
Therapy for ongoing graft-versus-host disease induced across the
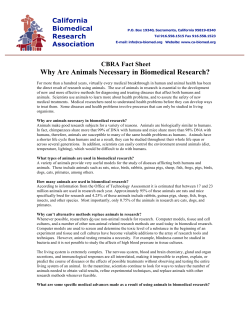
From www.bloodjournal.org by guest on October 15, 2014. For personal use only. 1995 86: 4367-4375 Therapy for ongoing graft-versus-host disease induced across the major or minor histocompatibility barrier in mice with anti-CD3F(ab')2-ricin toxin A chain immunotoxin DA Vallera, PA Taylor, A Panoskaltsis-Mortari and BR Blazar Updated information and services can be found at: http://www.bloodjournal.org/content/86/11/4367.full.html Articles on similar topics can be found in the following Blood collections Information about reproducing this article in parts or in its entirety may be found online at: http://www.bloodjournal.org/site/misc/rights.xhtml#repub_requests Information about ordering reprints may be found online at: http://www.bloodjournal.org/site/misc/rights.xhtml#reprints Information about subscriptions and ASH membership may be found online at: http://www.bloodjournal.org/site/subscriptions/index.xhtml Blood (print ISSN 0006-4971, online ISSN 1528-0020), is published weekly by the American Society of Hematology, 2021 L St, NW, Suite 900, Washington DC 20036. Copyright 2011 by The American Society of Hematology; all rights reserved. From www.bloodjournal.org by guest on October 15, 2014. For personal use only. Therapy for Ongoing Graft-Versus-Host Disease Induced Across the Major or Minor Histocompatibility Barrier in Mice With Anti-CD3F(ab‘)2-Ricin Toxin A Chain Immunotoxin By Daniel A. Vallera, Patricia A. Taylor, Angela Panoskaltsis-Mortari, and Bruce R. Blazar A new pharmacologic agent, anti-CDtF(ab‘ I2-ricin toxin A chain (RTA), was synthesized for thepurpose of targeting T cells and as a means of treating established graft-versushost disease (GVHD).The Fc region of anti-CD3 monoclonal antibody (MoAbl was removedt o prevent its abilityt o activate T cells. The resulting F(ab’ l2 fragments wereconjugated t o deglycosylated RTA (dgRTA), a catalytic and potent phytotoxin. The resulting immunotoxin (IT) was potent(greater than 95% inhibition) and selective in inhibiting T-cell mitogenesis in vitro. In vivo, the ITdepleted 80% of l cells in mice receiving bonemarrow (BM) transplants. Transplantation in an aggressive acute GVHD model usingC57BL/6 donor cells and H-2 disparate B1O.BR recipients resultedin an infiltration of CD3-expressing cells and a median survival time (MST) of 20 t o 30 days. A 5-day course of anti-CDSF(ab‘),-RTA (30 p g / d intraperitoneally) beginning 7 days after GVHD induction was beneficial in treating established GVHD in these mice, as evidenced by significantly prolonged survival (MST, greater than 80days), superior mean weight values, and improved clinical appearance. Neither intact anti-CD3, unconjugated anti-CD3 Flab‘ l2 fragments, nor a mixture of antiCD4 and anti-CD8 MoAbs (which are highly effective in prophylactic models) were as effective. F(ab’ lz fragments made from anti-Lyt-l (themurine homologueof human anti-CD51 linked t o RTA were also not effective, despite the fact that both anti-CDtF(ab’ ),-RTA and anti-Lyt-lF(ab’),-RTA had similar half-lives of about 9 hours. The IT also increased MST in two aggressive models of GVHD across non-H-2 minor histocompatibility barriers, indicating that theusefulness of anti-CDBF(ab’),-dgRTA is not limited to a single-strain combination. This agent should be further investigated as an alternative t o current strategies for treating steroid refractory GVHD. 0 1995 b y The American Society of Hematology. G CD5 functions as a T-cell costimulatory molecule recognizing the CD72 molecule on B cells.’’ Thus, MoAbs against CD5” or murine Lyt-l l4 trigger T-cell activation. Our previous studies show that ITS made with intact anti-CD3 MoAb that activate T cells have more nonspecific toxicity than ITS made with F(ab’), ITS that do not activate T cells.15Therefore, in this study, we synthesized a nonactivating IT by removing the Fc region of anti-CD~E MoAb and then linked it to RTA. Several facts indicated that anti-CD3 would be an excellent choice for targeting toxin to target cells. ( 1 ) The CD3 portion of the T-cell receptor (TCR) complex is expressed on all committed cytotoxic T cells and their precursors, and immunohistology studies reported herein show significant increases in CD3-expressing T cells in GVHD-target tissue. (2) Other studies showed that anti-human CD3-RTA effectively inhibited mitogen-activated T cells in vitro.I6 (3) In clinical studies, anti-CD3-RTA plus the potentiator NH4CI, when used to eliminate GVHD-causing T cells from donor RAFT-VERSUS-HOST disease (GVHD) results when donor T lymphocytes react against the organs of the immunosuppressed recipient.‘ It is a significant source of morbidityand mortality after bone marrow (BM) transplantation. Despite advances in preventing GVHD using in vivo chemotherapeutic prophylactic agents, ongoing GVHD is generally difficult to treat and represents a major clinical problem.’.’ Thus, better therapies for GVHD are needed. Although numerous GVHD studies have addressed the topic of prophylaxis, few studies have been directed at studying ongoing GVHD. Thus, we devised mouse models with the express purpose of studying established GVHD. In the model, donor marrow, as a source of stem cells, is mixed with splenocytes, as a source of T cells, and transplanted into H-2 or non-H-2 disparate recipients, resulting in lethal GVHD directed against major (H-2) or minor (non-H-2) histocompatibility disparities. The role of T cells in GVHD in our H-2 disparate model has been established in previous studies4,’ One approach for eliminating GVHD-causing T cells has beentotarget T cells with monoclonal antibody (MoAb) linked to the potent catalytic phytotoxin, ricin toxin A chain (RTA). RTA, the extractable A chain 30-kD component from the toxin ricin (from the plant Ricinis communis), was chosen for these studies because it requires only a single molecule in the cytosol for cell death.6 It is an enzyme with first order/ single hit kinetics that inhibits the 28s RNA component of the 60s ribosome, thereby inhibiting protein synthesis.’ RTA was chemically deglycosylated before conjugation, as studies show that the removal of naturally occurring carbohydrates diminishes nonspecific reactivity without compromising activity.’ The first in vivo studies with immunotoxin (IT) and GVHD therapy involved targeting of the CD5 differentiation antigen inhumans’ and Lyt-l, the murine CD5 homologue.l0.” CD5 is a 65-kD glycoprotein that is broadly expressed on T cells. Transient responses at best were obtained in both models. A problem with this approach may be that Blood, Vol 86. No 11 (December l ) , 1995: pp 4367-4375 From the Section on Experimental Cancer Immunology, Department of Therapeutic Radiology, and the Division of Bone Marrow Transplantation, Department of Pediatrics, University of Minnesota Hospital and Clinics, Minneapolis, MN. Submitted December 22, 1994; accepted July 21, 199.5. Supported in part by US Public Health Service Grants No. ROICA31618, ROI-CA3672.5, POI-CA21737, R01-A13449.5, and POIAI35296 awarded by the National Cancer Institute and the National Institute of Allergy and Infectious Disease, Department of Heatth and Human Services. B.R.B. is a recipient of the Edward Mallinckrodt Jr Foundation Scholar Award. Address reprint requests to Daniel A.Vallera,PhD, Box 367 UMHC, 420 SE Delaware St, Minneapolis, MN 554.55. The publication costsof this article were defrayedin part by page chargepayment. This article must therefore be hereby marked “advettisement” in accordance with IS U.S.C. section 1734 solely to indicate this fact. 0 1995 by The American Society of Hematology. 0006-4971/95/8611-0018$3.00/0 4367 From www.bloodjournal.org by guest on October 15, 2014. For personal use only. 4368 grafts before bone marrow transplantation (BMT), achieved aselective3-logdepletionof CD3-expressingcells and largely prevented lethal GVHD without the need for posttransplant imm~nosuppression.'~ Although it is more difficult tocontrol ongoing GVHDin vivo, these in vitro findings wereencouraging.(4)Anti-CD3-RTAwas morerapidly andcompletely internalized ascompared with anti-CDSRTA and anti-CD2-RTA." In a different study in which internalization wasmeasured withradionucleotide-labeled antibodies, anti-CD3 -RTA was internalized faster than antiCD5-RTA,anti-CD4-RTA,oranti-CD8-RTA." ( 5 ) In mice, studies have confirmed that anti-CD3-RTA or antiCD3F(abr),-RTA can be administered in vivo and eliminate the CD3+ cells responsible for BMgraft rejection, resulting in an overall promotion of long-term BM engraftment.'' (6) Anti-human CD3 has also been conjugated to intact diphtheria toxin" or to the diphtheria-binding site mutant CRM9,2' resulting in selective and potent ITS. In the current study, we show that anti-CD3 F(ab'),-RTA has a depletionary effect on CD3-expressing cells in vivo, and in amodelof aggressiveongoingGVHD, thatantiCD3F(ab'),-RTA is more effective than unconjugated antiCD3F(ab'), or anti-Lyt-IF(ab'),-RTA IT in the treatment of lethal GVHD inducedby major orminor antigen disparate BM transplants. VALLERA ET AL Phytohemagglutinin (PHAJ a s s y ~ s . PHA mitogenassays were performed as described." BMT. Our transplant protocol has been described in detail." B 10.BR recipients were conditioned with 8.0 Gy total body irradiation (TBI) administered from a Philips R T 250 Orthovoltage Therapy Unit (PhilipsMedicalSystems,Brookfield, WI) filtered through 0.35-mm Cu at a final absorbed dose rate of 0.41 Gylmin at 225 kV and I7 mA. Donor BM was collected into RPMI 1640 medium by flushing it from the shafts of femurs and tibias. Single-cell suspensions of donor splenocytes (as a source of GVHD-causing T cells) were obtained by passing minced spleens through a wire mesh and collecting them into RPMI 1640. Splenocytes were suspended with BM at a concentration of 108/mL,and 0.5 mL, containing 25 x 10" BMcellsplus 25 X IO" splenocytes,wasinfusedintothecaudal vein. As an additional control, some recipients received donor splenocytes that were depleted of T cells before BMT with anti-Thyl.2 + C'' ' (hybridoma 30-H-12, a rat IgG2b, provided by Dr Ledbetter). Pathologic examination of tissues. Mice were lulled and autopsied,andtissuesweretakenforhistopathologicanalysisasdescribed."' OrganswerescoredpositiveforGVHD if there was lymphocytic infiltrate with or without single-cell necrosis (skin. colon), crypt dropout (colon), periportal infiltrate with acute necrosis (liver), or endothelialitis with a lymphocytic infiltrate (lung). These features were present only in mice with active GVHD and not in normal mice or in irradiated recipients of syngeneic BMTs. Flow cytometv analysis. MoAbs were directly labeled with biotin, fluorescein isothiocyanate (FITC), or phycoerythrin (PE) as previously described.I5 Single-cell splenocyte preparations were suspended in buffer (phospbate-buffered saline [PBS] + 5% colosMATERIALS ANDMETHODS trum-free bovine serum + 0.015% sodium azide). Pelleted cells were incubated for 15 minutes at 4°C with 0.4 p g of an anti-Fc receptor Mice. BIO.BR/SgSnJ (H-2k,Mlslb/2b),C3H/HeJ (H-2', MIS MoAb (clone 2.462, provided by Dr Jay Unkless, Rockefeller Unilb/2a),CBA/J(H-2k, MIS ld2a), B10.D2(H-2d, MIS lb/2b),and versity, New York. NY) to prevent Fcbinding.*' Optimal concentraDBA-2J (H-2d,MIS l d 2 a ) mice were purchased from Jackson Labotions of directly conjugated (biotin-. PE-. or FITC-labeled) MoAb ratory (BarHarbor,ME).C57BL/6(H-2b)micewerepurchased were added to a total volume of 100 to 130 p L , and the mixture through the Frederick Cancer Research and Development Center, wasincubatedfor 1 hourat 4°C. For thebiotin-labeledMoAb, NationalCancerInstitute(Frederick,MD).Donorsandrecipients fluorescence was indirectly measured by adding streptavidin-labeled were females. Donors were 4 to 6 weeks old, and recipients were 8 1 hourat Red 613(GIBCO,GrandIsland,NY)foranadditional to 10 weeks old at the time of BMT. The C57BL/6 and BIO.BR donodhost strain combination are mismatched at the H-2 major his- 4°C. After final washing, cells were fixed in I % paraformaldehyde. ThefollowinglabeledMoAbsand reagents, obtainedfromPhartocompatibility complex (MHC) and at several minor antigen loci. Mingen (San Diego, CA) unlessotherwiseindicated,were used: The Bl0.BR and CBA donorhost strain combination are matched anti-CD3c (clone 145-2C11, hamster IgG), anti-CD8 (clone 53-6.72, at H-2', but not atthe MIS minorantigen loci. TheB10.D2and rat IgGZa, provided by Dr Ledbetter)," anti-CD4 (clone GK1.5, rat DBA-2 donorhost strain combination are matched at H-2d, but not IgG2b),anti-NKI.1(clonePK136,mouse IgGZa, provided by Dr at the Mls minor antigen loci. Gloria Koo, Rahway, NJ)," and an irrelevant rat IgG2b anti-human Reagents. Anti-CD3 is ahamster IgG MoAbproducedfrom antibody (clone 3Ale).'x All samples were analyzed on a FACscan hybridoma 345-2C1 I and was generously provided by Dr Jeffrey (BectonDickinson,PaloAlto, CA) usingconsort-30software. A Bluestone (University of Chicago, Chicago, IL).It is reactive against minimum of 20,000 events were examined. Background subtraction the CD3 epsilon component of the murine TCR2* and was purified usingadirectlyconjugatedirrelevantantibody control was perby ammonium sulfate precipitation followed by ion exchange chroformed for each sample. matography on DE52 (Whatman, Hillsboro, OR). F(ab')* fragments Radioiodinafion. The labeling of IT with iodine-l 25 (lz51) was were prepared as previously described' by incubating antibody at performed using Iodo-beads according to the manufacturer's speci37°C for 90 minutes with a 1 :100 ratio of pepsin (Sigma Chemical fications (Pierce, Rockford. 1L) and an adaptation of the method first CO, St Louis, MO) to antibody in 0.1 m o l L citrate buffer, pH 3.9. described by Markwell.'" A 20% loss of protein content during the The reaction was halted with the addition of 3.0 m o l L tris-HC1 (pH 8.6), and the mixture was dialyzed against borate-buffered saline, pH labeling procedure was assumed, based on previous studies, and all concentrationswereadjustedusing this value. Over82% of the 8.5. The F(ab'), fragments were purified on a protein A-Sepharose countsoflabeledantibodywereprecipitablewithtrichloroacetic column.*' ITwasproduced by linkingthe purified fragmentsto acid. deglycosylated RTA (dgRTA; Inland Laboratories, Austin, TX) usBlood clearance of "'I-labeled IT. Blood clearance was detering N-succinimidyl-3-(2-pyridyldithio)propionate(SPDP),asdemined as previously reported.'" Between 0.17 hours and 72 hours scribed in detail elsewhere."' An anti-Lyt-1F(ab')2-RTA conjugate afterinjectionintravenously(IV) of 20pCiradiolabeled IT, five was prepared similarly. Anti-Lyt-I from clone 53-7.313 (rat IgG2a) was provided by Dr Jeffrey Ledbetter, Bristol-Meyer Squibb, Seattle, C3WHeJ mice in each group were anesthetized and bledby retroor(25 WA.' ' An irrelevant control IT was prepared from irrelevant hamster bital venipuncture at nine different time points. Whole bloodpL) was aliquoted from each animal and countedin a liquid scintillation fragments (Rockland Laboratory, Gilbertsville, PA) linked to counter. Triplicate samples of the original injection standard were dgRTA. From www.bloodjournal.org by guest on October 15, 2014. For personal use only. 4369 ANTI-CD3F(ab‘)2IMMUNOTOXIN FOR GVHD THERAPY Table 1. Specific Activity of Anti-CDBF(ab‘)t-RTA Against PHA-ActivatedMurine T Cells CD3F(ab‘)2-RTA CD3F(ab‘)>-RTA + 300 pg CD3F(ab’), Hamster F(ab’h-RTA 53.6 2 14.8 -t 14.9 21.1 5 3.2 2.7 2 0.4 64.1 2 10.1 65.4 f 3.6 59.5 2 2.2 42.8 f 18.6 43.2 f 8.9 56.8 2 5.2 59.6 2 3.5 48.0 2 18.6 Concentration (pglmL) 0 50.40.1 1 10 Mouse splenocytes were incubated with IT for four hours at 37°C. For blocking studies, cells were treated with 300 pg/mLunconjugated anti-CD3F(abf),for 30 minutes before addition ofIT. After treatment, cells were washed, and PHA was added. After 3 days, cells were pulsed with tritiated thymidine and harvested. Data are presented as cpm x lo-’ f one SD unit. counted at the same time as tissues, allowing the determination of the activity in tissue as a percentage of the injected dose, corrected for the physical decay of the radionucleotide. The individual values for the animals in each group were averaged for each time point. The logarithms of the averages of the percentage of injected dose per milliliter were plotted over the time after treatment. Linear regression by a least squares method yielded a straight line, allowing an estimation of the biologic half-life of the radiolabeled antibodies. Biodistribution studies. C3wHeJ mice (n = 5 ) were given intraperitoneal (IP) injections of 2 pCi of ‘ZSI-labeledIT. The animals were killed 48 and 72 hours after injection of radiolabeled antibodies. The spleen and thymus were removed and counted. Tissues were counted on a Beckman 5500 gamma counter (Beckman, Arlington Heights, IL)with a ‘*’I window. Statistical analyses. Group comparisons of continuous data were performed using Student’s t test. Survival data were analyzed by lifetable methods using the Mantel-Peto-Cox summary of X’.’’ Probability (P)values less than .OS were considered significant. RESULTS IT composition. Purity of the IT was assessed by sodium dodecyl sulfate-polyacrylamide gel electrophoresis (SDSPAGE) as de~cribed.~’Both anti-CD3F(ab’),-RTA and anti-Lyt-lF(ab’),-RTA were heterogeneous, consisting of one, two, or three toxin molecules linked to F(ab’),, but the 1:1 species generally predominated (data not shown). Less than 13% unconjugated F(ab’), was present after purification, but no free toxin was detected. Inhibitory effect of anti-CD3F(ab1),-RTA on mouse splenocytes in vitro. To determine whether antiCD3F(ab’),-RTA selectively inhibited mouse T cells, C57BL/6 splenocytes were preincubated with antiCD3F(ab’),-RTA for 4 hours at concentrations of 0, 0.1, I , and 10 p&mL (Table 1). Inhibition of PHA-induced activation was dose-dependent, and at 10 pg/mL, counts per minute (cpm) were reduced 95% (2.7 x lo” as compared with 53.6 X lo3 in the untreated control) without the benefit of IT potentiators. Two control groups showed specificity: (1) The addition of 300 pg/mL unconjugated anti-CD3F(ab’), blocked the inhibitory effect of anti-CD3F(ab’),-RTA. (2) An irrelevant control polyclonal hamster antibody conjugated to dgRTA did not inhibit PHA activation. Depletionary effects of anti-CDJF(ab’)*-RTA. To determine whether anti-CD3F(abf),-RTA had a depletionary effect, C57BL/6 mice were irradiated and then given synge- neic BMTs to avoid complications of the sometimes immunosuppresive nature of GVHD occurring in allogeneic transplants. We studied the ability of anti-CD3F(abf),-RTA to deplete CD3+ cells (Table 2). Irradiation was given on day -1. Syngeneic BM and a single dose of anti-CD3F(ab’)*RTA were given on day 0. On day 2, mice were killed and splenocytes studied by flow cytometry. Mice given 400 pg unconjugated anti-CD3F(ab1), had 0.05 X lo6 CD3+ cells in the spleen, while mice given less than half that dosage of anti-CD3F(ab’),-RTA had 2.5-fold fewer CD3’ T cells. Compared with PBS-treated controls, mice given antiCD3F(ab‘),-RTA had about fivefold fewer CD3’ cells (a reduction of 82%). These findings show the depletionary effect of anti-CD3F(abf),-RTA as compared with antiCD3F(ab’), in the BMT setting. Anti-CD3F(ab’),-RTA treatment resulted in the same number of NK1.1+ cells as in the PBS control group, further indicating that antiCD3F(ab’),-RTA selectively depleted CD3-expressing cells. A significant reduction in these CD3’ T cells (42%) was still observed in anti-CD3F(abf),-RTA-treated mice at even 14 days postinjection of IT. A depletionary effect of anti-CD3F(abf),-RTA was also observed in normal mice, where a significant inhibition of both CD4-expressing and CD8-expressing cells was observed (data not shown). Effect of ar~ti-CDjlF(ab’)~-RTA on ongoing GVHD across the H-2 barrier. To determine whether anti-CD3F(ab’),RTA could inhibit established GVHD across the H-2 barrier, B1O.BR mice were given 8 Cy total body irradiation (TBI) and then transplanted with 25 X lo6 C57BL/6 BM cells and 25 X IO6 splenocytes. In situ studies showed that at day 9 after BMT, there is a dramatic infiltration of CD3-expressing lymphocytes observed in the colon of these mice (data not shown). No such cells were observed in controls given BM grafts without GVHD-causing splenocytes. Treatment with anti-CD3F(ab’),-RTA was initiated a week after GVHD induction to permit a graft-versus-host reaction before treatment. Mice were givendaily IP injections of 30 pg IT beginning on day 7 and continuing through day 11. Figure 1A shows that anti-CD3F(ab’),-RTA-treated mice had a median survival time (MST) of greater than 80 days. At 3 months posttransplant, 22% of the animals were still surviving. In contrast, control PBS-treated animals had an MST Table 2. Depletionary Effect of Anti-CDBF(ab’),-RTA on Mice Undergoing Syngeneic BMT CD3’ Cells by Flow Cytometty Treatment 96 Positive PBS 0.1 400 pg anti-CDJF(ab’), 150 pg anti-CD3F(ab’)?-RTA anti-Thyl.2 0.18 + C’ (in vitro) 36 27 9 25 Absolute Cell Count IXlO-’) 1 0.05 0.02 ~~~ ____ C57BU6 mice were given 9 GyTB1 on day -1 and 1 day later were given a syngeneic BMT with 15 x 10’ C57BU6 BM cells and 15 x 10’ splenocytes. Different groups (n = 3 per group) were given IP injections of PBS, 400 pg anti-CD3F(ab‘)2once on day 0, or 150 pg antiCD3F(ab’),-RTA once on day 0. One group wasgiven BM mixed with T-cell-depleted splenocytes. Splenocytes were harvested on day 2 and examined for CD3’ cells by flow cytometry. From www.bloodjournal.org by guest on October 15, 2014. For personal use only. 4370 VALLERA ET AL I anti-Thyl.2+C’ l ! T Ap~yi-CD3F(:”-RTA p ,001 compared to PES anti-CD&anti-CDB 0 B 3 22 Fig1. The in vivo effect ofanti-CDBF(ab’),-RTA injections on establishad GVHD induced across the MHC barrier in B10.M recipients of C57Bt.16 grafts. Irradiated (8 Gyl recipientswere given bone marrow andspleencells (25 x 10’ ofeach).Onegroup of mice received donorBM that was depletedof Tcells using anti-Thyl.2 C‘ before BMT. Groups were injectedon days7 through 11with PES, 50 p g l d antiCDBF(ab’), fragments, or 30 pgld anti-CD3F(ab’)2RTA. The remaining groups were given a single injection of 400 p g of intact anti-CD3 or 400 p g of antiC M (clone GK1.5) plus anti-CD8 (clone 2.43) on day 7. (A) Survival is plolted in an actuarial manner (n = 8 per group). (B) Mean weight curves are shown for the same mice. The course of injection of anti-CD3 F(ab’),-RTA is indicated by the bar. + Days Post Transplant of only 20 days, and none survived beyond 45 days postBMT. Treatment with 50 pg ar1ti-CD3F(ab’)~X 5 days on days 7 through 11 (250 pg total) did not result in significant protection against GVHD. Treatment with 400 pg of intact CD3 on day 7 resulted in a characteristic high percentage of early mortality (MST, 8 days) due to the activation of T cells and toxic side effects of anti-CD3 treatment, aspreviously reported.” Transient and nonsignificant protection from GVHD was noted when a combination of 400 pg antiCD4 and anti-CD8 MoAbs was administered on day 7. As a positive control, T cells were eliminated from the donor grafts before BMT using anti-Thy 1.2 plus complement in one group of animals. Eighty-eight percent of these mice were survivors on day 90, indicating that elimination of all donor T cells can prevent GVHD mortality in this model. We also studied the effects of an irrelevant control hamster F(ab’)2-RTA in a separate experiment using the exact dose and schedule for GVHD therapy as with anti-CD3F(ab’)zRTA (data not shown). No extension of MST was observed. Collectively, these findings indicate that anti-CD3F(ab‘)2RTA is potent and specific in its ability to inhibit an ongoing GVHD response across a full MHC disparity. To select the dayof GVHD treatment initiation, we identified the onset of GVHD in the mice shown in Fig 1A by monitoring weight loss over time. Our data in Fig 1B show that the first detectable GVHD occurred on days 7- 11. However, after an initial decline, weights of mice treated with anti-CDSF(ab’)*-RTA stabilized and remained around 18 g for the duration of the experiment. More precipitous drops in weight were noted in mice with higher GVHD mortality. These groups included mice treated with control PBS, antiCD3F(ab’)2 alone, or a combination of anti-CD4 plus antiCD8 MoAbs. Only the group of mice in which T cells were eliminated from the donor graft before BMT with antiThyl.2 plus complement underwent a steady increase in weight over the 76-day interval. These findings indicated that although anti-CD3F(ab’),-RTA inhibited GVHD, it was still present in these treated mice. From www.bloodjournal.org by guest on October 15, 2014. For personal use only. 437 1 ANTI-CD3F(ab‘)z IMMUNOTOXIN FOR GVHDTHERAPY Table 3. Effect of Various Dosages of Anti-CD3F(ab)2-RTA on Established GVHD Treatment PBS Anti-CD3F(ab’)z-RTA Anti-CD3F(ab’)?-RTA Anti-CMF(ab’)z-RTA Anti-CDJF(ab’)z-RTA Anti-CDBF(ab’),-RTA Anti-CD3 C‘ Anti-Thyl.2 + Dose (pg/d) - Schedule d 7-11 10 30 50 75 d 7-11 12’ d 7-11 d 7-11 d 7-11 400 + 25 d 7-11 400 d 7 only vitro In - MST (d) 26 36 42* 34 22 18 9 >76* % Actuarial Survival Rate at Day 60 0 0 0 0 0 0 100’ B1O.BR recipients were given lethal TB1 (n = 8 per group) on day -1, and on day 0 were transplanted with C57BU6 BM and spleen cells (25 x 10‘ of each). On day 7, mice were given a 5-day course of various concentrations of anti-CDBF(ab’),-RTA or unconjugated antiCDBF(ab’), fragments, or a mixture of unconjugated anti-CD3F(ab’)z fragments plus unconjugated RTA.One group was given a single and spleen injection of 400 pg anti-CD3. Another was given donor BM cells that were treated with anti-Thyl.2 C’ before BMT. Survival was monitored. * P < .05 compared with PES control. + Tissues from mice in the same experiment that were treated with unconjugated anti-CD3F(abr)2, anti-CD4 plus anti-CD8, or intact anti-CD3 and that were morbid between day 19 and day 39 were collected immediately before death (n = l or 2). Tissues were embedded in paraffin, blocked, sectioned, and stained with hematoxylin and eosin for histopathologic examination. All mice showed evidence of colonic GVHD including infiltrates and tissue necrosis. Two mice treated with anti-CD3F(abr),-RTA that survived were killed on day 90 post-BMT. These mice showed positive signs of GVHD in the colon, liver, and lung. Infiltrates and tissue necrosis were the most prominent features. Effect of varying dosages of anti-CD3F(ab’)2-RTA on ongoing GVHD across the H-2 barrier. In a different experiment, B 1O.BR recipients given C57BL/6 BM and spleen were treated with increasing concentrations of antiCD3F(ab’),-RTA (Table 3). Mice given control PBS had an MST of 26 days, similar to the previous experiment, and died of GVHD. MST was increased to 36 days in mice given a 5-day (days 7 through 11) course of 10 pg per injection anti-CD3F(abf),-RTA and to 42 days in mice given a course of 30 pg per injection anti-CD3F(abr),-RTA. However, MST decreased when the dosage was increased to 50 or 75 pg per injection. A group of control mice given a 5-day course of 400 pg unconjugated anti-CD3F(ab‘), plus 25 pg unconjugated RTA showed no protective effect from GVHD onset. A group of mice given anti-CD3 had an MST of only 9 days. Positive controls in which T cells were eliminated before transplant with anti-Thyl.2 plus complement in vitro had an MST of greater than 76 days. Using these data, we selected the dose of 30 pg per injection anti-CD3F(ab‘),RTA for subsequent studies. Our findings on the effectiveness of the IT were reproducible, and we established a working dose and schedule. Effect of anti-CD3F(abt),-RTA in protecting against es- tablished GVHD across non-H-2, minor histocompatibiliry barriers in two Afferent mouse models. To determine whether anti-CD3F(ab’),-RTA could be used to treat GVHD generated across non-H-2 minor histocompatibility antigen disparities, CBA mice were given 8 Gy T B 1 and then 20 X lo6 T cell-depleted, H-2-matched B1O.BRBM cells and 50 X lo6splenocytes (twice the splenocyte number used in the C57B46 into BlO.BR model). Table 4 shows that anti-CD3F(abr),-RTA treatment significantly extended the MST from 18 days in PBS controls to 46 days in ITtreated mice. Daily weight measurements showed that antiCD3F(ab’),-RTA enhanced the anti-GVHD effect compared with untreated controls, but that GVHD-related weight loss still occurred later (data not shown). Whereas GVHD generation in the mismatched C57BL/6-into-B10.BR model is CD4+ T cell-dependent, GVHD in this minor model is CD8+ T cell-dependent, indicating that this agent was active against both types of T cells.34 In a separate experiment ina different modelinwhich minor antigens are mismatched, DBN2 recipients given 8 Gy TB1 and 20 X lo6T cell-depleted B10.D2 BM cells and 50 X lo6 splenocytes developed GVHD. The MST was 21 days in a group of mice given control PBS injections. AntiCD3F(ab’),-RTA significantly extended the MST to 34 days in this minor mismatched model. Weight loss data indicated that the mice that died did undergo GVHD-related weight decline (data not shown). In both of these models, in vitro depletion of T cells from donor grafts before BMT resulted in an MST of greater than 83 days, with 100% of the animals surviving at day 60. Collectively, these findings show that anti-CD3F(abr),-RTA is notonly effective against lethal GVHD induced across the major histocompatibility barrier, but is also effective against GVHD in aggressive models in which minor antigens, and not major antigen differences, serve as targets for lethal GVHD. The data also Table 4. In Vivo Effect of Anti-CD3Flab)z-RTA Injections on Established GVHD Induced Acrossthe Minor Histocompatibility Barrier in Two Ditferent Strain Combinations Treatment E1O.BR into CBA PBS Anti-CD3F(ab‘)z-RTA Anti-Thyl.2 + C’ B10.D2 into DBA-2 PBS Anti-CDJF(ab‘)p-RTA 30 Anti-Thyl.2 C’ + Dose Idd) MST Id) % Survival at Dav 60 d 7-11 d 7-11 - vitroIn 18 46’ >85* 0 20s 100’ - 21 34* >83* Schedule - 30 d 7-11 d 7-11 - vitroIn 0 0 loo* BMTs were performed with two strain combinations. First, CBA recipients (n = 10 per group) were given 8 Gy lethal TB1 on day -1, and on day 0 were transplanted with 20 x lo6 B1O.BR BM cells and 50 x 10‘ spleen cells. On day 7, mice were given a 5-day course of anti-CDfF(ab’),-RTA or control PES. Another group was given donor BM and spleen cells that were treated with anti-Thyl.2 + C‘ before BMT. Survival was monitored. A second experiment was performed identically, except B10.D2 BM and splenocytes were transplanted into irradiated DBA-2 recipients (n = 10 per group). P < .05 compared with PBS control. From www.bloodjournal.org by guest on October 15, 2014. For personal use only. 4372 VALLERA ET AL Table 5. Effect of Anti-Lyl-F(ab’),-RTA on Established GVHD in the Mismatched C57BL/G-lnto-BlO.BR Model Dose MST (d) Treatment (pg/dl PBS - 7-11d 21 Anti-Lyl-F(ab’kRTA Anti-human CD5-RTA 30 30 30 20 25 Anti-CD3F(abf),-RTA Schedule 7-11d d 7-11 7-11d 77” % Actuarial Survival Rate at Day 60 0 0 0 62* B1O.BR recipients (n = 8 per group) were given lethal TB1 on day -1, and on day0 were transplanted withC57BU6 BM andspleen cells (25 x I O 6 of each). On day7, mice were given a 5-day course of PBS, anti-Lyl-F(ab’)2-RTA, anti-CD3F(abr),-RTA, or a control anti-human CD5-RTA. Survival was monitored. * P < .01 compared with PBS control. show that anti-CD3F(abr),-RTAisactive in models in which CD8+ T cells play a major role. EfSect of anti-Lyt-lF(ab’),-RTA on ongoing GVHD induced across the H-2 MHC barrier. As anti-LytlF(ab’),-RTA is the murine equivalentof anti-human CD5RTA currently used in clinical trials, we directly compared anti-Lyt-lF(ab’),-RTA and anti-CD3F(abr),-RTA for their efficacies in treating ongoing GVHDin the same experiment. Table 5 shows that anti-Lyt-lF(ab’),-RTA given in a5-day course did not result in asignificant anti-GVHD effect in B 1O.BR recipients of C57BL/6 BWspleen.In contrast, a 5-day course of anti-CD3F(ab’),-RTA significantly increased MST to day 77, as compared with day 21 in controls. Anti-human CD5-RTA, a noncrossreactive control IT, did not inhibit GVHD. To determine whether the failure of anti-Lyt-lF(ab’),RTA as opposedto anti-CD3F(ab‘),-RTA to protect against GVHD was related to IT potency or perhaps to a difference in the clearance of the two proteins in vivo, we performed additional studies. Pharmacokinetic studies showed that the serum half-lives of anti-Lyt-lF(ab’),-RTA and anti-CD3F(ab’),-RTA were similar (8.9 and 9.0 hours, respectively) in normal B10.BR mice. Both ITS accumulated in a similar manner in the spleen and thymus. In contrast, the abilities of these two ITS to inhibit T-cell proliferation in PHA assays were different, because the 50% inhibition concentration (I(&) of anti-Lyt-lF(ab’),-RTAwas10.2 pg/mL and the ICs0 of anti-CD3F(abf),-RTA was 2.1 pg/ mL when compared in the same assay without the addition of any potentiators. Collectively, these findings suggest that the failure of anti-Lyt-IF(ab’),-RTA to inhibit GVHD is more likely related to an issue of potency of the IT, rather than clearance and localization. second A anti-Lyt1F(ab’)2-RTA was prepared using another MoAb, SK69.6.38 generously provided by Dr Edward Boyse (Memorial Sloan-Kettering Cancer Center, New York, NY) and findings were identical. DISCUSSION Ongoing GVHD is acknowledged asa significant clinical problem and few murine studies have been directed at studying ongoing GVHD. The majorfinding of thisstudy was that antiLCD3F(ab’),-RTA extended MST in major and minor antigen-mismatched BMT recipients with established GVHD longer than any other IT thus far reported. MST was also extended in two additionalmodels of lethal GVHD where donors and recipients were disparate at minor antigen loci only. The effects of anti-CD3F(ab’),-RTA were specific, because flow cytometry studies on mice given syngeneictransplants [to studytheeffects of anti-CD3F(ab’),RTA in the absence of the immunosuppressive effects of allogeneic transplants] revealed that anti-CD3F(abr),-RTA was selectively depletionary in its effect on CD3-expressing T cells, butnot on cells expressing the unrelated NK 1.1 marker. An irrelevant IT control, hamster CD3F(abf)?-RTA, did not extend MST. Previous studies usingmiceindicatedthat effectiveIT could be synthesized using anti-CD3 MoAb totarget T cells, but only if we inhibited the ability of the MoAb to trigger T-cell activation through the removal of the Fc region.” ITS made with activating, intact anti-CD3 caused a high mortality rate and a precipitous release of inflammatory cytokines. In fact, therapy with anti-CD3 alone has shown potential for preventingorgangraftrejection, but has been limited by toxic side effects due to in vivo activation of T cells induced by ligation of the TCR and theFc region of anti-CD3.3”.35~”X ITS made with nonactivating anti-CD3F(ab’), did not cause cytokine release, were less toxic to nontarget organ systems, deleted CD3-expressingT cells, and prevented BM rejection in vivo. Evaluation of anti-CD3F(ab’)>-RTAand antiCD3-RTA in the same invitro PHA experiment showed that anti-CD3F(ab’)2-RTA is more potent.” Previous studies have demonstrated that ITS made with F(abO2 are more potent than ITS made with intact antib~dy.’”~” However, this is not always the~ a s e . ~ Collectively, ”~’ these studies indicate that certain F(ab’),-ITS such as anti-CD3F(ab’),-RTA may have advantages. We believed that itwas important to addressthe activation issue in these studies. CD5 interacts with costimulatory moleculeCD72 onantigen-presentingB cells.” Anti-CD5 MoAb triggersactivation of CD5-expressing humanT cells.” Likewise anti-Lyt-1 triggers murine T cells toproliferate.“ Thus, we prepared nonactivating anti-LytI.2F(abf),-RTA and compared it with anti-CD3F(ab’ )?RTA in the same experiment. The same RTA was used to prepare both reagents to ensure consistency of the toxic moiety of the ITS. Although the clearance andbiodistribution of thetwo agentsweresimilar, anti-CD3F(abf),-RTA was more effective in treatingestablished GVHD.Onefactor that correlatedwith thesuperior in vivoactivity of antiCD3F(abf),-RTA was its superior fivefold in vitro potency measured by PHA assay. We concluded that preparation of anti-Lyt-IF(ab‘)*-RTA provided no advantage. Then why was CD3 more effective than CD5 as a target molecule?Thereare severalpossibleexplanations. (1) In addition to the previously discussed studies in which antiCD3-RTA was morecompletelyand rapidlyinternalized than anti-Lyt- 1-RTA,”.” other subcellular compartmentalization studies inwhich anti-CD5-RTA wasradiolabeled andthendirectlymeasured in organelle fractions isolated from Percol gradients show that anti-CD5-RTA IT is rapidly From www.bloodjournal.org by guest on October 15, 2014. For personal use only. 4373 ANTI-CD3F(ab')2 IMMUNOTOXIN FOR GVHDTHERAPY transported to the lysosome, where unwanted degradation takes place.44 ( 2 ) Anti-CD5 IT permits the expansion of GVHD-causing T cells, which do not express CD5. Studies show that a large proportion of T lymphocytes lack CD5 expression after BMT?5346When human BM cells from GVHD patients were treated with an antiCD5 IT and then cultured in vitro for 16 days, CD5-negative T cells mostly expressing CD3 were detected. CD5-CD3+ cells that escape IT treatment retain an alloreactive cytotoxic repertoire capable of GVHD reaction?' These results with anti-CD3F(abf),-RTA are the best that have been attained in several published studies dealing with the treatment of ongoing GVHD in the same mismatched mouse model of allogeneic BMT.'0,30,48 Anti-Lyt-l antibody linked to RTA" or labeled with r a d i o n ~ c l i d ewas ~ ~ only partially protective. Attempts to treat established GVHD using the potent anti-T cell drug rapamycin?' a fungal macrolide, also produced transient protection. Allof these murine studies and the clinical studies resulted in significant but transient anti-GVHD effects. The lack of complete inhibition of GVHD during the efferent phase rather than the afferent phase indicates that it is far more difficult to inhibit GVHD once an alloresponse is initiated in vivo. This could be attributed to the difficulty of effectively delivering therapy to a relatively small GVHDcausing population of cells in a complex biologic environment. Alternatively, a network of cells may be involved in GVHD once the process has begun, thus making specific targeting difficult. Protection was more limited when mice were transplanted with BM with minor antigenic disparities because minor histocompatibility antigen differences sometimes can be even more potent at eliciting GVHD responses than fully mismatched MHC differences, because different mechanisms of GVHD may be operative in the two different systems34or because we gave higher numbers of donor T cells in the minor model. This is a topic of future investigation. The difficulty in inhibiting ongoing GVHD is evidenced by our results with anti-CD3F(abf)2 fragments alone. In past studies, we showed that unconjugated anti-CD3F(abr), fragments can be used prophylactically to prevent GVHD. In these current studies, anti-CD3F(abf), fragments were much less effective when compared with anti-CD3F(ab'),-RTA in treating established GVHD. Fragments given on day 7 post-BMT did not inhibit established GVHD in this model. This could be explained by the flow cytometry studies, which showed that anti-CD3F(ab'), fragments caused the modulation of CD3 from the cell surface of the T cells and only partial T-cell depletion. In contrast, the anti-CD3F(ab'),RTA, which was much more effective against ongoing GVHD in the present study, caused the deletion of CD3+ T cells. The internalization of anti-CD3F(ab'),-RTA eliminated the GVHD-causing cells. Whereas modulation may be an effective means of GVHD prophylaxis, it is better to delete T cells to treat GVHD once the response has been initiated. Although we have achieved a high degree of protection against ongoing GVHD with IT, we have not cured the mice, as evidenced by late onset of the disease. To further extend MST with ~ I I ~ ~ - C D ~ F ( ~ ~ ' ) ~it -may R T Abe, necessary to combine itwith other ITS or approaches such as d r ~ g s . 4 ~ Some reasons that anti-CD3F(ab'),-RTA is not fully protective are as follows. (1) Inadequate dosing and schedule may have resulted in incomplete elimination. This has been a serious limitation to the clinical use of IT, as clinical studies to date have mostly been limited by vascular leak syndrome and hepatotoxicity. However, we hope that a more thorough understanding of IT toxicity and agents that might diminish their toxicity will be of future help. ( 2 ) Immunohistology studies show that other donor cells, such as macrophages and natural killer cells, may play some role in established GVHD in this model (unpublished data, January 1995). Perhaps even greater anti-GVHD effects might be achieved by targeting these cells as well. (3) Antibody responses may develop against the antibody or toxin component of IT. Although several immunoglobulin responses have been noted in clinical trials:' it is likely that optimal doses of anti-T cell IT will not only target GVHD-causing cells, but also might inhibit the development of immunoglobulin responses, as these responses are also T cell-dependent. REFERENCES I . Korngold R, Sprent J: T cell subsets and graft-versus-host disease. Transplantation 44:335, 1987 2. Weisdorf D, Haake D, Blazar BR, Miller W, McGlave P, Ramsya NR, Kersey J, Filipovich A: Treatment of moderatekevere acute graft-versus-host disease following allogeneic bone marrow transplantation: An analysis of clinical risk factors and outcome. Blood 75:1024, 1990 3. Martin PJ, Schoch G, Fisher L: A retrospective analysis of therapy for acute graft-versus-host disease: Initial treatment. Blood 76: 1464, 1990 4. Blazar BR, Taylor PA, Snover DC, Bluestone JA, Vallera DA: Non-mitogenic anti-CD3F(ab')* fragments inhibit lethal murine graft-versus-host disease induced across the major histocompatibility barrier. J Immunol 150:265, 1993 5 . Blazar BR, Taylor PA, Vallera DA: In vivo or in vitro antiCD3 epsilon chain monoclonal antibody therapy for the prevention of lethal murine graft-versus-host disease across the major histocompatibility banier in mice. J Immunol 152:3665, 1994 6. Olsnes S, Pihl A: Abrin, ricin, and their associated immunoglobulins, in Cauatrecasas P (ed): Receptors and Recognition, series B. The Specificity and Action of Animal, Bacterial, and Plant Toxins. New York, NY, Chapman and Hall, 1976, p 129 7. Endo Y, Mitsui K, Motizuki M, Tsurugui K: The mechanism of action of ricin and related toxic lectins on eukaryotic ribosomes. J Biol Chem 2625908, 1987 8. Thorpe PE, Wallace PM, Knowles PP, Relf Mg, Brown ANF, Watson GJ, Blakey DC, Newel1 DR: Improved antitumor effects of immunotoxins prepared with deglycosylated ricin A-chain and hindered disulfide linkages. Cancer Res 48:6395, 1988 9. Byers VS, Henslee J, Keman N, Blazar BR, Gingrich R, Phillips GL, Lemaistre CF, Gilliland G, Antin JH, Vogelsang G , Martin P, Tutschka PJ, Trown P, Ackerman SK, O'Reilly RJ, Scannon PJ: Use of anti-pan T lymphocyte ricin A chain immunotoxin as targeted immunotherapy in steroid resistant acute graft-versus-host disease. Blood 75:1426, 1990 10. Vallera DA, Carroll SF, Snover D, Carlson GJ, Blazar B R Toxicity and efficacy of anti-T-cell ricin toxin A chain immunotoxins in a murine model of established graft-versus-host disease induced across the major histocompatibility barrier. Blood 77:182, 1991 11. Ledbetter JA, Rouse R, Spedding-Micklem H, Herzenberg L: From www.bloodjournal.org by guest on October 15, 2014. For personal use only. 4314 T cell subsets defined by expression of Lyt-l, 2, and 3 and Thy-l antigens. J Exp Med 152:280, 1980 12. Van de Velde H, von Hoegen I, Luo W, Parnes JR, Thielemans K: The B-cell surface protein CD72Lyb-2 is the ligand for CDS. Nature 351:662, 1991 13. Imboden JB, June CH, McCutcheon MA, Ledbetter JA: Stimulation of CD5 enhances signal transduction by the T cell antigen receptor. J Clin Invest 85:130, 1990 14. Hollander N: Immunotherapy of lymphoid and nonlymphoid tumors with monoclonal anti-Lyt-l antibodies. J Immunol 133:2801, I984 15. Blazar BR, Hirsch R, Gress R E , Carroll SF, Vallera DA: In vivo administration of anti-CD3 monoclonal antibodies or immunotoxins in murine recipients of allogeneic T-cell depleted marrow for the promotion of engraftment. J Immunol 147:1492, 1991 16. Martin PJ, Hansen JA, Vitetta ES: A ricin A chain-containing immunotoxin that kills human T lymphocytes in vitro. Blood 66:908, 1985 17.Martin PJ, Hansen JA, Torok-Storb B, Moretti L, Press 0: Effects of treating marrowwith a CD3-specific immunotoxin for prevention of acute graft-versus-host disease. Bone Marrow Transplant 4:215, 1989 18. Press OW, Vitetta ES, Farr AG, HansenJA, Martin PJ: Evaluation of ricin A-chain immunotoxins directed against human T cells. Cell Immunol 102:IO, 1986 19. Preijers FWMB, DeWitte T, Rijke-Schilder GPM, Tax WJM, Wessels JMC, Haanen C, Capel PJA: Human T lymphocyte differentiation antigens as target for immunotoxins or complement-mediated cytotoxicity. Scand J Immunol 28:185, 1988 20. Youle RJ, Uckun FM, Vallera DA, Colombatti M: Immunotoxins show rapid entry of diphtheria toxin but not ricin via the T3 antigen. J Immunol 136:93, 1986 21. Neville DM Jr, Scharff J, Srinivasahar K: In vivo T cell ablation by a holo-immunotoxin directed at human CD3. Proc Natl Acad Sci USA 89:2586, 1992 22. Leo 0, Foo M, Sachs DH, Samelson LE, Bluestone JA: Identification of monoclonal antibody specific for a murine T3 polypeptide. Proc Natl Acad Sci USA 84:1374, 1987 23. Ey PL, Prouse SJ, Jenkin CR: Isolation of pure IgG1, IgG2a, and IgG2h immunoglobulins from mouse serum using protein Asepharose. Immunochemistry 15:429, 1978 24. Vallera DA, Youle RJ, Neville DM, Kersey JH: Bone marrow transplantation across major histocompatibility barriers: V. Protectionof mice from lethal GVHD by pretreatment of donor cells with monoclonal anti-Thyl.2 coupled to the toxin ricin. J Exp Med 155:949, 1982 25. Blazar BR, Soderling CCB, Koo GC, Vallera DA: Absence of a facilitory role for NK 1.1 positive donor cells in engraftment across a major histocompatibility bamer in mice. Transplantation 45376, 1988 26. Unkless JC: Characterization of monoclonal antibody directed against mouse macrophage and lymphocyte Fc receptors. J Exp Med 150:580, 1979 27.Koo GC, Peppard JR: Establishment of monoclonal antiNK1.1 antibody. Hybridoma 3:301, 1984 28. Jansen B, Vallera DA, Jaszcz WB, Nguyen D,Kersey J: Successful treatment of human acute T-cell leukemia in SCID mice using anti-CD7-deglycosylated ricin A-chain immunotoxin DA7. Cancer Res 52:1314, 1992 29. Markwell MAK: A new solid state reagent to iodinate proteins: Conditions for the efficient labeling of antiserum. Anal Biochem 125:427,1982 30. Vallera DA, Schmidberger H, Buchsbaum DJ, Everson P, Blazar BR: Radiotherapy in mice with Yttrium-90 labeled anti-Lyl monoclonal antibody: Therapy of established graft-versus-host dis- VALLERA ET AL ease induced across the major histocompatibility barrier. Cancer Res 15:1891, 1991 31. Mantel N: Evaluation of survival data in two new rank order statistics arising in its consideration. Cancer Chemother 50: 163, 1966 32. Myers DE, Uckun FM, Swaim SE, Vallera DA: The effects of aromatic and aliphatic maleimide crosslinkers on antiLCD5 ricin immunotoxins. J Immunol Methods 121: 129, 1989 33. Hirsch R, Gress RE, Plutnik DH, Eckhaus M, Bluestone JA: Effects of in vivo administration of anti-CD3 monoclonal antibody on T cell function in mice. In vivo activation of T cells. J Immunol 142:737, 1989 34. Blazar BR, Taylor PA, Gray GS, Vallera DA: The role of T cell subsets in regulating the in vivo efficacy of CTLA4-Ig in preventing graft-versus-host disease in recipients of fully MHCor multiple minor histocompatibiliy (miH)-disparate donor inocula. Transplantation 58: 1422, 1995 35. Abramowicz D, Schandene L, Goldman M, Crusiaux A, Vereerstraeten P, DePauw L, Wybran J, Kinnaert P, Dupont E, Toussaint C: Release of tumor necrosis factor, interleukin-2, and gamma-interferon in serum after injection of OKT3 monoclonal antibody in kidney transplant recipients. Transplantation 47:606, 1989 36. Flamand V, Abramowicz D, Goldman M, Biernaux C, Huez G, Urbain J, Moser M, Leo 0: Anti-CD3 antibodies induce T cells from unprimed animals to secrete IL-4 both in vitro and in vivo. J Immunol 144:2875, 1990 37. Ferrand C, Sheehan K, Dy M, Schreiber R, Merite S , Landais P, Noel LH, Grau G, Bluestone J, Bach JF, Chatenoud L: Cytokine related syndrome following injection of anti-CD3 monoclonal antibody: Further evidence for transient in vivo T cell activation. Eur J Immunol 20509, 1990 38. Alegre ML, Vandenbeele P, Depierreux M, Florquin S, Deschodt-Lanckman M, Flamand V, Moser M,Leo 0, Urbain J, Fiers W, Goldman M: Cytokine release syndrome induced by the 145-2C11 anti-CD3 monoclonal antibody in mice: Prevention by high doses of methylprednisolone. J Immunol 146:1185, 1991 39. Derocq JM, Casellas P, Laurent G, Ravel S , Vidal H, Jansen F: Comparison of the cytotoxic potency of TlOl Fab, F(ab‘)2 and whole IgGF immunotoxins. J lmmunol 141:2837, 1988 40. Masuho Y, Kishida K, Saito M, Umemoto N, Hara T: Importanceofthe antigen-binding valency and the nature of the crosslinking bond in ricin A-chain conjugates with antibody. J Biochem (Tokyo) 91:1583, 1982 41. Ross WCJ, Thorpe PE, Cumber AJ, Edwards DC,Hinson CA, Davies AJS: Increased toxicity of diphtheria toxin for human lymphoblastoid cells following covalent linkage to anti-(human lymphocyte) globulin or its F(ab’)* fragment. Eur J Biochem 104:381, 1980 42. Ghetie MA, May RD, Till M, Uhr JW, Ghetie V, Knowles PP, Relf M, Brown A, Wallace PM, Janossy G, Amlot P, Vitetta KE, Thorpe P: Evaluation of ricin A chain-containing immunotoxins directed against CD19 and CD22 antigens on normal and malignant human B-cells as potential reagents for in vivo therapy. Cancer Res 48:2610, 1988 43. Ravel S, Casellas P: Internalization of the cytotoxic molecules of TI01 F(ab’)2-(ricin-A-chain) immunotoxin into human T-leukemic cells. Eur J Biochem 192:469, 1990 44. Manske JM, Buchsbaum DJ, Vallera DA: The role of ricin B chain in the intracellular trafficking of anti-CD5 immunotoxins. J Immunol 142:1755, 1989 45. Bierer BE, Burakoff SJ, Smith BR: A large proportion of T lymphocytes lack CD5 expression after bone marrow transplantation. Blood 73:1359, 1989 46. Bierer BE, Nishimura Y, Burakoff SJ, Smith BR: Phenotypic and functional characterization of human cytolytic T cells lacking expression of CDS. Clin Invest 81:1390, 1988 From www.bloodjournal.org by guest on October 15, 2014. For personal use only. ANTLCD3F(ab’)> IMMUNOTOXIN FOR GVHD THERAPY 47. Filipovich AH, Vallera D, McGlave P, Polich D, Gajl-Peczalska K, Haake R, Lasky L, Blazar B, Ramsay NKC, Kersey J, Weisdorf D: T cell depletion with anti CD5 immunotoxin in histocompatible bone marrow transplantation: The correlation between residual CD5 negative T cells and subsequent GVHD. Transplantation 50:410, 1990 48. Blazar BR, Taylor PA, Sehgal SN, Vallera DA: Rapamycin 4375 prolongs survival of murine recipients of fully allogeneic donor grafts when administered during the graft-versus-host disease process. Ann NY Acad Sci 685:73, 1992 49. Vallera DA: Immunotoxins: Will their clinical promise be fulfilled? Blood 83:309, 1994 50. Vitetta E, Thorpe PE, Uhr JW: Immunotoxins: Magic bullets or misguided missiles? Immunol Today 14:252, 1993









© Copyright 2026