
Document 282754
CLIN. CHEM. 27/11, 1896-1898 (1981)
Sample ViscosityCan Be a Source of AnalyticalErrorWhen Discrete
Sampler-DilutorsAre Used
Kwok-Mlng Chan and Jack H. Ladenso&
Total protein concentration in the serum of a patient with
vealed a well-differentiated
hyperviscosity syndrome differed as measured by the biuret procedure in the DuPont aca (80 g/L) and the SMA
12/60 (105 gIL), owing to viscosity-dependent errors with
the aca sampling system; the magnitude depended on
sample temperature and volume of sample aspirated. This
with a diagnosis
of Waldenstr#{246}m’s macroglobuhinemia.
The
relative viscosity of this patient’s serum increased during this
hospital admission, with values ranging from 2.0 to 9.0 (normal
1.5-1.8). Because of this, plasmapheresis was initiated, leading
to a decline in her serum 1gM value to 12.0 g/L and in relative
viscosity to 2.0.
Serum samples.
Serum was sampled from patient N.E. at
various times during her 1979 hospitalization
and stored at
-20 #{176}C
until analyzed.
Plasma samples were also obtained at plasmapheresis. After
defibrination
with added thrombin,
the serum was dialyzed
against two changes of 100 volumes of de-ionized water, lyophilized, and then re-dissolved
in water.
Glycerol
solutions.
We analyzed solutions
containing
constant concentrations
of albumin (50 g/L), creatinine (45
mg/L), and uric acid (50 mg/L) but various concentrations
of
glycerol (50-70 mL/dL) and blank solutions containing only
glycerol in the same concentrations.
Analytical
procedures.
Viscosity relative to water (relative
viscosity) was measured at 37 #{176}C
with a Cannon-Senske
viscosity tube (Kimax 100; Curtin-Matheson,
St. Louis, MO).
Measurements
of total protein, albumin,
uric acid, and creatinine were performed
with the aca according to the manufacturer’s
directions
(regular aca procedure).
A modified
aca procedure
was also used, consisting
of
adding the appropriate
volume of sample into the aca test
pack by means of a 0.1-mL syringe (Hamilton Co., Reno, NV
89510).The test pack was placed behind an empty sample cup
and then analyzed in the aca. This modification
assured accurate delivery of the appropriate
volume of sample, regardless of viscosity, to the reagent pack.
kind of error was not observed with the SMA 12/60 and
was far less severe when a Micromedic
sampler-dilutor
was tested. It could be eliminated in the case of the aca
by adding sample to test packs with a syringe rather than
with
the aca automated
ommend
sampler-dilutor.
We thus recof the syringe method when unusually viscous
use
samples (serum or other body fluids) are analyzed in the
aca.
AddItIonalKeyphrases: total serum protein
sourceof
.
.
variation,
hyperviscosity syndrome
Roller-pump dilutors reportedly
are affected significantly
by viscosity, leading to underestimates
exceeding 15% when
samples from patients
with hyperviscosity
syndrome
are analyzed (1, 2). It has been generally
assumed
that discrete
sampler-dilutor
devices are free of sampling errors originating
from variations
in viscosity.
However, we recently noticed a
25 g/L discrepancy
between total protein as measured
with
the aca discrete analyzer (DuPont Instruments-aca
Division,
Wilmington,
DE 19898) and a continuous-flow
analyzer (SMA
12/60; Technicon
Instruments
Corp., Tarrytown,
NY 10591)
in serum from a patient with hyperviscosity
syndrome.
This
led us to investigate
systematically
the influence of viscosity
on the accuracy of sampling
with three different
samplerdilutors and to conclude that some discrete sampler-dilutor
devices such as that used with the aca may be severely affected
by changes in sample viscosity.
plasma cell infiltrate,
compatible
Materials and Methods
Patient
studied.
The patient studied (N.E.) has been described in detail elsewhere (3). The discrepant protein values
were observed during her admission in 1979 forsevereanemia
and the presence of occult blood in feces. During this admission, her total-protein value was 105 gIL, albumin 19 g/L (both
measured on the SMA 12/60), and serum protein electrophoresis revealed a paraprotein. Her serum was subsequently
noted to be viscous at 4 #{176}C
but fluid at 25 or 37 #{176}C.
Immunoglobulin values (gIL) as determined by nephelometry with the
Beckman Immunochemistry
Analyzer were as follows: IgG
45.1, IgA 26.3, and 1gM 25.7. Bone-marrow
examination
re-
Division of Laboratory Medicine, Departments of Pathology and
Medicine, Washington University School of Medicine, St. Louis, MO
63110.
Presented in part at the 32nd national meeting, AACC, July 1980,
Boston, MA.
To whom reprint requests should be sent.
Received March 30, 1981; accepted June 22, 1981.
1896
CLINICAL CHEMISTRY, Vol. 27, No. 11, 1981
Experimental
Protocols
The influence of viscosity on the results for protein or other
analytes with the aca was assessed by analyzing
samples by
the regular and modified aca procedures. The errorcaused
by the sampler-dilutor
with the aca was then assessed as
follows:
% error
=
(results
by modified
aca
results
-
results by regular aca/
by modified aca) X 100
The influence of viscosity on another discrete samplerdilutor, the Micromedic
24004 with a 0.5-mm delivery tip
(Micromedic
Systems Inc., Horsham, PA 19044) was assessed
as follows. We diluted 150-zL samples threefold with a 150
mmol/L solution of NaC1, with both the Micromedic
dilutor
and the Hamilton syringe, then measured
total protein in all
these dilutions by the modified aca procedure. The error was
expressed as:
% error
=
(results
Micromedic
The influence
after syringe dilution
dilution/results
of viscosity
-
results
after syringe
on total protein
after
dilution)
X 100
values was also
3A
3B
plasma sample
patient N. E. ret ,, 12
Concentrated
horn
Glycerol solutions
rel ,,,
9
50
Oco
0
uJ
0
10
Microm.d<O
-
rned,c
Lu
SQ
TOTAL PROTEIN (gIL)
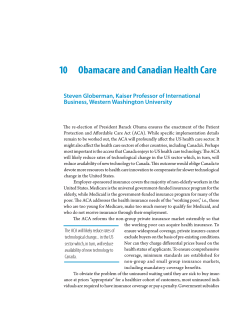
Fig. 1. Effect of serum temperature
protein with the DuPont aca
on the measurement of total
Serum samples obtaIned at varIous times from patIent N.E., maintained at eIther
4 (#{149}),
25(A), or 37 (#{149})
#{176}C
for at least 10 mln before analysis by the regular or
modifIed aca procedure
SAMPLE VOLUME (uL)
Fig.3. Effect
of sample volume on the viscosity-dependent error
of the aca (#{149})
and Micromedic sampler-dilutor (A)
assessed with the SMA 12/60. For these studies, total protein
measured with the SMA 12/60 and also with the modified
aca procedure and the error expressed as:
was
error = (results
by modified
aca
-
Concentrated plasma samples from patient N.E. at plasmapheresis (A) or solutions containing constant amounts of albumin, creatinine, and urIc acid but
various concentrations of glycerol (50-70 mL/100 mL). B, C, 0, were analyzed
at 25 #{176}C
as described in Materials and Methods
results by SMA 12/60/
results by modified
aca)
X 100
We evaluated
the influence
of temperature
by placing
samples at 4,25, and 37 #{176}C
(in a water bath) for at least 10 mm
just before assay.
The influence of the sampling volume was studied with both
the Micromedic
sampler-dilutor
and the aca. For the Micromedic studies, we used sampling volumes of 50, 100, 150,
and 200 tL. For the studies with the aca, we assessed the in-
fluence of sampling volumes on various analytical procedures
that require different volumes of serum: creatinine
(200 L
of sample), total protein (160 tL), uric acid (60 ML), and albumin (20 fzL).
Results
This investigation
was prompted in part by the observation
that serum from N.E. was notably viscous at 4 #{176}C
but fluid at
25 or 37 #{176}C.
We therefore assessed the influence of sample
temperature on the accuracy of total protein in this patient’s
serum as measured with the aca. When the protein concentration was <90 g/L, no errors were found at any sample
temperature (Figure 1). At higher protein concentrations,
progressively increasing errors were observed, strikingly so
when the sample was at 4 #{176}C.
To further assess the influence of viscosity, we tested the
aca, SMA 12/60, and the Micromedic, using solutions with
various glycerol concentrations.
Figure 2 shows that sampling
errors due to viscosity when total protein is measured can be
large by the regular aca procedure, are smaller with the Micromedic sample-dilutor, and are undetectable with the SMA
12/60.
Sampling error as a function of sample volume was assessed
by use of serum from patient N.E., obtained by plasmapheresis (Figure 3A), and with three different glycerol solutions
(Figures 3B, C, and D). Clearly, the amount of sample being
aspirated has a major effect on the viscosity-related
sampling
errors. At a given viscosity, the extent of sampling error was
proportional
to the volume of sample being aspirated.
RELATIVE VISCOSITY
Fig. 2. Effect of viscosity on the measurement of total protein
at 25 #{176}C
with the aca (A), SMA 12/60 (s), and Micromedic
sampler-dilutor
()
Samples were glycerol solutionsof variousviscosities but constant protein. For
the Micromedic sampler-dilutor, a 150-MLsample volume was diluted threefold
with 150 mmol/L NaCI before assay as described in Materials and Methods
Discussion
Our data indicate that falsely low values may be obtained
when viscous serum samples are used in the aca. Simulation
of this error by use of glycerol solutions allows each laboratory
or manufacturer
to assess viscosity effects in their own instruments. When we used a different discrete sampler-dilutor
CLINICAL CHEMISTRY,
Vol. 27, No. 11, 1981
1897
Sampler
Size
21-gauge needle
aca
Aspiration
0.145
Sera as well as other body fluids from patients
with these disorders may be viscous (pleural, peritoneal,
synovial, etc.) and may be subject to error when analyzed by
the regular aca procedure. We recommend the modified aca
procedure when analyzing such samples.
eases (5,6-12).
Table 1. Characteristics of Sampling Devices
Tested
time
s per 20 tL
of uniform i.d.,
mm
-0.6
Micromedic
sampler-
polyethylene tubing
of 2 mm i.d. taper-
dilutor,
Model 24004
K.-M. C. was supportedby NIH TrainingGrantno.0822ES07066A.
Carolyn Ann Craig for the viscosity determinations,
and
Linda Dickey for her secretarial assistance.
3 s for all vol
We thank
ing to a tip of
References
0.5 mm i.d.
SMA12/60
0.86 mm i.d.
-0.42
1. Vader, H. L., and Vink, C. L. J.,The influenceof viscosity
on
of serum sodi-
s per 20
dilution methods: Its problems in the determination
um. Clin. Chim. Acta 65, 379-388 (1975).
(cat. no.
A17 1-0343-0 1)
2. Haven, G. T.,and Haven, M. C.,Serum sodium measurement
manual and online dilutions. Clin. Chem. 19, 791 (1973). Letter.
SMA 12/60, these errors were either far
lower or not observed.This is because the sample probe of the
(Micromedic)
or a
aca has the smallest diameter
and the shortest sampling interval (Table 1).
Such sampling errors were negligible for samples with total
protein
<90 g/L from our patient, but relative viscosity of
serum will vary with type as well as concentration
of protein
(4). Our data suggest that samples with a relative viscosity
>9
are likely to result in sampling
error on the aca. However,
because
viscosity
widely
differing
relative
viscosity
is temperature-dependent,
content but
#{176}C
(the temperature
at
measured)
may behave
immunoglobulmn
viscosity at 37
is commonly
samples with
with the same
which relative
differently
at
or 4 #{176}C
(4). Although sampling of specimen
at 4 #{176}C
is unwarranted,
our data indicate that the errors are
greater at 4#{176}C-another
reason to ensure that samples should
not be analyzed while they are still at refrigerator tempera-
room temperature
ture.
High relative viscosity values are observed in 50% of patients with WaldenstrOms macroglobulinemia (4), in 8% of
patients with multiple myeloma (4), and (relatively infrequently) in patients with immunoglobulin-anti-immunoglobulin complexes occasionally associated with rheumatoid
arthritis, Sjogrens syndrome, or other connective tissue dis-
1898
CLIMCAL CHEMISTRY, Vol. 27, No. 11, 1981
by
3. Cryer, P. E., and Kissane, J. M., Rheumatoid arthritis with Felty’s
syndrome, hyperviseosity and immunologic hyperreactivity.
Am. J.
Med. 70,89-100 (1981).
4. Somer, T., The viscosity of blood, plasma and serum in dys- and
para-proteinemias.
Acta Med. Scand. Suppl. 456, 1097 (1966).
5. Fahey, J. L., Barth, W. F., and Solomon, A., Serum hyperviscosity
syndrome. J. Am. Med. Assoc. 192, 464-467 (1965).
6. Kosaka, M., and Solomon,A.,Hyperviscosity
syndrome associated
withan idiopathic
monoclonalIgA-rheumatoidfactor.
Am. J. Med
69, 145-165 (1980).
7. Hadler, N. M., Gabriel, D., Chung, K. S., et al., Polyclonal hyperviscosity
syndrome.Arthritis Rheum. 20, 1388-1395 (1977).
8. Pope, R. M., Fletcher,
M. A.,Mamby, A.,and Shapiro, C. M.,
Rheumatoid arthritis associated with hyperviscosity
syndrome
and
intermediate complex formation. Arch. Intern. Med. 135, 281-285
(1975).
9. Alarc#{243}n-Segovia,
D., Fishbein, E., Abruzzo, J. L., et al.,Serum
hyperviscosity in Sjogren’s syndrome. Interactionbetween serum IgG
and IgG rheumatoid factor.Ann. Intern. Med. 80, 35-42 (1974).
10. Blaylock, W. M., Waller, M,, and Normansell, D. E.,Sjogren’s
syndrome hyperviscosityand intermediate complexes. Ann. Intern.
Med. 80,27-34 (1974).
11. Abruzzo,J.L.,Heimer,R.,Guilianno,
V.,and Martinez,J.,The
hyperviscosity
syndrome,polysynovitis,
polymyositis
and an unusual
13S serum IgG component. Am. J. Med. 49, 258-264 (1970).
12. Jasin, H. E., LoSpalluto, J., and Ziff, M., Rheumatoid hyperviscosity syndrome. Am. J. Med. 49, 484-493 (1970).









© Copyright 2026