
Full Text PDF - Suomen Neuropsykologinen Yhdistys ry
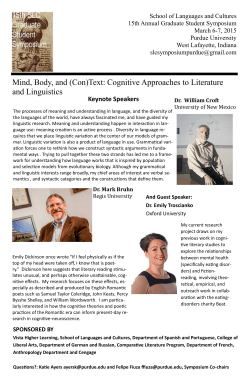
Integrating Interventions after Traumatic Brain Injury: A Synergistic Approach to Neurorehabilitation Kristen Dams-O’Connor and Wayne A. Gordon Department of Rehabilitation Medicine, Ichan School of Medicine at Mount Sinai, New York, NY, USA Deficits in attention, processing speed and executive functioning are among the most commonly reported and functionally limiting cognitive impairments among individuals with TBI. Changes in mood can exacerbate cognitive deficits and reduce life quality. Contemporary hierarchical models of cognitive functioning suggest that attention/arousal processes underlie and support higher-order functions. Building on decades of clinical research, a synergistic, integrative approach to neurorehabilitation is described, which combines bottom-up and top-town cognitive interventions in addition to psychotherapeutic interventions for mood. This approach is intended to address directly impairments in both foundational (i.e., attention) and higher-order (i.e., executive functions) processes. Executive dysfunction is addressed in a top-down fashion through the application of a series of problemsolving and emotional regulation modules that teach and integrate strategies that can be generalised across situations with practice. Attention, arousal and information processing are necessary prerequisites of successful higher-order thinking, attention skills, and are addressed in a bottom-up fashion through intensive individualised attention and processing training tasks. Combining top-down and bottom-up approaches within a comprehensive day-treatment programme can effect a synergistic improvement of overall functioning. Keywords: traumatic brain injury, neurorehabilitation, executive functioning Traumatic brain injury (TBI) can result in a wide range of consequences that include cognitive, behavioural, emotional and physical challenges; many of these can have a longstanding or lifelong impact on day-to-day functioning (Brown & Vandergoot, 1998; Dijkers, Brown, & Ashman, 2004; Ruff, 2005; Stratton & Gregory, 1995). Cognitive deficits commonly include impairments in attention, speed of information processing, memory and executive functioning (Gordon & Hibbard, 2005; Lezak, Howieson, & Loring, 2004). Injury-related alterations to neuromodulatory systems can also affect mood and behaviour (NIH Consensus Development Panel on Rehabilitation of Persons with Traumatic Brain Injury, 1999; Silver, McAllister, & Yudofsky, 2005), and there is often considerable psychological distress associated with adjustment to disability. Behavioural and emotional symptoms experienced after TBI may include depression, anxiety, impaired social communication, social isolation, post-traumatic stress, impulsivity, agitation/ aggression or apathy (Ashman, Gordon, Cantor, & Hibbard, 2006; Hibbard, Rendon, Charatz, & Kothera, 2005; Hibbard, Uysal, Kepler, Bogdany, & Silver, 1998). Commonly reported physical symptoms include fatigue, headaches, perception and visual changes, balance problems, seizures and endocrine dysfunction (Hibbard, Uysal, Sliwinski, & Gordon, 1998). There is tremendous heterogeneity across individuals in the constellation of symptoms Address for correspondence: Kristen Dams-O’Connor, PhD, Assistant Professor, Department of Rehabilitation Medicine, Ichan School of Medicine at Mount Sinai, One Gustave L. Levy Place, Box 1240, New York, NY 10029, USA. E-mail: Kristen.dams-o’[email protected] c The Author(s), published by Cambridge University Press on behalf of Australian BRAIN IMPAIRMENT VOLUME 14 NUMBER 1 MAY pp. 51–62 Academic Press Pty Ltd 2013 doi: 10.1017/BrImp.2013.9 51 KRISTEN DAMS-O’CONNOR AND WAYNE A. GORDON experienced after TBI. Therefore the degree of functional impairment associated with post-TBI deficits can vary greatly. The myriad consequences of TBI can impact multiple aspects of daily functioning, social relationships, community integration and quality of life. The cumulative impact of multiple deficits on daily functioning becomes particularly evident when one considers the fact that most tasks of daily living require the integration of multiple cognitive, behavioural and emotional skills. It is important to bear in mind that unlike more focal brain injuries such as stroke or neoplasm, TBI resulting from closed head injury usually causes diffuse injury throughout many areas of the brain and results in deficits in a variety of functional domains (Bernstein, 1999). A comprehensive, integrative approach to neurorehabilitation is required to rehabilitate the diverse array of capacities that support adaptive functioning. This manuscript presents an argument for an integrative approach to neurorehabilitation, and offers a model for a comprehensive neurorehabilitation intervention. Top-Down and Bottom-Up Interventions Cognitive rehabilitation interventions are commonly classified as either restorative or compensatory. Restorative or ‘bottom-up’ interventions target basic cognitive skills/functions such as arousal processes, attention and information processing, and directly engage these fundamental skills through repetitive drills or graded exercises (Mahncke, Bronstone, & Merzenich, 2006; Merzenich, Tallal, Peterson, Miller, & Jenkins, 1999). This approach is based on the notion that by training the brain to encode and process increasingly complex stimuli, more accurately and more quickly through intensive procedural learning, restoration of these basic cognitive functions may occur with repeated practice. Improvement of these foundational cognitive skills is theoretically an important prerequisite for advanced training in higher-order cognitive skills (memory, selfmonitoring, executive functioning), but restorative interventions alone are unlikely to generalise to untrained tasks (Cicerone et al., 2011). While there is some limited evidence suggesting that intensive bottom-up interventions can be associated with improvements on tasks of daily living (Edwards et al., 2002, 2005; Serino et al., 2007) and overall self-esteem (Parish & Oddy, 2007), most of the research suggests that significant gains are typically only seen in the specific tasks being trained. Although the exclusive use of therapist-led drills and exercises to remediate focal impairments is no 52 longer commonly seen in clinical contexts (Wilson, 1997), in more recent years a few computerised programmes designed to restore basic cognitive functions through computer-administered graded exercises have received preliminary empirical support (Barnes et al., 2009; Smith et al., 2009). Compensatory or ‘top-down’ approaches address deficits in higher-order ‘executive’ functions through the instruction and systematic practice of principles, strategies or rules that can be generalised across a variety of situations. Executive functions are a set of cognitive abilities that regulate and coordinate other abilities and behaviours. In defining executive functions, Cicerone and Giacino (1992) refer to the capacity for anticipation of consequences, goal formation, planning/organisation, initiation/execution of activities and self-monitoring, with correction of errors. Rieger and Gauggel (2002) cite planning, anticipation, action sequencing, cognitive flexibility, monitoring and inhibition as key components of executive function. Top-down interventions teach a guiding principle or rule for how to complete a higher-order task that can be applied across diverse contexts, as opposed to relying on ‘bottom-up’ approaches to re-learn a specific lower-order task or skill. In order to optimise self-regulation, metacognitive strategies rely on behavioural routines and internalisation of ‘self-talk’ to address executive function deficits (Cicerone & Giacino, 1992; Cicerone & Wood, 1987; Honda, 1999; Hux, Reid, & Lugert, 1994; O’Callaghan & Couvadelli, 1998). Individuals are trained to consciously use internal verbalisation of strategies and self-monitoring procedures across a variety of situations in which they experience difficulty (Mateer, 1999). Problem-solving deficits have been a primary focus of executive dysfunction interventions (Foxx, Martella, & Marchand Martella, 1989; Levine et al., 2000; Luria & Tsvetkova, 1964; Rath, Simon, Langenbahn, Sherr, & Diller, 2003; von Cramon, Matthes-von Cramon, & Mai, 1991; Webb & Glueckauf, 1994). One approach to problem solving training (D’Zurilla, 1988; D’Zurilla & Goldfried, 1971) teaches the patient ways to make available a variety of potentially effective response alternatives for dealing with problematic situations, and thereby increases the probability that the person will select the most effective response from among the various alternatives (D’Zurilla & Goldfried, 1971). The goal of training is to ensure that the pervasive problem-solving deficits of day-to-day life are addressed, rather than to provide the individual with discrete, situationbound learning strategies. Using this approach, executive dysfunction is addressed in a top-down fashion through a multistep process that generally A SYNERGISTIC APPROACH TO NEUROREHABILITATION involves recognising and defining a problem, identifying and choosing between possible solutions, enumerating steps required to enact the chosen solution, and evaluating the outcome (Ben-Yishay et al., 1985; D’Zurilla & Goldfried, 1971; Levine et al., 2000; Rath et al., 2003; von Cramon et al., 1991). By learning a set of guiding principles that can be applied across situations, the individual is able to learn to respond adaptively to situational demands as they arise. Metacognitive interventions can also be used to ameliorate deficits in more foundational functions by teaching executive strategies to manage environmental demands and monitor performance (e.g., time pressure management; Fasotti, Kovacs, Eling, & Brouwer, 2000). Compensatory strategies can involve the employment of external prostheses, such as a memory notebook or calendar. These external tools, which some may consider a bottomup intervention that replaces rather than restores once-intact skills, allow an individual with injuryrelated deficits to achieve similar functional outcomes through the systematic use of compensatory strategies. The over-arching goal of all metacognitive or top-down interventions is to allow processes that may have happened automatically prior to the TBI to become achievable through the deliberate use of structured compensatory strategies. Emotion and Neurorehabilitation A crucial element to consider within neurorehabilitation is the role and impact of emotions on the overall functioning of TBI survivors (Ashman et al., 2004; D’Zurilla, 1988; Prigatano, 1999). Changes in mood, emotional control and behavioural regulation represent common consequences of brain injury which may hinder or facilitate treatment and daily functioning. Put simply, our feelings impact our thoughts and behaviours. Emotional changes can result from neuropathological and neurochemical changes following TBI, stress disorders related to the traumatic events surrounding the injury, adjustment reactions to disability and injury-related limitations, pre-existing psychological factors, or a combination of each. The cognitive interventions discussed above do not traditionally address or incorporate emotional factors, although substantial research suggests that mood can impact motivation for treatment, participation and outcomes (e.g., Jorge, Robinson, Starkstein, & Arndt, 1994). Individuals with TBI often have difficulty regulating their emotions and behavioural reactions, which can result in inaction or impulsivity, and hinder the use of already-impaired thinking skills (Cicerone & Giacino, 1992; Gordon, Cantor, Ashman, & Brown, 2006a; Rath et al., 2003; Simon, 2001). Effective emotional regulation is considered a necessary prerequisite for problem solving and ‘clear thinking’ (Rath et al., 2003). To understand this concept, it is helpful to consider that productive, targeted thinking requires substantial cognitive energy. Cognitive energy is a finite resource, at least until it is restored through rest or relaxation. Emotional reactions can divert a substantial proportion of a person’s cognitive energy, resulting in diffusion and exhaustion of mental resources. Emotions, and the energy they require, must be monitored and calibrated to allow for purposeful adaptive functioning. Accordingly, it is important to integrate into cognitive remediation a treatment that addresses emotional reactions and the maladaptive self-talk that often accompanies negative emotions (Meichenbaum & Cameron, 1974). Strategy training that draws on tenets of cognitive behavioural therapy can facilitate emotional regulation, reduce impulsive reactions, provide alternatives to adynamic or ‘do nothing’ responses, and increase acceptance of problems as part of life. The ability to regulate emotions can foster a person’s confidence in his or her ability to cope with and solve problems (D’Zurilla, 1988), both in general and in the moment (i.e., during an emotionally charged situation). Finally, emotion recognition and emotional regulation strategies assist individuals in understanding the ways in which emotions affect cognitive functioning, thereby facilitating awareness of the functional impact of the TBI. Functionally Relevant Neurorehabilitation The traditionally drawn distinction between restorative interventions and compensatory interventions has motivated clinicians and researchers to debate which is superior, which creates the impression that a clinician should choose one of these approaches to guide his or her work with cognitively compromised individuals. However, it is clear that ‘real-world’ tasks do not require either foundational attention/arousal skills or executive abilities. Instead, everyday tasks require multiple cognitive systems that work together in an integrated fashion. Although bottom-up and top-down interventions may facilitate improvements in both trained and untrained domains of functioning, neither alone is likely to promote lasting functional improvement. Bottom-up approaches are essential ingredients to improving basic capacities for attention and arousal, which are necessary prerequisites 53 KRISTEN DAMS-O’CONNOR AND WAYNE A. GORDON for learning, memory and other higher functions. However, transfer of skills to complex tasks of daily living is a challenge that is difficult to meet with bottom-up interventions alone. Top-down approaches provide generalizable strategies or guiding principles that are widely applicable and relevant for ‘real-world’ functioning, but without adequate attention and information processing skills, the individual will be unable to learn, remember, process and incorporate feedback from the environment. Real-world functioning requires the integration of foundational and higher-order cognitive skills. Moreover, cognition does not occur in isolation: emotions and emotional reactions can support or undermine the effective use of cognitive skills. Thus the rationale for providing an integrative intervention is clear: meaningful improvements in productive real-world functioning can be achieved through the incorporation of bottom-up and topdown cognitive training along with emotional regulation training. Empirical and Theoretical Support for an Integrative Approach to Neurorehabilitation Evidence-based reviews have suggested that the most efficacious approach to cognitive rehabilitation is comprehensive day-treatment programmes (CDTPs) that include individual and group sessions for several hours per day, several days per week (Ben-Yishay et al., 1985; Cicerone et al., 2000, 2005). These programmes include a series of bottom-up and top-down approaches to cognitive rehabilitation, and many also strive to address mood and adjustment issues. Across several studies, CDTPs have been shown to be effective in improving rehabilitation outcomes, including cognition and mood (Ben-Yishay et al., 1985; Cicerone et al., 2000, 2005; Cicerone, Levin, Malec, Stuss, & Whyte, 2006; Cicerone, Mott, Azulay, & Friel, 2004; Donnelly et al., 2011; Gordon et al., 2006b; Klonoff, Lamb, & Henderson, 2000; Klonoff, Lamb, Henderson, & Shepherd, 1998; Malec, 2001; Malec & Basford, 1996; Scherzer, 1986). Given the diversity and range of symptoms experienced by survivors of TBI, the benefit of CDTPs is that they are designed to address a wide range of post-TBI cognitive and behavioural difficulties. Research suggests that many cognitive skills are functionally interrelated, providing support for comprehensive neurorehabilitation. Executive functioning, problem solving, emotional regulation and learning are mediated by atten54 tion and processing speed. Deficits in executive functioning are among the most disabling consequences of TBI, as they pose considerable challenge to social autonomy, community integration and vocational success (McDonald, Flashman, & Saykin, 2002; Sohlberg & Mateer, 1987). Clearly, being able to attend to external and internal events and process information accurately is a core prerequisite for intentional learning, emotional regulation and problem solving. Shallice (1981) postulates that regulation and verification of behaviour are controlled by an attentional supervisory executive system. Stuss, Shallice, Alexander, & Picton (1995) view attention, memory and executive functions as intimately related, and Stuss and Benson’s (1986) hierarchical model of cerebral organisation defines attention as the foundation of the hierarchy of functional systems. Indeed, several studies (Gray, Robertson, Pentland, & Anderson, 1992; Niemann, Ruff, & Baser, 1990; Sohlberg & Mateer, 1987; Sturm, Willmes, Orgass, & Hartje, 1997) have demonstrated that individuals with executive dysfunction benefit from interventions to improve attention. Research has also shown that processing speed is an important determinant of executive function (Frencham, Fox, & Maybery, 2005; Nelson, Yoash-Gantz, Pickett, & Campbell, 2009; Rassovsky et al., 2006). CDTPs are well positioned to address these functionally relevant challenges by addressing basic and more sophisticated cognitive functions using a variety of interventions. Top-down interventions for executive dysfunction are often embedded in CDTPs to enhance their efficacy. For example, Scherzer (1986) found that the effectiveness of a CDTP was significantly enhanced when a problem-solving approach was incorporated in the programme. These interventions not only view problem-solving from a neuropsychological perspective (Ben-Yishay et al., 1985; Levine et al., 2000; Luria, 1963), but also take into account the motivational, emotional and attitudinal factors that affect the problem-solving process as it unfolds in ‘real life’ (Rath et al., 2003). Intervention research on programmes other than CDTPs suggests that restorative interventions have a greater functional impact and are more effective when combined with training in compensatory or metacognitive strategies (Cicerone et al., 2005). Several studies have demonstrated the importance of incorporating both direct restorative interventions and compensatory strategy training to maximise treatment results and to enhance generalisation of learned skills to community activities (Meinzer, Djundja, Barthel, Elbert, & Rockstroh, 2005; Poggel, Kasten, & Sabel, 2004; Sohlberg et al., 2003; Tiersky et al., 2005). A SYNERGISTIC APPROACH TO NEUROREHABILITATION Guiding Principles for the Development of an Integrative Neurorehabilitation Intervention An integrative approach to neurorehabilitation for the diversity of TBI-related deficits is supported by the following clinically and empirically supported principles (Ben-Yishay et al., 1985; Cicerone et al., 2004, 2005; Gordon et al., 2006a; Malec, 2001): (a) effective ‘real-world’ functioning requires both basic and complex cognitive skills; (b) higher-order cognitive skills, such as self-monitoring, problem solving, and acquisition and execution of metacognitive strategies, are all mediated by foundational skills of attention and arousal; and (c) emotional factors can either facilitate or hinder effective cognitive functioning. Real-world Tasks are not Domain Specific It may be impossible to identify a real-life situation in which only one circumscribed cognitive skill is required (Sun & Zhang, 2004). Making a cup of tea requires sustained attention, sequencing, memory and executive self-monitoring skills. Even rote tasks, such as brushing one’s teeth, can require executive input when unanticipated events arise (e.g., running out of toothpaste). Similarly, most cognitive rehabilitation interventions, including those traditionally described as being either restorative or compensatory, do not rely exclusively on one or the other approach. It is well known that all learning (whether facilitated by bottom-up or top-down approaches) is a product of use-induced changes in the brain’s structure and functional organization (Buonomano & Merzenich, 1998). The distinction between compensatory and restorative approaches is actually quite nebulous, and attempts to design and deliver exclusively restorative or compensatory interventions do not reflect the multidimensionality of real-world functional task demands. Foundational Cognitive Skills Underlie and Support Higher-order Thinking There is a growing body of evidence that demonstrates that a central mechanism supporting all learning is the interaction between bottom-up and top-down neurocognitive processes that is made possible by structural and functional connections between underlying neural systems. Evidence suggests that the primary sensory cortex and posterior cortical regions play an important role in bottomup processes, and the frontal–parietal association cortex is involved in top-down processes (Adcock et al., 2009). The intricate interconnectedness of these neural systems is essential for adequate func- tioning. Basic science research on auditory processing conducted using animal models suggests, for example, that enduring receptive field plasticity in the adult auditory cortex requires repeatedly presented sensory stimuli, which are shaped by top-down regulatory mechanisms in the prefrontal cortex, parietal cortex or higher auditory areas (Polley, Steinberg, & Merzenich, 2006). Experimental evidence in humans reveals that cognitive processes that are typically classified as topdown behavioural phenomena, such as executive control and self-monitoring, require the integration of multiple brain systems, and rely on input from both primary sensory and cortical areas (Kastner, De Weerd, Desimone, & Ungerleider, 1998; Kastner & Ungerleider, 2000). When sensory inputs are unclear, undifferentiated or ‘noisy’, there is a greater cognitive load involved in the processing of these inputs, which results in impaired functioning due to competition for top-down cognitive resources (Adcock et al., 2009). Emotions Mediate Clear Thinking TBI-related cognitive deficits rarely exist in isolation: when a TBI survivor becomes aware of functional consequences of these deficits he or she can experience feelings of anxiety, frustration, failure and helplessness. When an individual finds himself unable to return to pre-injury roles and responsibilities, he must begin an often painful process of renegotiating and reconstructing an identity (Levack, Kayes, & Fadyl, 2010). The feelings of loss and sadness that can accompany this process can influence motivation for treatment, participation in the community and maintenance of social support networks. On a more immediate level, the in-the-moment experience of deficitrelated failure can cause a cascade of physiological changes, thoughts and feelings that serve to overwhelm cognitive resources, resulting in cognitive ‘flooding’ that derails effective thinking. Previous research suggests that providing training in cognitive behavioural strategies for emotional selfregulation (D’Zurilla & Goldfried, 1971; D’Zurilla & Nezu, 2001) prior to initiating metacognitive strategy training for problem-solving disorders results in improvements in self-reported problemsolving abilities and role-playing activities, which were maintained 6 months post treatment (Rath et al., 2003). The Pyramid of Cognitive Functioning: A Hierarchical Model A visual model of TBI-related impairments helps to conceptualise the treatment needs of individuals 55 KRISTEN DAMS-O’CONNOR AND WAYNE A. GORDON FIGURE 1 (Colour online) A hierarchical model of cognitive functioning. with TBI. Cognitive processes can be functionally described as being hierarchically organised into a pyramid in which foundational skills such as attention, arousal and processing speed are at the bottom of the pyramid. These basic skills underlie and support higher-order, more complex functions that are located at the top of the pyramid. An individual with TBI have can have a range of deficits in both basic skills and higher-order functions. Therefore, a comprehensive approach to neurorehabilitation that integrates the treatment of both foundational and supervisory skills through a combination of bottom-up and top-down interventions (see Figure 1) is needed in order to provide patients with the maximum opportunity to benefit from treatment. This pyramidal structure is based partially on a hierarchical model of independent but interactive brain operations proposed by Stuss and Benson (1986), and supports an integrative approach to treatment that is based on clinical and empirical evidence ((Ben-Yishay et al., 1985; Cicerone et al., 2004; Gordon et al., 2006a; Malec, 2001). As seen in Figure 1, at the base of the hierarchy lie the foundational skills of arousal, attention, and drive or motivation. The abilities to maintain arousal and alertness, initiate activation, and attend to external and internal events are core prerequisites for information processing, which is 56 necessary for intentional learning and subsequent recall. The ability to assimilate and integrate information and sensory experiences relies upon the accurate input and processing of incoming information. Thus, memory and learning are hampered by problems with attention and decreased processing speed. Next in the hierarchy are the executive or higher-order functions of goal-setting, anticipation and problem-solving. These executive functions integrate incoming information across domains of cognitive skills in order to successfully orchestrate and execute cognitive tasks. The top of the pyramid represents supervisory control, also known as the ability to self-monitor and make use of internal and external feedback. Based on elaborate networks of sensory, perceptual and cognitive input from all levels of the cognitive hierarchy, these functions adjust and direct ongoing automatic and intentional behaviours. Two psychological processes that can support or thwart functioning at any level of this pyramid are emotions and self-awareness. It is well known that poor emotional regulation can undermine and disrupt adaptive functioning directly and by interacting with and exacerbating cognitive impairments. Emotional control can help an individual to manage perseverative or impulsive responding, regulate and monitor emotional reactions, A SYNERGISTIC APPROACH TO NEUROREHABILITATION inhibit mood-related distractions, and facilitate clear thinking (Rath et al., 2003). Similarly, awareness of deficits can support adaptation, while low awareness (a common sequela of TBI) can be a major barrier to successful rehabilitation (Prigatano & Schacter, 1991). Awareness can be understood as the ability to use feedback from the environment and monitor performance, and adjust one’s strategy based on this information. Unawareness of deficits can negatively impact functioning (e.g., failure to recognise a memory problem, and needing to make several trips to the store due to refusal to use compensatory tools such as a grocery list). Individuals with reduced awareness are unlikely to be motivated to engage in rehabilitation aimed at ameliorating those deficits. Moreover, since changes in awareness are often accompanied by changes in mood or emotional state (particularly as individuals begin to appreciate the severity or chronicity of their impairments) (Lezak & O’Brien, 1990), the interaction between emerging awareness and the accompanying emotional reactions is likely to influence (enhance or degrade) cognitive functioning at any level of the hierarchy. TBI may affect one or more skills at any level in the hierarchy (Sohlberg, Mateer, & Stuss, 1993). As can be seen in this visual model (Figure 1), an interruption in functioning at any level in the hierarchy can impact overall adaptive functioning. For example, disruption at the most fundamental level may result in inability to initiate or carry out previously automatic tasks effectively (e.g., grooming); whereas disruption of executive control may result in poor planning, organisation and sequencing of components of more complex behaviour or inappropriate triggering of behavioural responses. Applying an Integrative Model of Neurorehabilitation The essential feature of an integrative approach to neurorehabilitation is the incorporation of both bottom-up and top-down approaches into all training activities, and emotional aspects of adjustment are addressed throughout training. This does not mean that restorative and compensatory approaches should be offered as distinct aspects of a training programme (i.e., first training attention skills and then treating executive functions), but rather that both approaches should be incorporated throughout programme activities and provided simultaneously. Individually tailored metacognitive strategies will be identified and practised during training of foundational cognitive skills, and principles of restorative interventions (e.g., practice and repetition) will add predictability and structure to metacognitive training for executive dysfunction. The rationale for integrating restorative, compensatory and metacognitive approaches should be made explicit during training, as explaining the intent and functional relevance of the interventions will allow individuals with TBI to be active participants in their neurorehabilitation. Moreover, the relevance and applicability of specific strategies or compensations to other cognitive domains or untrained tasks should be pointed out to facilitate generalisation of training. Strategies for managing emotional reactions and adjustment-related issues are embedded throughout training, instead of being offered as distinct components (e.g., individual psychotherapy) of the intervention. The integrative approach described herein builds on relevant empirical literature and clinical observations from comprehensive day-treatment programmes for individuals with TBI. Integrated Remediation of Foundational Cognitive Skills Intensive training of attention and processing skills strengthens the fundamental skills that are required for daily functioning, and facilitates the learning and implementation of higher-order metacognitive strategies. Attention training involves the use of empirically supported interventions that target and selectively train attention using graded, systematic exercises (Sohlberg & Mateer, 1987). Whereas a purely restorative approach might involve repetitive drill exercises to retain specific abilities, an integrative approach incorporates metacognitive strategies, highlights the personal relevance of trained tasks and strategies, and thereby maximises generalisation of training to everyday tasks. The provision of feedback by a trained therapist during structured bottom-up tasks is essential to the integrative approach. Individually tailored feedback facilitates awareness of strengths and weaknesses, and teaches an individual to monitor and correct behaviour. Feedback can also allow training tasks to serve as an experiential demonstration of the ways in which factors such as neurofatigue, emotional dysregulation and motivation can interact with basic cognitive skills. One example of an awareness-building intervention (Goverover, Johnston, Toglia, & Deluca, 2007) that can be incorporated into the training of foundational cognitive skills involves asking the participant to define their goal for a particular task, predict their performance, anticipate barriers or obstacles and identify strategies to overcome them, and compare actual with expected performance immediately following task completion. Ever vigilant of the impact of emotions on cognitive functioning, 57 KRISTEN DAMS-O’CONNOR AND WAYNE A. GORDON the therapist orchestrates a collaborative, almost empirical approach: together, as a team, the therapist and patient gather data (objective performance on training tasks) to either confirm or modify a patient’s perceived abilities, and to identify and circumvent barriers to success. In some ways, the training tasks themselves serve as a vehicle for the development of individualised metacognitive strategies that can be used to maximise attention (i.e., breaking a task into smaller pieces, removing external distractions during the task that require focus, taking rest breaks). These skills provide a foundation for the learning and practice of topdown strategies used in the treatment of executive dysfunction. Individually tailored attention strategies can be applied throughout the programme, including during the learning of metacognitive compensatory strategies and emotional regulation strategies, to maximise concentration during learning of these higher-order skills. During training of foundational skills, emotional reactions should be addressed pre-emptively, and also as they arise. Emotions and the thoughts, physiological reactions, and behaviours that can accompany them are an excellent example of internal distractions, and can be discussed in this context in the early stages of cognitive remediation. If an emotional internal distraction is identified prior to or during a cognitive training session (e.g., I got in an argument with my friend this morning and I’m still upset about it), metacognitive strategies for emotional regulation can be employed in the moment. Similarly, participation in structured cognitive tasks and receiving feedback can provide awareness of emotional triggers. Feelings of failure or frustration can serve as cognitive distractions, and anxiety over the implications of task performance can undermine further productive cognitive training during that session. Cognitive behavioural therapy approaches can be helpful in identifying thoughts that accompany these emotions (e.g., I made far more errors than I had hoped; now I’ll never be able to work again), and deconstructing and reframing maladaptive self-talk. It is appropriate to recognise and label cognitively demanding tasks as an emotional trigger, so that the patient can practice individually tailored strategies to prepare for the feelings that may arise (e.g., initiating deep breathing exercises to achieve a feeling of calm before starting the training task). Integrative Remediation of Executive Functions A top-down approach, in which guiding rubrics or processes are taught that can be generalised across situations, is ideal for remediating execu58 tive deficits. First, from a theoretical perspective, the hierarchical organisation of cognitive functions – with executive functions controlling subsidiary mental operations – suggests that top-down approaches are likely to be most effective in treating executive dysfunction (Stuss & Benson, 1986). Second, top-down approaches, by their very nature are more likely to generalise across situations and lead to enduring functional change. This can be facilitated by contextualising training activities into the daily lives of participants. Third, empirical findings consistently support the efficacy of top-down approaches to cognitive rehabilitation (Cicerone et al., 2000; Cicerone & Giacino, 1992; Levine et al., 2000; Ownsworth & Mcfarland, 1999). Problem-solving training is one commonly cited example of using a metacognitive step-bystep approach to treat executive deficits. Although several empirically supported problem-solving interventions exist (Cicerone et al., 2005, 2011), most involve identifying and defining the problem, generating alternative solutions, choosing between viable alternatives, implementing a plan based on the chosen solution, and evaluating the outcome of this process (Gordon et al., 2006a). Constant repetition and practice of the trained metacognitive strategies is encouraged across diverse situations and contexts. An integrative approach to neurorehabilitation emphasises the fact that extensive practice is required for learning and eventual habituation of metacognitive skills. The goal is that with sufficient practice the metacognitive skills being worked on will ‘kick in’ automatically when they are needed. As discussed above, the incorporation of individualised strategies indentified in attention training and a constant emphasis on structure and self-monitoring can maximise learning and independence in executive tasks. Implementing a problem-solving plan, for example, is an exercise that requires attention to detail and self-monitoring to ensure accuracy. The same individualised skills and methods that are identified and implemented during training of these foundational skills (e.g., removing distractions, building in external reminders, double-checking for accuracy) should be implemented during the execution of metacognitive strategies. External compensations can be incorporated for individuals whose cognitive impairments cannot be ameliorated through restorative and metacognitive approaches alone. For example, an alarm reminder system may help a person who has difficulty initiating or who forgets to stop and check for errors during a task. External tools can also scaffold and strengthen gains made in restorative and metacognitive interventions. For example, A SYNERGISTIC APPROACH TO NEUROREHABILITATION keeping a written log of deficits and compensatory strategies as they are identified during restorative interventions can help a person to achieve fuller awareness of injury-related deficits and the strategies that have been helpful in the past. A planner or memory notebook can be used to help a person organise his or her time. More specifically, a planner can be used to schedule time to implement components of a plan that is identified through a metacognitive problem-solving exercise. The steps involved in a particular metacognitive strategy can be recorded on a wallet-sized card, abbreviated with an acronym and printed on a bracelet, or otherwise cued by external memory aids that facilitate generalisation of strategies to everyday activities. Emotional reactions can be explicitly addressed by providing metacognitive training in emotion regulation, through the incorporation of top-down principles for processing and modulating emotional reactions. For example, individuals might be taught a series of strategies to maximise emotional regulation when confronted with problematic situations. One strategy involves the observation of behaviours, emotions, thoughts and physiological experiences that are manifest during a problem situation, and identifying the ways in which these reactions can interfere with cognitive functioning. Another strategy involves the identification of precursors to problem situations or identification of triggers for maladaptive emotional responses. A final, but crucial, strategy involves the reframing of problem situations, and identifying and practising more adaptive emotional, cognitive and behavioural reactions. As described elsewhere (Gordon et al., 2006b), the emotional and cognitive components of executive function are so intricately interconnected that concurrent treatment is warranted. In order for these principles to be implemented an individual must be able to recognise triggers of distressing and maladaptive emotions and their physiological, cognitive, behavioural and emotional consequences. Awareness of these factors can be facilitated by repetitive practice of structured self-monitoring exercises to observe physical sensations, thoughts and feelings in response to emotional triggers. As discussed above, constant repetition and practice of metacognitive strategies is required for the learning and eventual habituation of adaptive emotion regulation skills. Conclusions An integrative approach to neurorehabilitation combines top-down and bottom-up approaches with cognitive behaviourally based interventions for emotional regulation within a comprehensive neurorehabilitation programme to exert a synergistic impact on improving overall day-to-day functioning. It is recognised that neither a restorative nor compensatory approach alone is sufficient for real-world functional change; instead, beneficial effects of both top-down and bottomup approaches are enhanced by their integration. Bottom-up attention training can improve sustained attention, inhibition of distraction and arousal regulation. Improvements in these areas allow for more efficient learning and initiation of top-down strategies, which enhance the ability to benefit from strategy training. Improvements in real-world functioning require an integrative approach that addresses emotional and adjustment reactions in addition to simultaneously employing both top-down and bottom-up approaches in the remediation of cognitive and functional skills after TBI. Acknowledgements This work was supported by Grant No. H133B040033, National Institute on Disability and Rehabilitation Research, US Department of Education; Grant No. 5R49-CE-001171, Centers for Disease Control and Prevention. The authors report no conflict of interests. References Adcock, R.A., Dale, C., Fisher, M., Aldebot, S., Genevsky, A., Simpson, G. V., . . . Vinogradov, S. (2009). When top-down meets bottom-up: Auditory training enhances verbal memory in schizophrenia. Schizophrenia Bulletin, 35(6), 1132–1141. Ashman, T.A., Gordon, W.A., Cantor, J.B., & Hibbard, M.R. (2006). Neurobehavioral consequences of traumatic brain injury. The Mount Sinai Journal of Medicine, New York, 73(7), 999–1005. Ashman, T.A., Spielman, L.A., Hibbard, M.R., Silver, J.M., Chandna, T., & Gordon, W.A. (2004). Psychiatric challenges in the first 6 years after traumatic brain injury: Cross-sequential analyses of axis I disorders. Archives of Physical Medicine and Rehabilitation, 85(4 Suppl 2), S36–42. Barnes, D., Yaffe, K., Belfor, N., Jagust, W.J., DeCarli, C., Reed, B.R., . . . Kramer, J.H. (2009). Computerbased cognitive training for mild cognitive impairment: Results from a pilot randomized, controlled trial. Alzheimer Disease and Associated Disorders, 23(3), 205–210. Ben-Yishay, Y., Rattock, J., Lakin, P., Piasetsky, E.B., Ross, B., Silver, S., . . . Ezrachi, O. (1985). Neuropsychological rehabilitation: Quest for a holistic approach. Seminars in Neurology, 5, 252–258. Bernstein, D.M. (1999). Recovery from mild head injury. Brain Injury, 13, 151–172. 59 KRISTEN DAMS-O’CONNOR AND WAYNE A. GORDON Brown, M., & Vandergoot, D. (1998). Quality of life for individuals with traumatic brain injury: Comparison with others living in the community. The Journal of Head Trauma Rehabilitation, 13(4), 1–23. Buonomano, D.V., & Merzenich, M.M. (1998). Cortical plasticity: From synapses to maps. Annual Review of Neuroscience, 21, 149–186. Cicerone, K.D., Dahlberg, C., Kalmar, K., Langenbahn, D.M., Malec, J.F., Bergquist, T.F., . . . Morse, P.A. (2000). Evidence-based cognitive rehabilitation: Recommendations for clinical practice. Archives of Physical Medicine and Rehabilitation, 81(12), 1596–1615. Cicerone, K.D., Dahlberg, C., Malec, J.F., Langenbahn, D.M., Felicetti, T., Kneipp, S., . . . Catanese, J. (2005). Evidence-based cognitive rehabilitation: Updated review of the literature from 1998 through 2002. Archives of Physical Medicine and Rehabilitation, 86(8), 1681–1692. Cicerone, K., & Giacino, J. (1992). Remediation of executive function deficits after traumatic brain injury. NeuroRehabilitation, 2(3), 12–22. Cicerone, K.D., Langenbahn, D.M., Braden, C., Malec, J.F., Kalmar, K., Fraas, M., . . . Ashman, T. (2011). Evidence-based cognitive rehabilitation: Updated review of the literature from 2003 through 2008. Archives of Physical Medicine and Rehabilitation, 92(4), 519–530. Cicerone, K., Levin, H., Malec, J., Stuss, D., & Whyte, J. (2006). Cognitive rehabilitation interventions for executive function: Moving from bench to bedside in patients with traumatic brain injury. Journal of Cognitive Neuroscience, 18(7), 1212– 1222. Cicerone, K.D., Mott, T., Azulay, J., & Friel, J.C. (2004). Community integration and satisfaction with functioning after intensive cognitive rehabilitation for traumatic brain injury. Archives of Physical Medicine and Rehabilitation, 85(6), 943–950. Cicerone, K.D., & Wood, J.C. (1987). Planning disorder after closed head injury: A case study. Archives of Physical Medicine and Rehabilitation, 68(2), 111– 115. Dijkers, M.P., Brown, M., & Ashman, T. (2004). ‘Services’ may not be the answer to many needs after disability. Archives of Physical Medicine and Rehabilitation, 85, E12–E13. Donnelly, K., Donelly, J., Dunnam, M., Warner, G., Kittelson, C., Constance, J., . . . Alt, M. (2011). Relability, sensitivity, and specificitiy of the VA traumatic brain injury screening tool. Journal of Head Trauma Rehabilitation, 26(6), 439–453. D’Zurilla, T. (1988). Problem-solving therapies. In K. Dobson (Ed.), Handbook of cognitive-behavioral therapies. New York: Guilford Press. D’Zurilla, T.J., & Goldfried, M.R. (1971). Problem solving and behavior modification. Journal of Abnormal Psychology, 78(1), 107–126. D’Zurilla, T. J., & Nezu, A.M. (2001). Problem-solving therapies. In K.S. Dobson (Ed.), Handbook of cogni- 60 tive behavioral therapies (pp. 211–245). New York: Guilford Press. Edwards, J.D., Wadley, V.G., Myers, R.S., Roenker, D.L., Cissell, G.M., & Ball, K.K. (2002). Transfer of a speed of processing intervention to near and far cognitive functions. Gerontology, 48(5), 329–340. Edwards, J.D., Wadley, V.G., Vance, D.E., Wood, K., Roenker, D.L., & Ball, K.K. (2005). The impact of speed of processing training on cognitive and everyday performance. Aging & Mental Health, 9(3), 262–271. Fasotti, L., Kovacs, F., Eling, P.A., & Brouwer, W.H. (2000). Time pressure management as a compensatory strategy training after closed head injury. Neuropsychological Rehabilitation, 10 (1), 47–65. Foxx, R.M., Martella, R.C., & Marchand Martella, N.E. (1989). The acquisition, maintenance, and generalization of problem-solving skills by closed headinjured adults. Behavior Therapy, 20(1), 61–76. Frencham, K.A., Fox, A.M., & Maybery, M.T. (2005). Neuropsychological studies of mild traumatic brain injury: A meta-analytic review of research since 1995. Journal of Clinical and Experimental Neuropsychology, 27(3), 334–351. Gordon, W.A., Cantor, J., Ashman, T., & Brown, M. (2006a). Treatment of post-TBI executive dysfunction: Application of theory to clinical practice. Journal of Head Trauma Rehabilitation, 21(2), 156–167. Gordon, W.A., & Hibbard, M.R. (2005). Cognitive rehabilitation. In J.M. Silver, S.C. Yudoffsky & T.W. McAllister (Eds.), Neuropsychiatry of traumatic brain injury (2nd ed., pp. 655–660). Washington, DC: American Psychiatric Press. Gordon, W.A., Zafonte, R., Cicerone, K., Cantor, J., Brown, M., Lombard, L., . . . Chandna, T. (2006b). Traumatic brain injury rehabilitation: State of the science. American Journal of Physical Medicine & Rehabilitation/Association of Academic Physiatrists, 85(4), 343–382. Goverover, Y., Johnston, M.V., Toglia, J., & Deluca, J. (2007). Treatment to improve self-awareness in persons with acquired brain injury. Brain Injury 21(9), 913–923. Gray, J.M., Robertson, I., Pentland, B., & Anderson, S. (1992). Microcomputer-based attentional retraining after brain damage: A randomised group controlled trial. Neuropsychological Rehabilitation, 2(2), 97– 115. Hibbard, M.R., Rendon, D., Charatz, H., & Kothera, L. (2005). CBT in individuals with traumatic brain injury. In S.M. Freeman, & A. Freeman (Eds.), Cognitive behavior therapy in nursing practice (pp. 189– 220). New York: Springer. Hibbard, M.R., Uysal, S., Kepler, K., Bogdany, J., & Silver, J. (1998). Axis I psychopathology in individuals with traumatic brain injury. Journal of Head Trauma Rehabilitation, 13(4), 24–39. Hibbard, M.R., Uysal, S., Sliwinski, M., & Gordon, W.A. (1998). Undiagnosed health issues in individuals with traumatic brain injury living in the A SYNERGISTIC APPROACH TO NEUROREHABILITATION community. Journal of Head Trauma Rehabilitation, 13(4), 47–57. Honda, T. (1999). Rehabilitation of executive function impairments after stroke. Topics in Stroke Rehabilitation, 6(1), 15–22. Hux, K., Reid, R., & Lugert, M. (1994). Self-instruction training following neurological injury. Applied Cognitive Psychology, 8(3), 259–271. Jorge, R.E., Robinson, R.G., Starkstein, S.E., & Arndt, S.V. (1994). Influence of major depression on 1-year outcome in patients with traumatic brain injury. Journal of Neurosurgery, 81(5), 726–733. Kastner, S., De Weerd, P., Desimone, R., & Ungerleider, L.G. (1998). Mechanisms of directed attention in the human extrastriate cortex as revealed by functional MRI. Science, 282(5386), 108–111. Kastner, S., & Ungerleider, L.G. (2000). Mechanisms of visual attention in the human cortex. Annual Review of Neuroscience, 23, 315–341. Klonoff, P.S., Lamb, D.G., & Henderson, S.W. (2000). Milieu-based neurorehabilitation in patients with traumatic brain injury: Outcome at up to 11 years postdischarge. Archives of Physical Medicine and Rehabilitation, 81(11), 1535–1537. Klonoff, P.S., Lamb, D.G., Henderson, S.W., & Shepherd, J. (1998). Outcome assessment after milieu-oriented rehabilitation: New considerations. Archives of Physical Medicine and Rehabilitation, 79(6), 684–690. Levack, W.M., Kayes, N.M., & Fadyl, J.K. (2010). Experience of recovery and outcome following traumatic brain injury: A metasynthesis of qualitative research. Disability and Rehabilitation, 32(12), 986–999. Levine, B., Robertson, I.H., Clare, L., Carter, G., Hong, J., Wilson, B.A., . . . Stuss, D.T. (2000). Rehabilitation of executive functioning: An experimentalclinical validation of goal management training. Journal of the International Neuropsychological Society, 6(3), 299–312. Lezak, M.D., Howieson, D.B., & Loring, D.W. (2004). Neuropsychological assessment (4th ed.). Oxford: Oxford University Press. Lezak, M.D., & O’Brien, K. P. (1990). Chronic emotional, social, and physical changes after traumatic brain injury. In E.D. Bigler (Ed.), Traumatic brain injury: Mechanisms of damage, assessment, intervention, and outcome (pp. 365–380). Austin, Texas: Pro-Ed. Luria, A.R. (1963). Restoration of function after brain injury. New York: Basic Books. Luria, A.R., & Tsvetkova, I.D. (1964). The programming of constructive abilities in local brain injuries. Neuropsychologia, 2, 95–95.108. Mahncke, H.W., Bronstone, A., & Merzenich, M.M. (2006). Brain plasticity and functional losses in the aged: Scientific bases for a novel intervention. Progress in Brain Research, 157, 81– 109. Malec, J.F. (2001). Impact of comprehensive day treatment on societal participation for persons with ac- quired brain injury. Archives of Physical Medicine and Rehabilitation, 82(7), 885–895. Malec, J.F., & Basford, J.S. (1996). Postacute brain injury rehabilitation. Archives of Physical Medicine and Rehabilitation, 77(2), 198–207. Mateer, C.A. (1999). Executive function disorders: Rehabilitation challenges and strategies. Seminars on Clinical Neuropsychiatry, 4, 50–59. McDonald, B.C., Flashman, L.A., & Saykin, A.J. (2002). Executive dysfunction following traumatic brain injury: Neural substrates and treatment strategies. NeuroRehabilitation, 17(4), 333–344. Meichenbaum, D., & Cameron, R. (1974). The clinical potential of modifying what clients say to themselves. Psychotherapy: Theory, Research and Practice, 11(2), 103–117. Meinzer, M., Djundja, D., Barthel, G., Elbert, T., & Rockstroh, B. (2005). Long-term stability of improved language functions in chronic aphasia after constraint-induced aphasia therapy. Stroke; a Journal of Cerebral Circulation, 36(7), 1462–1466. Merzenich, M.M., Tallal, P., Peterson, B., Miller, S.L., & Jenkins, W.M. (1999). Some neurological principles relevant to the origins of – and the cortical plasticity-based remediation of –developmental language impairments. In J. Grafman (Ed.), Neuronal plasticity: Building a bridge from the laboratory to the clinic (pp. 169). New York: Springer-Verlag. Nelson, L., Yoash-Gantz, R., Pickett, T., & Campbell, T. (2009). Relationship between processing speed and executive functioning performance among OEF/OIF veterans: Implications for postdeployment rehabilitation. Journal of Head Trauma Rehabilitation, 24(1), 32. Niemann, H., Ruff, R.M., & Baser, C.A. (1990). Computer-assisted attention retraining in headinjured individuals: A controlled efficacy study of an outpatient program. Journal of Consulting and Clinical Psychology, 58(6), 811–817. NIH Consensus Development Panel on Rehabilitation of Persons with Traumatic Brain Injury. (1999). Rehabilitation of persons with traumatic brain injury, Journal of the American Medical Association, 282, 974–983. O’Callaghan, M.E., & Couvadelli, B. (1998). Use of self-instructional strategies with three neurologically impaired adults. Cognitive Therapy and Research, 22(2), 91–107. Ownsworth, T.L., & Mcfarland, K. (1999). Memory remediation in long-term acquired brain injury: Two approaches in diary training. Brain Injury, 13(8), 605–626. Parish, L., & Oddy, M. (2007). Efficacy of rehabilitation for functional skills more than 10 years after extremely severe brain injury. Neuropsychological Rehabilitation, 17(2), 230–243. Poggel, D.A., Kasten, E., & Sabel, B.A. (2004). Attentional cueing improves vision restoration therapy in patients with visual field defects. Neurology, 63(11), 2069–2076. 61 KRISTEN DAMS-O’CONNOR AND WAYNE A. GORDON Polley, D.B., Steinberg, E.E., & Merzenich, M.M. (2006). Perceptual learning directs auditory cortical map reorganization through top-down influences. Journal of Neuroscience, 26(18), 4970–4982. Prigatano, G.P. (1999). Principles of neuropsycholgical rehabilitation. New York: Oxford University Press. Prigatano, G.P., & Schacter, D.L. (1991). Awareness of deficit after brain injury: Clinical and theoretical issues. New York: Oxford University Press. Rassovsky, Y., Satz, P., Alfano, M.S., Light, R.K., Zaucha, K., McArthur, D.L., . . . Hovda, D. (2006). Functional outcome in TBI II: Verbal memory and information processing speed mediators. Journal of Clinical and Experimental Neuropsychology, 28(4), 581–591. Rath, J.F., Simon, D., Langenbahn, D.M., Sherr, R.L., & Diller, L. (2003). Group treatment of problemsolving deficits in outpatients with traumatic brain injury: A randomised outcome study. Neuropsychological Rehabilitation: An International Journal, 13(4), 461–488. Rieger, M., & Gauggel, S. (2002). Inhibition of ongoing responses in patients with traumatic brain injury. Neuropsychologia, 40(1), 76–85. Ruff, R. (2005). Two decades of advances in understanding of mild traumatic brain injury. Journal of Head Trauma Rehabilitation, 20(1), 5–18. Scherzer, B.P. (1986). Rehabilitation following severe head trauma: Results of a three-year program. Archives of Physical Medicine and Rehabilitation, 67(6), 366–374. Serino, A., Ciaramelli, E., Santantonio, A.D., Malagu, S., Servadei, F., & Ladavas, E. (2007). A pilot study for rehabilitation of central executive deficits after traumatic brain injury. Brain Injury, 21(1), 11–19. Shallice, T. (1981). Neurologic impairment of cognitive processes. British Medical Bulletin, 37, 187–192. Silver, J.M., McAllister, J.W., & Yudofsky, S.C. (2005). Textbook of traumatic brain injury (1st ed.). Washington, DC: American Psychiatric Publishing. Simon, D. (2001). Enhancing emotional control in persons with acquired brain damage (abstract). Rehabilitation Psychology, 46, 330. Smith, G.E., Housen, P., Yaffe, K., Ruff, R., Kennison, R.F., Mahncke, H.W., . . . Zelinski, E.M. (2009). A cognitive training program based on principles 62 of brain plasticity: Results from the improvement in memory with plasticity-based adaptive cognitive training (IMPACT) study. Journal of the American Geriatrics Society, 57(4), 594–603. Sohlberg, M., & Mateer, C. (1987). Effectiveness of an attention training program. Journal of Clinical and Experimental Neuropsychology, 9, 117–130. Sohlberg, M., Mateer, C.A., & Stuss, D. (1993). Contemporary approaches to the management of executive dyscontrol. Journal of Head Trauma Rehabilitation, 8, 45–58. Sohlberg, M.M., Avery, J., Kennedy, M., Ylvisaker, M., Coelho, C., Turkstra, L., . . . Yorkston, K. (2003). Practice guidelines for direct attention training. Journal of Medical Speech-Language Pathology, 11(3), 19-20-29. Stratton, M.C., & Gregory, R.J. (1995). After traumatic brain injury: A discussion of consequences. Brain Injury, 8(7), 631–645. Sturm, W., Willmes, K., Orgass, B., & Hartje, W. (1997). Do specific attention deficits need specific training? Neuropsychological Rehabilitation, 7, 81–103. Stuss, D., & Benson, D. (1986). The frontal lobes. New York: Raven Press. Stuss, D.T., Shallice, T., Alexander, M.P., & Picton, T.W. (1995). A multidisciplinary approach to anterior attentional functions. Annals of the New York Academy of Sciences, 769, 191–211. Sun, R., & Zhang, X. (2004). Top-down versus bottomup learning in cognitive skill acquisition. Cognitive Systems Research, 5, 63–89. Tiersky, L.A., Anselmi, V., Johnston, M.V., Kurtyka, J., Roosen, E., Schwartz, T., . . . Deluca, J. (2005). A trial of neuropsychologic rehabilitation in mildspectrum traumatic brain injury. Archives of Physical Medicine and Rehabilitation, 86(8), 1565–1574. von Cramon, D.Y., Matthes-von Cramon, G., & Mai, N. (1991). Problem-solving deficits in brain-injured patients: A therapeutic approach. Neuropsychological Rehabilitation, 1, 45–64. Webb, P., & Glueckauf, R. (1994). The effects of direct involvement in goal setting on rehabilitation outcome in persons with traumatic brain injury. Rehabilitation Psychology, 39(3), 179–188. Wilson, B.A. (1997). Cognitive rehabilitation: How it is and how it might be. Journal of the International Neuropsychological Society, 3(5), 487–496.









© Copyright 2026