
Document 348603
European Heart Journal (1996) 17, 1158-1166
Review Article
Phosphorus magnetic resonance spectroscopy of the
human heart: current status and clinical implications
H. P. Beyerbacht*, H. W. Vliegen*, H. J. Lambf, J. Doornbosf, A. de Roost,
A. van der Laarse* and E. E. van der Wall*
Departments of * Cardiology and ^Diagnostic Radiology, University Hospital Leiden, The Netherlands
Introduction
Heart muscle metabolism
Adenosine triphosphate (ATP) serves as a high-energy
intermediate for maintaining cellular homeostasis and
contractile function of the heart. The ATP concentration
in ventricular myocardium is remarkably constant and
quite independent of work load. Under normal conditions, the main part (40-70%) of ATP is formed
intramitochondrially, fuelled by ^-oxidation of fatty
acids. At the inner mitochondrial membrane, the highenergy phosphate bond of ATP is transferred to creatine
to yield phosphocreatine and adenosine diphosphate
(ADP), a reaction catalysed by mitochondrial creatine
kinase. Through the phosphocreatine shuttle, phosphocreatine is then transported to the cytosol and the
contractile elements where it is split by cytoplasmic
creatine kinase (isoenzymes CK-MM and CK-MB) in
order to form ATP and creatine. At the sarcomere
Key Words: Magnetic resonance spectroscopy, phosphorus-31, level, ATP is split by myosine-ATPase, resulting in the
myocardia! ischaemia, cardiomyopathy, left ventricular hyper- formation of ADP, inorganic phosphate (PJ and free
trophy, heart transplant.
energy — elements essential for contraction.
Revision submitted and accepted 21 November 1995.
During myocardial ischaemia, glucose becomes
by
Correspondence: Ernst E. van der Wall, MD, FESC, Uni- the predominant fuel whereby lactate is formed
+
anaerobic
glycolysis.
Accumulation
of
NADH,
H
and
versity Hospital Leiden, Department of Cardiology, C5-P25,
lactate inhibits several regulatory sites of metabolism,
Rijnsburgerweg 10, 2333 AA Leiden, The Netherlands.
0195-668X/96/081158 + 09 $18.00/0
© 1996 The European Society of Cardiology
Downloaded from by guest on October 21, 2014
Magnetic resonance spectroscopy is a non-invasive technique which, by means of a spectrum, can be used to
reveal the presence of certain molecules in a specific
area. Magnetic resonance spectroscopy uses a strong
external magnetic field and radiofrequency pulses to
detect the magnetic resonance signal of nuclei which
possess magnetic spin. Several biologically interesting
atomic nuclei are suitable for magnetic resonance spectroscopy, such as hydrogen ('H), carbon (13C), sodium
(23Na), and phosphorus ( 3I P). For non-invasive studies
of the heart in vivo, 31P magnetic resonance spectroscopy has been used extensively because it provides
information about the high-energy phosphate metabolism of the heart. The first cardiac 31P magnetic resonance spectroscopy experiments were conducted by
Gadian et al.m in 1976, using isolated Langendorffperfused animal hearts. In 1985 Bottomley121 reported
the first localized human cardiac 3I P spectra obtained in
healthy volunteers. Since then, the development of 3I P
magnetic resonance spectroscopy for studies in men has
grown steadily, but has been hampered by several technical difficulties. An important limitation of in vivo 31P
magnetic resonance spectroscopy is the relatively low
sensitivity of the technique resulting in long acquisition
times and a low spatial resolution. Consequently, 31P
magnetic resonance spectroscopy currently has no
well-defined application in clinical cardiology. Future
developments, such as the application of stronger magnetic field strengths, are expected to provide higher
spatial resolution. The promise of non-invasive insight
into the metabolic status of the heart seems so powerful,
especially when combined with magnetic resonance
imaging, that the question: 'when will this diagnostic
tool be available in clinical cardiology?', is more prominent than 'whether 31P magnetic resonance spectroscopy
will become available in clinical cardiology'.
The present report provides an overview of the
status, prospects and possible clinical implications of
cardiac 31P magnetic resonance spectroscopy. Results of
major human studies conducted to evaluate myocardial
ischaemia, heart transplantation, cardiomyopathy and
left ventricular hypertrophy will be discussed.
Review
including glycolysis. During the early stages of ischaemia, the myocardial ATP concentration is preserved at
the expense of phosphocreatine, which decreases rapidly
during ischaemia.
Heart failure can lead to metabolic changes
similar to those observed in ischaemia. The concentrations of creatine and phosphocreatine are diminished,
and this is accompanied by reduced total activity of
creatine kinase and altered isoenzyme distribution
of creatine kinase. The mechanisms behind these
adaptations are discussed later in the section entitled
'magnetization transfer'.
31
P magnetic resonance spectroscopy
Compared to hydrogen (*H), phosphorus (3lP) is
less magnetic resonance sensitive, but has a wider chemical shift range. The in vivo human 31P spectrum allows
the identification of signals from several important highenergy phosphate metabolites (Fig. I), such as phosphocreatine, the three separate signals (a, fi and y) from
ATP, the overlapping signals from phosphomonoesters,
2,3-diphosphoglycerate and inorganic phosphate (P,),
and finally a combined signal from phosphodiesters
and phosphatidylcholine (mainly serum phospholipids).
Because technical difficulties preclude the measurement
of accurate absolute metabolite concentrations relative
concentrations are most frequently used'3"51. In a recent
study by Yabe el al.[6i, 'absolute' phosphocreatine and
ATP concentrations were reported. However, these
measurements were based on a number of estimations
and assumptions resulting in high standard deviations'61.
Nevertheless, the use of 'absolute' instead of 'relative'
concentrations has advantages especially for disease
states which are associated with reduced or increased
concentrations of both phosphocreatine and ATP. The
ratios of phosphocreatine/ATP and phosphocreatine/Pi
are considered to represent the phosphate potential
(energy charge) of the myocardium within the volume
of interest'7"101. In studies of the human heart, the
phosphocreatine/ATP ratio is most often used as an
indication of energy charge since signal from Pj cannot
usually be observed as a separate peak in the spectrum.
This is due to the overlapping 2,3-diphosphoglycerate
signal which arises from blood within the volume of
interest. The chemical shift of P, and of 2,3diphosphoglycerate are almost identical but in some
cases the resonances can be resolved using a technique
called proton-decoupling1"1. When the P, peak is resolved, it can be used to estimate the pH within the
volume of interest because the chemical shift of P; is
pH-dependent at the physiological pH range whereas the
chemical shift of phosphocreatine is practically pHindependent. The difference in chemical shift between
the Pj and phosphocreatine peaks in a spectrum therefore provides a non-invasive measure of intracellular
pH [l ''. The phosphocreatine/ATP or phosphocreatine/P,
ratios are usually determined after 'curve fitting' of the
spectrum to estimate peak areas and chemical shifts.
In most cases the area under the curve rather than
the height of a peak is used to calculate ratios'121. The
/J-ATP signal is preferably used to determine the
phosphocreatine/ATP ratio since it is not contaminated
with signal from ADP, NAD + or NADH"21, as is the
case for the a and y ATP peaks.
To locate the volume of interest, several localization techniques have been developed, such as Depth
REsolved Surface coil Spectroscopy (DRESS), Image
Selected In vivo Spectroscopy (ISIS), and Chemical
Shift Imaging (CSI), each with its own advantages
and disadvantages. Depending on the technique used,
localization is possible in one, two or three dimensions.
Figure 2 shows an example of volume selection
with two-dimensional ISIS combined with onedimensional CSI. It is important to realize that, due to
the sensitivity profile of the surface coil, spectra can be
obtained from the anterior part of the left ventricular
wall only. In obese patients, and in females with a
more than average breast size, the distance between
the heart and the surface coil can even be too large
to obtain signal from the anterior myocardial wall.
For a detailed description of the magnetic resonance
spectroscopy technique we refer to more specific
literature17"91.
Localization techniques are necessary to minimize contamination of the spectra with signal from
outside the volume of interest. Signal contamination
is of serious concern in 3I P magnetic resonance
Eur Heart J, Vol. 17, August 1996
Downloaded from by guest on October 21, 2014
Magnetic resonance spectroscopy is performed with a
homogeneous magnetic field at a field strength of at least
1.5 Tesla. Only nuclei which possess a 'magnetic spin
moment' due to an odd number of protons and/or
neutrons are suitable for the technique. When nuclei
with a 'magnetic spin moment' are situated in a strong
external magnetic field, and are subjected to a radiofrequency pulse at the 'resonance frequency' of the nucleus,
their spin state is altered. Following the radiofrequency
pulse, the spins will precess around the direction of the
external magnetic field and produce a radiofrequency
signal which is detected by an antenna ('surface coil'),
positioned as close as possible to the tissue of interest.
The signal received by the surface coil is a timedependent voltage. After mathematical processing by
application of Fourier transformation, the frequency
information is obtained as a spectrum. The separation of
the peaks in a spectrum is caused by a phenomenon
called 'chemical shift'. Identical nuclei within one
molecule or in different molecules experience a slightly
different local magnetic field caused by differences in
chemical environment. This local magnetic field of a
nucleus gives rise to a specific resonance frequency.
Differences in resonance frequency or 'chemical shifts'
are expressed in Hertz, or as dimensionless parts per
million (p.p.m.), making it independent of the applied
magnetic field strength. The area under each peak is
proportional to the number of nuclei resonating at
that frequency and reflects the relative concentration
of specific metabolites within the volume of interest
('sample volume').
1159
1160 H. P. Beyerbacht et al.
15
10
-5
-10 -15
-20
-25
ppm - - •
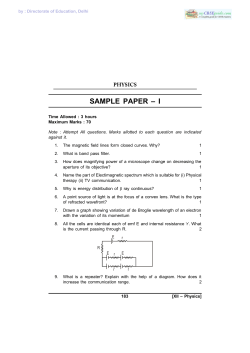
Figure 1 Myocardial 3 I P magnetic resonance spectrum
obtained from a healthy volunteer, (a) Spectrum
before curve-fitting, (b) Spectrum after curve fitting.
p.p.m. = parts per million; PCr=phosphocreatine; ATP =
adenosine
triphosphate;
PME=phosphomonoesters;
a = 2,3-diphosphoglycerate (2,3-DPG, with 3 I P at position
3); b=inorganic phosphate (P,)+2,3-DPG (with 3 I P at
position 2); PDE=phosphodiesters, mainJy serum
phospholipids (SPL).
To date, the smallest volume of interest reported is
8 cm3, which requires an external magnetic field of 4
Testa'15'161. Cardiac 31P magnetic resonance spectra may
often contain signal from blood, skeletal muscle from
the chest wall as well as from the diaphragm and signal
from the liver*5'""13'. Such contamination will considerably influence the phosphocreatine/ATP ratio. For example, the phosphocreatine/ATP ratio of skeletal muscle
is much higher than the myocardial phosphocreatine/
ATP ratio. Correction for this type of contamination
afterwards is not always possible'12-'3'. The contribution
of signal arising from ATP in blood to the total signal of
ATP in a cardiac 31P spectrum can be corrected for by
determining the amount of 2,3-diphosphoglycerate in
the 3I P spectrum. The ratio ATP/2,3-diphosphoglycerate
in blood is relatively constant, and blood contains
2,3-diphosphoglycerate in the absence of phosphocreatine151 U2 ' 17] .
Magnetization transfer
Figure 2 Sample volume selection with a combination of
two localization techniques called 'Image Selected In vivo
Spectroscopy' (ISIS) and 'Chemical Shift Imaging' (CSI).
A transverse spin-echo image through the chest is used to
determine the appropriate size and orientation of the
sample volume in two dimensions. The 3 I P spectra are
collected with a 10-cm diameter surface coil positioned
directly above the left ventricular wall. The column projected over the heart consists of sections, 1 cm thick, from
which separate spectra are collected.
spectroscopy1""131. Currently, most scanners, used for
clinical magnetic resonance spectroscopy operate at a
field strength of 1.5 Tesla and require volumes of interest
which exceed 25 cm3 to acquire a spectrum with
sufficient signal-to-noise ratio in a reasonable total
examination time1141. The use of stronger magnetic field
strengths improves spatial resolution but is expensive.
Eur Heart J, Vol. 17, August 1996
Magnetic resonance spectroscopy can also be applied
to determine the rate of enzymatic reactions using a
technique called 'magnetization transfer''5'19"24'. With
this technique the kinetics of creatine kinase have
been investigated in the myocardium of animals and
men'22"24'. The creatine kinase activity in patients with
dilated cardiomyopathy or left ventricular hypertrophy
(LVH) was 40% lower than in healthy controls'19'. The
relative contribution of the creatine kinase isoenzymes
CK-MB and CK-BB was higher, and that of the isoenzyme CK-MM lower in the myocardium of the dilated
cardiomyopathy patients. The altered expression of the
creatine kinase isoenzyme genes appears to be stimulated by increased wall stress'19'. Similar changes were
observed in patients with ischaemic heart disease1'9'.
Some investigators have suggested that, under stressful
conditions, the relative increase in the creatine kinase
isoenzymes CK-MB and CK-BB partly compensates for
decreased energy reserve caused by depletion of phosphocreatine and the decreased total creatine kinase
activity1'922"24'. Because of a higher affinity to ADP, the
B-containing isoenzymes are considered to be more
Downloaded from by guest on October 21, 2014
The severity of signal contamination by extracardiac tissues may differ between measurements even
within the same subject'18'. Many factors are important
in this respect, including positioning of the surface coil,
the site of the sample volume, motion of the subject, and
the used localization technique1101181. Consequently, the
results from different research centres vary widely. The
reported limits of 'normal' for the phosphocreatine/ATP
ratio in human myocardium range from 09 to 2-l[5'12',
but are still a matter of debate. Small changes in
acquisition technique and data processing may considerably alter the results, which makes it difficult to
compare data from different centres'12'. Interpretation
and comparison of 3I P magnetic resonance spectroscopy
data would benefit from a consensus about the appropriate acquisition technique and data processing1512>18'.
Review 1161
efficient than the MM isoenzyme in the formation of
ATP from phosphocreatine15'19'22-241.
Initial results with magnetic resonance
spectroscopy
Myocardial ischaemia
The effect of an ischaemic period on the myocardial
high-energy phosphate metabolism depends upon the
length and the severity of the ischaemic insult'25"341.
Both factors also influence the capability of recovery of
the heart following reperfusion'27'29'30'321. In a study of
Zhang et a/.'251 the left anterior descending coronary
artery of a canine heart was partially occluded for
several hours. After onset of occlusion, the myocardial
phosphocreatine concentration and phosphocreatine/
ATP ratio initially decreased considerably, accompanied
by a loss of contractile function. Several hours of
hypoperfusion led to a normalization of the myocardial
phosphocreatine concentration and phosphocreatine/
ATP ratio, although ischaemic myocardial segments
remained hypokinetic. Apparently, an adaptation process takes place which resembles the adaptation described for 'hibernating' myocardium. Consequently, a
normal phosphocreatine/ATP ratio does not exclude the
presence of ischaemia. Abnormal contractile function,
Eur Heart J, Vol. 17, August 1996
Downloaded from by guest on October 21, 2014
Using magnetic resonance spectroscopy, the high-energy
phosphate metabolism has been evaluated most extensively in animal studies, allowing repeat experiments
under controlled conditions. Examination of a heart in
vitro using a Langendorff preparation prevents contamination of the spectrum by signal arising from blood and
extracardiac tissue, and high spatial resolution can be
obtained by the application of a very strong external
magnetic field. Contamination of the spectrum by signal
arising from extracardiac tissue cart be markedly
reduced in vivo with the surface coil directly at the
myocardium during an open chest experiment in
animals'25"271. The absence of physiological circumstances, and the observed differences between different
species in myocardial high-energy phosphate metabolism when subjected to stress'281, raise the question of
how results from animal studies can be extrapolated to
findings in man.
Despite all differences of opinion about the limits
of 'normal' for the in vivo human myocardial
phosphocreatine/ATP ratio, and about the optimal protocol for measuring the phosphocreatine/ATP ratio,
much useful information about the cardiac high-energy
phosphate metabolism of both animals and men has
been gathered under a variety of physiological and
pathophysiological states, such as myocardial ischaemia,
transplanted hearts, cardiomyopathies and left ventricular hypertrophy. The following sections will deal with
these clinical disease states.
as can be evaluated using magnetic resonance imaging,
provides additional diagnostic information.
Weiss et a/.'351 examined 11 healthy volunteers
and 16 patients with left main or left anterior descending
coronary artery disease. Both groups were studied at
rest and during isometric handgrip testing. At rest the
myocardial phosphocreatine/ATP ratio was 1-72 ± 0 1 5
for controls and 1-45 ±0-31 for patients. During exercise, the myocardial phosphocreatine/ATP ratio for
healthy volunteers remained unchanged, but in patients
with left main or left anterior descending coronary
artery disease, the phosphocreatine/ATP ratio decreased
significantly to 0-91 ± 0-24. In these patients the myocardial phosphocreatine/ATP ratio recovered to 1-27 ± 0-38
within 2 min of discontinuing exercise. Following revascularization, the myocardial phosphocreatine/ATP
ratio normalized to 1 -60 ± 0-70 at rest and to 1-62 ± 0 1 8
during exercise.
In 27 patients with severe left anterior descending coronary artery disease, Yabe et alP6] compared the
results obtained with magnetic resonance spectroscopy
to the findings with thallium-201 scintigraphy. Patients
with a persistent scintigraphic defect did not show a
significant decrease in myocardial phosphocreatine/ATP
ratio during exercise (1-24 ±0-30 at rest versus
1 • 19 ± 0-28 during exercise), whereas patients with a
reversible scintigraphic defect had a significant decrease
in phosphocreatine/ATP ratio from 1-60 ±0-19 at rest to
096 ± 0-28 during exercise. The healthy controls studied
by Yabe et a/.'361 had a myocardial phosphocreatine/
ATP ratio of 1-85 ±0-28 at rest versus 1-90 ± 0 2 3
during exercise. These studies indicate that 3I P magnetic
resonance spectroscopy is a technique that can clinically
detect ischaemia of the anterior left ventricular wall.
Stress testing by means of physical exercise or
administration of pharmacological agents, such as
dobutamine, will play an important role in future 3I P
magnetic resonance spectroscopy studies'5'18'28'35'361.
Hearts that are hardly capable of maintaining their
energy reserves at rest will show a decrease in myocardial phosphocreatine/ATP ratio when subjected to
physically or pharmacologically induced stress'5'28'35'361.
The effects of a successful therapeutic intervention can
be deduced from a smaller decrease of the myocardial
phosphocreatine/ATP ratio during stress compared to
the baseline situation.
Yabe et aL[6] studied 41 subjects with significant
left anterior descending coronary artery disease, and
divided them into a group with fixed perfusion defects
and a group with reversible defects as assessed by
thallium-201 scintigraphy. The myocardial phosphocreatine concentration (expressed in umol. g ~' wet
heart tissue) was significantly lower in the group with
fixed perfusion defects compared with the group with
reversible defects (3-94 ± 2-21 versus 7-64 ± 3 0 0 , respectively). Also, the myocardial ATP concentration
(expressed in umol. g ~' wet heart tissue) was significantly lower in the patients with fixed defects compared
with the patients with reversible defects (6-35 ±3-17
versus 4-35 ± 1-52, respectively). The authors concluded
1162 H. P. Beyerbacht et al.
Transplanted hearts
Animal studies in rats have shown a significant correlation between the myocardial phosphocreatine/ATP
ratio and histological evidence of rejection whereby
a decrease of the phosphocreatine/ATP ratio even
preceded the histological evidence of rejection'37'38'.
Inspired by these experimental studies'37'38' one
would expect that 31P magnetic resonance spectroscopy
could provide a non-invasive means of early detection of
rejection in patients who received a heart transplant.
Several human studies, however, showed no reliable
relationship between the myocardial phosphocreatine/
APT ratio and the degree of rejection'5'17'39'. The
patients with severe rejection in particular, showed a
decreased myocardial phosphocreatine/ATP ratio, but
the specificity of this finding is low as there were also
patients with clear histological evidence of rejection and
a normal ratio'5'17'39]. Presumably, patients with severe
rejection have — like patients with a previous myocardial infarction — decreased myocardial phosphocreatine
and ATP concentrations in proportional quantities,
leaving their ratio unchanged.
Evanochko et a/.'40' found a normal myocardial
phosphocreatine/ATP ratio (181 ± 006) in five patients
with mild rejection, and a diminished phosphocreatine/
ATP ratio in four transplant patients with moderate
Eur Heart J, Vol. 17. August 1996
rejection as compared to healthy controls (1-13 ±0-17
versus 1 76 ±011). In a study by Wolfe et a/.'41', 13
patients who received a heart transplant had a similar
myocardial phosphocreatine/ATP ratio if the hearts
showed mild (n = 8) or moderate (n = 5) rejection
(1-29 ±0-13 versus 1-16 ± 110). In 13 patients who did
not show rejection, the myocardial phosphocreatine/
ATP ratio was significantly higher (1-45 ±009).
Bottomley et a/P9] examined 14 patients on 19 occasions
from 1 month to 6 years after transplanation. The
authors did not find a good relationship between the
myocardial phosphocreatine/ATP ratio and histological
biopsy scores for rejection. One explanation for the
differences between human and animal studies might be
the absence of immunosuppressive medication in the
animal studies, leading to more severe acute rejection in
rats(5).
In summary, both experimental and clinical
results make it unlikely that, in the near future, 3I P
magnetic resonance spectroscopy will become available
as a diagnostic modality for the management of patients
receiving a heart transplant. Future developments however, such as the use of stronger magnetic fields, yielding
higher sensitivity and resolution, and the measurement
of absolute instead of relative concentrations, may help
to overcome the present limitations.
Hypertrophic cardiomyopathy
Weiss et a/.'351 were the first to study patients with
hypertrophic cardiomyopathy, and they observed no
significant decrease in the myocardial phosphocreatine/
ATP ratio. However, only five patients were studied.
Conversely, subsequent 31P magnetic resonance spectroscopy studies by De Roos et a/.'"', Masuda et al.l42]
and Sakuma et a/.'43' showed a significantly lower
phosphocreatine/ATP ratio in hearts of patients with
hypertrophic cardiomyopathy compared with healthy
controls. De Roos et al.lu] found a lower myocardial
phosphocreatine/ATP ratio in eight hypertrophic cardiomyopathy patients compared with nine healthy controls (1-32 ± 0-29 vs 1 -65 ± 0-26). In the study of Masuda
et a/.'42', 12 patients with hypertrophic cardiomyopathy
had a myocardial phosphocreatine/ATP ratio of
1 43 ± 0-36 vs 209 ± 0-44 in 15 controls. Lastly, Sakuma
et a/.'43' found in 19 hypertrophic cardiomyopathy
patients a significant decrease in the phosphocreatine/
ATP ratio when compared to controls, with values of
1-07 ±0-10 and 1-71 ± 0 1 3 , respectively. They observed
no relationship between perfusion abnormalities
assessed by thallium-201 scintigraphy and the decreased
myocardial phosphocreatine/ATP ratio, indicating an
uncoupling of perfusion and metabolism. As most
studies show a decreased myocardial phosphocreatine/
ATP ratio in hypertrophic cardiomyopathy patients, 3I P
magnetic resonance spectroscopy may find a clinical
application in the diagnostic process when hypertrophic
cardiomyopathy is suspected. The pathophysiological
mechanism responsible for the lowered myocardial
Downloaded from by guest on October 21, 2014
that measurement of the ATP concentration in the
human heart with 31 P magnetic resonance spectroscopy
can be used clinically for the evaluation of myocardial
ischaemia and viability. Clinical use, however, is
hampered by the fairly large standard deviations of the
reported values'61.
The effects of a myocardial infarction on the
high-energy phosphate metabolism of the human heart
have been studied as well. In 20 patients with a previous
myocardial infarction, Mitsunami et a/.'3' measured a
decrease in myocardial concentrations of phosphocreatine and ATP. The phosphocreatine concentration in
post-myocardial infarction patients was 7-4 ± 26 versus
11 -3 ± 3-7 umol . g ~ ' myocardium in healthy volunteers
and the ATP concentration was 4-9 ± 20 versus
7-4 ± 2-9 umol. g~ ' myocardium, respectively. To
determine whether myocardium is infarcted requires
the measurement of absolute rather than relative
concentrations of phosphocreatine and ATP13"51.
In summary, 31P magnetic resonance spectroscopy in the assessment of myocardial ischaemia and
viability can be applied clinically, but technical restraints
limit its volume of interest to the anterior part of the left
ventricular wall and the interventricular septum. This
restriction is due to the loss of signal strength at greater
distance from the surface coil. It is difficult to improve
spatial resolution and to increase the depth at which
spectra can be obtained, but if these limitations could be
overcome the clinical value of 3I P magnetic resonance
spectroscopy in the assessment myocardial ischaemia
and viability would increase considerably.
Review 1163
phosphocreatine/ATP ratio in hypertrophic cardiomyopathy patients has not been elucidated yet, but a
lower vasodilator reserve, as demonstrated by Camici
et a/.'441, could be a contributing factor.
Dilated cardiomyopathy
Left ventricular hypertrophy
Left ventricular hypertrophy is known to be associated
with a decreased density of capillaries and a reduced
vasodilator reserve'46'471. In rats left ventricular hypertrophy has been shown to be associated with a decreased
myocardial ATP concentration and increased sensitivity
to ischaemia, when analysed in a Langendorff perfusion
model148"501.
Patients with left ventricular hypertrophy represent a heterogenous group which may be divided into
15.0
10.0
5.0
0.0
-5.0 -10.0 -15.0 -20.0 -25.0
ppm
- *•
3I
Figure 3 Myocardial P magnetic resonance spectrum
from a patient with dilated cardiomyopathy and from a
healthy control. Clearly visible is the larger 2,3diphosphoglycerate signal in tbe spectrum of the dilated
cardiomyopathy patient due to the larger amount of blood
in the sample volume; in this particular dilated cardiomyopathy patient the phosphocreatine/ATP ratio was
significantly lower than in die average healthy control.
This was not the case for the dilated cardiomyopathy
patients as a group. (With permission from de Roos
etaLiUi.)
those with pressure overload (hypertension, aortic valve
stenosis), volume overload (aortic valve insufficiency or
mitral valve regurgitation), or physical training (athlete's
heart) as causal factor15'1.
Conway et al.[52] studied 14 patients with left
ventricular hypertrophy, six of whom were treated for
heart failure (NYHA classes II-III). Only these six
patients could be distinguished from healthy controls on
the basis of the myocardial phosphocreatine/ATP ratio
(1-11 ±0-3 vs l-5±0-2), whereas the patients without
clinical signs of heart failure had an average myocardial
phosphocreatine/ATP ratio in the normal range
(1-6 ±0-2).
In 15 patients with left ventricular hypertrophy
due to aortic valve disease, Neubauer et a/.'531 showed
that the myocardial phosphocreatine/ATP ratio was
correlated to NYHA class, fractional shortening, pulmonary capillary wedge pressure and right atrial
pressure. No correlation was found between the myocardial phosphocreatine/ATP ratio and the left ventricular
ejection fraction or cardiac output'531. Dell' Italia
et a/.'54' studied 12 patients with left ventricular hypertrophy due to aortic stenosis both before and 3 months
after aortic valve replacement. Before surgery they
measured a myocardial phosphocreatine/ATP ratio
which was significantly lower than in controls
(105 ± 0-22 vs 1-30 ±015). Aortic valve replacement
surgery led to a significant functional improvement of
NYHA class, but not to an increase in myocardial
Eur Heart J, Vol. 17, August 1996
Downloaded from by guest on October 21, 2014
In patients with dilated cardiomyopathy a relationship
has been established between the severity of heart failure
and the decrease of the myocardial phosphocreatine/
ATP ratio'51. Neubauer et al.[4S] studied 19 dilated
cardiomyopathy patients and found a myocardial
phosphocreatine/ATP ratio of 1-94 ±0-43 in patients
with only mild symptoms of heart failure whereas
patients with severe signs of heart failure had a ratio of
1-44 ±0-52. The correlation between New York Heart
Association (NYHA) class and phosphocreatine/ATP
ratio was highly significant (r= -0-60, P<0005). Treatment of six patients with severe heart failure during 3
months, led to an average improvement in NYHA class
by 0 8 ± 0-3 points, which was accompanied by a rise in
myocardial phosphocreatine/ATP ratio from 1-51 ± 0-32
to 215 ± 027. The authors'451 also reported that such a
relation could not be established for the left ventricular
ejection fraction and the myocardial phosphocreatine/
ATP ratio.
De Roos et a/.'1'' compared nine healthy controls
(phosphocreatine/ATP 1-65 ±0-26) with nine patients
with dilated cardiomyopathy. The dilated cardiomyopathy patients showed, on average, a normal myocardial
phosphocreatine/ATP ratio (1 -52 ± 0-58), although some
individual dilated cardiomyopathy patients did show
a lowered phosphocreatine/ATP ratio compared to
healthy controls (Fig. 3). Differences in myocardial
phosphocreatine/ATP ratio between dilated cardiomyopathy patients may be due to differences in severity
of the disease between the patients. Measurement of
accurate myocardial phosphocreatine/ATP ratios in
dilated cardiomyopathy patients is hampered by a relatively thin anterior left ventricular wall. The sample
value may contain insufficient myocardium to generate a
spectrum with an acceptable signal-to-noise ratio1"1.
Follow-up studies in dilated cardiomyopathy patients
with progressive heart failure and assessment of efficacy
of therapy may become a clinical application of 3I P
magnetic resonance spectroscopy.
1164 H. P. Beyerbacht et al.
phosphocreatine/ATP ratio. In concordance with these
findings are the results of a study by Ito et a/.'551, who
observed that, after regression of left ventricular hypertrophy in rats, the heart remained more sensitive to
ischaemia. They showed that the vascular resistance,
which was higher in hypertrophic hearts, did not normalize parallel with regression of left ventricular hypertrophy. They considered an increased vascular resistance
as an independent risk factor for cardiac morbidity.
Longer follow-up periods than those used in the previously mentioned studies'54'551 may be warranted to
observe whether or not a normalization of the myocardial phosphocreatine/ATP ratio follows left ventricular
hypertrophy regression.
31
P magnetic resonance spectroscopy of the heart
might become of clinical value in patients with left
ventricular hypertrophy. Possible applications are improved detection of the optimal moment for surgery in
patients with aortic or mitral valve disease, an assessment of efficacy of therapy in patients with valve disease
or hypertension.
offers a means of showing latent shortages in highenergy phosphates and may improve sensitivity for
detecting the early stages of heart disease1'5'18'28'35'361.
Evaluation of therapy in patients with dilated cardiomyopathy, hypertrophic cardiomyopathy, left ventricular hypertrophy or myocardial ischaemia located in the
anterior wall of the left ventricular, may become a
realistic clinical application for 3I P magnetic resonance.
The range of clinical applications may increase when
absolute instead of relative metabolite concentration are
measured. Then 31P magnetic resonance spectroscopy
will allow evaluation of disease states in which myocardial phosphocreatine and ATP concentrations decrease or increase by equal amounts. Until now, the low
spatial resolution of >8 cm3, due to a low intrinsic
sensitivity and low abundance of phosphorus containing
molecules, the relatively long exposure times, and the
relatively high costs of magnetic resonance machines
and dedicated software packages still limit major clinical
applications. Ongoing technical progress will facilitate
the implementation of 31P magnetic resonance
spectroscopy in clinical cardiology.
Conclusions
3I
Eur Heart J. Vol. 17, August 1996
References
[1] Gadian DG, Hoult DI, Radda GK, Seely PJ, Chance B,
Barlow C. Phosphorous nuclear magnetic resonance studies in
normoxic and ischemic cardiac tissue. Proc Natl Acad Sci
USA 1976 1976; 73: 4446-8.
[2] Bottomley PA. Noninvasive study of high-energy phosphate
metabolism in human heart by depth-resolved
P NMR
spectroscopy. Science 1985; 229: 769-72.
[3] Mitsunami K, Okada M, Inoue T, Hachisuka M, Kinoshita
M, Inubushi T. In vivo 3 I P nuclear magnetic resonance
spectroscopy in patients with old myocardial infarction. Jpn
Circ J 1992; 56: 614-9.
[4] Tofts PS, Wray S. A critical assessment of methods of
measuring metabolite concentrations by NMR spectroscopy.
NMR Biomed 1988; 1: 1-10.
[5] Bottomley PA. MR spectroscopy of the human heart: the
status and the challenges. Radiology 1994; 191: 593-612.
[6] Yabe T, Mitsunami K, Inubushi T, Kinoshita M. Quantitative
measurements of cardiac phosphorus metabolites in coronary
artery disease by 31 P magnetic resonance spectroscopy
Circulation 1995; 92: 15-23.
[7] Osbakken MD, Mitchell MD. Magnetic resonance spectroscopy to study myocardial metabolism and cellular function.
In: Marcus ML, Skorton DJ, Schelbert HR, Wolf GL, eds.
Cardiac imaging: a companion to Braunwald's Heart disease.
Philadelphia: W. B. Saunders; 1991: 841-63.
[8] Gadian DG. Nuclear magnetic resonance and its application
to living systems. Oxford: Clarendon, 1982.
[9] Brown JJ, Mirowitz SA, Sandstrom JC, Perman WH.
MR spectroscopy of the heart. AJR Am J Roentgenol 1990;
155: 1-11.
[10] Stamper JJ, Pohost GM. Assessing myocardial ischemic insult
using nuclear magnetic resonance spectroscopy. Am J Card
Imaging 1992, 6: 244-58.
[11] de Roos A, Doombos J, Luyten PR, Oosterwaal LJMP, van
der Wall EE, den Hollander JA. Cardiac metabolism in
patients with dilated and hypertrophic cardiomyopathy
assessment with proton-decoupled P-31 MR spectroscopy
J Magn Reson Imaging 1992; 2: 711-9.
[12] Bottomley PA. The trouble with spectroscopy papers.
Radiology 1991; 181: 344-50.
Downloaded from by guest on October 21, 2014
P magnetic resonance spectroscopy is a valuable diagnostic tool but is currently restricted mainly to research
applications. Most likely in the future 31P magnetic
resonance spectroscopy of the heart will become available as a clinically useful diagnostic modality. The
combined information of structure, function and metabolism which can be obtained in a single study offers a
unique method for investigating these modalities in a
'one-stop-shop' fashion.
The use of slightly differing data-acquisition protocols and localization techniques by several research
groups warrants the development of a consensus about a
normal value for the 'true' myocardial phosphocreatine/
ATP ratio. Standardization of hardware, software and
study protocols would improve the reproducibility of
31
P magnetic resonance spectroscopy studies performed
by different research groups'5'121. To date, reproducibility may even present a problem within one research
group'12'181. This may be due, at least partly, to a
different extent of signal contamination with different
measurements, as the quantity of extracardiac tissue
within the sample volume varies among different
measurements. Small variations in sample volume selection may strongly affect the measured myocardial
phosphocreatine/ATP ratio"'- | 3 l 8 l.
Another limitation to the clinical use of 3I P
magnetic resonance spectroscopy is the ability of the
heart to maintain its high-energy phosphate metabolism
within normal ranges. Changes in the high-engergy
phosphate metabolism may therefore manifest relatively
late151. Studies in patients with left ventricular hypertrophy or dilated cardiomyopathy*513-45521 showed myocardial phosphocreatine/ATP ratios which were decreased
only if symptoms of heart failure were already present.
Stress testing during magnetic resonance spectroscopy
Review
[32] Rehr RB, Tatum JL, Hirsch JI, Wetstein L, Clarke G.
Effective separation of normal, actutely ischemic, and reperfused myocardium with P-31 MR spectroscopy Radiology
1988; 168: 81-9.
[33] Bottomley PA, Smith LS, Brazzamano S, Hedlund LW,
Redington RW, Herfkens RJ. The fate of inorganic phosphate
and pH in regional myocardial ischemia and infarction: a
noninvasive 3 I P NMR study. Magn Reson Med 1987; 5:
129-42.
[34] Rehr RB, Tatum FL, Hirsch JI, Quint R, Clarke G.
Reperfused-viable and reperfused-infarcted myocardium: differentiation with in vivo P-31 MR spectroscopy. Radiology
1989; 172: 53-8.
[35] Weiss RG, Bottomley PA, Hardy CJ, Gerstenblith G. Regional myocardial metabolism of high-energy phosphates during isometric exercise in patients with coronary artery disease.
N Engl J Med 1990; 323: 1593-600.
[36] Yabe T, Mitsunami K, Okada M, Mirikawa S, Inubushi T,
Kinoshita M. Detection of myocardial ischemia by 31 P
magnetic resonance spectroscopy during handgrip exercise.
Circulation 1994; 89: 1709-16.
[37] Fraser CD Jr, Chacko VP, Jacobus WE et al. Early phosphorus 31 nuclear magnetic resonance bioenergetic changes
potentially predict rejection in heterotopic cardiac allografts.
J Heart Transplant 1990; 9: 197-204.
[38] Fraser CK Jr, Chacko VP, Jacobus WE et al. Metabolic
changes preceding functional and morphologic indices of
rejection in heterotopic cardiac allgrafts. A 31P nuclear
magnetic resonance study. Transplantation 1988; 46: 346-51
[39] Bottomley PA, Weiss RG, Hardy CJ, Baumgartner WA.
Myocardial high-energy phosphate metabolism and allograft
rejection in patients with heart transplants. Radiology 1991;
181: 67-75.
[40] Evanochko WT, Bouchard A, Kirklin JK, Bourge RC, Luney
D, Pohost GM. Detection of cardiac transplant rejection in
patients by 3 I P NMR spectroscopy [abstract]. Society of
Magnetic Resonance in Medicine: Ninth annual scientific
meeting and exhibition; August 18-24, New York, NY USA.
Berkeley Calif. Society of Magnetic Resonance in Medicine,
1990: 246.
[41] Wolfe CL, Caputo G, Chew W et al. Detection of cardiac
transplant rejection by magnetic resonance imaging and spectroscopy [abstract]. Society of Magnetic Resonance in Medicine: Tenth annual scientific meeting and exhibition; August
10-16, 1991, San Francisco, Calif. USA. Berkely Calif. Society
of Magnetic Resonance in Medicine, 1991; 574.
[42] Masuda Y, Tateno Y, Ikehira H et al. High-enegy phosphate
metabolism of the myocardium in normal subjects and
patients with various cardiomyopatnies. The study using ECG
gated MR spectroscopy with a localization technique. Jpn
Circ J 1992; 56: 620-6.
[43] Sakuma H, Takeda K, Tagami T et al. 31 P MR spectroscopy
in hypertrophic cardiomyopathy: comparison with Tl-201
myocardial perfusion imaging. Am Heart J 1993; 125: 1323-8.
[44] Camici P, Chiriatti G, Lorenzoni R et al. Coronary vasodilatation is impaired in both hypertrophied and nonhypertrophied myocardium of patients with hypertrophic
cardiomyopathy: a study with nitrogen-13 ammonia and
positron emission tomography. J Am Coll Cardiol 1991; 17:
879-86.
[45] Neubauer S, Krahe T, Schindler R et al. 31 P magnetic
resonance spectroscopy in dilated cardiomyopathy and coronary artery disease. Altered cardiac high-energy phosphate
metabolism in heart failure. Circulation 1992; 86: 1810-8.
[46] Wexler LF, Lorell BH, Momomura S, Weinberg EO, Ingwall
JS, Apstein CS. Enhanced sensitivity to hypoxia-induced
diastolic dysfunction in pressure-overload left ventricular
hypertrophy in the rat: role of high-energy phosphate
depletion. Circ Res 1988; 62: 766-75.
[47] Vatner SF, Shannon R, Hittinger L. Reduced subendocardial
coronary reserve: a potential mechanism for impaired diastolic
function in the hypertrophied and failing heart. Circulation
1990; 81: 1118-14.
Eur Heart J, VoL 17, August 1996
Downloaded from by guest on October 21, 2014
[13] Higgins CB, Saeed M, Wendland M, Chew WM. Magnetic
resonance spectroscopy of the heart. Overview of studies in
animals and man. Invest Radiol 1989; 24: 962-8.
[14] Barrett EJ, Alger JR, Zaret BL. Nuclear magnetic resonance
spectroscopy: its evolving role in the study of myoardial
metabolism. J Am Coll Cardiol 1985; 6: 497-501.
[15] Menon RS, Hendrich K, Hu X, Ugurgil K. 31 P NMR
spectroscopy of the human heart at 4 T: detection of substantially uncontaminated cardiac spectra and differentiation of
subepicardium and subendocardium. Magn Reson Med 1992;
26: 368-76.
[16] Hetherington HP, Luney DJ, Vaughan T et al 3D 31 P
spectroscopic imaging of the human heart at 4.1 T. Magn
Reson Med 1995; 33: 427-31.
[17] van Dobbenburgh JO, de Jonge N, flopping C, Lahpor JR,
Woolley SR, van Echteld CJ. Postischemic alterations in
myocardial energy metabolism in heart transplant patients
[abstract]. Circulation 1993; 88: 1378.
[18] Lamb HJ, Doornbos J, den Hollander JA, Beyerbacht HP,
de Roos A. Strategies for cardiac " P - M R spectroscopy at
rest and during dobutamine stress: a study of reproducibility [abstract]. Society of Magnetic Resonance: Third
scientific meeting and exhibition; August 19-25, 1995; Nice,
France. Berkely Calif Society of Magnetic Resonance, 1995:
96.
[19] Ingwall JS. Is cardiac failure a consequence of decreased
energy reserve? Circulation 1993; 87: VII58-62.
[20] Ugurbil K. Magnetization-transfer measurements of individual rate constants in the presence of multiple reactions.
J Magn Reson 1985; 64- 207-19.
[21] Bittl JA, Ingwall JS. Intracellular high-energy phosphate
transfer in normal and hypertrophied myocardium. Circulation 1987; 75. 196—1101.
[22] Ingwall JS, Kramer MF, Fifer MA et al. The creatine kinase
system in normal and diseased human myocardium N Engl J
Med 1985; 313: 1050-4.
[23] Ingwall JS, Atkinson DE, Clarke K, Fetters JK. Energetic
correlates of cardiac failure: changes in the creatine kinase
system in the failing myocardium. Eur Heart J 1990; 11:
108-15
[24] Smith SH, Kramer MF, Reis I, Bishop SP, Ingwall JS.
Regional changes in creatine kinase and myocyte size in
hypertensive and nonhypertensive cardiac hypertrophy. Circ
Res 1990; 67: 1334-44
[25] Zhang J, Path G, Chepuri V et al. Responses of myocardial
high energy phosphates and wall thickening to prolonged
regional hypoperfusion induced by subtotal coronary stenosis.
Magn Reson Med 1993; 30: 28-37.
[26] Schaefer S, Camacho SA, Gober J et al. Response of myocardial metabolites to graded regional ischemia: 31 P NMR spectroscopy of porcine myocardium in vivo. Circ Res 1989; 64:
968-76.
[27] Wroblewski LC, Aisen AM, Swanson SD, Buda AJ. Evaluation of myocardial viability following ischemic and reperfusion injury using phosphorus 31 nuclear magnetic resonance
spectroscopy in vivo. Am Heart J 1990; 120: 31-9.
[28] Schaefer S, Schwartz GG, Steinman SIC, Meyerhoff DJ,
Massie BM, Weiner MW. Metabolic response of the human
heart to inotropic stimulation: in vivo phosphoms-31 studies
of normal and cardiomyopathic myocardium. Magn Reson
Med 1992; 25: 260-72.
[29] Heusch G, Schulz R. Chronische Myokardischamie —
hibernating myocardium: Merkmale und Grenzen. Z Kardiol
1993; 82(Suppl 5): 133-41.
[30] Wolfe CL, Moseley ME, Wikstrom M G d u l Assessment of
myocardial salvage after ischemia and reperfusion using magnetic resonance imaging and spectroscopy. Circulation 1989;
80: 969-82.
[31] Baer FM, Theissen P, Schneider CA, Voth E, Schicha H,
Sechtem U. Magnetresonanztomografische Untersuchungstechniken fur die myokardiale Vitalitatsdiagnostik. Herz 1994;
19: 51-64.
1165
1166 H. P. Beyerbacht et al.
[48] Bache RJ, Arentzcn CE, Simon AB, Vrobel TR Abnormalities in myocardial perfusion during tachycardia in dogs
with left ventricular hypertrophy metabolic evidence for
myocardial ischemia. Circulation 1984, 69' 409-17.
[49] Harmsen E, Schoemaker R, Yu J, Ruacka M, Leenen FHH.
Sensitivity to ischemic ATP breakdown in different models of
cardiac hypertrophy in rats. J Hypertens 1994; 12: 49-57.
[50] Lorell BH, Wexler LF, Momomura S, Weinberg E, Apstein
CS. The influence of pressure overload left ventricular hypertrophy on diastolic properties during hypoxia in isovolumically contracting rat hearts. Circ Res 1986; 58- 653-63.
[51] Schaefer S, Gober JR, Schwartz GG, Twieg DB, Weiner MW,
Massie B. In vivo phosphorus-31 spectroscopic imaging in
patients with global myocardial disease Am J Cardiol 1990;
65: 1154-61.
[52] Conway MA, Allis J, Ouwerkerk R, Niioka T, Rajagopalan
B, Radda GK. Detection of low phosphocreatine to ATP ratio
in failing hypertrophied human myocardium by 31 P magnetic
resonance spectroscopy. Lancet 1991; 338: 973-6.
[53] Neubauer S, Horn M, Mader H et al Clinical and hemodynamic correlates of impaired cardiac high-energy phosphate
metabolism in patients with aortic valve disease [abstract].
Proceedings of the Society fo Magnetic Resonance in Medicine; 1993 Augus 14-20; New York, NY USA. Berkeley,
Calif.: Society of Magnetic Resonance in Medicine, 1993: 55.
[54] Dell' Italia LJ, Evanochko WT, Blackwel) GG, den Hollander
J, Singleton HR, Pohost GM. Dissociation between mechanics and PCr/ATP in patients with volume overload hypertrophy [abstract]. Proceedings of the Society of Magnetic
Resonance in Medicine, 1993; August 14-20; New York, NY
USA. Berkeley, Calif.: Society of Magnetic Resonance in
Medicine, 1993: 356.
[55] Ito N, Isoyama S, Kuroha M, Takishima T. Duration of
pressure overload alters regression of coroanry circulation
abnormalities. Am J Physiol 1990. 258- HI753-60.
Downloaded from by guest on October 21, 2014
Eur Heart J. Vol. 17, August 1996









© Copyright 2026