
The vascular supply of the functional compartments of the human striatum
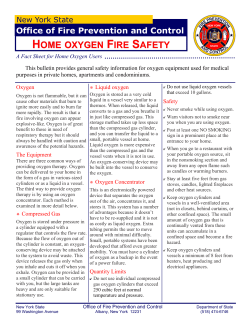
doi:10.1093/brain/awl158 Brain (2006), 129, 2189–2201 The vascular supply of the functional compartments of the human striatum Joel A. Feekes1 and Martin D. Cassell1,2 1 Neuroscience Program and 2Department of Anatomy and Cell Biology, University of Iowa, Iowa City, IA, USA Correspondence to: Martin D. Cassell, PhD, The University of Iowa, Department of Anatomy and Cell Biology, 1-512 Bowen Science Building, 51 Newton Road, Iowa City, IA 52242-1109, USA E-mail: [email protected] Keywords: basal ganglia; lacunar infarct; stroke; blood supply; striosome-matrix Abbreviations: BG = basal ganglia; CB = calbindin; LSA = lateral lenticulostriate arteries; RAH = recurrent artery of Heubner Received January 20, 2006. Revised April 17, 2006. Accepted May 16, 2006. Advance Access publication June 30, 2006 Introduction Several studies have demonstrated that sensorimotor, association and limbic cortical areas project in a segregated tripartite manner onto the striatum. This organization pattern also corresponds to zones of poor, intermediate and strong calbindin-D28k (CB) labelling, respectively (e.g. Holt et al., 1997; Karachi et al., 2002; Morel et al., 2002). In humans, the sensorimotor zone occupies a major dorsolateral sector of the post-commissural putamen (Pu) and a dorsolateral section of the body and head of the caudate nucleus (Cd) (Parent and Hazrati, 1995; Holt et al., 1997; Karachi et al., 2002; Leherichy et al., 2004). In non-human primates, this area is the major recipient of cortical fibres from the primary motor cortex (MI) (area 4), primary somatosensory cortex (SI) (areas 3, 1, 2 and 5), premotor cortex (PMC) (areas 8 and 6), supplementary motor area (SMA) and cingulate motor area (CMA) (Jones et al., 1977; Selemon and Goldman-Rakic, 1985; Alexander et al., 1990; Hedreen and DeLong, 1991; Flaherty and Graybiel, 1994; Francois et al., 1994; Kunishio and Haber, 1994; Parent and Hazrati, 1995; Takada et al., 1998, 2001; Karachi et al., 2002; Romanelli et al., 2005), and is thought to process motor information (Alexander et al., 1990; Karachi et al., 2002). The associative zone, marked by intermediate levels of CB staining, includes large portions of the Pu rostral to the anterior commissure and the majority of each segment of the Cd, with the exception of a small dorsolateral region adjacent to the internal # The Author (2006). Published by Oxford University Press on behalf of the Guarantors of Brain. All rights reserved. For Permissions, please email: [email protected] Downloaded from by guest on October 15, 2014 The basal ganglia (BG) contain several functional compartments and multiple, parallel segregated circuits processing different cortical information through cortical–BG–thalamus–cortical loops. Three zones of corticostriatal input are present: sensorimotor, associative and limbic, which correspond to poor, intermediate and strong calbindin (CB) labelling, respectively. Other functional compartments, such as striosomes, extrastriosomal matrix and matrisomes, also convey segregated projections. Microvascular territories in the human BG are spatially consistent with little overlap and few anastomoses. A high percentage of lacunar infarcts occur in the BG, yet the relationship between lacunae and functional compartments is unknown. We determined the relationship between microvascular territories and functional compartments within the human striatum. Microvascular territories were labelled by co-injection of diffusible dye, radio-opaque substance and gelatin into parental vessels and by sectioning each BG co-planar with the Talairach system. Sections underwent immunocytochemistry or histochemistry and the overlap of microvascular and functional territories was examined. CB staining of the arterial-injected striatum matched the functional compartments reported previously and overlay of microvascular territories revealed a correspondence between (i) the lateral lenticulostriate arteries (LSA) and sensorimotor zone; (ii) the medial LSA and associative zone; and (iii) the recurrent artery of Heubner (RAH) and limbic zone. A greater number of large vessels and capillaries were found in the matrix compared to striosomes, and a likely correspondence exists between high-density arteriole envelopes and matrisomes. The higher number of non-anastomotic vessels and capillary beds within the matrix predisposes these regions to both large lesions and small lacunar infarcts, creating specific symptoms based on striatal circuitry. 2190 Brain (2006), 129, 2189–2201 or infarcts within it may produce multiple and varied symptoms depending on the location of the lesion (e.g. Fisher, 1982; Bhatia and Marsden, 1994; Russmann et al., 2003). It is known that a higher percentage of strokes, particularly lacunar infarcts, occur within the striatum (Fisher, 1953, 1965; Hsieh and Cheng, 1990; Marinkovic et al., 1990) compared to other brain regions, in part due to non-anastomotic vessels (Hsieh and Cheng, 1990; Marinkovic et al., 1990; Feekes et al., 2005). Unfortunately, a clear understanding of the relationship between small striatal infarcts and the resulting clinical presentation does not exist. The regular arrangement and systematic spacing of both matrisomes and striosomes (Gimenez-Amaya and Graybiel, 1991) may correspond to the regularly organized vascular supply (Feekes et al., 2005) in some fashion, and therefore allow for greater predictability regarding lacunar stroke symptoms. Only one study to our knowledge has addressed the relationship between functional compartments and vascular supply but examined this in rodent, and their data suggest striosomes lie between penetrating vessels and have greater correspondence with the vasculature (Brown et al., 2004). Until recently, only the large-scale vascular territories of the human BG were known and with the exception of minor variations did not differ greatly among individuals (for a review see Feekes et al., 2005). However, the nature and distribution of small-scale microvascular territories, thought to produce lacunar infarcts, were not clear. Previously (Feekes et al., 2005), we were able to systematically clarify the microvascular territories of the human BG in Talairach space coordinates and found a spatially consistent arrangement of arterial envelopes which could account for the structural formation of lacunae. Here, we clarify the relationship between the microvascular supply of the human striatum and its functional compartments and use this to better understand the origin of symptoms from stroke in this region. Part of this work has appeared in abstract form (Feekes and Cassell, 2005). Material and methods Six normal human brains were used in this study and obtained from donors to the Deeded Body Program at the University of Iowa. In selecting brains, those that had obvious cerebrovascular accidents (e.g. major cortical strokes, subarachnoid hemorrhage), significant atherosclerotic plaques in the internal carotid (ICA), middle cerebral (MCA), anterior cerebral (ACA), or posterior cerebral (PCA) arteries, or neurological diseases (e.g. dementia, Parkinson’s disease) listed in medical case notes as chronic conditions or contributing to death were excluded. The age (range 52–85), sex (2 male, 4 female) and cause of death for each specimen were recorded. Postmortem interval before fixation ranged from 2 to 8 h. Before perfusion–fixation, cerebral vessels were flushed at pressures of 2–4 psi with ice-cold 0.05 M phosphate-buffered saline (PBS) by cannulation of the common carotid arteries and incisions of the jugular veins for rinse outflow. This rinse was maintained until clear PBS was seen flowing from the jugular veins to ensure vessels were devoid of blood. Brains were then perfusion-fixed at pressures of Downloaded from by guest on October 15, 2014 capsule (Selemon and Goldman-Rakic, 1985; Yeterian and Pandya, 1991; Francois et al., 1994; Parent and Hazrati, 1995; Holt et al., 1997; Karachi et al., 2002; Leherichy et al., 2004). This area receives projections from various association cortices in the frontal, cingulate, temporal and parietal cortices (Goldman and Nauta, 1977; Yeterian and Van Hoesen, 1978; Selemon and Goldman-Rakic, 1985; Alexander et al., 1990; Yeterian and Pandya, 1991, 1993, 1998; Francois et al., 1994; Eblen and Graybiel, 1995; Parent and Hazrati, 1995; Karachi et al., 2002), in non-human primates and is thought to process cognitive information (Alexander et al., 1990; Parent and Hazrati, 1995; Karachi et al., 2002). Finally, the limbic zone, which is strongly immunoreactive for CB, includes the nucleus accumbens (NA), deep parts of the olfactory tubercle and the ventral most regions of the Cd and Pu (Kunishio and Haber, 1994; Eblen and Graybiel, 1995; Haber et al., 1995; Parent and Hazrati, 1995; Holt et al., 1997; Karachi et al., 2002; Leherichy et al., 2004). Fibres from limbic and paralimbic cortices, including the amygdala, hippocampus, anterior cingulate (area 24), medial and orbitofrontal (areas 13, 13a, 13b) cortices, prelimbic cortex (area 32), insula and superior temporal gyrus (Russchen et al., 1985; Selemon and Goldman-Rakic, 1985; Alexander et al., 1990; Yeterian and Pandya, 1991; Kunishio and Haber, 1994; Eblen and Graybiel, 1995; Haber et al., 1995; Parent and Hazrati, 1995; Chikama et al., 1997; Yeterian and Pandya, 1998; Karachi et al., 2002), end in the limbic zone, which is thought to link emotional and motivational information with motor function (Alexander et al., 1990; Haber et al., 1995; Karachi et al., 2002). In addition to this broad territorial division, the striatum contains internal compartments of restricted size, the striosomes and the extrastriosomal matrix, distinguishable by their differential patterns of immunoreactivity for neurotransmitter-related substances (Graybiel and Ragsdale, 1978; Herkenham and Pert, 1981; Faull et al., 1989; JimenezCastellanos and Graybiel, 1989; Gerfen, 1992; Martin et al., 1993; Francois et al., 1994; Parent et al., 1996; Holt et al., 1997; Prensa et al., 1999). Striosomes and matrix also have different cortical inputs and outputs to the components of the globus pallidus (GP) and substantia nigra (SN) (Ragsdale and Graybiel, 1981, 1988, 1990; Donoghue and Herkenham, 1986; Faull et al., 1989; Jimenez-Castellanos and Graybiel, 1989; Langer and Graybiel, 1989; Gimenez-Amaya and Graybiel, 1990; Gerfen, 1992; Eblen and Graybiel, 1995; Parent et al., 1996; Karachi et al., 2002). Additional functional compartments, the matrisomes, have been identified within the matrix where cells are segregated into distinct clusters similar in size and shape to striosomes. The matrisomes maintain a systematic degree of order and spatial consistency, but currently lack a neurochemical marker (Jimenez-Castellanos and Graybiel, 1989; Gimenez-Amaya and Graybiel, 1991; Flaherty and Graybiel, 1993, 1994; Eblen and Graybiel, 1995; Parent and Hazrati, 1995). Given this complex, heterogeneous functional compartmentalization of the striatum, it is not surprising that lesions J. A. Feekes and M. D. Cassell Blood supply of striatal compartments 2191 and serially collected in PBS. The part of the striatum analysed in most detail extended from the level of the genu of the corpus callosum to the appearance of the internal segment of the GP. Each 50 mM section was used for immunocytochemistry or histochemistry to identify the striosome-poor, matrix-rich markers CB, tyrosine hydroxylase (TH) and acetylcholinesterase (AChE). For AChE histochemistry, a modified version of the GeneserJensen and Blackstad (1971) procedure was used on both 2 mm thick and 50 mM thin sections, which allowed for large-scale overlay comparison of vascular supply with functional compartments. Sections were rinsed in Tris-buffered saline (TBS) and then incubated in an adjusted (glacial acetic acid) pH (5.2) solution of distilled water, ethopropazine HCI (Sigma), acetylthiocholine iodide (Sigma), glycine, cupric sulphate and anhydrous sodium acetate for 20–24 h. To visualize the precipitate, sections were placed in a distilled water solution of 10% potassium ferricyanide for 5–8 min and the reaction stopped by rinsing in distilled water and saline. Sections were processed for CB using a monoclonal anticalbindin D-28k antibody (Swant, Swiss Antibodies, Bellinzona, Switzerland) (24 h) and an anti-mouse IGG secondary (Vector Laboratories, Burlingame, CA) (1 h), while sections processed for TH used a rabbit anti-tyrosine hydroxylase polyclonal antibody (Chemicon International, Inc., Temecula, CA) (24 h) and an antirabbit IGG secondary (Vector Laboratories) (1 h). Both procedures utilized the avidin–biotin–peroxidase complex method (Vectastain kit, Vector Laboratories) and the peroxidase was visualized with a nickel chloride-enhanced diaminobenzidine (DAB) (Vector Laboratories) reaction to produce a purple reaction product. The reaction was stopped by several rinses in tap water followed by PBS. Sections were mounted on to gelatin-coated glass slides, dehydrated through passages in ascending grades of alcohol followed by CitriSolv (Fisher) and cleared in xylene and coverslipped using Permount. This method labelled the somata and proximal dendrites and axons of medium-sized striatal spiny neurons and the surrounding neuropil. Consistent establishment of the boundaries between weak (sensorimotor), intermediate (associative) and strong (limbic) zones of CB immunoreactivity was achieved by digital densitometry. In brief, sections were photographed digitally on a fixed background illumination. Grey-scale histograms were generated for each image based on black (densest staining) and white (no staining). Histograms were partitioned into five equal segments and the original images re-processed (Adobe Photoshop 7.0) to show only these five levels. Comparison between these images and the original sections and those shown by others (Karachi et al., 2002; Morel et al., 2002) revealed a high degree of fidelity. All mounted AChE, CB and TH reactions were photographed macroscopically (Canon Powershot G2) or microscopically (Nikon Labophot-2 fitted with Pixera Pro 150ES digital camera), placed in Talairach coordinates if applicable, overlapped with the microvascular supply of the BG for that specimen, and analysed for microvascular supply, striosome-matrix and tripartite corticostriatal functional compartment relationships. All figures shown here were modified as necessary for brightness, illumination and size (Adobe Photoshop 7.0). To determine the relationship between vascular beds and striosome/matrix compartments, two additional analyses were undertaken. First, the location of vessels >100 mM was plotted on CB-stained sections and the relative position to striosomes mapped. Secondly, differences between striosomes and matrix and the microvascular supply were further analysed by counting Downloaded from by guest on October 15, 2014 2–4 psi with a solution containing 4% formaldehyde in PBS by postmortem cannulation of the common carotid artery, removed and prepared for arterial injection as described elsewhere (Feekes et al., 2005). Briefly, injections were made by selective insertion and ligation of polyethylene tubing with surgical silk (5-0; Ethicon, Inc.) into specific parental vessels [recurrent artery of Heubner (RAH), lenticulostriate arteries (LSA), anterior choroidal artery (AChA), medial striate branches of ACA and anterior communicating artery (ACoA)] along the circle of Willis and selective exclusion and ligation of others [distal MCA, distal ACA, ICA and posterior communicating artery (PCoA)]. Two fluorescent dyes were used in separate injections in separate arteries for comparison of territorial distributions and vascular borders within one hemisphere or specimen. A 0.15% solution of either Rhodamine B (Sigma, St Louis, MO) or Acridine Orange (Fisher, Hampton, NH), each containing 5% gelatin (DIFCO Laboratories) and 35% barium sulphate (Sigma) in double-distilled water, was injected into different brain vasculatures. Injections were completed by manual pressure with a 10 ml syringe and maintained for several minutes after backflow of injection was evident to ensure complete vessel filling. Previously (Feekes et al., 2005), each artery of interest was injected separately in this fashion and their territories plotted in Talairach space coordinates. This method revealed consistent vascular territories for each artery and from each specimen (n = 20 or 40 hemispheres) with very little or no overlap of separate territories, and allowed for visualization of vessels 50 mM in diameter. The consistent ability to inject vessels down to the pre-capillary arteriole or capillary level suggested complete injection, and that vessels were free of blood and clots. In addition, the lack of overlap between vascular territories, as defined by Talairach space coordinates, suggested a lack of anastomoses between major penetrating vessels of the striatum. This was confirmed by injections of different fluorescent dyes into separate arteries on one brain hemisphere. Anastomoses were very rarely, if ever, encountered, supported by findings from others claiming lack of anastomotic vessels in the human striatum (Hsieh and Cheng, 1990; Marinkovic et al., 1990). Therefore, the current method should not result in artificially inflated vascular territories owing to anastomotic vessels. High-resolution digital radiography was used to provide a detailed view of the barium sulphate-filled pre-capillary arterioles and terminal vascular beds (Fig. 1A and B), and the origin, course and variability of vessels leading to them. Contrasting software (Adobe Photoshop 7.0) was used to improve resolution of smaller vessels (Fig. 1C and D). The brains were scanned whole and then in progressively smaller block sections to a minimum of 1.27 cm with a 40 mM resolution mammograph (Lorad M-IV, TREX Medical Corp.). Next, the brains were sliced into 2 mm thick coronal serial sections with a commercial meat slicer (Globe GC512) and photographed under UV light with a digital camera (Canon Powershot G2) for identification of Rhodamine B or Acridine Orange stained territories. Territorial distributions were standardized by plotting vascular territory coordinates in the Talairach, three-dimensional proportional grid system (Talairach and Tournoux, 1988) (Fig. 2A and B), a method made possible by physically marking the Talairach reference planes on each brain and maintaining each plane by embedding the brain in agar prior to slicing (Feekes et al., 2005). After slicing each brain and examining the vascular territories, the entire striatum and GP segment was cut out of the 12 hemispheres from 6 different rostral–caudal positions, 2 mm apart from each other. These 2 mm thick coronal sections were then cut into 50 mM thick sections on a freezing microtome Brain (2006), 129, 2189–2201 2192 Brain (2006), 129, 2189–2201 J. A. Feekes and M. D. Cassell Downloaded from by guest on October 15, 2014 Fig. 1 Sample radiographs (A and B) and inverted and enhanced images (C and D) of barium sulphate-injected medial and lateral lenticulostriate arteries (mLSA and lLSA) and the recurrent artery of Heubner (RAH) in the human striatum revealing details of parental penetrating vessels, second- and third-order branches, and small pre-capillary arterioles. The LSA and RAH are shown maintaining a spatially consistent pattern and course. Arrows indicate tertiary arteriole envelopes. Cd, caudate nucleus; ic, internal capsule; and Pu, putamen. Line bars = 1 cm; slice thickness = 1.27 cm. capillaries within 400 mM square regions within each CB-defined compartment and comparing the differences in density. Striosomes and matrix were identified and photographed microscopically (·4 lens) and capillaries were counted within the 400 mM square region outlined within each compartment (Adobe Photoshop 7.0). A minimum of 10 samples were taken along the rostral–caudal axis of each of the six brain specimens and the capillaries were counted for all 60-plus square regions independently by both investigators. Results Corticostriatal zones The overall vascular architecture and extent of tertiary microvascular territories in the human striatum (Figs 1 and 2A) were consistent with those reported previously from 40 human brain hemispheres (Feekes et al., 2005). The appearance of CB, AChE and TH immunoreactivity of the arterial-injected human striatum (Fig. 3) corresponded very well with the differential patterns described by others (e.g. Holt et al., 1997; Karachi et al., 2002; Morel et al., 2002). In general, overlay of microvascular territories (Figs 2A, 4 and 5) revealed a correspondence between (i) the territory of the lateral LSA and the sensorimotor zone along the body and dorsolateral segment of the head of the Cd and Pu, and small portions of the associative zone along the head and a dorsolateral segment of the body of the Cd and Pu; (ii) the territory of the medial LSA and the associative zone along both the head and the body of the Cd and Pu, and small regions of both the lateral limbic zone and ventromedial Blood supply of striatal compartments Brain (2006), 129, 2189–2201 2193 Downloaded from by guest on October 15, 2014 Fig. 2 Coronal slice stained for acetylcholinesterase with overlap of barium sulphate-injected (inverted) vessels (A), and dye injection of same vessels (B) in the human striatum. Pictured are the lateral lenticulostriate arteries (LSA) (arrowhead) and the recurrent artery of Heubner (RAH) (arrow). Also shown is the overlap of the borders of corticostriatal zones (sensorimotor, white; associative, light grey; and limbic, dark grey) determined from calbindin immunoreactivity from 50 mM thick sections from the same brain. Note correspondence between the lateral LSA and sensorimotor zone and between the RAH and the limbic zone. Barium sulphate- and dye-defined vascular territories correspond. Vascular territories and corticostriatal zones were mapped in Talairach proportional grid space. Talairach coordinates are provided (a–d, medial to lateral; 1–12, dorsal to ventral; A–I, anterior to posterior, not shown). Cd, caudate nucleus; ic, internal capsule; Pu, putamen; and GP, globus pallidus. Line bars = 2 cm; slice thickness = 1.5 mm; barium sulphate-defined vessels from slice thickness = 1.27 cm. sensorimotor zone; and (iii) the territory of the RAH and the limbic zone along the body of the Cd and Pu, and small sections of the associative zone along the head and a ventromedial segment along the body of the Cd and Pu. The overall spatial inter-relationship between vascular territories and CB labelling was estimated by comparing the coordinates of the arterial and CB staining patterns in the Talairach proportional grid system (Fig. 2A and B). Coordinates for microvascular territories were similar to our previous study (Feekes et al., 2005) and not listed here. The CB-defined sensorimotor zone included coordinates ranging from the beginning of C to the end of E2 and 2194 Brain (2006), 129, 2189–2201 typically occupied Ca6, Ca7, Cb7, Cb8 to Da6–Da9, Db6–Db9, to E1a6, E1a7, E1b6–E1b9, to E2a6, E2b6– E2b9, with the most common regions where every brain was labelled including Ca7, Cb7, Da6, Da7, Db6–Db8, E1a6, E1b6–E1b9, E2b6, E2b8, and E2b9. The CB-defined associative zone included coordinates ranging from the beginning of C to the end of E2 and typically occupied Ca7, Ca8, Cb8 to Da6–Da9, Db7–Db9, to E1a6–E1a9, E1b6–E1b9, to E2a6, E2b6–E2b9, with the most common regions where every brain was labelled including Ca7, Ca8, Cb8, Da7–Da9, Db8, Db9, E1a6, E1a7, E1b7–E1b9, E2a6, E2b6, E2b8, and E2b9. The CB-defined limbic zone included coordinates ranging from the beginning of C to the end of E2 and typically occupied Ca8, Ca9, Cb8, Cb9 to Da6–Da10, Db8–Db10, to E1a6–E1a9, E1b6–E1b9, to E2a6, E2a9, E2b6, E2b8, E2b9, with the most common regions where every brain was labelled including Ca8, Ca9, Cb9, Da8, Da9, Db9, E1a7–E1a9, E1b8, E1b9, E2b6, E2b8, and E2b9. A comparison of corticostriatal zone coordinates with microvascular territory coordinates supports the Fig. 4 Calbindin (CB)-immunostained 50 mM thick section from human striatum with overlap of barium sulphate-injected (inverted) medial (open arrowhead) and lateral (closed arrowhead) lenticulostriate arteries (LSA) and the recurrent artery of Heubner (RAH) (arrow) from 1.27 cm thick section. Figure shows arrangement of penetrating vessels within striatum mainly co-registering with the matrix compared to striosomes (*). CB-immunoreactive section also shows dorsal–ventral gradient of weak to strong labelling which corresponds to sensorimotor, associative and limbic corticostriatal zones, respectively. Note co-registering between the lateral LSA and weak CB labelling, the medial LSA and intermediate labelling, and the RAH and strong labelling. Cd, caudate nucleus; ic, internal capsule; and Pu, putamen. Line bar = 1 cm. vascular–functional compartment correspondence described above. Typical Talairach coordinates for the lateral LSA territory and sensorimotor zone (Ca7, Cb7, Db7, Db8, E1b7–E1b9, E2b8, E2b9), the medial LSA territory and associative zone (Ca7, Cb8, Da7–Da9, Db8, Db9, E1a7, E1b7– E1b9, E2b8, E2b9), and the RAH territory and limbic zone (Ca8, Ca9, Cb9, Da8, Da9, Db9, E1a8, E1a9, E1b9) are similar (Feekes et al., 2005). Topographically, the lateral LSA territories and sensorimotor zone co-register along the dorsolateral rim of the head of the Cd and Pu, and extend along a larger dorsolateral segment of the body of the Cd and Pu (Figs 4, 5A and 5B). Occasionally, this includes a dorsomedial portion of the body of the Cd (Fig. 4). After the lateral LSA penetrate the anterior perforated substance they course along the ventral and lateral borders of the Pu to reach their intended territory of supply (Fig. 4). During this passage the lateral LSA co-register with a small lateral portion of the associative zone along the Pu and a small lateral portion of the limbic zone along the ventral Pu (Figs 4 and 5A). At the head of the Cd and Pu, the lateral LSA also co-register with the Downloaded from by guest on October 15, 2014 Fig. 3 Calbindin (CB)-labelled 50 mM thick section from human striatum revealing striosomes (arrows) and matrix, and the corticostriatal zones, sensorimotor, associative and limbic, as defined by the dorsal–ventral gradient of weak, intermediate and strong CB labelling, respectively. Corticostriatal zone borders are marked by dashed lines and the corresponding zone labelled. Cd, caudate nucleus; ic, internal capsule; Pu, putamen; and NA, nucleus accumbens. Line bar = 1 cm. J. A. Feekes and M. D. Cassell Blood supply of striatal compartments Brain (2006), 129, 2189–2201 2195 Downloaded from by guest on October 15, 2014 Fig. 5 Calbindin (CB)-labelled 50mM thick sections from four different rostral–caudal positions (A–D: rostral to caudal) in human striatum with overlap of barium sulphate (inverted)-injected medial (open arrowheads) and lateral (closed arrowheads) lenticulostriate arteries (LSA) and the recurrent artery of Heubner (RAH) (arrows) from 1.27 cm thick sections. CB-labelled sections have been re-processed to show the different densities of CB labelling. The corticostriatal input zones, sensorimotor, associative and limbic correspond to weak, intermediate and strong CB labelling, respectively. Some portions of overlapped vessels have been labelled with grey instead of black to help with identification. Figure reveals correspondence between the lateral LSA and weak (sensorimotor) CB labelling, between the medial LSA and intermediate (associative) CB labelling, and between the RAH and strong (limbic) CB labelling. Cd, caudate nucleus; ic, internal capsule; Pu, putamen; GP, globus pallidus; and Thal, thalamus. Line bar = 1 cm. associative zone, constituting the majority of the rostral extent of these nuclei. The medial LSA and associative zone co-register at the head of the Cd and Pu, particularly along the medial segment dorsoventrally, stretching almost completely from the medial to lateral borders of the Cd and Pu (Figs 4 and 5B). The medial LSA maintain this medial position and so co-register with the associative zone throughout the body of the Cd and Pu (Fig. 5C and D). After the medial LSA penetrate the anterior perforated substance they also course along the ventral and lateral borders of the Pu and GP to reach their intended area of supply. During this passage the medial 2196 Brain (2006), 129, 2189–2201 LSA also co-register with a lateral segment of the limbic zone. As the medial LSA stretch from lateral to medial regions of the Pu and Cd they occasionally supply a small ventromedial segment of the sensorimotor zone, mainly within the Cd (Fig. 5C). The RAH and limbic zone co-register along the width of the ventral segment of the head of the Cd and Pu (Figs 4, 5A and 5B). The RAH courses lateral to medial along the border of the NA all the way to the ventricular border of the Cd (Fig. 4). During its course, the RAH supplies the NA and ventral portions of the body of the Cd and Pu and so coregisters with the limbic zone here (Fig. 5B). At its medial most territory of supply, the RAH may co-register with the associative zone within the ventromedial segment of the Cd. At the head of the Cd and Pu, the RAH also co-registers with the ventral border of the associative zone. The small striate branches of the ACA and ACoA (Fig. 4) primarily supply the ventral striatal–pallidal complex including the NA (Feekes et al., 2005) and so are not reviewed in detail in this study of the dorsal striatum. Their vascular territories co-register with the limbic zone only. Examination of the relationship between striosomes and matrix with microvascular territories revealed a close correspondence between large penetrating branches and the matrix (Figs 6–8). Large vessels were found throughout the matrix (Fig. 6), but particularly along the matrix side Fig. 6 Striosome (black asterisk), potential matrisome (white asterisk) and matrix (unlabelled) determined by calbindin (CB) immunoreactivity from 50 mM thick section of human striatum. Next to a striosome is a region of particularly dense CB labelling distinguishable from surrounding CB-positive matrix. This extra dense CB-positive region is typically similar in size and shape to striosomes and pre-capillary arteriole envelopes and may represent a matrisome. Within the matrisome and around its borders are numerous capillaries, pre-capillary arterioles and larger vessels both in cross-section and running parallel with the section (closed arrows). Line bar = 0.5 mm. of striosome/matrix borders (Figs 6 and 7). Additionally, the density of vessels >100 mM in diameter within the matrix was greater than that found within striosomes (Fig. 8). The density of capillaries in the matrix was 138.4 (standard deviation, ) compared to 77.42 (standard deviation, 50.75) in striosomes (N = 62). The density of capillaries in the matrix was not uniform. This was particularly evident along tertiary branch terminals, where rich networks of precapillary arterioles formed spheroidal-shaped envelopes similar in size and shape to matrisomes (Gimenez-Amaya and Graybiel, 1991) in specific regions of the matrix. This is suggestive of a correspondence between the highest density arteriole envelopes and matrisomes, though in the absence of a specific matrisome marker this could not be confirmed. Discussion The present study has demonstrated two features of the vascular supply of the striatum: first, a correspondence between (i) the territory of the lateral LSA and the sensorimotor zone along the body and dorsolateral segment of the head of the Cd and Pu, as well as small portions of the associative zone along the head and a dorsolateral segment of the body of the Cd and Pu; (ii) the territory of the medial LSA and the associative zone along both the head and the body of the Cd and Pu, and small regions of both the lateral limbic zone and the ventromedial sensorimotor zone; and (iii) the territory of the RAH and the limbic zone along the body of the Cd and Pu, and small sections of the associative zone along the head and a ventromedial segment along the body of the Cd and Pu (Fig. 9); and secondly, a preponderance of both large penetrating vessels and capillaries within the matrix, potentially at matrisomes, compared to striosomes. These findings suggest that large infarcts involving the lateral LSA, medial LSA and RAH parental vessels affect primarily sensorimotor, associative and limbic zones, respectively, whereas lacunar infarcts may involve the matrix and matrisomes. Consistent with our previous study (Feekes et al., 2005), little variation was seen in vessel arrangement (e.g. branches, pattern) or dye-marked territories, in regard to their location relative to CB-stained areas. The findings in six brains, in terms of these anatomical features, were within the range of variation seen in a larger sample, so it is unlikely that any major alternative relationship between vascular supply and BG compartmentalization was missed. As shown previously (Feekes et al., 2005), vessels down to 50 mM in diameter (pre-capillary level) were identifiable using the radiographic method. The size limitation in this case was the level of resolution of the radiographic instrument (40 mM). Vessels smaller than this were not likely to be resolved. However, dye diffusion from capillaries and small arterioles remains localized and spatially consistent (Feekes et al., 2005) and thus serves as a marker for the smaller, un-resolvable Downloaded from by guest on October 15, 2014 Striosomes and matrix J. A. Feekes and M. D. Cassell Blood supply of striatal compartments Brain (2006), 129, 2189–2201 2197 capillaries. Overlapping of radiographically identified vessels or dye diffusion images with CB immunostained sections reveals identical results. Therefore it is unlikely that failure to directly visualize capillaries affected the overall findings. Although the transition from one corticostriatal zone to another may be gradual, each zone could clearly be identified based on CB labelling and their relative spatial locations specified from Talairach coordinates. These Talairach coordinates were similar between brain specimens and the location of zones matched those reported by others (Karachi et al., 2002; Morel et al., 2002). Additionally, although the major penetrating vessels of the striatum (lateral and medial LSA and RAH) do supply small portions of other corticostriatal zones, each vessel largely corresponds to only one zone: this is demonstrated by the close correspondence between the Talairach coordinates for a given penetrating vessel and the specific corticostriatal zone it supplies. The association made here between vascular territories and corticostriatal zones is an indirect one in that vascular territories have been correlated only with CB immunoreactivity which by extrapolation is correlated with functional territories. It is possible therefore that the correlation presented here could reflect simply the fact that CB is a better marker of vascular territories than it is of corticostriatal functional zones. Anatomical tracing studies that would directly define corticostriatal zones are not feasible in humans, so eliminating this possibility is difficult. However, imaging studies, such as diffusion tensor fibre tract (DTFT) imaging, appear to support a tripartite division of the striatum into zones similar to those outlined by different CB labelling densities (Leherichy et al., 2004). Vasculature of the striatum The vascular supply of the human striatum derives from two main sources: branches of the LSA from M1 and M2 segments of the MCA, and from the RAH off the A2 segment of the ACA (also see Fig. 1). Minor contributions come from small penetrating striate branches of the ACA and ACoA. Direct perforators from the MCA contribute very little to striatal supply due to their very short intraparenchymal course and small diameter (Feekes et al., 2005). Specifically, the most anterior–ventral portion of the striatum (including the internal capsule) is supplied by the RAH (Shellshear, 1920; Alexander, 1942; Rubinstein, 1944; Critchley, 1953; Westberg, 1963; Ahmed and Ahmed, 1967; Gillilan, 1968; Perlmutter and Rhoton, 1976; Rhoton et al., 1979; Takahashi et al., 1985; Feekes et al., 2005). The medial portions of the Cd, Pu and internal capsule, and lateral border of the external segment of the GP (GPe), are supplied by the medial LSA Downloaded from by guest on October 15, 2014 Fig. 7 Calbindin (CB) (A, C and D) and acetylcholinesterase (AChE) (B) labelled 50 mM thick sections of human striatum showing CB and AChE-poor striosomes surrounded by CB and AChE-rich matrix. Note typical arrangement of penetrating vessel branches, both in cross-section (arrows) and in parallel with section (arrowheads), bordering striosomes but mainly confined to the matrix. Line bars = 0.5 mm. 2198 Brain (2006), 129, 2189–2201 J. A. Feekes and M. D. Cassell Fig. 8 A traced outline of calbindin-labelled section of human striatum revealing relationship between penetrating vessel branches (small light grey lines/circles) and striosomes (large dark grey outlines/asterisk) and matrix. Note greater number of penetrating vessel branches in matrix compared to striosomes. Cd, caudate nucleus; ic, internal capsule; Pu, putamen; and NA, nucleus accumbens. Line bar = 1 cm. (Abbie, 1934; Alexander, 1942; Westberg, 1963; Kaplan, 1965; Leeds, 1974; Grand, 1980; Takahashi et al., 1985; Donzelli et al., 1998; Feekes et al., 2005) while the lateral LSA supply most of the lateral Pu and remaining Cd (Gillilan, 1968; Rosner et al., 1984; Takahashi et al., 1985; Marinkovic et al., 2001; Feekes et al., 2005) including the internal capsule between them. The medial and lateral LSA and RAH have similar branching patterns: after penetrating the anterior perforated substance, the primary vessels give rise to two to four secondary branches, each of which leads to tertiary branches, at the terminals of which are small precapillary arteriole envelopes (Feekes et al., 2005). Few anastomoses occur between these penetrating vessels or their branches (Feekes et al., 2005). Also, penetrating vessels supplying the dorsal striatum contribute very little to the basal forebrain, despite passing through it (Feekes et al., 2005). The present findings demonstrate that primary, secondary and most of the tertiary branches of the medial and lateral LSA and the RAH remain within a particular zone of CB staining (Figs 4 and 5). Occasionally, tertiary branches from all of these vessels were observed to extend into adjacent zones though more detailed study may reveal this to be due to a graduated boundary between zones. The fidelity with which the LSA and RAH are confined to a particular zone is indicated by the LSA supply to the caudal head and tail of the Cd, which has been partially cut off from the Pu by the internal capsule (Fig. 5C and D). The lateral LSA sends branches through the striatal cell bridges in the internal capsule to reach the body of the Cd but these branches only supply the sensorimotor zone, and not the associative zone. In terms of overall supply, the lack of anastomoses between major vessels supplying the striatum implies that haemodynamically, the three corticostriatal zones have independent vascular beds. Therefore, occlusion of a given parental vessel would cause damage largely restricted to a specific corticostriatal zone of the striatum. Corticostriatal zones and infarcts The consistent relationship between certain penetrating vessels and broad corticostriatal input zones predicts that specific symptoms would predominate after occlusion of a given vessel. For example, based on the current data, occlusion of the lateral LSA would produce largely motor (sensorimotor) signs whereas vascular disease affecting the RAH would lead to predominantly emotional and motivational (limbic) symptoms. Reports describing lesions involving the medial or lateral LSA generally support this notion and have identified primarily motor and motor-task performance deficits (e.g. motor hemiparesis, sensory-motor Downloaded from by guest on October 15, 2014 Fig. 9 Schematic representation of the functional compartments of the human striatum and their relationship with microvascular territories of supply. Two striosomes are marked (asterisks) for example. Closed circles at terminals of vessels represent tertiary, pre-capillary arteriole envelopes. Medial or lateral LSA, medial or lateral lenticulostriate arteries; RAH, recurrent artery of Heubner; Cd, caudate nucleus; ic, internal capsule; Pu, putamen; and NA, nucleus accumbens. Corresponding corticostriatal input zones are labelled. Blood supply of striatal compartments Striosomes, matrisomes and matrix While both large vessels and small pre-capillary arterioles may be found within striosome borders, the current study provides evidence for a much greater density of vessels within the matrix. The findings that vascular envelopes are less associated with striosomes are not in agreement with a previous study in rat (Brown et al., 2004) examining the relationship between striosomes, matrix and blood supply, in which they found a 2199 greater correspondence between striosomes and penetrating BG vessels. However, their results pointed to a lattice-like arrangement of penetrating vessels with striosomes between them, a scheme which does not exclude the possibility that matrisomes are situated directly along the vessels. Alternatively, there may be several key differences between the blood supply of the rat and human striatum. Interestingly, another study (Brown et al., 2002), which used deoxyglucose metabolic mapping in rat to test whether neutral behavioral states were associated with regions of high metabolic activity in the matrix, in striosomes, or in both, found peak metabolic activity primarily confined to the matrix. Increased metabolic activity requires an increased haemodynamic response and thus an increased perfusion of tissue. This is consistent with the current results showing a higher density of large and small vessels within the matrix. In the present and previous studies (Feekes et al., 2005) the microvascular territories of the human striatum were found to be highly consistent in terms of parent vessel orientation and position. If a strong relationship exists between the microvasculature and functional compartments, as the data provided here do concerning the matrix, then some form of regularity or order may exist for functional compartments. The patterns of anterograde and retrograde matrisome labelling in non-human primates indicate that such systematic arrangements are in fact present (Gimenez-Amaya and Graybiel, 1991). For example, alternating bands of striosomes, highly labelled matrix cells and weakly labelled matrix cells are found in the striatum following retrograde tracer injections into the GP and anterograde tracer injections into different cortical areas (GimenezAmaya and Graybiel, 1991). Additionally, the labelled matrisomes tended to line up along curved lines or bands with a regular periodicity of 0.25–0.3 mm separation, suggesting a regular arrangement for both striosomes and matrisomes in the striatum (Gimenez-Amaya and Graybiel, 1991). Human studies have shown that matrix CB-positive zones contain regions with cells expressing particularly high levels of CB, and which are often adjacent to CB poor zones (Holt et al., 1997). These regions of high-CB labelling may represent matrisomes, although no chemical markers definitive for matrisomes have been identified so any comparisons with vascular patterns may not be conclusive. The similar size and shape of matrisomes (GimenezAmaya and Graybiel, 1991) and pre-capillary arteriole envelopes (Feekes et al., 2005), along with the spatial consistency of both, however, suggests a correspondence between matrisomes and tertiary pre-capillary arteriole envelopes. The fact that these arteriole envelopes represent the probable site of lacunar infarcts (Feekes et al., 2005) frequent in the BG suggests that lacunae may specifically involve matrisomes. Matrisomal loss may remove the ability of neurons projecting from the matrix to inhibit the internal segment of the GP (GPi) and the pars reticulata of the SN (SNr), which inhibit thalamic nuclei (Houk and Wise, 1995; Parent and Hazrati, 1995), therefore resulting in a net decrease in Downloaded from by guest on October 15, 2014 dysfunction, ataxic hemiparesis with brachial predominance, dysarthria, dystonia, hemichorea-hemiballism), as well as abulia and, rarely, hemihypesthesia or pure sensory deficits (Takahashi et al., 1985; Ghika et al., 1991; Bhatia and Marsden, 1994; Giroud et al., 1997; Russmann et al., 2003). Similarly, lesions involving striate branches of the ACA and ACoA which supply the limbic zone, produce mainly ‘limbic’ deficits involving emotional and motivational related symptoms (e.g. altered personality, memory deficits, apathetic or decreased volition, psychosis, psychosomatic complaints, aphasia, autonomic and endocrine disorders), but only mild hemiparesis with brachial predominance (Critchley, 1953; Takahashi et al., 1985; Marinkovic et al., 1990). Conversely, RAH lesions, which would affect the limbic zone, have resulted in unexpected non-limbic symptoms (e.g. slight hemiparesis with brachial predominance, paralysis of the face, palate and tongue, hemiplegia with brachial dominance, aphasia, occasionally severe weakness in upper extremities and rigidity) in addition to decreased volition (Rubinstein, 1944; Takahashi et al., 1985). This may be the result of several factors. First, as shown here, each vessel supplies small portions of other corticostriatal zones, so some compounding of symptoms may occur. Alternatively, the intermingling of striosomes and matrix/matrisomes in all the corticostriatal zones may not allow various motivational and motor signs to be dissociated. Striosomes receive projections primarily from limbic cortices while matrix and matrisomes receive input primarily from sensorimotor and associative cortices (e.g. Donoghue and Herkenham, 1986; Ragsdale and Graybiel, 1990; Yeterian and Pandya, 1993, 1998; Kunishio and Haber, 1994; Eblen and Graybiel, 1995; Parent and Hazrati, 1995). Lesions involving matrisomes located in the limbic zone may still produce motor or cognitive deficits, while lesions involving striosomes located in sensorimotor zones may still produce emotional or motivational symptoms. This would be the case regardless of which vessel supplies them, since striosomes and matrix/ matrisomes are found in all vascular territories. Finally, all of the vessels supplying the striatum also supply the internal capsule, which runs between the Cd and Pu throughout the length of the BG. A lesion affecting a particular zone may compromise supply to the internal capsule, potentially causing motor, cognitive or limbic-related symptoms regardless of which vessel or zone is involved (Ghika et al., 1989; Nicolai et al., 1996). Brain (2006), 129, 2189–2201 2200 Brain (2006), 129, 2189–2201 movement. This decrease in motor output may be responsible for the development and presence of symptoms encountered in vascular parkinsonism (VP), a distinct clinical and pathological entity that is largely unresponsive to Ldopa therapy (Critchley, 1929; Tolosa and Santamaria, 1984; Friedman et al., 1986; Lazzarino et al., 1990; Murrow et al., 1990; Ikeda et al., 1996; Demirkiran et al., 2001; Zijlmans et al., 2004). This is supported by several studies indicating a relationship between VP and vascular deficits, including ischaemic lesions, small vessel disease or hypertension (Critchley, 1929; Tolosa and Santamaria, 1984; Winikates and Jankovic, 1999; Demirkiran et al., 2001; Zijlmans et al., 2004). Additionally, VP has already been reported to result from either multiple lacunae (Lazzarino et al., 1990; Murrow et al., 1990; Ikeda et al., 1996; van Zagten et al., 1998) or a single lacune (Lazzarino et al., 1990), but the mechanism for VP onset was unclear. Conclusions Acknowledgements The authors wish to express their gratitude to Sandra Maxwell McGruder and Allen McGruder for their assistance with mammography and radiographic images. We also wish to thank Patrick Elbert, Darrell Wilkins and Dennis Mickelson of the Deeded Body Program, University of Iowa, for their generous help in acquiring human brain specimens. References Abbie A. The morphology of the forebrain arteries, with especial reference to the evolution of the basal ganglia. J Anat 1934; 68: 433–70. Ahmed DS, Ahmed RH. The recurrent branch of the anterior cerebral artery. Anat Rec 1967; 157: 699–700. Alexander GE, Crutcher MD, DeLong MR. Basal ganglia-thalamocortical circuits: parallel substrates for motor, oculomotor, prefrontal and limbic functions. Prog Brain Res 1990; 85: 119–46. Alexander L. The vascular supply of the striopallidum. Res Publ Assn Res Nerv Mental Disord 1942; 21: 77–132. Bhatia KP, Marsden CD. The behavioral and motor consequences of focal lesions of the basal ganglia in man. Brain 1994; 117: 859–76. Brown LL, Feldman SM, Smith DM, Cavanaugh JR, Ackermann RF, Graybiel AM. Differential metabolic activity in the striosome and matrix compartments of the rat striatum during natural behaviors. J Neurosci 2002; 22: 305–14. Brown LL, Breuer O, Smith DM, Lawhorn C. The striosomal labyrinth of the striatum in mice and its relationship to the organization and density of blood vessels: more evidence for a lattice like functional organization in the striatum. Soc Neurosci Abstr 2004: 754.24. Chikama M, McFarland NR, Amaral DG, Haber SN. Insular cortical projections to functional regions of the striatum correlate with cortical cytoarchitectonic organization in the primate. J Neurosci 1997; 17: 9686–705. Critchley M. Arteriosclerotic parkinsonism. Brain 1929; 52: 23–83. Critchley M. The anterior cerebral artery and its syndromes. Brain 1953; 30: 120–65. Demirkiran M, Bozdemir H, Sarica Y. Vascular parkinsonism: a distinct, heterogeneous clinical entity. Acta Neurol Scand 2001; 104: 63–7. Donoghue J, Herkenham M. Neostriatal projections from individual cortical fields conform to histochemically distinct striatal compartments in the rat. Brain Res 1986; 365: 397–403. Donzelli R, Marinkovic SV, Brigante L, De Divitiis O, Nikodijevic I, Schonauer C, et al. Territories of the perforating (lenticulostriate) branches of the middle cerebral artery. Surg Radiol Anat 1998; 20: 393–8. Eblen F, Graybiel AM. Highly restricted origin of prefrontal cortical inputs to striosomes in the macaque monkey. J Neurosci 1995; 15: 5999–6013. Faull RLM, Dragunow M, Villiger JW. The distribution of neurotensin receptors and acetylcholinesterase in the human caudate nucleus: evidence for the existence of a third neurochemical compartment. Brain Res 1989; 488: 381–6. Feekes JA, Cassell MD. Relationship of microvascular territories in the human basal ganglia to its functional compartmentalization. Soc Neurosci Abstr 2005: 301.15. Feekes JA, Hsu SW, Chaloupka JC, Cassell MD. Tertiary microvascular territories define lacunar infarcts in the basal ganglia. Ann Neurol 2005; 58: 18–30. Fisher CM. Concerning strokes. Can Med Assoc J 1953; 69: 257–68. Fisher CM. Lacunes: small, deep cerebral infarcts. Neurology 1965; 15: 774–84. Fisher CM. Lacunar strokes and infarcts: a review. Neurology 1982; 32: 871–6. Flaherty AW, Graybiel AM. Two input systems for body representations in the primate striatal matrix: experimental evidence in the squirrel monkey. J Neurosci 1993; 13: 1120–37. Flaherty AW, Graybiel AM. Input-output organization of the sensorimotor striatum in the squirrel monkey. J Neurosci 1994; 14: 599–610. Francois C, Yelnik J, Percheron G, Tande D, Calbindin D- 28k as a marker for the associative cortical territory of the striatum in macaque. Brain Res 1994; 633: 331–6. Friedman A, Kang UJ, Tatemichi TK, Burke RE. A case of parkinsonism following striatal lacunar infarction. J Neurol Neurosurg Psychiatr 1986; 49: 1087–8. Geneser-Jensen FA, Blackstad TW. Distribution of acetylcholinesterase in the hippocampal region of the guinea pig. I. Entorhinal area, parasubiculum, and presubiculum. Zellforsch Mikrosk Anat 1971; 114: 460–81. Gerfen CR. The neostriatal mosaic: multiple levels of compartmental organization in the basal ganglia. Annu Rev Neurosci 1992; 15: 285–320. Ghika J, Bogousslavsky J, Regli F. Infarcts in the territory of the deep perforators from the carotid system. Neurology 1989; 39: 507–12. Ghika J, Bogousslavsky J, Regli F. Infarcts in the territory of lenticulostriate branches from the middle cerebral artery: etiological factors and clinical features in 65 cases. Arch Suisses Neurol Psychiatr 1991; 142: 5–18. Gillilan LA. The arterial and venous blood supplies to the forebrain (including the internal capsule) of primates. Neurology 1968; 18: 653–70. Gimenez-Amaya JM, Graybiel AM. Compartmental origins of the striatopallidal projection in the primate. Neuroscience 1990; 34: 111–26. Gimenez-Amaya JM, Graybiel AM. Modular organization of projection neurons in the matrix compartment of the primate striatum. J Neurosci 1991; 11: 779–91. Giroud M, Lemesle M, Madinier G, Billiar TH, Dumas R. Unilateral lenticular infarcts: radiological and clinical syndromes, etiology, and prognosis. J Neurol Neurosurg Psychiatr 1997; 63: 611–5. Goldman PS, Nauta WJH. An intricately patterned prefrontocaudate projection in the rhesus monkey. J Comp Neurol 1977; 171: 369–86. Downloaded from by guest on October 15, 2014 In summary, microvascular territories in the human striatum from the lateral LSA, medial LSA and RAH largely co-register with one corticostriatal zone, the sensorimotor, associative and limbic zone, respectively. Overall, there is a greater density of both large penetrating vessels and small pre-capillary arterioles and capillaries within the matrix compared to striosomes. Specifically, tertiary pre-capillary arteriole envelopes, the site of lacunar infarcts, correspond in size, shape and location with matrisomes. The preference of the vasculature for specific functional compartments in the human striatum may lead to distinctive symptoms depending on the vessel and its associated lesion location. J. A. Feekes and M. D. Cassell Blood supply of striatal compartments 2201 Prensa L, Gimenez-Amaya JM, Parent A. Chemical heterogeneity of the striosomal compartment in the human striatum. J Comp Neurol 1999; 413: 603–18. Ragsdale CW, Graybiel AM. The frontostriatal projection in the cat and monkey and its relationship to inhomogeneities established by acetylcholinesterase histochemistry. Brain Res 1981; 208: 259–66. Ragsdale CW, Graybiel AM. Fibers from the basolateral nucleus of the amygdala selectively innervate striosomes in the caudate nucleus of the cat. J Comp Neurol 1988; 269: 506–22. Ragsdale CW, Graybiel AM. A simple ordering of neocortical areas established by the compartmental organization of their striatal projections. Proc Natl Acad Sci USA 1990; 87: 6196–9. Rhoton AL, Saeki N, Perlmutter D, Zeal A. Microsurgical anatomy of common aneurysm sites. Clin Neurosurg 1979; 26: 248–306. Romanelli P, Esposito V, Schaal DW, Heit G. Somatotopy in the basal ganglia: experimental and clinical evidence for segregated sensorimotor channels. Brain Res Rev 2005; 48: 112–28. Rosner S, Rhoton A, Ono M, Barry M. Microsurgical anatomy of the anterior perforating arteries. J Neurosurg 1984; 61: 468–85. Rubinstein HS. Relation of circulus arteriosus to hypothalamus and internal capsule. Arch Neurol Psychiatr 1944; 52: 526–30. Russchen FT, Bakst I, Amaral DG, Price JL. The amygdalostriatal projections in the monkey. An anterograde tracing study. Brain Res 1985; 329: 241–57. Russmann H, Vingerhoets F, Ghika J, Maeder P, Bogousslavsky J. Acute infarction limited to the lenticular nucleus: clinical, etiologic and topographic features. Arch Neurol 2003; 60: 351–5. Selemon LD, Goldman-Rakic PS. Longitudinal topography and interdigitation of corticostriatal projections in the rhesus monkey. J Neurosci 1985; 5: 776–94. Shellshear J. The basal arteries of the forebrain and their functional significance. J Anat 1920; 55: 27–35. Takada M, Tokuno H, Nambu A, Inase M. Corticostriatal projections from the somatic motor areas of the frontal cortex in the macaque monkey: segregation versus overlap of input zones from the primary motor cortex, the supplementary motor area and the premotor cortex. Exp Brain Res 1998; 120: 114–28. Takada M, Tokuno H, Hamada I, Inase M, Ito Y, Imanishi M, et al. Organization of inputs from cingulate motor areas to basal ganglia in macaque monkey. Eur J Neurosci 2001; 14: 1633–50. Takahashi S, Goto K, Fukasawa H, Kawata Y, Uemura K, Kazuo S. Computed tomography of cerebral infarction along the distribution of the basal perforating arteries: Part I: striate arterial group. Radiology 1985; 155: 107–18. Talairach J, Tournoux P. Co-planar stereotaxic atlas of the human brain. New York: Thieme Medical; 1988. Tolosa ES, Santamaria J. Parkinsonism and basal ganglia infarcts. Neurology 1984; 34: 1516–8. van Zagten M, Lodder J, Kessels F. Gait disorder, parkinsonian signs in patients with stroke related to small deep infarcts and white matter lesions. Mov Disord 1998; 13: 89–95. Westberg G. The recurrent artery of Heubner and the arteries of the central ganglia. Acta Radiol Diagn (Stockh) 1963; 11: 949–54. Winikates J, Jankovic J. Clinical correlates of vascular parkinsonism. Arch Neurol 1999; 56: 98–102. Yeterian EH, Pandya DN. Prefrontostriatal conections in relation to cortical architectonic organization in rhesus monkeys. J Comp Neurol 1991; 312: 43–67. Yeterian EH, Pandya DN. Striatal connections of the parietal association cortices in rhesus monkeys. J Comp Neurol 1993; 332: 175–97. Yeterian EH, Pandya DN. Corticostriatal connections of the superior temporal region in rhesus monkeys. J Comp Neurol 1998; 399: 384–402. Yeterian EH, Van Hoesen GW. Corticostriate projections in the rhesus monkey: the organization of certain cortico-caudate connections. Brain Res 1978; 139: 43–63. Zijlmans JCM, Daniel SE, Hughes AJ, Revesz T, Lees AJ. Clinicopathological investigation of vascular parkinsonism, including clinical criteria for diagnosis. Mov Disord 2004; 19: 630–40. Downloaded from by guest on October 15, 2014 Grand W. Microsurgical anatomy of the proximal middle cerebral artery and the internal carotid artery bifurcation. Neurosurgery 1980; 7: 215–8. Graybiel AM, Ragsdale CW. Histochemically distinct compartments in the striatum of human, monkey and cat demonstrated by acetylcholinesterase staining. Proc Natl Acad Sci USA 1978; 75: 5723–6. Haber SN, Kunishio K, Mizobuchi M, Lynd-Balta E. The orbital and medial prefrontal circuit through the primate basal ganglia. J Neurosci 1995; 15: 4851–67. Hedreen JC, DeLong MR. Organization of striatopallidal, striatonigral and nigrostriatal projections in the macaque. J Comp Neurol 1991; 304: 569–95. Herkenham M, Pert CB. Mosaic distribution of opiate receptors, parafascicular projections, acetylcholinesterase in rat striatum. Nature 1981; 291: 415–8. Holt DJ, Graybiel AM, Saper CB. Neurochemical architecture of the human striatum. J Comp Neurol 1997; 384: 1–25. Houk JC, Wise SP. Distributed modular architectures linking basal ganglia, cerebellum and cerebral cortex: their role in planning and controlling action. Cereb Cortex 1995; 5: 95–110. Hsieh FY, Cheng TY. Distribution of cerebral infarcts on computed tomography. Kaohsiung J Med Sci 1990; 6: 523–8. Ikeda K, Kotabe T, Kanbashi S, Kinoshita M. Parkinsonism in lacunar infarcts of the basal ganglia. Eur Neurol 1996; 36: 248–9. Jimenez-Castellanos J, Graybiel AM. Compartmental origins of striatal efferent projections in the cat. Neuroscience 1989; 32: 297–321. Jones EG, Coulter JD, Burton H, Porter R. Cells of origin and terminal distribution of corticostriatal fibers arising in the sensory-motor cortex of monkeys. J Comp Neurol 1977; 173: 53–80. Kaplan H. The lateral perforating branches of the anterior and middle cerebral arteries. J Neurosurg 1965; 23: 305–10. Karachi C, Francois C, Parain K, Bardinet E, Tande D, Hirsch E, et al. Threedimensional cartography of functional territories in the human striatopallidal complex by using calbindin immunoreactivity. J Comp Neurol 2002; 450: 122–34. Kunishio K, Haber SN. Primate cingulostriatal projection: limbic striatal versus sensorimotor striatal input. J Comp Neurol 1994; 350: 337–56. Langer LF, Graybiel AM. Distinct nigrostriatal projection systems innervate striosomes and matrix in the primate striatum. Brain Res 1989; 498: 344–50. Lazzarino LG, Nicolai A, Toppani D. Subacute parkinsonism from a single lacunar infarct in the basal ganglia. Acta Neurol 1990; 12: 292–5. Leeds N. The striate (lenticulostriate) arteries, the artery of Heubner. In: Newton T, Potts D, editors. Radiology of the skull and brain. Mosby: St Louis, MO; 1974. p. 1527–39. Lehericy S, Ducros M, Van De Moortele PF, Francois C, Thivard L, Poupon C, et al. Diffusion tensor fiber tracking shows distinct corticostriatal circuits in humans. Ann Neurol 2004; 55: 522–9. Marinkovic SV, Milisavljevic MM, Marinkovic Z. Branches of the anterior communicating artery: microsurgical anatomy. Acta Neurochir 1990; 106: 78–85. Marinkovic SV, Gibo H, Milisavljevic M, Cetkovic M. Anatomic and clinical correlations of the lenticulostriate arteries. Clin Anat 2001; 14: 190–5. Martin LJ, Blackstone CD, Huganir RL, Price DL. The striatal mosaic in primates: striosomes and matrix are differentially enriched in ionotropic glutamate receptor subunits. J Neurosci 1993; 13: 782–92. Morel A, Loup F, Magnin M, Jeanmonod D. Neurochemical organization of the human basal ganglia: anatomofunctional territories defined by the distributions of calcium-binding proteins and SMI-32. J Comp Neurol 2002; 443: 86–103. Murrow RW, Schweiger GD, Kepes JJ, Koller WC. Parkinsonism due to a basal ganglia lacunar state: clinicopathologic correlation. Neurology 1990; 40: 897–900. Nicolai A, Lazzarino LG, Biasutti E. Large striatocapsular infarcts: clinical features and risk factors. J Neurology 1996; 243: 44–50. Parent A, Hazrati LN. Functional anatomy of the basal ganglia I. The corticobasal ganlia-thalamo-cortical loop. Brain Res Rev 1995; 20: 91–127. Parent A, Fortin M, Cote PY, Cicchetti F. Calcium-binding proteins in primate basal ganglia. Neurosci Res 1996; 25: 309–34. Perlmutter D, Rhoton A. Microsurgical anatomy of the anterior cerebralanterior communicating-recurrent artery complex. J Neurosurg 1976; 45: 259–72. Brain (2006), 129, 2189–2201









© Copyright 2026