
Cyprus National HES manual
Cyprus National HES manual This manual has been prepared by national experts from Cyprus. Maria Athanasiadou and Pavlos Palvou with their team from the Ministry of Health (http://www.moh.gov.cy/moh/moh.nsf/index_gr/index_gr?OpenDocument) wrote this manual. The EHES Pilot Project has received funding from the European Commission / DG Sanco. The views expressed here are those of the authors and they do not represent the Commission’s official position. More information about the EHES Pilot Project: http://www.ehes.info Contents Aims and purpose of the survey .................................................................................................................. 1 Organization and management of the national HES .................................................................................... 2 Timing of the survey ................................................................................................................................... 3 Target population and sample size .............................................................................................................. 4 Target population .......................................................................................................................................... 4 Sample size .................................................................................................................................................... 4 Sampling procedures .................................................................................................................................. 5 Sampling frame ............................................................................................................................................. 5 Sampling procedure ...................................................................................................................................... 5 Legal, ethical and data confidentiality issues .............................................................................................. 7 National legislation and regulations .............................................................................................................. 7 Process for ethical approval .......................................................................................................................... 7 Informed consent form ................................................................................................................................. 7 Obtaining informed consent ....................................................................................................................... 11 Recruitment, scheduling appointments and motivating participants ........................................................ 12 Quality assurance...................................................................................................................................... 14 Training programme .................................................................................................................................... 14 Training process for survey staff members ................................................................................................. 15 Pilot survey .................................................................................................................................................. 16 Quality control ............................................................................................................................................. 16 Data management .................................................................................................................................... 18 Selected measurements ............................................................................................................................ 20 Non-participant information ..................................................................................................................... 21 Selected examination site ......................................................................................................................... 22 Questionnaire and its administration and validation ................................................................................ 23 Questionnaire .............................................................................................................................................. 23 Administration mode................................................................................................................................... 27 Checking questionnaires and interviewing.................................................................................................. 28 Measurement procedures in the examinations ......................................................................................... 29 Blood pressure............................................................................................................................................. 29 Height .......................................................................................................................................................... 31 Weight ......................................................................................................................................................... 32 Waist circumference ................................................................................................................................... 33 Additional measurements ........................................................................................................................... 34 Feedback to the participants ....................................................................................................................... 34 Analytic laboratory, blood sample collection and storage of the samples ................................................. 36 Selection of the analytic laboratory ............................................................................................................ 36 Blood sample collection .............................................................................................................................. 36 Sample logistics ........................................................................................................................................... 40 Long term storage of the samples ............................................................................................................... 40 Fieldwork staff .......................................................................................................................................... 41 Coordination of the fieldwork ..................................................................................................................... 41 Safety issues ................................................................................................................................................ 44 Fieldwork logistics ....................................................................................................................................... 45 Dissemination, publicity and reporting ..................................................................................................... 46 Reporting ..................................................................................................................................................... 46 Budget and funding................................................................................................................................... 47 Risk assessment ........................................................................................................................................ 48 Evaluation ................................................................................................................................................. 50 4 Aims and purpose of the survey • Describe here the specific aims of the survey in your country. National Health Examination Surveys obtain information on health, diseases, health determinants etc. The aim of the health survey in Cyprus is to get a complete picture of the population health residing in the Government Controlled Areas of Cyprus, together with the information gathered from various sources such as registers and health surveys. • List the key public health issues to be described, evaluated and monitored using the data from this survey. A Health Examination Survey provides useful information concerning parameters that cannot be measured by any other means, such as anthropometric measurements, physiological measurements, clinical performance measurements and tests and the taking of blood samples. Through HES we can conclude helpful information of the lifestyle and the health behaviour of Cypriots. We can calculate the prevalence of some the most frequent health problems faced by Cypriots like diabetes, which is one of the main causes of death. 1 Organization and management of the national HES See EHES guidelines in the EHES Manual, Part A, Chapter 1. • Describe here who has commissioned the survey and who will conduct the survey. .................................. • Describe here the organization and management structure of the survey. .................................. 2 Timing of the survey See EHES guidelines in the EHES Manual, Part A, Chapter 6. • Specify here the year and months when the survey is expected to be carried out. The Health examination survey is expected to be carried out in the Autumn of 2014. • Estimate also the length of the fieldwork period. .................................. • If your country has previous national HESs, specify also their periods and describe how the previous survey(s) and other national surveys affect the timing of this survey. There weren’t any previous national HESs in my country. • Provide also information on which days of the week and which times of the day the survey is planned to be conducted. The time schedule of the survey will be planned on the basis of advice from the Statistical Service of Cyprus who have had previous experience in planning Health Interview Surveys. 3 Target population and sample size See EHES guidelines in the EHES Manual, Part A, Chapter 2. Target population • Provide here a detailed description of the target population. The geographical coverage of the national HES will be all districts in Cyprus in urban and rural areas that are controlled by the Government of the Republic of Cyprus. The core target population for national HES is the set of all persons permanently residing in Cyprus during the specific time period that the survey will be conducted, who are between the ages 25-64 years. • Define here also if institutionalized persons can be included to the target population and specify what kind of institutes can be included and which cannot. .......................................... • Specify also any other population groups that would be excluded from the survey. People who live permanently in institutions and illegal residents will be excluded from the survey Sample size • Provide here the sample size or the survey and how it was determined. The sample size of the national HES in Cyprus will include 4000 persons as this is specified by EHES. The specific sample size is required in order to provide statistical power. 4 Sampling procedures See EHES guidelines in the EHES Manual, Part A, Chapter 3. Sampling frame • Specify here the sampling frame(s) to be used in different stages of sampling. The most ideal and core sampling frame to be used is a population register, which could be used with other registers in order to collect more information about a person and the health status of a person (i.e. with cancer register, diabetes register, death register). Using multiple registers you could catch parts of the target population not covered by the main frame. • Provide further information about the sampling frames (when last updated, how is it updated, frequency of updating, what information relevant to the survey can be obtained from the sampling frame). The main sampling frame which is the population register is updated every 10 years when the census is conducted. Every year they do estimations for population considering the total number of deaths, births, immigrants and emigrants of the specific year. The population register was last updated in 2001. A new census is being conducted at the moment by the Statistical Service of Cyprus. Regarding the other registers (cancer register, diabetes register, and death register) we can find additional information about a person, like health status, whether is still alive a person or nor, if a person faced any other health problems. Sampling procedure • Describe here in detail how the sampling goes. How many stages are used, what are the Primary Sampling Units (PSU), what are the Secondary Sampling Units (SSU), what stratification is used and what is the sample size in each stage, etc. The sampling procedure can be summarised as follows: Selection of the sampling frame: a register with the most recent and best coverage of the individual persons in the target population. The most suitable sampling frame is the census population which is conducting at the moment and the results will be available to public in 2012. This will remove any problems of time lag. Define the Primary Sampling Units (PSUs): geographical areas where the HES will accomplish. Health Examination Survey must cover the whole territory of the government control areas of the Republic of Cyprus. Cyprus has six geographical strata (districts). All strata are sampled. Each stratum has PSUs i.e. Municipalities. Each Municipality is served mainly be one health centre. Stratification of the PSUs: stratification can be applied to rural, semi-urban and urban areas. Stratification of the eligible persons by gender and age. Definition of the sample sizes for PSUs and persons. Sampling of the PSUs. Sampling of the persons within sampled PSUs. Invitation to participate for the sampled persons. 5 The Secondary Sampling Units are the invitees in sampled site areas. Stratification could be by gender and age. 6 Legal, ethical and data confidentiality issues See EHES guidelines in the EHES Manual, Part A, Chapter 4. National legislation and regulations • Specify here the national legislation and regulations (ethical, medical research and data protection) which have an effect on conducting the HES. The processing of personal data (protection of individuals) Law 138 (I) 2001. [Office of the Commissioner for personal data protection] The bioethics Establishment and Function of the National Bioethics Committee Law [Cyprus National Bioethics Committee] • Describe also the implications of these laws and regulations on the survey. ................................... Process for ethical approval • Describe here which authority provides the ethical approval for the national survey. National Bioethics Committee of Cyprus. • Describe the process of obtaining the ethical approval and the documents needed for that. In order to obtain the ethical approval from the National Bioethics Committee we must use the appropriate forms according to the Operational Codes. For the application of the approval we need two forms: (a) Application for program/study review by an ethics committee. http://www.bioethics.gov.cy/Law/cnbc/cnbc.nsf/All/833D5C2DFC9627C6C22571E50 042A4CC/$file/EEBK02%20UK%20Application%20to%20Local%20EC.doc (b) Consent form http://www.bioethics.gov.cy/Law/cnbc/cnbc.nsf/All/D7BF2D1CAB174345C22571E50 042AC4E/$file/EEBK03%20UK%20Consent%20forms.doc In addition, the National Bioethics committee needs the entire proposal for the Health Examination Survey, as well as the budget. • Provide also an estimate of the time how long it takes to prepare the needed material and obtain the approval. Probably the estimated time needed for the entire process is a week. Informed consent form • If your country will start the HES soon, provide the informed consent form with all the supporting documents (information leaflet, etc.) approved by ethics committee. We won’t start the HES soon. • If you will start the HES later, provide a draft informed consent form with supporting documents. Take the national legislation is taken into account in drafting these. http://www.bioethics.gov.cy/Law/cnbc/cnbc.nsf/All/D7BF2D1CAB174345C22571E50042AC4E/$file/EEBK03%20UK%20Consent%20for ms.doc : link for the consent form 7 TEXT OF THE INFORMED CONSENT CONSENT FORM For Participation in a Research Study (These documents consist of ………….….. pages) You are requested to participate in a research program. Below (please see "Information for Patients and/or Volunteers") you will be provided with all the details and explanations, in simple language, regarding your participation in the study and what may happen to you, if you agree to participate. All the dangers concerning your health and rights, resulting from your participation in the study, will be explained to you in full detail. In addition, you will be warned for any possible discomfort that you may suffer. You will be informed on the information and/or material that you will be asked to provide voluntarily for the study and who will have access to this information and material. The duration, for which the investigators will have access to the information and/or material that you will provide, will be specified to you. The aims of the study, will be explained and what is hoped to be achieved as a result of your participation. Also, the benefits of the investigators and the financial sponsors, that may result from the study, will be outlined. You should not consent to participate in the study should you have any doubts concerning the study and your health and rights. You should not consent to participate if the study if you find it unclear. Should you decide to participate, you must provide information and details on whether you participated in any other research study within the last 12 months. Furthermore, if you decide to participate and you are a patient, your treatment will not be altered nor affected by your decision. You are free to withdraw from the study at any time you wish. If you are a patient, your decision to withdraw from the study, will have absolutely no repercussions on your present or future treatment. If you participate in the study, you are free to file substantiated complaints on any aspect or against any investigator of the study. These complaints may be filed/reported to the Ethics Committee that approved the study or directly to the Cyprus National Bioethics Committee. All the pages of these consent documents should bare your name and signature. Short title of the Program you are asked to participate Principal Investigator of the Program you are asked to participate 8 Last name: Signature: ……………………………………………….………. First name: ……………………………………….. ……………………………………………….………. Date: ……………………………………….. CONSENT FORM For Participation in a Research Study (These documents consist of ………….….. pages) Short title of the Program you are asked to participate Are you providing consent for yourself or someone else? If you are providing consent for someone else give details and his/her name. Question Yes or No Did you complete the consent documents your self? Within the last 12 months, did you participate in any other research study? Did you read and fully understand the information provided regarding the Study? Did you have a chance to ask questions you may have regarding the Study? Did you receive adequate answers and explanations to your questions? Do you understand that you can withdraw from the study at any time you wish? Do you understand that, should you withdraw from the study you do not have to provide any explanation for your decision to any one? Do you understand that, should you withdraw from the study there will be no consequences on possible therapeutic treatment you are receiving or may receive in the future? Do you agree to participate in the Study ? With whom did you meet and discuss the study? Last name: Signature: ……………………………………………….………. First name: ……………………………………….. ……………………………………………….………. Date: ……………………………………….. 9 CONSENT FORM For Participation in a Research Study (These documents consist of ………….….. pages) Short title of the Program you are asked to participate INFORMATION FOR PATIENTS AND/OR VOLUNTEERS …………………. Last name: ……………………………………………….………. Signature: ……………………………………………….………. 10 First name: ……………………………………….. Date: ……………………………………….. CONSENT FORM For Participation in a Research Study (These documents consist of ………….….. pages) Short title of the Program you are asked to participate INFORMATION FOR PATIENTS AND/OR VOLUNTEERS ………… Last name: ……………………………………………….………. Signature: ……………………………………………….………. First name: ……………………………………….. Date: ……………………………………….. Obtaining informed consent See EHES guideline in the EHES Manual, Part B, Chapter 3. • Describe here how the informed consent is obtained from the participants. In order the participant fully understands the scope of the study, the methods that will be used and how the data are going to be used; the potential participant must have a continuous active communication with the fieldwork staff. The process consists of providing information and answering to any questions that may arise. The consent should be obtained before carrying out any measurements. The participants should have the opportunity to ask questions at any time during the survey visit. They also need to be informed whom they can contact for further questions, even after the examination visit. 11 Recruitment, scheduling appointments and motivating participants See EHES guidelines in the EHES Manual, Part A, Chapter 1 for recruitment process and material and Part B, Chapter 2 for scheduling appointments and motivating participants. • Describe here the recruitment process: o How selected persons are contacted? The first contact attempt can be made for example by an invitation letter and information leaflet and then be followed by a phone call in order to schedule an appointment o What kind of recruitment material is used? Information leaflet Invitation letter Instructions to participant Information sheet o How many contact attempts are made before deciding that the person is a non-participant or not possible to contact. Regardless of how successful the first contact attempt is, at least 1-3 re-contacts should be made if feasible and not restricted by national legislation. • Describe here how the appointment scheduling for interviews and examinations are done. Appointments are schedule all weekdays. Mornings and afternoon sessions are arranged in order to include participants who work during the morning. Data collections on Saturdays are also foreseen so that individuals with very busy schedules can participate. Appointments are scheduled and arranged by the fieldwork team, but the personnel of the Health Centers (where the examination site is located) may also assist in the process. • Describe what methods are used to increase the overall interest of participation. Selection and training of personnel: Competent and motivated survey personnel play an important role during the recruitment process Factors affecting participation rate: Potential participants are also interested in personal benefits. For some participants a possibility to receive information on their own health status and risks may be an important reason for participation. Therefore, inclusion of additional examinations which offer more information to the participants on their health status should be considered Partnership for enhancing participation: Partnership and collaboration with local organizations, professionals and communities help to raise awareness of the importance of the survey, and to arrange easy access to the examinations. • Describe here what kinds of methods are used to motivate reluctant persons to get them to participate. Flexible scheduling. Organize the examination for the time most suitable for the potential participant. 12 If the full appointment seems to take too much time of the participant’s time; core measurements should be offered and a small questionnaire with the most essential questions. If a participant refuses to contribute to HES because of his/her health condition or time lack; the examination could occur at his/her place. 13 Quality assurance See EHES guidelines in the EHES Manual, Part A, Chapter 11 for components of the quality assurance and Part B, Chapter 7 for fieldwork specific quality control measures. Training programme See EHES guidelines in the EHES Manual, Part A, Chapter 15. • Describe here the plans for the national training programme. o Which personnel groups need training and what kind of? The national training programme is targeted to all staff involved in data collection and management, including those who are members of the fieldwork teams and those who are working at the central survey office and are involved in contacting participants (e.g. sending invitations, scheduling visits) or in data management. o Who are the trainers and what are their qualification, professions and how many there are? The national trainers should: − have participated in the EHES training seminars targeted to national trainers − be well informed both on the aims and purposes of the national survey as well as on EHES standards (e.g. members in the national survey project teams), and − have specific expertise in the subject area (e.g. survey ethics, blood pressure measurements). The supervisors and persons with experience from previous surveys can act as training assistants to train the other team members. They are needed in the practical training and in the role playing sessions. o How long the training will take, what issues are covered during the training and which are the training methods? Training is always organized before the fieldwork starts and includes sessions for a minimum of two days and maximum two weeks depending on the survey content and distribution of tasks between the fieldwork members. The training should include at least the following issues: − − − − − − − − − − − 14 Purpose and aims of the survey Ethical issues and confidentiality Random samples and the importance of high participation rates The importance of standardization and quality assurance Survey organization Communication skills, including similarities and differences in professional conduct during survey data collection and clinical practice in normal health care settings Working with the local health care professionals How the survey results will be reported and published The data management system and IT skills for data entry, handling and reporting Specific training to those who carry out measurements like blood pressure, anthropometric measurements, blood sample collection and other measurements. Specific procedures for each interview module or instrument − Specific measurements: rationale why they are measured, measurement techniques, including practical training and certification if needed − Giving feedback to participants concerning measurement results − Consulting survey physicians and local health care professionals when needed − Safety of the fieldwork team members (e.g. actions needed in case of needle stick injuries, violently acting and aggressive participants). Training process for survey staff members o When the training is planned to be organized in relation to the fieldwork? Training should be organized just before the fieldwork will be started, but some additional sessions may also be needed during the fieldwork. To allow substitution of other fieldwork team members when needed and rotating tasks (see chapter 9) it is recommended that each team member will be trained to handle several measurements, even if the measurements are carried out by teams where the staff members have different tasks. Retraining during fieldwork should be organized if the fieldwork lasts for more than two or three months to ensure that the standards are kept. Retraining is essential also if observer effects or non-adherence to survey standards are observed during audit visits or by other forms of quality control during the fieldwork. • If you have already organized the training or will do so in near future, provide training materials used. We haven’t organized the training yet. • If you don’t have your HES in near future, list to potential training materials which should be prepared. The Cyprus HES manual is the basis for all training materials. Additional materials can include PowerPoint presentations, videos and photos on interviewing and measurement techniques, web-based education tools. Lectures and open discussions can also be used, but they need to be short and concise and time to be allocated for staff members to practice the techniques. 15 Pilot survey • Describe here when the pilot survey will be conducted in relation to the full-size HES, where the pilot will be conducted and how. Pre-testing the data collection tools, piloting the HES procedures and evaluating the pilot is crucial to ensure a successful data collection. To increase the quality of the full-size survey, the pilot phase has to be conducted by the same personnel. Prior to the full-size HES, a pilot survey based on a sample of 200 individuals is necessary. The purpose of the pilot survey is to evaluate the entire survey process, obtain additional information for the planning of the actual survey and to assist fieldwork staff in familiarizing with potential practical problems. Quality control • Describe the internal quality control measures and external quality assessment planned for the survey. The internal quality control is a part of quality assurance. It includes monitoring of the correctness and completeness of the measurements and the data, and the actions taken to correct the observed shortcomings. Proper training and setting up the examination site are prerequisites for good quality of the fieldwork. These need to be complemented by quality control, which should address the entire process of data collection including the questionnaires, interviews, physical measurements and biological samples, as well as transfer of materials from one location to the other. In addition to the actual data collection, quality control during the fieldwork should also address issues related to contacting selected persons and participation rates. Regular checking of participation rates in different survey sites and by the fieldwork staff members who contact selected persons may reveal differences in practices. These should be evaluated to assure that best practices are used by all staff members and at each survey site. External audit (site visit) is carried out during the fieldwork of the EHES pilot. Other similar visits may also be arranged in the context of the Cyprus full HES by the EHES coordinator, another Organization that conducts a national HES, the funding Organization(s) or a third party specially recruited for this purpose. The audit includes checks during data collection (in the field), or administrative and financial checks. • Also measurement specific quality control procedures should be included. Calibration of measurement devices and data checking: For each measurement, the calibration of the measurement devices needs to be checked routinely. Depending on the device, this should be done before each measurement, daily or weekly Data and material transfer: When data and materials, such as paper questionnaires or blood samples, are transferred from one place to another, such as from the examination site to the national data centre or laboratory, it should be ensured that everything that was collected on the field will be received in the other end. Log books can be used to record all sufficient details of the shipments and to provide prompt inventory and acknowledgement by the receiving end. 16 Audit visits: The measurement procedures in the field should be monitored routinely by the fieldwork team coordinators. In addition, audit visits to the fieldwork site by a person outside the fieldwork team who knows the standard procedures well, are recommended. Re-training and duplicate measurements: If the fieldwork last several months or years, the fieldwork staff gets used to doing the measurements in routinely. This is good, but to avoid possible wrong routines, which may unintentionally develop over time, the retraining of the measurers and re-fresher sessions are needed. Also duplicate measurements by so called "gold standard" measurers or devices can be carried out as an additional quality control procedure, when feasible. 17 Data management See EHES guidelines in the EHES Manual, Part A, Chapter 12 for the data management structures and Part B, Chapter 6 for issues on data management during the fieldwork. • Describe here what kind of data management system is planned for the survey and how the data security is ensured. The data management system is necessary in all phases of the survey. Planning of the survey data management should be part of the general planning of the survey from the beginning. The things that need to be focused are: − detailed data flow in the survey − transfer, storage and security issues during each phase − rules for data correction (data correction procedures) To ensure data confidentiality and integrity it is necessary to use technical controls - e.g. passwords, network firewalls, access control lists, and/or data encryption - to monitor and control access to the computing systems and collected data. • Describe also the data back-up procedures. All data in electronic format should be backed up routinely for accidental breaks of the storage devices, failures in data transfer and unintentional deletion of data files. Especially during the fieldwork phase it will be important to back-up the data on local computers' hard-drives against accidental losses Technically several storage media can serve as back-ups. Here the primary options are: − Magnetic tapes − External hard disks − Optical disks (CD, DVD) − Another computer dedicated to back-up purpose Back-ups are needed not only for data in electronic format, but also for important paper documents, such as log books of the survey examinations. • Describe here how the subject identification is defined for the survey and how data confidentiality is ensured. To ensure data confidentiality and integrity it is necessary to use technical controls - e.g. passwords, network firewalls, access control lists, and/or data encryption - to monitor and control access to the computing systems and collected data. It is essential that the information connecting the survey data to the personal identification of the subject will be available only to persons who have authorized access to such data. Only authorized persons should have access to the data and all of them must understand the importance of the confidentiality of the data. After data collection, the information from which a person can be identified and the code which connects this information to the subject identification of the survey records, should be stored separately from the survey data, and maintained e.g. on encrypted hard drive. Normally only few people need access to the person identification information, whereas the rest of the survey data will need to be accessed by all who analyze the data. Specific precautions 18 should be defined for the handling and storage of paper forms in the examination site and elsewhere when these are used. • Describe here how the data are transferred from the field to the central office and to the database. Data transfer and import into the national HES database depends on whether the data are collected using computer-assistance or manually by using paper forms. Whenever data or samples are transferred from one place to another, it is important that the data transfer is logged properly. All data transfers should be traceable whether they are computerized or manual: The recipient of the data or samples should be able to check that he or she has received exactly the same records which were sent, and the person sending the data should make sure that everything was received. The transfer of the data into the central data storage, the national HES database, should be done regularly and via a secure data transfer medium. Good ways to transfer computerized data are through Internet via a secure connection and data encryption or by storing data on disks delivered via a secure mail. • Are the data entered directly to a computer or first recorded on paper forms and entered to a computer later? The best way is to record firstly on paper forms and then to a computer so data could be double checked in case of a shortcoming. • What kind of program is used for data entry? We can use an access file for the data entry. 19 Selected measurements See EHES guidelines in the EHES Manual, Part A, Chapter 5. • List here the selected measurements and questionnaire items for the survey and provide a rational behind their selection. The core physical measurements are: − Height − Weight − Waist circumference − Blood pressure Body Mass Index is calculated by height and weight. Body Mass Index (BMI) is a widely used indicator of obesity. It is defined as body weight divided by the square of height. The increase of obesity and overweight among the population is one of the most important public health issues in developed countries. Overweight and obesity represent a high risk factor for diseases of the circulatory system, diabetes and other chronic diseases .The evolution of the way of life and food consumption in the EU member States is characteristic by low physical activity and energetic food intake which increases the body mass index. Waist circumference is used as an indicator of abdominal obesity. Since increasing evidence has shown that waist circumference reflects the accumulation of visceral fat better than waist-to-hip ratio, the waist circumference is the preferred measure in population studies. Waist circumference is significantly associated with the risk incident of CVD events and type 2 diabetes. Measuring blood pressure gives a prevalence of actual and potential hypertension. Singleoccasion blood pressure measurement has been shown to be a strong indicator of coronary and cerebrovascular risk. However, the diagnosis of hypertension requires follow-up and observed high blood pressure on several occasions. 20 Non-participant information See EHES guidelines in the EHES Manual, Part A, Chapter 13. • Describe here what kind of information can and will be collected from the nonparticipants. Some key information, such as age, sex and possibly some aspects of social status can in most countries be obtained already from the sampling frame or other registries through record linkage. Other key information, and also these if not otherwise available, should be asked using a non-participant questionnaire. The questionnaire may include information like educational level, health status, diagnosed diseases, height and weight, smoking status. The questionnaire may be sent by mail or e-mail, or it can be filled in during a telephone interview or home visit. If the invited person is not available (by phone, e-mail or other means), proxy information may be used for completing the short non-participant questionnaire. • From which data sources non-participant information will be collected. Information for the non-participants may be collected through relevant registries i.e. Population registry. • If you use a specific questionnaire to collect information from the non-participants, attach the questionnaire to this manual. The template of the questionnaire will be in the same format as the example of the nonparticipant questionnaire formed by EHES team. 21 Selected examination site See EHES guidelines in the EHES Manual, Part A, Chapter 7. • Describe here the type(s) of examination site(s) planned for the survey and the rationale behind their selection. The potential examination site will be: − Participant's home: participants will have an easy access − Temporary examination site outside health care organizations, for example school premises: temporary examination sites could be located in a centralized place in order to service a larger number of potential participants. − Examination site within existing health care premises, such as a health centre or GP office (with the regular staff of with specific survey teams allowed to use the premises): Each municipality has a health care centre, which hundreds of people visit every day. The regular staff of the specific medical centre may conduct the Health Examination Survey to the potential participants of the particular municipality. − Mobile examination site, for instance a bus equipped for examination: a mobile examination site will be easy if it could be taken close to the participants. • If there were any national legislation or cultural norms affecting on decision, describe these as well. There is no national legislation or cultural norms affecting this decision. 22 Questionnaire and its administration and validation Questionnaire See EHES guidelines in the EHES Manual, Part B, Chapter 05,7. • Provide here selected questionnaire and rationale behind the questions. The core questionnaire will include the following questions derived from the HIS (Health Interview Survey, conducted by the Statistical Service of Cyprus): Q1. How many persons live in the household (including yourself)? (Modified from EHIS HH.1) |____| Q2. Sex (Modified from EHIS HH.2) |__| Male |__| Female Q3. Date of birth (dd.mm.yyyy)? (Modified from EHIS HH.2) |__||__| . |__||__| . |__||__||__||__| Q4. What is your legal marital status? (EHIS HH.5) |__| Single, that is, never married |__| Married (including registered partnership) |__| Widowed and not remarried |__| Divorced and not remarried (including legally separated and dissolved registered partnership) Q5. Are you living with someone as a couple? |__| Yes |__| No Q6. What is the highest education leaving certificate, diploma or education degree you have obtained ? (Please, include any vocational training) (EHIS HH.7) |__| No formal education or below (ISCED 1) |__| Primary education (ISCED 1) |__| Lower secondary education (ISCED 2) |__| Upper secondary education (ISCED 3) |__| Post-secondary but not-tertiary education (ISCED 4) |__| First stage of tertiary education (ISCED 5) |__| Second stage of tertiary education (ISCED 6) Q7. How many years have you spent at school or in full-time study? Q8. How would you define your current labour status? (EHIS HH.8) |__| Working for pay or profit (including unpaid work for a family business or holding, including an apprenticeship or paid traineeship, including currently not at work due to maternity, parental, sick leave or holidays) |__| Unemployed 23 |__| |__| |__| |__| |__| |__| Q9. Q10. Q11. Q12. Q13. Q14. 24 Pupil, student, further training, unpaid work experience In retirement or early retirement or has given up business Permanently disabled In compulsory military or community service Fulfilling domestic tasks Other, please specify:_____________________________________________ Have you ever worked for pay or profit (EHIS HH.9) |__| Yes |__| No Are (Were) you an employee, self-employed or working without payment as a family worker? (EHIS HH.10) |__| Employee |__| Self-employed |__| Family worker How is your health in general? (EHIS HS.1) |__| Very good |__| Good |__| Fair |__| Bad |__| Very bad |__| Don't know |__| Refusal Do you have any longstanding illness or health problem? (Longstanding means illnesses or health problems which have lasted, or are expected to last, for 6 months or more) (EHIS HS.2) |__| Yes |__| No |__| Don't know |__| Refusal For at least the past 6 months, to what extent have you been limited because of a health problem in activities people usually do? (EHIS HS.3) |__| Severely limited |__| Limited but not severely |__| Not limited at all |__| Don't know |__| Refusal Do you have or have you ever had any of the following diseases or conditions, diagnosed by a medical doctor? (Combined from HS.4 and HS.5) Myocardial infarction Yes |__| No |__| Coronary heart disease (angina pectoris) Yes |__| No |__| High blood pressure (hypertension) Yes |__| No |__| Q15. Q16. Q17. Q18. Q19. Q20. Q21. Elevated blood cholesterol Yes |__| No |__| Stroke (cerebral haemorrhage, cerebral thrombosis) Yes |__| No |__| Diabetes Yes |__| No |__| During the past two weeks, have you used any medicines (including dietary supplements such as herbal medicines or vitamins) that were prescribed or recommended for you by a doctor (for women, include also contraceptive pills or other hormones)? (EHIS MD.1) |__| Yes |__| No Were they medicines for ... ? (EHIS MD.2) High blood pressure Yes |__| No |__| Lowering the blood cholesterol level Yes |__| No |__| Diabetes Yes |__| No |__| When was your blood pressure last measured by a health professional? (modified from EHIS PA.5) |__| Within the past 12 moths |__| 1-2 years ago |__| 3-5 years ago |__| Never or more than 5 years ago |__| Don't know |__| Refusal Have you been told by a health professional in the past year (12 months) that you have elevated blood pressure or hypertension? (EHRM) |__| Yes |__| No |__| Uncertain When was your blood cholesterol last measured by a health professional? (modified from EHIS PA.7) |__| Within the past 12 moths |__| 1-2 years ago |__| 3-5 years ago |__| Never or more than 5 years ago |__| Don't know |__| Refusal Have you been told by a health professional in the past year (12 months) that you have raised (elevated) blood cholesterol? (EHRM) |__| Yes |__| No |__| Uncertain When was your blood sugar (glucose) last measured by a health professional? (Modified from EHIS PA.9) |__| Within the past 12 moths |__| 1-2 years ago 25 Q22. Q23. Q24. Q25. Q26. Q27. Q28. Q29. Q30. 26 |__| 3-5 years ago |__| Never or more than 5 years ago |__| Don't know |__| Refusal Have you been told by a health professional in the past year (12 months) that you have raised (elevated) blood sugar (glucose)? |__| Yes |__| No |__| Uncertain How tall are you without shoes? (BMI.1) |__||__| cm |__| Don't know |__| Refusal How much do you weight without clothes and shoes? (BMI.2) |__||__| kg |__| Don't know |__| Refusal Do you smoke at all nowadays? (EHIS SK.1) |__| Yes, daily |__| Yes, occasionally |__| Not at all On average, how many cigarettes do you smoke each day? (Modified from EHIS SK.3) Manufactured or hand-rolled cigarettes |__| Doesn't smoke cigarettes |__| Which of the products do you frequently smoke? (EHRM) Manufactured cigarettes Yes |__| No |__| Self-rolled cigarettes Yes |__| No |__| Pipe Yes |__| No |__| Cigars Yes |__| No |__| Have you ever smoked (cigarettes, cigars, pipes) daily, or almost daily, for at least one year? (EHIS SK.4) |__| Yes |__| No For how many years have you smoked daily? Count all separate periods of smoking daily. If you don't remember the exact number of years, please give an estimate. (EHIS SK.5) |__|__| years Which group represents your household's total net monthly income from all the sources (income from work, unemployment benefits, old-age or survivor's benefits, sickness or disability benefits, family/children related allowances, housing allowances, education-related allowance, other regular benefits) after deductions for income tax, national insurance, etc. (EHIS IN.04) Interviewer: Hand show card 12 (N.B. The values of the deciles' limits for each member state could be taken from a national survey on income, such as EU-SILC survey) |__| Below 1st decile |__| Between 1st decile and 2nddecile |__| Between 2nd decile and 3rd decile |__| Between 3rd decile and 4th decile |__| Between 4th decile and 5th decile |__| Between 5th decile and 6th decile |__| Between 6th decile and 7th decile |__| Between 7th decile and 8th decile |__| Between 8th decile and 9th decile |__| Above 9th decile |__| Refuse to answer • Were the selected questions and their translations validated? Yes • Were any of the selected questions part of some international or national set of questions? The selected questions are part of the HIS survey (Health Interview Survey), conducted by the Statistical Service of the Republic of Cyprus. • If the national HES is conducted soon, provide as an attachment a copy of the questionnaire. The Cyprus National HES will not accomplish soon. • If the national HES is not conducted soon, provide topic which most likely would be included to the questionnaire. The questionnaire will contain questions about the demographic and socio-economic characteristics of the respondents. Administration mode See EHES guidelines in the EHES Manual, Part A, Chapter 8. • Describe here which questionnaire administration modes are planned to be used in the survey and why they were chosen. The core EHES questions are collected through face-to-face interview. On the other hand, self-administration provides more privacy for the respondent and is particularly suitable for sensitive questions (e.g drug use, sexual behavior, income). • Describe also in which languages used questionnaire(s) are available/will be made available. Questionnaires will be available in Greek (native language) and in English because of the big number of foreigners in Cyprus. 27 • How long is the questionnaire and how long does it take to complete it? The questionnaire will contain the core EHES questions and/or some questions from Health Interview Survey (HIS). • Describe here the procedures used to pre-test the questionnaire. The questionnaire should start with the easy questions. When more difficult questions are placed at the end of the questionnaire and if respondent stop answering, at least some data for earlier questions have been collected. During the interview by asking the easy questions first may lead to trusting relationship between interviewer and respondent and then the respondent may be more willing to answer more difficult questions in the end. All the questions should be grouped by the topic. This makes answering easier. Also filtering questions should be used. The questionnaire must be short with not any complex and time-consuming questions. We must pre-test the exact time used to fill the questionnaire and keep in mind that some respondents may want an extension of time in order to accomplish it. If there are some questions of high sensitivity we could use an alternative administration mode e.g. Self-administration provides more privacy for the respondent and is particularly suitable for sensitive questions (e.g. drug use, sexual behaviour, income). Checking questionnaires and interviewing See EHES guidelines in the EHES Manual, Part B, Chapter 4. • Describe here how the completed questionnaires are checked on the field. Data from the interviews and self-administered questionnaires should be checked at regular intervals during the fieldwork to monitor item response and identify missing data for key items, as well as the frequency of response categories such as "don't know" or "refusal", which should be kept minimal. The data also needs to be checked for logical errors. In computer assisted data collection logical checks as well as check for the completeness of data (answers to all key questions) can be included in the data entry programme, allowing immediate corrections. • If some of the questionnaires are filled-in during the interview, describe also the instructions provided for the interviewers. Trying to fill in missing items: If the respondent has not filled in all questions because he/she has had problems in understanding the question or in choosing the answer, the fieldworker should give some further explanations. If the respondent has left the question open as he/she did not want to give an answer (e.g. finds the question too intimate), this should be recorded. Correcting items where the respondent has selected several options in questions where only one option is allowed: the fieldworker should ask the subject to choose the one that applies most/corresponds best his/her situation. Correcting if jump rules have not been followed: the fieldworker should help the respondent to clarify the situation. 28 Measurement procedures in the examinations See EHES guidelines in the EHES Manual, Part B, Chapter 5. Blood pressure • Describe equipment planned to be used for the blood pressure measurement. Mercury sphygmomanometer Required devices are: − Simple mercury sphygmomanometer − Stethoscope − 3-4 cuffs of different sizes: small, medium and large cuffs. Ideally also an extra large cuff (cuff for leg) should be available for obese persons. − Non-elastic measurement tape − Stopwatch, digital wrist watch or watch with second hand − Thermometer − Watch (for recording the time of the measurement) automated blood pressure monitoring device Required devices are: − An automated blood pressure monitoring device, which has passed the validation either based on the International protocol (O'Brien 2002), Association for the Advancement of Medical Instrumentation (AAMI) protocol (AAMI 1993) or the British Hypertension Society protocol (O'Brien 1993). From the British Hypertension Society web site (http://www.bhsoc.org/blood_pressure_list.stm) can be found a list of validated automated blood pressure measurement devices with reference to the published validation results. − 3-4 cuffs of different sizes: small, medium and large cuffs. Ideally also extra large cuff (cuff for leg) should be available for obese persons. − Non-elastic measurement tape − Thermometer − Watch (for recording the time of the measurement) • Describe the detailed measurement protocol. Measurement protocol Mercury sphygmomanometer 1. The participant is asked to sit still for 5 minutes before starting the measurement. At this time the measurement procedure should be explained for the participant and emphasized that he/she should not move during and between measurements as that will increase the blood pressure. 2. The participant is asked not to talk during the measurements. It should be explained that talking during or between measurement will increase the blood pressure. 3. The arm circumference is measured and correct cuff size selected. 4. The cuff is placed on the right arm so that its bottom edge is 2-3 cm above the antecubital fossa. The top edge of the cuff should not be restricted by 29 clothing. Make sure that the tubes from the cuff are not under the arm or otherwise tided up. 5. The radial pulse is palpated and the pulse rate is counted for 60 seconds, measured by a stop watch, a digital wrist watch or watch with a second hand. 6. Record 60-second pulse count and whether or not the pulse was regular. 7. Determine the peak inflation level: a. The mercury column has to be at 0 level b. The participant's radial pulse is again palpated. c. The cuff is inflated and the level of the top of the meniscus of the mercury column is noted at the point when the radial pulse disappears. The cuff is immediately deflated by completely opening the valve. d. The peak inflation level is determined by adding 30 mm to the pressure where the radial pulse disappeared. 8. The venous blood pool in the forearm is normalized by waiting at least 30 seconds or by raising the arm for 5-6 seconds. 9. The brachial pulse is located and the bell of the stethoscope is placed immediately below the cuff at the point of maximal pulsation If it is not possible to feel the brachial pulse, the bell of the stethoscope should be placed over the area of the upper arm immediately inside the bicep muscle tendon. The bell should not touch the cuff, rubber or clothing. 10. The cuff is rapidly inflated to the peak inflation level and then deflated at a rate of 2 mmHg per second. 11. The pressure should be reduced steadily at this rate until the occurrence of the systolic level at the first appearance of a clear repetitive tapping sound (Korotkoff Phase I) and the diastolic level at the disappearance of the repetitive sounds (Phase 5) have been observed. The cuff should then be rapidly deflated by fully opening the valve of the inflation bulb. Note: There may be a brief period (auscultatory gap) between systolic and diastolic pressure, when no Korotkoff sounds are heard. Thus the 2 mmHg/second deflation should be continued until the diastolic blood pressure is definitely established. If Korotkoff sounds persist until the cuff is completely deflated, a diastolic blood pressure of 0 is recorded. 12. The measurement is recorded to the nearest 2 mmHg. If the top of the meniscus falls halfway between two markings, the marking immediately above is chosen. The participant is not told his/her blood pressure at this point. 13. After waiting one minute to allow for the redistribution of blood in the forearm, a second measurement is made by repeating steps 9 to 11. The participant should not change position during this wait. 14. After another minute, the third measurement is made by repeating steps 10 to 12. Automated blood pressure measurement device The detailed measurement protocol for the automated blood pressure measurement devices is type specific and should be adjusted for the instructions provided by the manufacturer of the specific device. Here is the generic measurement protocol. 30 1. The participant is asked to sit still for 5 minutes before starting the measurement. At this time the measurement procedure should be explained for the participant and emphasized that he/she should not move during and between measurements as that will increase the blood pressure. 2. The participant is asked not to talk during the measurements. It should be explained that talking during or between measurement will increase the blood pressure. 3. The arm circumference is measured and correct cuff size selected. 4. Attach the air tube of the cuff to the air jack of the machine. The cuff must be airless. 5. Make sure that the batteries are inserted or that the adapter is on. 6. The radial pulse is palpated and the pulse rate is counted for 60 seconds, measured by a stop watch, a digital wrist watch or watch with a second hand. 7. Record 60-second pulse count and whether or not the pulse was regular. 8. Press the "ON" button: all the symbols on the display will light up in order to check the display. Note: in some models, pressing "ON" will start the measurement. In case you are using such a device, omit steps 9 and 10. 9. All the symbols then disappear and the air release symbol begins to flash. 10. The cuff is placed on the right arm so that its bottom edge is 2-3 cm above the antecubital fossa. The top edge of the cuff should not be restricted by clothing. Make sure that the tubes from the cuff are not under arm or otherwise tide up. 11. Push the "START" button: the device automatically determines the correct level of inflation pressure. 12. When the target inflation values are reached, the air is automatically released. The value in the display counts downwards. 13. As soon as the monitor detects the pulse, the symbol begins to flash. 14. When the monitor no longer detects the pulse while the cuff pressure is dropping, the systolic and diastolic pressure are displayed. 15. The measurement is recorded as shown in the display. In case the device gives an error code, this is recorded. The participant is not told his/her blood pressure at this point. 16. After one minute, the second measurement is made by repeating steps 1115. The participant should not change position during this wait. Note: some automated devices can be programmed to take 2 or 3 measurements automatically with one minute between the measurements. If device like that is used, measurer does not need to repeat steps 11-15 manually. 17. After another minute, the third measurement is made by repeating steps 1115. Height • Describe equipment planned to be used for the height measurement. Equipment Stadiometer (portable or fixed) (photos) Steps Carpenter's level 31 Standardized length rods (i.e. 100 cm and 200 cm) • Describe the detailed measurement protocol. Measurement protocol The measurement site should be private. The fixed stadiometer or height rule is attached vertically to the hard flat wall surface with the base at floor level. A carpenter's level is used to check the vertical placement of the rule. If the height rule does not have a fixed rod, it is recommended to mark with tape or marker the straight line for the rule down to the floor. When a portable, stand-alone stadiometer is used, the device is assembled based on the instructions of the device. A carpenter's level is used to check the vertical and horizontal placement of the stadiometer. If needed, that portable stadiometer is also fixed to the floor or wall, so that it will not move when participant steps on and off. The floor surface under the height rule must be hard. If no such floor is available, a hard wooden platform should be placed under the base of the height rule. Weight • Describe equipment planned to be used for the weight measurement. Equipment Balanced beam scale or an electronic scale (with EC type-examination certificate for medical use) or a validated bioimpedance (body composition) scale. The scale should comply with the directive 93/43/ECC June 14 1993 (http://eurlex.europa.eu/LexUriServ/LexUriServ.do?uri=CONSLEG:1993L0042:20071011:e n:PDF), updated in 2007/47*EC September 2007 (http://eurlex.europa.eu/LexUriServ/LexUriServ.do?uri=OJ:L:2007:247:0021:0055:en:PDF). There should be a sticker at the bottom of the scale with a code and symbol to specify that the device complies with these directives (CE 09 CE 0109) and marking of precision class III, specifying that the device has been calibrated according to the EC directive. Calibration weights (e.g. 10 kg up to 100kg) A carpenter's level (if the scale does not have build in level) • Describe the detailed measurement protocol. Measurement protocol The measurement site should be private. The scale should be placed on a hard floor surface. The floor should not be carpeted or otherwise covered with soft material. If there is not such floor available, a hard wooden platform should be placed under the scale. A carpenter's level (portable or in scale) should be used to verify that the scale is in horizontal position. Device specific instructions for setting up the scale should be followed. The participant is asked to undress to his/her underwear. If participant refuses or feels not comfortable to undress, he/she should be asked to take off the shoes, heavy garments such as jacket, pullover, belts, heavy jewellery and to empty pockets. The use of extra clothes during the measurement should be recorded. 32 Balanced beam scale − The participant is asked to stand in the centre of the platform with about a 10 cm gap between the heels. − The weight should be distributed evenly on both feet. − The participant is asked to stand still. − The weights are moved until the beam balances, meaning the arrows are aligned. − The weight is recorded to the resolution of the scale. Electronic scale − For turning the electronic scale on, follow the device specific instructions. − The participant is asked to stand in the center of the platform with about a 10 cm gap between the heels and arms hanging loosely at his/her sides. − The weight should be distributed evenly on both feet. − The participant is asked to stand still. − For the weight measurement, follow the device specific instruction. − The weight is recorded to the resolution of the scale. Bioimbedance device − Follow the device specific instruction − The weight is recorded to the resolution of the scale. Weight is written also to the participant's feedback form. The measurer can have a table (or this can be in the computerized data entry program) where she can read the BMI for the participant. The measurer can explain for example: "according to the BMI you are underweight, normal, little overweight or obese etc." When the measurement is performed at participant's home, the same protocol should be followed. The position of the device and participant should be carefully checked. Any deviations from the protocol should be recorded. Waist circumference • Describe equipment planned to be used for the waist circumference measurement. Equipment Non-elastic measurement tapes (200cm and 250cm) (photo) The full body length mirror, when ever feasible • Describe the detailed measurement protocol. 1. The participant is asked to reveal the waist, by loosening the belt, lowering the pants/skirt and lifting the shirt. Nothing should strain the waist. The measurement is done on bare skin. 2. The participant is asked to stand in the front of the measurer. The measurer is sitting on a chair. If the mirror is used, the measurer should have a clear view of it. 3. The participant is asked to stand feet fairly close together (10 cm) and weight equally distributed on both legs. 4. The hands are hanging loosely beside the body. 33 5. The measurer palpates the waist to find the right measurement place; midway between the lower rip margin and the iliac crest. The position is checked from both right and left side of the body. 6. The measurer checks that the measuring tape is in horizontal position for example by moving with the chair to see to the back of the participant, asking the participant to turn around or checking from the mirror. 7. The measuring tape is held firmly, ensuring the horizontal position. The tape should not be too tight or too loose. The measurer should be able to place one finger between the tape and the subject’s body. 8. The participant is asked to breathe normally; the reading is taken at the end of light exhale. 9. The waist circumference is recorded to the nearest millimeter. In some cultures undressing may not be acceptable. This should be respected. The waist circumference can then be measured over light underwear, like a thin shirt. Any exceptions on dressing should be recorded. When the measurement is performed at participant's home, the protocol should be followed as closely as possible. Any deviations from the protocol should be recorded. Self-reported waist circumference is not acceptable. The waist circumference is recorded on recording form (paper or computer). It should also be recorded to the feedback form which will be given to participant. In the feedback form also recommended maximum waist circumference for men and women can be given. Additional measurements • List the additional measurements which are planned to be included to the HES. Additional measurements are serum total cholesterol, HDL-cholesterol and plasma glucose, blood HbA1c, lung function test, ECG (electrocardiography), cognitive functioning test, bone density, urine and saliva samples. • For each additional measurement, describe equipment planned to be used for the measurement. .................................. • For each additional measurement, describe in detail the measurement protocol. .................................. Feedback to the participants • Describe the feedback that is planned to be provided to the participants on the results of the measurements before they leave the examination site. The feedback on anthropometric measurements and blood pressure can be provided to the participants right after the measurements. There are several ways to do this: a. Results are written to the form which is then given to the participant. The form does not include interpretation of the results. Results are explained verbally to the participant and they have an opportunity to ask questions. b. Results are written to the form which also has a short, basic interpretation of them (e.g. reference values). This form is then given to the participant and results are also explained to them verbally. 34 • Describe also the feedback they get later. Results of the blood analysis usually need more time and cannot be provided at the same visit when blood samples are collected. • Also describe how and by whom the feedback is provided. If the results are not provided directly to the participant, they are mailed to the general practitioner (GP) of the participant. It is expected that the GP explains the results to the participant. In cases where the laboratory analyses indicate acute need for medical attention, personal contacts (like a phone call by the survey physician) should be considered instead of only a mailed letter. When results are explained verbally to the participants, the field work staff should be provided with a few formulated model sentences which can be used. It has to be always emphasized that the survey measurements or samples, taken at one time cannot be used for diagnostic purposes. In case of any abnormal results, these have to be confirmed by repeated measurements, possibly with other additional tests and interpreted by a physician. The measurement results will also depend on adherence to instructions before the measurement (e.g. smoking or fasting), and these need to taken into account. During the examination visit important information on the participant's health status may be lacking, which is why all interpretations and comments should be made with caution. 35 Analytic laboratory, blood sample collection and storage of the samples See EHES guidelines in the EHES Manual, Part A, Chapter 10 and Part B, Chapter 5.5. Selection of the analytic laboratory • Describe here which laboratory will analyse the blood samples. State General Laboratory (SGL) of Cyprus Nicosia General Hospital Laboratory • Provide justification why this specific laboratory was chosen. The SGL is a dynamic centre of official control, monitoring, research and consultation utilized by the various state services, with national and European recognition. It is the Official Government Laboratory and the main laboratory for the surveillance and monitoring of foodstuffs, pharmaceuticals, cosmetics and for the examination of illegal drugs and other police exhibits from cases brought to court for justice. In cooperation with the competent authorities it is also the main centre for environmental monitoring and pollution control. Within the framework of its responsibilities the SGL carries out research to support the development and application of policies or to provide solutions to existing or emerging problems mainly in the areas of food safety, authenticity of products and environment and health. • Is the laboratory accredited and if yes, specify the accreditation authority. The SGL was the first laboratory in Cyprus that implemented strict quality criteria and since 2001 it is accredited by the Greek Accreditation Body ESYD according to the international standard ISO/IEC/EN 17025. http://www.moh.gov.cy/moh/sgl/sgl.nsf/DMLaccreditation_en/DMLaccreditation_en?OpenDocument Blood sample collection • Describe equipment planned to be used for blood sample collection. Blood samples Equipment − Blood sampling vacuum tubes − Needle for vacuum tubes − Needle holder/adapter into which the needle is pushed. It may contain an easy mechanism to release the needle. − Needle disposal container − Stasis − Disinfection solution − Swabs, gauze pads − Skin tape − Disposable gloves, latex and nitrite − Centrifuge tubes for use in case of incomplete clotting of sera and re-centrifugation. − Thin glass or plastic rods to manipulate an incomplete blood clot Other equipment 36 Blood collection tubes − Serum evacuated tubes containing gel (10/8 ml) or plain serum tubes (10/9 ml) − Fluoride-citrate plasma tube (5/2 or 5/3 ml) − EDTA plasma tube (5/3 or 5/4 ml) − EDTA plasma tubes (10/9 ml) Storage tubes − Cryotube 1.5 ml for -70 °C storage − Plastic tube 3 ml for -20 °C storage − Tube for pooling serum 15 ml Storage boxes − storage box for 1.5 ml cryotubes − storage box for 3 ml plastic tubes − storage box for small whole blood tubes − storage box for large whole blood tubes Pipets − Pipet with disposable tip for transferring 1.5 ml. Also spare pipet should be available. − Disposable tips − Disposable Pasteur- pipets • Describe the detailed blood sample collection protocol. Blood samples drawing protocol An 8-14-hour fasting is necessary before blood is sampled for the lipid and glucose analyses. Usually 10-12 hours are requested. Subjects should be sitting when the blood sample is taken after a 10-15 min resting period. For safety reasons disposable gloves should be worn during blood sampling and when processing serum, plasma and blood. 1. Place the first label from the left upper corner of the sheet of labels on the participant form. 2. Gently tap (e.g. against your hand) the fluoride citrate plasma tube (grey cap) if it contains granules. This way the granules from the stopper will drop to the bottom of the tube. 3. Gently twist the sample needle to break the seal. Release the cover from the end of the needle. Leave the needle protector case still on the needle. Connect the holder and sample needle. Leave the needle protector case on the needle. 4. Apply a tourniquet around the participant's upper arm. 5. Place the arm in a downward position and disinfect the puncture site. It is more comfortable for the participant if the arm rests on a pillow. 6. Remove the protector case from the needle. 7. Perform the venipuncture using the accepted technique. 8. Collect blood first into the 2 plain serum tubes (red cap). Press the tube at the bottom of the holder that the needle will puncture the stopper and start filling. Support the tube during filling. 9. Remove the tourniquet when the bloodstream runs. 37 10. When the bloodstream stops, take the tube out of the holder. Check that the tube is filled to the accurate volume. 11. Immediately after taking the plain serum tube out of the holder it should be adequately mixed 5 times by inverting the tube completely top-down. The tubes should be stored in a vertical position until sample handling. 12. Next, introduce and fill the fluoride-citrate plasma (grey cap) tube. 13. Immediately after taking the fluoride-citrate tube out of the holder it should be adequately mixed 15 times by inverting the tube completely top-down. The tubes should be stored in a vertical position until sample handling. 14. Next introduce and fill the 3 EDTA tubes (violet cap). 15. Immediately after taking the EDTA tube out of the holder it should be adequately mixed 5 times by inverting completely top-down. The tubes should be stored in a vertical position until sample handling. 16. Remove the needle from the vein. Immediately apply pressure on the puncture site with a gauze pad until bleeding stops. 17. Label the successfully filled blood sampling tubes according to the sampling chart, Figure x. 18. All material contaminated with blood should be considered hazardous. All needles and other sharps must be discarded into a needle dispose container and all other material into a biological waste container. NOTE! The last 2 EDTA tubes should not be centrifuged nor the caps removed!! The HbA1c analysis is made from whole blood and blood for DNA extraction may become contaminated • Describe the sample handling protocol. Centrifugation Sample processing includes centrifugation of blood tubes, labelling of storage tubes, pipetting aliquots into storage tubes and transferring storage tubes into freezers at the earliest convenience. Before centrifugation, make sure that the blood has clotted in the plain serum tube (red cap). Centrifugation of the clotted blood to obtain serum should be performed after making sure that the blood has clotted. The waiting for the blood to be clotted is at least 30 minutes at room temperature, 20-22 °C. Do not prolong the waiting for over 60 minutes. Immediately after the waiting period the plain serum tube (red cap), the fluoride-citrate (grey cap) and the 1st EDTA (violet cap) plasma tubes are centrifuged. The last two EDTA tubes designated for HbA1c and DNA extraction must not be centrifuged! Place the plain serum tube (red cap) and fluoride-citrate (grey tube) and the 1st EDTA (violet cap) plasma tubes in the centrifuge. Don't remove the caps from the tubes. Before centrifugation is started check that all tubes are resting on the bottom of the centrifuge rack. The tubes may not hang on the cap as this might result in separation of the tube and cap and spilled blood and the cap will then swirl in the centrifuge head and cause severe damage. Always check that the centrifuge rotor is in balance. 38 Centrifuge the tubes 2000 g for 10 minutes at room temperature. The relative centrifugal force (RCF) can be calculated by using an empirical equation or by using a nomogram for converting RCF to rpm. Sample handling after centrifugation Immediately after centrifugation, the caps must be removed except from the last two EDTA tubes. The samples are distributed as follows: Place the bar code labels properly. The code must be upright or else the reading with barcode reader is impossible If a bar code label is damaged, replace it with an extra label (empty ones on the sheet) and copy the bar code number and the sample type from the damaged label to the extra label with a water resistant pen. Pour the serum from the 2 serum collection tubes into the pooling tube, mix gently by swirling the contents. Pipette 2 x 1.5 ml serum from the pooling serum tube into the 3 ml plastic tube and 1.5 ml aliquots into the 1.5 ml storage cryotubes. Check that the serial number (person ID) is the same in the label of the serum collection tube and the labels of the cryotubes. Pipette 2 x 1.5 ml from the fluoride-citrate plasma tube into two 1.5 ml cryotubes. Pipette 2 x 1.5 ml from the EDTA tube into two 1.5 ml cryotubes. The last two EDTA tubes are not centrifuged nor are the caps removed. Close the cryotubes with caps and freeze the tubes at once. When frozen, the tubes must be kept in an upright position. Take special care in closing the tubes in order to prevent evaporation. Some tubes may be stored for decades before use. Put the frozen samples in their respective boxes in the freezer to wait for the shipment. Fill an entire box before taking a new one. All sheets of labels, both used and unused, should be returned to the NHES Lab at the end of the study. Note! It is important to pipet no more than 1.5 ml into cryotubes since serum ans plasma will expand during freezing. The right volume can be checked from the scale on the tube wall. Handling blood collection tubes with gel The temperature during centrifugation should be at least 20-22oC. At lower temperature the viscosity of the gel will result in incomplete separation of serum and cells. Because separation of serum in a gel tube is complete, the serum can be poured directly into a pooling tube in case of several blood tubes. The gel tube should be inspected after centrifugation for the following: − − − − − The surface of the gel should be horizontal The serum and cell layers should be separated clearly No red cells on top of the gel should be visible There should be no fibrin strands in the serum The serum should not be clotted, it should appear as a liquid. Blood in a gel tube can be centrifuged only once due to red cell contamination of the serum. If any red cell streaks are seen in the serum, transfer the serum into an empty centrifuge tube and re-centrifuge. 39 Sample logistics • Describe here how the samples are planned to be stored on the field. The frozen samples in their respective storage boxes should be sent packed in dry ice in one or a few batches at the end of the fieldwork period to the Laboratory. The sample boxes should be packed in leak proof secondary packaging. Enough absorbent material must be placed in the secondary packaging. Adhere to the national regulations concerning transport/mailing of biological samples. • Describe the transfer of the sampled from the examination site to the laboratory for analysis. The transportation should be organized well in advance (with a courier company). A courier company will provide the service including necessary paper work for "door-todoor" transport. Before sending the shipment, please inform the contact person of the receiving laboratory of date, courier and tracking details by email. The receiving laboratory should acknowledge the receiver shipments by e-mail or phone. The examination centre should keep a log book of all shipments, where also the acknowledgments are recorded. The courier will collect the samples at the Laboratory and will provide insulated rigid outer packaging and an adequate amount of dry ice. The company will also help you take care of the paperwork. Before the courier arrives, please make sure that the amount of storage boxes you will be shipping is known so that the amount of dry ice supplied is sufficient for the samples to stay frozen. To make sure that the samples are kept frozen and are in good condition when arriving at the Laboratory, one tube should be placed upside down in every box. Before sending the samples to either laboratory, please inform the contact persons by email about the sending details (date, mode of transport and the courier). This ensures that the transport will be documented for future checking. Long term storage of the samples • Describe here the plans for the long term storage of the collected samples. For long term storage reserved for additional measurements and future use, the samples must be frozen at -70°C. Note that tubes intended for core measurements should not be discarded after analyses, but should be returned to the original storage temperature. • What samples will be stored for future use, how and where? .................................. 40 Fieldwork staff See EHES guidelines in the EHES Manual, Part A, Chapter 9 and Part B, Chapter 1. • Describe here the possible legal requirements and cultural norms which may affect the selection of the survey staff in your country. .................................. • Describe the composition of the fieldwork team and the number of teams needed for the survey. The composition of the fieldwork teams depends on the type of the examination site (home visit/ local examination centre/ mobile examination unit), the measurements and possible additional national requirements. Each team should have a named Fieldwork team supervisor, and his/her deputy. Depending on the number of fieldwork teams and geographical coverage, several local/regional team supervisors may be needed. They need to work in close collaboration with the national fieldwork coordinator. The number of teams needed for the survey will determine in the future. Coordination of the fieldwork See EHES guidelines in the EHES Manual, Part B, Chapter 1. • Describe here the division of tasks between team members. Figure 1.1 provides an example of the structure of the fieldwork organization. In the first example, the laboratory (National HES laboratory) is part of the Central office (at the same organization), but it can also be a separate outsourced laboratory. In this example the different teams cover different survey sites. Close coordination of the work is needed between the laboratory, Central office and fieldwork team supervisors (Figure 1.2). This may be challenging when the laboratory is in a different organization. When examinations are carried out by home visits, the fieldwork supervisor is often responsible for the staff at several fieldwork locations. Figure 1.1 41 42 Figure 1.2 • Describe how the fieldwork is supervised. The fieldwork supervision has two levels: The national coordinator at the Central office has an overall responsibility of the fieldwork teams and fieldwork activities. She/he should visit regularly the survey sites. These visits are important especially in the beginning of the fieldwork to see how plans are working in practice. Regular visits from the central office are also important to support and motivate the fieldwork staff as well as for quality control The fieldwork team supervisors should meet or otherwise keep in contact regularly with the central office to share up to date information from the site. The fieldwork team supervisors bring also information from the central office back to their teams, e.g. feedback from quality control. They are responsible for monitoring that team members carry out their tasks well in daily basis. If there are problems, that cannot be solved within the team, the supervisors should contact the central office and unclear issues should be sorted out as soon as possible. It is important that the fieldwork team supervisors receive support from the central office and do not have to deal problems alone. The satisfaction of the staff is an important issue for the work quality. The national survey coordinator and fieldwork team supervisor have an important role in creating a positive work environment which effects to the staff satisfaction. A good leader should be visible, consult with staff and provide praise and recognition. • Describe how the communication within team and to the central coordinating office is organized. Sharing information between the central office and fieldwork teams as well as between and within fieldwork teams is important for the success of the work. Communication between the central office and fieldwork teams should include at least issues relating to 43 the progress of the work and to possible changes in the practices or personnel. Between the fieldwork teams, changing the experiences is an important part of the communication. Within the fieldwork teams communication is often focused on daily activities like division of tasks, absences, moving to new location, etc. Internal communication can be organized in many different ways; face-to-face meetings, video meetings, telephone meetings, extranet and internet sites, newsletters, SMS text messaging, instant messaging like Skype and Windows Messenger or even through social media. The key of communication is to make sure that every member of the team gets same information in timely manner. Formal meetings are useful for disseminating important information and for making decisions. Informal meetings such as coffee breaks give the possibility to share instant issues. It is important that the personnel are able to share their thoughts between colleagues and get advice if needed. The fieldwork staff may need extra support after unexpected incidents at the survey field. Group discussions are usually useful and increase the feeling of belonging and support among the fieldwork personnel. Safety issues See EHES guidelines in the EHES Manual, Part B, Chapter 1. • Describe here how the safety of the fieldwork team members is ensured. Safety issues during fieldwork should be considered both from the perspective of the participants and the staff. Safety issues related to each measurement should be covered in the national manual under the instructions for each measurement In general, the employer is responsible for providing − safe work place and equipment; − safe work process; − protective equipment where needed; and − information, instructions and training. The employee is responsible for − following the provided safety instructions; − using protective equipment and clothing in a correct manner; − informing either the fieldwork team supervisor or national fieldwork coordinator about hazards and injuries, and − taking part to the provided safety training. • What safety training and instructions are provided? Safety instructions should include guidelines for each step of the survey fieldwork; moving to new examination site, setting up the examination site, measurements themselves, and personal safety of the fieldwork team members. 44 Fieldwork logistics See EHES guidelines in the EHES Manual, Part B, Chapter 1. • Describe here how the fieldwork teams, equipment and materials are moved from an examination site to another. If equipment is moved by survey team members, special attention should be paid to the packing of the equipment properly both to moving containers and to the car, how to lift heavy equipment and how to protect equipment from theft. 45 Dissemination, publicity and reporting See EHES guidelines in the EHES Manual, Part A, Chapter 14. • Provide here the national dissemination and publicity plans for the survey. The outline of the dissemination plan could be: The role and main objectives of dissemination in the national HES. What we want to accomplish with dissemination. Key messages. What is our message to be disseminated in different points of time to different target groups. Key target groups for dissemination. Means of dissemination. Time scale and concrete actions. Organization of dissemination. Who will do, what, when and how. Reporting • Describe here the national reports. .................................. 46 Budget and funding See EHES guidelines in the EHES Manual, Part A, Chapter 16. • Calculate the survey budget for full-size HES (including also costs of the planning and preparation, and a fieldwork pilot, as well as the basic reporting). 4000 persons * 100 Euros = 400000 Euros • What are the potential sources of funding for the national HES? The annual budget of the Ministry of Health There is an anticipation of co-funding by the FP7 (Framework Programme 7). 47 Risk assessment See EHES guidelines in the EHES Manual, Part A, Chapter 1. • Prepare a risk assessment for the survey. .................................. • What are the expected risks, their implications and how these could be solved? Risk Problems caused Options for avoiding and controlling the risk Insufficient personnel resources for planning and preparation Shortcomings in planning and preparation leading to problems during fieldwork, in standardization and quality of data Shortage of fieldwork personnel Difficulties in keeping time schedules: problems caused for participants as well as in getting results Careful preparation of the survey organization, and seeking mandate from the ministries (health and research). Seeking specific funding for the planning and preparation, careful budgeting and diverse fund raising (see chapter 16), ensuring that the needed resources are available. Raising interest towards the survey in the ministries and professional organizations, careful piloting and planning for the time schedules, taking potential sick leaves into account when planning the size of fieldwork team(s). Acknowledging the aims and significance of the pilots. Careful preparation for the time schedule. Insufficient time between Not possible to correct pilot and actual fieldwork errors, specify manuals and training or adapt protocols, problems in standardization Problems in collaboration Difficulties in utilizing all between different expertise needed, and organizations and actors problems in keeping time schedules Low motivation among Low response, selective the population to participation, biased participate results Violation of personal Loss of confidence data protection rules 48 National or local political or ecological crisis situations Epidemics Loss of data Safety risks during Harm caused to staff Absences of fieldwork staff, difficulties in participation Well defined leadership, building local partnerships throughout the survey process, careful planning for the supervision of the fieldwork teams Media campaigns and careful planning of the recruitment process Careful planning and preparation for data management and proper training for all survey staff. Timely data transfer to central national and European data centres. Little possibilities to avoid: infectious disease control at fieldwork settings and offering seasonal flu vaccinations to fieldwork staff. A medical doctor must be available for fieldwork members or participants consultation or present at the fieldwork site. The protocol for needle stick injuries should be easily available to all staff members at all examination sites. Situations with aggressive and violent participants and other safety risks during fieldwork covered in manuals and training. Adequate supervision of field work staff throughout the fieldwork process. 49 Evaluation See EHES guidelines in the EHES Manual, Part A, Chapter 1. • Prepare a plan how the survey would be evaluated at the end. .................................. • List indicators for the evaluation of the survey? Survey stage Process indicators program operations Output indicators direct results or products of project activities Survey design Organized meetings and seminars First version of the survey proposal Planning and preparation Number and type of experts involved in the survey planning, personnel resources needed Training seminars organised for the fieldworkers: hours of training Number of invited persons Detailed survey plan with a budget Fieldwork during pilot(s) and the actual survey 50 Number of fieldwork staff members who participated in the national training (% of all fieldworkers) Number of days for the fieldwork Numbers of participants, those who were found to be ineligible, those who were not contacted and those who refused (by age and gender) Recorded length of examinations per participant – reported average length per participant (minutes/hours) Place of examinations: number of participants examined at the clinic setting/at home/ at an institution Outcomes indicators impacts or changes that can be attributed to the project activities National consensus on carrying out the HES and timing of the surveys. National HES plans approved by national authorities with at least preliminary decisions for funding for the HES. Ethical approval Participation rate (per age/gender) Cost of the survey data collection/participant








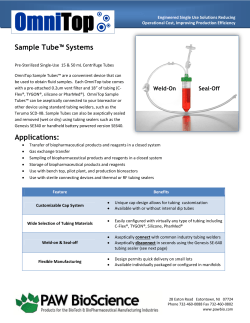
© Copyright 2026