
2 0 1 3 Interventional Radiology Coding Update nineteenth edition
Interventional Radiology Coding Update 2 0 13 nineteenth edition 2013 Interventional Radiology Coding Update Coding for Endovascular and Interventional Procedures and Services Society of Interventional Radiology American College of Radiology Edition 2013 Copyright © 2013 by the Society of Interventional Radiology and the American College of Radiology. All rights reserved. No part of this publication covered by the copyright hereon may be reproduced or copied in any form or by any means—graphic, electronic or mechanical, including photocopying, taping or information storage and retrieval systems—without written permission of the publishers. CPT® five-digit codes, nomenclature and other data are copyright © 2012 American Medical Association. No fee schedules, basic units, relative values or related listings are included in CPT. The AMA assumes no liability for the data contained herein. CPT is a listing of descriptive terms and five-digit numeric identifying codes and modifiers for reporting medical services performed by physicians. This edition of the Update contains only CPT terms, codes and modifiers that were selected by SIR for inclusion in this publication. table of contents 5 Foreword 7 Glossary of Acronyms 9 Categories of CPT® Codes 11 The Basics of Coding and Reimbursement 19 Evaluation and Management (E&M) Codes 24 Revised Interventional Radiology Codes for 2013 24 Vertebral Body, Embolization or Injection 24 Respiratory System 27 New 2013 CPT Codes Common to Interventional Radiology 27 Thoracentesis 27 Cervicocerebral Angiography 30 Deleted RS&I Codes 31 Foreign Body Retrieval 31 Transcatheter Thrombolysis 33 Diagnostic Radiology (Diagnostic Imaging) 34 Endovascular Revascularization 39 Special Coding Note for 2013: Embolization Therapy for Benign Prostatic Hyperplasia (BPH) 42 Frequently Asked Questions 2013 INTERVENTIONAL RADIOLOGY C O D I N G U P D AT E PA G E 4 ONLINE SUPPLEMENT TA B L E O F CONTENTS 45 Individual Coverage Request Sample Letters 45 Percutaneous Radiofrequency Ablation of Pulmonary Tumor(s) 50 Ovarian Vein Embolization (OVE) to Treat Pelvic Congestion Syndrome (PCS) 56 MRI of the Pelvis for UFE 60 Sample 2013 Charge Sheets 2013 INTERVENTIONAL RADIOLOGY C O D I N G U P D AT E PA G E 5 ONLINE SUPPLEMENT FOREWORD foreword The 2013 Interventional Radiology Coding Update provides coding information to physicians, coders and administrators on what is new for 2013 in coding and reimbursement in the specialty of interventional radiology. By providing specialized information, as well as presenting some common coding scenarios, the intent is to supplement the Current Procedural Terminology (CPT) manual. Readers should always consult the CPT Professional manual as the definitive source of coding information. Other AMA resources, such as the CPT Assistant series, also commonly cover coding topics of interest to endovascular specialties. In 2013, the trend of bundling existing codes continued. In response to coding “screens” utilized by the Centers for Medicare and Medicaid Services (CMS), and implemented by the American Medical Association’s Specialty Society RVS Update Committee (RUC), specialty societies were instructed to develop new CPT codes that combined the procedure codes with the radiological supervision and interpretation (RS&I) code. New CPT codes were established for foreign body retrieval, carotid angiography, thrombolysis and chest tube procedures. These new codes are described in this Update. Coding of interventional radiology procedures can often seem a daunting task. While the transition to bundled codes is ongoing, many codes that are part of the component coding system remain in effect. This has resulted in something of a hybrid coding system, with new bundled codes existing alongside older component codes. Physicians and coders should exercise care, as there are some scenarios where the two coding systems can be utilized together. In this Update, we point out several of those scenarios. Over the past years, the amount of volunteer time that SIR and ACR members contribute to the coding and reimbursement process has 2013 INTERVENTIONAL RADIOLOGY C O D I N G U P D AT E PA G E 6 ONLINE SUPPLEMENT FOREWORD continued to grow. The efforts of the volunteer coders, physicians and associates are gratefully acknowledged by the Society of Interventional Radiology and American College of Radiology. Their work and insightful comments have directly resulted in this 2013 Update. Fairfax, Virginia Reston, Virginia 2013 INTERVENTIONAL PA G E 7 RADIOLOGY C O D I N G U P D AT E ONLINE SUPPLEMENT G L O S S A RY glossary of acronyms AAA ABN ABPTS ACO ACR AMA APC ASC AV AVF CAC CF CMD CMS CPT DRG E&M GPCI HCFA HCPCS HOPPS ICD-CM ICD-9-CM IDE IDTF IVUS LCD MAC MP Abdominal Aortic Aneurysm Advanced Beneficiary Notice American Board of Physical Therapy Specialties Accountable Care Organization American College of Radiology American Medical Association Ambulatory Payment Classification Ambulatory Surgical Center Arteriovenous Arteriovenous Fistula Carrier Advisory Committee Conversion Factor Carrier Medical Director Centers for Medicare and Medicaid Services Current Procedural Terminology Diagnosis-related Group Evaluation and Management Geographic Practice Cost Index Health Care Financing Administration Healthcare Common Procedure Coding System Hospital Outpatient Prospective Payment System International Classification of Diseases, Clinical Modification International Classification of Diseases, Ninth Revision, Clinical Modification Investigational Device Exemption Independent Diagnostic Testing Facility Intravascular Ultrasound Local Coverage Determination Medicare Adminstrative Contractor Malpractice OF ACRONYMS 2013 INTERVENTIONAL PA G E 8 RADIOLOGY C O D I N G U P D AT E ONLINE SUPPLEMENT G L O S S A RY MPFS MPPR MUE NCCI NEC NCHS NOS NP PA PE PIN POS PTA RAC RAW RBMA RBRVS RFA RS&I RS/IS&I RUC RVS RVU SIR SOAP TAA Medicare Physician Fee Schedule Multiple Procedure Payment Reduction Medically Unlikely Edit National Correct Coding Initiative Not Elsewhere Classified National Center for Health Statistics Not Otherwise Specified Nurse Practitioner Physician’s Assistant Practice Expense Provider Identification Number Place of Service Percutaneous Transluminal Angioplasty Recovery Audit Contractor Relativity Assessment Workgroup Radiology Business Management Association Resource-based Relative Value Scale Radiofrequency Ablation Radiological Supervision and Interpretation Radiological Supervision and Interpretation/Imaging Supervision and Interpretation RVS Update Committee Relative Value Scale Relative Value Unit Society of Interventional Radiology Subjective Evaluation, Objective Evaluation, Assessment and Plan Thoracic Aortic Aneurysm OF ACRONYMS 2013 INTERVENTIONAL RADIOLOGY C O D I N G U P D AT E PA G E 9 ONLINE SUPPLEMENT C AT E G O R I E S OF CPT CODES C AT E G O RY I C AT E G O RY I I categories of CPT ® codes CPT code proposal requests submitted to the AMA CPT Editorial Panel must identify what category of CPT code is being sought. The Panel reviews requests for three types of CPT codes. C AT E G O R Y I C O D E S These represent established services and procedures, performed by a variety of providers, in multiple geographical locations, with appropriate FDA approval for all aspects of the procedure. C AT E G O R Y I I C O D E S These codes are used to track performance measures. They are intended to facilitate data collection and not serve for billing purposes. Category II codes also are used in the Physician Quality Reporting System (PQRS) to report quality measures related to services provided under the Medicare Physician Fee Schedule. The PQRS is a voluntary pay-for-performance program in Medicare. It offers a financial incentive to physicians and other eligible professionals who successfully satisfy quality measures related to their services. C AT E G O R Y I I I C O D E S These are issued for emerging technologies not meeting standards for a Category I code. Additional information regarding the different categories of CPT codes can be found on the AMA Web site at www.ama-assn.org/ama/pub/physician-resources/solutions-managing-yourpractice/coding-billing-insurance/cpt/about-cpt/category-iii-codes.shtml. C AT E G O RY I I I 2013 INTERVENTIONAL PA G E RADIOLOGY 10 C O D I N G U P D AT E ONLINE SUPPLEMENT C AT E G O R I E S OF CPT CODES OTHER HCPCS CODES OTHER HCPCS CODES CMS may also issue Level II Healthcare Common Procedure Coding System (HCPCS) codes to report physician services, including G - C o d e s These are temporary codes issued by CMS to describe procedures and professional services. S - C o d e s These are temporary codes issued by CMS, often at the request of a commercial carrier. While S-codes are NOT eligible for use within the Medicare program, commercial carriers may elect to utilize these codes to facilitate claims processing. A listing of current HCPCS Level II codes may be found at www.cms.hhs.gov/HCPCSReleaseCodeSets/ANHCPCS/list.asp. 2013 INTERVENTIONAL PA G E RADIOLOGY 11 C O D I N G U P D AT E ONLINE SUPPLEMENT THE BASICS OF CODING RBRVS the basics of coding and reimbursement T H E R E L AT I V E VA L U E P AY M E N T S Y S T E M ( R B R V S ) In 1992, Medicare adopted a national system of payment using the Resource-based Relative Value Scale (RBRVS). Under the RBRVS, procedures are weighted and assigned a value on the basis of their difficulty, intensity, time and resource utilization. In the RBRVS system, a procedure’s RVU total is derived by summing the physician’s work (time and intensity), the practice expense (PE) related to performing the service, and malpractice costs associated with the procedure. Additionally, in order to take into account regional cost variations, CMS folds in what is termed the Geographic Practice Cost Index (GPCI). The GPCI rates are reviewed annually by CMS for their relevancy and accuracy. Finally, every year, CMS publishes in the Final Rule for the Physician Fee Schedule a figure called the conversion factor (CF). For CY 2013, the CF is $34.0230. Determining how much a service is paid is not a straightforward task. In recent years, most of the Medicare Administrative Contractors (MACs) have published on their Web sites helpful tables that show the physician fee schedule for the coming year for their covered region. Depending on whether a provider practices in the nonfacility (i.e., physician office) or facility (i.e., hospital) setting, the actual formula for provider payment is as follows: 2013 INTERVENTIONAL PA G E RADIOLOGY 12 C O D I N G U P D AT E ONLINE SUPPLEMENT THE BASICS OF CODING CPT PROCESS 2013 Nonfacility Pricing Amount = [(Work RVU * Work GPCI) + (Transitioned Nonfacility PE RVU * PE GPCI) + (MP (Malpractice) RVU * MP GPCI)] * CF 2013 Facility Pricing Amount = [(Work RVU * Work GPCI) + (Transitioned Facility PE RVU * PE GPCI) + (MP RVU * MP GPCI)] * CF On the member’s homepage of www.SIRweb.org, SIR has created tables that display all of the RVU component values for the common interventional radiology CPT codes. CPT PROCESS CPT codes are developed by the AMA CPT Editorial Panel in consultation with CMS and the CPT Advisory Committee which includes representatives from numerous specialty and subspecialty societies and allied medical societies. CPT Advisory Committee membership is limited to those national medical societies seated in the AMA House of Delegates. Since the practice of medicine is dynamic, the need for new CPT codes to reflect changes in practice often arises. Code change proposals are submitted to the AMA through the medical specialty societies, or individually, through a standard application process. Assessment of the supporting scientific literature and informal survey by the societies of a number of individuals performing the procedure in question helps assess the need for the new procedural code, its validity and the language that will be proposed to describe it. After a case can be made to support editing CPT to include a new procedure, the application is heard by the CPT Editorial Panel, which contains representatives of approximately 20 medical and allied organizations. 2013 INTERVENTIONAL PA G E RADIOLOGY 13 C O D I N G U P D AT E ONLINE SUPPLEMENT THE BASICS OF CODING RUC PROCESS The AMA holds three CPT Editorial Panel meetings per year, most commonly in February, May and October. To ensure release of the upcoming year’s updated CPT manual each fall, all proposed additions or revisions to Category I CPT codes for the upcoming calendar year must be heard by the Panel by the preceding February meeting. For example, new Category I codes approved by the Panel at the May 2011, October 2011 and February 2012 Panel meeting are reflected in the 2013 edition of CPT. The CPT cycle has stringent deadlines for submission of proposals that are well in advance of Panel meetings to ensure all advisers have an opportunity to review and comment. The general public is allowed to register for and attend AMA CPT Editorial Panel meetings. Information regarding CPT submission deadlines and Panel meetings can be found on the AMA Web site, www.ama-assn.org/ama/pub/category/3113.html. RUC PROCESS When the CPT Editorial Panel approves a new Category I CPT code, including newly bundled codes, the RUC process is initiated and a recommended relative value is developed. This provides Medicare and other payers a uniform scale on which to base payment. In the case of a revised code, depending on the nature of the change, the code’s value may be reevaluated through the RUC process. Category III codes are not referred to the RUC for valuation; instead reimbursement levels are set directly by those carriers electing to provide coverage for the performance of these “emerging technologies.” The RVS Update Committee (RUC) develops physician work RVU recommendations for new and revised CPT codes. Specialties comprising the RUC Advisory Committee designate their level of interest for developing 2013 INTERVENTIONAL PA G E RADIOLOGY 14 C O D I N G U P D AT E ONLINE SUPPLEMENT THE BASICS OF CODING RUC PROCESS work RVU recommendations based on recent actions taken by the CPT Editorial Panel. The supporting societies must survey members of their organizations using a standardized survey tool for data on time, intensity and risk of the procedure, including all the necessary pre- and postprocedural work. Based on the amount of physician work involved, each individual surveyed is asked to weigh the procedure in comparison to a defined standard procedure with which they are familiar. These data are assimilated and summarized for the valuation process. If more than one specialty is involved, a consensus value must be reached. Direct practice expenses including supplies, equipment and clinical staff time are also examined for both in-facility(hospital) and nonfacility (office) settings. For example, even for facility-based services there is often a direct practice expense for clinical staff time spent on the completion of preservice diagnostic/referral forms, coordination of presurgery services, scheduling of facility space for a procedure, review of test and exam results, follow-up phone calls and prescriptions. As with the physician work value, these data are also summarized for consideration by the RUC and, if more than one specialty is involved, consensus regarding these inputs must be reached. The proposed work value along with practice expense inputs for officebased procedures are submitted for consideration by the (RUC). After debate, the RUC will recommend physician work and practice expense values that serve as recommendations to the Centers for Medicare and Medicaid Services (CMS), which is the final decision-maker regarding RVUs. CMS’ final decision on RVUs and other payment policies usually appear each November in the Federal Register. (A copy of the Physician Fee Schedule is available to the general public for download via the CMS Web page, www.cms.hhs.gov/PhysicianFeeSched/PFSRVF/list.asp.) Mandated “budget neutrality” may negatively impact the payment associated with RVUs of existing codes when new codes are created. The extent of any 2013 INTERVENTIONAL PA G E RADIOLOGY 15 C O D I N G U P D AT E ONLINE SUPPLEMENT THE BASICS OF CODING CMS SCREENS change is determined by the number of RVUs assigned to the procedure and the number of times the procedure is performed annually. This provides a clear incentive to societies with representatives on the RUC to assure that all valuations are fair and accurate. The Medicare RVS is designed to pay for services on the basis of the amount of work involved without regard to the specialty of the provider(s) performing the service. Since 1992, all physician specialty types use the same code(s) to report the procedural component of an interventional radiology service. Similarly, the supervision of imaging personnel and interpretation of images obtained during the procedure is reported by the use of radiological supervision and interpretation/imaging supervision and interpretation (RS/IS&I) code(s) without regard to the specialty of the physician who performs the service. If a single physician performs both phases of the service, that single physician utilizes both codes (i.e., procedural and RS/IS&I). If several physicians perform portions of a service, each reports only those codes reflecting the procedure that they performed. CMS SCREENS AND HOW CODES ARE ASSIGNED TO THE RUC PROCESS In their rule-making process, CMS has identified groups of codes they feel are misvalued using 12 different screens including: New Technology, High Volume Growth, Fastest Growing Procedures and old Harvard-valued codes with utilization over 30,000 procedures annually. For additional information on the RUC screening process, see www.ama-assn.org/resources/doc/rbrvs/five-year-progress.pdf. 2013 INTERVENTIONAL PA G E RADIOLOGY 16 C O D I N G U P D AT E ONLINE SUPPLEMENT THE BASICS OF CODING THE FIVE-YEAR REVIEW THE FIVE-YEAR REVIEW Since the implementation of the Medicare Resource-based Relative Value Scale (RBRVS) Physician Fee Schedule in January 1992, Congress (through the Omnibus Budget Reconciliation Act of 1990) has required CMS to review the physician’s work relative value units within the Medicare Fee Schedule (MFS). CMS is required to conduct these reviews at least once every five years. This process, known as the Five-year Review, is used to identify, and reconsider the valuation of, potentially misvalued codes. The results from the first Five-year Review were implemented on Jan. 1, 1997, and subsequent reviews have been implemented every five years with the most recent implementation in 2012. Currently, the review process focuses only on the physician work RVU values. However, it is expected that future reviews will include re-examination of the practice expense RVU values for potentially misvalued codes as well. THE RUC ROLLING FIVE-YEAR REVIEW In 2006, prompted by concerns raised by MedPAC, legislators, CMS and others, the AMA established the Five-year Review Identification Workgroup as a subcommittee under the RUC. The Five-Year Review Identification Workgroup (now known as the Relativity Assessment Workgroup [RAW]) engages in a “rolling,” ongoing process to identify potentially misvalued codes outside the traditional, formal Five-year Review process. Since its inception, the Workgroup has targeted more than 320 codes for further review by the RUC including many radiology and interventional radiology codes. 2013 INTERVENTIONAL PA G E RADIOLOGY 17 C O D I N G U P D AT E ONLINE SUPPLEMENT THE BASICS OF CODING NCCI N AT I O N A L C O R R E C T C O D I N G I N I T I AT I V E ( N C C I ) In order to prevent payment of perceived abuses in procedural reporting, Congress authorized HCFA (now CMS) to begin the National Correct Coding Initiative (NCCI) in 1996. The primary intent of the NCCI has been to identify coding pairs that cannot or should not be performed at the same time (so called "mutually exclusive" pairs), and to promote “correct coding” of services reported together including the prevention of billing of inherent procedures in conjunction with comprehensive procedures (commonly referred to as “unbundling”). NCCI edits are developed by CMS through a subcontract with Correct Coding Solutions LLC (http://correctcodingsolutions.com/). Most proposed new NCCI edits are distributed by the AMA to specialty societies for comment, which may include critique of the appropriateness of the edits, as well as applicable use of the NCCI modifier indicator. CMS and Correct Coding Solutions review comments with follow-up communication when necessary. Following the comment process, edits to be implemented go forward as part of regular quarterly carrier system updates. An NCCI modifier indicator of “0” indicates that NCCI-associated modifiers cannot be used to bypass the edit. A modifier indicator of “1” indicates that NCCI-associated modifiers can be used to bypass an edit under appropriate circumstances. (Please see the Modifier chapter for additional information.) NCCI edits including identification of the associated modifier indicator status are available to the public free-of-charge and can be downloaded from the CMS Web page, www.cms.hhs.gov/NationalCorrectCodInitEd/NCCIEP/list.asp#TopOfPage. 2013 INTERVENTIONAL PA G E RADIOLOGY 18 C O D I N G U P D AT E ONLINE SUPPLEMENT THE BASICS OF CODING MUES Effective Jan. 1, 2013, two new NCCI-associated modifiers have been added: modifiers - 2 4 and - 5 7 . M o d i f i e r - 2 4 Unrelated evaluation and management service by the same physician or other qualified health care professional during a postoperative period M o d i f i e r - 5 7 Decision for surgery M E D I C A L LY U N L I K E LY E D I T S ( M U E S ) Beginning in January 2007 CMS began using national “medically unlikely edits” (MUEs). These edits are commonly referred to as frequency unit edits; they result in the limitation of the frequency (or number of units) that a particular service can be reported by the same provider/provider group for a given date of service. ADD-ON CODE EDITS Edits are also known to exist that limit the use of certain “add-on” codes (those codes are identified with a “+ ” designation). These edits result in rejection of the add-on code when reported in conjunction with a code not on the approved list. CMS has asserted that these edits are determined at the local level. The SIR and ACR coding advisers carefully review all the proposed NCCI edits, and the Society frequently comments and submits opinion letters objecting to a proposed edit if clinical scenarios and typical patient care practices indicate that the edit might be in error. 2013 INTERVENTIONAL PA G E RADIOLOGY 19 C O D I N G U P D AT E ONLINE SUPPLEMENT E VA L U AT I O N & MANAGEMENT CODES evaluation and management (E&M) codes Several years ago, CMS eliminated payment for outpatient (9 9 2 4 1 to 9 9 2 4 5 ) and inpatient (9 9 2 5 1 to 9 9 2 5 5 ) consultation codes. Consultations performed in an outpatient office are coded using the existing codes for new (9 9 2 0 1 to 9 9 2 0 5 ) or established (9 9 2 1 1 to 9 9 2 1 5 ) patients. Consultations performed on inpatients are coded using the existing codes for initial (9 9 2 2 1 to 9 9 2 2 3 ) or subsequent (9 9 2 3 1 to 9 9 2 3 3 ) hospital care visits. This does not mean that consultations should not be performed on Medicare patients. The CPT codes for consultation services have not been eliminated. When these services are provided to Medicare patients, they will be billed with different codes as outlined above. Elimination of payment for consultation codes has been evolving for several years because of discrepancies between the CMS requirements for consultations and the AMA interpretation of these requirements. This led to a CMS finding that consultation services were often billed inappropriately by not meeting the definition of a consultation or not having appropriate documentation to support the use of consultation codes. Furthermore, the documentation requirements for consultations, which were initially stricter than for other types of E&M services, are now similar to these other services and, therefore, do not warrant the higher payment that was associated with consultation services. The work relative value units (RVUs) for new and established office visits have increased by approximately 6 percent to reflect the elimination of the office consultation codes. The work RVUs for initial hospital and facility 2013 INTERVENTIONAL PA G E RADIOLOGY 20 C O D I N G U P D AT E ONLINE SUPPLEMENT E VA L U AT I O N & MANAGEMENT CODES visits are increased by approximately 2 percent. This has increased the payments for both of these services. In addition, the increased use of these visits will be incorporated into PE and MP RVU calculations. Finally, the incremental work RVUs for the E&M codes that are built into the 10-day and 90-day global surgical codes were increased as well. Third-party payers have not released information about reporting consultations. Payers may or may not choose to follow this policy. Therefore, all physicians providing consultation services must be aware of the payment policies from their local and regional providers to know which codes to submit when rendering these services. E&M CODING AND INTERVENTIONAL RADIOLOGISTS Over the past several years, SIR has encountered a handful of instances in which some hospital systems or payers deny payment for E&M claims submitted by radiologists and interventional radiologists. SIR’s standing position is that E&M services are allowable and can be appropriately claimed by any provider performing the services, including radiologists and interventional radiologists. Interventional radiologists perform total patient care; it is fully appropriate for interventional radiologists to document such care with E&M codes. We understand that some carriers have denied payments for E&M services provided by all radiologists because they have assumed that the services that were being reported were not true E&M services but rather focused history and physicals to satisfy Joint Commission (formerly Joint Commission on Accreditation of Healthcare Organizations) requirements for current documentation on the chart for invasive procedures. Our Society has worked with several of these carriers to educate them on the actual E&M work provided by clinical interventional radiologists and to 2013 INTERVENTIONAL PA G E RADIOLOGY 21 C O D I N G U P D AT E ONLINE SUPPLEMENT E VA L U AT I O N & MANAGEMENT CODES differentiate these E&M services from the work that is already included in invasive procedure valuations. Many interventional radiology procedures require longitudinal care, identical to many other fields of medicine. Patients are evaluated preprocedure to determine their state of health, presenting illness and underlying conditions. Appropriate testing is ordered to fully diagnose their pathology. The patient is advised of all potential treatment options including, but not limited to, options provided by interventional radiologists. If the patient’s condition is deemed suitable for treatment by the interventional radiologist, then he or she is scheduled for treatment and the service is rendered. Follow-up care is given as appropriate, and patients are often followed in a clinical office to monitor the effectiveness of the therapy and the progress of the underlying condition. Additionally, radiologists providing breast care, specifically mammography services, also perform separate E&M services, advising patients on treatment options. This is entirely analogous to services as provided by medical and surgical specialists such as gastroenterologists, surgeons and cardiologists. In another example of appropriate E&M, an interventional radiologist is asked to provide his or her clinical opinion regarding the appropriateness of a procedure for a given patient. When a patient is referred by another physician, the specialist physician routinely documents his or her services with an E&M code. For example, interventional radiologists see patients who have been referred for possible procedures for spinal fractures (vertebroplasty/kyphoplasty), peripheral arterial disease, uterine fibroids and oncologic cases (e.g., ablation therapies and Y-90 spheres). For inpatients, it is appropriate to perform and document consults. If the consult is performed and fully documented on the same day as a procedure, one should add modifier – 5 7 to the E&M code, designating that the consult 2013 INTERVENTIONAL PA G E RADIOLOGY 22 C O D I N G U P D AT E ONLINE SUPPLEMENT E VA L U AT I O N & MANAGEMENT CODES led to a decision to treat and is a separate service. Inpatient rounds also lead to frequent changes in patient management. For inpatient rounds, IR physicians should follow the global period rules for billing. As a result of these evaluations, many patients referred for a specific procedure may ultimately have care that differs from the procedure named on the request. A procedure may be cancelled or changed to a different procedure and follow-up or additional imaging may be recommended rather than a procedure. Hospitals may use different information systems, but it is important to note that, when a physician orders a procedure from the interventional radiology department, the interventional radiologist will still be required to exercise his or her clinical evaluative skills and judgment before performing the procedure. There are easily conceivable scenarios in which a procedure is ordered but, after a review of all medical information, the interventional radiologist decides that such a procedure is not warranted. The interventional radiologist would communicate this decision to the referring physician and would document and charge for his or her consultation but not the procedure. If the procedure is indeed warranted and performed by the IR, the IR will still have been required to evaluate the patient. For inpatient rounds, interventional radiologists should follow the global period rules for billing. Inpatient rounds lead to frequent changes in patient management. All of the above clinical actions are appropriately billed with E&M codes. E&M coding is appropriate for IR clinical work and indicates that a higher level of care is being offered to patients under the care of that IR practice. SIR has always made a distinction between routine preprocedure care and the more complex and time-consuming patient interaction that takes place as part of a formal consult. To help clarify the guidelines, SIR stated in 2006: “If you are asked to see a patient for input into that patient’s management and you evaluate that patient to develop an 2013 INTERVENTIONAL PA G E RADIOLOGY 23 C O D I N G U P D AT E ONLINE SUPPLEMENT E VA L U AT I O N & MANAGEMENT CODES assessment and plan and then document the encounter and your recommendations appropriately, then you have performed the work of a consultation and should bill the correct E&M code. However, if you are seeing a patient before a previously arranged procedure and the purpose of that visit is to confirm that the patient can go through that procedure and to obtain informed consent for the procedure, then consider that encounter to be bundled into the procedure itself and do not bill separately for that encounter. Only you will know the reason for the encounter and therefore only you can make that decision.” (“Coding for Consultations in Interventional Radiology,” IR News, Nov./Dec. 2006, p. 14; http://members.SIRweb.org/members/newsPDF/IRNewsNovDec2006.pdf). 2013 INTERVENTIONAL PA G E RADIOLOGY 24 C O D I N G U P D AT E ONLINE SUPPLEMENT NEW AND REVISED IR CODES REVISED IR CODES FOR NEW AND REVISED interventional radiology codes for 2013 REVISED INTERVENTIONAL RADIOLOGY CODES FOR 2013 For 2013, a number of revisions and code clarifications were added to several common codes used by interventional radiologists. Ve r t e b r a l B o d y, E m b o l i z a t i o n o r I n j e c t i o n The add-on code + 2 2 5 2 2 (each additional thoracic or lumbar vertebral body [List separately in addition to code for primary procedure]) has been revised to include moderate (conscious) sedation. The AMA CPT manual denotes the inclusion with the bull’s eye symbol ☉. Respiratory System New codes for endoscopy procedures have been created for 2013. Bronchoscopy Codes 3 1 6 2 2 – 3 1 6 4 8 include fluoroscopic guidance, when performed. ☉3 1 6 2 2 Bronchoscopy, rigid or flexible, including fluoroscopic guidance, when performed, diagnostic, with cell washing, when performed (separate procedure) ☉31623 with brushing or protected brushings 2013 2013 INTERVENTIONAL PA G E RADIOLOGY 25 C O D I N G U P D AT E ONLINE SUPPLEMENT NEW AND REVISED IR CODES REVISED IR ☉31624 with bronchial alveolar lavage ☉31625 with bronchial or endobronchial biopsy(s), single and multiple sites ☉31626 with placement of fiducial markers, single or multiple ☉31627 with computer-assisted, image-guided navigation (list separately in addition to code for primary procedure(s) ☉31628 with transbronchial lung biopsy(s), single lobe ☉31629 with transbronchial needle aspiration biopsy(s), trachea, main stem and/or lobar bronchus(i) ☉31634 with balloon occlusion, assessment of air leak, with administration of occlusive substance (e.g., fibrin glue) if performed (Do not report 3 1 6 3 4 in conjunction with 3 1 6 4 7 , 3 1 6 5 1 at the same session.) ☉31635 with removal of foreign body (For removal of implanted bronchial valves see 3 1 6 4 8 – 3 1 6 4 9 .) ☉31647 with balloon occlusion, when performed, assessment of air leak, airway sizing and insertion of bronchial valve(s), initial lobe ☉31648 with removal of bronchial valve(s), initial lobe removal and insertion of bronchial valve at the same session, see 3 1 6 4 7 , 3 1 6 4 8 and 3 1 6 5 1 ) (3 1 6 5 6 has been deleted. To report, see code 3 1 8 9 9 .) CODES FOR 2013 2013 INTERVENTIONAL PA G E RADIOLOGY 26 C O D I N G U P D AT E ONLINE SUPPLEMENT NEW AND REVISED IR CODES REVISED IR Bronchial Thermoplasty CODES FOR 2013 ☉ 3 1 6 6 0 Bronchoscopy, rigid or flexible, including fluoroscopic guidance, when performed; with bronchial thermoplasty, 1 lobe ☉31661 with bronchial thermoplasty, 2 or more lobes (3 1 7 1 5 has been deleted. To report, use code 3 1 8 9 9 .) Lungs and Pleura (3 2 4 2 0 has been deleted. To report, use 3 2 4 0 5 .) (3 2 4 2 1 and 3 2 4 2 2 have been deleted. To report, see codes 3 2 5 5 4 , 3 2 5 5 5 .) (3 2 5 5 1 has been revised for tube thoracostomy to indicate that this code is now used for reporting an open procedure.) ☉ 3 2 5 5 3 Placement of an interstitial device(s), for radiation therapy guidance (e.g., fiducial markers, dosimeter), percutaneous, intrathoracic, single or multiple (Report supply of device separately.) For percutaneous placement of an interstitial device(s), such as fiducial marker or dosimeter, for radiation therapy guidance within the abdomen, pelvis (except prostate) and/or retroperitoneum, report ☉ 4 9 4 1 1 . Imaging guidance codes (7 6 9 4 2 , 7 7 0 0 2 , 7 7 0 1 2 or 7 7 0 2 1 ) and device codes (e.g., A 4 6 4 8 tissue marker, A 4 6 5 0 implantable radiation dosimeter or A 4 6 4 9 surgical supply) are reported separately in conjunction with the percutaneous placement procedure codes. 2013 INTERVENTIONAL PA G E RADIOLOGY 27 C O D I N G U P D AT E ONLINE SUPPLEMENT NEW AND REVISED IR CODES NEW 2013 NEW 2013 CPT CODES COMMON TO INTERVENTIONAL RADIOLOGY Thoracentesis Four new codes have been created describing thoracentesis and pleural drainage. Codes 3 2 5 5 4 – 3 2 5 5 7 are NOT to be reported in conjunction with codes 3 2 5 5 0 , 3 2 5 5 1 , 7 6 9 4 2 , 7 7 0 0 2 , 7 7 0 1 2 , 7 7 0 2 1 , 75989. 3 2 5 5 4 Thoracentesis, needle or catheter, aspiration of the pleural space; without imaging guidance 32555 with imaging guidance 3 2 5 5 6 Pleural drainage, percutaneous, with insertion of indwelling catheter; without imaging guidance 32557 with imaging guidance To report insertion of indwelling tunneled pleural catheter with cuff, see code 3 2 5 5 0 . Moderate sedation is NOT inherent to procedure codes 3 2 5 5 4 – 3 2 5 5 7 and should be reported separately when these services are provided. Cervicocerebral Angiography Eight new cervicocerebral angiography codes have been created to report nonselective and selective arterial catheter placement and diagnostic imaging of the aortic arch, carotid and vertebral arteries, 3 6 2 2 1 – 3 6 2 2 8 . Accompanying the new codes is extensive introductory language describing the new codes and reporting instructions. This new section starts on p. 207 of the CPT 2013, Professional Edition code book. CPT CODES 2013 INTERVENTIONAL PA G E RADIOLOGY 28 C O D I N G U P D AT E ONLINE SUPPLEMENT NEW AND REVISED IR CODES NEW 2013 These codes describe arterial contrast injections with arterial, capillary and venous-phase imaging, when performed. Accessing the vessel, placement of catheter(s), contrast injection(s), fluoroscopy, RS&I and the closure of the arteriotomy by pressure or by application of an arterial closure device is inherent in codes 3 6 2 2 1 – 3 6 2 2 6 and not separately reportable. Moderate sedation is included in the new codes, and is not separately reportable. Codes 3 6 2 2 1 – 3 6 2 2 6 progress up a hierarchy in which the lesser intensive services are included in the higher intensity code—i.e., use the code of the most intensive service provided. For example, 3 6 2 2 1 is reported for nonselective catheter placement, thoracic aorta, with angiography of the aortic arch and great vessel origins. Do not report 3 6 2 2 1 in conjunction with 3 6 2 2 2 – 3 6 2 2 6 selective codes, as these include the work of 3 6 2 2 1 when performed. ☉ 3 6 2 2 1 Nonselective catheter placement, thoracic aorta, with angiography of the extracranial carotid, vertebral, and/or intracranial vessels, unilateral or bilateral, and all associated radiological supervision and interpretation, includes angiography of the cervicocerebral arch, when performed. (Do not report 3 6 2 2 1 with 3 6 2 2 2 – 3 6 2 2 6 .) ☉ 3 6 2 2 2 Selective catheter placement, common carotid or innominate artery, unilateral, any approach, with angiography of the ipsilateral extracranial carotid circulation and all associated radiological supervision and interpretation, includes angiography of the cervicocerebral arch, when performed. ☉ 3 6 2 2 3 Selective catheter placement, common carotid or innominate artery, unilateral, any approach, with angiography of the ipsilateral intracranial carotid circulation and all associated radiological supervision CPT CODES 2013 INTERVENTIONAL PA G E RADIOLOGY 29 C O D I N G U P D AT E ONLINE SUPPLEMENT NEW AND REVISED IR CODES NEW 2013 and interpretation, includes angiography of the extracranial carotid and cervicocerebral arch, when performed. ☉ 3 6 2 2 4 Selective catheter placement, internal carotid artery, unilateral, with angiography of the ipsilateral intracranial carotid circulation and all associated radiological supervision and interpretation, includes angiography of the extracranial carotid and cervicocerebral arch, when performed. Do not report 3 6 2 2 2 , 3 6 2 2 3 or 3 6 2 2 4 together for ipsilateral angiography. Select the most comprehensive service following the hierarchy of complexity. ☉ 3 6 2 2 5 Selective catheter placement, subclavian or innominate artery, unilateral, with angiography of the ipsilateral vertebral circulation and all associated radiological supervision and interpretation, includes angiography of the cervicocerebral arch, when performed. ☉ 3 6 2 2 6 Selective catheter placement, vertebral artery, unilateral, with angiography of the ipsilateral vertebral circulation and all associated radiological supervision and interpretation, includes angiography of the cervicocerebral arch, when performed. Do not report 3 6 2 2 5 with 3 6 2 2 6 for ipsilateral angiography. Select the most comprehensive service following the hierarchy of complexity. ☉ + 3 6 2 2 7 Selective catheter placement, external carotid artery, unilateral, with angiography of the ipsilateral external carotid circulation and all associated radiological supervision and interpretation (List separately in addition to code for primary procedure.) (Use 3 6 2 2 7 in conjunction with 3 6 2 2 2 , 3 6 2 2 3 or 3 6 2 2 4 .) ☉ + 3 6 2 2 8 Selective catheter placement, each intracranial branch of the internal carotid or vertebral arteries, unilateral, with angiography of the selected vessel circulation and all associated radiological supervision and CPT CODES 2013 INTERVENTIONAL PA G E RADIOLOGY 30 C O D I N G U P D AT E ONLINE SUPPLEMENT NEW AND REVISED IR CODES NEW 2013 interpretation (e.g., middle cerebral artery, posterior inferior cerebellar artery). (List separately in addition to code for primary procedure.) (Use 3 6 2 2 8 in conjunction with 3 6 2 2 4 or 3 6 2 2 6 .) (Do not report 3 6 2 2 8 more than twice per side.) Add modifier – 5 0 to codes 3 6 2 2 2 – 3 6 2 2 8 if the same procedure is performed on both sides. Modifier – 5 9 may be used to indicate when different carotid and/or vertebral arteries are being studied in the same session. Report 7 6 3 7 6 or 7 6 3 7 7 for 3D rendering when performed in conjunction with 3 6 2 2 1 – 3 6 2 2 8 . Report 7 6 9 3 7 for ultrasound guidance for vascular access, when performed in conjunction with 3 6 2 2 1 – 3 6 2 2 8 . Deleted RS&I Codes As part of the new bundled cervicocerebral angiography codes, several angiography supervision and interpretation codes have been deleted. These are in the radiology section of CPT, under the subheading Vascular System—Aorta and Arteries RS&I. 7 5 6 5 0 To report see codes 3 6 2 2 1 – 3 6 2 2 6 . 7 5 6 6 0 To report see code 3 6 2 2 7 . 7 5 6 6 2 To report use code 3 6 2 2 7 and append modifier – 5 0 . 7 5 6 6 5 To report see codes 3 6 2 2 3 , 3 6 2 2 4 . 7 5 6 7 1 To report see codes 3 6 2 2 3 and 3 6 2 2 4 and append modifier – 5 0 as appropriate. CPT CODES 2013 INTERVENTIONAL PA G E RADIOLOGY 31 C O D I N G U P D AT E ONLINE SUPPLEMENT NEW AND REVISED IR CODES NEW 2013 7 5 6 7 6 To report see codes 3 6 2 2 2 – 3 6 2 2 4 . 7 5 6 8 0 To report see codes 3 6 2 2 2 – 3 6 2 2 4 and append modifier – 5 0 as appropriate. 7 5 6 8 5 To report see codes 3 6 2 2 5 – 3 6 2 2 6 . Fo r e i g n B o d y R e t r i e v a l For 2013, a new bundled CPT code has been created that bundles the procedure with the radiological supervision and interpretation. The previous CPT code for foreign body retrieval, 3 7 2 0 3 , has been deleted, along with the RS&I code, 7 5 9 6 1 . ☉ 3 7 1 9 7 Transcatheter retrieval, percutaneous, of intravascular foreign body (e.g., fractured venous or arterial catheter), includes radiological supervision and interpretation, and imaging guidance (ultrasound or fluoroscopy), when performed (7 5 9 6 1 has been deleted. To report, use code 3 7 1 9 7 .) (For percutaneous retrieval of a vena cava filter, use 3 7 1 9 3 .) Tr a n s c a t h e t e r T h r o m b o l y s i s Four new codes have been created to report transcatheter thrombolytic arterial or venous infusion. These new codes cover the entire therapeutic period of time. Critical guidance on these new codes is shown on p. 218 of the CPT 2013 Professional Edition printed code book. Codes 3 7 2 1 1 and 3 7 2 1 2 are used to report the initial day of transcatheter thrombolytic infusion including follow-up CPT CODES 2013 INTERVENTIONAL PA G E RADIOLOGY 32 C O D I N G U P D AT E ONLINE SUPPLEMENT NEW AND REVISED IR CODES NEW 2013 arteriography/venography and catheter position change or exchange, when performed. When initiation and completion of thrombolysis occur on the same calendar day, report only 3 7 2 1 1 or 3 7 2 1 2 . Catheter placement(s), diagnostic studies and other percutaneous interventions may be reported separately. Codes 3 7 2 1 1 – 3 7 2 1 4 include fluoroscopic guidance and associated RS&I. Ultrasound guidance for vascular access—see code 7 6 9 3 7 —may be reported separately when all required elements are performed. Bilateral thrombolytic infusion through separate access site(s) may be reported with modifier – 5 0 in conjunction with 3 7 2 1 1 , 3 7 2 1 2 . Radiological supervision and interpretation codes 7 5 8 9 6 and 7 5 8 9 8 have been revised and are not to be reported in conjunction with 3 7 2 1 1 – 3 7 2 1 4 for thrombolysis infusion management. 3 7 2 1 1 Transcatheter therapy, arterial infusion for thrombolysis other than coronary, any method, including radiological supervision and interpretation, initial treatment day. 3 7 2 1 2 Transcatheter therapy, venous infusion for thrombolysis, any method, including radiological supervision and interpretation, initial treatment day. 3 7 2 1 3 Transcatheter therapy, arterial or venous infusion for thrombolysis other than coronary, any method, including radiological supervision and interpretation, continued treatment on subsequent day, during course of thrombolytic therapy, including follow-up catheter contrast injection, position change, or exchange, when performed 37214 cessation of thrombolysis including removal of catheter and vessel closure by any method CPT CODES 2013 INTERVENTIONAL PA G E RADIOLOGY 33 C O D I N G U P D AT E ONLINE SUPPLEMENT NEW AND REVISED IR CODES NEW 2013 The previous code for thrombolysis, 3 7 2 0 1 , has been deleted—see codes 37211–37214. Code 7 5 9 0 0 has been deleted; see codes 3 7 2 2 1 – 3 7 2 1 4 for reporting exchange of a previously placed intravascular catheter during thrombolytic therapy. Diagnostic Radiology (Diagnostic Imaging) Chest 7 1 0 4 0 , 7 1 0 6 0 have been deleted. To report, use 7 6 4 9 9 . Spine and Pelvis 7 2 0 4 0 Radiologic examination, spine, cervical; 3 views or less 72050 4 or 5 views 72052 6 or more views 7 2 2 7 5 Epidurography, radiological supervision and interpretation (7 2 2 7 5 includes 7 7 0 0 3 ) (For injection procedure, see 6 2 2 8 0 – 6 2 2 8 2 , 6 2 3 1 0 – 6 2 3 1 9 , 6 4 4 7 9 – 6 4 4 8 4 .) (Use 7 2 2 7 5 only when an epidurogram is performed, images documented, and a formal radiologic report is issued.) (Do not report 7 2 2 7 5 in conjunction with 2 2 5 8 6 , 0 1 9 5 T , 0 1 9 6 T , 0 3 0 9 T .) CPT CODES 2013 INTERVENTIONAL PA G E RADIOLOGY 34 C O D I N G U P D AT E ONLINE SUPPLEMENT NEW AND REVISED IR CODES ENDOVASCULAR R a d i o l o g y G u i d e l i n e s , Va s c u l a r P r o c e d u r e s — Aorta and Arteries Parenthetical revisions have been added for aortography codes 7 5 6 0 0 , 7 5 6 0 5 and 7 5 6 3 5 and angiography, pulmonary codes 7 5 7 4 6 , 7 5 7 5 6 and 7 5 7 7 4 . Providers may review these changes in the CPT® 2013 codebook. E N D O VA S C U L A R R E VA S C U L A R I Z AT I O N Guidelines have been updated for lower-extremity endovascular procedures for 2013 to inform users of specific types of closure procedures that are inherent to these procedures, and which specify services that are separately reportable. When treating multiple vessels within a territory, report each additional vessel using an add-on code, as applicable. Select the base code that represents the most complex service using the following hierarchy of complexity (in descending order of complexity): atherectomy and stent> atherectomy >stent >angioplasty. When treating multiple lesions within the same vessel, report one service that reflects the combined procedures, whether done on one lesion or different lesions, using the same hierarchy. These codes take into account that multiple techniques may be needed in order to open areas of disease in some vessels, and that these interventions may take place in different vascular territories. In general, the codes for interventions progress up a hierarchy of intensity with the work of the lessintense intervention included in the higher intensity code. For example, angioplasty prior to a stent placement would be a progression up this hierarchy and only the stent code would be reported. Each of these codes includes the work of accessing the artery, selecting the vessel, crossing the lesion, interpreting the images, performing therapeutic intervention(s) in REVASCULARIZATION 2013 INTERVENTIONAL PA G E RADIOLOGY 35 C O D I N G U P D AT E ONLINE SUPPLEMENT NEW AND REVISED IR CODES ENDOVASCULAR the entire vessel segment, using any embolic protection device, performing final image interpretation and closing the arteriotomy by any method. If angioplasty is performed in addition to facilitate a more advanced procedure, such as atherectomy, or stenting, it is included in the code for the more advanced procedure. Moderate sedation is also included in each of these codes. Mechanical thrombectomy and thrombolysis are not included in the work of codes 3 7 2 2 0 – 3 7 2 3 5 and can be reported additionally with the appropriate component codes when these techniques are used in combination with PTA/stenting/atherectomy to restore flow to areas of occlusive disease. As in the past, thrombolysis used as part of mechanical thrombectomy is not separately reportable. When a thrombolytic infusion is performed either subsequent or prior to mechanical thrombectomy, it is separately reported. The codes apply to the procedure if performed percutaneously or open. Revascularization procedures are grouped into three vascular territories based on the anatomy and are specific to the procedures of angioplasty, stenting or atherectomy. (PTA is considered an inherent part of stenting or atherectomy procedures and is not separately reportable.) Each code applies to a single extremity. 1 Iliac territory: subdivided into common, internal and external iliac artery a 37220–37223 b Single code used for a single vessel c Add-on codes used for additional iliac vessels that are treated (common, internal or external) 2 Femoral/popliteal territory: this entire territory is considered a single vessel a 37224–37227 REVASCULARIZATION 2013 INTERVENTIONAL PA G E RADIOLOGY 36 C O D I N G U P D AT E ONLINE SUPPLEMENT NEW AND REVISED IR CODES ENDOVASCULAR b Includes the common, deep and superficial femoral as well as popliteal c Since it is a single vessel, only a single code may be reported, even if multiple lesions are treated d If two procedures are performed in different areas of the vessel territory, report the code that includes all therapies provided in that region. 3 Tibial/peroneal territory: subdivided into anterior tibial, posterior tibial and peroneal a 37228–37235 b Report the initial vessel treated as the primary code for the highest level of service provided within the tibial-peroneal territory with addon codes for additional vessels treated (not additional lesions or procedures in the same vessel) c The tibioperoneal trunk is not considered a separate vessel If a lesion extends across the margin of a territory, but is opened with a single therapy, report with only a single code. For example, if a distal popliteal artery stenosis extends into the tibioperoneal trunk and the lesion is treated with a single angioplasty spanning both lesions, only code a single vessel treatment. If both legs are treated at the same time, use modifier – 5 9 to indicate separate and distinct services performed on the same day. A “+ ” sign indicates an add-on code that must be used after the appropriate code for the initial vessel treated. REVASCULARIZATION 2013 INTERVENTIONAL PA G E RADIOLOGY 37 C O D I N G U P D AT E ONLINE SUPPLEMENT NEW AND REVISED IR CODES ENDOVASCULAR Iliac Artery Revascularization 3 7 2 2 0 Revascularization, endovascular, open or percutaneous, iliac artery, unilateral, initial vessel; with transluminal angioplast 37221 with transluminal stent placement(s), includes angioplasty within same vessel when performed.) + 3 7 2 2 2 Revascularization, endovascular, open or percutaneous, iliac artery, each additional ipsilateral iliac vessel; with transluminal angioplasty (List separately in addition to code for primary procedure) (Used in conjunction with 3 7 2 2 0 , 3 7 2 2 1 for additional iliac segment PTA.) +37223 with transluminal stent placement(s), includes angioplasty within the same vessel, when performed (List separately in addition to code for primary procedure) (Used in conjunction with 3 7 2 2 1 for additional iliac segment stent placement) Femoral/Popliteal Artery Revascularization 3 7 2 2 4 Revascularization, endovascular, open or percutaneous, femoral, popliteal artery(s), unilateral; with transluminal angioplasty 37225 with atherectomy, includes angioplasty within the same vessel, when performed 37226 with transluminal stent placement(s), includes angioplasty within the same vessel, when performed 37227 with transluminal stent placement(s) and atherectomy, includes angioplasty within the same vessel, when performed REVASCULARIZATION 2013 INTERVENTIONAL PA G E RADIOLOGY 38 C O D I N G U P D AT E ONLINE SUPPLEMENT NEW AND REVISED IR CODES ENDOVASCULAR Ti b i a l / P e r o n e a l A r t e r y R e v a s c u l a r i z a t i o n 3 7 2 2 8 Revascularization, endovascular, open or percutaneous, tibial, peroneal artery, unilateral, initial vessel; with transluminal angioplasty 37229 with atherectomy, includes angioplasty within the same vessel, when performed 37230 with transluminal stent placement(s), includes angioplasty within the same vessel, when performed 37231 with transluminal stent placement(s) and atherectomy, includes angioplasty within the same vessel, when performed + 3 7 2 3 2 Revascularization, endovascular, open or percutaneous, tibial/peroneal artery, unilateral, each additional vessel; with transluminal angioplasty (List separately in addition to code for primary procedure.) (Used in conjunction with 3 7 2 2 8 – 3 7 2 3 1 .) +37233 with atherectomy, includes angioplasty within the same vessel, when performed. (List separately in addition to code for primary procedure.) (Used in conjunction with 3 7 2 2 9 , 3 7 2 3 1 .) +37234 with transluminal stent placement(s), includes angioplasty within the same vessel, when performed. (List separately in addition to code for primary procedure.) (Used in conjunction with 3 7 2 2 9 – 3 7 2 3 1 .) +37235 with transluminal stent placement(s) and atherectomy, includes angioplasty within the same vessel, when REVASCULARIZATION 2013 INTERVENTIONAL PA G E RADIOLOGY 39 C O D I N G U P D AT E ONLINE SUPPLEMENT NEW AND REVISED IR CODES BENIGN performed. (List separately in addition to code for primary procedure.) (Used in conjunction with 3 7 2 3 1 .) S P E C I A L C O D I N G N O T E F O R 2 0 1 3 : E M B O L I Z AT I O N T H E R A P Y F O R B E N I G N P R O S T AT I C H Y P E R P L A S I A ( B P H ) Benign prostatic hyperplasia (BPH) is a common ailment affecting many men as they age. Symptomatic patients often suffer considerable lowerurinary-tract discomfort, and decreased quality of life is often associated with BPH symptoms. Embolization of the prostatic arteries is a procedure that has shown some promise as a method to treat BPH in early small research studies, mostly done in Europe and South America. Further clinical research and trials are expected to commence in 2013 in the United States. SIR supports research on this procedure and will be supporting and closely following these trials to assess the early data and outcomes. In terms of coding and reimbursement, given the experimental nature of the procedure, SIR’s position is that physicians should discuss any proposed prostatic embolization procedure with their patients’ relevant Carrier Medical Directors. Since embolization for BPH is clearly an investigational procedure at this time, physicians should check with the insurance carrier prior to performing the procedure to determine if the procedure will be covered and how the procedure should be coded. The carriers could request that the procedure be coded with CPT code 3 7 7 9 9 (Unlisted Procedure, vascular surgery) to indicate its investigational nature. If component coding is allowed, the appropriate codes could include: P R O S TAT I C HYPERPLASIA 2013 INTERVENTIONAL PA G E RADIOLOGY 40 C O D I N G U P D AT E ONLINE SUPPLEMENT NEW AND REVISED IR CODES BENIGN • 3 7 2 0 4 (x1) (Transcatheter occlusion or embolization (e.g., for tumor destruction, to achieve hemostasis, to occlude a vascular malformation), percutaneous, any method, noncentral nervous system, non-head or neck), • 7 5 8 9 4 (x1) (Transcatheter therapy, embolization any method, radiological supervision and interpretation) • 3 6 2 4 7 (Up to maximum of 2 times) (Selective catheter placement, arterial system; initial third order or more selective abdominal, pelvic or lower-extremity artery branch, within a vascular family) • 3 6 2 4 8 catheter placement, arterial system; additional second order, third order, and beyond, abdominal, pelvic, or lower extremity artery branch, within a vascular family). 3 6 2 4 8 may be used if 2 branches have to be catheterized for study and/or embolization on the same side • 7 5 8 9 8 (x1) (Angiography through existing catheter for follow-up study for transcatheter therapy, embolization or infusion, other than for thrombolysis) Diagnostic angiography would, in most cases, not be additionally reported since the imaging of the pelvic vessels done prior to the embolization would be done for roadmapping purposes rather than diagnosis of BPH. However, if an interventional radiologist is performing the embolization as part of a clinical trial site, the physician should likewise discuss the trial and get pre-approval from the carrier prior to enrolling patients. There should be agreement with the carrier prior to enrolling patients as to how the procedures will be coded and paid. Some FDA IDE trials will allow use of existing CPT codes while others may designate that existing CPT codes are not applicable. In 2013, SIR will draft a new Category III CPT code to describe prostatic artery embolization for presentation to the American Medical Association’s P R O S TAT I C HYPERPLASIA 2013 INTERVENTIONAL PA G E RADIOLOGY 41 C O D I N G U P D AT E ONLINE SUPPLEMENT NEW AND REVISED IR CODES BENIGN CPT Editorial Panel. Category III codes describe emerging technologies or investigational procedures and also allow for data collection. If the new code is approved, SIR will inform members promptly through its outreach and educational venues, and it is anticipated that most carriers will require use of the new Category III code for reporting prostatic artery embolization to treat BPH. P R O S TAT I C HYPERPLASIA 2013 INTERVENTIONAL PA G E RADIOLOGY 42 C O D I N G U P D AT E ONLINE SUPPLEMENT FA Q S frequently asked questions FA Q 1 How do I code for internal iliac artery embolizations at the time of EVAR? Embolization performed at the time of an endovascular repair of an aneurysm (thoracic endovascular aortic repair [TEVAR] and endovascular aneurysm repair [EVAR]), including embolization of a hypogastric artery, is separately billable. Codes 3 7 2 0 4 , 7 5 8 9 4 , 7 5 8 9 8 and typically 3 6 2 4 5 are all appropriate to report this procedure. Use of a selective catheter placement code for embolization obviates the use of the 3 6 2 0 0 for placing a catheter in the aorta under coding convention rules. FA Q 2 What are the appropriate codes to report for sclerotherapy of nonvascular structures, such as seromas, cysts, lymphoceles or abscesses? The following CPT codes are reported for all nonvascular sclerosis procedures (e.g., seroma, cyst, lymphocele, abscess): 2 0 5 0 0 (Injection of sinus tract; therapeutic [separate procedure]) 7 6 0 8 0 (Radiologic examination, abscess, fistula or sinus tract study, radiological supervision and interpretation) The use of different agents (e.g., alcohol, tetracycline, betadine) does not limit or alter the reporting of these codes. Moderate sedation is not inherent to code 2 0 5 0 0 and is separately reportable. 2013 INTERVENTIONAL PA G E RADIOLOGY 43 C O D I N G U P D AT E ONLINE SUPPLEMENT FA Q S 9 9 1 4 4 Age 5 years or older, first 30 minutes intra-service time +99145 Each additional 15 minutes intra-service time Note that this is an add-on code (+ ) and must be used in conjunction with 9 9 1 4 4 . If the patient is being seen for new or worsening symptoms and E&M services provided by the interventionalist to evaluate those symptoms, those E&M services should be separately documented and coded. This E&M service may need to be reported with the use of appropriate modifiers (e.g., – 2 4 , – 2 5 ) as the patient’s recent operative history demands. FA Q 3 What are the appropriate codes to use when microwave ablation is the energy source used for liver, lung or renal lesions? The existing CPT codes for tumor ablation are defined for radiofrequency ablation. This definition has led to some confusion, occasionally resulting in the use of unlisted procedure codes for microwave ablation. SIR does not recommend the use of unlisted procedure codes for microwave ablation of kidney, lung or liver tumors. Microwave is part of the radiofrequency spectrum and uses a different part of the radiofrequency spectrum to generate heat energy to destroy abnormal soft tissue. Microwave ablation equipment is substantially comparable to operate in practice, which is also reflected in the U.S. Food and Drug Administration (FDA) approval of microwave devices under the 510(K) clearance process as equivalent to radiofrequency. As such, SIR recommends that CPT codes 4 7 3 8 2 , 3 2 9 9 8 and 5 0 5 9 2 be used for both microwave and radiofrequency ablation in their respective anatomic locations, in conjunction with the appropriate imaging guidance code: 2013 INTERVENTIONAL PA G E RADIOLOGY 44 C O D I N G U P D AT E ONLINE SUPPLEMENT FA Q S 4 7 3 8 2 Ablation, 1 or more liver tumor(s) percutaneous, radiofrequency; with appropriate image guidance code: 7 7 0 1 3 (CT), 7 6 9 4 0 (US), 7 7 0 2 2 (MRI) 3 2 9 9 8 Ablation therapy for reduction or eradication of 1 or more pulmonary tumor(s) including pleura or chest wall when involved by tumor extension, percutaneous, radiofrequency, unilateral; with appropriate image guidance code: 7 7 0 1 3 (CT), 7 6 9 4 0 (US), 7 7 0 2 2 (MRI) 5 0 5 9 2 Ablation, 1 or more renal tumor(s), percutaneous, unilateral, radiofrequency; with appropriate image guidance code: 7 7 0 1 3 (CT), 7 6 9 4 0 (US), 7 7 0 2 2 (MRI) 2013 INTERVENTIONAL PA G E RADIOLOGY 45 C O D I N G U P D AT E ONLINE SUPPLEMENT SAMPLE LETTERS individual coverage request sample letters The following are examples of a few common coverage request letters. The examples include letters for coverage for radiofrequency ablation of pulmonary tumor(s), ovarian vein embolization for pelvic congestion syndrome and MRI imaging of the uterus prior to uterine fibroid embolization. These templates include data, arguments for need and benefit and can save you considerable work P E R C U TA N E O U S R A D I O F R E Q U E N C Y A B L AT I O N O F P U L M O N A R Y T U M O R ( S ) [DATE ] [CARRIER MEDICAL DIRECTOR ] [COVERAGE RECONSIDERATION DEPARTMENT ] [CARRIER NAME ] [CARRIER ADDRESS ] [CARRIER CITY, STATE ZIP ] RE: [PATIENT NAME ] [PATIENT ID ] Request for coverage for Percutaneous Radiofrequency Ablation (RFA) of Pulmonary Tumor(s) [CARRIER MEDICAL DIRECTOR ]: On [INSERT DATE OF PRECERTIFICATION/COVERAGE REQUEST DENIAL ], notice was received from your company that radiofrequency ablation (RFA) of pulmonary tumor(s) is considered experimental and investigational, and, therefore, a noncovered service. This is a formal request for individual 2013 INTERVENTIONAL PA G E RADIOLOGY 46 C O D I N G U P D AT E ONLINE SUPPLEMENT SAMPLE LETTERS consideration to extend coverage for RFA of pulmonary tumor(s) for [PATIENT NAME ], who has been diagnosed with [INSERT DIAGNOSIS: lung cancer, lung metastases, lung malignancies, including stage ]. [PATIENT NAME ] has been seen and evaluated by a [SELECT REFERRING PHYSICIAN TYPE: thoracic surgeon/oncologist/oncology physician team ] who [is/are ] in agreement that pulmonary tumor RFA is the best treatment option for [PATIENT NAME ] at this time. [PATIENT NAME ] is not alone in suffering from [INSERT CONDITION: lung cancer, lung metastases, lung malignancies, including stage ]. Lung cancer kills more Americans than any other type of malignancy. The disease kills some 160,000 Americans a year—more than breast cancer, colon cancer and prostate cancer combined. Pulmonary Tumor RFA Is Safe and Effective The Society of Interventional Radiology “finds that RFA of pulmonary tumor(s) is a safe and effective treatment for a subset of patients with metastases to the lung, and patients with primary lung malignancies who are poor surgical candidates or refuse resection. In addition to tumor eradication, radiofrequency ablation is used to ‘debulk’ or reduce lung tumor increasing the effectiveness of adjunctive chemo- and/or radiation therapy or as a stand-alone treatment after failed conventional therapy for chest wall pain palliation.” Pulmonary tumor RFA has been shown to be an effective palliative therapy providing tumor control and pain relief. In order to provide an appropriate framework in which to accurately evaluate the efficacy of pulmonary RFA, we provide background information regarding traditional treatments. Life Expectancy, Rate of Tumor Growth and Tumor Control, for Lung Cancer Patients. Life expectancies for lung cancer patients vary according 2013 INTERVENTIONAL PA G E RADIOLOGY 47 C O D I N G U P D AT E ONLINE SUPPLEMENT SAMPLE LETTERS to the stage and overall health of the patient. For patients with metastases to the lung, nodule size typically doubles in 2–10 months. The rate of lung cancer spread varies greatly with each individual and cell type. However, tumor growth is typically seen over a few months and may result in the patient’s demise. For stage IV NSCLC patients, those “who do not receive any treatment live for an average of four months and approximately 5–10% remain alive one year from diagnosis.” For those patient receiving chemotherapy, the “average duration of patients’ survival was similar for all four [chemotherapy] treatment regimens and was between seven and eight months.” http://patient.cancerconsultants.com/lung_cancer_treatment.aspx?id=805 Typically, the only cure for lung cancer is surgical removal of the tumor(s). Typically, surgical intervention is only considered for stage I and II patients, with stage III patients occasionally found to be viable candidates. Surgery is rarely considered a treatment option for stage IV patients. The majority of lung cancer patients are found to have advanced disease at the time of initial diagnosis and are not considered viable surgical candidates. Even for those treated surgically, recurrence rates are quite high. The American Cancer Association does not present surgery as a definitive cure but rather advises that surgery “may cure lung cancer.” Historically, the surgical options offered are local wedge resection, lobectomy and pneumonectomy, several of which have been in use for well over a century. According to the National Cancer Institute (NCI), the efficacy of traditional surgical treatments for lung cancer is equivalent to the odds associated with tossing a coin: according to one study, recurrence rates are as high as 50% for stage I patients treated with wedge or segment resection. Per the NCI, the mortality rate for lobectomy is 3–5% and according to the Southern Illinois University Division of Cardiothoracic Surgery, a provider of these services, a thoracotomy incision is considered to be “one of the more 2013 INTERVENTIONAL PA G E RADIOLOGY 48 C O D I N G U P D AT E ONLINE SUPPLEMENT SAMPLE LETTERS painful incisions.” Recovery time after these invasive surgical treatments is substantial with at least a two-day stay in the Intensive Care Unit (ICU), and a total hospital stay of 5–10 days after lung resection. Chemotherapy and radiation can be considered as adjunctive therapies to surgical intervention. These techniques cannot be given earlier than 8 weeks after surgery since they may interfere with the body’s ability to heal. At this time, just as with traditional invasive surgical treatments, it is not known whether pulmonary RFA is a definitive “cure” for lung cancer. However, as adeptly stated by the Radiological Society of North America, “RFA is a relatively quick procedure that does not require general anesthesia. Recovery is rapid so that chemotherapy may be resumed almost immediately. Even when RFA does not remove all of a tumor, a reduction in the total amount of tumor may extend life for a significant time.” Control and Comfort It is generally accepted that tumor control results in increased life expectancy for patients with lung cancer. The FDA defines an “effective” drug [treatment] as one that achieves a 50% or more reduction in tumor size for 28 days. At this time, the focus of RFA is tumor control and at this time there are numerous studies that support that RFA is effective in tumor control. Tumor control is also commonly associated with relief of symptoms, providing patients with an increased quality of life. Body of Scientific Literature Supporting RFA of Pulmonary Tumor(s) As an Effective Treatment Studies show that patients who have pulmonary tumor(s) treated with RFA experience reduction and, in many instances, complete eradication of tumor(s). This is believed to extend life expectancy and/or result in increased comfort. Please see “Attachment A” for a list of supporting 2013 INTERVENTIONAL PA G E RADIOLOGY 49 C O D I N G U P D AT E ONLINE SUPPLEMENT SAMPLE LETTERS scientific literature for radiofrequency ablation of pulmonary tumor(s). Also, enclosed is a table (see Attachment B) summarizing the scientific articles available supporting RFA as an effective treatment. Proposed Treatment Plan for [INSERT PATIENT NAME ] In this procedure, the interventional radiologist guides a small needle through the skin into the tumor. Radiofrequency energy is transmitted to the tip of the needle, where it produces heat in the tissues. The tumor tissue shrinks and slowly forms a scar. It is ideal for nonsurgical candidates and those with smaller tumors. Once a patient such as [PATIENT NAME ] has been diagnosed with [INSERT CONDITION—lung cancer, lung metastases, lung malignancies—including stage ], it is imperative to implement treatment as quickly as possible. Depending on the size of the tumor, RFA can reduce the size and often completely eradicate the tumor. By decreasing the size of a large mass, or treating new tumors in the lung as they arise, the pain and other debilitating symptoms caused by the tumors are often relieved. While the tumors themselves may not be painful, they can cause mass affect on nerves or vital organs, eliciting pain. I respectfully request that you extend coverage to [PATIENT NAME ] for pulmonary tumor RFA. I hope you have found this information helpful in support of [reversing the previous denial authorizing coverage] for this procedure. Please feel free to contact me if you require any further information. Sincerely, [SIR/ACR MEMBER NAME ], MD CC: [PATIENT NAME ] [STATE INSURANCE COMMISSIONER ] 2013 INTERVENTIONAL PA G E RADIOLOGY 50 C O D I N G U P D AT E ONLINE SUPPLEMENT SAMPLE LETTERS O VA R I A N V E I N E M B O L I Z AT I O N ( O V E ) T O T R E AT P E LV I C C O N G E S T I O N S Y N D R O M E ( P C S ) [DATE ] [CARRIER MEDICAL DIRECTOR ] [COVERAGE RECONSIDERATION DEPARTMENT ] [CARRIER NAME ] [CARRIER ADDRESS ] [CARRIER CITY, STATE ZIP ] RE: [PATIENT NAME ] [PATIENT ID ] Request for coverage for Ovarian Vein Embolization (OVE) to treat Pelvic Congestion Syndrome (PCS) [CARRIER MEDICAL DIRECTOR ]: On [INSERT DATE OF PRECERTIFICATION/COVERAGE REQUEST DENIAL ], notice was received from your company that ovarian vein embolization (OVE) is considered experimental and investigational and therefore, a noncovered service. This is a formal request for individual consideration to extend coverage for OVE for [PATIENT NAME ], who is believed to be suffering from pelvic congestion syndrome (PCS). [PATIENT NAME ] has presented with symptoms consistent with pelvic congestion syndrome, which is a well defined condition. She has been seen by a vascular medicine physician, [VASCULAR MEDICINE PHYSICIAN NAME ], MD. Both Dr. [VASCULAR MEDICINE PHYSICIAN NAME ] and my findings are consistent; confirming that [PATIENT NAME ] has had recurrent varicose veins in the lower extremity(ies). Additionally, [LIST RELEVANT DIAGNOSTIC STUDY(IES). FOR EXAMPLE: an MR venogram of the pelvis shows large ovarian and 2013 INTERVENTIONAL PA G E RADIOLOGY 51 C O D I N G U P D AT E ONLINE SUPPLEMENT SAMPLE LETTERS pelvic veins, and an ultrasound of the pelvis has been performed, which demonstrated enlarged pelvic varicosities, more prominent on the left than the right. Reflux was noted in the left greater saphenous vein as well ] supporting a diagnosis of PCS for this patient. OVE has been found to be an effective minimally invasive procedure to treat the symptoms of PCS and is recommended for this patient. PCS Symptoms [PATIENT NAME ] is not alone in suffering with the symptoms of PCS. It has been estimated that almost 40% of all women will experience chronic pelvic pain during their lifetime and that 15% of all women between the ages of 18–50 experience chronic pelvic pain. Of note, 15% of all hysterectomies and 35% of all diagnostic laparoscopies are performed due to chronic pelvic pain. Ovarian vein incompetence has been shown to occur in approximately 10% of women. This phenomenon can lead to PCS and its associated symptoms in 60% of these patients. Despite this incidence, PCS is significantly under-diagnosed. It typically results in pelvic pain that is often described as dull and aching. The pain is typically worse in an upright position and becomes more severe with walking and postural changes. It may be associated with dyspareunia or a postcoital ache. These symptoms of pelvic congestion syndrome (PCS) are typically caused by the development of varicosities in the infundibulopelvic and broad ligaments within the pelvis. The exact reason why these varicosities develop is unknown, but one important factor is the absence or incompetence of valves in the ovarian veins. It is felt that there is an anatomic component to this as well, since reflux occurs more often on the left than the right. This may be due to the fact that veins are absent more often on the left than the right, but is also likely due to the fact that the left ovarian vein drains into the left renal vein before draining into the inferior vena cava, while the right ovarian vein drains directly into the inferior vena cava. This is why 2013 INTERVENTIONAL PA G E RADIOLOGY 52 C O D I N G U P D AT E ONLINE SUPPLEMENT SAMPLE LETTERS symptoms are often more common or more severe on the left side than the right, which is what we are seeing with [PATIENT NAME ]. A hormonal component is also felt to contribute to the development of PCS as well since it mainly affects premenopausal women. The pain associated with PCS has been directly attributed to the presence of these dilated veins within the pelvis. OVE Treatment Plan for PCS Once a patient such as [PATIENT NAME ] has been diagnosed with PCS, it is important to direct treatment towards eliminating retrograde flow in the abnormal ovarian vein(s). This reduces pressure in the pelvic veins which eliminates the development of these varicosities and the pain that they cause. This can all be accomplished with the use of ovarian vein embolization (OVE), which is a percutaneous, catheter-based procedure that results in occlusion of the abnormal ovarian vein(s). For the past 15 years, this treatment has been associated with good clinical outcomes in most women suffering from the symptoms of PCS. Currently, this procedure is technically successful in almost 100% of patients. Symptomatic improvement tends to be seen in >80% of patients undergoing OVE. Specific data includes that reported in 2006 by Kim, et al who found an 83% success rate in 127 patients treated with OVE. This particular study reported results after 4-year follow-up. Kwon, et al also reported data in 2007 that described symptomatic improvement in 82% of 67 patients treated with OVE. In 2002, Venbrux, et al reported symptomatic improvement in 96% of the 56 patients 12 months after being treated with OVE. Other reports by Mowatt, et al, Capasso, et al, Sichlar, et al, Tarazov, et al, Maleux, et al, and Cordts, et al have reported similar data to the studies outlined above. The OVE treatment plan includes an ovarian venogram to confirm that retrograde flow is present in the ovarian veins. If reflux and retrograde flow is identified within the left and/or right ovarian vein, then one would 2013 INTERVENTIONAL PA G E RADIOLOGY 53 C O D I N G U P D AT E ONLINE SUPPLEMENT SAMPLE LETTERS proceed with embolization of the abnormal vein to eliminate this reflux and reduce the pressure within these pelvic varicosities. This procedure would be performed on an [OUTPATIENT/INPATIENT ] basis. Patient’s Medical History Consistent With Varicose Veins of the Lower Extremity(ies)/Pelvis Otherwise Known As “PCS” A review of [PATIENT NAME ]’s medical history finds that she had [LIST RELEVANT FINDINGS SPECIFIC TO THE PATIENT’S HISTORY. FOR EXAMPLE: recurrent varicose veins following a vein stripping of her right leg. She had also developed labial varicosities with her first pregnancy and then with her second pregnancy the labial varicosities had markedly increased. She has also had increasing right varicose veins. ] Patient’s Current Symptoms Are Typical of Pelvic Congestion Syndrome [PATIENT NAME ]’s current symptoms are typical of PCS. The patient is experiencing extreme heaviness and discomfort in her pelvis with standing and also following sexual intercourse. Her pelvic discomfort is least in the morning and worsens during the day as she is standing. Her symptoms are very typical for ovarian vein reflux or potentially reflux into the internal iliac veins. PCS is initially caused by reflux into the ovarian vein, which then causes increased flow and pressure in the pelvic veins and causes severe pain in the pelvis. This is exactly the same as with varicoceles that are found in men. Body of Scientific Literature Supporting OVE As an Effective Treatment for PCS Attached is a comprehensive listing of the scientific literature available that supports OVE as an effective treatment for PCS (see Attachment A). Also 2013 INTERVENTIONAL PA G E RADIOLOGY 54 C O D I N G U P D AT E ONLINE SUPPLEMENT SAMPLE LETTERS enclosed is a table (see Attachment B) summarizing the scientific articles available supporting ovarian vein embolization as an effective treatment for PCS; many of these articles support that in many patients embolization of other pelvic veins may be required in addition to the OVE. To deny the existence of PCS contradicts these multiple articles. Tubal ovarian varices were described in the 1950s. The association between pelvic pain and varicosities was first described in 1928 and again in 1949. The association of these pelvic varicosities with PCS was described in 1964. In a 1984 study of laparoscopic and venographic studies in woman with unexplained chronic pelvic pain, 91% of them were found to have marked pelvic venous congestion. In 2002, a study examining incompetent ovarian veins demonstrated that with ligation of these veins 54% of them had resolution of their pelvic pain with improvement in 23%. There has been increasing recognition of this problem with multiple articles including a study from Korea where patients with documented pelvic congestion syndrome were randomized to hysterectomy (with either oopherectomy of ovary on the side of an incomplete gondal vein or bilateral oopherectomy) and OVE. OVE demonstrated significantly better results than surgery.To deny the existence of PCS contradicts these multiple articles. Tubal ovarian varices were described in the 1950s. The association between pelvic pain and varicosities was first described in 1928 and again in 1949. The association of these pelvic varicosities with PCS was described in 1964. In a 1984 study of laparoscopic and venographic studies in woman with unexplained chronic pelvic pain, 91% of them were found to have marked pelvic venous congestion. In 2002, a study examining incompetent ovarian veins demonstrated that with ligation of these veins 54% of them had resolution of their pelvic pain with improvement in 23%. There has been increasing recognition of this problem with multiple articles including a study from Korea where patients with documented pelvic congestion syndrome were randomized to hysterectomy (with either oopherectomy of 2013 INTERVENTIONAL PA G E RADIOLOGY 55 C O D I N G U P D AT E ONLINE SUPPLEMENT SAMPLE LETTERS ovary on the side of an incomplete gondal vein or bilateral oopherectomy) and OVE. OVE demonstrated significantly better results than surgery. Equitable Coverage Sought for Equivalent Treatments for Comparable Syndromes Found in Men and Women Varicose veins in the testicle of men is called varicoceles. Varicose veins of the uterus and pelvis of women is called pelvic congestion syndrome. These are comparable syndromes suffered by men and women. Your company will authorize coverage for testicular vein embolization to treat varicoceles in men. Yet, you are currently denying coverage for the equivalent treatment for the comparable syndrome (ovarian vein embolization for pelvic congestion syndrome) found in women. It is incomprehensible that men are allowed to undergo a procedure to cure their problem and that this same procedure, used to treat an equivalent syndrome, is denied for women. Your reversal of this inappropriate determination is respectfully requested. Please extend coverage [PATIENT NAME ] for ovarian vein embolization to treat pelvic congestion syndrome. I hope that you will find this information helpful in reversing the previous denial [FOR PREAUTHORIZATION/OF COVERAGE ]. Please feel free to contact me if you require any further information. Sincerely, [SIR/ACR MEMBER NAME ], MD [SIR/ACR MEMBER TITLE ] CC: [PATIENT NAME ] [STATE INSURANCE COMMISSIONER ] 2013 INTERVENTIONAL PA G E RADIOLOGY 56 C O D I N G U P D AT E ONLINE SUPPLEMENT SAMPLE LETTERS M R I O F T H E P E LV I S F O R U F E To Whom It May Concern: I am writing this letter to appeal your decision to deny coverage for an MRI of the pelvis for [PATIENT NAME ], (DOB: [INSERT DATE OF BIRTH ]; [PATIENT ID ]) prior to a uterine artery embolization (UAE) procedure to treat symptomatic uterine fibroids. As you know, UAE is a uterine-sparing procedure that effectively treats the symptoms associated with uterine fibroids and reduces both uterine and fibroid volume due to fibroid infarction. Prior to UAE, the interventional radiologist performing the procedure needs to be certain that the procedure is being performed for an appropriate indication. When fibroids were treated exclusively with hysterectomy, pre-procedure imaging was not critical to gynecologists because the uterus, in its entirety, was being removed. As a result, a pathologic evaluation performed on the uterus after surgery was the primary means of determining the etiology of the presenting symptoms. Uterine artery embolization is different. Since the uterus is remaining in its anatomic position and the fibroids are not being removed, it becomes incumbent upon the physician responsible for performing this procedure to obtain definitive imaging of the pelvis prior to the procedure. The standard imaging modality used to evaluate patients with suspected uterine fibroids is ultrasound. In fact, almost all patients presenting in consultation for UAE have been evaluated previously with a pelvic ultrasound that has demonstrated fibroids. While ultrasound is certainly a good test to evaluate patients for fibroids, it is an operator-dependent imaging modality that has recognized limitations when it comes to evaluating patients specifically for UAE. Omary, et al (J Vasc Interv Radiol 2013 INTERVENTIONAL PA G E RADIOLOGY 57 C O D I N G U P D AT E ONLINE SUPPLEMENT SAMPLE LETTERS 2002; 13:1149–1153) evaluated the importance of imaging prior to UAE and recommended that MRI be considered in all patients prior to this procedure. They did this by evaluating the diagnostic confidence and anticipated treatment plan both before and after performance of a pelvic MRI. They found that MRI significantly increased diagnostic confidence. In addition, they found that MRI changed the initial diagnosis in 18% of patients and the immediate clinical management in 22% of patients. Overall, 19% of women who were anticipated to undergo UAE prior MRI did not undergo that procedure as a result of the findings on MRI, which most often included abnormalities other than fibroids. MRI has also been shown to potentially predict the response to UAE and can therefore be helpful with patient selection for this procedure. An MRI can accurately determine the location and size of fibroids within the uterus. As described by Cura, et al (Acta Radiol 2006; 47:1105–1114), UAE may not be the appropriate therapy if a patient’s symptoms do not correlate with the size and location of their fibroids. For example, a small subserosal fibroid is not likely to be responsible for abnormal bleeding so UAE may not be indicated in this particular type of patient. In addition, MRI is helpful in differentiating degenerated fibroids from cellular fibroids, which is important since cellular fibroids typically have the best response to UAE. Cellular fibroids have characteristic MRI findings with high signal intensity on T2 weighted images and enhancement after contrast administration (Yamashita, et al, Radiology 1993; 189:721–725) so fibroids with these characteristics may be expected to respond best to UAE. This has been supported by Burn, et al (Radiology 2000; 214:729–734), who reported on the good response of fibroids with high signal intensity on T2-weighted images, and by Jha, et al (Radiology 2000; 217:228–235), who reported that hypervascular fibroids which enhanced after contrast administration had a greater response to UAE. Therefore, an MRI can help determine which patients are appropriate candidates for UAE on the basis of size, location, 2013 INTERVENTIONAL PA G E RADIOLOGY 58 C O D I N G U P D AT E ONLINE SUPPLEMENT SAMPLE LETTERS signal characteristics and degree of enhancement after contrast administration. The findings on MRI can also help determine if vessels other than the uterine arteries provide arterial supply to the fibroids. Kroencke, et al (Radiology 2006; 241:181–189) determined that contrast-enhanced MRI can help predict the presence of ovarian arterial supply to uterine fibroids. This information is important to have prior to UAE because if these vessels are not recognized, the ability of this procedure to induce infarction within the treated fibroids becomes significantly limited. In addition, knowing that ovarian arteries may need to be treated during a UAE procedure is something that is important to discuss with a patient prior to UAE since treating these vessels could increase the possibility of post-procedure amenorrhea. Finally, MRI is very helpful in determining if patients are potentially at risk for complications after UAE. For example, pedunculated submucosal fibroids are potentially at risk for transcervical expulsion or infection and pedunculated subserosal fibroids can potentially separate from the uterus and result in intraperitoneal complications. Pelvic MRI is able to define the morphology of pedunculated fibroids far better than ultrasound and therefore help determine which patients are potentially at risk for these complications. This was well described by Verma, et al (AJR 2008; 190:1220–1226) who reported on the utility of MRI in defining the interface between pedunculated submucosal fibroids and the endometrium. They found that this helps define the risk of fibroid migration into the endometrial cavity with subsequent transcervical expulsion after UAE. In summary, an MRI of the pelvis provides the information that is necessary for an interventional radiologist to determine if a patient with symptomatic uterine fibroids is a suitable candidate for uterine artery embolization. It can potentially provide information regarding the cellular morphology of 2013 INTERVENTIONAL PA G E RADIOLOGY 59 C O D I N G U P D AT E ONLINE SUPPLEMENT SAMPLE LETTERS fibroids, the presence or absence of other pathology that could explain a patient’s symptoms, the contribution of other blood vessels responsible for the arterial supply of fibroids, and the potential risk of complications associated with pedunculated fibroids. As a result, MRI has been shown to potentially change the treatment plan in a significant number of patients, underscoring its importance as a pre-procedure imaging test. It is my hope that this information will help support a reversal of your decision to deny coverage to [PATIENT NAME ] for an MRI of the pelvis prior to her planned uterine artery embolization procedure. 2013 INTERVENTIONAL PA G E RADIOLOGY 60 C O D I N G U P D AT E ONLINE SUPPLEMENT SAMPLE CHARGE SHEETS sample 2013 charge sheets Find the updated 2013 interventional radiology coding charge sheets at http://members.SIRweb.org/members/coding/chargeSheets.cfm www.acr.org/codingpubs. VASCULAR INTERVENTIONAL CHARGE SHEET DATE: REFERRING PHYSICIAN: INTERVENTIONAL RADIOLOGIST: Catheterization and Imaging Separately Reportable Unless Specifically Noted Otherwise for ALL Therapeutic Procedures MCS-Moderate Conscious Sedation Indicator @: Do NOT additionally report Moderate Conscious Sedation codes in conjunction with these Valuation for codes with @ in the MCS indicator column includes the physician work for conscious sedation. Procedure S&I Procedure S&I (x) MCS code Code (x) MCS Code Code THROMBOLYSIS AND INFUSION THERAPY DIALYSIS ACCESS INTERVENTIONS Transcatheter therapy, arterial infusion for thrombolysis other than coronary 37211 Clot removal any method @ 36870 N/A Venous infusion for thrombolysis 37212 Dialysis Fistulagram @ 36147 N/A 37213 Add'l puncture (document in dictation) @ 36148 N/A Continued thrombolytic infusions(s) on subsequent day(s) 37214 PTA, A-V fistula arterial 35475 75962 Thrombolytic infusion(s) Final Day of therapy 37202 75896 PTA, A-V fistula venous 35476 75978 Infusion, Non-Thrombolytic Infusion for Thrombolysis, cerebral 37195 75970 Fistulogram with needles in N/A 75791 Intravascular stent 37205 75960 Angio thru exist cath F/U embo/other than for thrombolysis 49418 N/A N/A 75898 Insertion of tunneled intraperitoneal catheter (eg, dialysis) N/A MECHANICAL THROMBECTOMY includes imaging guidance Insertion of tunneled intraperitoneal catheter w/ subcutaneous po 49419 Primary Arterial Mech Thromb - initial vessel @ Peritoneal dialysis catheter placement open 49421 N/A 37184 49422 N/A Removal of tunneled intraperitoneal catheter Primary Arterial Mech Thromb @ 37185 Peritoneogram (Air &/or contrast) 49400 74190 2nd/and all subsequent vessel(s) Secondary Mech Thromb- "rescue", suction, snare basket @ 37186 TRANSCATHETER THERAPY MISC. Venous Mech Throm - Day 1 @ 37187 Foreign Body Retrieval @ 37197 N/A IVC Filter Insertion @ 37191 Venous Mech Throm - repeat mech thrombectomy on subsequent day during a course of therapy IVC Filter Respositioning @ 37192 @ 37188 x __ IVC Filter Retrieval (Removal) @ 37193 EMBOLIZATION (per surgical field) INTRAVASCULAR ULTRASOUND* Embolization (Non-Neuro, Non-UFE)* 37204 75894 imaging and catheterization(s) 37210 IVUS initial vessel 37250 75945 @ Each additional vessel IVUS 37251 75946 Cerebral Balloon Occlusion Test (BOT) includes 61623 imaging and catheterization of target vessel PERCUTANEOUS ANGIOPLASTY PTA, Renal or Visceral Artery @ 35471 75966 Embolization (CNS)* permanent 61624 75894 61626 75894 PTA, Aorta @ 35472 75966 Embolization (non-CNS) Head or Neck F/U Angio study for transcatheter therapy, embolization or infusion, other than for thrombolysis PTA, Brachiocephalic Arteries @ 35475 75962 N/A 75898 PTA, Venous @ 35476 75978 Add'l agent -prescribing, handling, and bolus administration chemotherapeutic agent 96420 PTA, Each add'l visceral vessel @ 35471 x __ 75968 x __ PTA, Each add'l brachiocephalic vessel @ 35475 x __ 75964 x __ 79445 radioactive agent TIPS (includes catheterization and associated imaging) PTA, Each additional venous @ 35476 x __ 75978 x __ INTRA-OPERATIVE (OPEN) ANGIOPLASTY TIPS 37182 PTA, Renal or Visceral Artery 35450 75966 TIPS Revision @ 37183 PTA, Aorta 35452 75966 36011 or 75894 PTA, Brachiocephalic vessels 35458 75962 Embolization of varix* 36012 + 75898 PTA, Venous 35460 75978 + 37204 *Note: Report selective catheterization codes in addition to embolization. INTRACRANIAL DILATION, ANGIOPLASTY, STENT MODERATE (CONSCIOUS) SEDATION includes selective catheterization and all imaging of target vessel Intracranial angioplasty 61630 provided by same physician performing the Dx-Tx service 61635 Intracranial angioplasty with stent Intraservice Start Time: __________ End Time:___________ 61640 99144 Dilation of intracranial vasospam, initial vessel Conscious Sedation AGE 5 or OLDER first 30 min 61641 99145 x __ each add vessel same vascular family each additional 15 minutes 61642 99143 each add vessel different vascular family Conscious Sedation UNDER 5 first 30 min 99145 x __ each additional 15 minutes INTRAVASCULAR STENTS Intravascular Stents Non-Coronary/Non-Carotid/Non-Vertebral/Non-Intracranial OTHER Intravascular Stent, perc., initial 37205 75960 Pseudoaneurysm TX Injection (Thrombin) 36002 Specific Imaging Guidance for Needle Plcmnt (circle one) US-76942 fluoro-77002 CT-77012 MR-77021 Intrasvascular Stent, perc., each add'l vessel 37206 75960 Intravascular Stent, open, initial 37207 75960 Closure Device G0269 Intrasvascular Stent, open, each add'l vessel 37208 75960 CT, limited or localized follow-up 76380 Intravascular Stents Cervical Carotid US Guidance for Vascular Access 76937 includes all ipsilateral selective cath, ipsilateral cervical/cerebral angiography (required documentation on file) Intravascular Stent w/ distal embolic protection @ 37215 N/A UNLISTED IMAGING CODES Intravascular Stent w/out distal embolic protection @ 37216 N/A Unlisted, Fluoroscopic procedure 76496 Intravascular Stents Extracranial Vertebral/Intrathoracic Carotid Unlisted, CT procedure 76497 includes all ipsilateral selective cath, target vessel angiography Unlisted, MR procedure 76498 Intravascular Stent, perc; initial vessel 0075T N/A Unlisted, US procedure 76999 Intravascular Stent, perc; each addl. vessel 0076T N/A UNLISTED VASCULAR PROCEDURE Unlisted, vascular surgery 37799 Append Clinical Trial Modifier PRESENTING PROBLEM(S)/DIAGNOSIS ICD-9: _____ Dx 1: __________________ Service provided within FDA approved clinical trial PATIENT: PROCEDURE: ATTACH REPORT (and device approved for use in the trial at the time the service was rendered.) IDE # -Q0 CPT Only copyright 2012 American Medical Association. All Rights Reserved. Dx 2 :_________________ ICD-9: _____ Copyright 2012, Society of Interventional Radiology. All Rights Reserved. VASCULAR INTERVENTIONAL CHARGE SHEET PATIENT: 2 DATE: REFERRING PHYSICIAN INTERVENTIONAL RADIOLOGIST PROCEDURE: X MCS ENDOVASCULAR VARICOSE VEIN TREATMENT includes imaging guidance catheterization is considered inherent to EVAT Radiofrequency - 1st vein treated. RFA - 2nd & subs. vein(s) Laser EVAT- includes imaging- 1st vein Laser - 2nd & subs. vein(s) OTHER VARICOSE VEIN TREATMENT PROCEDURE CODE 36475 36476 36478 36479 Injections of sclerosing solutions (single/multiple), spider veins; limb or trunk 36468 Injections of sclerosing solutions (single/multiple), spider veins; face Injection of sclerosing solution- single vein Injection of sclerosing solution- multiple veins, same leg 36469 36470 36471 Stab phlebectomy of varicose veins, one extremity, 10-20 incisions 37765 Stab phlebectomy of varicose veins, one extremity, more than 20 incisions 37766 MODERATE (CONSCIOUS) SEDATION provided by same physician performing the Dx-Tx service Intraservice Start Time: __________ End Time:___________ Conscious Sedation AGE 5 or OLDER first 30 min each additional 15 minutes Conscious Sedation UNDER 5 first 30 min each additional 15 minutes 99144 99145 x __ 99143 99145 x __ CPT Only copyright 2012 American Medical Association. All Rights Reserved. Copyright 2012 Society of Interventional Radiology All rights reserved VASCULAR DIAGNOSTIC CHARGE SHEET PATIENT: DATE: REFERRING PHYSICIAN: PROCEDURE: INTERVENTIONAL RADIOLOGIST: *@ designates moderate conscioius sedation included SELECTIVE VASCULAR CATHETERIZATIONS ARTERIAL VASCULAR FAMILY 1st (X) Order Selective cath place thoracic or Brachiocephalic Subclavian initial 3rd oder of more selctive Each Add'l 2nd 2nd 3rd or 3rd Order* (X) Order* (X) Order* (X) # of Vessels For same session RADIOLOGICAL S&I ARTERIOGRAPHY (X) 36215 36215 36215 36216 36216 36216 36217 36217 36217 336218 x __ 36218 x __ 36218 x __ Thoracic Aortogram Abdominal Aortogram Abd Aortogram w Run-Offs @ 36215 36245 36216 36246 36217 36247 36218x_ 36248 x __ Brachial, Retrograde Spinal, Selective, Each Vessel SMA @ 36245 36246 36247 36248 x __ Extremity, Unilateral IMA Renal, Unilateral Renal, Bilateral IIiac, Ipsilateral Common IIiac, Contralateral Common Femoral, Ipsilateral Common Femoral, Contralateral Other Abdominal Aorta Vascular Family Right Heart or Pulmonary Trunk Only Left Pulmonary (includes pressures) Right Pulmonary (includes pressures) @ @ @ @ @ @ @ @ 36245 36251 36252 36245 36245 36245 N/A 36245 36013 N/A N/A 36246 36253 36254 36246 36246 36246 36246 36246 N/A 36014 36014 36248 x __ Extremity, Bilateral Visceral w-w/o Flush, Each Vessel Adrenal, Unilateral Adrenal, Bilateral Pelvic, Each Vessel, Sel. Pulmonary, Unilateral Pulmonary, Bilateral Pulmonary, Nonselective Internal Mammary Each Add Vessel After Basic AV Dialysis Shunt Existing Access VENOGRAPHY (X) Extremity, Unilateral Extremity, Bilateral IVC SVC Renal, Unilateral Renal, Bilateral Adrenal, Unilateral Adrenal, Bilateral Sinus or Jugular Superior Sagittal Sinus Epidural Orbital Hepatic w Hemodynamic Eval Hepatic wedge pressures no venogram Additional 2nd/3rd VENOUS VASCULAR FAMILY (X) 1st Order* 36011 36011 36011 NA 36011 36500 x __ 36011 x __ 36481 36247 36253 36254 36247 36247 36247 36247 36247 N/A 36015 36015 1st, 2nd 1st & 2nd & (X) Order* (X) 3rd Order* (X) 36012 36012 36012 36012 36012 36012 36012 36012 36012 36012 36248 x __ 36248 x __ 36248 x __ 36248 x __ 36248 x __ N/A 36015 x __ 36015 x __ Each Add'l 2nd or 3rd* 36012 36012 36012 36012 36012 Right Renal Left Renal Jugular Left Adrenal Right Adrenal Selective Organ Blood Sampling (x #) Other Venous Vascular Family 36012 x __ 36012 x __ 36012 x __ Portal Venogram *CATHETERIZATION CODING CONVENTIONS 1) Code multiple catheterizations in the same vascular family to the highest order 2) Use the "Each Additional" code for each additional second or third order vessel within the same vascular family 3) Code catheterizations of different vascular families separately Cervicocerebral Arch Angiography Bilateral bilat diff territory Append -59 Non-selective cath thoracic/ aorta 36221 @ bilat/unil w/ imaging -59 -50 Selective unil carotid/innominate w/ipsil @ extracranial imaging -59 36222 -50 Selective unil carotid/innominate w/ipsil intracranial/extracranial imaging DX and TX RS&I Append -59 75605 75625 75630 -59 -59 -59 75658 75705 x __ -59 -59 75710 -59 75716 75726 x __ 75731 75733 75736 x __ 75741 75743 75746 75756 75774 x __ 75791 CODE 75820 75822 75825 75827 75831 75833 75840 75842 75860 75870 75872 75880 75889 -59 -59 -59 -59 -59 -59 -59 -59 -59 -59 -59 -59 -59 -59 -59 -59 -59 -59 -59 -59 -59 -59 -59 -59 -59 75889-52 -59 Hepatic w/o Hemodynamic Eval 75891 -59 Venous Sampling (E.G. renins) 75893 x __ -59 @ Selective unil internal carotid w/ipsil @ intra/exracranial imaging Selective unil subclavian/innom w/ipsil @ vertebral imaging Selective unil vertebral w/ipsil vertebral @ imaging Selective unil external carotid w/ipsil ext @ carotid imaging Selective internal carotid or vertebral, @ ea branch w/ imaging NON-SELECTIVE VASCULAR CATHETERIZATIONS 36223 -50 -59 LYMPHANGIOGRAPHY 36224 -50 -59 Extremity only, unilateral 75801 -59 36225 -50 -59 Extremity only, bilateral 75803 -59 36226 -50 -59 Pelvic/abdominal, unilateral 75805 -59 36227 -50 -59 Pelvic/abdominal, bilateral 75807 -59 36228 -59 -50 (X) @ CODE 36200 36140 36620 36147 Aorta, Catheter (Femoral, Brachial, Axillary) Extremity Artery, Needle/Intracatheter, Unilateral Radial artery catheter for pressures/monitoring Arteriovenous Dialysis Shunt including RS&I @ AV dialysis shunt additional access for therapeutic intervention @ 36148 Extremity Vein, Needle/Intracath, Uni (Including contrast Inj) 36005 Aorta, Translumbar 36160 Carotid/Vertebral, direct puncture 36100 Retrograde Brachial 36120 Superior or Inferior Vena Cava, Catheter 36010 MODERATE (CONSCIOUS) SEDATION provided by same physician performing the Dx-Tx service (X) Intraservice Start Time: __________ End Time:___________ Conscious Sedation AGE 5 or OLDER first 30 min 99144 each additional 15 minutes 99145 x __ Conscious Sedation UNDER 5 first 30 min 99143 each additional 15 minutes 99145 x __ MISCELLANEOUS CODE * (MAX 2X PER SIDE) (X) OTHER (X) Splenoportogram UNLISTED IMAGING CODES CODE CODE 75810 -59 (X) Unlisted, Fluoroscopic procedure Unlisted, CT procedure Unlisted, MR procedure Unlisted, US procedure Attach Report Attach Report Attach Report Attach Report PRESENTING PROBLEM(S)/DIAGNOSIS Dx 1: __________________ ICD-9: _____ Dx 2 :_________________ ICD-9: _____ (X) Closure Device G0269 CT, limited or localized follow-up US Guidance for Vascular Access (Required documentation on file) 76937 76380 CPT Only copyright 2012 American Medical Association, All Rights Reserve Copyright 2012, Society of Interventional Radiology. All Rights Reserved. PATIENT: DATE: PROCEDURE: REFERRING PHYSICIAN: INTERVENTIONAL RADIOLOGIST: NONVASCULAR INTERVENTIONAL CHARGE SHEET MCS-Moderate Conscious Sedation Indicator @: Do NOT additionally report Moderate Conscious Sedation codes in conjunction with these services. Valuation for codes with @ in the MCS indicator column includes the physician work for conscious sedation. S&I (X) MCS Procedure S&I DRAINAGE PROCEDURES GASTROINTESTINAL TRACT (X)MCS Procedure Perc. Transhepatic Cholangiogram 47500 74320 20501 76080 Fistula or Sinus Tract Study Perc. Biliary Drainage (External) Thoracentesis needle or cath, w/out imaging 47510 75980 32554 N/A Thoracentesis needle or cath, with imaging 47511 75982 32555 N/A Perc. Biliary Drainage (Int. and Ext.) Abscess Drainage, Pleural (Empyema) w/out imaging 47505 74305 32556 N/A Injection, Cholangiography, Existing Cath., T-tube Abscess Drainage, Pleural (Empyema) w/ imaging Change of Biliary Drainage Catheter @ 47525 75984 32557 N/A Revise/Reinsert Transhepatic tube Abscess Drainage, Lung 47530 75984 @ 32201 75989 Perc. Dil Biliary Stricture w/o Int. Stent Insertion, Indwelling Tunneled Pleural Cath 47555 74363 @ 32550 75989 Perc. Dil Biliary Stricture with Int. Stent 32552 N/A 47556 74363 Removal of Indwelling Tunneled Cath w/ cuff 47552 N/A fibrinolysis via chest tube/catheter, agent initial 32561 N/A Cholangioscopy, perc., w/ or w/o brushing or wash 32562 N/A 47553 N/A fibrinolysis viacatheter, agent subs Cholangioscopy, perc., with biopsy 47554 N/A @ 44901 75989 Cholangioscopy, perc., with calculus/calculi remova Abscess Drainage, Appendiceal 47630 74327 @ 47011 75989 Biliary Stone Removal via T-Tube Abscess/Cyst Drainage, Liver 74300 @ 48511 75989 Pancreatic Pseudocyst Drainage Intraoperative Cholangiogram 74301 @ 49021 75989 Intraoperative Cholangiogram Additional Abscess Drainage, Peritoneal @ 49041 75989 Naso/oro gastric tube placement 43752 Abscess Drainage, Subdiaphragmatic @ @ 49061 75989 G-tube placement under fluoro guidance 49440 Abscess Drainage, Retroperitoneal @ 49082 Paracentesis, Abdominal wo imaging guidance J-tube placement under fluoro guidance 49441 49083 Paracentesis, Abdominal w imaging guidance duodenostomy tube placement under fluoro guidan @ 49442 49423 75984 cecostomy/colonic tube placement under fluoro gu @ 49442 Change of Abscess Drain (inc. injection) @ 49440 + 49446 49424 76080 G-J tube placement under fluoro guidance Abscessogram (Tube Check) 49446 Conversion of previously placed G-tube to G-J @ @ 58823 75989 Pelvic, transvaginal or transrectal @ 50021 75989 G-tube replacement under fluoro guidance 49450 Abscess Drainage, Renal or Perirenal BIOPSIES J-tube replacement under fluoro guidance 49451 20206 by modality* 49451 duodenostomy tube replacement under fluoro guid Muscle, Percutaneous G-J tube replacement under fluoro guidance 20220 by modality* 49452 Bone, Superficial, Percutaneous Mechanical removal obstructive material G-, J-, G20225 by modality* Bone Deep, Percutaneous 49460 J, C tube under fluoro guidance 32400 by modality* Pleura, Percutaneous Contrast Injection for G-, J-, G-J, C tube @ 32405 by modality* Lung, Percutaneous 49465 Perc. Cholecystostomy complete Lymph Nodes, Sup., Percut 47490 N/A 38505 by modality* Pneumoperitoneum 49400 74190 Liver, Percutaneous, Separate @ 47000 by modality* ** Liver, Percutaneous, w/ Other Procedure @ 47001 by modality* ERCP 43260 @ ** ERCP w/ biopsy 43261 Pancreas, Percutaneous 48102 by modality* @ 43262 ** Abdomen/Retrop., Percutaneous 49180 by modality* ERCP for Spincterotomy/Papillotomy @ Renal, Percutaneous ERCP calculus/calculi Removal @ 43264 ** @ 50200 by modality* Prostate ERCP calculus/calculi Destruction @ 43265 ** 55700 by modality* Thyroid, Percutaneous ERCP Insert Nasobiliary/Nasopancreatic tube @ 43267 ** 60100 by modality* ERCP Biliary/Pancreatic Stent @ 43268 ** 62269 by modality* Spinal Cord ERCP Stent Removal or Change @ 43269 ** 10021 N/A Fine needle aspiration, w/out imaging guidance 43271 ** 10022 by modality* ERCP Balloon Dilation @ Fine needle aspiration, w/ imaging guidance Esophagus Dilation @ 43453 74360 *Imaging Guidance Modality Used (circle one) Esophageal Plastic Tube or Stent @ 43219 ** US 76942 CT 77012 MR 77021 Fluoro 77002 **ERCP RS&I S&I 74328 (X) MCS Procedure OTHER **ERCP Biliary Ducts RS&I 74329 Tracheal/Bronchial Stent 31631-62 N/A **ERCP Pancreatic Ducts RS&I S&I 74330 TRANSCATHETER BIOPSY (X) MCS Procedure **ERCP Pancreatic and Biliary Ducts RS&I URINARY PROCEDURES (X) Procedure S&I 37200/36011 75970 Transjugular liver biopsy Perc Antegrade Pyelogram (thru needle) 50390 74425 ABLATION PROCEDURES (X) Procedure S&I Nephrostomy 50392 74475 Percutaneous RFA, Liver Tumor(s) @ 47382 by modality* Nephrostogram (thru existing catheter) 50394 74425 Percutaneous Cryoablation, Liver Tumor(s) 47399 by modality* Nephrostomy Tube Change 50398 75984 Percutaneous RFA, Renal Tumor(s) @ 50592 by modality* 74485 Dilation of Nephrostomy Tract/Pyelostomy 50395 Percutaneous Cryoablation, Renal Tumor(s) @ 50593 by modality* Ureterography Through Existing Catheter 50684 74425 32998 by modality* Percutaneous RFA Lung Tumor(s) Percutaneous RFA Bone Tumor(s) Ureteral Dilation 53899 74485 @ 20982 URETERAL STENT includes CT guidance 19499 by modality* Percutaneous RFA Breast Tumor(s) Internally Dwelling Percutaneous injection of ablative agent (i.e. Placement through renal pelvis 50393 74480 47399 by modality* alcohol or acetic acid), liver @ - exchange, perc. approach includes imaging 50382 @ 47380** 76362 - removal, perc. approach includes imaging 50384 Open RFA, Liver Tumor(s) using U/S guidance Transuretheral approach @ xchange, transurtheral approach includes imaging 50385 Open Cryo, Renal Tumor(s) 50250** @ - removal, transurtheral approach includes imaging 50386 includes US guidance Externally Dwellling (externally accesible transnephric ureteral stent/ **Use modifier -62 when service is provided by co-surgeons. *Imaging Guidance/Monitoring Modality Used for Ablation (circle one) -exchange, includes imaging @ 50387 -removal, includes imaging 50389 US 76940 CT 77013 MR 77022 -removal NOT requiring imaging*** 99XXX*** *** Considered inherent to E&M, report appropriate level of E&M provid 50688 Change ureterostomy tube/ureteral stent via ileal Whitaker Test 50396 Nephrostolithotomy <2cm Nephrostolithotomy >2cm Aspiration, Renal Cyst by Needle Contrast study of renal cyst Ileoconduit Injection Aspirate bladder (Diagnostic) by trocar/catheter Suprapubic Catheter (incl. Bladder aspiration) Cystogram Urethrocystogram, Voiding Cystography/VCU w/Chain Urethrocystogram, Retrograde Change Cystostomy Tube, Simple Change Cystostomy Tube, Complex **use 76001 in lieu of 76000 if > 1 hr fluoro *Imaging Guidance Modality Used (circle one) 50080 50081 50390 50390 50690 51101 51102 51600 51600 51605 51610 51705 51710 US 76942 CT 77012 Fluoro 77002 75984 74425/74475 /74480 76000** 76000** by modality* 74470 74425 by modality* by modality* 74430 74455 74430 74450 75984 75984 Procedure S&I FALLOPIAN DILATATION (X) Hysterosalpingogram 58340 74740 Hysterosonography, w/ or w/o color flow 58340 76831 Fallopian Dilatation 58345 74742 MODERATE (CONSCIOUS) SEDATION provided by same physician performing the Dx-Tx service Intraservice Start Time: __________ End Time:___________ Conscious Sedation AGE 5 or OLDER first 30 min 99144 each additional 15 minutes 99145 x ___ Conscious Sedation UNDER 5 first 30 min 99143 each additional 15 minutes 99145 x ___ PRESENTING PROBLEM(S)/DIAGNOSIS Dx 1: __________________ ICD-9: _____ Dx 2 :_________________ ICD-9: _____ MR 77021 CPT Only copyright 2012 American Medical Association. All Rights Reserved. Copyright 2013 Society of Interventional Radiology. All rights reserved TRANSLUMINAL ANGIOPLASTY/STENT/ ATHERECTOMY CHARGE SHEET PATIENT: DATE: REFERRING PHYSICIAN PROCEDURE: INTERVENTIONAL RADIOLOGIST MCS-Moderate Conscious Sedation Indicator @: Do NOT additionally report Moderate Conscious Sedation codes in conjunction with these services. Valuation for codes with @ in the MCS indicator column includes the physician work for conscious sedation. (x) MSC Procedure S&I code Code N/A (x) MCS PERCUTANEOUS TRANSLUMINAL ANGIOPLASTY/STENT/ATHERECTOMY* PTA, Iliac Artery, unilateral Stent, Iliac, with PTA when performed, unilateral @ 37220 @ 37221 N/A PTA, each add'l illiac vessel, unilateral Stent, Iliac, with PTA when performed, each add'l vessel, unilateral @ 37222 N/A @ 37223 N/A PTA, Femoral/Popliteal Arteries, unilateral Atherectomy, Femoral/Popliteal, with PTA when performed, unilatera Stent, Femoral/Popliteal, with PTA when performed, unilateral unilateral @ 37224 N/A @ 37225 N/A @ 37226 N/A @ 37227 N/A PTA, Tibial/Peroneal Artery, unilateral Atherectomy, Tibial/Peroneal, with PTA when performed, unilateral Stent, Tibial /Peroneal,y,with PTA when performed, unilateral , p , unilateral @ 37228 N/A @ 37229 N/A @ 37230 N/A @ 37231 N/A PTA, Tibial/Peroneal, each add'l vessel, unilateral Atherectomy, Tibial/Peroneal, with PTA when performed, each add'l vessel, , unilateral , p , , unilateral Stent and Atherectomy, Tibial/Peroneal, with PTA when performed, each add'l vessel, unilateral @ 37232 N/A @ 37233 N/A @ 37234 N/A @ 37235 N/A Renal artery Visceral artery (except renal) each vessel Abdominal aorta Brachiocephalic trunk and branches, each vessel Illicac artery, each vessel 0234T 0235T 0236T 0237T 0238T N/A N/A N/A N/A N/A Endovascular repair of iliac artery bifurcation using a bifurcated external and internal iliac artery 0254T 0255T Intravascular Stent, perc; initial vessel 0075T N/A Intravascular Stent, perc; each addl. vessel 0076T N/A Category III codes to describe transluminal atherectomy above Inguinal ligaments percutaneously and/or though open surgical exposure (includes RS&I) Intravascular Stents Extracranial Vertebral/Intrathoracic Carotid includes all ipsilateral selective cath, target vessel angiography PRESENTING PROBLEM(S)/DIAGNOSIS Dx 1: __________________ Dx 2 :_________________ CPT Only copyright 2012 American Medical Association. All Rights Reserved. ICD-9: _____ ICD-9: _____ Copyright 2012 Society of Interventional Radiology Procedure S&I Code Code PATIENT: DOB IDENTIFICATION NUMBER: DATE: AAA-TA-IA ENDOVASCULAR REPAIR CHARGE SHEET Procedure Code EXPOSURE FOR ENDOPROSTHESIS Femoral Cutdown 34812 Bilat Fem-fem graft 34813 Iliac Retroperitoneal Exposure 34820 Bilat CATHETERIZATION: NON-SELECTIVE *Report cath codes in addition to exposure Aorta, Catheter (Femoral, Brachial, Axillary) 36200 Bilat Iliac, nonselective 36140 Bilat CATHETERIZATION: SELECTIVE --Circle code(s)-1st 1st & 2nd Arterial Vascular Family**** Order Order IIiac, Ipsilateral 36245 36246 Common IIiac, Contralateral 36245 36246 Common Femoral, Ipsilateral 36245 36246 Common Femoral, Contralateral N/A 36246 Common Iliac or Femoral, Axillary or Brachial Approach 36245 36246 Other Abdominal Aorta Vascular Family 36245 36246 Code AAA ENDOPROTHESIS DEPLOYMENT 75952 AAA endo repr w/ aorto-aortic tube device 34800 AAA endo repr w/ modular bifurcated device (1-limb) 34802 75952 AAA endo repr w/ modular bifurcated device (2-limb) 34803 75952 AAA endo repr w/ unibody bifurcated device 34804 75952 AAA endo repair, aorto-uni-iliac/aorto-unifemoral device 34805 75952 AAA endo repair w/ visceral branches using prosthesis 0080T 0078T AAA EXTENSIONS/CUFFS DEPLOYMENT*** Imaging code 75953 billed per vesse 75953 initial vessel 34825 34826 75953 each additional vessel visceral extension prosthesis, ea visceral branch 0079T 0081T Code TA ENDOPROTHESIS DEPLOYMENT 75956 TA endo repair w/ coverage of subclavian origin 33880 TA endo repair w/out coverage of subclavian origin 33881 75957 Open subclavian to carotid artery transposition performed in 33889 conjunction with TA endo repair, neck incision Graft with other than vein, transcervical retropharyngeal carotid33891 carotid performed in conjuncition with TAA Procedure Code 34812-50 Physician #1 34820-50 Physician #2 36200-50 36140-50 1st, 2nd & or 3rd Orde 3rd Order # of Vessels Modifier(s) 36247 X36248 36247 X36248 36247 X36248 36247 X36248 36247 X36248 36247 X36248 Modifier(s) - 62 / -26 - 62 / -26 - 62 / -26 - 62 / -26 - 62 / -26 - 62 / -26 / -26 / -26 / -26 Modifier(s) - 62 / -26 - 62 / -26 TA EXTENSIONS/CUFFS DEPLOYMENT Proximal - initial 33883 75958 / 75958 / 33886 75959 REFERRING PHYSICIAN: -26 -26 / MODIFIER DEFINITIONS -22 Extended Services -26 Professional Component -50 Bilateral Procedure -51 Multiple Procedures -52 Reduced Service -53 Discountinued Service -58 Staged/Related Procedure -59 Distinct Procedural Service -62 Two Surgeons (Co-Surgeons) -76 Repeat Procedure, Same Physician -77 Repeat Procedure, Different Physician -78 Return for Related Procedure During Globa -79 Unrelated Procedure, -80 Assistant Surgeon -RT Right-side -LT Left-side -Q0 FDA Approved IDE#______________ -GA Advanced Beneficiary Notice (ABN) on File CODING GUIDELINES: * Stents placed inside the endoprosthesis treatment zone are not separately billable. ** Balloon dilatation of endoprosthesis is not separately billable. *** Multiple cuffs in the same vessel are not reportable beyond the first. ****Code caths of different vascular families separately per standard catheter coding conventions. **** Code Multiple Caths in the Same Vascular Family to the Highest Order. **** Use the "Each Additional" Code for Each Add/l 2nd or 3rd Order Vessel. -26 Delayed distal (not at time of initial repair) IA ENDOPROSTHESIS DEPLOYMENT 34900 75954 / -26 Endovasc iliac aneuryem repr OCCLUSION DEVICE (x) (x) Procedure Endovasc iliac occlusion device 34808 by by Code Modifier(s) OPEN CONVERSION BYPASS #1 #2 34830 Fempop with vein Open aortic tube prosth repr 35556 34831 Fempop non vein 35655 Open aortoiliac prosth repr Open aortofemor prosth repr 34832 THROMBOENDARTERECTOMY Code Code Modifier(s) Iliofemoral OTHER CONCOMMITANT SERVICES 35355 ANGIOPLASTY** @-Conscious Sedation included in codes marked @ Femoral, common 35371 Perc TA, Renal or Visceral Artery @ 35471 75966 / -26 Femoral, deep 35372 35450 75966 / -26 Open TA, Renal or Visceral Artery EMBOLECTOMY THROMBECTOMY Perc TA, Aorta (within treatment zone NOT reportable) @ 35472 75966 / -26 Fempop 34201 Open TA, Aorta (within treatment zone NOT reportable) 35452 75966 / -26 Popliteal-tibio-peroneal 34203 Perc TA, Brachiocephalic Arteries @ 35475 75962 / -26 ARTERIAL REPAIR Open TA, Brachiocephalic vessels 35458 75962 / -26 Lower extremity, direct 35226 35476 75978 / -26 Lower extremity, vein graft 35256 Perc TA, Venous @ 35460 75978 / -26 Lower extremity, non vein graft 35286 Open TA, Venous Perc TA, Each add'l visceral vessel @ 35471 x 75968 x / -26 Dx CODES Open TA, Each add'l visceral vessel 35450 x 75968 x / -26 Inclusion of a DX code is not meant to imply that payors have approved coverage. Please check with local payors for a list of approved DX codes for these services. Perc TA, Each add'l brachiocephalic vessel @ 35475 x 75964 x / -26 Open TA, Each add'l brachiocephalic vessel 35458 x 75964 x / -26 405.01 Malignant secondary renovascular hypertension INTRAVASCULAR ULTRASOUND 440.21 Artherosclerosis, extremity w/ claud. IVUS initial vessel 37250 75945 / -26 440.22 Artherosclerosis, extremity w/ rst pain 37251 75946 / -26 440.23 Artherosclerosis, extremity w/ ulcer Each additional vessel IVUS 440.24 Artherosclerosis, extremity w/ gangrene INTRAVASCULAR STENTS* Intravascular Stent, perc., initial 37205 75960 / -26 441.02 Dissection of abdominal aorta Intrasvascular Stent, perc., each add'l vessel 37206 75960 / -26 441.3 Abdominal aneurysm, ruptured Intravascular Stent, open, initial 37207 75960 / -26 441.4 Abdominal aneurysm without mention of rupture 37208 75960 / -26 442.2 Iliac artery aneurysm or pseudoaneurysm Intrasvascular Stent, open, each add'l vessel EMBOLIZATION *for embolization, follow up completion angio (75898) is separately reportable 442.82 Aneurysm or pseudoaneurysm of subclavian artery 75894 / -26 444.22 Lower extremity arterial embolism/thrombosis -26 585 Embolization (Non-Neuro) 37204 +75898 / Chronic renal failure 747.64 Iliac arteriovenous fistula OTHER *Required documentation on file US for Vascular Access* 76937 / -26 747.69 Aortic arteriovenous fistula CT, limited or localized follow-up 76380 / -26 901.1 Injury subclavian artery Placement of wireless sensor in sac during endo repair 34806 902.0 Aortic injury/trauma 902.53 Injury iliac artery Noninvasive physiological study of implanted wireless sensor 93982 Not typically billable at the Additional Services--(please describe) 902.54 Injury iliac vein 998.2 Iatrogenic rupture of vessel Category III codes effective Jan 1, 2011 Endovascular repair of iliac artery bifurcation using a bifurcated external and internal iliac artery 0254T 0255T Other (please specify) ____________________________ CPT Only copyright 2012 American Medical Association. All Rights Reserved. Copyright 2012 Society of Interventional Radiology. All Rights Reserved PATIENT: DATE: PROCEDURE: REFERRING PHYSICIAN: VENOUS ACCESS PROCEDURES CHARGE SHEET MCS-Moderate Conscious Sedation Indicator @: Do NOT additionally report Moderate Conscious Sedation codes in conjunction with these services. \Valuation for codes with @ in the MCS indicator column includes the physician work for conscious sedation. CENTRALLY INSERTED DEVICE Procedure (x)MCS Code Placement Centrally Inserted Non Tunneled child <5 Non Tunneled ( 5+ older) Tunneled child <5 no port, no pump Tunneled (5+ older) no port, no pump Tunneled port child <5 Tunneled port (5+ older) Tunneled pump 2 tunneled cath, 2 access sites (no port, no p Two tunneled cath, two access sites, w/ port Repair Non Tunneled no port, no pump, cent or per Tunneled no port, no pump, cent or periph Tunneled port, cent or periph Tunneled pump, cent or periph Two tunneled cath, two access sites (no port Two tunneled cath, two access sites, w/ port Partial Replacement (Cath Only) Port, cent or periph Pump, cent or periph Two tunneled cath, two access sites, w/ port @ @ @ @ @ @ @ @ 36555 36556 36557 36558 36560 36561 36563 36565 36566 36575 36575 @ 36576 @ 36576 36575 (X2)* @ 36576 (X2)* @ 36578 @ 36578 @ 36578 (X2)* Complete Replacement thru same venous access Non Tunneled 36580 Tunneled, no port no pump @ 36581 Tunneled port @ 36582 Tunneled pump @ 36583 Two tunneled cath, two access sites (no port @ 36581 (X2)* @ 36582 (X2)* Two tunneled cath, two access sites, w/ port Removal Non Tunneled no port, no pump Tunneled no port, no pump Tunneled port Tunneled pump Two tunneled cath, two access sites (no port Two tunneled cath, two access sites port @ @ @ 99XXX** 36589 36590 36590 36589 (X2) 36590 (X2) IMAGING for Central/Peripheral Device Procedures Fluoro guidance replacement, partial or complete 77001 Fluoro guidance removal 77001 US guidance for vascular access 76937 (required documentation on file) 76380 CT, limited or localized follow-up 76000 Fluoro only - no archived image SVC gram 75827 IVC gram 75825 Extremity venogram 75820 CPT Only copyright 2012 American Medical Association. All Rights Reserved. PERIPHERALLY INSERTED DEVICE Procedure (x)MCS Code Placement Peripherally Inserted 36568 Non Tunneled PICC child <5 @ 36569 Non Tunneled PICC ( 5+ older) 36570 PICC w/ port child <5 @ PICC w/ port (5+ older) 36571 @ Repair PICC PICC no port, no pump PICC w/ port @ 36575 36576 Partial Replacement (Cath Only) PICC w/ port @ 36578 Complete Replacement thru same vein access PICC 36584 @ PICC w/ port 36585 Removal Non Tunneled no port, no pump PICC w/ port @ 99XXX** 36590 CENTRAL/PERIPHERAL CVA DEVICE MAINTENANCE 76000 Reposition central venous catheter 36597 N/A Thrombolytic declotting of vascular access 36593 75901 CVA maintenance fibrin stripping (sep access) 36595 75902 CVA maintenance through lumen (brus 36596 Non-Selective Catheter Plcmnt- superio 36010 Selective Catheter Plcmnt- venous 1st 36011 Selective Catheter Plcmnt- venous 2nd 36012 Radiological Catheter Evaluation 36598 MODERATE (CONSCIOUS) SEDATION provided by same physician performing the Dx-Tx service (Do NOT report withcodes marked with @) Intraservice Start Time: __________ End Time:_________ Conscious Sedation AGE 5 or OLDER first 30 min 99144 each additional 15 minutes 99145 x ___ Conscious Sedation UNDER 5 first 30 min 99143 each additional 15 minutes 99145 x ___ * For multi-catheter devices use the appropriate repair, ** Removal of a non-tunneled device is considered inherent to E&M, report Copyright © 2012, Society of Interventional Radiology. All Rights Reserved. PATIENT: DATE: PROCEDURE: REFERRING PHYSICIAN: INTERVENTIONAL RADIOLOGIST NONVASCULAR INTERVENTIONAL CHARGE SHEET 2 BREAST Aspiration Breast Cyst each additional cyst Fine Needle Aspiration, w/ imaging guidance (X) CS Procedure 19000 19001 x ___ 10022 S&I by modality* by modality* by modality* Breast, Perc. Core Bx, Image Guided 19102 x ___ by modality* (per lesion) Breast, Perc Bx. vacuum assisted/rotating device (per 19103 x ___ by modality* lesion) Plcmnt each Localizing Clip 19295 x ___ by modality* (use w/ 19102/19103) see above ablation procedures RFA Breast Tumor(s) Breast Wire Localization 19290 77032 each additional localization 19291 x ___ 77032 x ___ Galactogram, Single Duct 19030 77053 Galactogram, Multiple Ducts 19030 x ___ 77054 x ___ Sentinel Node Injection 38792 by modality* *Guidance Modalities for Breast Procedures Stereotactic Guidance, each lesion 77031 x ___ Mammographic Guidance, each lesion 77032 x ___ Ultrasound Guidance for needle placement 76942 x ___ CT Guidance for needle placement 77012 x ___ Fluoroscopy Guidance needle placement 77002 x ___ MR Guidance for needle placement 77021 x ___ Specimen Services (X) Breast Specimen X-ray 76098 x ___ MISCELLANEOUS Closure Device CT, limited or localized follow-up US Guidance for Vascular Access (required documentation on file) PRESENTING PROBLEM(S)/DIAGNOSIS (X) G0269 76380 76937 Dx 1: __________________ ICD-9: _____ Dx 2 :_________________ ICD-9: _____ CPT Only copyright 2012 American Medical Association. All Rights ReservCopyright 2012 Society of Interventional Radiology. All Rights Reserved PATIENT: DATE: PROCEDURE: REFERRING PHYSICIAN: INTERVENTIONAL RADIOLOGIST: CT/MR Angiography - Cardiac MRI Charge Sheet MR ANGIOGRAPHY MRA Head w/out contrast MRA Head w/ contrast MRA Head w/out & w/ contrast MRA Neck w/out contrast MRA Neck w/ contrast MRA Neck w/out & w/ contrast MRA Chest w/ or w/out contrast MRA Spinal Canal w/ or w/out contrast MRA Pelvis w/out & w/ contrast MRA Upper Ext w/ or w/out contrast MRA Lower Ext w/ or w/out contrast MRA Abdomen w/ or w/out contrast (X) CODE 70544 70545 70546 70547 70548 70549 71555 72159 72198 73225 73725 74185 74185 MRA - Abdominal Aorta including iliacs w/ bilateral runoff 73725-RT MRA - Thoracic and Abdominal Aorta including iliacs w/ bilateral runoff 71555 74185 73725-RT 73725-LT 73725-LT MODERATE (CONSCIOUS) SEDATION* provided by same physician performing the Dx-Tx service (X) Intraservice Time Start Time: _____ AGE 5 or OLDER - first 30 min 99144 each additional 15 minutes 99145 x __ UNDER 5 YRS of AGE- first 30 min 99143 each additional 15 minutes 99145 x __ *Requires midpoint of time be reached in order to assign code. OTHER (X) CODE US guidance for vascular access CT ANGIOGRAPHY CTA Head w/out & w/ contrast CTA Neck w/out & w/ contrast CTA Chest w/out & w/ contrast CTA Pelvis w/out & w/ contrast CTA Upper Ext w/out & w/ contrast CTA Lower Ext w/out & w/ contrast CTA Abdomen/Pelvis w/contrast & wo/contrast when performed CTA Abdomen w/out & w/ contrast CTA Heart, coronary arteries & bypass grafts…w/contrast CTA Aorta w/ Run-offs w/out & w/ contrast 70496 70498 71275 72191 73206 73706 74174 74175 75574 75635 CARDIAC MRI (X) CODE Cardiac MRI for morphology and function without contrast 75557 with stress imaging 75559 Cardiac MRI for morphology and function with and without contrast 75561 with stress imaging 75563 Cardiac MRI for velocity flow mapping 75565 3-D RENDERING with interpretation and report under concurrent supervision use in addition to base imaging code NOT requiring postprocessing on an independent workstation (X) CODE 76376 76377 REQUIRING postprocessing on an independent workstation Do NOT report 3-D rendering, 76376/76377 in conjunction with codes for which postprocessing is considered inherent including: 31627, 70496, 70498, 70544-70549, 71275, 71555, 72159, 72191, 72198, 73206, 73225, 73706, 73725, 74174, 74175, 74185, 74261-74263, 75557, 75559, 75561, 75563, 75565, 75571-75574, 75635, 78012, 78013,78015-78999, 0159T. INJECTION (X) CODE C1-C2 puncture with injection for DX/Treatment 61055 Lumbar puncture, for myelogram (Valuation for code 62284 includes conscious sedationDo NOT additionally report 99141.) 76937 (required documentation on file) PRESENTING PROBLEM(S)/DIAGNOSIS Dx 1: __________________ Dx 2 :_________________ ICD-9: _____ ICD-9: _____ CPT Only copyright 2013 American Medical Association. All Rights Reserved. (X) CODE Copyright 2012, Society of Interventional Radiology. All Rights Reserved. 62284 INTERVENTIONAL RADIOLOGY ONCOLOGY CHARGE SHEET PATIENT: DATE: REFERRING PHYSICIAN: INTERVENTIONAL RADIOLOGIST: PROCEDURE: MCS-Moderate Conscious Sedation Indicator @: Do NOT additionally report Moderate Conscious Sedation codes in conjunction with these services. Valuation for codes with @ in the MCS indicator column includes the physician work for conscious sedation. BIOPSY Muscle, Percutaneous Bone, Superficial, Percutaneous Bone Deep, Percutaneous Pleura, Percutaneous Lung, Percutaneous Lymph Nodes, Sup., Percut Liver, Percutaneous, Separate Liver, Percutaneous, w/ Other Procedure Pancreas, Percutaneous Abdomen/Retrop., Percutaneous Renal, Percutaneous Prostate Thyroid, Percutaneous Spinal Cord Fine needle aspiration, w/out imaging Fine needle aspiration, w/ imaging gu (X) MCS Procedure 20206 20220 20225 32400 @ 32405 38505 @ 47000 @ 47001 48102 49180 @ 50200 55700 60100 62269 10021 10022 S&I by modality* by modality* by modality* by modality* by modality* by modality* by modality* by modality* by modality* by modality* by modality* by modality* by modality* by modality* N/A by modality* ABLATION PROCEDURES (X) Percutaneous RFA, Liver Tumor(s) Percutaneous Cryoablation, Liver Tumor(s) Percutaneous RFA, Renal Tumor(s) Percutaneous Cryoablation, Renal Tumor(s) Percutaneous RFA Lung Tumor(s) Percutaneous RFA Bone Tumor(s) includes CT guidance Percutaneous RFA Breast Tumor(s) Percutaneous injection of ablative agent (i.e. alcohol or acetic acid), liver US 76942 CT 77012 Fluoro 77002 Percutaneous placement of an interstitial device(s),fiducial marker or dosimeter for radiationoftherapy Percutaneous placement an @ MISCELLANEOUS Closure Device CT, limited or localized follow-up US Guidance Vascular Access (required documentation on file) 32553 Start Time: __________ Conscious Sedation AGE 5 or OLDER first 30 min each additional 15 minutes Conscious Sedation UNDER 5 first 30 min each additional 15 minutes 20982 19499 by modality* 47399 by modality* 47380** CT 77013 MR 77022 HEPATIC EMBOLIZATION @ Selective Catheterization 3rd order @ Additional Selective Catheterization 2nd/3rd+ @ Selective Catheterization 2nd order Selective Catheterization 1st order @ Dx Angio- visceral selective (if indicated) Dx Angio- selective add'l vessel beyond basic exam 36247 36248 x ___ 36246 36245 75726 75774 Embolization (Non-Neuro)* G0269 76380 37204 75894 REPORT ONLY ONCE PER SURGICA F/U Angio study for transcatheter therapy, embolization or infusion, other 75898 Add'l agent -prescribing, handling, and bolus administration 96420 chemotherapeutic agent radioactive agent 79445 Yttirum-90 @ 36247 Selective Catheterization 3rd order @ 36248 x ___ Additional Selective Catheterization 2nd/3rd+ 76937 Selective Catheterization 2nd order 55876 (X) MODERATE (CONSCIOUS) SEDATION - requires midpoint of time be reached in order provided by same physician performing the Dx-Tx service Intraservice @ S&I by modality* by modality* by modality* by modality* by modality* MR 77021 49411 interstitial device(s), such as fiducial marker or dosimeter for radiation Placement of interstitial device(s) for rad therapy guidance, prostate Procedure 47382 47399 50592 50593 32998 76940 Open Cryo, Renal Tumor(s) 50250** includes US guidance **Use modifier -62 when service is provided by co-surgeons. *Imaging Guidance/Monitoring Modality Used for Ablation (circle one) US 76940 Procedure S&I 37200/36011 75970 88172 (X) @ @ Open RFA, Liver Tumor(s) using U/S guidance *Imaging Guidance Modality Used (circle one) TRANSCATHETER BIOPSY Transjugular liver biopsy Cytohistologic study of specimen MCS @ End Time:___________ 99144 99145 x ___ 99143 99145 x ___ @ @ Selective Catheterization 1st order Dx Angio- visceral selective (if indicated) Dx Angio- selective add'l vessel beyond basic exam Embolization (Non-Neuro)* REPORT ONLY ONCE PER SURGICA F/U Angio study for transcatheter therapy, embolization or infusion, other than for thrombolysis 36246 36245 75726 75774 37204 75894 75898 Yttirum- Radiopharmaceutical therapy, by intra-arterial particulate 90 administration 79445 77263 Radiation therapy planning 77300 Radiation therapy dose plan 77790 Radiation handling PRESENTING PROBLEM(S)/DIAGNOSIS Dx 1: __________________ ICD-9: _____ Dx 2 :_________________ ICD-9: _____ CPT Only copyright 2012 American Medical Association. All Ri Copyright 2012 Society of Interventional Radiology PATIENT: DATE: PROCEDURE: REFERRING PHYSICIAN: INTERVENTIONAL RADIOLOGIST: MUSCULOSKELETAL CHARGE SHEET SPINE MYELOGRAM (X) Procedure S & I* 62284 see myelogram codes VERTEBROPLASTY unilat or bilat procedur (X) Thoracic one vertebral body w/bone bx Lumbar puncture, for myelogram (Valuation for code 62284 includes moderate (conscious) sedation - Do NOT separately report.) Cervical puncture, for myelogram 61055 Cervical Myelogram Thoracic Myelogram see myelogram codes 72240 72255 Lumbar Myelogram Spinal Canal Myelogram two or more regions Lumbar puncture, Tx for drainage Cervical puncture, w/o injection Puncture Shunt Tubing NEUROLYTIC INJECTION/INFUSION Subarachnoid Cervical or Thoracic Epidural Lumbar, Single Epidural NON-NEUROLYTIC INJECTION Dx/Tx, Cerv or Thoracic, Epi/Subara., Dx/Tx., Lumb or Sac., Epi/Subara., Cont. Infusion OR Intermittent Cerv or Thoracic, Epi/Subara. Cont. Infusion Lumb or Sac., Epi/Subara 62272 61050 61070 72265 72270 77003 77003 75809 62280 62281 62282 77003* 77003* 77003* 62310 62311 77003* 77003* 62318 62319 77003* 77003* Injection, epidural, of blood or clot patch 62273 77003* FACET JOINT INJECTION per joint level Inject Anesthesia, cervical or thoracic; single joint level 64490 N/A second level 64491 N/A third and any additional level(s) 64492 N/A Inject Anesthesia Lumbar/Sacral, single joint level 64493 N/A second level 64494 N/A third and any additional level(s) 64495 N/A FACET JOINT NERVE DESTRUCTION BY NEUROLYTIC INJECTION per nerve level Cervical/thoracic, single nerve level w/guidance 64633 cervical/thoracic, each additional nerve level 64634 Lumbar/sacral, single nerve level w/guidance 64635 lumbar/sacral, each additional nerve level Injection(s), diagnostic or therapeutic agent, paravertebral facet (zygapophyseal) joint (or nerves innervating that joint) with ultrasound guidance, cervical or thoracic; single level second [cervical/thoracic] level third and any additional [cervical/thoracic] level(s) @ Lumbar one vertebral body w/bone bx Procedure 22520 S&I by modality* by modality* @ Each add'l T or L vertebral body @ sacroplasty unilat injection sacroplasty bilat injection KYPHOPLASTY unilat or bilat injection(s) Thoracic one vertebral body Lumbar one vertebral body Each add'l T or L vertebral body *Guidance Modalities for Vertebroplasty 22521 22522 x ___ 0200T 0201T by modality* by modality* by modality* 22523 by modality* 22524 22525 x ___ by modality* by modality* 72291 x ___ Fluoroscopic guidance, per vert. body CT guidance, per vertebral body 72292 x ___ BIOPSIES Bone, Superficial, Percutaneous 20220 by modality* Bone Deep, Percutaneous 20225 by modality* Spinal Cord 62269 by modality* *Bx Imaging Guidance Modality Used (circle one) Fluoro 77002 76942 CT 77012 MR 77021 RADIOFREQUENCY ABLATION Percutaneous RFA Bone Tumor(s) (Valuation for code 20982 includes moderate (conscious) sedation - Do NOT OTHER Perc. Aspiration of Nucleus Pulposus Sinogram, Therapeutic Sinogram, Diagnostic Aspiration &/or Injection Small Joint Arthrocentesis Medium Joint Arthrocentesis Large Joint Sacroiliac Joint Injection w/o imaging ARTHROGRAPHY (X) 20982 (X) Procedure 62287 20500 20501 20600 20605 20610 20552 S&I Code 77003 76080 76080 77002 by modality by modality Procedure Radiographic S&I* CT S&I** Arthrogram, TMJ 21116 70332 70487 Arthrogram, Shoulder 23350 73040 Arthrogram, Elbow 24220 73085 Arthrogram, Wrist 25246 73115 27093 73525 27095 73525 MR S&I** 64636 0213T 0214T 0215T US only US only US only Injection(s), diagnostic or therapeutic agent, paravertebral fac 0216T US only second [lumbar or sacral] level (s) 0217T US only third and any additional [lumbar or sacral] level(s) 0218T US only ANESTHETIC/STEROID INJECTION TRANSFORMINAL EPIDURAL Cervical/thoracic, single level 64479 N/A cervical/thoracic, each additional level 64480 x ___ N/A Lumbar, single level 64483 N/A lumbar, each additional level 64484 x ___ N/A *Use 72275 instead of 77003 if formal epidurography is also done. Report 72275 or 77003 ONCE per each spinal region Codes 62275 OR 77003 are to be coded ONCE per each spinal REGION MODIFIERS 21 Prolonged E/M Services 22 Extended Services 24 Unrelated E/M During Global 25 Separate E/M Same Day of Procedure 26 Professional Component 50 Bilateral Procedure 51 Multiple Procedures 52 Reduced Service 53 Discountinued Service 57 Decision to Operate 58 Staged/Related Proc., During Global, Same MD 59 Distinct Procedural Service 62 Two Surgeons (Co-Surgeons) 76 Repeat Procedure, Same Physician 77 Repeat Procedure, Different Physician 78 Return for Related Procedure During Global 79 Unrelated Procedure, Same Physician During Global 99 Multiple Modifiers RT Right-side Arthrogram, Hip without anesthesia Arthrogram, Hip with anesthesia Arthrogram, Sacroiliac Joint (incl's imaging) Arthrogram, Knee 73201 or 73202 73201 or 73222 or 73223 73222 or 73202 73201 or 73202 73701 or 73702 73701 or 73702 73223 73222 or 73223 73722 or 73723 73722 or 73723 73701 or 73722 or 73702 73701 or 73723 73722 or 27096 27370 73580 Arthrogram, Ankle 27648 73615 73702 73723 **Flouroscopic Guided 77002 77002 Inj for CT/MR *Do not additionally report 77002 in conjunction with radiographic arthrography S&I codes. MODERATE (CONSCIOUS) SEDATION provided by same physician performing the Dx-Tx service Intraservice Time Start Time: _______ End Time: ________ (X) 99144 Conscious Sedation AGE 5 or OLDER first 3 each additional 15 minutes 99145 x __ Conscious Sedation UNDER 5 first 30 min 99143 each additional 15 minutes 99145 x __ (X) MISC 76380 CT, limited or localized follow-up US Guidance for Vascular Ac Access 76937 (require documentation in file) LT Left-side PRESENTING PROBLEM(S)/DIAGNOSIS Dx 1: __________________ ICD-9: _____ Dx 2 :_________________ ICD-9: _____ CPT Only copyright 2012 American Medical Association. All Rights Reserved. 1. Codes 64622, 64623, 64626, 64627 are to be coded per NERVE LEVEL. NOTE: Reporting of associated RS&I/imaging guidance code72275/ 76005 has been limited to once per each spinal REGION. Copyright 2012 Society of Interventional Radiology. All Rights Reserved OFFICE WITH ULTRASOUND CAPABILITY CHARGE SHEET PATIENT: DATE: EVALUATION & MANAGEMENT SERVICES CONSULTATION Office/Outpatient OFFICE VISIT (x) NEW PATIENT History and Examinatio Complexity of Medical n Decision Making NEW OR ESTABLISHED PATIENT (x) ESTABLISHED PATIENT Straightforward 99211 99241 Problem focused Straightforward 99202 Problem focused Straightforward 99212 99242 Expanded Straightforward Expanded Low 99243 99244 Low Moderate 99213 99214 Detailed Detailed Comprehensive Moderate Comprehen sive High 99215 99245 Comprehensive High ENDOVASCULAR VARICOSE VEIN THERAPY (x) VARICOSE VEIN IMAGING DX/FOLLOW-UP Non-invasive physiological study extremity veins, complete 93965 bilateral study (Doppler) 93970 Duplex scan of extremity veins - Bilat 93971 Duplex scan of extremity veins - unilat/limited study ENDOVASCULAR VARICOSE VEIN TREATMENT 36475 Radiofrequency EVAT- includes imaging- 1st vein 36476 Radiofrequency - 2nd & subs. vein(s) 36478 Laser EVAT- includes imaging- 1st vein 36479 Laser - 2nd & subs. vein(s) OTHER VARICOSE VEIN TREATMENT Injections of sclerosing solutions (single/multiple), spider 36468 veins; limb or trunk Injections of sclerosing solutions (single/multiple), spider 36469 veins; face 36470 Injection of sclerosing solution- single vein 36471 Injection of sclerosing solution- multiple veins, same leg Stab phlebectomy of varicose veins, one extremity, 10-20 37765 incisions Stab phlebectomy of varicose veins, one extremity, more 37766 than 20 incisions ULTRASOUND GUIDED BIOPSY (x) (x) Complexity of Medical Decision Making Problem focused 99205 (x) History and Examination 99201 99203 99204 (x) (x) BIOPSY 20206 Muscle, Percutaneous 32400 Pleura, Percutaneous 32405 @ Lung, Percutaneous 38505 Lymph Nodes, Sup., Percut 47000 @ Liver, Percutaneous, Separate 47001 @ Liver, Percutaneous, w/ Other Procedure 48102 Pancreas, Percutaneous 49180 Abdomen/Retrop., Percutaneous 55700 Prostate 60100 Thyroid, Percutaneous 10021 Fine needle aspiration, w/out imaging guidance 10022 Fine needle aspiration, w/ imaging guidance ULTRASOUND IMAGING GUIDANCE 76942 US guidance needle placement Referring Physician: ____________________ Presenting Problem(s)/Diagnosis Dx 1: ICD-9: _____________ Dx 2: Dx 3: ICD-9: ICD-9: _____________ _____________ Common Presenting Problem(s)/Diagnosis Varicose Vein TX 454.0 454.1 454.2 454.8 454.9 459.81 453.8 451.0 Varicose vein of lower extremities with ulcer Varicose vein of lower extremities with inflammation Varicose vein of lower extremities with ulcer and inflammation Varicose vein of lower extremities with other complications Varicose vein of lower extremities asymptomatic varicose vein Venous (peripheral) insufficiency, unspecified Other venous embolism and thrombosis of other specified veins Superficial thrombophlebitis Presenting Problem(s)/Diagnosis Not Listed Dx 1: Dx 2: ICD-9: ICD-9: Common Presenting Problem(s)/Diagnosis for BX 729.89 muscle (limb) lump 782.2 784.2 786.6 localized superficial swelling, mass, lump 789.3X 789.30 789.31 789.32 789.33 789.34 789.35 789.36 789.37 789.39 head and neck swelling, mass, lump chest/lung swelling, mass, or lump abdominal/pelvic swelling, mass, or lump (5th digit required) unspecified site right upper quadrant left upper quadrant right lower quadrant left lower quadrant periumbilic epigastric generalized other unspecified- multiple site Presenting Problem(s)/Diagnosis Not Listed INTERVENTIONAL RADIOLOGIST: _____________________________________________________________________ CPT Only copyright 2012 American Medical Association, All Rights Reserved. Dx 1: Dx 2: for ICD-9: ICD-9: Copyright 2012 Society of Interventional Radiology



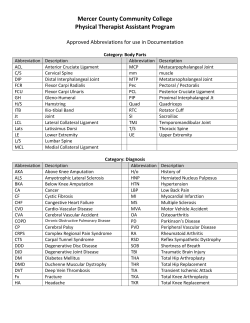







© Copyright 2026