction and appendices of the protocol document. Expect to find questions related to Protocols, Skills and 12-Lead ECG interpretation. Below are the directions for the exam as well as several sample questions followed by an answer key for study purposes. Before taking the actual examination, please be sure to review the entire protocol document as well as the Region III Optional Drug List. Past history has taught us that candidates that failed to study the protocols were unsuccessful greater than 90% of the time. This examination assesses a paramedic’s ability to treat a patient based upon the protocols (standing orders and medical control options). This is not an ACLS, PALS or EMT-P certification examination. The physicians in Region III want to be assured that a paramedic working within the region knows what is allowed by protocol as a standing order and what needs a medical control order. <<<NEXT PAGE FOR SAMPLE TEST>>> NorthEast Emergency Medical Services, Inc. Massachusetts Region III ALS Credentialing Examination Study Guide 2/2004 <<<<THIS IS A SAMPLE TEST>>>> For Study Purposes Only SECTION I RHYTHM INTERPRETATION AND TREATMENT Please correctly identify the following rhythms and associated treatments according to the scenario’s directions. All answers should be based upon the Statewide Treatment Protocols and the Region III optional medications. Assume that the patient’s rhythm does not change during treatment. Be sure to carefully review all possible answers prior to selecting the best choice for the following questions. (Each Question is valued at 2 points) A. You are treating a 78-year-old male who is complaining of mild shortness of breath. The patient has a cardiac history (MI x 1 about a year ago). His blood pressure is 156/90 and his respiratory rate is 20. His skin is warm, pink and dry. You find the following rhythm on the monitor: 1. What is the correct rhythm for this patient? A. B. C. D. 2. Atrial Fibrillation Atrial Flutter SVT Sinus-Tachycardia with PACs According to Standing Orders what electrical and/or pharmaceutical interventions may you administer to this patient? A. B. C. D. Synchronized Cardioversion at 50 joules Adenosine 6.0 mg Cardizem 0.25 mg/kg slow IV push None of the Above NorthEast Emergency Medical Services, Inc. Massachusetts Region III ALS Credentialing Examination Study Guide 2/2004 B. You are treating a 63-year-old female patient who is in cardiac arrest. The patient became pulseless and apneic while in the care of the BLS responders after complaining of weakness and lethargy. You perform a “quick look” and find the following rhythm: 3. What is the correct rhythm for this patient? A. B. C. D. 4. Which of the following medications may you administer to this patient as a standing order? A. B. C. D. 5. Ventricular Tachycardia Idioventricular Pulseless Electrical Activity Torsades de points Lidocaine 1.5 mg/kg IV Push Magnesium Sulfate 2-4 gm IV Push Amiodorone 300 mg Slow IV Push Epinephrine (1:1,000) 1.0 mg IV Push After a brief resuscitation effort, the patient regains a carotid pulse and blood pressure of 90/60. The patient appears to be in a Junctional rhythm at 56 bpm. What medication may you administer according to standing orders? A. B. C. D. Sodium Bicarbonate 0.5 – 1.0 mEq/kg IV Push Calcium Chloride 10% 2.0 – 4.0 mg/kg IV Push (Slowly) Lidocaine Infusion 2mg – 4mg/minute Atropine 1.0 mg IV Push NorthEast Emergency Medical Services, Inc. Massachusetts Region III ALS Credentialing Examination Study Guide 2/2004 C. Upon intercepting a BLS unit you find a 57-year-old male complaining of a near syncopal episode. The patient’s blood pressure is 88/60; his respiratory rate is 24; the pulse-ox reads 94% on room air; and his skin is cool and moist. The following rhythm is on the monitor: 6. What is the correct rhythm for this patient? A. B. C. D. 7. Assuming the patient is on a monitor, high concentration oxygen has been applied and an IV has been initiated, which of the following may be performed via standing orders and is the most appropriate first advanced treatment? A. B. C. D. 8. Second Degree Type I Block Ventricular Tachycardia Ventricular Bigeminy Third Degree Heart Block Lidocaine 0.5 mg - 1.0 mg/kg IVP Synchronized Cardioversion starting at 100 joules Atropine 0.5 mg IV Push Aspirin 162-325 mg Chewable According to the protocols, which of the following medical control options is not appropriate for this patient? A. B. C. D. Atropine 0.5 mg IV Push Lidocaine 0.5 mg - 1.0 mg/kg IVP Lidocaine Infusion 2-4 mg/min Calcium Chloride 10% 2-4 mg/min NorthEast Emergency Medical Services, Inc. Massachusetts Region III ALS Credentialing Examination Study Guide 2/2004 SECTION II Please select the best answer to the following questions. All correct answers are based upon the Massachusetts Statewide Treatment Protocols and Appendices as well as the Region III Specific Optional Medications. Each question is valued at 2 points. PEDIATRIC PROTOCOLS 1. In the Pediatric Coma/Altered Mental Status protocol you are allowed to give Dextrose to a known diabetic patient. How Much Dextrose do you give an 11-year-old patient that weighs 55 kg? A. D10 0.5 gm/kg B. D25 0.5 gm/kg C. D50 0.5 gm/kg D. D50 1.0 gm/kg 2. In the Pediatric Bradydysrhythmias Protocol what is the correct initial dose of Epinephrine for a symptomatic patient according to standing orders? A. Epinephrine (1:10,000) 0.1 mg/kg IV Push B. Epinephrine (1:10,000) 0.01 mg/kg IV Push C. Epinephrine (1:1,000) 0.01 mg/kg ETT D. None of the Above 3. In the Pediatric Pain Protocol, you may administer which of the following to a patient who weighs 20 kg: A. 1.0 mg Morphine IV/IM/IO/SC B. 2.0 mg Morphine IV/IM/IO/SC C. 1.0 mg Diazepam IV/IO D. 2.0 mg Diazepam IV/IO ADULT PROTOCOLS 4. According to the anaphylactic protocol, which of the following signs and symptoms would indicate the need to administer Epi, Benadryl, and Albuterol per standing order? A. Itching B. Isolated uticaria C. Nausea D. None of the above NorthEast Emergency Medical Services, Inc. Massachusetts Region III ALS Credentialing Examination Study Guide 2/2004 5. You are treating a 62-year-old male patient who has an altered mental status with leftsided weakness and is slurring his words when speaking. What medication(s) are you allowed to administer via standing orders according to the protocols? A. Dextrose B. Narcan C. Thiamine D. Both A and C 6. The patient you are treating is in atrial fibrillation at approximately 160 bpm. The patient has a blood pressure of 106/70 and is complaining of chest discomfort. What is the first choice of medication for this patient? A. Adenosine 6 mg rapid IV push over 1-3 seconds B. Verapamil 5-10 mg Slow IV push C. Amiodorone 150 mg IV slowly over 10 minutes D. Diltiazem HCL 0.25 mg/kg slow IV over 2 minutes 7. Part of the assessment/treatment priorities for a multi-system trauma patient is determining the patient’s history using the S-A-M-P-L-E model. Please define the letter “S” in the acronym S-A-M-P-L-E. A. Swelling B. Severity C. Signs and Symptoms D. Space 8. Which of the following is a complication of a Needle Cricothyrotomy? A. Thyroid Perforation B. Esophageal Perforation C. Posterior Tracheal Wall Perforation D. All of the Above 9. In the chemical weapons protocol patients who have been exposed to a nerve agent may be administered Mark I kit(s) or Atropine IM. How much atropine may be administered to a patient suffering from a mild reaction if no Mark I kit(s) are available? A. 1.0 mg Atropine IM B. 2.0 mg Atropine IM C. 4.0 mg Atropine IM D. 6.0 mg Atropine IM NorthEast Emergency Medical Services, Inc. Massachusetts Region III ALS Credentialing Examination Study Guide 2/2004 10. You are treating a 49-year-old male patient who has experienced a sudden onset of chest pressure and shortness of breath. He has received aspirin and nitroglycerin according to protocols and you have just acquired the following 12-lead ECG. Based upon the findings of the 12-Lead ECG, what classic pattern of myocardial injury is present? A. Anterior B. Inferior C. Lateral D. Combination NorthEast Emergency Medical Services, Inc. Massachusetts Region III ALS Credentialing Examination Study Guide 2/2004 ANSWER KEY AND REASONINGS Section I 1. D (Sinus-Tachycardia with PACs). The rate is greater than 100 and there are p waves associated with all QRS Complexes. 2. D (None of the Above). This patient is stable with a heart rate less than 150 and a blood pressure greater than 100. The patient (as noted above) is not in an SVT or A-Fib or Flutter negating the other treatment options listed in the question. For further information see Protocols 1.2, 1.3, 1.5, and 1.9. 3. A. (Ventricular Tachycardia) A wide and bizarre complex with no p waves 4. A. (Lidocaine). The Lidocaine dosage is the only appropriate medication listed under standing orders. The epinephrine is the wrong concentration and the Magnesium Sulfate is a medical control option for Torsades. Amiodorone is in the protocols for pulseless VTach, but it is not allowable within Region III. For further information please see protocol 1.10 as well as the medication list for optional medications. 5. C. (Lidocaine Infusion). The patient has converted to a perfusing rhythm and has been given an anti-arrhythmic. A Lidocaine infusion is allowable as a standing order in both protocols 1.10 and 1.6 (post resuscitation care). 6. C. (Ventricular Bigeminy). This rhythm presents with an alternating unifocal PVC and a Normal Sinus Beat. 7. A. (Atropine). This patient has an intrinsic rate below 50 (not counting PVCs). According to the protocols, a patient with a rate less than 50 should receive 0.5 mg Atropine and not Lidocaine. See protocol 1.7 for further information. 8. D. (Calcium Chloride). In protocol 1.7 the medical control options are limited to Atropine, Lidocaine and Lidocaine Bolus. Section II 1. C. (Dextrose 50% 0.5 gm/kg). The threshold for D50 is 50 kg (D25 for less than 50 kg). See protocol 5.6 for further information. 2. B. (Epi 1:10,000 0.01 mg/kg IV). All other Epi doses do not meet the protocol requirements. The ETT dose should be 1:1000, but at 0.1 mg/kg. See protocol 5.3 for further information. 3. B. (2.0 mg Morphine IV/IM/IO/SC). Valium is not an appropriate medication for pain control. The correct Morphine dose is 0.1 mg/kg to a maximum of 5 mg. See protocol 5.13 for more information. NorthEast Emergency Medical Services, Inc. Massachusetts Region III ALS Credentialing Examination Study Guide 2/2004 4. D. (None of the Above). The listed signs and symptoms are all considered mild. The three medications may not be administered unless severe signs and symptoms exist. See protocol 3.2 for further information. 5. C. (Thiamine). This question comes from two possible protocols: Stroke or Altered Mental Status. Both protocols warn that Dextrose should not be administered with possible signs of a stroke. Dextrose becomes a medical control option. Additionally, Narcan should only be administered when there is an obvious/suspected narcotic overdose. See protocol 3.3 and 3.11 for further information. 6. D. (Diltiazem). This patient is symptomatic, but stable with a rate greater than 150. This patient should receive a drug regimen. If the rate was below 150 the patient should receive supportive care and perhaps aspirin and nitroglycerin as a chest pain. Additionally, if the blood pressure was below 100 the patient should be considered for immediate Cardioversion and not a drug therapy. Medical control is always and option for this type of patient. See protocol 1.2 for further information. 7. C. (Signs and Symptoms). Swelling and Severity both are part of other mnemonics, DCAP-BTLS and O-P-Q-R-S-T respectively. Most mnemonics are found in the text of the protocols and in the introduction. 8. D. (All of the above). All of the complications are listed in the appendices of the protocol document. 9. B. (2.0 mg Atropine). This is a new protocol which addresses an optional skill for services, but must be taught to all providers in case of chemical exposures/chemical weapons. The protocol outlines the amount of medication to be administered by severity of symptoms. See protocol 2.6 for further information. 10. D. (Combination). This is a basic analysis of a 12-Lead based upon the required competencies for the state. This 12-Lead shows an Inferolateral AMI. There is significant ST Segment elevation in Lead II, III and aVF with reciprocal changes of ST depression in leads I and aVL. In addition, there is ST elevation in V3 to V6 consistent with a lateral wall infarct. NorthEast Emergency Medical Services, Inc. Massachusetts Region III ALS Credentialing Examination Study Guide 2/2004







© Copyright 2026