
ADVANCED PRACTICE NURSE RECREDENTIALING MANUAL DEPARTMENT OF
DEPARTMENT OF SURGERY ADVANCED PRACTICE NURSE RECREDENTIALING MANUAL Created: 0 6 / 3 0 /2014 Last Updated: 08/06/2014 DEPAR RTMENT OF F SURGERY Y AD DVANCED PRACTICE P NURSE RE ECREDENT TIALING MANUAL TABLE E OF CO ONTENT TS Page 2 4 6 7 8 9 10 11 14 18 19 20 21 24 25 26 28 46 Defining D the Recredentiali R ing Process The T Department of Surgery y Recredentiaaling Checkliist for Advancced Practice N Nurses 2014 2 APN Ex xecutive Coun ncil 2014 2 Advanced Practice Nurse N Quarterly Meeting Scchedule APN A Credenttialing and Privileging Com mmittee Mem mbers Medical M Stafff Office Checcklist Application A for f Reappointm ment Information I Release R and Acknowledgem A ment Form Advanced A Praactice Nursing g Written Collaborative A Agreement Instructions I for f Delineation of APN Priivileges Rene wal Form Delineation D of o APN Privileeges Renewal Form APN A Peer Reeview Helpfull Guidelines APN A Peer Reeview Form an nd Peer Comm ments Additional A Do ocumentation n Required APN A Biograp phy Informatio on Form F H-2 – Claim C Experieence Verificattion Form (U UCMC) State S of Illino ois Health Carre Professionaal Recredentiialing Form Common C Lin nks used in thee Recredentiaaling Process Recredentialing Process The recredentialing process occurs prior to an Advanced Practice Nurse’s two year anniversary or sooner for new hires. The Medical Staff Office (MSO) Coordinators identify APNs to be recredentialed during the specified cycle based on the last digit of the APNs’ social security number. The Coordinators notify Surgery HR and the Surgery Business Administrator of those APNs scheduled for recredentialing and prepares the application packets for distribution. Departments are provided four to six weeks to complete the packet with their APNs. The Section Administrator will be notified via email that the MSO recredentialing application has been sent to the APN directly. The Business Administrator will send the APN an e-mail reminder. The Section Administrator (and/or their designate) will need to make him/herself available as a resource to the APN for completing the application prior to the due date. Once the APN has completed the application, he/she should return the packet to the Section Administrator. The Section Administrator should review the completed packets for any errors before returning them to the Department of Surgery Business Administrator in O-200. Once the completed packet is returned to the Business Administrator, he or she will complete a final review, and if complete, save the application on the MSO Directory and deliver the application to the MSO Credentialing Coordinator in room B-132 for review to verify the standards, qualifications and documentation for appointment and/or approval of privileges. The MSO Credentialing Coordinator notifies Surgery HR & the Surgery Business Administrator if there is any information that is found to be incomplete or inconsistent on an application. The Business Administrator will notify the Section Administrator of any deficiencies that need to be addressed. Recredentialing packets that have met all of the standards/qualifications are assigned to a member of the Advanced Practice Nurse Credential Committee for review and recommendation to the full committee. The Chief Nursing Officer must sign all APN packets and return them to the MSO Office. The MSO will schedule for the Practitioner Credentials and Privileges (PCP) Committee. After its evaluation of the application, the PCP committee will forward the packet to the Medical Executive Committee. The Medical Executive Committee will conduct any further investigation that it deems appropriate and either recommends to the Board that the applicant be approved or denied for medical staff privileges. The packet will then be sent to the Board of Trustees for final approval. Once the renewal is approved the APNs typically will not have to go through this process for another two years (note: this may vary depending upon SSN or special circumstances). Recredentialing Packet The recredentialing packet consists of different forms the APNs must complete. When a Section Administrator receives the packet it will include the following items: Medical Staff Office Recredentialing Checklist (p. 9) Application for Reappointment to the Medical Staff (p. 10) Information Release and Acknowledgement form (pp. 11-13) Advanced Practice Nursing Written Collaborative Agreement (pp. 14-17) Delineation of APN Privileges Renewal Form (p. 19) APN Peer Review Form and Peer Comments (pp. 21-23) 2 Form H-2- Claim Experience Verification Form (UCMC) (p. 26) Form K- Medicare Attestation Statement (p. 27) The following items are not included in the initial packet but need to be added to the recredentialing packet by the Section Administrator: IDPH State of Illinois form (pp. 28-51) o IDPH State of Illinois Form (recredentialing)- www.idph.state.il.us/about/credentialing.htm RN license (Copy) APN license (Copy) DEA license (Copy) (if applicable) State Controlled Substance license (Copy) (if applicable) ProCred Report o ProCred Report- http://corecompetency.uchicago.edu. The APN will have to use their CNet ID and password to login the system. CME Credit Report o To obtain a CME Credit Report, please email [email protected]. Please request a CME transcript for the past and current fiscal year for your APN. External category 1 CME credit (a minimum of 20 category 1 credits are needed within the last two years) Please note: It is always preferable that we submit a complete packet to the MSO. However, in certain cases, it may prove more expeditious to submit an incomplete packet so that the MSO can begin the review. The following is a list of items that are required in the packet before MSO will begin their review: Signed Application (p. 9) Release of Authorization (pp. 11-13) Form H-2 (p. 26) Illinois State Form (pp. 28-51) 3 D EPARTMENT OF SURGERY T The University off Chicago 55841 S. Marylandd Avenue R Room O200 (MC 5030) C Chicago, Illinois 660637 P Phone: 773-702-77508 F Fax: 773-702-22140 MEDIC CAL STAFF OFFICE O REC CREDENTIAL LING CHECK KLIST – ADV VANCED PRA ACTICE NUR RSE Name: Section: Top portio on completed by Business Administrrator Privilege Expiration E Da ate: n to Section Administrator: Date given Please mak ke sure all item ms below are in ncluded and com mpleted beforee returning the packet and siggned checklist tto Amanda O’Connell O in O--200. IMPORT TANT: When n making co orrections on o forms, DO O NOT use white out. Please draw wa line thro ough the errror and then n initial and d date the co orrection. D Do not remo ove ANY verification reports that are atttached to th his packet. _____ Complete C the e “Application n for Recred dentialing” fo orm. Form n need to be signed and dated by applicant and a collaborrating physic cian. _____ Sign and da ate the “Inforrmation Rele ease and Accknowledgem ment Form”. _____ Complete C the e “Advanced Practice Nu ursing Writte en Collabora ative Agreem ment”. This iss to be completed d by the applicant and co ollaborating physician. T The agreeme ent must be signed by the e advanced practice p nurs se and the ccollaborating g physician. _____ Complete C the e Claim Expe erience Veriffication Form m with signa ature and datte. If the advanced pra actice nurse has been in nsured for cla aims by anyy other insura ance carrierr other than the e University of Chicago Medical Cen nter Self-Insurance Prog gram, they w will need to comp plete an for each e carrier.. A form will be needed ffor any pend ding claims/ssuits and recent se ettlements made m during the current 2 2-year MSO O recredentia aling period. _____ Sign S and date e the “Form K – Medicarre Attestatio on Statementt (UCMC)”. _____ Complete C the e “Delineation of APN Prrivileges Ren newal Form””. _____ In nclude the “A APN Peer Re eview Form”” and “Peer Comments” signed by the APN bein ng re eviewed and d the APN re eviewer. edentialing F _____ Complete C the e State of Illin nois Health Care Professsional Recre Form & Business Data D Gatherin ng Form and d attach it with the packe et. Please no ote these forms are not in ncluded in th he packet an nd may be do ownloaded ffrom this site e: http://www.idph.state.il.us s/about/cred dentialing.htm m _____ Attach A the mo ost recently completed fiscal f year an nd current F FY ProCred C Core Report and make sure sections Competency C s are e compliant a according to guidelines. 4 The system can be accessed through the UCMC intranet site at http://corecompetency.uchicago.edu by using your CNETID and password. Contact your section administrator if you need assistance. Please note: ProCred must be complete per policy in accordance with the date the PA recredentialing packet is going to Committee, i.e. even though he/she may be compliant per policy at the time of submission, additional sections may need to be completed in advance. _____ Complete the “APN Directory Bio” and submit online or fax to Janet Karol at (773) 8341578. _____ Attach a copy of RN license. _____ Attach a copy of APN license. _____ Attach a copy of current Federal DEA registration (if applicable). _____ Attach a copy of current Controlled Substance License (if applicable). _____ Attach a copy of CME Credits. Date submitted to Business Administrator Section Administrator Date Date TO BE COMPLETED BY DOS ADMINISTRATION Reviewed for quality assurance and submitted to MSO Business Administrator Total number of delinquencies before privileges approved Privileges approved Date 5 Informationa al Resource that can be referenced d during and a post com mpletion on the recreden ntialing packket 2014 APN A EXE ECUTIVE E COUN NCIL Miche ele Rubin, AP PN, CNS APNC C Chair mich hele.rubin@ @uchospitals..edu Anne Pohlman, APN, A CNS APNC C Co-Chair apoh hlman@med dicine.bsd.uchicago.edu u Kelly Kramer, APN N, CNP kkra [email protected] go.edu Annem marie O’Con nnor, APN, CNP C anne emarie.ocon [email protected] Janet Friant, APN N, CNP jane et.karol@uch hospitals.edu u Ann Nelson, N APN, CNP anellson1@med dicine.bsd.ucchicago.edu Nancy y Spiewak, APN, A CRNA NSp [email protected] Judy Holleman, H APN,CNP A jholl [email protected] du Elizab beth Hood, RN, R MS, MBA A, APN/C CPNP ehoo [email protected] ago.edu Linda Bond, APN, CNP jbond d@medicine e.bsd.uchica ago.edu Josep ph Giannini, APN, CNP jose eph.giannini@ @uchospitalls.edu 6 To be reta ained by AP PN (Informatiional Purposses Only) 2014 Advanced d Practice Nurse Quarterly Q Meeting M Sc chedule All arre on a Thu ursday and d Mandatory Date Location e Time January 16,, 2014 Dora De D Lee 1 12:00pm-1::00pm April A 17, 2014 Dora De D Lee 1 12:00pm-1::00pm July 17, 201 14 Dora De D Lee 1 12:00pm-1::00pm October O 16,, 2014 Dora De D Lee 1 12:00pm-1::00pm 7 To be retained by APN (Informational Purposes Only) APN Credentialing and Privileging Committee Members Michele Rubin, APN, CNS Chair Ann Nelson Annemarie O’Connor Janice Colwell Mary Ann Francisco Nada Williamson Pamela Beauduy Stefanie Blummer [email protected] [email protected] [email protected] [email protected] [email protected] [email protected] [email protected] [email protected] 8 MSO Use Only: __________ Expiration Date The University of Chicago Medical Center Medical Staff Office __________ Received Date __________ Secondary Reviewer Advanced Practice Nurse Recredentialing Checklist Please provide the items below. The packet will be returned if not complete. Name: ______________________Department _______________ Section ________________ ______ Application for Reappointment ______ Information Release and Acknowledgement ______ Collaborative Agreement ______ Delineation of Privileges Form ______ Peer Review Form ______ State of Illinois Health Care Professional Recredentialing & Business Data Gathering Form ______ Claim Experience Verification Form (H) ______ Form K – Medicare Attestation ______ Copy of RN License ______ Copy of APN License ______ Copy of Controlled Substance License (if applicable) ______ Copy of DEA Registration (if applicable) ______ CME Credits ______ Copy of Certifications ______ Completed ProCred for previous year and current year-to-date showing progress 9 Iff the informatio on that is pre-populated on thiis form is incorrrect, APN muust update (i.e. - pager #,, home addresss, etc.). Please draw d a line thro ough any errorrs and then inittial and date. THE UNIVE ERSITY OF CHICAGO MEDICAL C CENTER 5841 Sou uth Maryland Avenue, Chiccago, Illinois 60637 APP PLICATION FOR F RECRED DENTIALING G N NAME: DEPARTME ENT: M MEDICAL CE ENTER ADDRESS: Phone # _________ Mail Code # ___________ ________ Fax:_________________________ Pager # _______________ ____ __________ E--Mail Addresss: RESS (if diffferent from ab bove Medical Center Addrress) OFFICE ADDR Street City Statee Z Zip Telephone City Statee Z Zip Telephone H HOME ADDR RESS: Street Answer Yes or No to o each question n H Have any claim ms alleging negligence n beeen filed agaiinst you sinc e your last aappointment?? Y Yes ____ No _____ _ IF F YES, Complete Form B (If “YES”, com mplete Form B) B H Have you been n insured forr claims of prrofessional negligence n byy any insuran nce carrier, oother than Th he U University of Chicago C Med dical Center Self-Insuran nce Program m, since your llast appointm ment? (If “YES”, return with w applicatiion Form H-22 for each caarrier) Y Yes ____ No _____ _ Answer Yes or No to each questio on IF YES S, Complete Fo orm H-2 __ __________ __________ ___________ __________ ___ A Applicant’s Sig gnature _____ __________ __________ _ Date APN must m sign and date A APPROVED: As Collaboraating Physiciaan, I have rev viewed this prractitioner's quualifications aand clinical aactivities ovver the past tw wo years, inclluding his/herr physical and d mental fitneess, and recom mmend him/hher for recredeentialing. ysician Signaturee Coollaborating Phy Prrinted Name Date Addvance Practice Nurse Credentiaal Committee Prrinted Name Date Chhief Nursing Offficer Prrinted Name Date M Medical Executivee Committee Prrinted Name Date Collab borating Phy ysician mus st sign and d date A Approved: Do ocument signatures for “Collaboratin “ ng Physician n” should be consistent w with the pri rimary physic cian worked with under primary p servvice line. Booard Member, Prrofessional Liability and Practice Subcommitteee Prrinted Name Date Iff this Advancced Practice Nurse N is not recommendeed for reapp pointment, pllease providee a written exxplanation. 10 0 The University of Chicago Medical Center (“UCMC”) INFORMATION RELEASE AND ACKNOWLEDGMENT I the undersigned practitioner hereby provide to UCMC the information requested in the Application materials in connection with my application for clinical privileges and for participation in the various University of Chicago Physician Group health plans, managed care plans and Medicare and Medicaid programs. I hereby authorize the Medical Staff Office (MSO) to provide the information to the medical staff and to any organizations for whom the Medical Staff Office performs delegated credentialing, for their use in evaluating my application to participate with them. I further authorize the MSO to provide the information to such other persons and entities as the Organizations may require and designate in connection with that evaluation. In consideration of the MSO making available such information to those Organizations, and of my application being considered and processed by such Organizations, I specifically submit the information subject to the following terms and conditions and agree to be legally bound by them. A. Representations I represent that all of the Information provided in or attached as part of this Application is accurate and complete. I understand and agree that my application will not be processed if it is not complete or if I fail to submit the information or documents requested. I also understand that any material misrepresentation, misstatement, or omission from my application, whether intentional or not, may be a basis for denial by the Organization of clinical privileges. In the event that approval of clinical privileges has been granted prior to the discovery of such misrepresentation, misstatement, or omission, such discovery may be deemed to constitute automatic relinquishment of my clinical privileges. B. Authorizations (1) I authorize the UCMC MSO, the Organizations, their medical staffs, and their authorized representatives to consult with any third party who may have information bearing on my professional qualifications, credentials, clinical competence, character, ability to perform safely and competently, ethics, behavior, or any other matter reasonably having a bearing on my qualifications for initial and continued appointment to the medical staff, or to otherwise participate with the Organizations. This authorization includes the right to inspect or obtain any and all communications, reports, records, statements, documents, recommendations or disclosures of said third parties that may be relevant to such questions. In addition, I specifically authorize these third parties to release such information to the MSO, the Organizations, their medical staffs, and their authorized representatives upon request. This includes release of such information during the interim between appointment and reappointment for credentialing and peer review purposes, such as for ongoing professional practice evaluation. (2) I authorize the Organizations, their medical staffs, and their authorized representatives to release such information to other organizations, health care facilities, managed care entities, and their agents, who solicit such information for the purpose of evaluating my qualifications pursuant to a request for clinical privileges, participating provider status or other credentialing matter. This includes release of such information for credentialing and peer review purposes, such as for ongoing professional practice evaluation. (3) I authorize the release of information to such parties as I may specifically designate in the future in connection with my application for participation with additional organizations or entities. (4) I authorize UCMC affiliated hospitals and provider entities for which I am an applicant, including the medical staffs and authorized representatives of the foregoing, to release to one another and share with one another any information that bears on my professional qualifications, credentials, clinical competence, character, ability to perform safely and competently, ethics, or professional conduct. This authorization includes the right to inspect or obtain any communications, reports, records, statements, documents, recommendations or disclosures bearing on such matters. C. Information (1) I understand that it is my responsibility to produce adequate information so that my application can be properly evaluated. In addition to the information provided in this application, I also agree to provide the Organizations with any additional information which they or their authorized representatives may request. My failure to provide any requested information will cause my application to be incomplete and will prevent it from being processed. (2) I also agree to keep this Information Form current by informing the Organization of any changes in the Information provided, including, but not limited to, any investigations by a state licensure agency, any change in my professional liability insurance coverage, the filing of a professional liability lawsuit against me, any change in my status at any other health care organization, any change in my eligibility for participation in the Medicare or Medicaid programs, and any change in my ability to safely and competently exercise my clinical privileges because of health status issues, including impairment. 11 (3) I will make myself available for interview in regard to my application. D. Acknowledgements I acknowledge that (1) Clinical privileges or other forms of participation at the Organization are not a right of every licensed professional who makes application for the same; (2) My request will be evaluated in accordance with prescribed procedures defined by the Organizations and their medical staff bylaws, rules and regulations; (3) All medical staff recommendations relative to my application are subject to the ultimate action of the Organizations’ Boards of Directors, whose decisions shall be final; (4) If appointed, my clinical privileges shall be provisional for the time period determined by the Organization’s Board of Directors; (5) I have the responsibility to keep this Information Form current by informing the Organizations, through the Chief Executive Officer or designee, of any change in the areas of inquiry contained herein, including but not limited to any change in my professional liability insurance coverage, the filing of a lawsuit against me and any change in my status at any other organization; (6) Continued clinical privileges remain contingent upon my continued demonstration of professional competence and cooperation, my general support of the Organizations, as evidenced by treatment and continuous care and supervision of patients for whom I have responsibility and acceptable performance of all responsibilities related thereto as well as the other factors deemed relevant by the Organizations. Continued clinical privileges shall be granted only on formal application, according to organization and medical staff bylaws, rules and regulations, and upon final approval of the Organizations’ Boards of Directors; E. Release and Immunity By applying for clinical privileges, I accept the following conditions and intend to be legally bound by them, regardless of whether or not I am granted appointment and/or clinical privileges. These conditions shall remain in effect for the duration of any term of clinical privileges that I may be granted. (1) To the fullest extent permitted by law, I extend absolute immunity to, release from any and all liability, and agree not to sue the Organization, its medical staff, their authorized representatives, and appropriate third parties for any matter relating to appointment, reappointment, clinical privileges, or my qualifications for the same. This includes any actions, recommendations, reports, statements, communications, or disclosures involving me, which are made, taken, or received by the Organization, the medical staff, their authorized representatives, or appropriate third parties. (2) I extend absolute immunity to, and release from any and all liability, the Organizations, their authorized representatives and any third parties, as defined in subsection (3) below, for any acts, communications, reports, records, statements, documents, recommendations or disclosures involving me, performed, made, requested or received by the Organizations and their authorized representatives to, from, or by any third party, including otherwise privileged or confidential information, relating, but not limited to, the following: (a) (b) (c) (d) (e) (f) (g) (h) (i) (j) applications for clinical privileges, including temporary privileges; periodic reappraisals undertaken for increase or decrease in clinical privileges; proceedings for suspension or reduction of clinical privileges or for denial or revocation of clinical privileges or any other disciplinary sanctions; summary suspensions; hearing and appellate reviews; medical care evaluations; utilization reviews; any other organization, department, service or committee activities; matters or inquiries concerning my professional qualifications, credentials, clinical competence, character, mental or emotional stability, physical condition, ethics or behavior, and any other matter that might directly or indirectly have an effect on my competence, on patient care or on the orderly operation of this or any other organization or health care facility. 12 (3) The term “Organizations and their authorized representatives” means for each of the designated Organizations, the Organization corporation and any of the following individuals who have any responsibility for obtaining or evaluating my credentials, or acting upon my application or conduct in the Organization; the members of the Organization’s Board of Directors and their appointed representatives; the Chief Executive Officer or his designees; other Organization employees, consultants to the Organization, the Organization’s attorney and his partners, associates or designees, and all appointees to the medical staff. The term “third parties” means all individuals, including appointees to the Organization’s medical staff, and appointees to the medical staffs of other organizations or other physicians or health practitioners, nurses, or other government agencies, organizations, associations, partnerships and corporations, whether organizations, health care facilities or not, from whom information has been requested by the Organization or its authorized representatives or who have requested such information from the Organization and its authorized representatives. (4) If, notwithstanding the provisions in this Section F, I institute legal action again the Organization, its medical staff, or their authorized representatives and do not prevail, I agree to reimburse the Organization, and any medical staff members, directors, officers, employees and representatives who are named in the action for all costs incurred in defending such legal action, including reasonable attorney’s fees. The foregoing shall be privileged to the fullest extent permitted by law. Such privilege shall extend to the Organization and its authorized representatives, and to any third parties. _________________________________ Name (print) ____________________ Date APN must print name, sign and date ______________________________ Signature 13 Complete all sections ADVANCED PRACTICE NURSING WRITTEN COLLABORATIVE AGREEMENT A. ADVANCED PRACTICE NURSE INFORMATION 1. NAME: 2. ILLINOIS RN LICENSE NUMBER: ILLINOIS APN LICENSE NUMBER: ILLINOIS CONTROLLED SUBSTANCE LICENSE NUMBER: FEDERAL MID-LEVEL PRACTITIONER DEA NUMBER: List all certified specialties if applicable. 3. AREAS OF CERTIFICATION: 4. CERTIFYING ORGANIZATION: 5. CERTIFICATION EXPIRATION DATE: 6. CERTIFICATION NUMBER: List 7. PRACTICE SITES: Medical Center 8. CONTACT NUMBERS: information ________________________ FAX NUMBER: Always UCMC; can include additional off-sites EMERGENCY NUMBERS: (e.g., pager, answering service) 9. ATTACHMENTS: Copy of Certification/Recertification Copies of RN & APN License Copy of Certificate of Insurance Copy of Mid-Level Practitioner License Note attachments required B. COLLABORATING PHYSICIAN INFORMATION Collaborating MD Complete all sections 1. NAME: 2. ILLINOIS LICENSE NUMBER: 3. PRACTICE AREA OR CONCENTRATION: 4. BOARD CERTIFICATION (if any): 5. CERTIFYING ORGANIZATION: 6. PRACTICE SITES: 7. CONTACT NUMBERS: ________________________ FAX NUMBER: EMERGENCY NUMBERS: (e.g., pager, answering service) ------------------------------------------------------------------------------------------------------------------------------14 1. NAME: 2. ILLINOIS LICENSE NUMBER: 3. PRACTICE AREA OR CONCENTRATION: 4. BOARD CERTIFICATION (if any): 5. CERTIFYING ORGANIZATION: 6. PRACTICE SITES: 7. CONTACT NUMBERS: ________________________ FAX NUMBER: Do not complete additional collaborati ng physician information unless necessary. This refers to all other “consulting physicians” in service line. EMERGENCY NUMBERS: (e.g., pager, answering service) ------------------------------------------------------------------------------------------------------------------------------1. NAME: 2. ILLINOIS LICENSE NUMBER: 3. PRACTICE AREA OR CONCENTRATION: 4. BOARD CERTIFICATION (if any): 5. CERTIFYING ORGANIZATION: 6. PRACTICE SITES: 7. CONTACT NUMBERS: ________________________ FAX NUMBER: EMERGENCY NUMBERS: (e.g., pager, answering service) ------------------------------------------------------------------------------------------------------------------------------- 15 C. ADVANCED PRACTICE NURSE COLLABORATING PHYSICIAN WORKING RELATIONSHIP 1. SCOPE OF PRACTICE Under this agreement, the advanced practice nurse will work with the collaborating physician in an active practice to deliver health care services to . This includes, but is not limited to, the diagnosis, treatment and management of acute and chronic health problems; ordering, interpreting and performing laboratory and radiology tests; prescribing medications, including controlled substances, to the extent delegated; receiving and dispensing stock and sample medications; performing other therapeutic or corrective measures as indicated. Describe the type If applicable, the advanced practice nurse shall maintain allied health personnel privileges at the following of hospitals for the designated services: patients seen Hospitals: A copy of this written collaborative agreement shall remain on file at all sites where the advanced practice nurse renders service and shall be provided to the Illinois Department of Professional Regulation upon request. Any joint orders or guidelines are set forth or referenced in Attachment B. Typically UCMC 2. MEDICAL DIRECTION Physician medical direction shall be adequate with respect to collaboration with Certified Nurse Practitioners, Certified Nurse Midwives, and Certified Clinical Nurse Specialists if a collaborating physician: (A) participates in the joint formulation and joint approval of orders or guidelines with the advanced practice nurse and periodically reviews those orders and the services provided patients under those orders in accordance with accepted standards of medical practice and advanced practice nursing practice; (B) is on site at least once a month to provide medical direction and consultation; and (C) is available through telecommunications for consultation on medical problems, complications, or emergencies or patient referral. (See 225 ILCS 60/54.5(6).) The written collaborative agreement shall be for services the collaborating physician generally provided to his or her patients in the normal course of clinical practice. Medical direction for a Certified Registered Nurse Anesthetist shall be adequate if: (A) an anesthesiologist or a physician participates in the joint formulation and joint approval of orders or guidelines and periodically reviews those orders and the services provided patients under those orders; and (B) for anesthesia services, the anesthesiologist or physician participates through discussion of and agreement with the anesthesia plan and is physically present and available on the premises during the delivery of anesthesia services for diagnosis, consultation, and treatment of emergency medical conditions. Anesthesia services in a hospital shall be conducted in accordance with Section 10.7 of the Hospital Licensing Act and in an ambulatory surgical treatment center in accordance with Section 6.5 of the Ambulatory Surgical Treatment Center Act. (See 225 ILCS 60/54.5(b-5).) 16 3. COMMUNICATION, CONSULTATION AND REFERRAL The advance practice nurse shall consult with the collaborating physician by telecommunication or in person as needed. In the absence of the designated collaborating physician, another physician shall be available for consultation. The advanced practice nurse shall inform each collaborating physician of all written collaborative agreements he or she has signed with other physicians, and provide a copy of these to any collaborating physician upon request. 4. DELEGATION OF PRESCRIPTIVE AUTHORITY It is intended that this collaboration will include the prescription of medications by the APN, in conjunction with protocols and guidelines developed between the CP and the APN. The CP will review the prescription of medications by the APN periodically but at least annually. The APN will obtain a D.E.A. number if this collaboration includes the prescription of medications. The CP will file with the Department of Professional Regulation a notice of delegation of prescriptive authority and termination of such delegation, in accordance with rules to be established by the IDPR. The APN will register with the IDPR as a mid-level practitioner to receive a controlled substances license in Illinois. NOTE: ADVANCE PRACTICE NURSE MAY ONLY PRESCRIBE CONTROLLED SUBSTANCES UPON RECEIPT OF AN ILLINOIS MID LEVEL PRACTITIONER CONTROLLED SUBSTANCE LICENSE. WE THE UNDERSIGNED AGREE TO THE TERMS AND CONDITIONS OF THIS WRITTEN COLLABORATIVE AGREEMENT. Same date for both APN and APN must sign and date Collaborating Physician is Advanced Practice Nurse Date NOT required. APN must type or (Advanced Practice Nurse’s Typed or Printed Name) print name Collaborating Physician Date (Physician’s Typed or Printed Name) Collaborating Physician Date (Physician’s Typed or Printed Name) Collaborating Physician Collaborating MD must sign and date Date Collaborating MD must type or print name (Physician’s Typed or Printed Name) Collaborating Physician Date (Physician’s Typed or Printed Name) Collaborating Physician Date (Physician’s Typed or Printed Name) Collaborating Physician Date (Physician’s Typed or Printed Name) 17 Instructions for Delineation of APN Privileges Renewal Form: Definitions: Collaborating Physician – the primary physician with whom the APN is privileges and shares collaborative practice. Consulting Physician – other attending physicians working with the APN in practice at UCMC Board Certification – NP’s and CNS’s AMCC Certification, i.e. ACNP, FNP, PNP, Adult Health CNS Specialty Certification – Additional certifications, i.e. CCRN, ambulatory care nursing 1. Complete all form header information. Please copy all certifications for your file. 2. For every privilege requested, please circle either Renewal = R, Initiate = I, or Terminate = T request in the 2nd column. 3. For every privilege requested, please complete the approximate number of times in which you performed the stated privilege independently in the past year. 4. For any privilege not requested, please line out, initial, and date next to the privilege. 5. (Shaded Columns) Complete the shaded columns if you are requesting any new privileges from the previous approval. For all initial requests for APN privileges (not appearing on your previous forms, or marked ‘Initial’ request in the 2nd column) Please complete the # of times the requested privilege was proctored/performed prior to completion of this document. Depending on your practice specialty, proctoring for privileges may be completed by collaborating MD, consulting MD, or other APN. 6. Statement of competency: Please have the collaborating MD initial each privilege in the final column 7. APN and Collaborating Physician must both sign and date the bottom of the form. 8. APN Privileges are completed every 2 years and can be found on the UCMC Website at http://home.uchospitals. 18 Do not include a Consulting Physician. 1 2 If renewing privilege, # of times cannot equal zero 3 5 4 6 7 19 APN Peer P Rev view Helpful Gu uidelines s 1. Id dentify a fellow creden ntialed APN with similar clinical skillss for the Pee er Review. If you need assistance in identifying an a APN for your y review, please notiffy one of the e APNs on th he APN Council C for as ssistance or recommend dations. 2. Case C Review w: Choose a case which is typical fo or your speciialty and with hin your sco ope of care whether w patie ent care, research, educ cation, etc. F For example e, select a ca ase from the e most frrequent diagnosis seen in i your practtice or a proj oject that is tyypical of you ur practice. Incorporate evidenced-ba ased practice e and focus on outcome es. Include e educational materials, use of protocols, inte erdisciplinarry involveme ent, treatmen nt plans, etc.. relevant to the review. The review w should be a comprehens c ive discussio on of your p ractice. 3. Patient P Case e Review: Provide an ov verview of th he patient an nd treatmentt plan. Include presenting sy ymptoms, ph hysical asses ssment, labss and proced dures necesssary for diag gnosing and d trreating this in ndividual. Site S evidence e-based stud dies, UCMC policies and d protocols, or findings which w were considered in n coming to a diagnosis and treatme ent plan. 4. An A overview of o treatmentt plan and orr discharge p planning which addresse es patient trreatment, education and d follow up care. c Note all a referrals, ancillary carre departme ents you invo olved in the ca are of this pa atient. Offerr how these intervention ns addressed d quality pattient care an nd co ontributed to o evidence based b care. Please do n not have pa atient names s on any records. EXAMPLES: E A. All patients presenting for trea atment with symptoms o of depression are assesssed for suicidality; plan fo or suicide; ac ccess to wea apons and a ability to contract for safe ety. B. Patien nt presenting g with acute MI symptom ms receive a aspirin at the e time of arrivval to the emerg gency room or upon com mplaint and a assessmentt as an inpatient. C. Pneum monia patien nts receive the following g upon admisssion: a) oxyygenation asssessment; blood cultures tim mes three prio or to antibiottic; initial antibiotic receiived within 6 hours of hospittalization. 5. Research R Prroject, Educ cational Pro ogram, Absttract Presen ntation, etc: Choose a project or re esearch topic and demonstrate how your researrch, project or program developed h has co ontributed to o the educattional develo opment of nu urses or patients, improvved the quality of patientt ca are, enhanced interdisciiplinary colla aboration, im mproved com mmunication n among dep partments, patients etc. Incorporate written prottocols, resou urces utilized d, project im mplementation, use of evidenced ba ased practice e and the ide entification o of results or outcomes achieved. This should be e a comprehensive overvie ew of your prroject with a n evaluation n of the outco omes and im mpact on quality of care e. 6. Peer P Review wer commen nts: APN pe eer reviewerr comments should asse ess the APN in the ca ategories as s outlined in the Peer Re eview. Pleasse be sure to o address ea ach category ry. Comments C should s be based b on the e reviewers s experience e with the A APN in theirr area of clinical and professiona al practice only. o The Sec ction Adminis strator is ressponsible forr confirming all PHI in nformation is s excluded b before submission. 20 0 A APN must ccomplete all in nformation. APN A Name & Credentials s: ________ ___________ __________ __________ ________ T The reviewerr should be a Current C Certiffications: __ ___________ __________ __________ ___________ _______ ccolleague w with similar Position: P ____ ___________ __________ ___________ ___________ __________ ________ skills. APN A Pe eer Rev view Form Reviewer: R __ ___________ __________ __________ ___________ __________ ________ Case Review: R Choose C an a example typical o of your prractice, sh how how yyour practice e is evide enced based, have copies off your doccumentatio on (i.e. H& &P, consultt form, tele ephone notes, plan n of care, education n etc.) tha at is appro opriate to your ca ase review w. Please e attach additional a pages ass necessa ary. _______ ___________ __________ ___________ ___________ __________ __________ ___________ __________ _ _______ ___________ __________ ___________ ___________ __________ __________ ___________ __________ _ Choose a _______ ___________ __________ ___________ ___________ __________ __________ ___________ __________ case e which is _ _______ ___________ __________ ___________ ___________ __________ __________ ___________ __________ _ typiccal for _______ ___________ __________ ___________ ___________ __________ __________ ___________ __________ yourr specialty _ _______ ___________ __________ ___________ ___________ __________ __________ ___________ _ within and __________ _______ ___________ __________ ___________ ___________ __________ __________ ___________ __________ yourr scope of _ _______ ___________ __________ ___________ ___________ __________ __________ ___________ care e__________ whether _ _______ ___________ __________ ___________ ___________ __________ __________ ___________ __________ patie ent care, _ _______ ___________ __________ ___________ ___________ __________ __________ ___________ __________ _ rese earch, _______ ___________ __________ ___________ ___________ __________ __________ ___________ __________ _ educcation, _______ ___________ __________ __________ ___________ __________ __________ ___________ _ etc. __________ _______ ___________ __________ ___________ ___________ __________ __________ ___________ __________ _ _______ ___________ __________ ___________ ___________ __________ __________ ___________ __________ _ _______ ___________ __________ ___________ ___________ __________ __________ ___________ __________ _ _______ ___________ __________ ___________ ___________ __________ __________ ___________ __________ _ _______ ___________ __________ ___________ ___________ __________ __________ ___________ __________ _ _______ ___________ __________ ___________ ___________ __________ __________ ___________ __________ _ _______ ___________ __________ ___________ ___________ __________ __________ ___________ __________ _ _______ ___________ __________ ___________ ___________ __________ __________ ___________ __________ _ _______ ___________ __________ ___________ ___________ __________ __________ ___________ __________ _ _______ ___________ __________ ___________ ___________ __________ __________ ___________ __________ _ _______ ___________ __________ ___________ ___________ __________ __________ ___________ __________ _ _______ ___________ __________ ___________ ___________ __________ __________ ___________ __________ _ _______ ___________ __________ ___________ ___________ __________ __________ ___________ __________ _ _______ ___________ __________ ___________ ___________ __________ __________ ___________ __________ _ _______ ___________ __________ ___________ ___________ __________ __________ ___________ __________ _ _______ ___________ __________ ___________ ___________ __________ __________ ___________ __________ _ _______ ___________ __________ ___________ ___________ __________ __________ ___________ __________ _ Tip: T Include protocols off practice, re eferences, guideline es, etc. 21 APN Reviewer Comments: All sections must be completed by the reviewer Please assess the applicant/APN under the categories listed below. Comments should be based on experience with the applicant in the professional setting only. 1. Medical/Clinical Knowledge: Applies APN training, expertise and experience to enhance clinical practice to achieve quality patient care outcomes. Utilizes best practice principles and evidenced based protocols/guidelines to guide patient care delivery. 2. Technical and Clinical Skills: Demonstrates an understanding of the contexts and systems in which healthcare is provided and applies this knowledge to improve and optimize health care. Utilizes the electronic medical record, clinical tools and resources to maximize efficiency, accuracy of information and best practice principles in the delivery of patient care. 3. Clinical Judgment: Uses evidenced based practice and methods to investigate, evaluate, and improve patient care decision making and outcomes. Understands scope of practice and appropriately seeks consultation with collaborating or consulting physicians and other clinical experts as is appropriate. 4. Interpersonal Skills: Demonstrates interpersonal skills that enable him/her to establish and maintain professional relationships with patients, families, and other members of health care teams. Works cooperatively and collegially with others and shares appropriate information and resources to improve patient care outcomes. 22 5. Communication Skills: Demonstrates communication skills that enable him/her to establish and maintain professional relationships with patients, families, and other members of health care teams. Demonstrates diplomacy in dealing with others and respects the diverse backgrounds and opinions of others. Manages conflict in a productive manner and follows through to resolution. 6. Professionalism: Demonstrates behaviors that reflect a commitment to continuous professional development, ethical practice, respect of others, sensitivity to diversity and a responsible attitude towards his/her patients, profession, and society. Attends professional meetings, participates in ongoing professional education activities and participates in the education of others i.e. unit based educational seminars, patient care rounds, bedside consultation and education of nursing staff, speaking engagements at conferences, nursing grand rounds, etc. APN requesting privileges must sign Signature of APN being reviewed: ____________________________________ Signature of APN reviewer: _______________________________________ Date of review: ______/______/______ APN reviewer must sign Review date must be less than 90 days old. 23 Please com mplete and atttach the foll owing required docume ents: State of Illinois Health h Care Professio onal Recreden ntialing and Busin ness Data Ga athering Form http://w www.idph.sttate.il.us/abo out/credentia aling.htm ProCred Core C Competency Online Da atabase Repo ort Cards for the most rec cently ed fiscal yearr and complete current year-to-date. y http://p procred.uchicago.edu APN Direc ctory Bio – Submit on nline or fax to Janet Karol at 773-834-1578 7 APN Bio Inforrmation_distribute 24 4 Submit this form online or fax to Janet Karol at (773) 834-1578. APN Bio Information Name (including credentials): Title: Department: Section: Area of Clinical Focus: Interested in mentoring graduate school nurses? Short Bio paragraph: Highest Nursing Degree Achieved: Highest Non-Nursing Degree Achieved (if applicable): Certifications Achieved and Maintained (i.e. ACNP-BC): Contact Information: Phone: Pager: Fax: Email: Department Address: 25 CLAIM EX XPERIENC CE VERIFIC CATION FO ORM (UCM MC) INSTRUC CTIONS: Complete on ne form for each e carrie r listed in s section “C” (pgs. 7-8) o of the Illinois s Healthcare e Professio nal Data Ga athering Form UNIV VERSITY OF F CHICAGO MEDICAL C CENTER MEDICAL STAFF F OFFICE RYLAND AVE ENUE M/C 1 1130, Chicago, Illinois 6 60637 5841 S. MAR PHO ONE: (773) 702-3559 7 FA AX: (773) 83 34-0694 Applicant A to o complete top portion n only. Retu urn with application fo or appointm ment. APN should write UCMC Self Insured d Trust here. To: __ __________ __________ ___________ __________ __________ ___________ __________ rrier provides If another ca________ s Name off Self Insuring Institutio on, Employ yer or Insura ance Carrie er coverage as well, APN should dupliccate this form and provide________ tthat carrier’s Address s: ________ ___________ __________ ___________ ___________ __________ __________ information. For outside carriers, phone and fax Phone: __________ _ ___________ _ Fax: __ __________ __________ _ numbers, dates insured and policy nu umber must Dates Insured: ____ __________ _______ to __________ _ ________ Policy#:___ __________ ________ be included. I was ins sured by yo our institutio on or insura ance compa any for the periods listted above. This is to request that you co omplete the information n set forth b below and s submit it to o the Univerrsity of Chicago o Medical Sttaff Office, in i connectio on with my application n for privileg ges. _______ ___________ __________ __________ ___________ _______ Signaturre Date APN must sign, date, prrint or type nam me & SSN ______ __________ ________ Socia al Security # _______ ___________ __________ __________ ___________ ________ Print or Type Name e Do NOT writte below this liine _______ ___________ __________ __________ ___________ __________ __________ ___________ _________ Have the ere been any y medical ma alpractice cla aims made o or cases file ed against th he above pra actitioner, or settlements made on n behalf of th he practitione er in the passt ten years? ? _____ YES ___ ________ NO ______ If the ans swer to this s question is i yes, pleas se submit tthe followin ng on a sepa arate docum ment: o Claim Date of Name of Claimant e/claim pend ding? Is case If case e is closed: date d of closu ure, disposition and amou unt, if any, p paid in settlem ment or judg gment ________ ___________ ____________ ___________ ___________ ____ Signature e Date ________ ___________ ____________ ___________ ___________ ____ Title Phone Please fo orward to University U of o Chicago Medical M Cen nter, Medica al Staff Office (This form m may be du uplicated as necessary) 26 FORM K – MEDICARE ATTESTATION STATEMENT (UCMC) INSTRUCTIONS: PLEASE READ CAREFULLY BEFORE SIGNING PRACTITIONER ATTESTATION CLAUSE NOTICE TO PRACTITIONER "Medicare/CHAMPUS/Medicaid payment to the Medical Center is based in part on each patient's principal and secondary diagnoses and the major procedures performed on the patient, as attested to by the patient's attending physician by virtue of his or her signature in the medical record. Anyone who misrepresents, falsifies, or conceals essential information required for payment of federal funds, may be subject to fine, imprisonment, or civil penalty under applicable Federal laws." Please note that you may not “Opt-Out” of Medicare participation in any clinical setting (including private practice). If you Opt-Out of Medicare you are unable to bill Medicare in all settings for a minimum of 2 years. Participation in Medicare is a requirement of holding privileges at The University of Chicago Medical Center. PRACTITIONER'S ACKNOWLEDGMENT I acknowledge that I have received the above notice from The University of Chicago Medical Center. _______________________________________ Signature ___________________________________ Typed or Printed Name ________________ Date APN must sign, date, and print or type name 27 STATE OF ILLINOIS Health Care Professional Recredentialing and Business Data Gathering Form The Health Care Professional Credentials Data Collection Act [410 ILCS 517] requires that this form be collected from health care professionals by hospitals, health care entities, and health care plans which desire to credential such professional. Each hospital, health care entity, and health care plan may also require completion of supplemental forms. INSTRUCTIONS This form is for recredentialing only. Other forms are required for credentialing and for updating information. YOU ONLY HAVE TO FILL OUT AND SUBMIT WHAT IS REQUESTED BY THE CREDENTIALING ENTITY. PLEASE REFER TO THE INSTRUCTIONS PROVIDED TO YOU BY THE ORGANIZATION YOU ARE APPLYING TO FOR THEIR REQUIREMENTS. This form has been segmented into two (2) different Chapters, each containing various sections: Chapter A: Chapter B: Practice and Professional Information Business Information As previously noted, please consult the specific credentialing entity instructions for their individual Chapter or Section requirements for submission. GENERAL INSTRUCTIONS: Wherever this application requests information but does not provide sufficient space to provide a complete response (for example, you have more licenses, specialties, work history, etc.) provide attachments which contain all of the information requested in the relevant section OR duplicate the relevant section as many times as necessary and attach it to the back of this application. The data marked as “Confidential Information” shall be maintained in confidence to the extent required by law. They may be used by the health care plan, entity or hospital and by their agents for credentialing and internal business purposes. Other data contained in this form may be released. Health Care Professionals Recredentialing & Business Data Gathering Form Applicant Name: 28 ATTACHM MENTS A Attach formss A-F as need ded to supporrt “yes” resp ponses in Secction G: Proffessional Histtory and cop pies of the ffollowing: Curricu ulum Vitae CONFIDENTIAL IN NFORMATIO ON: Alll Current Profeessional Licensses Cu urrent Federal DEA D License, If I Applicable Curren nt State Controlled Substancee License(s), Iff Applicable Curren nt Professionall Liability Insu urance Face Shheet or Declaraation of Insurannce with Effective E Datee, Expiration Date D and Amoount Displayedd per Occurrennce and In n Aggregate Curren nt CLIA Certifi ficate, If Appliccable Curren nt W-9s, If App plicable AFFIRM MATION OF INFORMATIO ON I reprresent and waarrant that all of the inform mation provid ded and the reesponses giveen are correct and completee to the best of o my kknowledge an nd belief. I understand th hat falsificatiion or omissiion of inform mation may bbe grounds fo for rejection or o termiination, in addition to any penalties pro ovided by law w. I further aggree to prompptly inform all entities to w which this form m sent and not was t rejected of any change required to be updated by the Healtth Care Proffessional Credentialing an nd Businness Data Gatthering Updaate Form. I undderstand that this t applicatio on does not en ntitle me to paarticipation inn any hospitall, health care entity, or heaalth plan. APNs will need to sign and a print namee and date (datee must be han ndwritten, not typed). s and older copies oof this form cannnot be accepteed if the Forms witthout original signatures form is daated more than 180 days of beeing recredentiialed. Appllicant’s Signaature ** ** ** Type oor Print Namee Date PLEASE BE B ADVISED D THAT EACH HOSPIT TAL, HEALT TH CARE EN NTITY, AND HEA ALTH CARE E PLAN MAY Y ALSO REQ QUIRE COMP PLETION O OF AN ATT TESTATION N AND RELEA ASE OF INF FORMATION N FORM. ** *** *** Healthh Care Professio onals Recredentiaaling & Business Data 29 9 APN must m complete this t entire pagee. CHAPTER C R A: PRACTICE P E AND PR ROFESSIONAL IN NFORMAT TION SECTION S A. GENERAL L INFORMA ATION Namee: Last First MI Degrree List oother names by y which you hav ve been known n: First Last M MI If youu have been kn nown by other names, n please explain e why yo our name changged: Birth Date: (mm/dd d/yy) Sex: Male Female U.S. Citizen n? Yes No If no, do you u have a legal right to reside permanently p annd work in the U U.S.? Yes N No CONF FIDENTIAL IN NFORMATIO ON Resiident Visa No: Thiss information iss nnot required. Sociial Security Num mber: Emeergency Contacct Person: Last First MI Telep phone Numberr: ( ) Mailiing Address: Sttreet Daytiime Phone: ( ) City State Zip Fax Numberr: ( ) E-Maail Address: h appendeed additional in nformation fo or this section:: Checck here if you have (P Please continuee next page) Applican nt name must either e appear on n the bottom off each page orr be excluded frrom every page. 30 0 SECTION B. B PROFESS SIONAL INF FORMATIO ON A APN must enteer license numbber aand indicate iff it is unlimitedd or not. Illinoois Professionall License Number: License Un nlimited? Yes Y No If No, please p explain llimitation: Currrent Profession nal License(s) in Other States S State: License #: Liceense Unlimited d? Yes Exp. Date: No If No, please eexplain limitatiion: License #: S State: d? Liceense Unlimited Yes Exp. Date: No Liceense Unlimited d? Yes ((mm/dd/yy) If No, please eexplain limitatiion: License #: S State: (mm/dd/yy) Exp. Date: No ((mm/dd/yy) If APN has licenses in other states, they must enter the license number and indicate if license is unlimited or not. If No, please eexplain limitatiion: M Must enter DEA A license numbber, eexpiration date and indicate iff the license is unlim mited or not. C Check here if you y have appeended addition nal informatio on for this secttion: Current Federal DEA License Number: CONF NFIDENTIAL IINFORMATIO ON D DEA License Number N Expiraation Date: License Unlim mited? Yes N No If No, pleaase explain limiitation: C Check here if you y have appeended addition nal informatio on for this secttion: Currrent State Con ntrolled Substa ance Number((s): CONFID DENTIAL INF FORMATION N CS Liceense #: S State: Expiratioon Date: (mm m/dd/yy) S State: CS Liceense #: Expiratioon Date: S State: CS Liceense #: Expiratioon Date: (mm m/dd/yy) APN must list the state for their current controlled substance license, the license number and expiration date. (mm m/dd/yy) P Please identiify liimitation. all lim mitation rela ated to the above C Controlled S Substances Number(s) Applicant name mus st either appea ar on the bottom m of each page e or be exclude ed from every page. and explain n 31 APNs musst enter their NPI numbeer. P ID# (UPIN): ( Mediicare Unique Provider Natioonal Provider Identification n Number (NP PI): See “Commonn Links” for morre info regarding NPI. Mediicaid ID#: X-Raay Certificatio on: State: Certificaate #: Exp iration Date: Checck here if you have h appendeed additional in nformation fo or this section:: mm/dd/yy) (m APNs m may leave “X-R Ray Certificatioon” blank. COM MPLETE FO OR EACH SPECIALTY Speciialty I: oard Certified in Specialty I? Yes Are you Bo No N If Yes, nam me of Certifyin ng Board: Date of Ceertification: Date of Recertification R (if applicable): (m mm/yy) (mm/yy) If No, havee you taken or are you schedu uled to take thee specialty boarrds certificationn? Yes If Certifyin ng Boards taken, give date: No Certification Expiration Datte, if Any: (mm/yy) ((mm/yy) If not taken n, date schedulled to take Speccialty Boards: (mm/yy) Speciialty/Subspeciialty II: Are you Bo oard Certified in Specialty II?? Yes No N APNs must enter areas of certification (i.e. Pediatric Nurse Practitioner Primary Care). This information can be found on the verification reports included in their packet. If Yes, nam me of Certifyin ng Board: Date of Ceertification: Date of Recertification R (if applicable): (m mm/yy) (mm/yy) If No, havee you taken or are you schedu uled to take thee specialty boarrds certificationn? Yes If Certifyin ng Boards taken, give date: No Certification Expiration Datte, if Any: (mm/yy) ((mm/yy) If not taken n, date schedulled to take Speccialty Boards: (mm/yy) (P Please continu ue next page) Applican nt name must either e appear on n the bottom off each page orr be excluded frrom every page. 32 2 Speciialty/Subspeciialty III: Are you Bo oard Certified in Specialty IIII? Yes No N If Yes, nam me of Certifyin ng Board: Date of Ceertification: Date of Recertification R (if applicable): (m mm/yy) (mm/yy) If No, havee you taken or are you schedu uled to take thee specialty boarrds certificationn? Yes If Certifyin ng Boards taken, give date: No Certification Expiration Datte, if Any: (mm/yy) ((mm/yy) If not taken n, date schedulled to take Speccialty Boards: (mm/yy) Speciialty/Subspeciialty IV: Are you Bo oard Certified in Specialty IV V? Yes No N If Yes, nam me of Certifyin ng Board: Date of Ceertification: Date of Recertification R (if applicable): (m mm/yy) (mm/yy) If No, havee you taken or are you schedu uled to take thee specialty boarrds certificationn? Yes If Certifyin ng Boards taken, give date: No Certification Expiration Datte, if Any: (mm/yy) ((mm/yy) If not taken n, date schedulled to take Speccialty Boards: (mm/yy) Checck here if you have h appendeed additional in nformation fo or this section:: CURRE ENT PROFE ESSIONAL LIABILITY L INSURANCE I E This section is blank w when it is givenn to the APNs, but theyy must enter thheir current professional liiability insurannce as shown. CONFID DENTIAL INF FORMATION:: Carrier: University of Chicago Medical Center Selff Insured Trustt Address: _5841 S. Maaryland Ave. Chicago C Street umber: Policy Nu IL City State Original Effeective Date: cotterminus (mm/dd/yy) Policy Liimits: 60637 Zip E Expiration Datee: w/employmeent (mm/dd/yyy) Per Occurrence: O $ Aggregate: $ Amounts are not f required for UCMC tru ust Retroactiive Date: (mm/d dd/yy) Check Occu urrence What type of coverage do d you have? Claims Made M xO Occurrence Has any judgment j or paayment of claim m or settlementt amount exceeeded the limits of this coveragge? No Yes Circle Yes or No o Applic cant name mus st either appear on the bottom m of each page e or be exclude ed from every page. 33 3 Inforrmation listed on o this page caan serve as anotther way to verrify the numbeer of H-2 Formss needed for eaach packet. A separate H-2 Forrm is needed fo or each insuran nce carrier. Alll facilities coveered under the U UCMC Self-Innsured Trust onnly require onee H-2 Form. MEMBERSH M HIP STATUS S – USE FOR R SECTIONS S C AND D Please usee the following g key to indiccate membersship status in Sections C (H Hospital Mem mbership – Cu urrent and Pendiing) and D (Am mbulatory Surgery Center Practice) P beloow. A. Active A nded / Terminaated/ Resigned E. Suspen I. Provisionnal B. Courtesy F. Active Provisional Sttaff J. Affiliate C. Consulting G. Seniorr Staff K. Pendingg D. Adjunct A H. Associiate L. Other (S Specify) SECTIO ON C. HOSPIITAL MEMBERSHIP - CURRENT A AND PENDIING Please list all hospitals at which you are a membeer of the Mediical Staff and d have clinicall privileges orr have applications for privileg ges pending. (Include ( additio onal sheets if m more than threee hospitals.) APN must list A. Primary Hospital UCMC as N Hospital Name: the primary Address: hospital Street S City ty State Zipp where Membersh hip Status: Dates: To Present they are a F From (mm/yy) member of the Departmen nt/Division: Medicall Staff Office F FAX #: ( ) Medical Departmen nt Telephone #: ( ) Staff and have Any Limitaations in Your Area of Speciaalty at this Hosspital? clinical or pending privileges. B. O Other Hospita al Hospital Name: N Address: Street S City ty Membersh hip Status: Dates: F From (mm/yy) Departmen nt/Division: State Zipp To: To (mm/yyy) Medicall Staff Office F FAX #: ( ) Departmen nt Telephone #: ( ) Any Limitaations in Your Area of Speciaalty at this Hosspital? Applic cant name mus st either appear on the bottom m of each page e or be exclude ed from every page. APN must list any other hospitals at which they are a member of the Medical Staff and have clinical privileges or pending privileges. 34 4 C. O Other Hospita al Hospital Name: N Address: Street S City ty Membersh hip Status: Dates: From (mm/yy) F Departmen nt/Division: State Zipp To: To (mm/yyy) Medicall Staff Office F FAX #: ( ) Departmen nt Telephone #: ( ) Any Limitaations in Your Area of Speciaalty at this Hosspital? If APNs work at more than three hospitals they may attach a separate piece of paper listing this information. Checck here if you have h appendeed additional in nformation fo or this section:: (Please contiinue next pagee) Applican nt name must either e appear on n the bottom off each page orr be excluded frrom every page. 35 Leav ve this sheet bllank. SECTIION D. AMB BULATORY Y SURGERY Y CENTER P PRACTICE Please listt all ambulato ory surgery centers c where you currentlly have or prreviously had privileges. U Use the Membersh hip Status key y at the top of o page 7. (In nclude additionnal sheets if m more than threee ambulatory ssurgery centers.) A) P Primary Ambu ulatory Surgeery Center ASC Namee: Address: Street S Citty Telephone: ( ) State Ziip Fax Numberr: ( ) hip Status: Membersh Dates: To: F From (mm/yy) To (mm/yyy) B) O Other Ambula atory Surgery Center ASC Namee: Address: Street S Citty Telephone: ( ) State Ziip Fax Numberr: ( ) hip Status: Membersh Dates: To: F From (mm/yy) To (mm/yyy) C) O Other Ambula atory Surgery Center ASC Namee: Address: Street S Citty Telephone: ( ) State Ziip Fax Number:: ( ) Membersh hip Status: Dates: To: From (mm/yy) F To (mm/yyy) h appendeed additional in nformation fo or this section:: Checck here if you have (Please contiinue next pagee) Applican nt name must either e appear on n the bottom off each page orr be excluded frrom every page. 36 SE ECTION E. WORK W HIST TORY List chronologically (m most recent first) f all worrk engagemen nts (includingg employmen nt, self-employyment, service ass an independ dent contractor, and military service) iin the last foour (4) years.. Do not duplicate internship p, residency, and a fellowship p information previously reeported. If there is any gap p of greater th han 30 days in chronology, exp plain it on a sep parate page. Currrent work placce: University of Chicago Medical M Centerr Address: 5841 5 S Mary yland Avenu ue Ch icago Street S Telephone: ( ) IL 60 0637 Citty State Ziip Citty State Ziip APNs must list their current place of work. Be sure to list UCMC as current work place. Note: You only need to list places worked since last Appointment. Fax x Number: ( ) Title or Pro ofessional Occupation: Time in thiis employmentt: From: to Prresent (mm/y yy) Previious work placce: Address: Street S Telephone: ( ) Fax Number: ( ) ofessional Occupation: Title or Pro Time in thiis employmentt: From: to: (mm/y yy) (mm/yy) Previious work placce: Address: Street S Telephone: ( ) ty City State Zipp Citty State Ziip Fax Numberr: ( ) ofessional Occupation: Title or Pro to: Time in thiis employmentt: From: (mm/y yy) (mm/yy) Previious work placce: Address: Street S Telephone: ( ) Fax Numberr: ( ) ofessional Occupation: Title or Pro Time in thiis employmentt: From: to: (mm//yy) (mm/yy) Applican nt name must either e appear on n the bottom off each page orr be excluded frrom every page. 37 7 APNs may leave this sheeet blank SECTION F. F MEDICAL L EDUCATIION/CLINIC CAL TRAIN NING UPDAT TE Please pro ovide an upda ate of your medical m educattion and cliniccal training oover the past four years. D Do not duplicate internship, reesidency, and fellowship in nformation prreviously repoorted. (Attachh additional shheets if necessary.)) FIRST UPDATE U Residency Fellowsh hip Other O Instituution Name: Depaartment Chair or o Program Direector: Last Nam me Firstt Name MI Degree Mailiing Address: Sttreet Datess attended: State City Telepphone Number:: ( ) Zipp Fax Num mber: ( ) From: F To: mm/yy Type of in nternship: mm/y yy Ro otating Sttraight Did you su uccessfully com mplete this program? Iff straight, pleasse list specialtyy: Yes No If no, pleaase attach an exxplanation. Weree you the subjecct of any discip plinary action during d your atteendance at thiss institution? Yes No (Attach an n explanation oof a “Yes” answ wer.) SECON ND UPDATE Fellowsh hip Residency Other O Instituution Name: Depaartment Chair or o Program Direector: Last Nam me Firstt Name MI Degree Mailiing Address: Sttreet City Telepphone Number:: ( ) Datess attended: State Zipp Fax Num mber: ( ) From: F To: mm/yy Type of in nternship: Ro otating mm/yy Sttraight Did you su uccessfully com mplete this program? Iff straight, pleasse list specialtyy: Yes No If no, pleaase attach an exxplanation. Weree you the subjecct of any discip plinary action during d your atteendance at thiss institution? Yes No (Attach an n explanation oof a “Yes” answ wer.) Checck here if you have h appendeed additional in nformation fo or this section:: Applica ant name must either appear on o the bottom o of each page o or be excluded from every page. 38 SECT TION G. PRO OFESSIONA AL HISTOR RY: CONFID DENTIAL ADVERSE OR OTHER AC CTIONS APN must aanswer each quuestion in this section. If APNs answ wer “Yes” to anny of the questiions, they will have to complete Foorm A. ns to the bestt of your knoowledge with a “yes” or S Submit with all a application ns. Please ansswer the follo owing question ““no.” If you answer a “yes” to any questio on(s) please co omplete Form m A. Please m make copies off Form A as n needed and ccomplete one form f for each “yes” answer. P Please providee information on your profeessional history y over the passt four (4) yearrs. 1. Has your liccense to practtice in any jurrisdiction everr been denied , restricted, limited, susspended, revoked, canceled d and/or subjject to probaation either voluntarily or o involuntarilly, or has you ur application for a licensee ever been withdrawn? Yes N No Have you beeen reprimandeed and/or fined d, been the subjject of a compplaint and/or have you beeen notified in writing w that you have been in nvestigated as tthe possible subject of a criminal, civill or disciplinarry action by an ny state or fedderal agency which licenses providers? Yes N No 3. Have you losst any board ceertification(s), and/or a failed to o recertify? Yes N No 4. Have you been examined by b a Certifying Board but faileed to pass? Yes N No 5. Has any info ormation pertaaining to you, including i malp practice judgm ments and/or disciplinary action, ever been b reported to t the Nationaal Practitioner Data Bank (NPDB) and d/or any other practitioner p dataa bank? Yes N No Has your fed deral DEA nu umber and/or state s controlled d substances liicense been restricted, liimited, relinqu uished, suspen nded or revok ked, either volluntarily or involuntarily y, and/or have you ever been n notified in writing w that youu are being investigated as the possib ble subject of a criminal orr disciplinary aaction with our DEA or con ntrolled substan nce registration? respect to yo Yes N No Have you, orr any of your hospital h or amb bulatory surgery center priviilegesand/or membership been denied, revoked, susp pended, reducced, placed onn probation, proctored, pllaced under maandatory consu ultation or non-rrenewed? Yes N No Have you vo oluntarily or in nvoluntarily rellinquished or failed f to seek rrenewal of your hospitall or ambulatory y surgery centeer privileges for any reason? Yes N No Have any disciplinary actio ons or proceed dings been insttituted against you and/or are any discciplinary action ns or proceediings now pend ding with resppect to your hospital or am mbulatory surg gery center priivileges and/or your license? Yes N No Have you beeen reprimandeed, censured, excluded, e suspended and/or ddisqualified from particiipating, or vo oluntarily with hdrawn to av void an investtigation, in Medicare, Medicaid, M CHA AMPUS and/or any other go overnmental heealth-related programs? Yes N No Yes N No 2. 6. 7. 8. 9 10. 11. Have Medicare, Medicaid,, CHAMPUS, PRO authoritiies and/or anyy other third party payorss brought charges against yo ou for alleged inappropriate fees and/or quality-of-caare issues? Applica ant name must either appear on the bottom of each page o or be excluded d from every page. 39 9 12. 13. Have you beeen denied mem mbership and/o or been subject to probation, rreprimand, sanction or disciplinary d acttion, or have you y ever been notified n in wriiting that you aare being investigated as the possible p subjecct of a criminaal or disciplinaary action by aany health care organization, o e..g. hospital, HM MO, PPO, IPA A, professional group or socieety, licensing boaard, certificatio on board, PSRO O, or PRO? Y Yes No Have you withdrawn w an application a or any a portion off an applicationn for appointm ment or reappointtment for clin nical privilegees or staff appointment or for a licensee or membership in an IPA, PH HO, professionaal group or socciety, health caare entity or heealth care plan prior to a finaal decision to avoid a proffessional revieew or an adveerse decision? Y Yes No PRO OFESSIONA AL LIABILIITY ACTION NS APNs musst answer each question in this section. If “Y Yes” is answered too any question,, they will havee to complete F Form B. IIf you answer yes to any queestion(s) in thiis section please complete F FORM B. Pleaase make copies of FORM B if n needed, and co omplete one fo or each yes answer. 1. Have any pro ofessional liabiility judgmentss ever been enteered against yoou? Y Yes No 2. Have any pro ofessional liabiility claim settllements ever beeen paid by yo u and/or paid oon your behalf? Y Yes No Are there any y currently pen nding professio onal liability su uits, actions andd/or claims fileed against you? Y Yes No our clinical actions? Has any persson or entity beeen sued for yo Y Yes No 3. 4. LIA ABILITY INSURANCE These answers must be consisstent with the yes/no answers provided d on page 10 (Applicatio on for Reappointm ment). AP PNs must answ wer this questioon. If “Y Yes” is answereed, they will haave to coomplete Form C C. y to this question please co omplete FORM M C. Iff you answer yes Havve you been denied d or volu untarily relinqu uished your professional p liaability insurannce coveerage, and/or have had your professional liability insurrance coveragee canceled, noonreneewed or limits reduced? r CR RIMINAL AC CTIONS Y Yes No APNs m must answer eaach question inn this section. IIf “Yes” is answ wered, they willl have to compplete Form D. IIf you answerr yes to any question(s) q in this section please p complette FORM D. Please makee copies of FO ORM D if n needed, and co omplete one fo or each yes answer. 1. 2. Have you been b charged with w or convicted of a crim me (other thann a minor traaffic offense) in th his or any otheer state or cou untry and/or do o you have anyy criminal charrges pending otheer than minor trraffic offenses in this state or any other statee or country? Y Yes No Have you beeen the subjectt of a civil or criminal c comp plaint or adminnistrative actionn or been notified d in writing th hat you are beeing investigatted as the posssible subject at a civil, crimin nal or adminisstrative action n regarding seexual miscondduct, child abuuse, domestic vio olence or elder abuse? Y Yes No Applic cant name mus st either appearr on the bottom m of each page or be excluded d from every page. 40 0 ME EDICAL CON NDITION IIf you answer yes to this queestion please complete c FOR RM E. APNs must answer this question. If “Yes” is answered, thhey will have tto complete Foorm E. Do you have a medical m conditio on, physical deefect or emotiional impairmeent which in aany or limits your ab bility to practicce medicine wiith reasonable sskill and safetyy? wayy impairs and/o Y Yes No APNs mu must answer thhe questions in this section. Iff “Yes” is answ wered, they wiill have to compleete Form F. CH HEMICAL SU UBSTANCES OR ALCO OHOL ABUS SE IIf you answerr yes to any question(s) q in this section please p compleete FORM F. Please makee copies of FO ORM F if n needed, and co omplete one fo or each yes answer. 1. Are you currrently engaged in illegal use of o any legal or illegal substannces? Y Yes No 2. Do you curreently overuse and/or a abuse alccohol or any otther controlledd substances? Y Yes No 3. If you use alccohol and/or ch hemical substaances, does you ur use in any w way impair andd/or limit your ab bility to practice medicine witth reasonable sk kill and safety?? Y Yes No 4. Are you cu urrently particcipating in a supervised rehabilitation r program andd/or professional assistance pro ogram which monitors you for alcohol aand/or substannce abuse? Not A Applicable Y Yes No APNs mustt answer this quuestion. If “Yes” is answeredd, they will have too provide an exxplanation. INV VESTMENT TS In thhe last five (4) years have you y and/or a member m of you ur family purchhased or madee an inveestment in (oth her than securrities of a pub blicly traded company), c or otherwise havve a busiiness interest in n any clinical laboratory, l diaagnostic or testting center, hosspital, surgicennter, and//or other busin ness dealing wiith the provisio on of ancillary y health servic es, equipment or suppplies? Y Yes No If Yees, please prov vide explanatio on: (P (Please continu ue next page) App plicant name must either appe ear on the botto om of each pag ge or be exclud ded from every page e. 41 CHAPTER C R B: BUSINE ESS INFO ORMATIO ON SECTION H. PRIMA ARY SITE IN NFORMATIION ormation for the t primary siite at which yoou practice. Pleasse provide the following info Prim mary Siite Group/Business Name N Primary site should always be UCMC. APNs must provide all of the requested information. Buillding Name Offiice Address – Number N and Sttreet – Suite City y County ( ) Maiin Telephone Number N ( ) FAX F Number ( ) Emeergency Number ( ) Answering A Serv vice Are yyou currently acccepting new patients p at this location? l Ziip Firrst Office O Adminisstrator – Last ( ) Beeeper Number State MI E -mail Yes No Iff yes, describe any restrictions (e.g., appointtment type, pattient type): n of activ ve patients enro olled with you at this site: Please provide the number Please provide the number n of patieent visits you have h at this sitee per year: List aany special sk kills or qualiffications you or o your officee staff have th hat enhance yyour ability too practice meedicine or trea at certaain patients orr classes of patients. List separately an ny special lan guage skills, such as fluen ncy in a foreiggn language or o profiiciency in sign language. S Special Skills of o Practitioner: S Special Skills of o Staff: L Languages Spo oken by Practitiioner: L Languages Wriitten by Practitiioner: Questiions in this sectionn can be left blaank. L Languages Spo oken by Staff: L Languages Wriitten by Staff: ext page) (Pleasse continue nex Applica ant name must either appear on the bottom of each page o or be excluded d from every page. 42 2 APN may y leave this pagge blank. Pleasse provide the following infformation about physician(ss)/practitionerr(s) who proviide coverage ffor patients en nrolled at thiss site w when you are not n available. Namee: Firstt Last MI Degrree Specialty: Address: Telepphone: ( ) Street S Availabilitty: Days Nights City Weekends Statee Holidays Zip CONFIDE ENTIAL INFO ORMATION: Tax ID #: Namee: Firstt Last MI Degrree Specialty: Address: Street S Availabilitty: Days Nights City Weekends Statee Holidays Telephone: ( ) Zip CONFIDE ENTIAL INFO ORMATION: Tax ID #: Namee: Firstt Last MI Degrree Specialty: Address: Street S Availabilitty: Days Nights City Weekends Statee Holidays Telephone: ( ) Zip CONFIDE ENTIAL INFO ORMATION: Tax ID #: (Please contiinue next pagee) Applica ant name must either appear on the bottom of each page o or be excluded d from every page. 43 3 APN will on nly need to com mplete this pag ge if they work at additional ssites. (NOT RE EQUIRED) SECTION I.. ADDITION NAL SITE IN NFORMATIION Pleasse provide the following info ormation for each e additiona al site at which h you practicee. Siite # Group/Business Name N Buillding Name Offiice Address – Number N and Sttreet – Suite City y County ( ) N Maiin Telephone Number Office O Adminisstrator – Last ( ) Beeeper Number ( ) FAX F Number ( ) Emeergency Number ( ) Answering A Serv vice Are yyou currently acccepting new patients p at this location? l Statee Firrst E -mail Yes Zip MI Questions in this section can be left blank. No Iff yes, describe any restriction ns (e.g., appointtment type, pattient type): n of activ ve patients enro olled with you at this site: Please provide the number Please provide the number n of patieent visits you have h at this sitee per year: List aany special sk kills or qualiffications you or o your officee staff have th hat enhance yyour ability too practice meedicine or trea at certaain patients orr classes of patients. List separately an ny special lan guage skills, such as fluen ncy in a foreiggn language or o profiiciency in sign language. S Special Skills of o Practitioner: S Special Skills of o Staff: L Languages Spo oken by Practitiioner: L Languages Wriitten by Practitiioner: L Languages Spo oken by Staff: L Languages Wriitten by Staff: (Please conttinue next pagge) Applican nt name must either e appear on o the bottom o of each page orr be excluded ffrom every e page. 44 4 APN Ns may leave th his page blank.. Pleasse provide the following infformation about physician(ss)/practitionerr(s) who prov ide coverage ffor patients en nrolled at thiss site w when you are not n available. Namee: Firstt Last MI Degrree Specialty: Address: Street S Availabilitty: Days Nights City Weekends Statee Holidays Telephone: ( ) Zip CONFIDE ENTIAL INFO ORMATION: Tax ID #: Namee: Firstt Last MI Degrree Specialty: Address: Street S Availabilitty: Days Nights City Weekends Statee Holidays Telephone: ( ) Zip CONFIDE ENTIAL INFO ORMATION: Tax ID #: Namee: Firstt Last MI Degrree Specialty: Address: Street S Availabilitty: Days Nights City Weekends Statee Holidays Telephone: ( ) Zip CONFIDE ENTIAL INFO ORMATION: Tax ID #: End Recredenttialing and Business D Data Gatheering Form m. Atttach Form ms A-F As R Required. Applicant name mu ust either appe ear on the botto om of each pag ge or be exclud ded from every page . 45 APNs must complete this paage if they answ wered “Yes” to o a question in the Adverse an and Other Actioons section. FORM A – AD DVERSE AND D OTHER ACT TIONS ATE this form m as necessarry to completee separate sh heet for EACH H occurrence that applies.. Use DUPLICA reverse sid de of this form m if additional space is needed. Appliicant Name: Last First M MI Indicaate the numberr of ONE of thee questions in Section S J to whhich you answeered “yes”: Quuestion Numbeer: A. D Describe the circcumstances surrrounding this occurrence. Please include thhe date of the ooccurrence. B. Prrovide an explaanation of any actions taken. Please includee the date the aaction was takeen. C. Prrovide the currrent status of th he issue. D. Iff known: Co ontact: Department/Com D mmittee: Address: A Streeet State Citty Telephone: ( ) Signaature: Date: Zipp If this form haas been completed, A APN must sign andd date. Applicant name must eitther appear on the bottom of each page or b be excluded fro om very page. ev 46 APN N must complette this page if they t answered “Yes” to a queestion in the Prrofessional Liabbility Actions section. All fieelds must be ccompleted on th his page. BILITY ACTIONS FORM B – PROFESSIIONAL LIAB DUPLICA ATE this form m as necessary to complete a separate sheeet for EACH aaction or alleggation. Use reeverse side of thiss form if addittional space iss needed. Appliicant Name: Last First M MI First M MI A. Pllaintiff’s Namee: Last If court casse, Case Name & Case Numbber: B. Y Your Involvemeent in the Care (Attending, Co onsulting, Etc.)): C. Y Your Status in th he Case (Sole Defendant, D Co--Defendant, Ow wnership Intereest in Providerr Practice Namee in Suuit, Etc.): D. A Allegations, inclluding Patient Outcome, if Av vailable: E. Date of Incidentt (mm/yy): If this form has been completed, E through H are required. F. Date Filedd (mm/yy): G. D Date Case Closeed (mm/yy): R Resolution Casee: Dismisssed Settlem ment out of Cou urt Judgm ment Pend ding Arrbitration M ediation H. A Amount Paid on n Your Behalf (if ( any): $ I. Proofessional Liab bility Insurer Name N (if one waas involved): J. Inssurer Telephon ne Number: ( ) Other APN must provide informationn for letters I through L L, which shouuld correlate with the H--2 form. K. Policy Numbeer: L. Innsurer Address (Street, City, State, S Zip Codee): If this form hhas been completed, A APNs must sign annd date. Signaature: Date: Applic cant name mus st either appea ar on the bottom m of each page e or be exclude ed from every page. 47 7 APN N must compllete this page iff they answered “Yes” to a quuestion in the L Liability Insuraance section. FORM M C – LIABILIITY INSURAN NCE DUPLICA ATE this form m as necessary to complete a separate sheeet for EACH aaction or alleggation. Use reeverse side of thiss form if addittional space iss needed. Appliicant Name: Last First M MI A. H History of Proffessional Liabiility Insurancee (Please check k One) Canceled Voluntarily V Non-Reenewed Canceled Involuntarily I Applicattion Denied B. Carrier Name: C. Caarrier Telephon ne Number: ( ) D. Poolicy Number: E. Caarrier Address (Street, City, State, S Zip Codee): F. Daates of Coverag ge: From (m mm/yy): To (mm/yy): G. Ciircumstances In nvolved: If this form haas been completed, APN must sign and date.. Signaature: Date: Applicant name n must eith her appear on the t bottom of e each page or b be excluded from eve ery page. 48 APN must m complete this page if they answered “Y Yes” to a questtion in the Crim minal Actions ssection. FORM M D – CRIMIINAL ACTION NS DUPLICA ATE this form m as necessary to complete a separate sheeet for EACH iincident. Use reverse side oof this form if ad dditional spacee is needed. Appliicant Name: Last First M MI A. D Date of Incidentt (mm/yy): Date of Complaiint or Conviction (mm/yy): B. D C. Date of Resolutiion (mm/yy): d, Plea Bargain n, Misdemeano or, Felony): D. Tyype of Resoluttion (Dismissed E. Alllegation(s): F. Deetails of Incideent: Actions Taken Against A You: G. A H. C Current Status of o Situation: If this form has beenn complleted, APN muust sign aand date. ult of This Situ uation: I. Meedical Practice Privileges Afffected as a Resu Signaature: Date: Applic cant name mus st either appea ar on the bottom m of each page e or be exclude ed from every page. 49 9 APNss must complette this page if they answered “Yes” to a queestion in the Meedical Conditioon section. FORM M E – MEDICA AL CONDITIION DUPLICA ATE this form m as necessary y to complete a separate sh heet for EACH H condition. U Use reverse siide of this form if i additional space is needed d. Appliicant Name: Last First M MI A. D Describe this meedical conditio on: B. Too what extent does d or could th his condition affect a your currrent ability to ppractice mediciine in your speccialty arrea or to perforrm a full range of clinical actiivities? C. W What is the current status of yo our condition? D. Prrovide the nam me and address of your person nal physician/health care provvider who can pprovide inform mation about yoour health coondition. Name Teleephone Number ( ) Laast First MI Degreee Laast First MI Degreee ( ) Signaature: If this form hhas been completed, APN must sign andd date. Date: Applicantt name must eiither appear on n the bottom off each page or be excluded frrom ev very page. 50 0 APN A must com mplete this pagee if they answerred “Yes” to a question in thee Chemical Subbstances or Alcoho ol Abuse sectioon. FORM F – CHEMICA AL SUBSTAN NCES OR ALC COHOL ABU USE DUPLICA ATE this form m as necessary to complete a separate sheeet for EACH cchemical substtance incident. Use U reverse siide of this form m if additionall space is need ded. Appliicant Name: Last First M MI Descrribe the substan nce you use: A. To what extent does, d or could, your use of this substance afffect your curreent ability to prractice medicinne in your sspecialty area or o to perform a full range of clinical c activitiees? Monitored by Sttate Board Man ndate (Name an nd Address) B. M C. Monitoredd Voluntarily (N Name and Address) Other informatio on about the cu urrent status off your use of su ubstances: D. O ( E. Abbstinent since (mm/yy): F. Prrovide the nam me and address of your person nal physician/h health care proovider who cann provide inforrmation about your treatmentt foor alcohol or ch hemical substan nce use and can n comment on what impact (iif any) it has onn your current//future professiional practice. Name: Address: Street S Telephone: ( ) Signaature: City State Ziip If this form hhas been completed, A APN must sign and datte. Date: App plicant name must either appe ear on the botto om of each pag ge or be exclud ded from every page e. 51 Common Links Used for the Recredentialing Application IDPH State of Illinois Form (recredentialing)- http://www.idph.state.il.us/about/credentialing.htm ProCred Report- http://corecompetency.uchicago.edu The physician will have to use their CNet ID and password to login the system. NPI Number- https://nppes.cms.hhs.gov/NPPES/NPIRegistrySearch.do?subAction=reset&searchType=ind License Lookup: https://www.idfpr.com/licenselookup/licenselookup.asp 52






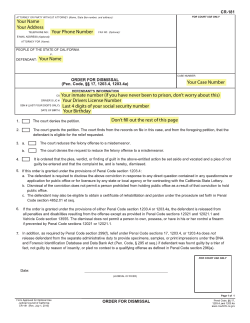


© Copyright 2026